")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Prevalence of Skin Disease and Its Associated Factors Among Primary Schoolchildren: A Cross-Sectional Study from a Northern Ethiopian Town
Authors Mengist Dessie A , Fenta Feleke S , Getaye Workie S, Getinet Abebe T , Mossu Chanie Y, Kassa Yalew A
Received 3 February 2022
Accepted for publication 20 April 2022
Published 29 April 2022 Volume 2022:15 Pages 791—801
DOI https://doi.org/10.2147/CCID.S361051
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Anteneh Mengist Dessie,1 Sefineh Fenta Feleke,2 Sewnet Getaye Workie,3 Tiruayehu Getinet Abebe,1 Yonas Mossu Chanie,4 Anteneh Kassa Yalew5
1Department of Public Health, College of Health Science, Debre Tabor University, Debre Tabor, Ethiopia; 2Department of Public Health, College of Health Science, Woldia University, Woldia, Ethiopia; 3Department of Public Health, College of Medicine and Health Science, Debre Berhan University, Debre Berhan, Ethiopia; 4Yigem Health Center, Menz Mama Worda, North Shoa, Ethiopia; 5Department of Public Health, College of Medicine and Health Science, Wolkite University, Wolkite, Ethiopia
Correspondence: Anteneh Mengist Dessie, Email [email protected]
Background: Skin disease affects people of all ages, yet children are one of the most common victims of it. Although some data indicate a high prevalence of skin disorders among Ethiopian primary schoolchildren, little is known regarding it, particularly in the study area. Hence, the study aimed to investigate the prevalence of skin disease and its associated factors among primary schoolchildren in Debre Berhan town, North Shoa, Ethiopia.
Methods: Institutional-based cross-sectional study was conducted. The samples were chosen using a multistage stratified random sampling technique. Data were collected using both a self-administered and an interviewer-administered questionnaire. Children were clinically examined to detect and record the dermatological findings. A potassium hydroxide test was used to confirm some doubtful cases. The data were entered in Epi Info version 3.5.1 and analyzed using SPSS version 20.0. Variables with a p-value < 0.05 were designated as having statistical significance.
Results: The overall point prevalence of any skin disease was 61.2% (95% CI: 56.4– 66.1). In a multivariable logistic regression model, a significant association between skin diseases and the occupation of the father being a farmer (AOR: 4.21, 95% CI: 1.06– 16.63), bad personal hygiene (AOR: 1.78, 95% CI: 1.03– 4.38), previous history of skin disease (AOR: 2.74, 95% CI: 1.41– 5.30), exchange of clothes and towels with other family members (AOR: 1.50, 95% CI: 1.09– 2.85), presence of trauma in the last one month (AOR: 2.09, 95% CI: 1.18– 3.72) and not being a member of health insurance (AOR: 1.95, 95% CI: 1.16– 3.28) has been found.
Conclusion: The point prevalence of any skin disorder is alarmingly high. The commonest disorders found in this study were simple and could usually be cured easily. Hence, preventive and curative health services should be provided for these schoolchildren to achieve a considerable reduction in the prevalence of skin disorders.
Keywords: Debre Berhan town, Ethiopia, prevalence, primary schoolchildren, skin disease
Introduction
Skin disorders occur all over the world at a significant level and pose a significant public health burden both in developing and developed countries.1 It affects people of all ages, yet children are one of the most common victims of skin diseases since their skin is thin and more delicate.2 The clinical evaluations indicated a general decrease in softness, smoothness, and overall skin condition with increased child age.3 Because of these developmental differences, the skin in children may be more sensitive to irritation and inflammation.4 Minor skin injuries and exposure to germs and physical agents such as excessive temperature (hot/cold) are also common in children, making them more susceptible to skin disease. A study from northern India showed that over a third of schoolchildren are affected by skin disease at any given time.5 The school environment makes schoolchildren vulnerable to cross-transmission of communicable skin diseases because they engage in activities that involve interpersonal contact, especially at games or play.6
Skin and subcutaneous diseases were responsible for 41.6 million Disability Adjusted Life Years (DALYs) and 39.0 million Year Lost due to Disability (YLDs) in 2013 which makes them the 18th leading cause of global DALYs. Excluding mortality, skin diseases were the fourth leading cause of disability worldwide. Skin and subcutaneous disease grew 46.8% between 1990 and 2017.1 In a review of 18 prevalence studies (13 provided data specific to children), 21 to 87% of skin diseases were reported.7 However, research efforts and funding do not match the relative disability of skin diseases.
Although most dermatological conditions do not result in death, they lead to misery and incapacitations. It has an impact on patients’ social, physical, and emotional well-being, as well as their friends, partners, and families.8,9 Children, in particular, experience significant discomfort and embarrassment, which leads to unnecessary absences from school.7 The impact of skin disease on patients’ lives is often overlooked by not only health policymakers but also physicians. They were diverted to diseases that are perceived as more serious.
