Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
The Multidisciplinary Perioperative Management of Conjoined Twin Separation Surgery During the Pandemic
Authors Giwangkancana G ![]() , Kusmayadi DD, Kadi F, Utariani A, Haryawan Z
, Kusmayadi DD, Kadi F, Utariani A, Haryawan Z ![]()
Received 24 September 2022
Accepted for publication 10 November 2022
Published 18 November 2022 Volume 2022:15 Pages 2669—2678
DOI https://doi.org/10.2147/JMDH.S390419
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gezy Giwangkancana,1,2 Dikki Drajat Kusmayadi,3 Fiva Kadi,4 Arie Utariani,2 Zahran Haryawan5
1Department of Anesthesiology and Intensive Care, Faculty of Medicine Universitas Padjadjaran/Dr. Hasan Sadikin National Referral Hospital, Bandung, West Java, Indonesia; 2Sub-Specialistic Study of Pediatric Anesthesia Study Faculty of Medicine Universitas Airlangga Surabaya, Surabaya, East Java, Indonesia; 3Department of Pediatric Surgery, Faculty of Medicine Universitas Padjadjaran/Dr. Hasan Sadikin National Referral Hospital Bandung, Bandung, West Java, Indonesia; 4Division of Neonatology, Department of Pediatrics, Faculty of Medicine Universitas Padjadjaran/Dr. Hasan Sadikin National Referral Hospital Bandung, Bandung, West Java, Indonesia; 5Faculty of Medicine Universitas Padjadjaran, Bandung, West Java, Indonesia
Correspondence: Gezy Giwangkancana, Tel +628122005952, Email [email protected]
Background: Conjoined twin management, especially separation surgery, is a complex procedure which requires multidisciplinary work in the perioperative period. This complexity further increased with the COVID-19 pandemic, where social distancing protocols and the general reduction in non-COVID-19-related health-care services added a new dimension to the modern form of teamwork.
Methods: This study focused on the process of preparation for conjoined twin separation surgery during the pandemic from March 2020 to May 2022 with pre-pandemic era comparison. We described the decision-making process and the available facilities in terms of equipment, human resources, and the inclusion of information and technology.
Results: Among the essential requirements for separation surgery are doctors from various disciplines, pediatric anesthesiologists, nurses from different specialties, radiologists, rehabilitation specialists, nutritionists, pharmacists, psychologists, social workers, public relations, and information and technology staff. The team composition may change depending on the patient’s clinical characteristics and social needs. Surgery preparation consists of a prognostication period, preoperative management, surgery, and discharge.
Conclusion: Complex surgery such as conjoined twin separation can be managed effectively by a team of multidisciplinary experts. The application of information technology, to manage changes in multidisciplinary work pre- and post-pandemic, can reduce pandemic-related social restrictions while maintaining effectiveness and increasing efficiency.
Keywords: coronavirus, COVID-19, emergency, management, operating room, pandemic, surgery
Highlights / Major Themes
- Management and preparation of conjoined twin separation surgery requires multidisciplinary work, including medical and non-medical personnel.
- Telemedicine, online meeting platforms, and long-distance data sharing during the pandemic increases effectiveness and efficiency of conjoined twin management.
- Checklists and simulations increase team effectiveness and reduce errors.
- Fundings may include national insurance, private or non-governmental organization, and community involvement through charity.
Background
Conjoined twins (CJ) always have and will be a source of human awe and medical interest. Conjoined twins extremely rare, since their incidence is reported at 1:1000.000 to 1:200.000 live births.1–3 Although there were reports dating back to 1000 years BC on CJ, actual documentation of this unique human form was popularized by the circus owner P.T. Barnum. In 1811, Chang and Eng, the first well-known CJ, traveled with Barnum’s circus all around Europe, and until now, the term “Siamese” twins is well known due to their Thai origin.1
Based on their site of attachment, CJ are classified as cephalopagus (face), craniopagus (skull), ischiopagus (pelvis), omphalopagus (abdomen), pyopagus (gluteal/terminal spine/sacrum), thoracopagus (thorax), and rachipagus (back).4 Combination of attachments could also be found, such as thoraco-omphalopagus, where the thoracic cage and the abdomen are attached. Sites of attachment and the extent of organ shared determine surgical separation’s viability and prognosis.1–4
The development of modern medicine, especially in radio imaging, surgery, and anesthesia, has allowed many conjoined twins to undergo separation surgery to become single entities and live a full life.5–7 Few surgeries have as much complexity as the surgical separation of a conjoined twin. The separation requires massive planning and multidisciplinary cooperation during the perioperative period.
