Back to Journals » Advances in Medical Education and Practice » Volume 11
The Need for Transgender Healthcare Medical Education in a Developing Country
Authors Martins RS ![]() , Saleh R
, Saleh R ![]() , Kamal H, Gillani M, Merchant AAH, Munir MM, Iftikar HM, Shah Z, Hussain MHZ, Azhar MK, Qadri F, Saleem S
, Kamal H, Gillani M, Merchant AAH, Munir MM, Iftikar HM, Shah Z, Hussain MHZ, Azhar MK, Qadri F, Saleem S ![]()
Received 1 April 2020
Accepted for publication 13 May 2020
Published 8 June 2020 Volume 2020:11 Pages 405—413
DOI https://doi.org/10.2147/AMEP.S255483
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Video abstract presented by Raisa Saleh.
Views: 4194
Russell S Martins,1 Raisa Saleh,1 Hasan Kamal,1 Mishal Gillani,1 Asma AH Merchant,1 Muhammad M Munir,1 Hamza M Iftikar,1 Zara Shah,1 Muhammad HZ Hussain,1 Mohammad K Azhar,1 Fatima Qadri,1 Sarah Saleem2
1Medical College, Aga Khan University Hospital, Karachi 74800, Pakistan; 2Department of Community Health Sciences, Aga Khan University Hospital, Karachi 74800, Pakistan
Correspondence: Russell S Martins
Email [email protected]
Purpose: The single most significant barrier to healthcare for people who identify as transgender is poor access to healthcare providers trained in trans-health. Despite this, trans-health education is far from being a routine component of the undergraduate medical curriculum in developing countries like Pakistan. This study aimed to assess knowledge and attitudes regarding people who identify as transgender, as well as the perceived need for trans-health in the curriculum, amongst medical students in Pakistan.
Materials and Methods: A cross-sectional study using a self-designed questionnaire was carried out amongst undergraduate medical students at the Aga Khan University. Stratified random sampling was used, whereby students were stratified based on their current year of medical education.
Results: A total of 249 students were included in this survey. The majority (61%) had poor overall knowledge, with a significantly higher percentage of pre-clinical students (79.6%) having poor knowledge regarding differences in transgender health needs compared to clinical students (60.3%; p = 0.001). Most students acknowledged that individuals who identified as transgender faced a lack of access to healthcare (78.3%), were poorly integrated into society (92.0%) and were treated differently in a clinical setting (58.6%). Many students were unsure of how to address (49.8%) and clinically examine (38.2%) patients identifying as transgender. However, most students demonstrated good (49.4%) or fair (45.0%) attitudes towards individuals who identified as transgender, and the majority reported a high (54.6%) or moderate (42.2%) perceived need for the inclusion of trans-health in the medical curriculum.
Conclusion: Despite deficiencies in trans-health education in the medical school curriculum, positive attitudes and a high perceived need among students lay the foundation for developing a medical curriculum that gives due priority to trans-health. In developing countries, this can help bridge disparities in healthcare provision to people who identify as transgender.
Keywords: transgender, medical education, developing country, medical curriculum
Plain Language Summary
Globally, people who identify as transgender suffer severe disparities in healthcare provision, especially in developing countries such as Pakistan. A major reason for this is lack of access to providers who are well-trained in trans-health. Adding trans-health to the medical curriculum in developing countries could help reduce this barrier and educate doctors who are skilled enough to cater to the needs of people who identify as transgender.
We conducted a survey amongst medical students at the Aga Khan University, Pakistan. In this study, we assessed existing knowledge regarding the transgender identity, attitudes towards individuals and patients who identify as transgender, and the perceived need for adding trans-health to the curriculum.
Our results showed that although medical students currently lack sufficient knowledge regarding trans-health, they reported positive attitudes towards individuals who identify as transgender. Students also perceived a significant need for adding trans-health to the curriculum, as they felt this would make them better equipped to treat patients who identify as transgender. These findings are of benefit to the medical education system in Pakistan and other developing countries, as they lay a foundation for the development of trans-health curricula in medical schools.
Introduction
Individuals identifying as transgender, numbering around 25 million globally, face major disparities in healthcare.1 Although different spectrums of disease exist in this population,2,3 this aspect of medicine (termed “trans-health”) is reluctantly explored. In developing countries, such as Pakistan, the situation is even more alarming. Personal, societal and institutional prejudice against people who identify as transgender leads to low literacy and employment rates.3,4 This forces many into sex work and substance abuse.5,6 Moreover, healthcare systems are grossly ill-equipped to cater to their needs, with the biggest barrier being a lack of healthcare providers trained in trans-health.7
Medical students represent the doctors of the future. It is vital that they be trained to provide healthcare that can meet the needs of individuals identifying as transgender. Although trans-health is not routinely taught, studies in developed countries show the effectiveness of adding trans-health to the existing medical curriculum.8 Though nascent, these landmark educational interventions are improving knowledge and attitudes towards trans-health.9
However, healthcare systems in developing countries like Pakistan have yet to attribute priority to education in trans-health. The first step towards improving education and training in trans-health is to understand existing knowledge and attitudes of learners towards individuals and patients who identify as transgender. Thus, this study aims to assess knowledge and attitudes regarding the transgender identity, as well as the perceived need for trans-health in the medical curriculum, amongst medical students at the Aga Khan University, Pakistan.
