Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Improving Psychological Health Outcomes in Children with Atopic Dermatitis
Received 26 August 2023
Accepted for publication 3 October 2023
Published 10 October 2023 Volume 2023:16 Pages 2821—2827
DOI https://doi.org/10.2147/CCID.S393254
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Niyaz Mostafa,1 Saxon D Smith2
1Faculty of Medicine, The University of Sydney, Sydney, NSW, Australia; 2ANU Medical School, ANU College of Health and Medicine, The Australian National University, Canberra, ACT, Australia
Correspondence: Niyaz Mostafa, Email [email protected]
Introduction: Atopic dermatitis (AD) is a chronic inflammatory skin disease that usually develops in early childhood. AD has a significant impact on quality of life and psychological health outcomes in both adults and children. There are increased reported rates of psychiatric comorbidities including anxiety, depression, ADHD and suicidal ideation compared to the general population. Primary caregivers of children with pediatric eczema and their families may also have derangements in psychological health and quality of life. A number of interventions exist for AD and address wellbeing outcomes as an important aspect of effective treatment.
Methods: A comprehensive literature search was conducted using PubMed/Medline, Embase, the Cochrane Central Register of Controlled Trials in February 2023. Published studies up to April 2023 were included related to interventions for childhood AD that included psychological health or quality of life outcomes. These interventions were stratified according to type and evidence quality.
Results: Search strategy revealed a wide variety of interventions with demonstrated improvements in quality of life or wellbeing of patients with pediatric AD or their families. Both pharmacological and non-pharmacological interventions demonstrated effectiveness in improving disease outcomes.
Conclusion: A variety of both pharmacological and non-pharmacological interventions may be employed to improve psychological health outcomes in children with AD.
Keywords: eczema, atopic dermatitis, psychology, wellbeing, children, pediatric
Introduction
Atopic dermatitis (AD) is a chronic inflammatory skin disease that usually develops in early childhood. The disease is characterised by the presence of pruritic, scaly and erythematous lesions that are relapsing and remitting.1 The worldwide prevalence of AD in children is estimated to be as high as 15%.2 These rates of prevalence are growing worldwide, and vary based on geographical location.3
AD has a significant impact on quality of life and psychological health outcomes in both adults and children. Symptoms of AD, specifically pruritus, are associated with a lower health-related quality of life.4 AD also has a serious impact on the mental health of both adults and children, with increased reported rates of psychiatric comorbidities including anxiety, depression, ADHD and suicidal ideation compared to the general population.5,6 Primary caregivers of children with chronic illness may also be adversely affected.7 Previous reports of parents of children with AD have been demonstrated to have increased rates of stress, anxiety, depression and suicidal ideation than those without.8,9 These effects on quality of life extend beyond parents and can affect families of children with AD across various domains including sleep, relationships and finances.10
Across the literature, a wide variety of interventions have been investigated for AD, ranging from medical therapies to therapeutic adjuncts such as educational programs.11,12 Given the significant burden of AD on psychological health and quality of life (QoL), improvements in these domains have become an important indicator for effectiveness when investigating interventions. Various outcome measures exist to quantify changes in mental health status, which directly address related symptoms of mental health derangement.13 However, an increasingly used measure related to wellbeing and psychological health are health-related quality of life (HRQoL) outcome measures, such as the dermatology life quality index (DLQI) and the children’s dermatology life quality index (CDLQI).14,15 These measures, including the DLQI, have previously demonstrated correlation with psychiatric outcome measures.16 In paediatric eczema, a number of studies have utilised HRQoL measures as a marker for holistic health and improvements in wellbeing. However, there is limited literature summarising the interventions that may improve HRQoL and psychological outcomes in childhood AD.
In order to address this knowledge gap, this review article aims to identify and stratify strategies to improve psychological health outcomes in children with atopic dermatitis.