Preparation for conjoined twin separation is complicated with the COVID-19 pandemic in 2020. Although all elective surgery were postpones in the early pandemic era but were soon resumed and hence several containment protocols during the pandemic such as lockdowns and social restrictions plus reduction in hospital capacity and resources for handling non-COVID-19 patients, presented conjoined twin management team with various obstacles and also opportunities never before seen. We aim to describe the multidisciplinary approach for perioperative management of conjoined twin separation surgery during the pandemic era. Secondly we aim to describe conjoined twins managed in our center from 2012 to 2020.
Method
This study was a restrospective descriptive study of conjoined twins management from March 2020 to May 2022 with reference to cases that started in 2012, in a tertiary referral and teaching hospital in Indonesia. The setting of this study was in a 1000-bed government-owned hospital where Conjoined Twin Special Unit (CTSU) started performing separation surgery in 2012 and, by May 2022, had completed the separation of seven conjoined twins, observed one separation in a district hospital, and managed a total of 24 conjoined twins within 10 years (Table 1).
 |
Table 1 Characteristics of Conjoined Twins Managed in Dr Hasan Sadikin National Referral Hospital 2012–2022 |
Our hospital review board considered this study a quality improvement project, not human research; hence the Institutional Review Board (IRB) waived consent requirements. The observations and data collected in this study are connected to our co-study regarding conjoined twins reviewed which was given ethical clearance or the IRB number: LB.02 0.01/X.6.5/296/2021. Epidemiological data from our co-study is presented in this paper. The Standards for QUality Reporting Excellence (SQUIRE) were used as a general guideline for writing this report.
Results
A task force was formed to manage conjoined twins in 2012. The task force consisted of three prominent members: a task force leader, a vice leader, and a secretary. The team leadership could be changed but generally consisted of a pediatric surgeon, an anesthesiologist, and a neonatologist. The task force included members such as a fetomaternal obstetric specialist, pediatric sub-specialties in multiple fields, including surgeons, anesthesiologists, radiologist, cardiologist, nutritionist, intensivist, developmental specialist, physical rehabilitation specialist, psychologist, and social worker. The surgeons were specialized in pediatric, cardiothoracic, plastic and reconstruction, urology, orthopedic, vascular, and neuro surgery. Upon completion of the separation surgery, a supporting team consisting of a non-medical team including a pharmacist, an information and technology officer, public relations, human welfare, finance, and other hospital management were deployed. Team was supervised by the medical ethic committee as an independent body outside the team (Figure 1).