Materials and Methods
A survey was conducted among the undergraduate medical students at the Aga Khan University (AKU) after obtaining ethical approval from the Institutional Review Board.
Sampling Technique
A minimum sample size of 216 was calculated using a precision level of 5%, an anticipated frequency of 50% and a confidence interval of 95%. The population size was 490 students, distributed across 5 classes (Years 1–5) of medical students currently enrolled at AKU. The first eleven authors of this study, themselves medical students, were excluded from the population.
Students were stratified according to the year of medical education (batch), and a random number generator was used to identify 65 students from each batch of 100 students. These students were approached by the members of the research team, and a signed informed consent for participation was obtained after the students were thoroughly briefed regarding the scope and nature of the study. Students were then provided the self-administered questionnaire in a Manila envelope to fill in an empty classroom to ensure their privacy. A member of the research team was available nearby for any clarifications regarding the questionnaire. No personal identifiers were recorded in the questionnaire, and the consent form was collected separately to ensure the anonymity of participants.
Data Collection Tool and Coding
The questionnaire used in this study (Appendix in Supplemental File) was self-designed by the research team in close association with the faculty at the Department of Community Health Sciences at AKU. The questionnaire was pretested on 5% of our population size to identify any ambiguity in the questions. Six questions were eliminated after the pre-test due to ambiguities. The final questionnaire had a high level of consistency (Cronbach’s alpha = 0.910) and contained the following six sections: (1) demographics, (2) knowledge, (3) perceptions and attitudes, (4) clinical experiences, (5) personal interactions, and (6) perceived need for trans-health within the medical curriculum.
Demographics
This section recorded students’ age, gender identity, year of medical education (batch), area of residence and ethnicity. Options for gender identity included cis-male, cis-female, transgender and others (please specify), to ensure participant inclusivity.
Knowledge: (2.1) Knowledge of the Transgender Identity and (2.2) Knowledge of Differences in Health Needs
According to the statement, Strongly Disagree/Disagree or Strongly Agree/Agree were scored as Correct (2 points) or Incorrect (0 points), while Unsure was scored 1 point. A total of each individual’s points was computed for each 10 question sub-section (2.1 and 2.2), leading to a total between 0 and 20 points for each sub-section. A cut-off of 75% (15/20) was used to categorize participants’ knowledge as Good Knowledge (≥15 points) or Poor Knowledge (<15 points) for each sub-section.
The total points for the sub-sections “2.1. Knowledge of the Transgender Identity” and “2.2. Knowledge of Differences in Health Needs” were summed, leading to a grand score for the section between 0 and 40 points. A cut-off of 75% (30/40) was used to categorize participants’ knowledge as Good Overall Knowledge (≥30 points) or Poor Overall Knowledge (<30 points).
Perceptions and Attitudes: (3.1) Societal Perceptions and (3.2) Personal Attitudes
In section 3.1 (Societal Perceptions), respondents were required to rate on a 5-point Likert Scale (Strongly Disagree to Strongly Agree) to what extent they agreed with statements regarding societal perceptions of individuals who identify as transgender. In section 3.2 (Personal Attitudes), responses to negatively phrased statements were recoded so that Strongly Agree and Agree represented positive attitudes towards individuals who identify as transgender and the transgender identity. Points were assigned to each response – Strongly Agree (5), Agree (4), Unsure (3), Disagree (2), Strongly Disagree (1) – and a total score was computed for the 14 questions in section 3.2 (ranging between 14 and 70 points). Cut-offs of 56 (4 x 14) and 42 (3 x 14) were used to categorize respondents’ attitudes as Good, Fair or Poor.
Clinical Experiences
Respondents were required to rate on a 5-point Likert Scale (Strongly Disagree to Strongly Agree) to what extent they agreed with statements regarding clinical encounters with individuals who identify as transgender.
Personal Interactions
Respondents were asked about their personal interactions with individuals who identify as transgender, as well as sources of information regarding trans-health.
Perceived Need for Trans-Health Within the Medical Curriculum
In Section 6, responses to negatively phrased statements were reworded so that Strongly Agree and Agree represented high perceived need for trans-health within the medical curriculum. Points were assigned to each response – Strongly Agree (5), Agree (4), Unsure (3), Disagree (2), Strongly Disagree (1) – and a total score was computed for the 14 questions in this section (ranging between 14 and 70 points). Cut-offs of 56 (4 x 14) and 42 (3 x 14) were used to categorize respondents’ perceived need as High, Moderate and Low.