Factors like the Human Immunodeficiency Virus (HIV) pandemic, changing lifestyles of the societies, dislocation from home, increasing use of industrial chemicals, global warming, and more have a role in the rise of the prevalence of skin diseases.10 There is also a variation in disease burden when stratified by age and geographic regions. For instance, eczema is common in developed countries while infections and infestations in developing countries.11 Pyoderma, tinea capitis, and to a lesser extent, scabies is common in children than in adults.12 Most dermatological cases can be managed at peripheral health units cost-effectively and sustainably, leading to significant health gains for both individual patients and public health. Despite this, few systematic attempts have been made to develop such public-health interventions.13
In Ethiopia, a piece of studies reported a high prevalence of skin disorders among primary school children. There is also an outbreak of skin disease scabies in different parts of North Shoa zone14 and cold extreme weather condition in Debre Berhan town which makes children more likely to develop skin diseases.15 Despite this, no study regarding the pattern of skin diseases among children in Debre Berhan town, Ethiopia has been carried out. Hence, this study was designed to determine the prevalence of skin diseases among primary-school children in Debre Berhan town and to describe their association with various factors.
Methods
Study Design, Area and Period
An institutional-based cross-sectional study was conducted among primary school children in Debre Berhan town, North Shoa zone, Amhara National Regional State from May 1 to 30, 2018. Debre Berhan town is located 130km from Addis Ababa, the capital city of Ethiopia. The town has an elevation of 2840 meters, which makes it the highest town of this size in Africa. It is one of the coolest cities found in the subtropical zone of Ethiopia. The town has a typical subtropical highland climate. The average annual temperature of the town during the day and night hours is 20.7 °C and 8.2 °C respectively with precipitation of 964mm. In this town, the total estimated number of children who are joined from grade 4 to grade 8 is 8429, and there are 9 governmental and 7 private primary schools that provide service up to grade 8 at that time.
Study Participants
Children from grade 4–8 both in governmental and private primary schools, present in school during the data collection period, and those long term residents of the study area (at least six months) were included in the study. Children aged greater than or equal to 18 years, those who were mentally ill and unable to hear were excluded from the study.
Sample Size Determination and Sampling Technique
The sample size was determined based on the single population proportion formula using a 95% CI, 5% margin of error, and an assumption that 80.4% of schoolchildren in Debre Berhan town will have one or more skin diseases,16 a 10% non-response rate and 1.5 design effects. A total sample size of 402 children was required.
A Multistage stratified random sampling technique was applied to select the study participants. First, we obtained a list of all Primary Schools which provide service up to grade 8 in Debre Berhan town. Then, using simple random sampling two governmental and one private school were selected. Stratification was done by their grade level (Grade 4, 5, 6, 7, and 8) via considering all these three selected schools as one and allocate the sample size proportionally to each stratum. Finally, students (study subjects) were selected by simple random sampling from each stratum.
Study Variables
The dependent variable was skin disease and independent variables were socio-demographic characteristics (gender, area of residence, father’s educational status, mother’s educational status, child’s grade, age of the child, parent’s occupation, parent’s marital status, a child live with), medical history, and hygiene and sanitary conditions.
Operational/Term Definitions
Skin disease: A condition or disorder of the skin having sign and symptoms which is clinically recognized by the physician or confirmed by laboratory examination.
Personal hygiene: Considered as good if a child wash hair at least once per week for female and two times a week for male, take a shower at least four times per month by using soap, wash their hand and face at least one times per day by soap and wear one cloth without washing at most one week.
Body Mass Index (BMI): Categorized as underweight (<18.5kg/m2), healthy weight (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2) and obese (30.0 kg/m2 and above).
Trauma: Injuries/accidents to the skin anywhere on the body surface that result in bruising, puncture wounds, laceration, abrasion, avulsion, or burn wounds.
Data Collection Procedure
A self-administered, semi-structured questionnaire was designed by the researchers after a thorough review of several pieces of literature. The questionnaire was distributed to each selected student to be answered by their parents. Verbal assent was obtained from the children, who were asked to bring written informed consent from their parents for participation in the study. Then for the students who returned with written informed consent and completed responses, an interviewer-administered questionnaire was administered by graduate public health officers and the consultant dermatologist clinically examines the exposed parts of the body in a well-illuminated private class to document the findings. Laboratory confirmation was used only if the diagnosis was doubtful. Only ten samples by skin rubbing and four samples by hair plucking were obtained to be placed in a potassium hydroxide (KOH) solution and analyzed under a microscope.
Data Analysis and Presentation
Data were entered in Epi Info version 3.5.1 and analyzed using SPSS software, version 20.0. Descriptive statistics were used to determine the magnitudes of events in the study. Categorical variables were summarized as numbers and percentages to be displayed by using frequency tables and graphs, whereas continuous variables were presented as mean/median and standard deviations/ inter quartile range based on the distribution of the data. Logistic regression was employed; crude and adjusted odds ratios were computed to identify determinants of skin disease. A p-value of ≤0.2 was used to select variables for multi-variable regression and on multi-variable regression p-value <0.05 with 95% Confidence Interval (CI) was set as statistical significant.
Result
Socio-Demographic Status
A total of 402 students spread across the three selected schools were recruited for the survey, of which 387 students eventually participated, giving a response rate of 96.3%. The number of students from governmental and private schools was 306 (79.1%) and 81 (20.9%) respectively. The mean age (± SD) of the children was 13.37 (±1.83) years. The mean family size was 4.8 ± 1.49 with 71.3% of them having a family size of less than or equal to five. Table 1 shows all of the socio-demographic characteristics (Table 1).
