Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
The Prevalence, Knowledge, and Awareness Level of Atopic Dermatitis Among a Sample of Adult Jordanian Population
Authors Saleh MM ![]() , Al-Qerem W
, Al-Qerem W ![]() , Karaki LA, Al-Zayadneh A, Al-Awawdeh A
, Karaki LA, Al-Zayadneh A, Al-Awawdeh A
Received 12 May 2026
Accepted for publication 26 June 2026
Published 10 July 2026 Volume 2026:19 624003
DOI https://doi.org/10.2147/CCID.S624003
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Monica K. Li
Mais M Saleh,1 Walid Al-Qerem,2 Lubna A Karaki,1 Ayah Al-Zayadneh,1 Ali Al-Awawdeh1
1Department of Pharmaceutics and Pharmaceutical Technology, School of Pharmacy, The University of Jordan, Amman, 11942, Jordan; 2Department of Pharmacy, AlZaytoonah University of Jordan, Amman, Jordan
Correspondence: Mais M Saleh, Email [email protected]
Purpose: Atopic dermatitis (AD) causes significant physical and psychosocial distress. This study aimed to determine the self-reported prevalence of AD and evaluate disease-related knowledge among adult Jordanians.
Methods: A cross-sectional study was conducted from October to December 2025 using a self-administered online questionnaire distributed via social media. Data on sociodemographic characteristics, AD-related knowledge, awareness, clinical features, and treatments were collected from 818 Jordanian adults (aged ≥ 18 years) and analysed using SPSS 28.
Results: While 94.6% of participants had heard of AD, the median knowledge score was suboptimal at 8 (7– 10) out of 14. Awareness was high regarding the necessity of regular moisturization (93.9%) and aggravating role of triggers (≥ 86.5%). However, knowledge gaps were observed regarding the disease’s hereditary nature (45.6% recognizing parental inheritance) and the “atopic march”; few recognized associations with asthma (30.4%) or allergic rhinitis (37.7%). The self-reported AD prevalence was 16.4% (n=134). Affected participants primarily reported itching (65.7%), redness (61.9%), and dryness with skin cracking (60.4%), with the hands being the most affected site (59.7%). Moisturizers were the most common treatment (49.3%), while AD affected daily performance in 42.5% and sleep at night in 41.8% of affected participants. Lower socioeconomic status (among those without AD), male gender, and lack of a family history of AD (among those with AD) were significantly associated with lower knowledge scores.
Conclusion: Detailed knowledge of AD among Jordanian adults is insufficient, with significant gaps in hereditary nature and allergic associations (atopic march). Targeted public health educational initiatives are essential to improve understanding, promote disease self-management, and enhance patient quality of life.
Keywords: atopic dermatitis, atopic march, self-reported prevalence, awareness, knowledge, dermatology, skin disease, cross-sectional studies, Jordan
Introduction
Atopic dermatitis (AD) is a chronic skin condition marked by a cycle of itching, dryness, and inflammatory lesions. As one of the world’s most skin disorders, it impacts individuals of all age groups.1 Epidemiological data suggest approximately 6.3% of adults worldwide suffer from AD, underscores the significant global burden.2 Recent estimates from the Global Burden of Disease Study 2021 indicates that the global AD cases increased from 107 million in 1990 to 129 million in 2021, with projections suggesting a rise to 148 million by 2050.3 The pathogenesis of AD is multifaceted, involving a genetic predisposition, epidermal barrier disruption, immune system dysfunction, and environmental triggers.4 Mechanistically, loss-of-function mutations in the filaggrin (FLG) gene impair skin barrier integrity, increasing transepidermal water loss and allergen penetration.5,6 This disruption is central to disease persistence and the maintenance of chronic inflammation.6 Furthermore, AD is also frequently associated with asthma and allergic rhinitis, a progression known as the “atopic march”.7,8 Highlighting AD as a systemic immune-mediated inflammatory disorder.9
Exacerbations are triggered by environmental irritants, allergens, climate shifts, stress, and microbial colonization, leading to inflammatory flares.10 Management transitions from basic skincare (emollients and trigger avoidance) to topical corticosteroids, calcineurin inhibitors, and systemic immunosuppressants.11 However, achieving optimal disease control remains challenging,12 frequently driven by poor treatment adherence, corticosteroid phobia, and inadequate self-management.13 Patient awareness and knowledge are critical to improving treatment adherence and clinical outcomes.14–16 Many patients lack adequate knowledge regarding the correct topical dosing, such as the fingertip units, leading to suboptimal effectiveness.17 Additionally, corticosteroid phobia negatively influences treatment adherence.16 Consequently, effective management requires extensive patient education on emollients use, bathing techniques, and therapies such as wet wraps9,16,18 to improve disease control and overall quality of life.9
Previous studies identify persistent gaps in understanding disease management and atopic comorbidities18,19 which fuel misconceptions in real-life settings.13,16 Despite growing international and regional literature, epidemiological data and assessment of AD knowledge and awareness among the general adult population in Jordan remain severely lacking, as local research has largely focused on AD therapy in specific subgroups, such as paediatric cohorts or adults.20–22 Accordingly, this study aimed to determine the self-reported prevalence of AD among adult Jordanian and evaluate their disease-related knowledge and awareness to help guide targeted educational and awareness strategies.
Methodology
Study Design and Setting
This study adopted a cross-sectional design aimed at assessing the level of knowledge, awareness, and general attitudes regarding AD via anonymous Google form (one response per participant) targeting the adult Jordanian public between October and December 2025. The study protocol was conducted in strict according to declaration of Helsinki, and approved by the Department of Pharmaceutics and Pharmaceutical Technology and the Institutional Review Board (IRB) of Deanship of Academic Research at the University of Jordan (decision no.489/2025). Participants were fully informed about the research objectives and assured of the confidentiality of all submitted responses, as well as their absolute right to withdraw from the study at any time without consequence. No personally identifiable information was collected.
Data Collection
Data were collected using a structured, digital, self-administered questionnaire created via Google Forms and distributed remotely to the adult population in Jordan. The survey instrument (Supplementary Appendix 1) was adapted from a previously validated and reliable instrument designed by ZahrAllayali et al23 which was successfully deployed to evaluate public AD awareness within a comparable regional demographic in Saudi Arabia. The first section of the questionnaire consists of an informed consent form. The second section (9 questions) is a demographic profile, aimed to collect participants’ demographic data such as gender, age, nationality, location, education, monthly income, employment, marital status, and family history of AD. The third section was about AD knowledge and attitude (a total of 14 true/false questions covering the disease nature, role of treatment, importance of the use of daily moisturizers, risk factors, triggers, and how it affects quality of life). Based on this section items, a 14-point knowledge score was calculated as the sum of equally weighted binary items (one point for each correct response and zero for an incorrect or “I do not know” response); the full scoring key, correct answers, reliability estimate, and threshold used to interpret suboptimal knowledge are provided in the Supplementary Appendix 2.
The fourth section (2 questions) asked about diagnosis with AD, and specialty of the physician. The fifth section (8 questions) is clinical characteristics, including symptoms, affected areas, severity, symptoms frequency, impact on quality of life, and treatment modalities. The clinical manifestations reported in this study were based on participant-reported symptoms. Consequently, disease status was assessed through the subjective perception of disease burden and symptom frequency, rather than clinically measured severity via validated instruments such as the Eczema Area and Severity Index (EASI) or Scoring Atopic Dermatitis (SCORAD).