Data Analysis
Statistical analyses were run using Statistical Package for Social Sciences (SPSS) version 21. Continuous data were reported as mean ± standard deviation and were compared using independent sample t-tests. Categorical data were reported as gross numbers and percentages (n; %) and was compared using chi-squared tests. Pearson’s correlation was used to explore significant associations between total scores of the knowledge (section 2), personal attitudes (section 3.2) and perceived need for trans-health within the medical curriculum (section 6) sections. A p-value of <0.05 was considered as significant for all analyses.
Results
Demographics
A total of 249 students responded to the questionnaire, fulfilling our minimum sample size and giving a response rate of 76.6%. Individuals identifying as cis males comprised 57.0% of the sample, with the remaining 43.0% identifying as cis females. None of the respondents in our study identified as transgender. The largest representation was from Year II (n = 61; 24.5%). The demographics of the respondents are shown in Table 1.
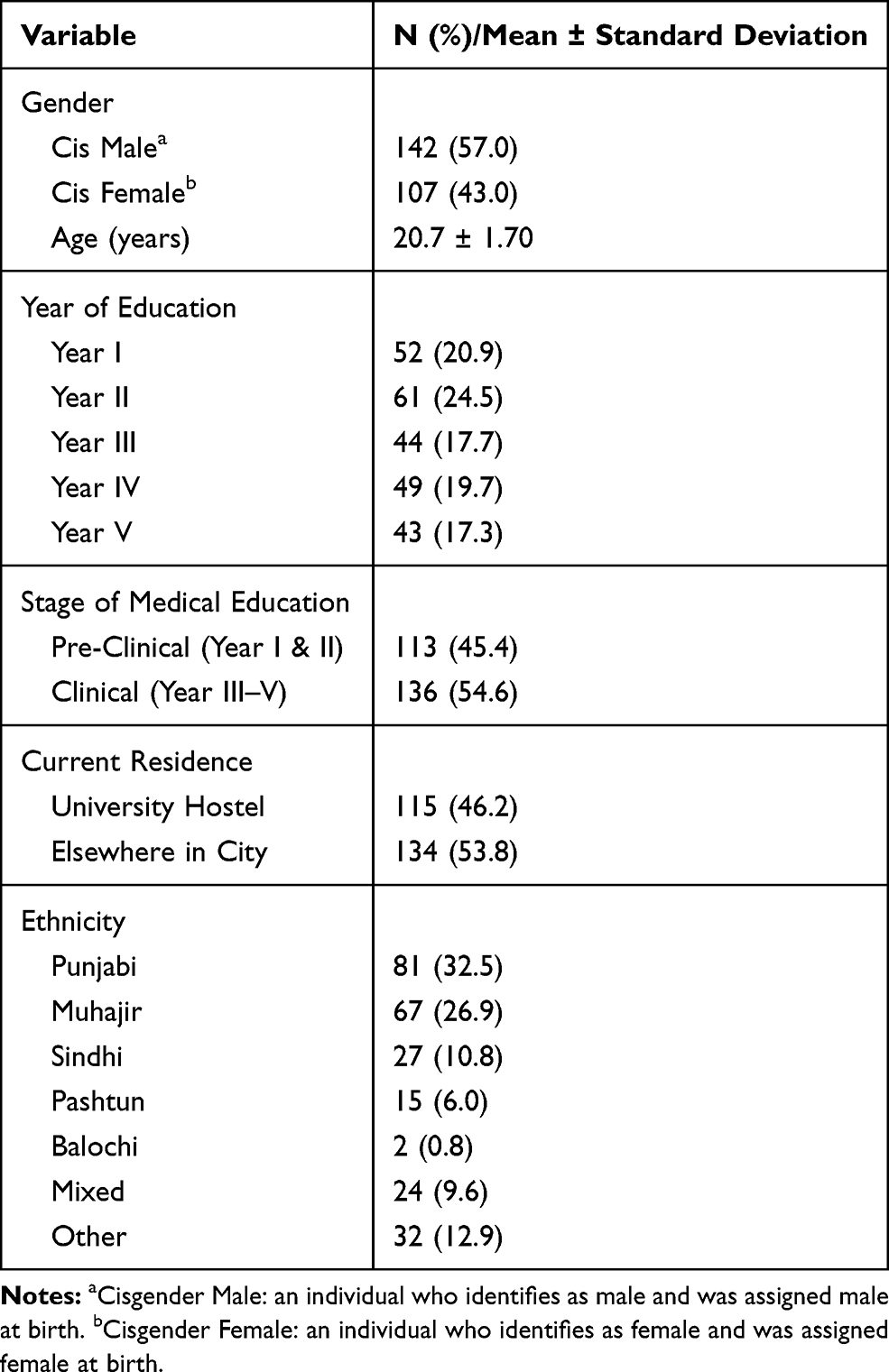 |
Table 1 Demographics (Section 1) |
Knowledge
The majority of students had Poor Overall Knowledge (n = 152; 61.0%). A significantly higher percentage of pre-clinical students had Poor Overall Knowledge as compared to clinical students (p = 0.004), while a significantly higher number of male students had Poor Overall Knowledge as compared to female students (p = 0.014). The results of the Overall Knowledge are shown in Figure 1.