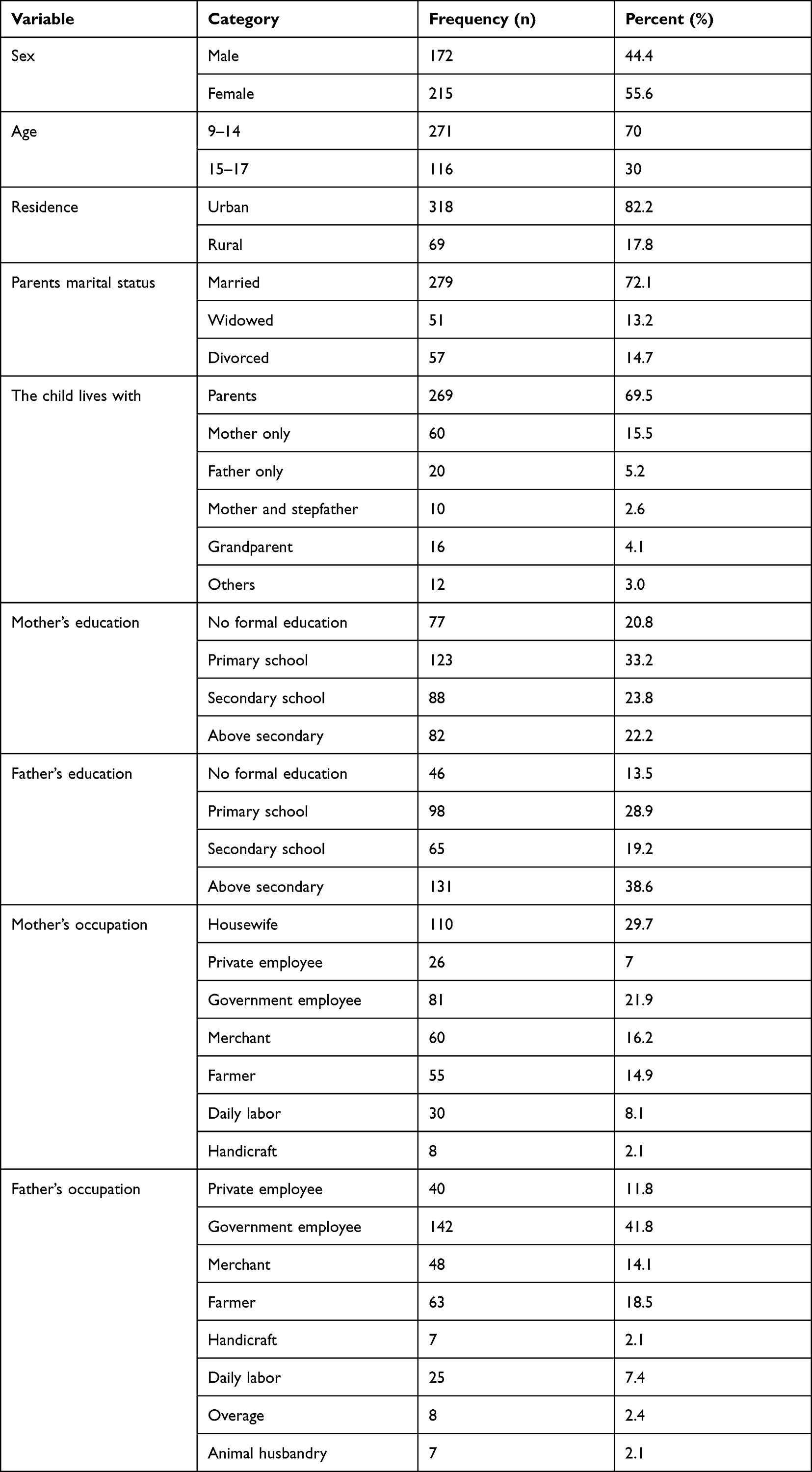 |
Table 1 Socio-Demographic Characteristics of the Primary Schoolchildren in Debre Berhan Town, North Shoa, 2018 |
Hygiene and Sanitary Condition
One hundred four (27%) children share clothes and towels with their families. Of 387 children, 214 (55.3%) wore closed shoes and 28 (7.2%) were barefoot. The majority, 244 (63%) and 214 (52.2%) of children take a shower four times per month and wash their hair once per week respectively. A total of 317 children (82%) use soap while washing their hands and face. Domestic animals were found in 251 (64.9%) of children’s houses, with 140 (55.7%) of children having close contact with them. Domestic animal waste was dumped on an open field in 54 (21.4%) of the children’s houses.
Medical History
Ninety-one children (23.5%) have a family member who suffered from skin disease currently and in the past 1 year and 109 (28.2%) of children were suffered from skin disease before. A total of 138 children (35.7%) got trauma in the last month; of these 58 (42%) were lacerations. Of 387 children, 285 (73.6%) uses any cosmetics among them 181 (63.7%) were females. Regarding their BMI status, 71 (18.3%), 299 (77.3%), and 17 (4.4%) children were categorized as underweight, healthy weight, and overweight. A family of 189 children has health insurance.
Prevalence of Skin Disease
The prevalence of skin disease was 61.2% (95% CI: 56.4–66.1). The most common skin disease categories were dandruff 91 (38.4%), followed by pityriasis Alba 82 (34.6%), and any type of dermatitis 39 (16.5%) (Table 2).