Methods
A comprehensive literature search was conducted using PubMed/Medline, Embase, the Cochrane Central Register of Controlled Trials in February 2023. Variations of the search terms “atopic dermatitis” and “children” and “quality of life” or “psychology” were combined either as text words or MESH headings. Published studies up to April 2023 were included. Any study investigating a form of intervention for children or caregivers of children with AD in atopic dermatitis was included if they reported any quality of life outcome or anecdotal mention of psychological health or quality of life improvement. The highest level of evidence and grade of recommendation was noted for each intervention, using a modified version of the Oxford Centre for Evidence-based Medicine levels of evidence table (Table 1).17
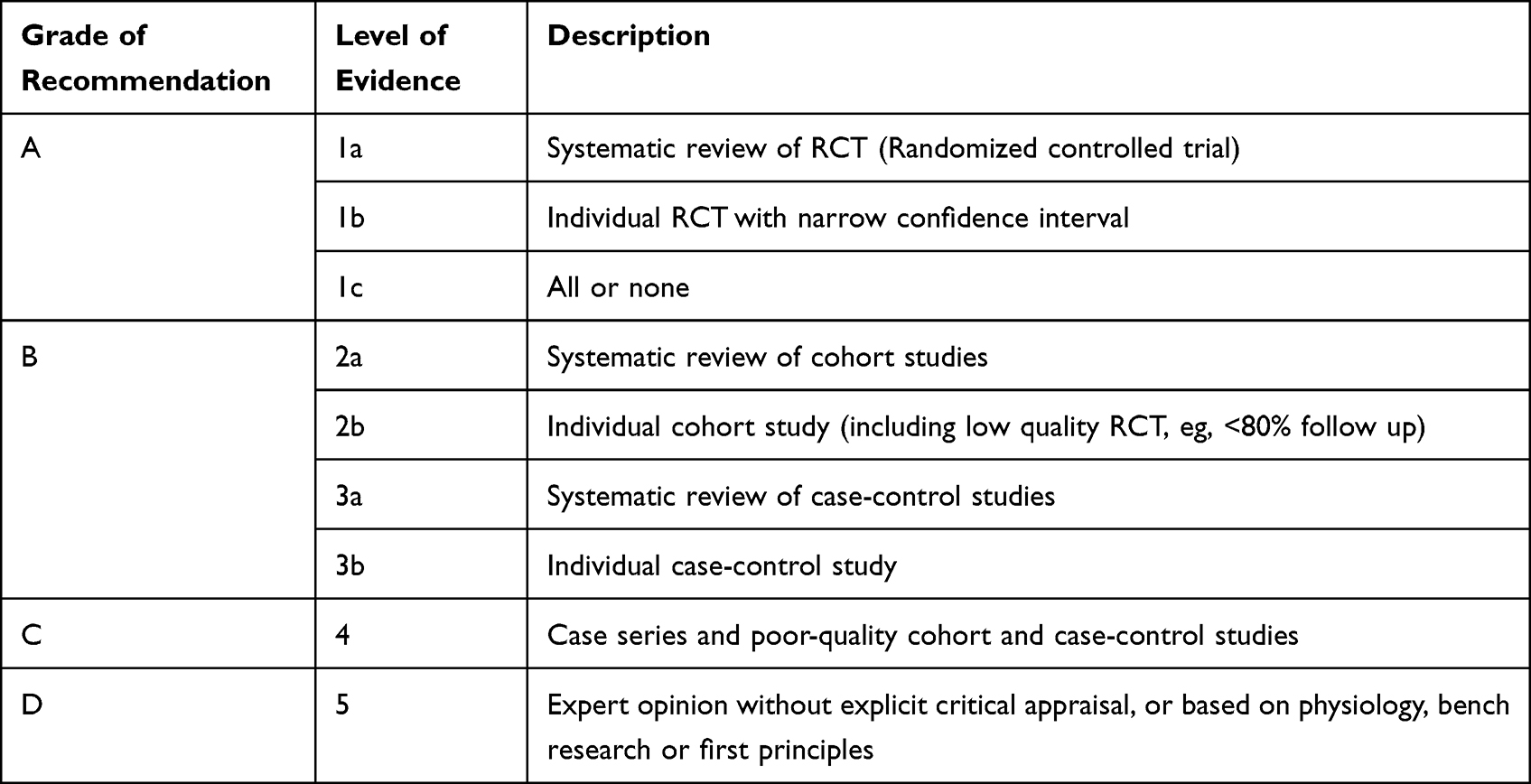 |
Table 1 Levels of Evidence and Associated Grade of Recommendation. Modified from the Oxford Centre for Evidence-Based Medicine Levels of Evidence |
Results
Pharmacological Interventions
The psychological health and HRQoL outcomes in children with AD are directly related to objective disease severity and improvements in disease severity correlate with improvements in psychological wellbeing.18 Medical management of AD is an effective method in improving disease severity. A number of evidence-based clinical guidelines recommend a stepwise approach to treating childhood AD based on the degree of eczema severity.19 Current recommended therapeutic options include emollients, topical treatments and systemic therapies.