 |
Figure 1 Percentage of students with poor overall knowledge; *p = 0.014; **p = 0.004. |
Knowledge of the Transgender Identity
The vast majority of students strongly disagreed/disagreed that the transgender identity was a disease state (82.7%), mental illness (80.3%), or a modern concept due to the influence of the media (70.3%). However, there were mixed responses to other statements in this section: 26.9% believed (strongly agreed/agreed) that gender identity was the same as sex assigned at birth and 28.5% that the transgender identity was an inherited condition. Moreover, 25.3% believed that the transgender identity was always a choice made by the individual. A significantly higher percentage of pre-clinical students believed that gender identity was synonymous with sexual orientation (29.2% vs 16.2%; p = 0.044) and the term “transgender” was synonymous with “transvestite” (9.7% vs 4.4%; p < 0.001). Additionally, a significantly higher percentage of male students believed that the transgender identity was a mental illness (7.7% vs 3.7%; p = 0.035) and a disease (8.5% vs 4.7%; p = 0.037). These results are shown in Supplementary Table.
Most of the respondents had Good Knowledge regarding the transgender identity (n = 147; 59%). There were no significant differences in the percentage of respondents with Good Knowledge of the transgender identity between pre-clinical and clinical students (53.1% vs 64.0%; p = 0.082) or male and female students (57.0% vs 61.7%; p = 0.461).
Knowledge of Differences in Health Needs
Most students acknowledged that patients who identify as transgender have unique health risks and needs (53.0%), with 51.8% agreeing that individuals who identify as transgender have a higher risk of mental illness and 50.6% that they have higher rates of suicide. However, a large percentage of students were unsure of whether individuals who identify as transgender are naturally sterile (40.2%), whether their population has a higher incidence of substance abuse (49.8%) or sexually transmitted illness (46.1%), and whether hormonal therapy makes individuals who identify as transgender more susceptible to certain conditions (58.7%). Nevertheless, most students felt that there are insufficient treatment guidelines (51.8%) and transgender health-related research (58.2%) to guide proper evidence-based treatment for individuals who identify as transgender. There were significant differences between pre-clinical and clinical students in responses to several statements. A significantly higher percentage of clinical students agreed that individuals who identify as transgender have a higher incidence of sexually transmitted illness (47.1% vs 27.4%; p = 0.003), higher rates of suicide (57.4% vs 42.5%; p = 0.007) and are more susceptible to certain conditions due to hormonal therapy (41.9% vs 22.1%; p = 0.004). A greater percentage of females disagreed that individuals who identify as transgender always have physical deformities (72.0% vs 56.3%; p = 0.008) and that there are sufficient guidelines for the treatment of individuals who identify as transgender (60.7% vs 45.1%; p = 0.040). These results are shown in Supplementary Table.
The majority of the respondents had Poor Knowledge regarding differences in health needs (n = 172; 69.1%). A greater percentage of pre-clinical students had Poor Knowledge of differences compared to clinical students (79.6% vs 60.3%; p = 0.001). There was no difference in the percentage of respondents with Poor Knowledge between male and female students (69.7% vs 68.2%; p = 0.801).
Perceptions and Attitudes
Societal Perceptions
The 5-point Likert Scale was collapsed to a 3-point scale (Strongly Disagree/Disagree, Unsure, Strongly Agree/Agree), and participants responding Unsure to any statement were excluded (not more than 25% of students responded Unsure to any statement). The response to each of the 11 statements in this sub-section is shown in Figure 2. Interestingly, a significantly higher percentage of males disagreed that individuals identifying as transgender face a lack of access to healthcare (13.4% vs 6.5%; p = 0.039), and were unsure of whether they experience rejection from their own families (12.0% vs 1.9%; p = 0.011). These results are shown in the Supplementary Table.