Tool Translation and Validation
The questionnaire was reviewed for content validity by an expert panel consisting of two dermatology specialists and two clinical pharmacists. The panel assessed the relevance, clarity, and appropriateness of the items in relation to AD knowledge, awareness, clinical characteristics, and treatment-related domains. The Brislin Translation Model24 was then applied to ensure linguistic and conceptual equivalence between the original English instrument and the Arabic version. Two independent translators performed forward translation from English into Arabic, producing two separate Arabic versions. These versions were compared and reconciled by the translators and research team into a single Arabic draft. Subsequently, two independent translators performed independent back-translation from Arabic into English. The back-translated versions were compared with the original English questionnaire, and any discrepancies were discussed and resolved by consensus among the translators and researchers.
To establish face validity and content clarity, a pilot study was conducted with a convenience sample of 10 adult participants selected from diverse demographic backgrounds, in accordance with established methodological guidance for initial cognitive debriefing and pre-testing. Pilot participants completed the digital survey to assess question comprehensibility, identify potential ambiguities in the Arabic phrasing, and determine the average completion time. Minor wording modifications were made to improve readability, while no structural modifications or conceptual changes were required based on participant feedback. Therefore, pilot data were omitted from the final analysis, and the questionnaire was finalized for distribution. Internal consistency of the 14-item binary knowledge score was acceptable in the current sample, with a KR-20/Cronbach’s alpha value of 0.649. A threshold of 0.5 was considered appropriate because the score was based on dichotomous knowledge items, and lower alpha values may be expected with binary response formats.25–28
Sampling and Recruitment
The sample size was calculated for a cross-sectional study using the single-population proportion formula (eq.1). In the absence of reliable national estimates for AD prevalence and awareness in Jordan, a conservative proportion of 50% was assumed to ensure adequate precision. Using a 95% confidence level (Z = 1.96) and a margin of error of 5%, the minimum required sample size was 385 participants. To account for the cluster sampling design (same cluster, ie, same city, same university) (design effect = 1.5) and an anticipated non-response rate of 10%, the final target sample size was increased to approximately 650 participants.

An online questionnaire link was disseminated digitally via sharing its link across various social media platforms, including WhatsApp, Facebook, and Instagram, to maximize reach across different age groups and geographic areas. Participation was entirely voluntary, and the inclusion criteria required respondents to be Jordanian adults aged 18 years or older, currently residing in the Hashemite Kingdom of Jordan, and able to read and understand Arabic.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics version 28.0. Categorical variables were summarized as frequencies and percentages. Participants were classified according to self-reported AD status into those with AD and those without AD. Bivariate associations between AD status and participants’ demographic characteristics, as well as differences in knowledge items between the two groups, were examined using Pearson’s chi-square test. A two-sided p value of less than 0.05 was considered statistically significant.