Emollients
Emollients are routinely used in pediatric eczema and are effective in improving the skin barrier and reducing flares in AD by increasing skin hydration. Multiple national treatment guidelines recommend the use of regular emollients in the management of eczema for all severities of disease.20 Previous evidence has demonstrated improvements in both disease severity and quality of life through routine use of emollients.21 However, there is limited difference in effectiveness between the different major types of emollients including lotions, creams, gels and ointments. Instead, the type of emollient should be selected based on individual patient needs and the type that will be used most consistently.22 Prophylactic use of emollients may also reduce the risk of developing eczema in some infants by improving the skin barrier from birth.23
Grade of recommendation: A (Level 1a evidence)
Topical Therapy
In mild-to-moderate AD, topical therapeutic options such as topical corticosteroids and topical calcineurin inhibitors are the current gold standard as first-line treatment and recommended for use in most clinical guidelines.20 There is extensive documented evidence supporting the use of both of therapies in terms of safety, improving disease severity and patient quality of life.24 However, effective treatment use is marred by a number of barriers. Examples of treatment barriers include poor treatment adherence, user dependency and topical corticosteroid phobia.25 Overall, topical therapy remains an optimal treatment approach in the management of pediatric eczema and improving related psychological health outcomes.
Grade of recommendation: A (Level 1a evidence)
Systemic Treatment
In severe or treatment-resistant childhood AD, systemic treatment may be considered as a therapeutic option. Cyclosporine is the recommended first-line systemic treatment for short-term use due to its efficacy, safety and tolerability.26–28 Cyclosporine may also improve the HRQoL of mothers of children with paediatric eczema.29 However, there is a lack of consensus for long-term treatment options in pediatric AD.26 Methotrexate and mycophenolate mofetil are both possible treatment options that have demonstrated efficacy and improvements in HRQoL.30–32 Similarly, azathioprine is an effective alternative in pediatric eczema, however usage of these treatments is cautioned due to the risk of adverse events.33–35
In recent years, biological therapy has found increasing use in dermatology. Dupilumab is the only FDA approved treatment for children older than 6 months with demonstrated improvements in disease severity and HRQoL.36 Additional promising monoclonal agents including lebrikizumab, tralokinumab and nemolizumab which have demonstrated efficacy in adult populations are presently undergoing pediatric trials.37 Janus kinase inhibitors (JAK) are another new class of oral and topical medications that have emerged in the treatment of pediatric eczema. Topical ruxolitinib and oral upadacitinib are both medications that have been FDA approved for adolescent cohorts, with demonstrated improvements in disease severity and quality of life.38,39 While there are numerous systemic therapies available with demonstrated efficacy in pediatric, cohorts, their safety profile needs to be considered in conjunction to their indication for use.
Grade of recommendation: A (Level 1a evidence)
Non-Pharmacological Interventions
While medical interventions are the mainstay of treatment for childhood AD, given the chronic nature of the disease and lack of an established cure, there is a significant role in non-medical interventions as treatment adjuncts. These interventions can improve the use of medical interventions or address wellbeing related comorbidity and overall, help to improve disease severity, Qol and psychological outcomes.
Phototherapy
Phototherapy is a recommended treatment in both adult and pediatric AD as an alternative treatment in disease recalcitrant to topical therapies.40 While there is previously documented evidence favouring ultraviolet A and ultraviolet B phototherapy as both safe and effective in children, there is limited efficacy on psychological health and HRQoL.41–44 Further, there is also no long-term safety and efficacy data on phototherapy use in children.45 Phototherapy may improve psychological health outcomes, by improving disease severity, however further research in this domain is required to support continued use.
Grade of recommendation: B (Level 2b evidence)
Patient Education
Patient education is a useful therapeutic adjunct that can provide patients and caregivers with a better understanding of disease and related self-management strategies. A number of recent Eczema guidelines have recommended patient education as a key part of management approaches.26,40,46 Systematic reviews of educational interventions have demonstrated improvements in disease severity but did not appear to provide significant improvements in HRQoL.12,47,48 However, the results are difficult to interpret and generalise due to the variety of different educational approaches. Major differences include scope, frequency, and modality of education as well as study sample size and end points. Study quality is an important factor for consideration as factors such as longer education sessions, multidisciplinary approaches and nursing led session were effective as forms of education.12,49,50 Conventional education programs may be limited by lack of attendance, strengthening the role of newer modalities including online interventions, such as the “Eczema Care Online program” as a self-management strategy.51 Regardless, there is still a lack of consensus in treatment guidelines for optimal educational approaches. However, a structured interdisciplinary program suited to the patient’s educational and cultural needs is recommended in all severities of AD.
