Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Relationship Between Dietary Inflammatory Index and All-Cause, Cardiovascular Disease-Related, and Cancer-Related Mortality
Authors Gao Y, Wang Y, Zhang D, Wu T, Li Q
Received 19 June 2023
Accepted for publication 24 August 2023
Published 30 August 2023 Volume 2023:16 Pages 2543—2556
DOI https://doi.org/10.2147/JMDH.S423558
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Yonghong Gao,1 Yan Wang,1 Dandan Zhang,2 Tingting Wu,1 Qingwei Li1
1Department of Cardiology, Shanghai Jinshan District Tinglin Hospital, Shanghai, 201505, People’s Republic of China; 2Department of General Practice, Shanghai Jinshan District Tinglin Hospital, Shanghai, 201505, People’s Republic of China
Correspondence: Qingwei Li, Department of Cardiology, Shanghai Jinshan District Tinglin Hospital, Shanghai, 201505, People’s Republic of China, Email [email protected]
Background: In the general population of the United States (U.S.), the relationship between dietary inflammatory index (DII) and mortality (all-cause, cardiovascular disease (CVD)-related, and cancer-related) is still unclear. Therefore, in this research, we examined the association of DII with mortality caused by all-cause, CVD-related, and cancer-related causes.
Methods: Data from the National Health and Nutrition Examination Survey (NHANES) from 1999– 2018 was used for exploring the link between DII and all-cause, CVD-related, and cancer-related mortality through the use of Cox proportional hazard models and restricted cubic spline model. In addition, subgroup analyses were further performed.
Results: The study included 29,013 individuals from the NHANES from 1999 to 2018. The DII scores were nominated as low (T1: − 5.281– 0.724), medium (T2: 0.725– 2.513), and high-grade inflammation (T3: 2.514– 5.795), with T1 serving as the reference group. The linear positive correlation between DII and all-cause and CVD-related mortality was studied using Cox regression analysis. In the full-adjusted model, as compared with the individuals with T1 DII scores, adjusted odds ratios with 95% confidence intervals for all-cause and CVD-related mortality were 1.149 (1.059, 1.247), and 1.186 (1.084, 1.297), as well as 1.197 (1.032, 1.387), and 1.198 (1.019, 1.409), respectively. However, there was no statistical significance between DII and cancer-related mortality. The RCS plot also showed a significant increase in all-cause and CVD-related mortality with increased DII. Nevertheless, as DII scores increased, cancer-related mortality first increased and then decreased.
Conclusion: All-cause and CVD-related mortality are linked independently to high DII scores, independently. Further study of the association of DII scores with mortality caused by all-cause, CVD-related, and cancer-related causes is necessary to explore.
Keywords: all-cause mortality, cancer-related mortality, cardiovascular disease-related mortality, dietary inflammation index, National Health and Nutrition Examination Survey
Introduction
In the United States (U.S.), cardiovascular disease (CVD) remains the leading cause of death, accounting for about 928,741 deaths in the year 2020.1 In addition, the second leading cause of death is cancer, accounting for about 609,360 deaths in the year 2022.2 The substantially rising absolute numbers of incident and prevalent CVD and cancer cases still need to be urgently addressed in the context of population growth and aging.3 In the recent decade, increased attention to dietary management as one of the ideal cardiovascular health promotion strategies has also been seen globally.4,5 An unhealthy lifestyle and diet have been recognized as one of the underlying pathophysiological processes that contribute to chronic inflammation, which is widely believed to be a cause of many chronic diseases, particularly cancer and CVD.6–9 Healthy diets defined in other ways may work through inflammation, with the Mediterranean diet score, alternative healthy eating index-2010, and dietary inflammatory index (DII) associated with circulating concentrations of inflammatory biomarkers.10,11 In order to assess the overall inflammatory potential of the diets of individuals, the DII was developed.12 To better quantify the pro-inflammatory and anti-inflammatory properties of the diet on a continuum, the DII was introduced by researchers at the University of South Carolina in 2007 and further refined and improved in 2014 based on the validation of nearly two thousand peer-reviewed articles.13 The DII allows us to show the complex interaction between a range of dietary components and various inflammatory markers such as C-reactive protein (CRP); interleukin (IL)-6, −1β, −4, and −10; and tumor necrosis factor (TNF)-α).8,13 There is a high correlation between the DII score and the pro-inflammatory effects of the food, and vice versa, therefore suggesting that the anti-inflammatory effects are stronger the higher the DII score.
