Back to Journals » Advances in Medical Education and Practice » Volume 14
The Morning Report Practice and Its Contribution to Education of Internal Medicine Residents: A Multicenter Cross-Sectional Survey in the Eastern Province, Saudi Arabia
Authors Al Qarni A ![]() , Habib A, Abdelgadir E, Al Sarawi A, Alqannas N, Alkroud A
, Habib A, Abdelgadir E, Al Sarawi A, Alqannas N, Alkroud A
Received 30 March 2023
Accepted for publication 3 July 2023
Published 10 July 2023 Volume 2023:14 Pages 713—722
DOI https://doi.org/10.2147/AMEP.S414986
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Ali Al Qarni,1– 3 Ahmad Habib,4 Elbadri Abdelgadir,1 Abdulaziz Al Sarawi,1,3 Naif Alqannas,5 Ammar Alkroud6
1Department of Medicine, King Abdulaziz Hospital, Ministry of National Guard Health Affairs, Al Ahsa, Saudi Arabia; 2King Abdullah International Medical Research Center, Al Ahsa, Saudi Arabia; 3King Saud bin Abdulaziz University for Health Sciences, Al Ahsa, Saudi Arabia; 4Department of Medicine, King Fahd Military Medical Complex (KFMMC), Dhahran, Saudi Arabia; 5Saud Al Babtain Cardiac Centre, Eastern Health Cluster, Dammam, Saudi Arabia; 6Department of Medicine, Johns Hopkins Aramco Healthcare (JHAH), Al Ahsa, Saudi Arabia
Correspondence: Ali Al Qarni, Consultant Endocrinologist, King Abdulaziz Hospital, Ministry of National Guard Health Affairs, Po Box 2477, Al Ahsa, 31982, Saudi Arabia, Tel +966500133678, Email [email protected]; [email protected]
Background: Morning Report (MR) is a ubiquitous traditional educational activity in internal medicine residency training. It is under-researched; hence, this study was conducted. It aimed to examine the practice of MR by internal medicine residents, their motivation to engage with it, and their perception of its contribution to education.
Methods: This was a multi-center cross-sectional study. The data was collected using an online self-administered 12-item questionnaire that covered MR practice, respondents’ motivation for participation, MR contribution to education, and its impact on the practice of evidence-based medicine and quality improvement and patient safety.
Results: One hundred seventy residents returned the online questionnaire (54.7%). The respondents’ gender and year of training were balanced (P > 0.05). The most common MR frequency and duration were five days per week (85.4%) and 45– 60 minutes (47.1%), respectively. The most common format was handover combined with an emergency long case presentation (55.8%), and consultants were the most common facilitators (79.7%). The respondents’ motivation to engage with MR was predominantly intermediate. The top reasons for attending and not attending MR were mandatory attendance and embarrassing questions, respectively. The perceived MR contribution to residents’ different roles development was predominantly intermediate; however, it was predominantly very low/low (42%) for overall education. The perceived MR impact on the practice of EBM and QIPS were both predominantly intermediate.
Conclusion: MR was found to be a commonly practiced educational activity in internal medicine residency training programs in the eastern province of Saudi Arabia. The case discussion was the core format for education. The respondents’ motivation to participate in MR and their perception of its contribution to education was predominantly intermediate. To our best knowledge, this is the first study in Saudi Arabia that examined MR. We hope its findings will be taken for further MR studies and actions for improvement.