To evaluate factors associated with AD knowledge among participants without AD, the knowledge score was treated as the dependent variable. Before model construction, the distribution of the knowledge score was assessed using the Shapiro–Wilk test and normal Q–Q plots. These assessments indicated that the knowledge score was not normally distributed; therefore, quantile regression analysis was performed rather than parametric linear regression. The independent variables entered into the model were age group, gender, educational level, monthly income, employment status, marital status, and family history of AD in one of the parents. Regression coefficients, 95% confidence intervals, and corresponding p values were reported.
Multicollinearity among the independent variables was assessed using variance inflation factor values prior to fitting the regression model. No evidence of multicollinearity was identified. Statistical significance was set at p < 0.05 throughout the analysis.
Results
Demographic Information and Clinical Characteristics
Table 1 shows participants’ demographic characteristics. A total of 818 participants were included in the study, of whom 684 (83.6%) reported not suffering from AD and 134 (16.4%) reported suffering from AD. Most participants were aged 21–30 years (57%), the majority of respondents were female (67.1%), while 32.9% were male. Regarding educational level, most participants held a bachelor’s degree (69.1%), and reported a monthly income of 500–1000 JOD (44.5%). More than half of participants were students (44.9%), and most were unmarried (69.3%). Regarding family history of AD, the majority (82%) reported no family history, while 18% reported a positive family history. Bivariate analysis was conducted to assess the association between AD and different demographical variables and the only significant association was found between AD and family history of AD (p value <0.001).
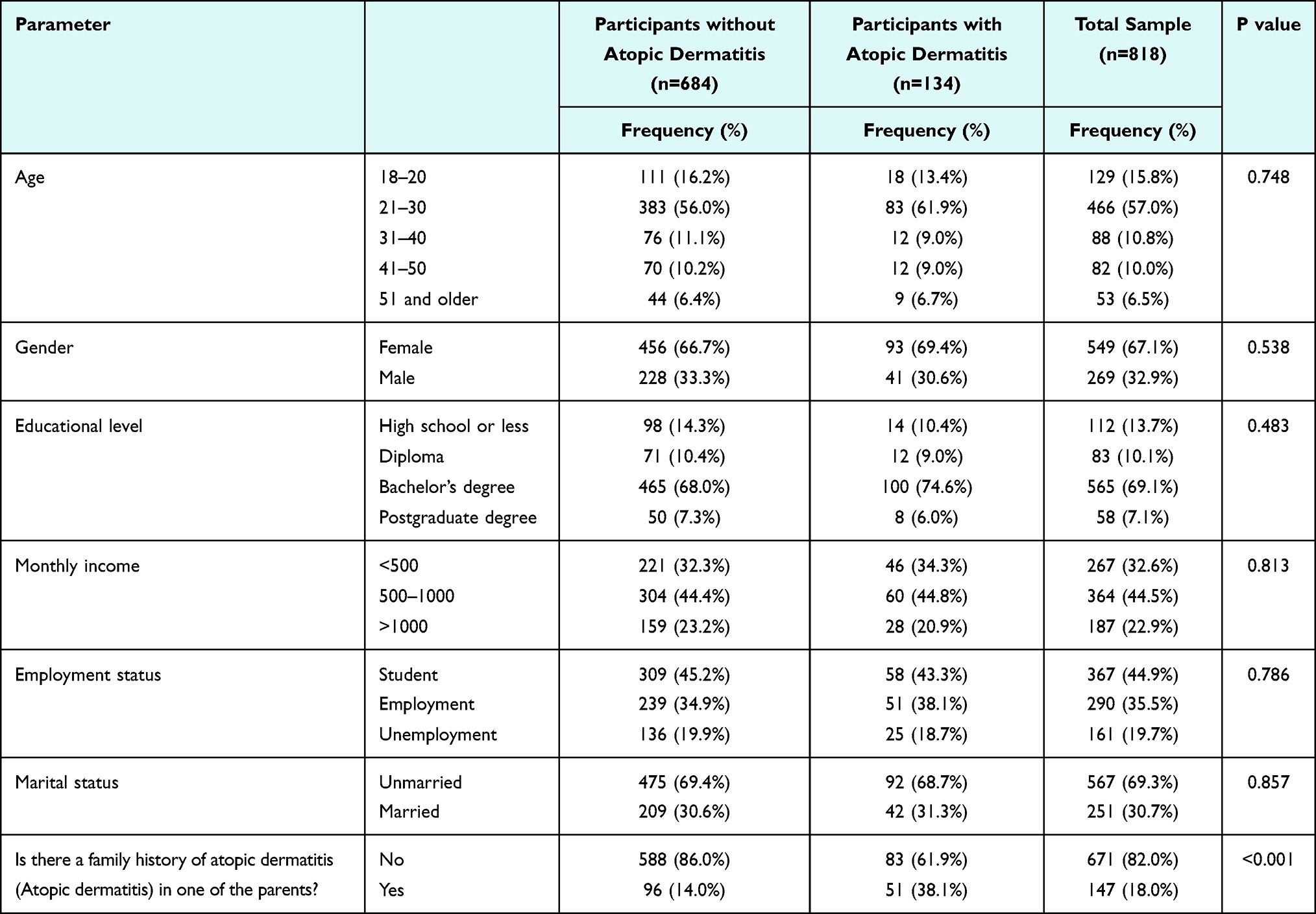 |
Table 1 Participants’ Demographic Characteristics |
Details of the severity of AD and treatment among the patient’s cohort are reported in Figures 1–3 and Table 2. As illustrated in Figure 1, more than half of AD cohort reported itching symptom (65.7%), followed by redness (61.9%) and dryness with skin cracking (60.4%). Small raised bumps were reported by (39.6%), while oozing or scaling with crust formation was the least frequently reported symptom (28.4%). Figure 2 illustrates most commonly affected body sites among AD cohort. The hands were the most commonly reported site of skin rash (59.7%), followed by the face (21.6%) and the chest or back (14.2%). Lower frequencies were reported for the elbow (12.7%), neck (10.4%), ankle (9.0%), knee (7.5%), and sensitive areas (4.5%). Table 2 shows that AD symptoms varied in frequency, with 29.9% of participants reporting rarely symptoms and the same proportion reporting them more than once a week. In addition, (42.5%) stated that AD affected their daily activities or work/study performance, while 41.8% reported that itching disturbed their sleep at night. Figure 3 illustrates treatments used by participants with AD. The most frequently used treatment was moisturizer (49.3%), followed by topical corticosteroids (37.3%) and antihistamines (14.9%), whereas a small portion used chronic corticosteroids (7.5%), topical immunosuppressants (3.7%), and chronic immunosuppressants (1.5%).