Previous research has demonstrated the association between DII and a range of physical and psychological health outcomes, such as mortality caused by all-cause, CVD-related, and cancer-related causes.9,14 Several meta-analyses of observational studies, mainly from Australia, Europe, Japan, and North America, have found an increased risk of CVD and its mortality associated with a pro-inflammatory diet.8,14 However, recently, in the general population of the United States, the strength of the association of DII scores with mortality caused by CVD-related causes is still unclear. For example, as mentioned in a recent meta-analysis, there were only six cohort studies included in their final analysis, and the statistical power might not be well guaranteed.14 The quality and strength of the evidence for the above association have also been challenged by an umbrella review with meta-analyses, wherein weak or lower evidence of CVD mortality and DII was reported in the review.15 Moreover, Li et al did examine three large prospective cohorts from the US and revealed that dietary patterns with a higher proinflammatory property were related to higher CVD incidence; however, they adopted the empirical dietary inflammatory pattern score rather than the DII as the exposure measurement.7 For another, the relationship between the highest quartiles of DII score, as referred to as a pro-inflammatory diet, and all-cause mortality seemed robust in two large Spanish cohorts by 2018, which has been consistent with the previous ten cohort studies, while only four studies from the US and the newest one were from 2017.9,16 Sadeghi found that an increase in lung cancer odds was associated with adherence to a pro-inflammatory diet in adults, particularly among males.17 Shivappa also revealed that those without a history of hepatitis B or C infection and males who consume pro-inflammatory diets are at increased risk for hepatocellular cancer.18 Additionally, according to a meta-analysis of several studies, an association was found between a higher DII and increased cancer incidence, risk, and mortality, consistent across cancer types and across different countries, with a strong and significant positive relationship.19 An updated relationship needs to be reported in order to capture the changing pattern of this association since mortality caused by all-cause, CVD-related, and cancer-related causes has been a significant public health outcome for the general population, and promoting a healthy or lower-inflammatory diet as one of the most cost-effective public health interventions demands up-to-date evidence to further indicate global and national cardiovascular health strategies, especially when facing an aging population.3 The National Health and Nutrition Examination Survey (NHANES) is a cross-sectional survey database that collects information on the health and nutrition of the US household population.20 This database sample was selected using stratified multistage sampling to obtain a representative sample of US residents.21 Data from the NHANES 1999–2018 were used to analyze DII scores within population-based cohorts in the US general population.22 And our study aimed to explore the association of DII with mortality caused by all-cause, CVD-related, and cancer-related causes.
Materials and Methods
Study Population
The NHANES database is an ongoing US national population-based nutrition and health survey. It uses complex, multi-stage, and probability sampling techniques rather than a simple random sample based on the US population. In the study, we removed 8875 participants with missing food-frequency questionnaire data and 35,649 people with missing outcome data from the 96,811 eligible individuals. In addition, we also removed the patient’s missing demographic and biochemical data to ensure the accuracy of the results (n = 23,394). Finally, this study included a total of 29,013 participant (Figure 1). All study procedures were authorized by the National Center for Health Statistics Ethics Review Board prior to data collection, and all participants signed informed consent forms. More information about the data can be found at (https://www.cdc.gov/nchs/nhanes/index.htm).21
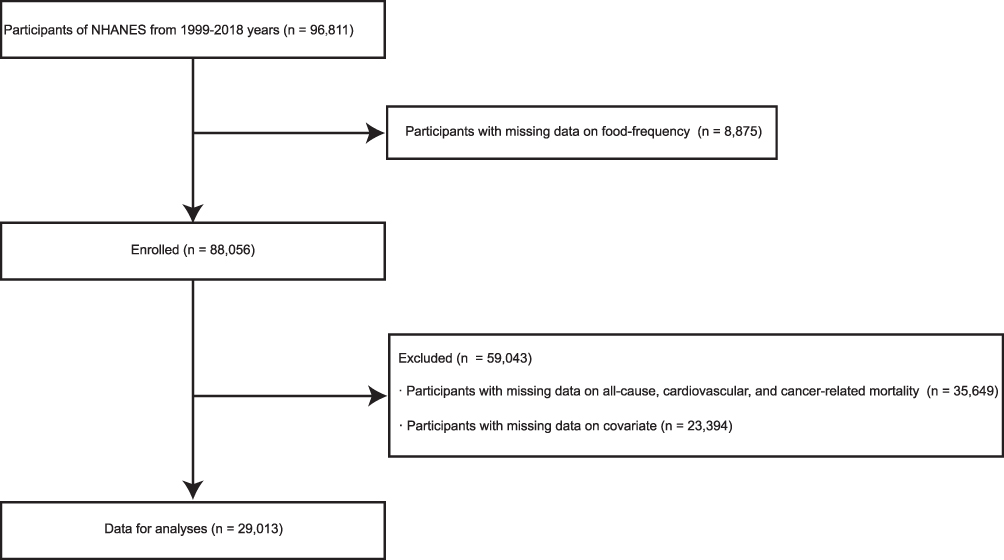 |
Figure 1 Study flow chart. Abbreviation: NHANES, National Health and Nutrition Examination Surveys. |
Calculation of the Dietary Inflammation Index
The DII score system was developed by Shivappa based on a literature review and can be used to assess the potential inflammatory level of dietary components.13 Based on the 24 hours prior to the interview (midnight to midnight), professional staff were able to estimate the total intake of food energy (calories), nutrients, and non-nutrient food components from foods and beverages consumed. The participants were asked to complete a short questionnaire after 24 hours to determine whether the person’s intake on the previous day was usual or unusual, the source of tap water consumed, the use of salt, special diet use, and the frequency of fish and shellfish consumption during the past 30 days.9 Dietary consumption’s effects on inflammation are calculated from 45 nutrients in DII. It is calculated by adding the scores from each component of the diet consumed in 24 hours, including the scores from the pro-inflammatory and anti-inflammatory diets. A Z-score can be calculated by subtracting the global daily mean intake and dividing by the standard deviation, and then the result is converted to a percentile score by doubling each percentile score and subtracting “1” to produce a symmetrical distribution. By multiplying the percentile value by the corresponding “overall inflammation effect score”, we can produce an individual “overall DII score”. In our study, the DII was calculated based on 28 nutrients, including cholesterol, protein, alcohol, carbohydrates, fiber, folic acid, saturated fat, total fat, monounsaturated fatty acids (MUFAs), n-3 fatty acids, polyunsaturated fatty acids (PUFAs), vitamin A/B12/C/D/E, thiamin (vitamin B1), Fe, Mg, n-6 fatty acids, caffeine, niacin, riboflavin (vitamin B2), zinc, selenium, beta-carotene, and energy.23 Detailed calculation procedures of DII are provided in Supplementary Table 1.