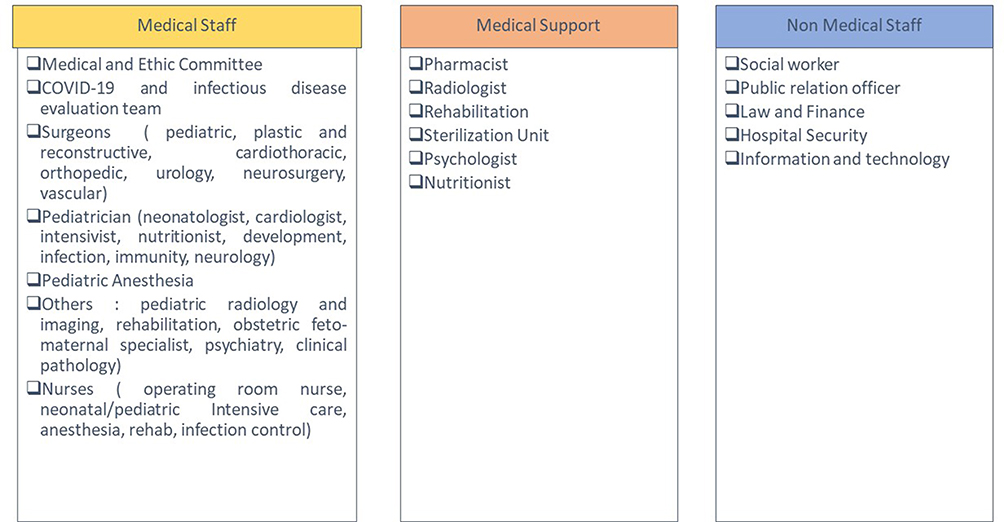 |
Figure 1 Conjoined -Twin Management Team Members. |
Phase One: Prognostication
All pregnancies with suspected conjoined twin diagnosis in our referral area, which included West Java with some parts of Sumatera and Kalimantan, were encouraged to opt for assisted birth via elective cesarean section in our hospital. This outreach were carried out by our fetomaternal department and adjoining national body, the Indonesian Association of Obstetrics and Gynecologists, and the regional Indonesian Ministry of Health. This policy was taken to ensure the safety of both mother and child since labor of the conjoined twins may be complicated by life-threatening issues, such as hanging breech labor, uterine rupture, obstructed labor, or arrest of descent.8–11 During labor, a perinatologist with conjoined twin specialization was present to provide rapid stabilization to the twins. An intensive neonatal unit with respiratory support and round-the-clock care was prepared for the twins. Centralized birth also provided a quick and efficient prognostic imaging study. Multiple imaging modalities, such as ultrasonography (USG), computed tomography (CT scan), angiography, and magnetic resonance imaging (MRI), were used, organized by a pediatric radiologist and cardiologist. It is important to note that an MRI scan involving conjoined twins is challenging since two sets of MRI-suitable metal-free anesthetic and monitoring sets are needed. Technically, older patients, especially the ischiophagus type with dangling legs on each side, may not fit inside an MRI machine. Hence, at our center, MRI requires an anesthetic and radiological technical preparation not discussed in this paper.
The centralized specialized care model (CSCM) we adopted at our center was developed from similar models in the United Kingdom,12 Nordic countries, and13 France.14 The CSCM model which was initially developed for high-risk rare pediatric cases, such as biliary atresia, premature infant surgery, and children transplant, has been shown to improve survival and lower morbidity.12–14
Early after birth, both twins were stabilized, though there are cases in our center where one or both children did not survive the first 24 hours of life. A series of imaging was conducted within the hour of birth, and the twins were deemed fit. Further team meetings were set up for early organ evaluation, which was critical since, in some cases, there was a possibility of an emergency separation.3,15,16 The meeting took place 48 hours after birth, supervised by the hospital ethical committee.
Phase Two: Preparation
If surgical separation was deemed possible, elective surgery at our center would be scheduled when each childr weighed at least 5 kilograms and were more than 8 months old at the time of separation. This policy was taken based on our experience with survival and time from surgery to discharge (Table 1).
Separation timing may differ from center to center and may involve other variables, such as nutrition status, emergency status, and type of conjoined twins. A meta-analysis of thoracophagus twin separation showed that the median age at separation was 47 days in 92 cases (IQR 12, 120), with 51% survival. The same study concluded that, in thoracophagus patients, the outcome was better (70% vs 17%, p < 0.0001) if the children were older during their separation (93 days vs 9 days) and the surgery was elective.17
A systematic review concluded that late surgery performed before 10–12 months is linked to successful separation, but another study recommended early separation around 3 months of age, which is linked to an increased incidence of wound infection.5,18 Several technical aspects need to be considered, like older children provide a more accessible technical approach for the anesthesiologist to access their airway and for the use of invasive monitoring devices. The additional time also provides a window for better preoperative evaluation, enough tissue expansion for future repair, and time for the multidisciplinary team to prepare for their work. As they are frequently premature and underweight at birth, it enables the patients to reach crucial developmental milestones, like independent feeding for proper weight gain and basic vaccination requirements for better survival in the future.