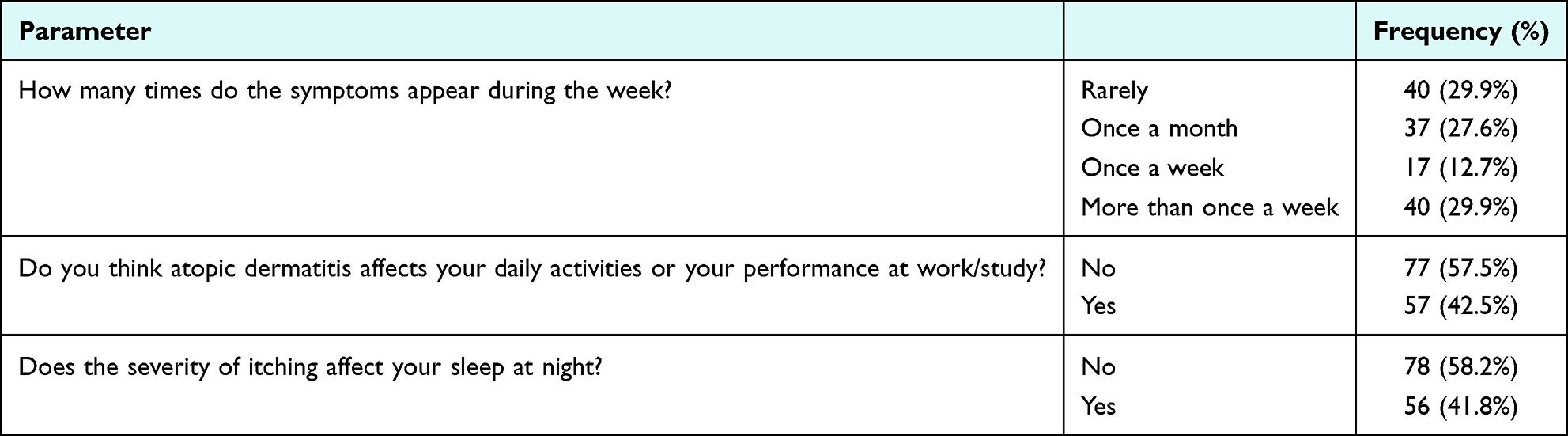 |
Table 2 Severity of Atopic Dermatitis Symptoms Among Patient Cohorts (n=134) |
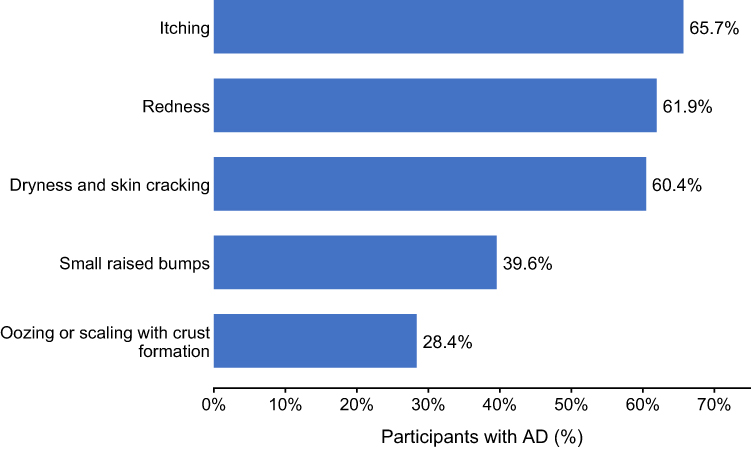 |
Figure 1 Reported skin symptoms among participants with Atopic dermatitis (n=134). |
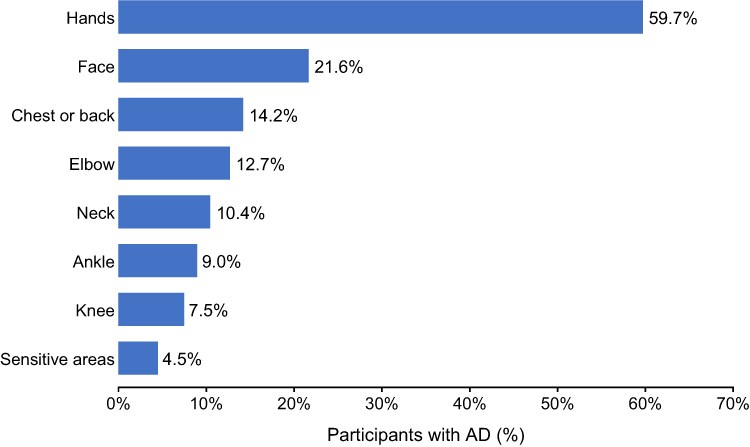 |
Figure 2 Most commonly affected body sites among participants with Atopic dermatitis (n=134). |
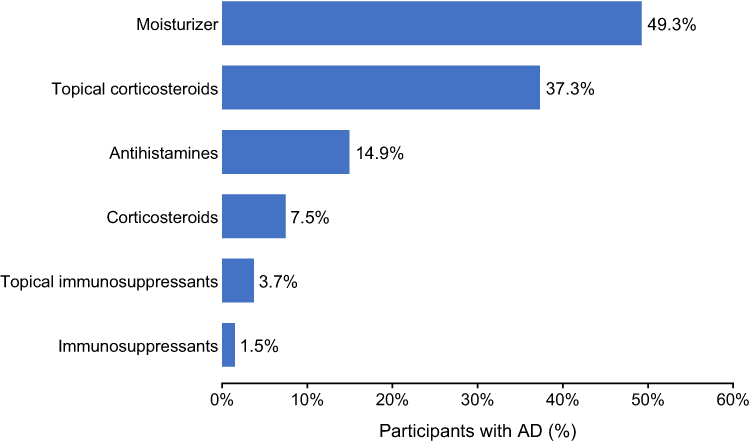 |
Figure 3 Treatments used by participants with Atopic dermatitis (n=134). |
Participants’ Knowledge
Table 3 presents participants’ knowledge regarding AD according to AD status. Overall, the pattern of responses was largely similar between participants without AD and those with AD, with most comparisons showing no statistically significant differences. High proportions of correct responses were observed for having previously heard of AD (94.4% among participants without AD and 95.5% among those with AD), recognizing the importance of daily moisturization in AD treatment (94.0% vs 93.3%), and identifying perfumes or scented soaps as factors that may worsen AD (86.5% vs 87.3%). In contrast, lower proportions of correct responses were reported for items addressing the possible association of AD with asthma (30.7% vs 29.1%) and allergic rhinitis (37.3% vs 39.6%), its effect on school performance (36.4% vs 38.1%), vaccination schedules (24.6% vs 29.9%), and inheritance from a parent (44.3% vs 52.2%). The only statistically significant difference between groups was observed for the item asking whether every child with AD has the disease for life, where correct responses were lower among participants with AD than among those without AD (63.4% vs 74.4%, p = 0.011). The knowledge score distribution is shown in Figure 4. The median score was 8 (IQR 7–10) in the total sample, among participants without AD, and among those with AD; scores ranged from 0–14, 0–14, and 3–13, respectively. Using the prespecified threshold of <10 out of 14 (<70%) to indicate suboptimal knowledge, 556 participants (68.0%) in the total sample were classified as having suboptimal knowledge, including 464 participants without AD (67.8%) and 92 participants with AD (68.7%).
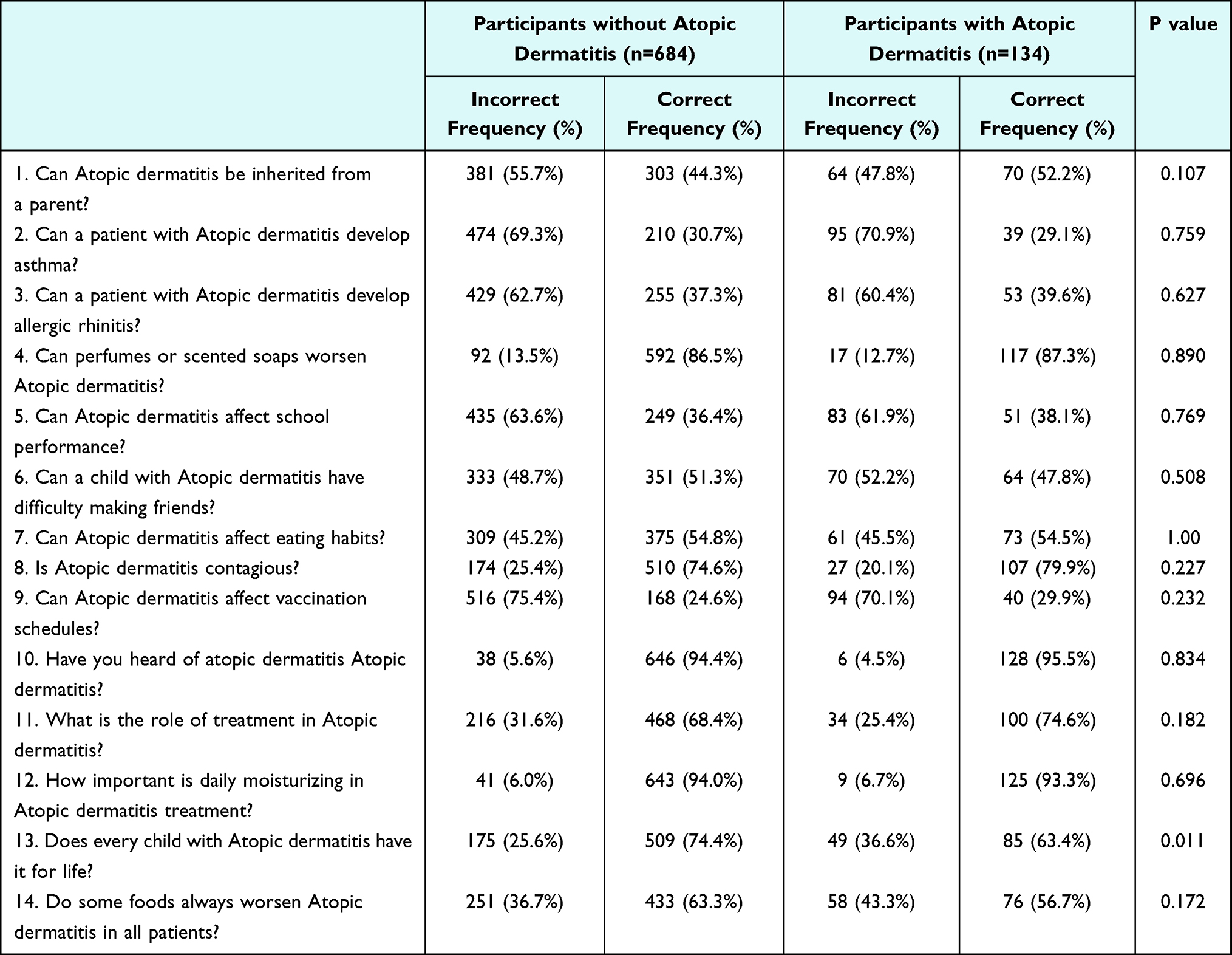 |
Table 3 Participants’ Knowledge Regarding Atopic Dermatitis |
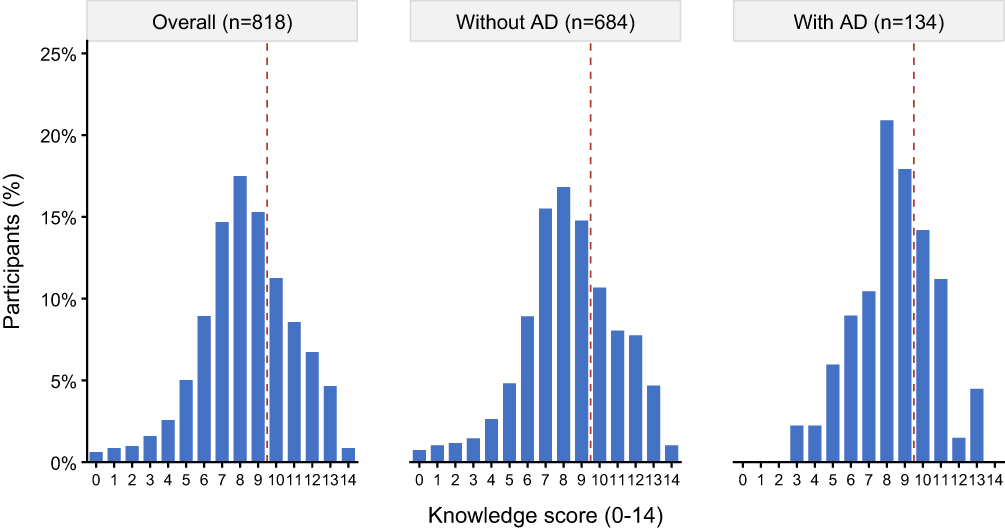 |
Figure 4 Distribution of the 14-point Atopic dermatitis knowledge score overall and according to Atopic dermatitis status (n=818). The dashed line indicates the threshold for adequate knowledge (score of 10 or higher). |
Among participants without AD, the quantile regression model showed that educational level and income were the main predictors of AD knowledge (Table 4). Compared with participants holding a postgraduate degree, lower knowledge scores were observed among those with high school education or less (beta = −2.000, p = 0.002) and those with a diploma (beta = −1.500, p = 0.014), while the association for bachelor’s degree holders did not reach statistical significance (beta = −1.000, p = 0.057). Participants with a monthly income below 500 JOD had lower knowledge scores than those with income above 1000 JOD (beta = −1.000, p = 0.011). Gender, age group, employment status, marital status, and family history of AD were not statistically significant predictors in this subgroup.