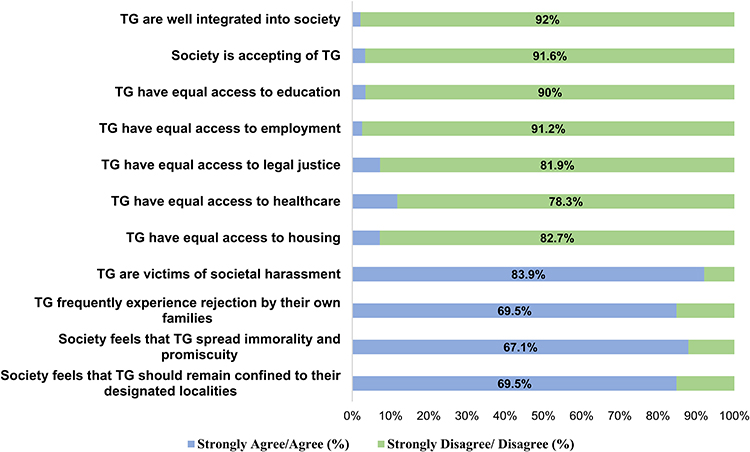 |
Figure 2 Societal perceptions; TG: individuals who identify as transgender; responses marked unsure are not included. |
Personal Attitudes
In this section, most students reported overall Good (49.4%) or Fair (45.0%) attitudes towards people who identify as transgender (Figure 3A). The majority of students reported that they were comfortable around individuals who identify as transgender (65.5%), that they would be comfortable treating a patient who identified as transgender (87.6%), and that they believed individuals who identify as transgender should be treated with the same respect and dignity as any other person (95.2%). Moreover, 78.3% agreed that individuals who identify as transgender should be facilitated to medically/surgically transition if they wished, and 77.5% agreed that they should be allowed to raise children. These results are shown in Supplementary Table.
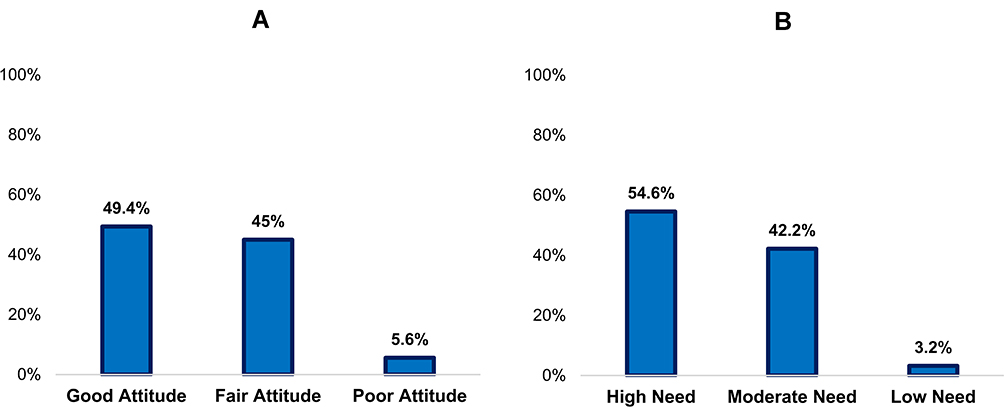 |
Figure 3 (A) Personal attitudes towards individuals who identify as transgender (Section 3b). (B) Level of perceived need for trans-health in medical curriculum (Section 6). |
Clinical Experiences
The greatest percentage of students Strongly Agreed/Agreed that patients who identify as transgender are treated differently (58.6%), that they would feel unsure of how to address (49.8%) and clinically examine (38.2%) patients who identify as transgender, and that they were unsure of the need for a chaperone while clinically examining patients identifying as transgender (34.1%). A significantly greater percentage of clinical students reported feeling unsure of how to address patients identifying as transgender as compared to pre-clinical students (54.4% vs 44.2%; p = 0.047). These results are shown in Supplementary Table.
Personal Interactions
Only 8 (5.9%) clinical students reported having interacted with a patient who identified as transgender in the clinical setting. However, 108 (43.4%) students reported having interacted on a personal basis outside the clinical setting with individuals who identify as transgender. Out of these students, 28 (25.9%) reported that the closest relationship they had with an individual who identified as transgender was as a friend while 37 (34.2%) reported similarly for acquaintance.
The commonest sources that students reported hearing or seeing transgender health-related information from were social media (89.6%), television/movies/documentaries (88.4%) and the news (78.3%). Only 51.0% reported having received such information from formal educational platforms such as classes or seminars.
Perceived Need for Trans-Health Within the Medical Curriculum
The majority (54.6%) of students reported a High perceived need for the inclusion of a trans-health component in the undergraduate medical curriculum (Figure 3B). Perceived need was associated with gender, with 63.6% of females having a High perceived need as compared to 47.9% of males (p = 0.012). There was no significant association of perceived need with being a pre-clinical or clinical student (p = 0.175).
In this section, the majority of students Strongly Agreed/Agreed that they needed to be taught medical history (85.2%), clinical examination (87.2%), and counseling (90.0%) of patients who identify as transgender. Moreover, the majority also felt that trans-health education would improve patient care quality (91.2%) and make them better doctors (88.8%). The majority also felt that incorporating trans-health into the routine medical curriculum would encourage individuals who identifed as transgender to seek help (92.0%), and ultimately improve the healthcare system of Pakistan (89.6%). These results are shown in Supplementary Table.