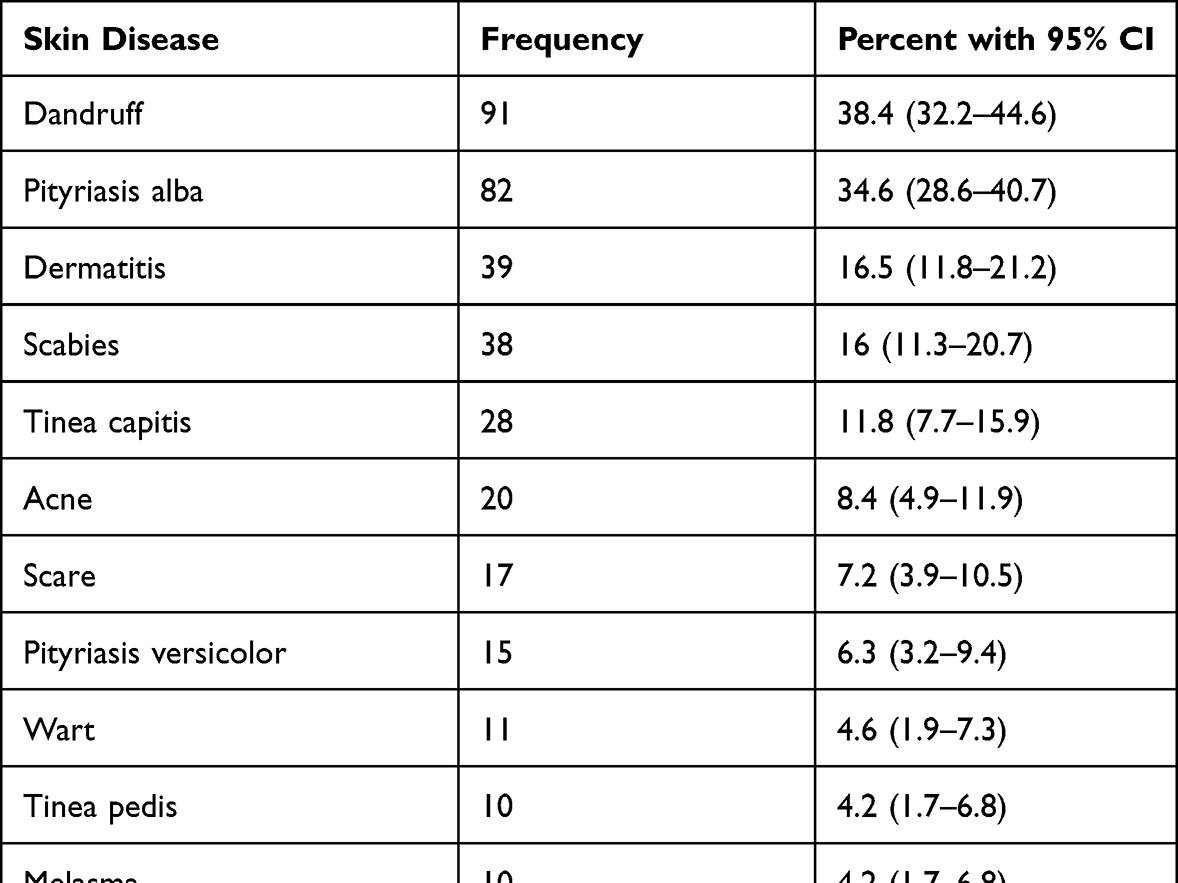 |
Table 2 Distribution of Skin Disease Among These Primary Schoolchildren Who Suffered from Skin Disease in Debre Berhan Town, North Shoa, 2018 |
Associated Factors of Skin Disease
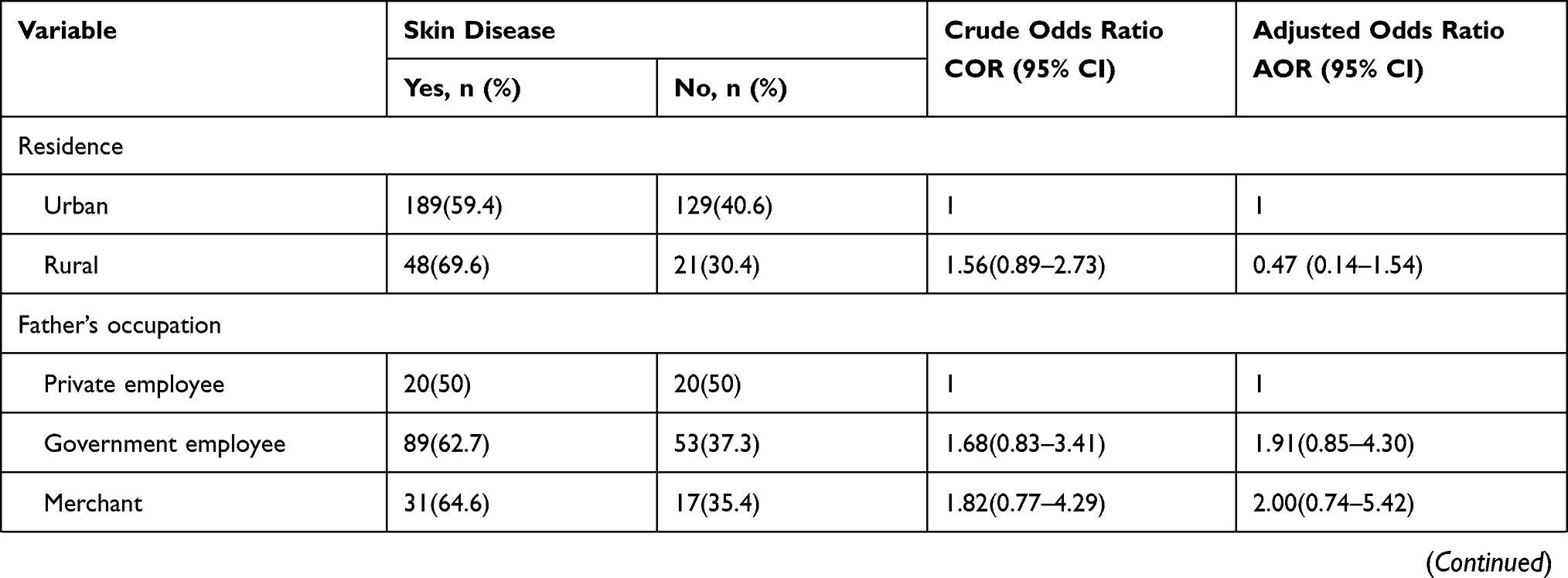
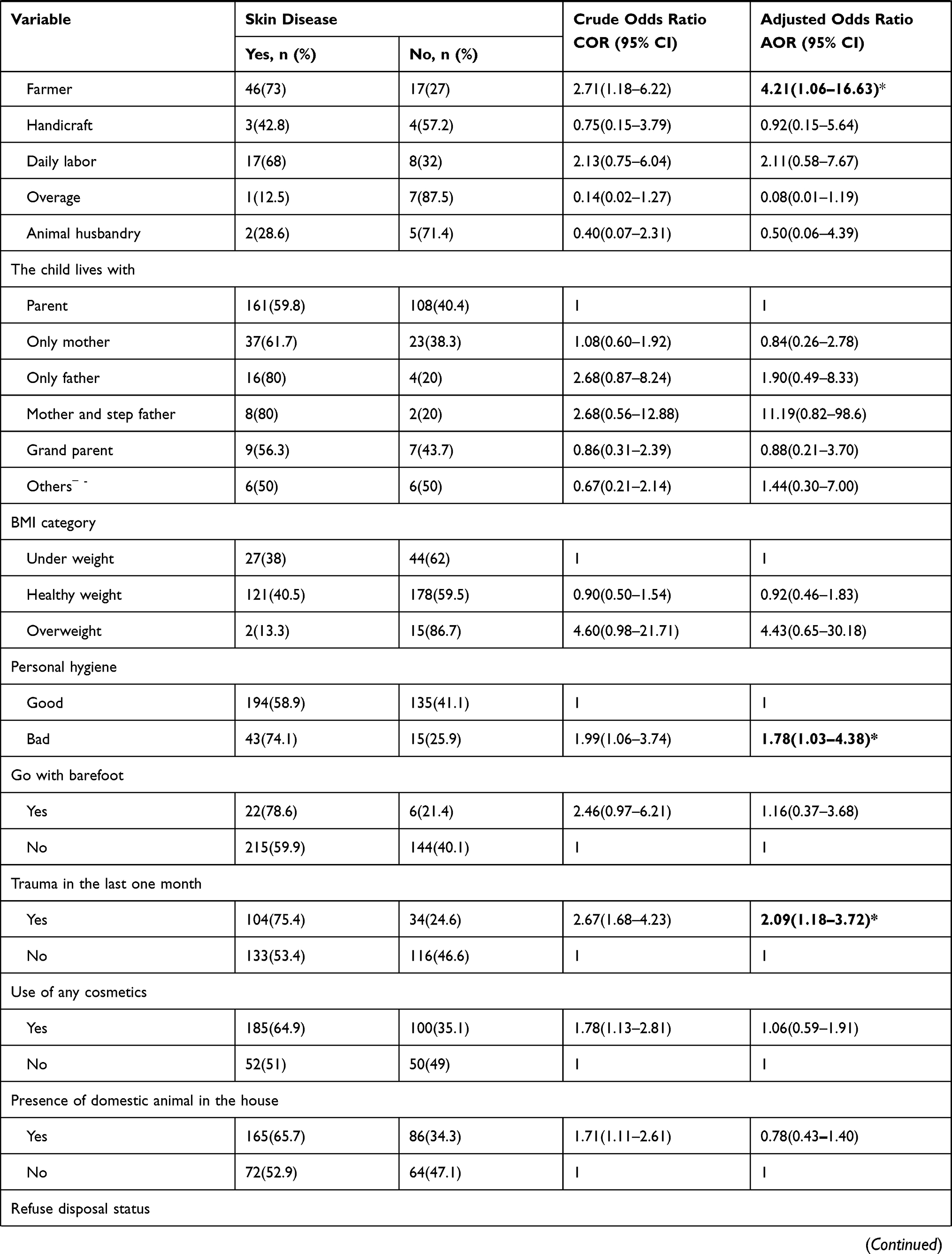
In the bivariable logistic regression residence, father’s occupation, the child lives with, BMI, personal hygiene, go with barefoot, trauma in the last one month, use of any cosmetics, presence of domestic animal in the house, refuse disposal status, family member suffered by skin disease currently or in the last one year, exchange of clothes and towels to the other family member, previous history of skin disease and presence of health insurance for the family was statistically associated with skin disease at a p-value of≤0.2. However, in multivariable logistic regression; the occupation of the father being a farmer (AOR: 4.21, 95% CI: 1.06–16.63), the bad personal hygiene (AOR: 1.78, 95% CI: 1.03–4.38), previous history of skin disease (AOR: 2.74, 95% CI: 1.41–5.30), exchange of clothes and towels to other family members (AOR: 1.50, 95% CI: 1.09–2.85), presence trauma in the last one month (AOR: 2.09, 95% CI: 1.18–3.72) and not the presence of health insurance for the family (AOR: 1.95, 95% CI: 1.16–3.28) were the variables significantly associated with skin disease among the primary schoolchildren in Debre Berhan town. Table 3 shows the variables that have a significant relationship with the occurrence of skin disease in both bivariable and multivariable logistic regression (Table 3).