All-Cause, CVD-Rated and Cancer-Related Mortality
The National Center for Health Statistics tracked survey participants’ vital status and cause of death from the survey participation interview date until December 31, 2018. The primary outcome was all-cause mortality, which was defined as death from any cause during the study period, including cerebrovascular diseases (I60-I69), malignant neoplasms (C00-C97), nephritis, nephrotic syndrome, and nephrosis (N00-N07, N17-N19, N25-N27), accidents (unintentional injuries) (V01-X59, Y85-Y86), Alzheimer’s disease (G30), diseases of the heart (I00-I09, I11, I13, I20-I51), diabetes mellitus (E10-E14), influenza and pneumonia (J09-J18), chronic lower respiratory diseases (J40-J47), and all other causes (residual). A follow-up examination was conducted as soon as the baseline examination was completed. The secondary outcome was cardiovascular-related mortality, which included death from cerebrovascular diseases (I60–I69) and diseases of the heart (I00–I09, I11, I13, and I20–51). The third outcome was cancer-related mortality, which included deaths owing to malignant neoplasms (C00–C97). We presented in detail the cause of death information (all-cause, CVD-specific, and cancer-specific) and ICD codes in Supplementary Table 2. Additionally, on the NHANES website (https://www.cdc.gov/nchs/nhanes/), you will find a wealth of information regarding this program and its procedures.
Covariates
The covariates include demographic data, test results, lab results, and survey results. Sex, age, education level, race/ethnicity, family poverty income ratio (PIR), and marital status were all included in the demographic data. Waist circumference and body mass index (BMI) were test data. Hemoglobin (Hb), high-density lipoprotein cholesterol (HDL-C), blood urea nitrogen (BUN), triglyceride (TG), serum creatinine (Scr), uric acid (UA), total cholesterol (TC), fast glucose, and estimated glomerular filtration rate (eGFR) were measured in the laboratory. Finally, questionnaire results included information on alcohol use, smoking, the complications of hypertension, diabetes mellitus (DM), heart attack, congestive heart failure (CHF), stroke, angina pectoris, and coronary heart disease (CHD). More information regarding the variables used in this study is available at https://www.cdc.gov/nchs/nhanes/index.htm or Supplementary Table 3.
Statistical Analysis
Statistical analyses were performed using R version 3.6.4 (R Foundation for Statistical Computing, Vienna, Austria) and SPSS version 22.0 (SPSS Inc., Chicago, IL, USA). A P-value < 0.05 was determined to be significant. We used the sample weight provided by NHANES. All continuous variables were presented as mean ± standard. Categorical variables are presented as frequencies and percentages. The differences between groups were tested with one-way analysis of variance (ANOVA) for continuous variables and the chi-square test for categorical variables according to DII scores, respectively. Cox regression analysis model, also known as the proportional risk regression model, is a semi-parametric regression model. This model does not need to assume the distribution of survival analysis, so survival outcome and survival time can be used as dependent variables, and the influence of many factors on survival outcome can be analyzed simultaneously. To examine the association between DII scores and mortality caused by all-cause, CVD-related, and cancer-related, we constructed three Cox regression analysis model three models (Model 1, Model 2, and Model 3). First, model 1 was adjusted for sex and age. Second, model 2 was further adjusted for smoker, race/ethnicity, marital status, family PIR, education level, drinker, the complication of DM, and hypertension. Finally, model 3 was further adjusted for the complications of heart attack, CHD, stroke, angina pectoris, and CHF, fast glucose, waist circumference, BUN, BMI, Hb, TC, UA, TG, Scr, HDL-C, and eGFR. The Kaplan–Meier curves were performed to present the rate of all-cause, CVD-related, and cancer-related mortality. Survival rates for different DII were compared using the Log rank test.
Results
Characteristics of Participants by DII Tertile
DII was divided into tertiles in order to further explore the association of DII with mortality caused by all-cause, CVD-related, and cancer-related causes (Table 1). The DII scores were nominated as low (T1: −5.281–0.724), medium (T2: 0.725–2.513), and high-grade inflammation (T3: 2.514–5.795), with T1 serving as the reference group. Age, the complication of angina pectoris, the levels of fast glucose, TG, Scr, and eGFR, and the incidence of CVD-related and cancer-related mortality had no significant difference among T1, T2, and T3. Additionally, the T3 group occupied the highest proportion of the complications of DM, hypertension, CHD, heart attack, angina pectoris, CHF, and stroke. Individuals in T1 seem to be the youngest, with 20.6% of them being males. Participants in T1 had the lowest fast glucose, waist circumference, BMI, DBP and TC, the highest mean energy intake, family PIR, UA, Hb, Scr, BUN, HDL-C, and eGFR, with higher education. Compared with the T1 and T3 individuals, individuals in T2 had the highest level of SBP.