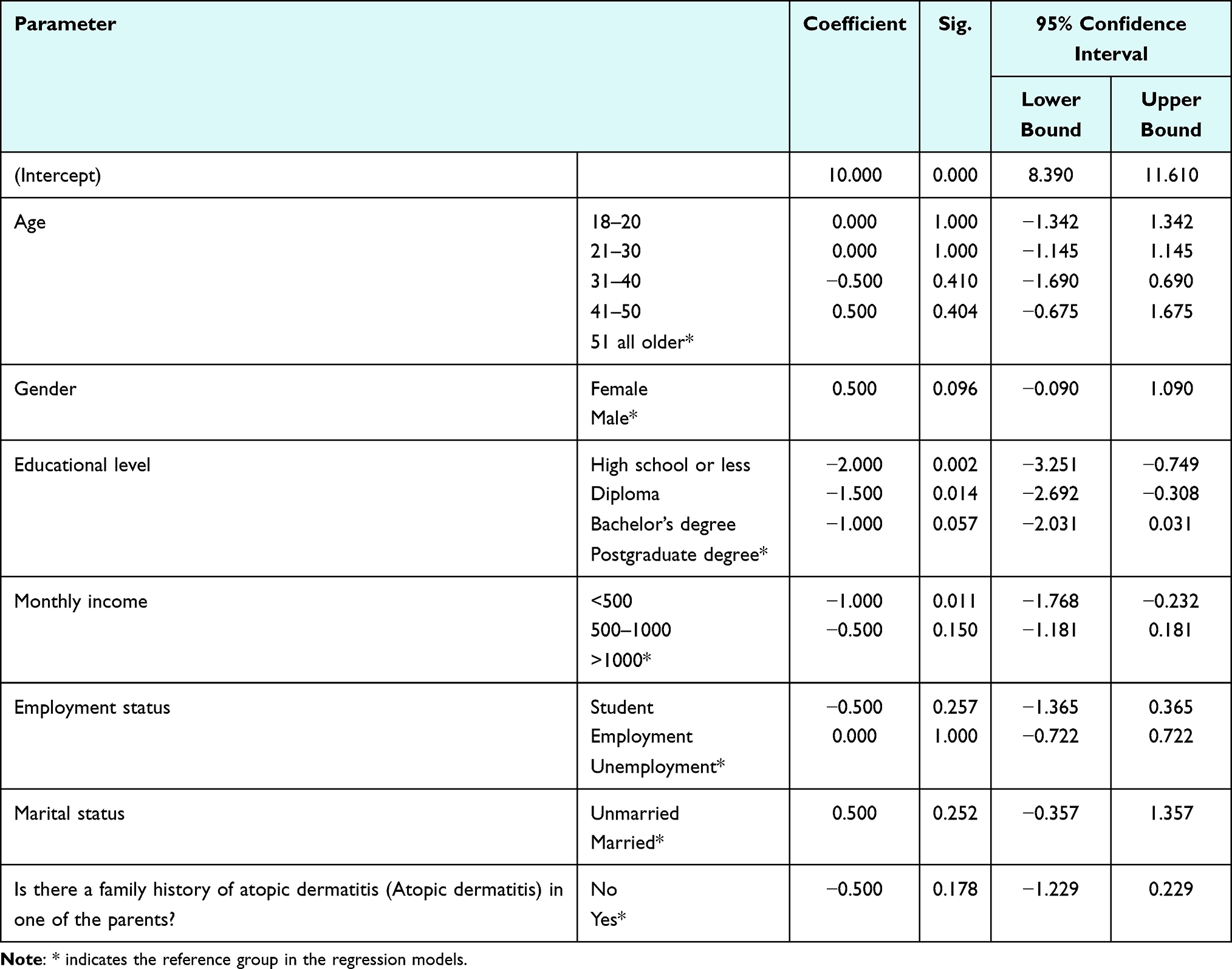 |
Table 4 Quantile Regression Model for Atopic Dermatitis Knowledge Score Among Participants Without Atopic Dermatitis |
Among participants with AD, the regression model showed a different pattern of predictors (Table 5). Female gender was associated with a higher knowledge score compared with male gender (beta = 1.500, p = 0.010), and absence of a family history of AD was associated with a lower knowledge score compared with having a family history (beta = −1.500, p = 0.009). Educational level, monthly income, age group, employment status, and marital status were not statistically significant predictors among participants with AD. These findings should be interpreted with caution because this subgroup was smaller, which produced wider confidence intervals for several predictors.