 |
 |
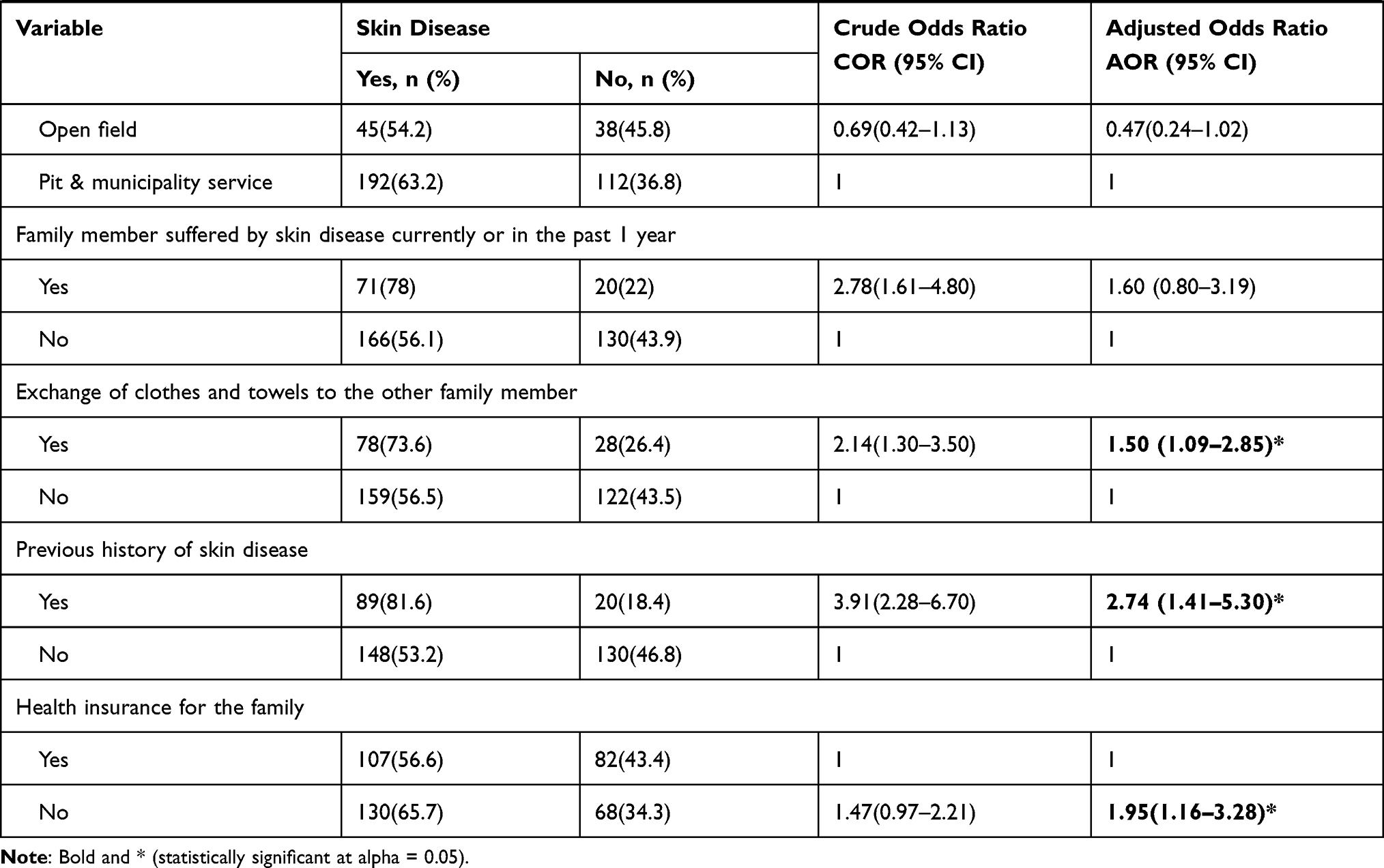 |
Table 3 Factors Associated with Skin Disease Among Primary Schoolchildren in Debre Berhan Town, North Shoa, 2018 |
Discussion
The overall aim of this study was to investigate the prevalence of skin disease and its associated factors among primary schoolchildren in Debre Berhan town, North Shoa, Ethiopia. Accordingly, the prevalence of any skin disorder was 61.2% (95% CI: 56.4–66.1). Dandruff, pityriasis alba, dermatitis, and scabies were the first four prevalent skin disorders discovered. The following factors: occupation of the father being a farmer, bad personal hygiene, previous history of skin disease, exchange of clothes and towels with other family members, presence of trauma in the last one month, and not the presence of health insurance for the family were identified as significant predictors of skin diseases.
The point prevalence of any skin disorder in this study is comparable to that of a previous study conducted among primary schoolchildren in the Illubabor zone (58.3%) and India (59.3%),17,18 but less than that of a study among schoolchildren in rural Ethiopia (80.4%).16 It might be due to the previous study being done totally among rural students who will have a high risk of developing skin disease.