 |
Table 1 Distribution of Baseline Characteristics of NHANES Cohort Across Tertiles of DII |
Association of DII with All-Cause Mortality
The results of the Cox logistic regression analysis of DII and all-cause mortality is presented in Table 2. After adjusting for all underlying confounding variables, the hazard ratios (HRs) with 95% confidence intervals (CIs) for all-cause mortality across rising tertiles were 1.149 (1.059, 1.247), 1.186 (1.084, 1.297) for DII, compared to T1. The restricted cubic spline plot curve illustrates the linear positive correlation between DII and all-cause mortality (P for nonlinearity = 0.124; Figure 2A). A higher DII score is significantly associated with a higher risk of all-cause mortality.
 |
Table 2 Cox Regression Analysis of DII for All-Cause Mortality in Participants |
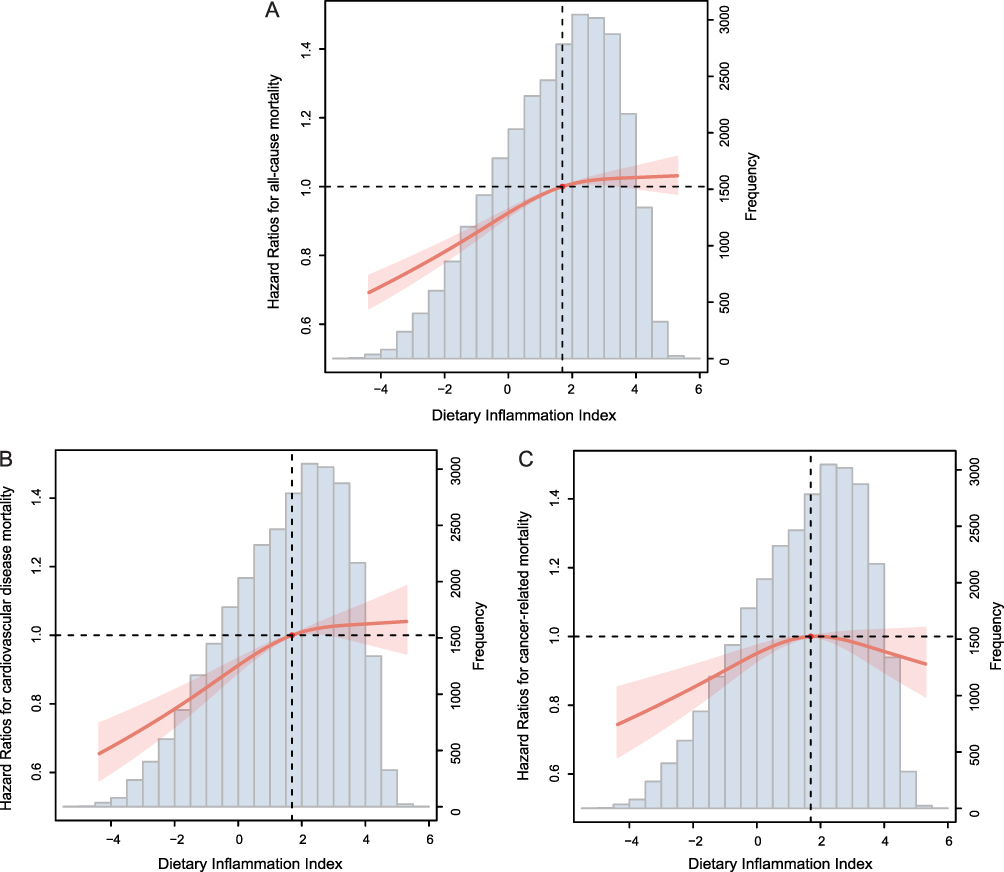 |
Figure 2 The restricted cubic spline plot of the association between DII with (A) all-cause mortality (B) CVD-related mortality (C) cancer-related mortality. Abbreviations: DII, Dietary inflammation index; CVD, cardiovascular disease. |
Association of DII with CVD-Related Mortality
Compared with the lowest quartile (T1), the HRs with 95% CIs for cardiovascular-related mortality across the quartiles were 1.197 (1.032, 1.387), 1.198 (1.019, 1.409) for DII in the fully adjusted model (Table 3). Figure 2B also depicts the linear positive correlation between DII and CVD-related mortality (P for nonlinearity =0.354). A higher DII score is also significantly associated with a higher risk of CVD-related mortality.
 |
Table 3 Cox Regression Analysis of DII for CVD-Related Mortality in Participants |
Association of DII with Cancer-Related Mortality
Compared with the T1, the HRs of cancer-related mortality throughout the tertiles were 1.197 (1.032, 1.387) and 1.198 (1.019, 1.409) for DII (Table 4). There was no significant association between cancer-related mortality and DII. Figure 2C depicts the non-linear association between DII and cancer-related mortality (P for nonlinearity =0.034). Initially, the cancer-related mortality increased with the change in DII, and then it decreased. We found that DII inflection points were at 2.042 in the curve.
 |
Table 4 Cox Regression Analysis of DII for Cancer-Related Mortality in Participants |
Survival Analysis
The Kaplan-Meier survival curves for all individuals stratified by the DII tertiles are shown in Figure 3. Participants in the T3 group had the highest risk of all-cause (Log-rank P <0.001; Figure 3A), CVD-related (Log-rank P <0.001; Figure 3B), and cancer-related mortality (Log-rank P =0.026; Figure 3C).