Grade of recommendation: A (level 1b evidence)
Eczema Action Plans
Eczema action plans are a potential treatment guideline that can be used alongside verbal instructions. Two previous studies including a randomised controlled trial and a quality improvement project have demonstrated improved outcomes of adding an eczema action plan to verbally instructed treatment regimens.52,53 Documented benefits include increased parental understanding surrounding eczema management, decreased disease severity and improved quality of life in parents and children with eczema.
Grade of recommendation: B (level 2b evidence)
Bleach Baths
Bathing in dilute bleach is a commonly used adjunctive treatment for AD. The antiseptic properties of bleach are believed to improve AD severity due to its antiseptic staphylococcal and anti-inflammatory effects. A recent systematic review of RCTs of mostly pediatric studies (9/10 of included RCTs) demonstrated that bleach baths provided some improvement in disease severity.54 However, CLDLQI scores were investigated by only one study and revealed no significant difference compared to usual water baths.55 Given the improvements in disease severity, the use of bleach baths may provide some indirect improvements in psychological health as a treatment adjunct.
Grade of recommendation: A (level 1a evidence)
Psychological Interventions
The adverse psychological effects of AD may be worsened by behaviours related to symptoms of disease including the itch-scratch cycle. Negative emotions such as anxiety and stress can also be a trigger for itch. Psychological interventions addressing these behaviours and associated mental health comorbidities may lead to improvements in these outcomes as well as disease severity. However, there is limited and heterogeneous evidence of effective psychological interventions in a paediatric population. An early study examining the effect of hypnotherapy and biofeedback strategies has demonstrated some improvements in disease severity.56 Anecdotal evidence may also support the implantation of psycho-dermatology clinics involving both dermatologists and clinical psychologists in the management of childhood eczema and improving HRQoL for families.57 In this style of clinic, patients and their caregivers can see both a consultant dermatologist, for medical treatment and a clinical psychologist who manages psychological concerns through strategies such as habit reversal for itch. Mindfulness therapy for parents has also been shown to improve both disease severity and QoL in a very small case series parameters in small case series.58 Psychological interventions may have an important role in the management of childhood AD, however further evidence is required to support their benefit.
Grade of recommendation: C (level 4 evidence)
Allergen Immunotherapy
Allergens may play a role in the pathogenesis of AD by driving innate and adaptive inflammatory responses.59 Allergen immunotherapy improves disease severity in other atopic diseases such as asthma and rhinitis. In adult populations, allergen immunotherapy for AD improves disease severity and QoL.60 The evidence in paediatric cohorts is less robust, however may support the use of sublingual allergen immunotherapy for AD.61,62
Grade of recommendation: A (level 1b evidence)
Infant Massage
Infant massage is a traditional practice used across the world, with demonstrated benefits in improving child sleep and increasing interaction with parents and caregivers.63 One randomized trial has investigated the effect of mother performed infant massage on infantile eczema and maternal state. Their study demonstrated significant improvement in eczema severity, infant quality of life as well as maternal anxiety and depression scores. Infantile massage performed in children with eczema may be mutually beneficial for the psyche of both child and caregiver.64
Grade of evidence: B (Level 2b evidence)
Conclusion
AD has a significant psychological burden on children and their families, due to the chronic nature of disease and its associated symptoms. Improving HRQoL and psychological outcomes is an important factor when considering management approaches. A range of pharmacological and non-pharmacological outcomes may provide benefit in this domain and should be utilised based on patient needs, in order to achieve optimal treatment outcomes. Emerging evidence will strengthen guidance and recommendations on addressing these psychological outcomes in the clinical setting, in order to improve disease outcomes and HRQoL of patients and caregivers.
Disclosure
Niyaz Mostafa reports no conflicts of interest in this work. Saxon Smith is a principal investigator for ABBVIE and Sanofi Genzyme; on the advisory board for ABBVIE, Sanofi Genzyme, Pfizer and Eli Lilly; received education speaker fees from ABBVIE; received consultancy and education speaker fees from Sanofi Genzyme, Pfizer and Eli Lilly; outside the submitted work.