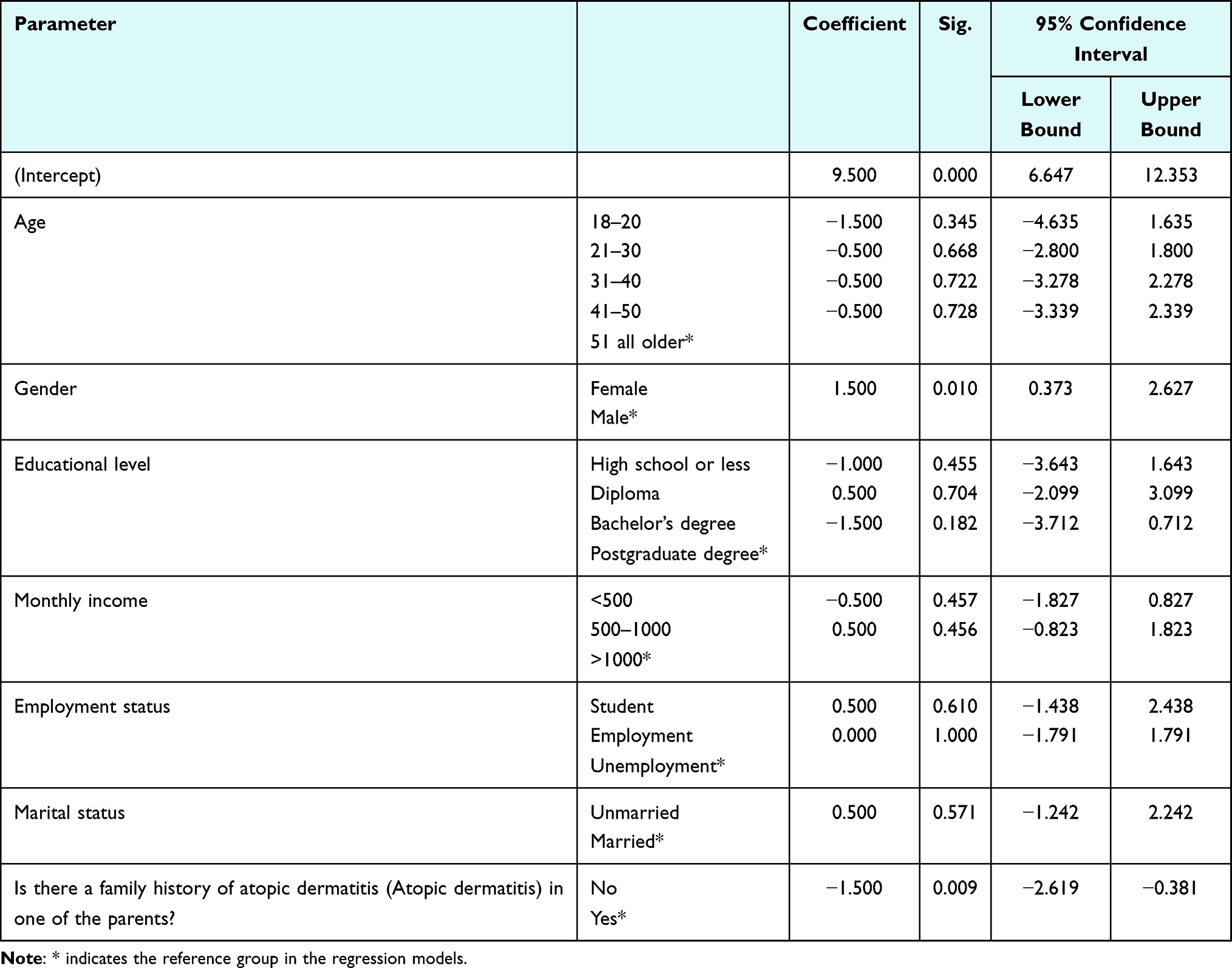 |
Table 5 Quantile Regression Model for Atopic Dermatitis Knowledge Among Participants with Atopic Dermatitis |
Discussion
This study aimed to assess the self-reported prevalence of AD and examine the level of knowledge and attitudes toward it among adults in Jordan. It also sought to provide a clearer understanding of how widespread the condition is within this population. The results are especially significant when compared with prevalence rates reported in other regions.
Our study showed that family history of AD was the only demographic variable significantly associated with AD status, while no significant associations were observed with other sociodemographic factors. Multiple cross-sectional studies have shown that children and adults with a familial history of AD or other atopic conditions have a significantly higher risk of developing AD, supporting the role of inherited defects in skin barrier function and immune regulation.29–31
The results of this study indicate that the self-reported prevalence of AD in this sample of the adult Jordanian population was 16.4%. When compared to the surrounding region, our findings are notably lower than the 30% AD prevalence reported among adult Saudis in one local study,23 yet they align more closely with the other regional data of the international AWARE-1 survey, which reported a comparable prevalence rate of 15.3% in Saudi Arabia.8 In contrast, other Middle Eastern studies report much lower rates; a survey of 4969 respondents in the UAE revealed an AD prevalence of 11.6%,8 a study in Kuwait found a prevalence of 6.4% among young adults aged 18–26 years,32 and a large-scale study of 8110 respondents in Egypt reported a prevalence of only 3.6%.8 Interestingly, these regional studies consistently noted a higher proportion of male respondents.
On a global scale, our findings (16.4%) closely mirror international data from the AWARE-1 survey in Taiwan, which reported a prevalence rate of 17.0%.8 However, wider global data demonstrates significant divergence. For instance, a lifetime prevalence of 21% was reported across all age groups in Finland.33 Conversely, much lower adult prevalence rates have been documented in Western and Asian nations, including 7.3% in the United States,34 4.4% in the European Union, 3.5% in Canada, and 2.1% in Japan.35 This marked global and regional variation likely reflects critical differences in baseline population characteristics, geographic climate, sampling methodologies, and whether the studies relied on self-reported questionnaires or clinically validated diagnostic criteria.36,37
Furthermore, household income demonstrated a significant positive correlation with disease-specific health literacy. Our findings demonstrated that low income group (below 500 JOD) was associated with a lower knowledge score than high an income group (above 1000 JOD). This was similar to a previous study in KSA where public AD Knowledge was significantly correlated with income levels.23
In the current study, the majority of respondents with self-reported AD were female (69.4%) compared to male (30.6%). While this numeric distribution reflects the global trend toward a female majority in adult AD cohorts post-puberty, our analysis confirmed that gender was not statistically significantly associated with AD status. This finding contrasts with larger-scale Western and Middle Eastern epidemiological surveys, which frequently demonstrate a statistically significant female predominance in adulthood that varies from the male predominance seen in childhood cases.1
In the present study, socioeconomic status demonstrated no significant association with AD. This contrasts with a large-scale English study utilizing primary care data from 3.85 million individuals, which identified a nuanced relationship: while higher socioeconomic status correlated with increased AD incidence in infants under age two, an inverse relationship was observed across all other age groups.38
The results of the present study indicate that the participants’ knowledge regarding AD was suboptimal, with 68% demonstrating inadequate knowledge and 32% exhibited good knowledge. In contrast, a study conducted in Saudi Arabia reported that the largest proportion of participants (43%) of demonstrated a fair level of knowledge, 30% had poor knowledge, and 26% exhibited a good knowledge.23 However, awareness of hereditary nature is lower in the current study, as only 45.6% of participants recognized that AD can be passed from parent to child, whereas a higher proportion (56.4%) reported that in cross-sectional study in Saudi Arabia.23
Our finding revealed that the hands among patients with AD is the most affected body site followed by face, chest, elbow, neck, ankle, knee, whereas a study conducted in USA found that the area of AD lesions was mostly in head/neck, followed by hands/fingers, front, upper extremities, and lower extremities.39 Nearly 43% participants reporting symptoms once a week or more which was less compared that of Saudi population (65%).23
In our study, more than half of AD cohort reported itching symptom, redness and dryness with skin cracking. This was similar to an international qualitative study found out that Itch, skin redness, and dry, flak, or scaly skin were the most frequently reported symptoms, with over 75% of patients suffering from these symptoms every 1 to 3 days.40
The most common treatment which was reported in our study is the use of moisturizers (49.3%) followed by topical corticosteroids (37.3%). The use of moisturizers which is an indicator of basic treatment knowledge was less compared to a previous study conducted in parents of children (79% reported using a moisturizers).21 However, the low usage of advanced therapies (topical or systemic immunosuppressants) may reflect either a limited access and negative attitudes toward systemic medications which is a trend often seen in regional studies.