Keywords: morning report, MR, internal medicine residency, contribution to education, residents’ role development
Introduction
Morning report (MR) is a traditional activity in the practice of medicine and one of the most important classic teaching activities of trainee residents.1 It is composed of regular meetings (usually daily) between the trainees and senior physicians.2 It is a widely used educational tool in residency training programs worldwide with education being the primary aim.3–6 While the MR format varies between institutes, its core teaching method is a case-based discussion in which a case is presented by a trainee and the discussion is led by senior staff.7,8
MR was shown to influence patients’ outcomes like the length of stay and cost of care, although its essential purpose continued to be education.9–11 In addition, it can also be used as an authentic situation in which feedback on certain physicians’ roles can be covered when residents’ performance is directly observed eg, collaborator and communicator.12 It was found at King Abdulaziz Medical City-Riyadh, Saudi Arabia that MR in internal medicine residency training program can be used as a venue to enhance the integration of residents’ roles in daily practice.13
MR was also found to be a valuable educational experience by internal medicine trainee residents and was rated as the second most common venue for teaching clinical reasoning in internal medicine clerkship in the USA.14,15
A paradigm shift of medical education to be competency-based rather than time spent-based occurred toward the end of the 20th century.16 Hence, several competency-based medical education frameworks were developed eg the Canadian Medical Education Directives for Specialists (CanMEDS) and the Saudi Medical Education Directives (SaudiMED) which have remarkable similarities with CanMEDS when they were compared.17,18 In addition, other aspects of MR have evolved like the active involvement of residents in teaching rather than being only passive learners.19 Obviously, MR as an educational activity must meet these changes. A key contributor to the successful implementation of MR is constant re-evaluation combined with the flexibility to adapt to changing needs.20 According to a systematic review published in 2013, making a firm conclusion about the contribution of MR to resident education was not possible due to the difficulty to measure its outcomes.21 There are also several recognized challenges for optimizing its educational benefits including increasing volume and acuity of patients, restriction of duty hours, and pressure to discharge patients.7
Internal medicine residency training in Saudi Arabia is one of the major postgraduate training programs under the Saudi Commission for Health Specialties (SCFHS) which is the responsible body for supervising, regulating, and evaluating postgraduate medical education in Saudi Arabia.22 The program is a 4-year structured training that awards Saudi Board in Internal Medicine as a specialty certificate. The first 2 years are designated as the junior level and the second 2 years as the senior level. The years in the program are designated as first-year (R1), second-year (R2), third-year (R3), and fourth-year (R4).23
MR as an educational activity is included in the internal medicine residency training curriculum by SCFHS with specific educational objectives linked to trainees’ role development as a manager, medical expert, professional, and scholar, it is expected accordingly to be conducted in the morning from Sunday to Thursday (weekdays) each week, lasting 45–60 minutes, and to include short cases, long cases, data interpretation, and a topic presentation.23
In light of the ubiquity of morning reports, the increased incorporation of learning theories in medical education,24,25 the emergence of the best evidence-based medical education26 and the shift to competency-based medical education,16 with the paucity of published studies from Saudi Arabia about MR role as an educational tool in internal medicine residency training, this cross-sectional study using an online survey was conducted in the eastern province of Saudi Arabia with the aim to identify the practice and perceived educational contribution of MR by internal medicine residents. The aim of this study was to examine the practice of MR by internal medicine residents, their motivation, and their perception of its contribution to education with the following specific objectives: (1) Determine MR practice (frequency, duration, and format), (2) Assess residents’ motivation (3) Identify the perceived MR contribution to education and role development and (4) Identify the MR impact on the practice of evidence-based medicine (EBM) and quality improvement and patient safety (QIPS). These study findings are relevant to postgraduate medical education in Saudi Arabia, particularly internal medicine residency training. To the best of our knowledge, no previous similar study was published in Saudi Arabia.
Method
This was a cross-sectional study using an online survey. The study proposal was approved by the Institutional Research Board (IRB) at King Abdullah International Medical Research Center (Reference Number IRBC/0321/20). The study was conducted in the eastern province of Saudi Arabia. At the time of the study, there were a total of 314 registered residents belonging to 14 different internal medicine residency training programs accredited by SCFHS for the academic year 2019/2020. All residents of all levels were eligible to participate in this survey without exclusion. Participation was anonymous and voluntary. There was no benefit provided for participation.
Data Collection
Data were collected using a self-administered online questionnaire (Supplement 1) which was created on the SurveyMonkey platform and distributed by email on 1st September 2020 and kept open for participation till 30 September 2020 during which follow-up reminders were followed. The questionnaire was new and developed by the authors of this study taking into consideration the MR format and objectives as per the internal medicine training program curriculum by SCFHS.23 Input from 2 program directors, 5 trainers, and 5 residents were obtained. Accordingly, the questionnaire was modified to its final version.