References
1. Bieber T. Atopic dermatitis. N Engl J Med. 2008;358(14):1483–1494. doi:10.1056/NEJMra074081
2. Nutten S. Atopic dermatitis: global epidemiology and risk factors. Ann Nutr Metab. 2015;66(Suppl 1):8–16. doi:10.1159/000370220
3. Odhiambo JA, Williams HC, Clayton TO, Robertson CF, Asher MI; ISAAC Phase Three Study Group. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J Allergy Clin Immunol. 2009;124(6):1251–1258.e23. doi:10.1016/j.jaci.2009.10.009
4. Lifschitz C. The Impact of Atopic Dermatitis on Quality of Life. Ann Nutr Metab. 2015;66(Suppl. 1):34–40. doi:10.1159/000370226
5. Xie QW, Dai X, Tang X, Chan CHY, Chan CLW. Risk of mental disorders in children and adolescents with atopic dermatitis: a systematic review and meta-analysis. Front Psychol. 2019;10:1773. doi:10.3389/fpsyg.2019.01773
6. Loo EXL, Ooi DSQ, Ong M, et al. Associations between eczema and attention deficit hyperactivity disorder symptoms in children. Front Pediatr. 2022;10:837741. doi:10.3389/fped.2022.837741
7. Chow MYK, Morrow AM, Cooper Robbins SC, Leask J. Condition-specific quality of life questionnaires for caregivers of children with pediatric conditions: a systematic review. Qual Life Res. 2013;22(8):2183–2200. doi:10.1007/s11136-012-0343-z
8. Lee HJ, Lee GN, Lee JH, Han JH, Han K, Park YM. Psychological stress in parents of children with atopic dermatitis: a cross-sectional study from the Korea National Health and Nutrition Examination Survey. Acta Derm Venereol. 2023;103:2242. doi:10.2340/actadv.v103.2242
9. Moore K, David TJ, Murray CS, Child F, Arkwright PD. Effect of childhood eczema and asthma on parental sleep and well-being: a prospective comparative study. Br J Dermatol. 2006;154(3):514–518. doi:10.1111/j.1365-2133.2005.07082.x
10. Yang EJ, Beck KM, Sekhon S, Bhutani T, Koo J. The impact of pediatric atopic dermatitis on families: a review. Pediatr Dermatol. 2019;36(1):66–71. doi:10.1111/pde.13727
11. Davari DR, Nieman EL, McShane DB, Morrell DS. Current perspectives on the management of infantile atopic dermatitis. J Asthma Allergy. 2020;13:563–573. doi:10.2147/JAA.S246175
12. Ersser SJ, Cowdell F, Latter S, et al. Psychological and educational interventions for atopic eczema in children. Cochrane Database Syst Rev. 2014;2014(1):CD004054. doi:10.1002/14651858.CD004054.pub3
13. Kwan B, Rickwood DJ. A systematic review of mental health outcome measures for young people aged 12 to 25 years. BMC Psychiatry. 2015;15:279. doi:10.1186/s12888-015-0664-x
14. Lewis-Jones MS, Finlay AY. The Children’s Dermatology Life Quality Index (CDLQI): initial validation and practical use. Br J Dermatol. 1995;132(6):942–949. doi:10.1111/j.1365-2133.1995.tb16953.x
15. Lewis-Jones MS, Finlay AY, Dykes PJ. The Infants’ Dermatitis Quality of Life Index. Br J Dermatol. 2001;144(1):104–110. doi:10.1046/j.1365-2133.2001.03960.x
16. Ali FM, Johns N, Salek S, Finlay AY. Correlating the Dermatology Life Quality Index with psychiatric measures: a systematic review. Clin Dermatol. 2018;36(6):691–697. doi:10.1016/j.clindermatol.2018.08.014
17. Phillips B, Ball C, Sackett D. Oxford centre for evidence-based medicine: levels of evidence; 2009 [cited July 31, 2023]. Available from: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009.
18. Na CH, Chung J, Simpson EL. Quality of Life and Disease Impact of Atopic Dermatitis and Psoriasis on Children and Their Families. Children. 2019;6(12):133. doi:10.3390/children6120133
19. de Graaf M, Janmohamed SR, Schuttelaar MLA, et al. Systemic treatment of children and adolescents with atopic dermatitis aged ≥2 years: a Delphi consensus project mapping expert opinion in Northern Europe. J Eur Acad Dermatol Venereol. 2022;36(11):2153–2165. doi:10.1111/jdv.18410
20. van Halewijn KF, Lahnstein T, Bohnen AM, et al. Recommendations for emollients, bathing and topical corticosteroids for the treatment of atopic dermatitis: a systematic review of guidelines. Eur J Dermatol. 2022;32(1):113–123.