Limitations
This study is subject to several limitations. First, AD diagnosis was entirely self-reported by participants without clinical confirmation by a dermatologist. Consequently, this may lead to an overestimation or misclassification of prevalence rates, hence further studies using clinically validated criteria are needed to confirm the exact prevalence. Second, due to the survey-based nature of the study, a validated clinical severity assessment (such as Scoring Atopic Dermatitis (SCORAD)) was not performed, limiting our ability to correlate knowledge levels with objective disease severity. Third, the remote online recruitment via social media introduces potential selection bias and limits generalizability to the broader Jordanian population, as the sample was skewed toward younger adults and females, ie, a demographic imbalance observed in similar regional electronic surveys.41 Finally, exclusive reliance on a digital platform introduces selection bias by restricting participation to individuals with device access, stable internet connectivity, and functional digital literacy. This requirement potentially underrepresents older or lower-income populations.
Conclusions
This study demonstrates that AD knowledge among adult Jordanians is suboptimal, despite widespread recognition. While most participants were familiar with AD and moisturization benefits, significant gaps persist regarding inheritance, systemic comorbidities, and topical treatments. To translate these findings into clinical utility, we propose a multi-tiered public health framework. First, standardized patient education protocols should be integrated into routine primary care encounters and community pharmacy consultations. Second, health authorities must lead national, culturally tailored awareness campaigns using digital platforms and Arabic-language materials. These targeted interventions are crucial for enhancing self-management, reducing stigma, and improving treatment adherence in Jordan.
Acknowledgment
The authors would like to express their sincere gratitude to Abdulrahman Al-Ghazawi, Khaled Al-Zaheri, Bashar Nawafleh, Rahmeh Almadani, Sara Khalifah, Hadeel Al-Masri, Aya Othman, Dana Al-Zubi, and Sara Nofal for their invaluable assistance and dedicated efforts in the data collection process of this study.
Author Contributions
All authors made substantial contributions to the work reported, whether in the conception, study design, execution, data acquisition, or analysis and interpretation. Specifically: M.M.S. contributed to conceptualization, methodology, investigation, data collection, drafting, and critical revision of the manuscript. W.Q. contributed to formal analysis, data interpretation, and critical revision of the manuscript. L.K. and A.Z. contributed to questionnaire development, data collection, drafting, and critical revision of the manuscript. A.A. contributed to data collection, drafting, and critical revision of the manuscript. Ultimately, all listed authors fulfilled the five mandatory authorship conditions of the journal: they actively participated in drafting or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work’s integrity and accuracy.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Bylund S, Kobyletzki LB, Svalstedt M, Svensson Å. Prevalence and incidence of atopic dermatitis: a systematic review. Acta Derm Venereol. 2020;100(12):adv00160. doi:10.2340/00015555-3510
2. Migliavaca CB, Lazzarini R, Stein C, et al. Prevalence of atopic dermatitis: a systematic review and meta-analysis. Dermat Contact Atopic Occup Drug. 2025;36(6):575–13. doi:10.1089/derm.2024.0165
3. Oh J, Kim S, Kim MS, et al. Global, regional, and national burden of asthma and atopic dermatitis, 1990–2021, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Respir Med. 2025;13(5):425–446. doi:10.1016/S2213-2600(25)00003-7
4. Yang G, Seok JK, Kang HC, Cho YY, Lee HS, Lee JY. Skin barrier abnormalities and immune dysfunction in atopic dermatitis. Int J Mol Sci. 2020;21(8):2867. doi:10.3390/ijms21082867
5. Schuler CF, Tsoi LC, Billi AC, Harms PW, Weidinger S, Gudjonsson JE. Genetic and immunological pathogenesis of atopic dermatitis. J Invest Dermatol. 2024;144(5):954–968. doi:10.1016/j.jid.2023.10.019
6. Stefanovic N, Irvine AD. Filaggrin and beyond: new insights into the skin barrier in atopic dermatitis and allergic diseases, from genetics to therapeutic perspectives. Ann Allergy Asthma Immunol. 2024;132(2):187–195. doi:10.1016/j.anai.2023.09.009
7. Afshari M, Kolackova M, Rosecka M, Čelakovská J, Krejsek J. Unraveling the skin; a comprehensive review of atopic dermatitis, current understanding, and approaches. Front Immunol. 2024;15:1361005. doi:10.3389/fimmu.2024.1361005
8. Maspero J, De Paula Motta Rubini N, Zhang J, et al. Epidemiology of adult patients with atopic dermatitis in AWARE 1: a second international survey. World Allergy Organ J. 2023;16(3):100724. doi:10.1016/j.waojou.2022.100724
9. Kapur S, Watson W, Carr S. Atopic dermatitis. Allergy Asthma Clin Immunol. 2018;14(2):52. doi:10.1186/s13223-018-0281-6
10. Tamagawa-Mineoka R, Katoh N. Atopic dermatitis: identification and management of complicating factors. Int J Mol Sci. 2020;21(8):2671. doi:10.3390/ijms21082671
11. Sidbury R, Alikhan A, Bercovitch L, et al. Guidelines of care for the management of atopic dermatitis in adults with topical therapies. J Am Acad Dermatol. 2023;89(1):e1–e20. doi:10.1016/j.jaad.2022.12.029
12. Andrade LF, Abdi P, Mashoudy KD, et al. Effectiveness of atopic dermatitis patient education programs - a systematic review and meta-analysis. Arch Dermatol Res. 2024;316(5):135. doi:10.1007/s00403-024-02871-y
13. Kim JE, Lee YB, Lee JH, et al. Disease awareness and management behavior of patients with atopic dermatitis: a questionnaire survey of 313 patients. Ann Dermatol. 2015;27(1):40–47. doi:10.5021/ad.2015.27.1.40
14. Khela J, Wilken B, Asai Y. Knowledge assessment tools in atopic dermatitis patient education: a scoping review. Allergy Asthma Clin Immunol. 2025;21(1):26. doi:10.1186/s13223-025-00970-7
15. Chow S, Seow CS, Dizon MV, et al. A clinician’s reference guide for the management of atopic dermatitis in Asians. Asia Pac Allergy. 2018;8(4):e41. doi:10.5415/apallergy.2018.8.e41
16. Wilken B, Zaman M, Asai Y. Patient education in atopic dermatitis: a scoping review. Allergy Asthma Clin Immunol. 2023;19(1):89. doi:10.1186/s13223-023-00844-w