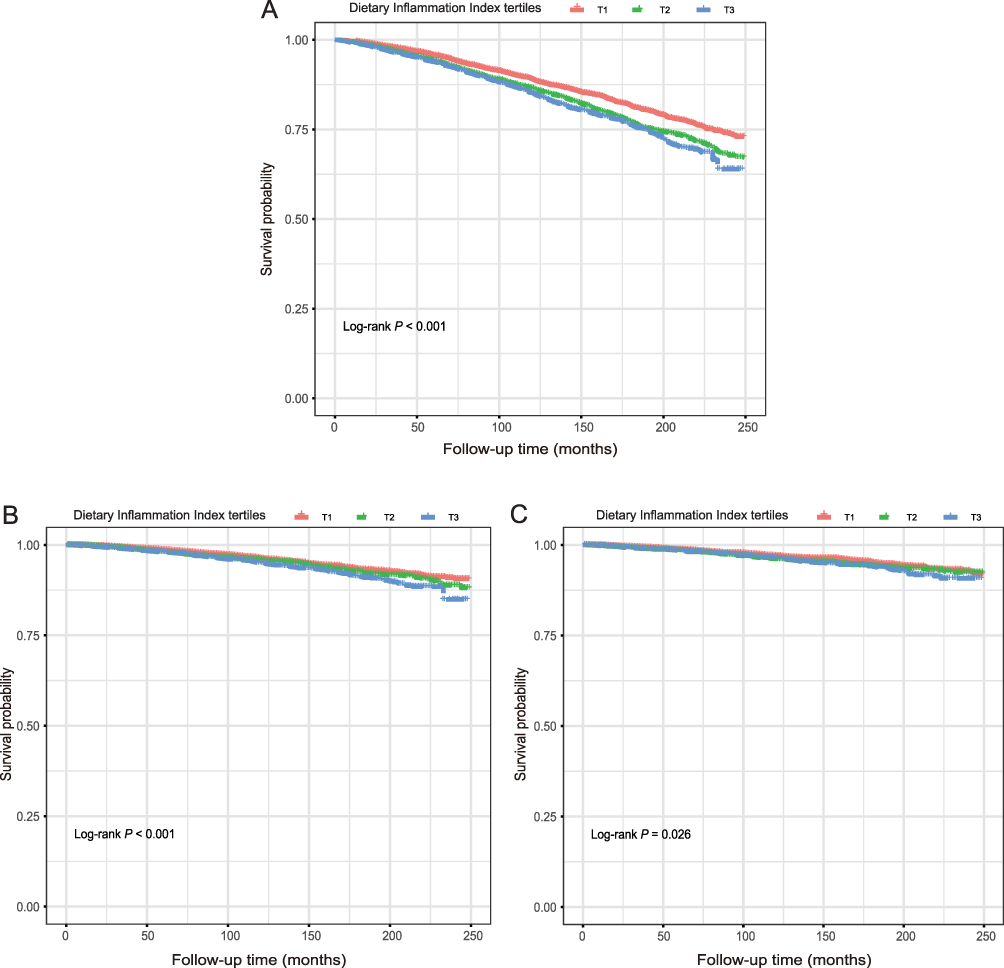 |
Figure 3 Kaplan-Meier survival curve for (A) all-cause mortality (B) CVD-related mortality (C) cancer-related mortality. Abbreviation: CVD, cardiovascular disease. |
Subgroup Analysis
Age, sex, hypertension, DM, and obesity were stratified, and the analysis confirmed positive associations between DII and all-cause mortality in most subgroups. No association was observed between DII and all-cause mortality among participants who aged <60 or ≥60 years, were female, with DM, and with BMI ≥30 kg/m2. The stratified model showed that in age, sex, DM, and obesity populations, the relationship between DII and all-cause mortality was significantly different (Table 5). We further explored the association of DII with CVD-related mortality stratified by age, sex, hypertension, DM, and obesity (Table 6). The hypertension, DM, and obesity-stratified models suggest that the association of DII and CVD-related mortality was significant among participants without hypertension, with DM, and with BMI <30 kg/m2. In addition, the interaction of DII with the hypertension, DM, and obesity status was significant.
 |
Table 5 Subgroups Analysis for the Associations of DII with All-Cause Mortality |
 |
Table 6 Subgroups Analysis for the Associations of DII with CVD-Related Mortality |
Correlation Between DII and Sociodemographic and Cardiovascular Outcomes
The correlation heatmap of DII and covariates revealed that DII was positively associated with gender (correlation coefficient, r = 0.19, P <0.001) and negatively associated with family PIR (correlation coefficient, r = −0.17, P <0.001; Figure 4).