Nutrition and overall growth-development were essential to wound healing and survival in pediatric surgery.19 This aspect was controlled religiously by a dedicated team. Before the pandemic, our team provided this procedure, but since our movements were limited during social distancing, we recruited a small team in various district hospitals and primary health-care workers where the patients originated. Telemedicine and chat message applications (WhatsApp, USA) were then used to monitor their progress.
Telemedicine using several platforms (Zoom, USA and Google Meet, USA) has taught us about a new health-care organization in a context of cost-effectiveness and, hence, given us the ability to effectively and efficiently manage our remote patients. Telemedicine promotes effective coordination and interprofessional collaboration, which is permitted and controlled by hospital-health-territory law. The COVID-19 pandemic contributed to our team’s development toward improving our referral and teaching hospital role to our associated district hospitals through the involvement of technology.20
In Indonesia, separating conjoined twins costs between 20,000 USD and 60,000 USD. This cost can be funded privately, partially through national insurance or community involvement. Crowdfunding is a practical option for fund procurement. Social networking is leveraged to connect charitable benefactors with patients who have unmet medical needs. Donations are commonly used to collect funds for exceptional cases and rare diseases worldwide while the development of social media platforms helped catapeled the ease of information spreading and further assist crowdfunding. In Charlie Gard’s case, over one million dollars were collected within 6 months.21
Preoperative Phase
Before the pandemic, our protocol stated that the patient should be brought to our outpatient department multiple times in the months before surgery and 7 days before the separation procedure for preoperative examination, but during the pandemic, this step was taken over by the district hospitals using a. Consequently, the patients were admitted to our center 3–5 days before the surgery for a final preoperative examination, blood product preparation, microbial testing, and COVID-19 polymerase chain reaction (PCR) testing. During this time, a support team led by a psychologist, a social worker, a religious leader, and volunteers who were parents of our previous conjoined twins provided the CJ parents with sessions to provide mental support and encouragement. Several studies have found that support groups improve patient satisfaction and experience during perioperative period, especially in pediatric surgery.22
The last step of the preoperative phase is technical preparation and pre-op simulation. Our hospital created a specific central operating theatre workflow enhanced by a rundown checklist. These checklists were separated into a general rundown, anesthesia, surgery, infection control, and media and information. This preparation was also designated for non-medical aspects. Our central operating theatre had a multimedia room. Multimedia room and online meeting platforms enamble other physicians, nurses,residents and students who did not participate directly in the procedure could observe the surgery while maintaining social distancing protocol. Simulation with all team members present was done on the day before surgery. Media coverage was performed while maintaining patient protection policy of our center.
Surgery
On the day of surgery, two operating rooms and an educational media room were prepared. One master operating room with video-conferencing technology was staged as the primary operating theatre. A second operating room adjoining the master operating room was also prepared. The anesthesia team prepared the room layout according to the type of conjoined twin to be separated. This layout mainly consisted of an operating table or a modified one according to the patients’ size and anatomy, three anesthesia machines, two drug trolleys, two airway trolleys, two video laryngoscopes, two ultrasound machines, and two sets of other required tools, such as defibrillators and suctions, all of which were regulated in the preparation checklist (Figure 2).
 |
Figure 2 Preparation for Conjoined twin separation surgery. (A) Note the use of manikin-babies for simulation purposes. (B) Preoperative simulation involving all team members. (C) Media room and spokesperson. (D) Information and technology control room for education, reporting, and information purposes. (E) Two color codes (pink and blue) were used to mark the patients, team members, and equipment. |
Clinical communication in the team was maneuvered using a control table with the patient’s primary data, lab results, emergency doses, critical time during separation, and point of testing results. The central operating theatre also prepared required sets and drapes according to the patients’ needs.