The overall prevalence of skin disease in comparable studies done elsewhere in the Anand district of India (15.41%), Upper Egypt (86.93%), Nigeria (39.6%), Iraq (40.9%), and North India in Lucknow (42.3%) has shown a different finding from this study.2,19–22 Different reasons may justify this considerable variation in the prevalence of skin disease. The possible justification will be the difference in the socio-economic status of the population and the place where information was gathered. Unlike the current study, some previous studies were conducted in countries with high and middle-income economy in which there are somewhat better health care system and service utilization than low-income countries like Ethiopia.23,24 Other important reasons might include the non-uniformity in sample size, study design, diagnostic criteria, and disease definition. For instance, in a study from Upper Egypt, data were collected for two years, from December 1994 to December 1996, resulting in a high prevalence of the illness because skin disease usually does not result in death and has no a short recovery time.
Many studies have found that infectious skin diseases are the most common findings among schoolchildren,16,17,19,20,22 which is consistent with our findings. In contrast to our study findings, some research indicates that noninfectious and non-transmissible skin diseases are common.2,21,25 Possibly, it will be justified as this study was conducted on the area which has low social class, low treatment-seeking behavior, and bad hygienic habit which results in a high prevalence of infectious skin diseases than that of the noninfectious one. It will have an implication those health extension workers who are the main health personnel visiting these children within the community should get training about the diagnosis and management of these skin disorders. It will also use as a gate to incorporate problems relating to skin diseases in Integrated Management of Newborn and Childhood Illness (IMNCI) and other programs.
Similar to that of the study in Nigeria,20 in our study, previous history of skin disease and personal hygiene were significantly associated; and BMI, age, parental education, and occupation of the mother were not significantly associated with the presence of skin disorders. In contrast, parental education showed a statistically significant association in a study from north India, Iraq, Chennai India, and Nigeria.17,21,22,26 This might be because schoolchildren above nine years of age perform most of their daily self-care and hygienic activities independently, while those below nine years of age depends on their parents for most of their hygiene and grooming activities, and the participants in this study were children above nine years of age.
The odd of skin disorder was higher in children whose father is farmer when compared to those whose father is private employee. The prevalence of skin disease was also higher in children who share towels/cloth with other family members and have poor personal hygiene. In line with our study finding, another study also found a significant association of skin disease with parents’ occupation, poor personal hygiene, and sharing of cloth/bed.18 This could be partly explained by children from farmer family will have long-term exposure to outdoor environmental conditions, repeated contact with chemicals from plants, pesticides, and herbicides, and no better opportunity for personal and environmental sanitation.
Community-based health insurance (CBHI) membership is found to be one of the significant factors that affect the development of skin disease in this study. Accordingly, those schoolchildren from a family who are not members of CBHI have a higher odd of developing skin disease. It might be due to the fact that CBHI improves access to healthcare in turn it results in the improvement of health-seeking behavior. For instance, a study conducted in North-West Ethiopia reveals that health services utilization among insured households with CBHI was higher.27 Since it has an effect on health-seeking behavior and members undergo prevention practice and early treatment, being a member of CBHI may also decrease the prevalence of skin disease among schoolchildren.
Limitations of the Study
The following limitations should be considered while interpreting the result of this study. First, the cross-sectional nature of the study will underestimate the burden of the disease since point prevalence studies often miss diseases of short duration. Second, social desirability bias will be there with potential over-reporting of favorable behaviors regarding hygienic practice, for which controlling was difficult. The wealth index, which will be the main factor in developing skin disorders,28 was not also assessed in this study.
Conclusion and Recommendation
The study concludes that the point prevalence of skin disorder is alarmingly high and the most common type of skin disorder found in this study was dandruff followed by pityriasis alba and dermatitis. Occupation of the father being a farmer, bad personal hygiene, previous history of skin disease, exchange of clothes and towels with other family members, presence of trauma in the last one month, and not the presence of health insurance for the family were the significantly associated with skin disease among the primary children in Debre Berhan town. So, preventive and curative health services should be provided for these schoolchildren in Debre Berhan town by improving school health programs to achieve a considerable reduction in the prevalence of skin disorders. With regard to students’ personal hygiene, teachers should fulfill their responsibility of monitoring students’ hygiene daily in the classroom or in the queue. It is also better to strengthen the national capacity to scale up health insurance coverage in the community. Further large scale studies with a strong design and large sample size should be done on both pre-schoolchildren and schoolchildren to assess the overall prevalence of skin disease and its associated factors.
Abbreviations
AOR, adjusted odds ratio; BMI, body mass index; CBHI, community-based health insurance; CI, confidence interval; COR, crude odds ratio; DALYs, disability-adjusted life year; HIV, human immunodeficiency virus; IMNCI, Integrated Management of Newborn and Childhood Illness; KOH, potassium hydroxide; YLD, years lost due to disability.
Data Sharing Statement
The data is available from the corresponding author upon reasonable request.
Ethical Approval
The study was approved by the institutional Ethics committee of Debre Berhan University. Written informed consent from the school and parents, and verbal assent from each participant in the study were obtained. The study is in compliance with the principle of the declaration of Helsinki. The confidentiality of information was maintained by excluding personal identifiers. Children with a skin disease who did not visit health centers during the study period were brought to health facilities to be treated.