 |
Figure 4 The association between DII and covariates. Abbreviations: DII, dietary inflammation index; family PIR, family poverty-income ratio; smoker, DM, diabetes mellitus; CHD, chronic heart disease; CHF, chronic heart failure; SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; Hb, hemoglobin; BUN, blood urea nitrogen; UA, uric acid; Scr, serum creatinine; HDL-C, high density lipoprotein-cholesterol; TC, total cholesterol; TG, triglycerides; eGFR, estimated glomerular filtration rate. |
Discussion
Through the restricted cubic spline curve, Cox proportional hazard models, survival analysis, and subgroup analysis, we used the data from the large general population between 2013 and 2014 in the US to examine the relationship between DII and mortality caused by all-cause, CVD-related, and cancer-related causes. Our study found a positive and significant association between DII scores and the risk of all-cause and CVD-related mortality. However, the association between the risk of cancer-related mortality and the DII score in our study was not consistent with most of the previous studies.9,24
The results on the association of DII scores with risk of all-cause mortality in our study reassured findings from many prospective cohort studies. However, most studies were conducted based on either data that has not been updated, or population in Europe.9,16,24 In our study, we reached a similar conclusion: individuals with more pro-inflammatory diets, as estimated by the highest tertiles compared to the lowest tertile, were 23% more likely to die from any cause, while in previous studies this percentage has ranged from 8% to 34%.9,24 In addition, we found the attenuation of the direct association at higher tertiles of DII scores when DII was positive, so our results are also consistent with two Spanish cohorts.16 CVD-related mortality, as our secondary outcome, showed the same pattern of a significant association between the risk of CVD-related mortality and DII scores. Two recent meta-analyses have demonstrated a strong association between increasing DII scores and the risk of CVD-related mortality. The consumption of foods with anti-inflammatory properties like fruits and green leafy vegetables could decrease the risk of cardiovascular-related mortality, while people consuming more pro-inflammatory dietary components like processed meat and sugar might be exposed to a higher risk of cardiovascular-related mortality.8,14 Another two cohort studies based on NHANES III dataset have also shown that compared to subjects in tertile 1, those in tertile 3 were 46% and 52% more likely to suffer from CVD, respectively.9,24 Nevertheless, in a previous study including NHANES respondents from 2005–2010, the highest quartile of DII scores was associated with previously self-reported congestive heart failure, heart attack, stroke, and hypertension among women. In other words, individuals who preferred pro-inflammatory diets might be excluded at the baseline.25 Mozos et al found that a variety of dietary components can slow down vascular aging by improving inflammation, endothelial function, platelet function, oxidative stress, controlling vascular tone, apoptosis, and reducing blood pressure both in the short- and long-term. Additionally, several pro-inflammatory foods, including caffeine, meat, sodium, and potassium, are able to increase arterial stiffness and vascular age.26 Our third outcome, cancer-related mortality, showed a pattern of no significant association between DII scores and cancer-related mortality. The pro-inflammatory diet was found to be strongly and independently associated with breast cancer risk, regardless of menopausal status.27 According to Hua, the most pro-inflammatory diets (with the highest DII scores) are associated with an increased risk of upper aerodigestive tract cancer.28 Guo et al suggested that pancreatic cancer risk may be increased by eating a diet characterized by high inflammation (high DII score).29 Shivappa and team also found that a healthier anti-inflammatory diet is important for preventing colorectal cancer.30 Across cancer types, study populations, and study designs, higher DII was consistently associated with higher incidence and mortality of cancer.19 As DII increased, cancer-related mortality increased first and then decreased in this study. A majority of previous DII and cancer-related risk findings were inconsistent with the findings of this study. Additionally, according to the umbrella review of meta-analyses in 2021, the evidence on the strength of the association of DII with mortality, including CVD-related and cancer-related, was still weak.15 Therefore, more relevant studies are encouraged to provide more robust evidence regarding DII and cancer-related mortality.
There is substantial evidence that suggests that diet may play a crucial role in regulating the body’s inflammatory response.4 A growing number of studies have proved that chronic subclinical systemic inflammation is one of the key factors contributing to the pathogenesis of DM, CVD, and certain types of cancer.31–33 Therefore, diet can raise the level of inflammation in the body, which has been associated with mortality. Unhealthy lifestyles may contribute to chronic inflammation. A number of lifestyle factors have been implicated in weight gain and obesity development, with the early work of Kaplan and Kaplan suggesting that one contributing factor to obesity is stress-induced eating, resulting in a preference for nutrient-dense foods, particularly those containing high amounts of sugar and fat.34 Torres SJ also has found that chronic life stress may contribute to weight gain, particularly in men.35 Meanwhile, the environmental conditions in which individuals are living also contribute to obesity. Li T and his team revealed that the beneficial effect of higher diet quality on the risk of obesity could be attenuated by environmental exposure to higher levels of heavy metals (Pb, Hg, and Cd).36 Regular exercise plays a significant role in preventing the development of all-cause mortality, primarily by preventing CVD and DM.37 In addition, Petersen and Pedersen also revealed that the health-beneficial effects of exercise may be mediated by myokines, which in particular may protect against chronic diseases associated with low-grade inflammation, including DM and CVD.38 The risk of mortality from all eight causes examined was reduced by engaging in recommended aerobic physical activity, but engaging in muscle-strengthening activity reduced mortality risk from three causes, including CVD, cancer, and chronic lower respiratory tract diseases.39 Additionally, Li H and his team suggested that high levels of SII may increase total mortality and CVD-related mortality, while physical activity appears to have a beneficial effect on these outcomes.40 Therefore, according to our results, we hypothesized that compared with individuals consuming anti-inflammatory diets, including the fatigue reduction diet, leaky gut diet, Mediterranean diet, and Nordic diet, those consuming pro-inflammatory diets had a higher risk of all-cause and CVD-related mortality. Considering the importance of inflammation in diseases, dietary interventions should be established as early as possible to prevent poor health outcomes.