The patient’s preparation during the day of surgery began with admission to the operating theatre based on the agreed timeline. A standard patient safety checklist was commenced. To reduce crowding during the pandemic, only the anesthesia team was allowed inside the master operating room during induction. The hospital infection prevention staff continuously monitored the surgery on-site and applied social distancing and infection control protocols.23 A requirement of vaccination and booster dose completion, noted on the national vaccination application for COVID-19 (PeduliLindungi, Indonesian Ministry of Information), was also applied for staff and visiting observers.
A senior pediatric anesthesiologist headed the anesthesia team, consisting of two anesthesia team leaders (pink and blue team) as airway managers, two anesthesiologists as drugs and circulation staff, three anesthesia residents on each team, and two anesthetic nurses. The patient was positioned according to their severity, where the “healthier” twin was placed closest to the exit for easier transport upon separation. Induction procedure started with the more severe or “frail” twin due to fear of complications and drug transmission to the healthier child. Upon the second twin’s induction, the patients were draped and invasive monitoring devices were placed (arterial line and central venous canulation).3
Surgery was conducted after the anesthesia team announced that it was safe to commence. The twins were surgically prepped, and the skin incision was made by the plastic surgeons according to the incision drawings and planning. Skin drawings were necessary since the exposed organs’ closure highly depended on the first incision. After completion of the musculocutaneous incision on the connection bridge tissue, fused organs were separated by a specific surgeon. For example, the pediatric surgeon performed separation using a harmonic scalpel in patients twin where the liver is fused. In the case of a thoracoabdominophagus, a cardiothoracic surgeon first separates the sternum, pericardium, or other related structures. In the case of ischiopagus twins, the urologic and orthopedic surgeon would have more prominent roles. Each conjoined twin case would have a very tailored approach.
After separating the twins, the anesthesiologist moved the more stable twin to the adjoining room, where closure was made. Surgery was planned to be as short as possible, and surgery would be planned in stages whenever complications with time may be seen. During the surgical procedure, a live training video was broadcasted to a lecture room and an online discussion link (Zoom app; USA), where students could follow the surgery without being present in the operating room.24 Later, both children were sent to pediatric intensive care for further treatment (Figure 3).
 |
Figure 3 Conjoined Twins Separation. (A) Anesthesia induction. (B) Surgery, note that the surgical team leader (doctor with glasses) continuously supervises different surgical departments. (C) Twins separated, note that team pink and team blue (marked by colored hair caps) were focused only on one twin each. (D) Pediatric critical care. (E) Discharge meeting with parents, rehabilitation specialist, pediatrics, and social worker. (F) Discharge. |
Discharge
Both children would be discharged after a complete evaluation by all members of the team of specialists. Evaluation was needed for specific conditions anticipated by each medical field, vaccination status, nutritional status, and assessment by a medical rehabilitation specialist. As conjoined twins are rare and unique, the medical rehabilitation specialist would arrange a particular program and equipment to aid the development of the patients. As local primary health care played a significant role in the preparation phase of the separation, it would also have a vital role in assessing the separated conjoined twins in coordination with our center. The patient’s follow-up must be done continuously because the management of the conjoined twins was not finished after the separation. The follow-up management would help the patients maintain their stable condition, adapt to new body forms, and achieve developmental milestones to survive well.5 In the child’s life, the separation process is crucial during the time of a diagnosis, during surgery, and in the event of difficulties. Finally, it was time to advise parents on creating rituals to help them deal with their issues during these times of increased commotion and stress. Each additional area of care was enhanced by psychological assistance. A single child’s illness can upset the dynamics of the entire family. As a result, the strategy should be both comprehensive and sympathetic.25
Discussion
Unique ethical and palliative care challenges are present in any conjoined twin case. The formation of a team facilitates the development of care objectives that direct decision-making by fostering communication between the medical team and the patient’s family. Regardless of the intended course of therapy, they are crucial in assisting the families. The team’s interdisciplinary structure encourages this assistance, which may be of a social or spiritual nature.