Correlations Between Knowledge, Attitudes and Perceived Need
A significant positive correlation was found between personal attitudes towards individuals identifying as transgender and the perceived need for trans-health within the medical curriculum (r = 0.335; p < 0.001). Similarly, a significant positive correlation was found between overall knowledge with both perceived need (r = 0.219; p = 0.001) and personal attitudes (r = 0.323; p < 0.001).
Discussion
Medical education is a fundamental means to address health inequities faced by people who identify as transgender.10 To our knowledge, this is the first study to assess the need for trans-health in medical education in a developing country. Our results show that despite deficiencies in knowledge regarding transgender healthcare, students’ attitudes towards individuals who identify as transgender are generally positive and there is a high perceived need for the introduction of trans-health into the undergraduate medical curriculum.
The growing commitment to transgender healthcare is reflected by the World Health Organization’s (WHO) agenda to improve transgender healthcare globally,3 especially in low- and middle-income countries.1 In this regard, the WHO strongly endorses the inclusion of trans-health into mainstream medical curricula.1 Embodying this ethos, medical education systems in developed countries have taken steps to incorporate trans-health into their curriculum.
In 2007, the Association of American Medical Colleges (AAMC) published a series of best practice recommendations for medical institutions to address the health needs of individuals identifying as transgender.11 Coursework included appropriate social and sexual history-taking, transgender-related community-based clerkships, transgender-related endocrinology and transgender-related psychiatry. Following AAMC recommendations, the Lesbian, Gay, Bisexual, & Transgender Medical Education Research Group (LGBT MERG) was founded at the Stanford University School of Medicine. LGBT MERG has emerged as a pioneer for trans-health research in the US. A nation-wide survey showed that across all 176 allopathic and osteopathic medical schools in US and Canada, the time dedicated to trans-health curricula was low, and the quality of educational interventions was extremely variable.12 A subsequent survey of medical students (n = 9522) across these 176 medical schools revealed that most students rated their LGBT-related curriculum “fair”, “poor” or “very poor”, and emphasized that more curricular coverage was called for.13 This is reflected in the results of our study, which show deficiencies in knowledge but a high perceived need for trans-health curricula.
At Boston University, a survey revealed generally poor knowledge across medical students, with pre-clinical students having poorer knowledge than clinical students.14 This pattern is reflected by our study as well, as the majority of students had poor overall knowledge, with a greater percentage of pre-clinical students having poor knowledge. Moreover, our study also shows the high degree of uncertainty anticipated by medical students concerning interactions with patients who identify as transgender. On a positive note, the study highlighted the eagerness of medical students towards learning opportunities regarding trans-health, as well as the amenability of the knowledge deficiencies to educational interventions.14 Once again, similar results are seen in the high levels of perceived need displayed by the students in our study. Trans-health curriculum additions at Boston University include didactic sessions on the biology of gender identity and strategies of hormone therapy for patients who identify as transgender,8,15 as well as clinical rotations with patients who identify as transgender.16 All of these interventions improved knowledge and increased comfort of medical students in trans-health.
A holistic approach to reducing disparities in transgender healthcare is emphasized, focused on increased awareness, comfort, knowledge and skills.17 At other institutions in North America, clinical year students exposed to patients identifying as transgender are often subsequently more comfortable working with such patients, as well as more knowledgeable regarding their healthcare.16,18 Other interventions, such as interactive patient panels, small-group discussions and standardized patients offer varying degrees of effectiveness in helping bridge the gap in transgender health proficiency.19–25 In addition to this, a study at the Northern Ontario School of Medicine also identified suitable assessment modalities for testing the effectiveness of interventions.25 Interventions have been shown to be most effective when longitudinally taught and pedagogically based on clinical skills.9,25
Student-led interventions have been shown to be particularly effective in improving other students’ knowledge and confidence in delivering transgender healthcare.26 Interestingly, LGBT MERG at Stanford University was founded by medical students, and this study itself is also an initiative of medical students at the Aga Khan University. It is possible that the steady overall societal decrease in transphobia and increase in awareness regarding the rights of individuals identifying as transgender manifest most powerfully amongst the most junior in our healthcare system. Medical students, in our study and others,13,14,25,27 report generally positive attitudes towards individuals who identify as transgender, in the face of exceedingly negative societal perceptions. However, although a study in Canada reported no association between level of knowledge and comfort with individuals identifying as transgender25, our results show a weak but significant positive correlation between knowledge and personal attitudes.