Strengths of this study included the relatively large sample size, reduced recall bias to the full extent via a 24-hour report, and the adoption of the novel and validated indicator DII to explore the association of inflammatory potentials in diet with all-cause, cardiovascular, and cancer-related mortality. This study also had several limitations. Firstly, the complications of CHF, CHD, angina pectoris, heart attack, and stroke diagnosis were based on personal interviews, which may lead to recall bias. Secondly, the dietary data included in this study were from the participants’ 24-hour daily records, which do not represent their long-term eating habits. Thirdly, due to the cross-sectional study design, we were unable to obtain a causal relationship between DII scores and mortality caused by all-cause, CVD-related, and cancer-related causes. Finally, the study did not exclude bias due to other possible confounding factors that were not taken into account in this study.
Conclusion
According to our study, there is a significant and positive association between the DII and mortality caused by all-cause, and CVD-related, which may allow the DII to be used as a clinical predictor for all-cause and CVD-related mortality. The potential mechanisms of food-derived inflammation in mortality caused by all-cause, CVD-related, and cancer-related causes need further exploration.
Data Sharing Statement
The survey data are publicly available on the internet for data users and researchers throughout the world (www.cdc.gov/nchs/nhanes/).
Ethics Approval and Informed Consent
The NHANES 1999–2018 was approved by the NCHS Research Ethics Review Board (Continuation of Protocol #1999–2018), and each participant signed the written informed consent.
Acknowledgments
The authors thank the staff and the participants of the NHANES study for their valuable contributions.
Funding
This work was supported by the Jinshan District medical health science and technology innovation fund project (2023-WS-59) to Yonghong Gao.
Disclosure
The authors declare that they have no competing interests.
References
1. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics-2023 update: a report from the American Heart Association. Circulation. 2023;147(8):e93–e621. doi:10.1161/CIR.0000000000001123
2. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7–33. doi:10.3322/caac.21708
3. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
4. Galland L. Diet and inflammation. Nutr Clin Pract. 2010;25(6):634–640. doi:10.1177/0884533610385703
5. Phillips CM, Chen LW, Heude B, et al. Dietary inflammatory index and non-communicable disease risk: a narrative review. Nutrients. 2019;11(8):1873. doi:10.3390/nu11081873
6. Ruiz-Canela M, Bes-Rastrollo M, Martínez-González MA. The role of dietary inflammatory index in cardiovascular disease, metabolic syndrome and mortality. Int J Mol Sci. 2016;17(8):1265. doi:10.3390/ijms17081265
7. Li J, Lee DH, Hu J, et al. Dietary inflammatory potential and risk of cardiovascular disease among men and women in the U.S. J Am Coll Cardiol. 2020;76(19):2181–2193. doi:10.1016/j.jacc.2020.09.535
8. Shivappa N, Godos J, Hébert JR, et al. Dietary inflammatory index and cardiovascular risk and mortality-a meta-analysis. Nutrients. 2018;10(2):200. doi:10.3390/nu10020200
9. Deng FE, Shivappa N, Tang Y, Mann JR, Hebert JR. Association between diet-related inflammation, all-cause, all-cancer, and cardiovascular disease mortality, with special focus on prediabetics: findings from NHANES III. Eur J Nutr. 2017;56(3):1085–1093. doi:10.1007/s00394-016-1158-4
10. Li SX, Hodge AM, MacInnis RJ, et al. Inflammation-related marker profiling of dietary patterns and all-cause mortality in the melbourne collaborative cohort study. J Nutr. 2021;151(10):2908–2916. doi:10.1093/jn/nxab231
11. Afshar N, Hodge AM, Shivappa N, et al. Dietary inflammatory index, alternative healthy eating index-2010, mediterranean diet score and the risk of pancreatic cancer. Cancer Epidemiol. 2023;82:102295. doi:10.1016/j.canep.2022.102295
12. Cavicchia PP, Steck SE, Hurley TG, et al. A new dietary inflammatory index predicts interval changes in serum high-sensitivity C-reactive protein. J Nutr. 2009;139(12):2365–2372. doi:10.3945/jn.109.114025
13. Shivappa N, Steck SE, Hurley TG, Hussey JR, Hébert JR. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014;17(8):1689–1696. doi:10.1017/S1368980013002115
14. Ji M, Hong X, Chen M, Chen T, Wang J, Zhang N. Dietary inflammatory index and cardiovascular risk and mortality: a meta-analysis of cohort studies. Medicine. 2020;99(20):e20303. doi:10.1097/MD.0000000000020303
15. Marx W, Veronese N, Kelly JT, et al. The dietary inflammatory index and human health: an umbrella review of meta-analyses of observational studies. Adv Nutr. 2021;12(5):1681–1690. doi:10.1093/advances/nmab037
16. Garcia-Arellano A, Martínez-González MA, Ramallal R, et al. Dietary inflammatory index and all-cause mortality in large cohorts: the SUN and PREDIMED studies. Clin Nutr. 2019;38(3):1221–1231. doi:10.1016/j.clnu.2018.05.003