17. Matsuki F, Suzuki S, Hirose T, et al. Prescription and application adequacy of topical corticosteroids based on the finger-tip unit method in adult patients with atopic dermatitis: a cross-sectional study. J Gen Fam Med. 2025;26(6):547–554. doi:10.1002/jgf2.70055
18. Nie Z, Fan P, Zhou Y, Han S. Knowledge, attitudes, and practices in adult patients and parents of pediatric atopic dermatitis patients: a cross-sectional study. Front Public Health. 2024;12:1460044. doi:10.3389/fpubh.2024.1460044
19. Zheng H, Shen C, Xu D, et al. Knowledge, attitudes, and practices towards atopic dermatitis among parents of children with atopic dermatitis: a cross-sectional study. J Asthma Allergy. 2026;19:571448. doi:10.2147/JAA.S571448
20. Alzyoud R. Off-label use of omalizumab in a 6-year-old child with severe atopic dermatitis. Qatar Med J. 2022;2022(2):21. doi:10.5339/qmj.2022.fqac.21
21. Muhaidat J, Fawwaz AM, Al-Qarqaz F, et al. Moisturizer use in children with atopic dermatitis: real-life practice, beliefs, and challenges among a cohort of Jordanian patients. Pediatr Dermatol. 2025;42(2):289–295. doi:10.1111/pde.15821
22. Qeyam H, Al-Shaimi R, Alfattah NA, et al. The hidden epidemic of topical steroid use: prevalence and impact among Jordan’s general population. Clin Cosmet Invest Dermatol. 2025;18:2285–2295. doi:10.2147/CCID.S553615
23. ZahrAllayali AM, Allbdi DS, Alanazi TF, Alhumaidan LS, Albarrak SK, Aldhafiri HJ. The prevalence, knowledge and attitude regarding atopic dermatitis among adult population in Saudi Arabia. Dermatol Dermat. 2024;9. doi:10.31579/2578-8949/152
24. Brislin RW. Back-translation for cross-cultural research. J Cross-Cult Psychol. 1970;1(3):185–216. doi:10.1177/135910457000100301
25. Al-Qerem W, Jarab AS, Qarqaz R, Hayek MA. Attitudes of a sample of Jordanian young adults toward different available COVID-19 vaccines. Vacunas. 2022;23:S56–S63. doi:10.1016/j.vacun.2021.07.008
26. Sharma DB. A focus on reliability in developmental research through Cronbach’s Alpha among medical, dental and paramedical professionals. Asian Pac J Health Sci. 2016;3(4):271–278. doi:10.21276/apjhs.2016.3.4.43
27. Cortina JM. What is coefficient alpha? An examination of theory and applications. J Appl Psychol. 1993;78(1):98–104. doi:10.1037/0021-9010.78.1.98
28. Streiner DL, Norman GR, Cairney J. Health Measurement Scales: A Practical Guide to Their Development and Use. Oxford University Press; 2014. doi:10.1093/med/9780199685219.001.0001
29. Apfelbacher CJ, Diepgen TL, Schmitt J. Determinants of eczema: population-based cross-sectional study in Germany. Allergy. 2011;66(2):206–213. doi:10.1111/j.1398-9995.2010.02464.x
30. Irvine AD, McLean WHI, Leung DYM. Filaggrin mutations associated with skin and allergic diseases. N Engl J Med. 2011;365(14):1315–1327. doi:10.1056/NEJMra1011040
31. Nutten S. Atopic dermatitis: global epidemiology and risk factors. Ann Nutr Metab. 2015;66 Suppl 1(Suppl. 1):8–16. doi:10.1159/000370220
32. Ziyab AH. Prevalence and risk factors of asthma, rhinitis, and eczema and their multimorbidity among young adults in Kuwait: a cross-sectional study. BioMed Res Int. 2017;2017:2184193. doi:10.1155/2017/2184193
33. Kiiski V, Salava A, Susitaival P, Barnhill S, Remitz A, Heliovaara M. Atopic dermatitis in adults: a population-based study in Finland. Int J Dermatol. 2022;61(3):324–330. doi:10.1111/ijd.15912
34. Chiesa Fuxench ZC, Block JK, Boguniewicz M, et al. Atopic dermatitis in America study: a cross-sectional study examining the prevalence and disease burden of atopic dermatitis in the US adult population. J Invest Dermatol. 2019;139(3):583–590. doi:10.1016/j.jid.2018.08.028
35. Barbarot S, Auziere S, Gadkari A, et al. Epidemiology of atopic dermatitis in adults: results from an international survey. Allergy. 2018;73(6):1284–1293. doi:10.1111/all.13401
36. Mahmoud O, Yosipovitch G, Attia E. Burden of disease and unmet needs in the diagnosis and management of atopic dermatitis in the Arabic population of the Middle East. J Clin Med. 2023;12(14):4675. doi:10.3390/jcm12144675
37. Volke A, Toompere K, Laisaar KT, et al. 12-month prevalence of atopic dermatitis in resource-rich countries: a systematic review and meta-analysis. Sci Rep. 2022;12(1):15125. doi:10.1038/s41598-022-19508-7
38. de Lusignan S, Alexander H, Broderick C, et al. The epidemiology of eczema in children and adults in England: a population-based study using primary care data. Clin Exp Allergy J Br Soc Allergy Clin Immunol. 2021;51(3):471–482. doi:10.1111/cea.13784
39. Lio PA, Wollenberg A, Thyssen JP, et al. Impact of atopic dermatitis lesion location on quality of life in adult patients in a real-world study. J Drugs Dermatol JDD. 2020;19(10):943–948. doi:10.36849/JDD.2020.5422
40. Wollenberg A, Gooderham M, Katoh N, et al. Patient-reported burden in adults with atopic dermatitis: an international qualitative study. Arch Dermatol Res. 2024;316(7):380. doi:10.1007/s00403-024-03130-w
41. Saleh MM, Awwad O, Abdel Jalil MH, et al. Correlation of skin cancer and actinic keratosis-related knowledge and sun protection behaviors and sunscreen use among a sample of Jordanian population. J Cosmet Dermatol. 2022;21(12):7066–7074. doi:10.1111/jocd.15377
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence of Skin Disease and Its Associated Factors Among Primary Schoolchildren: A Cross-Sectional Study from a Northern Ethiopian Town
Mengist Dessie A, Fenta Feleke S, Getaye Workie S, Getinet Abebe T, Mossu Chanie Y, Kassa Yalew A
Clinical, Cosmetic and Investigational Dermatology 2022, 15:791-801
Published Date: 29 April 2022
Caregiver Perspectives on Physiotherapy Treatment for Paediatric Burns in the United Arab Emirates
Mohamed Muftah Alzaabi FS, Bairapareddy KC, Alaparthi GK, Hegazy F
Patient Preference and Adherence 2022, 16:1477-1486
Published Date: 17 June 2022
The Prevalence of Complementary and Alternative Medications Use Among Dermatology Patients in Aseer Region, Saudi Arabia
Al-Atif HM, AL-Ghamdi HS, Alzubaidi WA, Alnaem NM, Qahtani SH
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2607-2615
Published Date: 6 December 2022
Improving Psychological Health Outcomes in Children with Atopic Dermatitis
Mostafa N, Smith SD
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2821-2827
Published Date: 10 October 2023
Depression Among University Students in Jordan After the COVID-19 Pandemic: A Cross-Sectional Study
Alhemedi AJ, Qasaimeh MG, Abdo N, Elsalem L, Qaadan D, Alomari E, lssa Q, Alhadeethi M, Abdul Kareem HM, Almasri A, Elkhateeb O, Naser AY
Psychology Research and Behavior Management 2023, 16:4237-4249
Published Date: 18 October 2023