21. Kritsanaviparkporn C, Sangaphunchai P, Treesirichod A. Efficacy of moisturizers in paediatric atopic dermatitis: a systematic review and meta-analysis of randomised controlled trials. IJDVL. 2021;88(1):22–31. doi:10.25259/IJDVL_1384_20
22. Ridd MJ, Santer M, MacNeill SJ, et al. Effectiveness and safety of lotion, cream, gel, and ointment emollients for childhood eczema: a pragmatic, randomised, Phase 4, superiority trial. Lancet Child Adolescent Health. 2022;6(8):522–532. doi:10.1016/S2352-4642(22)00146-8
23. Liang J, Hu F, Tang H, et al. Systematic review and network meta-analysis of different types of emollient for the prevention of atopic dermatitis in infants. J Eur Acad Dermatol Venereol. 2023;37(3):501–510. doi:10.1111/jdv.18688
24. Siegfried EC, Jaworski JC, Kaiser JD, Hebert AA. Systematic review of published trials: long-term safety of topical corticosteroids and topical calcineurin inhibitors in pediatric patients with atopic dermatitis. BMC Pediatr. 2016;16(1):75. doi:10.1186/s12887-016-0607-9
25. Sokolova A, Smith SD. Factors contributing to poor treatment outcomes in childhood atopic dermatitis. Australas J Dermatol. 2015;56(4):252–257. doi:10.1111/ajd.12331
26. Wollenberg A, Barbarot S, Bieber T, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part II. J Eur Acad Dermatol Venereol. 2018;32(6):850–878. doi:10.1111/jdv.14888
27. Seger EW, Wechter T, Strowd L, Feldman SR. Relative efficacy of systemic treatments for atopic dermatitis. J Am Acad Dermatol. 2019;80(2):411–416.e4. doi:10.1016/j.jaad.2018.09.053
28. Schmitt J, Schmitt N, Meurer M. Cyclosporin in the treatment of patients with atopic eczema - a systematic review and meta-analysis. J Eur Acad Dermatol Venereol. 2007;21(5):606–619. doi:10.1111/j.1468-3083.2006.02023.x
29. von Rueden U, Bunikowski R, Braeutigam M, Staab D. Cyclosporin A treatment of children with severe atopic dermatitis improves quality of life of their mothers. Dermatol Psychosom. 2002;3(1):14–18. doi:10.1159/000051358
30. Downing HJ, Pirmohamed M, Beresford MW, Smyth RL. Paediatric use of mycophenolate mofetil. Br J Clin Pharmacol. 2013;75(1):45–59. doi:10.1111/j.1365-2125.2012.04305.x
31. Dvorakova V, O’Regan GM, Irvine AD. Methotrexate for severe childhood atopic dermatitis: clinical experience in a tertiary center. Pediatr Dermatol. 2017;34(5):528–534. doi:10.1111/pde.13209
32. Anderson K, Putterman E, Rogers RS, Patel D, Treat JR, Castelo-Soccio L. Treatment of severe pediatric atopic dermatitis with methotrexate: a retrospective review. Pediatr Dermatol. 2019;36(3):298–302. doi:10.1111/pde.13781
33. Fuggle NR, Bragoli W, Mahto A, Glover M, Martinez AE, Kinsler VA. The adverse effect profile of oral azathioprine in pediatric atopic dermatitis, and recommendations for monitoring. J Am Acad Dermatol. 2015;72(1):108–114. doi:10.1016/j.jaad.2014.08.048
34. Cusack C, Connolly C, Watson R, Irvine A. Experience with azathioprine in a childhood population with severe atopic eczema over an eight year period. Arch Dis Child. 2008;93(Suppl 2):174–ps174. doi:10.1136/adc.2007.127266
35. Caufield M, Tom WL. Oral azathioprine for recalcitrant pediatric atopic dermatitis: clinical response and thiopurine monitoring. J Am Acad Dermatol. 2013;68(1):29–35. doi:10.1016/j.jaad.2012.07.001
36. Paller AS, Siegfried EC, Thaçi D, et al. Efficacy and safety of dupilumab with concomitant topical corticosteroids in children 6 to 11 years old with severe atopic dermatitis: a randomized, double-blinded, placebo-controlled Phase 3 trial. J Am Acad Dermatol. 2020;83(5):1282–1293. doi:10.1016/j.jaad.2020.06.054
37. Johnson H, Yu J. Current and emerging therapies in pediatric atopic dermatitis. Dermatol Ther. 2022;12(12):2691–2703. doi:10.1007/s13555-022-00829-4
38. Guttman-Yassky E, Teixeira HD, Simpson EL, et al. Once-daily upadacitinib versus placebo in adolescents and adults with moderate-to-severe atopic dermatitis (Measure Up 1 and Measure Up 2): results from two replicate double-blind, randomised controlled phase 3 trials. Lancet. 2021;397(10290):2151–2168. doi:10.1016/S0140-6736(21)00588-2