17. Sadeghi A, Parastouei K, Seifi S, et al. Inflammatory potential of diet and odds of lung cancer: a case-control study. Nutr Cancer. 2022;74(8):2859–2867. doi:10.1080/01635581.2022.2036770
18. Shivappa N, Hébert JR, Polesel J, et al. Inflammatory potential of diet and risk for hepatocellular cancer in a case-control study from Italy. Br J Nutr. 2016;115(2):324–331. doi:10.1017/S0007114515004419
19. Fowler ME, Akinyemiju TF. Meta-analysis of the association between dietary inflammatory index (DII) and cancer outcomes. Int J Cancer. 2017;141(11):2215–2227. doi:10.1002/ijc.30922
20. Xiao S, Wang X, Zhang G, et al. Association of systemic immune inflammation index with estimated pulse wave velocity, atherogenic index of plasma, triglyceride-glucose index, and cardiovascular disease: a large cross-sectional study. Mediators Inflamm. 2023;2023:1966680. doi:10.1155/2023/1966680
21. Ahluwalia N, Dwyer J, Terry A, Moshfegh A, Johnson C. Update on NHANES dietary data: focus on collection, release, analytical considerations, and uses to inform public policy. Adv Nutr. 2016;7(1):121–134. doi:10.3945/an.115.009258
22. Fain JA. NHANES: use of a free public data set. Diabetes Educ. 2017;43(2):151. doi:10.1177/0145721717698651
23. Liu H, Tan X, Liu Z, et al. Association between diet-related inflammation and COPD: findings from NHANES III. Front Nutr. 2021;8:732099. doi:10.3389/fnut.2021.732099
24. Shivappa N, Steck SE, Hussey JR, Ma Y, Hebert JR. Inflammatory potential of diet and all-cause, cardiovascular, and cancer mortality in national health and nutrition examination survey III study. Eur J Nutr. 2017;56(2):683–692. doi:10.1007/s00394-015-1112-x
25. Wirth MD, Shivappa N, Hurley TG, Hébert JR. Association between previously diagnosed circulatory conditions and a dietary inflammatory index. Nutr Res. 2016;36(3):227–233. doi:10.1016/j.nutres.2015.11.016
26. Mozos I, Jianu D, Stoian D, et al. The relationship between dietary choices and health and premature vascular ageing. Heart Lung Circ. 2021;30(11):1647–1657. doi:10.1016/j.hlc.2021.07.009
27. Chen H, Gao Y, Wei N, Du K, Jia Q. Strong association between the dietary inflammatory index(DII) and breast cancer: a systematic review and meta-analysis. Aging. 2021;13(9):13039–13047. doi:10.18632/aging.202985
28. Hua R, Liang G, Yang F. Meta-analysis of the association between dietary inflammatory index (DII) and upper aerodigestive tract cancer risk. Medicine. 2020;99(17):e19879. doi:10.1097/MD.0000000000019879
29. Guo Z, Hong Y, Cheng Y. Dietary inflammatory index and pancreatic cancer risk: a systematic review and dose-response meta-analysis. Public Health Nutr. 2021;24(18):6427–6435. doi:10.1017/S1368980021001579
30. Shivappa N, Godos J, Hébert JR, et al. Dietary inflammatory index and colorectal cancer risk-a meta-analysis. Nutrients. 2017;9(9):1043. doi:10.3390/nu9091043
31. Ridker PM, Cushman M, Stampfer MJ, Tracy RP, Hennekens CH. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. N Engl J Med. 1997;336(14):973–979. doi:10.1056/NEJM199704033361401
32. Shacter E, Weitzman SA. Chronic inflammation and cancer. Oncology. 2002;16(2):
33. Calle MC, Fernandez ML. Inflammation and type 2 diabetes. Diabetes Metab. 2012;38(3):183–191. doi:10.1016/j.diabet.2011.11.006
34. Kaplan HI, Kaplan HS. The psychosomatic concept of obesity. J Nerv Ment Dis. 1957;125(2):181–201. doi:10.1097/00005053-195704000-00004
35. Torres SJ, Nowson CA. Relationship between stress, eating behavior, and obesity. Nutrition. 2007;23(11–12):887–894. doi:10.1016/j.nut.2007.08.008
36. Li T, Yu L, Yang Z, et al. Associations of diet quality and heavy metals with obesity in adults: a cross-sectional study from National Health and Nutrition Examination Survey (NHANES). Nutrients. 2022;14(19):4038.
37. Pedersen BK, Wagenmakers AJM. The anti-inflammatory effect of exercise: its role in diabetes and cardiovascular disease control. Essays Biochem. 2006;42:105–117. doi:10.1042/bse0420105
38. Petersen AM, Pedersen BK. The anti-inflammatory effect of exercise. J Appl Physiol. 2005;98(4):1154–1162. doi:10.1152/japplphysiol.00164.2004
39. Zhao M, Veeranki SP, Magnussen CG, Xi B. Recommended physical activity and all cause and cause specific mortality in US adults: prospective cohort study. BMJ. 2020;370:m2031. doi:10.1136/bmj.m2031
40. Li H, Wu X, Bai Y, et al. Physical activity attenuates the associations of systemic immune-inflammation index with total and cause-specific mortality among middle-aged and older populations. Sci Rep. 2021;11(1):12532. doi:10.1038/s41598-021-91324-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Systemic Immune Inflammation Index with All-Cause, Cardiovascular Disease, and Cancer-Related Mortality in Patients with Cardiovascular Disease: A Cross-Sectional Study
Xiao S, Wang Z, Zuo R, Zhou Y, Yang Y, Chen T, Liu N
Journal of Inflammation Research 2023, 16:941-961
Published Date: 6 March 2023