To spark the required change in the medical education system in developing countries, institutions can draw guidance from resources available through institutions in developed countries. LGBT MERG recommends several resources to help build a transgender-friendly medical education and healthcare system, including recommendations regarding core competencies and surveillance methods for intervention quality and impact.28 Additionally, organizations such as The World Professional Association for Transgender Health and the Endocrine Society have also developed comprehensive best-practice guidelines to promote the highest standards of healthcare for individuals identifying as transgender.29,30 These resources can provide valuable guidance for institutions seeking to develop a trans-health component in their medical curriculum. Developing countries will likely face many challenges in this undertaking, a major one being to overcome a hardwired transphobic culture that exists in many organizations.31
The student population at the Aga Khan University come from diverse social and ethnic backgrounds across the country, boosting the generalizability of this study. The multiple measures of anonymity employed ensured a high response rate and low social desirability bias. This, in conjunction with the stratified random sampling method used, contributes to a low response bias, which has been a limitation of previous studies. Moreover, the questionnaire in this study was adapted using elements from pre-existing questionnaires,32–34 and was constructed in close collaboration with the Aga Khan University’s Department of Community Health Sciences. Thus, the development of the questionnaire was informed by faculty experts in Community Medicine, Reproductive Health and Epidemiology, who contributed their perspectives gained from working with community members and patients who identify as transgender. The questionnaire also demonstrated a high degree of internal consistency.
Limitations of this study include it lacking the perspective of medical educators and curriculum experts, as well as the personal perspective of individuals who identify as transgender. However, these gaps represent a rich potential for further research.
Conclusion
The undergraduate medical curriculum is currently ill-equipped to bridge the healthcare disparities faced by individuals who identify as transgender, in developing countries like Pakistan. There are obvious deficiencies in knowledge amongst medical students, our doctors of the future, regarding transgender healthcare. However, positive personal attitudes of medical students towards individuals identifying as transgender and a high student-perceived need for trans-health education lay the foundation for creating a medical curriculum that gives due priority to transgender healthcare in developing countries.
Data Sharing Statement
The Supplemental Table in the Supplemental File contains all participants’ responses to the survey.
Ethics Approval
This study was approved by the Institutional Review Board of the Aga Khan University.
Acknowledgments
We acknowledge the Department of Community Health Sciences at the Aga Khan University and its faculty and staff for providing us with support throughout this project, including study design, questionnaire development and data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Aaron O. Growing recognition of transgender health. Bull World Health Organ. 2016;94:790–791.
2. Feldman J, Brown GR, Deutsch MB, et al. Priorities for transgender medical and health care research. Curr Opin Endocrinol Diabetes Obes. 2016;23(2):180. doi:10.1097/MED.0000000000000231
3. Thomas R, Pega F, Khosla R, Verster A, Hana T, Say L. Ensuring an inclusive global health agenda for transgender people. Bull World Health Organ. 2017;95(2):154. doi:10.2471/BLT.16.183913
4. Nazir N, Yasir A. Education, employability and shift of occupation of transgender in Pakistan: a case study of khyber pakhtunkhwa. Dialogue (Pakistan). 2016;11(2).
5. Haq N, Riaz S, Nasim A, Tahir M. The transgender prostitution: threat to the rise of AIDS in Pakistan. J Infect Public Health. 2017;11.
6. Shah H, Rashid F, Atif I, et al. Challenges faced by marginalized community such as transgender in Pakistan. Pan Afr Med J. 2018;30.
7. Sanchez NF, Sanchez JP, Danoff A. Health care utilization, barriers to care, and hormone usage among male-to-female transgender persons in New York City. Am J Public Health. 2009;99(4):713–719. doi:10.2105/AJPH.2007.132035
8. Safer JD, Pearce EN. A simple curriculum content change increased medical student comfort with transgender medicine. Endocr Pract. 2013;19(4):633–637. doi:10.4158/EP13014.OR
9. Dubin SN, Nolan IT, Streed CG
10. Mayer KH, Bradford JB, Makadon HJ, Stall R, Goldhammer H, Landers S. Sexual and gender minority health: what we know and what needs to be done. Am J Public Health. 2008;98(6):989–995. doi:10.2105/AJPH.2007.127811
11. Joint A-G. AAMC-OSR Recommendations Regarding Institutional Programs and Educational Activities to Address the Needs of Gay, Lesbian, Bisexual and Transgender (GLBT) Students and Patients. Washington, DC: Association of American Medical Colleges; 2007. 74–77.