39. Papp K, Szepietowski JC, Kircik L, et al. Efficacy and safety of ruxolitinib cream for the treatment of atopic dermatitis: results from 2 phase 3, randomized, double-blind studies. J Am Acad Dermatol. 2021;85(4):863–872. doi:10.1016/j.jaad.2021.04.085
40. Sidbury R, Davis DM, Cohen DE, et al. GUIDELINES OF CARE FOR THE MANAGEMENT OF ATOPIC DERMATITIS. J Am Acad Dermatol. 2014;71(2):327–349. doi:10.1016/j.jaad.2014.03.030
41. Clayton TH, Clark SM, Turner D, Goulden V. The treatment of severe atopic dermatitis in childhood with narrowband ultraviolet B phototherapy. Clin Exp Dermatol. 2007;32(1):28–33. doi:10.1111/j.1365-2230.2006.02292.x
42. Jekler J, Larkö O. UVB phototherapy of atopic dermatitis. Br J Dermatol. 1988;119(6):697–705. doi:10.1111/j.1365-2133.1988.tb03490.x
43. Tay YK, Morelli JG, Weston WL. Experience with UVB phototherapy in children. Pediatr Dermatol. 1996;13(5):406–409. doi:10.1111/j.1525-1470.1996.tb00711.x
44. Uetsu N, Horio T. Treatment of persistent severe atopic dermatitis in 113 Japanese patients with oral psoralen photo-chemotherapy. J Dermatol. 2003;30(6):450–457. doi:10.1111/j.1346-8138.2003.tb00415.x
45. Musters AH, Mashayekhi S, Harvey J, et al. Phototherapy for atopic eczema. Cochrane Database Syst Rev. 2021;10(10). doi:10.1002/14651858.CD013870.pub2
46. Katayama I, Aihara M, Ohya Y, et al. Japanese guidelines for atopic dermatitis 2017. Allergol Int. 2017;66(2):230–247. doi:10.1016/j.alit.2016.12.003
47. Zhao M, Liang Y, Shen C, Wang Y, Ma L, Ma X. Patient education programs in pediatric atopic dermatitis: a systematic review of randomized controlled trials and meta-analysis. Dermatol Ther. 2020;10(3):449–464. doi:10.1007/s13555-020-00365-z
48. de Bes J, Legierse CM, Prinsen CAC, de Korte J. Patient education in chronic skin diseases: a systematic review. Acta Derm Venereol. 2011;91(1):12–17. doi:10.2340/00015555-1022
49. Schuttelaar MLA, Vermeulen KM, Drukker N, Coenraads PJ. A randomized controlled trial in children with eczema: nurse practitioner vs. dermatologist. Br J Dermatol. 2010;162(1):162–170. doi:10.1111/j.1365-2133.2009.09502.x
50. Moore E, Williams A, Manias E, Varigos G. Nurse-led clinics reduce severity of childhood atopic eczema: a review of the literature. Br J Dermatol. 2006;155(6):1242–1248. doi:10.1111/j.1365-2133.2006.07534.x
51. Santer M, Muller I, Becque T, et al. Eczema Care Online behavioural interventions to support self-care for children and young people: two independent, pragmatic, randomised controlled trials. BMJ. 2022;379:e072007. doi:10.1136/bmj-2022-072007
52. Rork JF, Sheehan WJ, Gaffin JM, et al. Parental response to written eczema action plans in children with eczema. Arch Dermatol. 2012;148(3):391–392. doi:10.1001/archdermatol.2011.2267
53. Gilliam AE, Madden N, Sendowski M, Mioduszewski M, Duderstadt KG. Use of Eczema Action Plans (EAPs) to improve parental understanding of treatment regimens in pediatric atopic dermatitis (AD): a randomized controlled trial. J Am Acad Dermatol. 2016;74(2):375–377.e1–e3. doi:10.1016/j.jaad.2015.08.067
54. Bakaa L, Pernica JM, Couban RJ, et al. Bleach baths for atopic dermatitis: a systematic review and meta-analysis including unpublished data, Bayesian interpretation, and GRADE. Ann Allergy Asthma Immunol. 2022;128(6):660–668.e9. doi:10.1016/j.anai.2022.03.024
55. Hon KL, Tsang YCK, Lee VWY, et al. Efficacy of sodium hypochlorite (bleach) baths to reduce Staphylococcus aureus colonization in childhood onset moderate-to-severe eczema: a randomized, placebo-controlled cross-over trial. J Dermatolog Treat. 2016;27(2):156–162. doi:10.3109/09546634.2015.1067669
56. Sokel B, Christie D, Kent A, et al. A comparison of hypnotherapy and biofeedback in the treatment of childhood atopic eczema. Contemp Hypnos. 1993. Available from: https://www.semanticscholar.org/paper/A-comparison-of-hypnotherapy-and-biofeedback-in-The-Sokel-Christie/ec29e10b32a7f5eb252fc0e6160f43687f04c67a.