Acknowledgment
First, we would like to express our appreciation and respect to the study participants for their sincere interest and consent to participate in this study; besides, we like to acknowledge Debre Berhan University, from which ethical clearance was obtained. We would like to take also this opportunity to express our profound gratitude and deep regard to our friends for their unreserved support throughout the development of this paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We have no specific grant for this research from any funding agency.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Karimkhani C, Dellavalle RP, Coffeng LE, et al. Global skin disease morbidity and mortality: an update from the global burden of disease study 2013. JAMA Dermatol. 2017;153(5):406–412.
2. Vora R, Bodiwala N, Patel S, Krishna S. Prevalence of various dermatoses in school children of Anand district. National J Commun Med. 2012;3(1):100–103.
3. Kong F, Galzote C, Duan Y. Change in skin properties over the first 10 years of life: a cross-sectional study. Arch Dermatol Res. 2017;309(8):653–658.
4. Stamatas N. Early inflammatory processes in the skin. Curr Mol Med. 2013;13(8):1250–1269.
5. Dogra S, Kumar B. Epidemiology of skin diseases in school children: a study from northern India. Pediatr Dermatol. 2003;20(6):470–473.
6. Henshaw EB, Olasode OA, Ogedegbe EE, Etuk I. Dermatologic conditions in teenage adolescents in Nigeria. Adolesc Health Med Ther. 2014;5:79.
7. World Health Organization. Epidemiology and Management of Common Skin Diseases in Children in Developing Countries. World Health Organization; 2005.
8. Bezie Z, Deboch B, Ayele D, et al. Common skin diseases. Int Dev. 2005;13:200–204.
9. Hay RJ, Johns NE, Williams HC, et al. The global burden of skin disease in 2010: an analysis of the prevalence and impact of skin conditions. J Investigative Dermatol. 2014;134(6):1527–1534.
10. Kawshar T, Rajesh J. Sociodemographic factors and their association to prevalence of skin diseases among adolescents. Our Dermatology Online. 2013;4(3):45.
11. Sharma S, Bassi R, Sodhi MK. Epidemiology of dermatoses in children and adolescents in Punjab, India. J Pakistan Assoc Dermatologists. 2012;22(3):53.
12. Al Mendalawi M, Ibrahim J. Pattern of dermatoses in Iraqi children. EMHJEastern Mediterranean Health J. 2012;18(4):365–371.
13. Morrone A, Toma L, Franco G. Skin diseases highlighting essential global public health priorities. Int J Dermatol. 2005;44(5):384–390.
14. FDRE M. Scabies Outbreak Preparedness and Response Plan; 2015.
15. Diller KR, Khoshnevis S, Brothers M. Effects of Cold Temperature on the Skin. In: Dermatological Cryosurgery and Cryotherapy. Springer; 2016:39–43.
16. Figueroa JL, Fuller LC, Abraha A, Hay RJ. The prevalence of skin disease among school children in rural Ethiopia—a preliminary assessment of dermatologic needs. Pediatr Dermatol. 1996;13(5):378–381.
17. Janaki M, Jaiganesh D, Rajendran A. Prevalence of skin diseases among government primary school children in Pulianthope Zone, Chennai, India. Int J Recent Trends Sci Technol. 2013;9(2):182–185.
18. Lulu Y, Tolesa G, Cris J. Prevalence and associated factors of skin diseases among primary school children in Illuababorzone, Oromia Regional State, South West Ethiopia. Indo Am J Pharma Res. 2017;7(1):7374–7383.
19. Abdel‐Hafez K, Abdel‐Aty MA, Hofny ER. Prevalence of skin diseases in rural areas of Assiut Governorate, Upper Egypt. Int J Dermatol. 2003;42(11):887–892.
20. Amoran O, Runsewe-Abiodun O, Mautin A, Amoran I. Determinants of dermatological disorders among school children in Sagamu, Nigeria. Educ Res. 2011;2(12):1743–1748.
21. Khalifa K, Al Hadithi T, Al Lami F, Al Diwan J. Prevalence of skin disorders among primary-school children in Baghdad governorate, Iraq. EMHJEastern Mediterranean Health J. 2010;16(2):209–213.
22. Tulsyan SH, Chaudhary S, Mishra D. A school survey of dermatological disorders and associated socio-economic factors in Lucknow; a region of north India. Egyptian Dermatol Online J. 2012;8(2):4.
23. Mills A. Health care systems in low-and middle-income countries. New England Journal of Medicine. 2014;370(6):552–557.
24. Wagstaff A. Poverty and health sector inequalities. Bull World Health Organ. 2002;80:97–105.
25. Sula B, Uçmak D, Saka G, et al. Prevalence of skin disorders among primary school children in Diyarbakir, Turkey. Arch argent Pediatr. 2014;112(5):434–438.
26. Oyedeji O, Okeniyi J, Ogunlesi T, Onayemi O, Oyedeji G, Oyelami O. Parental factors influencing the prevalence of skin infections and infestations among Nigerian primary school pupils. Internet J Dermatol. 2006;3(2):1531–3018.
27. Atnafu DD, Tilahun H, Alemu YM. Community-based health insurance and healthcare service utilisation, North-West, Ethiopia: a comparative, cross-sectional study. BMJ open. 2018;8(8):e019613.
28. Chu S, Mehrmal S, Uppal P, Giesey RL, Delost ME, Delost GR. Burden of skin disease and associated socioeconomic status in Europe: an ecologic study from the Global Burden of Disease Study 2017. JAAD int. 2020;1(2):95–103.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.