Kallberg stated that before conjoined twins’ developing personalities provide a solid indicator of whether they prefer separation and whether they will realize the benefits of being separated, it is unethical to separate them.26 The twins, in some union types, such as the end-to-end ischiopagus, will never stand up and will be bedridden. Independent walking is not possible with other unions. We find such restrictions on living unbearable, yet parents have the final decision.27
Religious beliefs also play an essential role in such ethical issues and dilemmas. An earlier ethical analysis focused on Jodie and Mary, children of devoted Catholics. Without separation, the surgeons estimated that Mary would pass away within 3–6 months and that her sister would exsanguinate into the body of her deceased sister within hours. Jodie would be able to have a somewhat normal life after the surgery, but Mary would pass away shortly after the aortic connection was severed, making surgical separation possible during the neonatal period. Their parents rejected the procedure because they thought Mary’s death was wrong and God should decide what would happen to their children.28
Despite the likelihood of one twin dying, there are several reasons why the surgery should go through. Clinicians are encouraged by law to perform in conformity with recognized medical standards. The decision to forgo the procedure prompts several concerns. Is an act of omission preferable to a commission that causes collateral damage? Is the physician right to decline the parents’ request, given their attempts at separation? Is violating the “sanctity of life” a good enough reason to refrain from doing something that will kill one of the twins? More importantly, is trying to save one child and letting the other die a better moral position than allowing the death of two children? Different conclusions usually arise depending on which twin’s viewpoint was used while examining the cases through the eyes of autonomy, beneficence, nonmaleficence, and justice.
Conclusion
Complex surgery such as conjoined twin separation can be managed effectively by a team of multidisciplinary experts. The application of information technology, to manage changes in multidisciplinary work pre- and post-pandemic, can reduce pandemic-related social restrictions while maintaining effectiveness and increasing efficiency.
Images
Patient and staff in the figures had been informed and provided informed consent for the images to be published.
Ethical Clearance
Dr Hasan Sadikin National Referral Hospital Institutional Ethical Review Board Number LB.02 0.01/X.6.5/296/2021.
Acknowledgments
This paper was highly influenced by the RSHS Bandung Conjoined Twin task force, especially the works of the late Prof Dadang as his work inspired us all. Thank you to the pediatric anesthesia team of Prof Kaswiyan, dr Ezra, dr Ruli, dr Doddy, dr Indriasari, dr Akhmad Rhesa, dr Radian and anesthesia nurses Mr Ugun, Ms Rita, Mr Yana,Ms Iis plus other anesthesia team members. Dr Bustanul, dr Rizky, dr Emil, dr Vita, dr Okky and Pediatric surgery team. Pediatric team of Prof Abdurachman, Prof Sjarief Hidayat, dr Tetty, dr Dzulfikar, dr Stanza Uga, dr Fina, dr Rahmat Budi, dr Tisna, dr Susi Susana and the pediatric team. dr Harry Galuh and team from the department of radiology. Dr Eliana and dr Marietta with their highly dedicated medical rehabilitation team. The late dr Rachim, dr Tri Wahyu, Dr Rama and dr Navy and the cardiothoracic surgical team. Dr Hardi, dr Lisa, dr Ira, dr Rani and the plastic surgery team. Prof Yoyos and dr Fatur from the pediatric orthopedic team. Dr Syafendra, dr Jupiter and pediatric urology team. Ns Yani Setiasih and the NICU team, Ns Whina and the PICU. Pharmacist Mr Ilman,Ms Ozzy and Miss Siti. Dr Indriasari, Mr Abdul, Ms Lilis and RSHS COT team. Our dedicated social workers, nutritionist, psychologist, finance department, public relation and all other member of our conjoined twin extended team that we cannot mention in this paper. We honor all doctors, nurses, residents, medical students, other medical and non medical staff in RSHS for their continuous dedication and commitment during the COVID-19 pandemic and their dedication in conjoined twins management. We also salute the dedication of our district hospitals, provincial and sub-state government, KitaBisa non governmental organization and the Indonesian people for their contribution and support for the conjoined twin program in RSHS. May God bless you all.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in public, commercial or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kennedy GE. The 3000-year history of conjoined twins. West J Emerg Med. 2001;175:176–177.