12. Obedin-Maliver J, Goldsmith ES, Stewart L, et al. Lesbian, gay, bisexual, and transgender–related content in undergraduate medical education. JAMA. 2011;306(9):971–977. doi:10.1001/jama.2011.1255
13. White W, Brenman S, Paradis E, et al. Lesbian, gay, bisexual, and transgender patient care: medical students’ preparedness and comfort. Teach Learn Med. 2015;27(3):254–263. doi:10.1080/10401334.2015.1044656
14. Liang JJ, Gardner IH, Walker JA, Safer JD. Observed deficiencies in medical student knowledge of transgender and intersex health. Endocr Pract. 2017;23(8):897–906. doi:10.4158/EP171758.OR
15. Eriksson SE, Safer JD. Evidence-based curricular content improves student knowledge and changes attitudes towards transgender medicine. Endocr Pract. 2016;22(7):837–841. doi:10.4158/EP151141.OR
16. Park JA, Safer JD. Clinical exposure to transgender medicine improves students’ preparedness above levels seen with didactic teaching alone: a key addition to the Boston University model for teaching transgender healthcare. Transgender Health. 2018;3(1):10–16. doi:10.1089/trgh.2017.0047
17. Awosogba T, Betancourt JR, Conyers FG, et al. Prioritizing health disparities in medical education to improve care. Ann N Y Acad Sci. 2013;1287(1):17. doi:10.1111/nyas.12117
18. Sanchez NF, Rabatin J, Sanchez JP, Hubbard S, Kalet A. Medical students’ ability to care for lesbian, gay, bisexual, and transgendered patients. Fam Med Kansas City. 2006;38(1):21.
19. Kelley L, Chou CL, Dibble SL, Robertson PA. A critical intervention in lesbian, gay, bisexual, and transgender health: knowledge and attitude outcomes among second-year medical students. Teach Learn Med. 2008;20(3):248–253. doi:10.1080/10401330802199567
20. Hollenbach AD, Eckstrand KL, Dreger AD. Implementing Curricular and Institutional Climate Changes to Improve Health Care for Individuals Who are LGBT, Gender Nonconforming, or Born with DSD: A Resource for Medical Educators. Association of American Medical Colleges; 2014.
21. Parkhill AL, Mathews JL, Fearing S, Gainsburg J. A transgender health care panel discussion in a required diversity course. Am J Pharm Educ. 2014;78(4):81. doi:10.5688/ajpe78481
22. Wallick MM, Cambre KM, Townsend MH. Influence of a freshman-year panel presentation on medical students’ attitudes toward homosexuality. Acad Med. 1995.
23. Brondani MA, Paterson R. Teaching lesbian, gay, bisexual, and transgender issues in dental education: a multipurpose method. J Dent Educ. 2011;75(10):1354–1361.
24. Sullivan W, Eckstrand K, Rush C, Peebles K, Lomis K, Fleming A. An intervention for clinical medical students on LGBTI health. MedEdPORTAL. 2018.
25. Dudar KJ, Ghaderi G, Gallant J, Dickinson J, Abourbih J, Briggs M. Queering the medical curriculum: how to design, develop, deliver and assess learning outcomes relevant to LGBT health for health care professionals. MedEdPublish. 2018;7(1). doi:10.15694/mep.2018.0000048.1
26. Grosz AM, Gutierrez D, Lui AA, Chang JJ, Cole-Kelly K, Ng H. A student-led introduction to lesbian, gay, bisexual, and transgender health for first-year medical students. Fam Med. 2017;49(1):52–56.
27. Nama N, MacPherson P, Sampson M, McMillan HJ. Medical students’ perception of lesbian, gay, bisexual, and transgender (LGBT) discrimination in their learning environment and their self-reported comfort level for caring for LGBT patients: a survey study. Med Educ Online. 2017;22(1):1368850. doi:10.1080/10872981.2017.1368850
28. MERG L. LGBT MERG resources; 2020. Available from: http://med.stanford.edu/lgbt/resources.html.
29. Hembree WC, Cohen-Kettenis PT, Gooren L, et al. Endocrine treatment of gender-dysphoric/gender-incongruent persons: an endocrine society* clinical practice guideline. J Clin Endocrinol Metab. 2017;102(11):3869–3903. doi:10.1210/jc.2017-01658
30. Coleman E, Bockting W, Botzer M, et al. Standards of care for the health of transsexual, transgender, and gender-nonconforming people, version 7. Int J Transgend. 2012;13(4):165–232. doi:10.1080/15532739.2011.700873
31. Lunn MR, Obedin-Maliver J. Lesbian, gay, bisexual, and transgender health and medical education—reply. JAMA. 2011;306(21):2326–2327. doi:10.1001/jama.2011.1783
32. Kanamori Y, Cornelius-White JH, Pegors TK, Daniel T, Hulgus J. Development and validation of the transgender attitudes and beliefs scale. Arch Sex Behav. 2017;46(5):1503–1515. doi:10.1007/s10508-016-0840-1
33. Kooy RE. Knowledge and Attitudes Toward Trans Persons. Humboldt State University; 2010.
34. Rowan SP, Lilly CL, Shapiro RE, et al. Knowledge and attitudes of health care providers toward transgender patients within a rural tertiary care center. Transgender Health. 2019;4(1):24–34. doi:10.1089/trgh.2018.0050
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.