The questionnaire was then piloted on fifteen residents to assess internal consistency; hence, Cronbach coefficient alpha was 0.95. Those participants in the pilot study were included in the final analysis.
The questionnaire (Supplement 1) has twelve items which cover demographics (age, gender, and training year), MR setup (frequency and duration), MR format and facilitation, experience with attendance and motivation for participation, perception of MR contribution to education, the practice of evidence-based medicine and QIPS.
The questionnaire was composed of five level Likert type items and multiple-choice questions with the possibility of more than one choice including others for free text to reflect residents’ own experience if not included in the options. No personal identifying information was included. It was possible to skip answering any item and submit the rest except the question about the training year which was mandatory.
The questionnaire was initially written on a word document, then the final version was transferred to the monkey survey platform. It started with an invitation message for anonymous volunteer participation which included IRB approval reference, the study purpose, and the name and contact information of the primary investigator. Volunteer completion of the questionnaire and submitting it by participants was accepted as informed consent to participate. This was stated in the letter to the participants at the beginning of the questionnaire.
Data Analysis
Descriptive statistics were expressed as the mean and standard deviation for age as the only numerical variable in our data which was normally distributed; the rest of the variables were categorical and expressed as frequency and percentage. Chi-square was used to compare the difference in responses by gender and year of training with a p-value <0.05 as the significance level. Statistical Package for the Social Sciences (SPSS) version (28) was used for calculation. Free-text answers under “others” in some questions were presented without change as reported by respondents. These questions were related to the morning report setup.
Results
The online questionnaire was completed by 172 residents out of the 314 residents who were sent the survey link making a response rate of 54.7%. The demographic characteristics are presented in (Table 1) which shows the mean age of 28-year-old. There was a balanced distribution of respondents by gender and training year (R1 to R4). Most of the respondents (85.5%) indicated that MR took place 5 times per week during the weekdays only, while daily including weekends was indicated by an extremely small proportion (0.6%) and only one respondent (0.6%) indicated a lack of MR. The duration of MR (Table 1) varied between 15 to 30 minutes to >60 minutes; however, a duration of 45–60 minutes was reported by about half of the respondents (47.1%) and a duration of 30–45 minutes by about third of the respondents (31.4%).
 |
Table 1 Demographics Morning Report Setup and Format |
Handover combined with a long emergency case presentation and discussion was the most frequent MR format (55.8%), followed by emergency long case presentation only and discussion and discussion (33.7%), then inpatient long case presentation and discussion only (16.3%). Long and short case presentations and discussions were reported by 1.7% only (Table 1). Journal club in MR on some days and exam preparation were reported by 52.9% and 13%, respectively.
Consultants were found to be the most frequent MR facilitators (moderators) and reported by 79.7%, while senior and junior residents were reported by 8.7% and 7.6%, respectively (Table 1).
We found that the top reason for attending MR regularly was mandatory attendance (54.7%) followed by case discussion (45.9%), then educational benefit (41.9%), whereas the facilitator (moderator) was reported as a reason for attendance by about a third (27.3%) of the respondents (Table 2A). On the other hand, embarrassing questions (55.8%) were the top reason for not attending MR regularly followed by the facilitator (moderator) (43.6%) then being busy with patient care (25.6%), whereas lack of educational benefits was reported by 23.3% of the respondents (Table 2B).
 |
Table 2 Reasons for Attending/Not Attending Morning Report Regularly |
The respondents’ perceived motivation for regular MR attendance was predominantly intermediate (42%) and for active participation was predominately very-low/low (36%) and intermediate (36%); on the other hand, it was predominately very-low/low (67%) for taking a facilitator (moderator) role (Figure 1).