2. Spitz L, Kiely E, Pierro A. Conjoined twins. In: Rickham’s Neonatal Surgery. London: Springer; 2018:457–474.
3. Mian A, Gabra NI, Sharma T, et al. Conjoined twins: from conception to separation, a review. Clin Anat. 2017;30(3):385–396. doi:10.1002/ca.22839
4. Mathew RP, Francis S, Basti RS, et al. Conjoined twins - role of imaging and recent advances. J Ultrason. 2017;17(71):259–266. doi:10.15557/JoU.2017.0038
5. Tannuri ACA, Batatinha JAP, Velhote MCP, Tannuri U. Conjoined twins: twenty years’ experience at a reference center in Brazil. Clinics. 2013;68(3):371–377. doi:10.6061/clinics/2013(03)OA14
6. Spitz L, Kiely EM. Experience in the management of conjoined twins. Br J Surg. 2002;89(9):1188–1192. doi:10.1046/j.1365-2168.2002.02193.x
7. Shafarenko MS, Zuker RM. Conjoined Twin Separation: review of 30-year case experience and lessons learned. Plast Reconstr Surg. 2022;150(1):133–144. doi:10.1097/PRS.0000000000009267
8. Greco PS, Pitts DA, Weadock WJ, et al. Conjoined twins: an obstetrician’s guide to prenatal care and delivery management. J Perinatol. 2021;41(10):2424–2431. doi:10.1038/s41372-021-01107-5
9. Laima C, Meller T, Nwukwa G. Conjoined twin presenting as a case of “hanging breech” in labor – case report. Trop J Obstet Gynaecol. 2019;36(2):299–300.
10. Leigh MB, John-Cole V, Kamara M, et al. A Triple Obstetric Challenge of Thoracopagus-Type Conjoined Twins, Eclampsia, and Obstructed Labor: a Case Report from Sub-Saharan Africa. Case reports in obstetrics and gynecology; 2017:6815748.
11. Veena P, Chaturvedula L. Two rare complications of twin gestation manifesting as arrest of descent in the second stage of labor. Int J Adv Med Heal Res. 2016;3(2):94–96. doi:10.4103/2349-4220.195941
12. Durkin N, Davenport M. Centralization of pediatric surgical procedures in the United Kingdom. Eur J Pediatr Surg off J Austrian Assoc Pediatr Surg. 2017;27(5):416–421.
13. Pakarinen M, Bjørland K, Qvist N, Wester T. Centralized pediatric surgery in the nordic countries: a role model for Europe? Eur J Pediatr Surg off J Austrian Assoc Pediatr Surg. 2017;27(5):395–398.
14. Kohaut J, Guérin F, Fouquet V, et al. First liver transplantation for biliary atresia in children: the hidden effects of non-centralization. Pediatr Transplant. 2018;22(6):e13232. doi:10.1111/petr.13232
15. Cummings BM, Paris JJ. Conjoined Twins separation leading to the death of one Twin: an expanded Ethical analysis of issues facing the ICU team. J Intensive Care Med. 2018;34(1):81–84. doi:10.1177/0885066618791953
16. Thomas A, Johnson K, Placencia FX. An ethically-justifiable, practical approach to decision-making surrounding conjoined-twin separation. Semin Perinatol. 2018;42(6):381–385. doi:10.1053/j.semperi.2018.07.016
17. Collins RT, O’Connor MJ. The outcomes of surgical separation in thoracopagus twins with conjoined hearts: an analysis of the literature. Pediatr Cardiol. 2021;42(4):875–882. doi:10.1007/s00246-021-02555-8
18. Villarreal JA, Yoeli D, Masand PM, Galvan NTN, Olutoye OO, Goss JA. Hepatic separation of conjoined twins: operative technique and review of three-dimensional model utilization. J Pediatr Surg. 2020;55(12):2828–2835. doi:10.1016/j.jpedsurg.2020.06.047
19. Canada NL, Mullins L, Pearo B, Spoede E. Optimizing perioperative nutrition in pediatric populations. Nutr Clin Pract off Publ Am Soc Parenter Enter Nutr. 2016;31(1):49–58.