57. Sears AV, Ali R, O’Connor J, Baron S. Establishing and developing a paediatric psychodermatology service and our experience of a new paediatric psychodermatology clinic during the Covid 19 pandemic. Skin Health Dis. 2022;2(4):e151. doi:10.1002/ski2.151
58. Heapy C, Norman P, Emerson LM, Murphy R, Bögels S, Thompson AR. Mindful parenting intervention for parents of children with skin conditions: a single group experimental cases series. Behav Cogn Psychother. 2022;50(5):462–480. doi:10.1017/S1352465822000170
59. Kita H. How are airborne allergens remembered by the immune system? J Allergy Clin Immunol. 2022;149(6):1940–1942. doi:10.1016/j.jaci.2022.02.014
60. Yepes-Nuñez JJ, Guyatt GH, Gómez-Escobar LG, et al. Allergen immunotherapy for atopic dermatitis: systematic review and meta-analysis of benefits and harms. J Allergy Clin Immunol. 2023;151(1):147–158. doi:10.1016/j.jaci.2022.09.020
61. Song K, Kim M, Park M, Rhee E, Yu J. The Therapeutic and Preventive Effect of Sublingual Immunotherapy in Mite-Sensitized Children with Atopic Dermatitis: A Randomized, Open, Parallel-Group Study. 111 River St, Hoboken 07030-5774, NJ USA: Wiley; 2020:47–48.
62. Pajno GB, Caminiti L, Vita D, et al. Sublingual immunotherapy in mite-sensitized children with atopic dermatitis: a randomized, double-blind, placebo-controlled study. J Allergy Clin Immunol. 2007;120(1):164–170. doi:10.1016/j.jaci.2007.04.008
63. Abdallah B, Badr LK, Hawwari M. The efficacy of massage on short and long term outcomes in preterm infants. Infant Behav Dev. 2013;36(4):662–669. doi:10.1016/j.infbeh.2013.06.009
64. Lin L, Yu L, Zhang S, Liu J, Xiong Y. The positive effect of mother-performed infant massage on infantile eczema and maternal mental state: a randomized controlled trial. Front Public Health. 2022;10:1068043. doi:10.3389/fpubh.2022.1068043
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Managing Atopic Dermatitis with Lebrikizumab – The Evidence to Date
Labib A, Ju T, Yosipovitch G
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1065-1072
Published Date: 8 June 2022
Sleep Disturbances in Chinese Children with Epilepsy: Associations with Behavioral Problems and Quality of Life
Zhao F, Sun X, Wang Y, Zhou Y, He Y, Wang C, Han F, Liu J, Tsai SY, Wang G, Wang J
Nature and Science of Sleep 2022, 14:1225-1236
Published Date: 2 July 2022
Practical Guidance for the Use of Voxelotor in the Management of Sickle Cell Disease
Barriteau CM, Badawy SM
Journal of Blood Medicine 2022, 13:739-745
Published Date: 29 November 2022
Young XLH Patients-Reported Experience with a Supportive Care Program
Rothenbuhler A, Gueorguieva I, Lichtenberger-Geslin L, Audrain C, Soskin S, Bensignor C, Rossignol S, Bertholet-Thomas A, Naudeau L, Bacchetta J, Linglart A
Patient Preference and Adherence 2023, 17:1393-1405
Published Date: 9 June 2023
The Prevalence, Knowledge, and Awareness Level of Atopic Dermatitis Among a Sample of Adult Jordanian Population
Saleh MM, Al-Qerem W, Karaki LA, Al-Zayadneh A, Al-Awawdeh A
Clinical, Cosmetic and Investigational Dermatology 2026, 19:624003
Published Date: 10 July 2026