20. Cheggour S, Turpeau S. Télémédecine et coordination des soins : les deux piliers de l'optimisation du parcours de soins en cardiologie [Telemedicine and care coordination: the two cornerstones of optimising the cardiology care pathway]. Ann Cardiol Angeiol. 2021;70(5):348–350. French. doi:10.1016/j.ancard.2021.09.012
21. Kubheka BZ. Bioethics and the use of social media for medical crowdfunding. BMC Med Ethics. 2020;21(1):96. doi:10.1186/s12910-020-00521-2
22. Schier F, Korn S, Michel E. Experiences of a parent support group with the long-term consequences of esophageal atresia. J Pediatr Surg. 2001;36(4):605–610. doi:10.1053/jpsu.2001.22299
23. Omer AAA. Directives of general surgical practice during the COVID-19 pandemic: a systematic review. J Educ Health Promot. 2021;10:395. doi:10.4103/jehp.jehp_233_21
24. Dinis J, Prsic A, Junn A, Hsia H, Alperovich M. Implementing live virtual surgery in the COVID era: overcoming medicolegal, technical, and educational hurdles. Plast Reconstr Surg. 2021;148(6):1092e–1094e. doi:10.1097/PRS.0000000000008565
25. Rempel GR. Technological advances in pediatrics: challenges for parents and nurses. J Pediatr Nurs. 2004;19(1):13–24. doi:10.1016/j.pedn.2003.09.003
26. Kallberg L. The ethics of separating conjoined twins: two arguments against. Theor Med Bioeth. 2018;39(1):27–56. doi:10.1007/s11017-018-9435-2
27. Spitz L. Ethics in the management of conjoined twins. Semin Pediatr Surg. 2015;24(5):263–264. doi:10.1053/j.sempedsurg.2015.06.008
28. Wheeler R. Conjoined twins: surgically and legally exceptional. Arch Dis Child. 2021;106(12):1158LP–1159 . doi:10.1136/archdischild-2020-321079
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perioperative Management for Emergency Surgery in Pediatric Patients with COVID-19: Retrospective Observational Study
Giwangkancana G, Oktaliansah E, Ramlan AAW, Utariani A, Kurniyanta P, Arifin H, Widyastuti Y, Pratiwi A, Syukur R
Open Access Emergency Medicine 2022, 14:515-524
Published Date: 20 September 2022
Impact of the COVID-19 Pandemic on Breastfeeding Support Services and Women’s Experiences of Breastfeeding: A Review
Lubbe W, Niela-Vilén H, Thomson G, Botha E
International Journal of Women's Health 2022, 14:1447-1457
Published Date: 6 October 2022
Impact of Enhanced in-Hospital Infection Prevention During the COVID-19 Pandemic on Postoperative Pneumonia in Older Surgical Patients
Ju JW, You J, Hong H, Kang CK, Kim WH, Lee HJ
International Journal of General Medicine 2023, 16:1943-1951
Published Date: 23 May 2023
Re-Emerging COVID-19: Controversy of Its Zoonotic Origin, Risks of Severity of Reinfection and Management
Chala B, Tilaye T, Waktole G
International Journal of General Medicine 2023, 16:4307-4319
Published Date: 20 September 2023
Effectiveness of Drug Repurposing and Natural Products Against SARS-CoV-2: A Comprehensive Review
Velásquez PA, Hernandez JC, Galeano E, Hincapié-García J, Rugeles MT, Zapata-Builes W
Clinical Pharmacology: Advances and Applications 2024, 16:1-25
Published Date: 4 January 2024