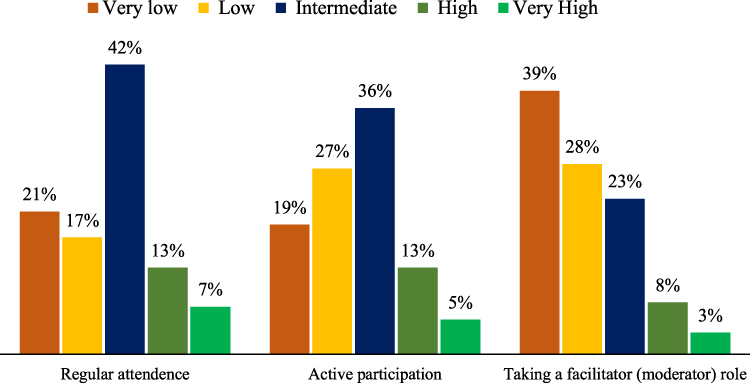 |
Figure 1 Residents’ motivation for involvement in the morning report. |
The contribution of MR to respondents’ education and role development is shown in (Figure 2); the respondents’ perceived a predominant intermediate contribution of MR to their role development as a medical expert (39%), leader (40%), communicator (40%), and professional (38%). On the other hand, MR contribution to scholar development was predominantly perceived as very low/low (63%), and to overall education was predominantly perceived as very low/low (42%). Also, MR contribution to respondents’ performance in the exam was predominantly perceived as very low/low (57%).
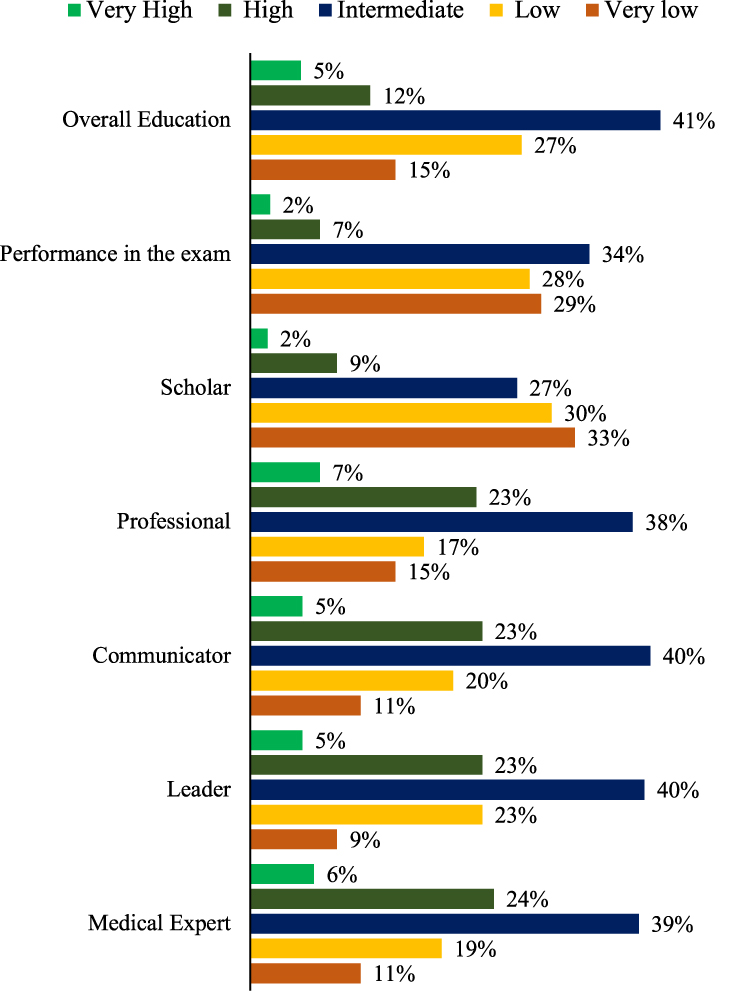 |
Figure 2 Perceived contribution of the morning report to residents’ role development, overall education, and performance in the exam. |
The impact of MR on the practice of EBM was reported as high/very high by a minority of respondents (23%); on the other hand, the MR impact on the practice of QIPS was predominantly intermediate (47%) (Figure 3).
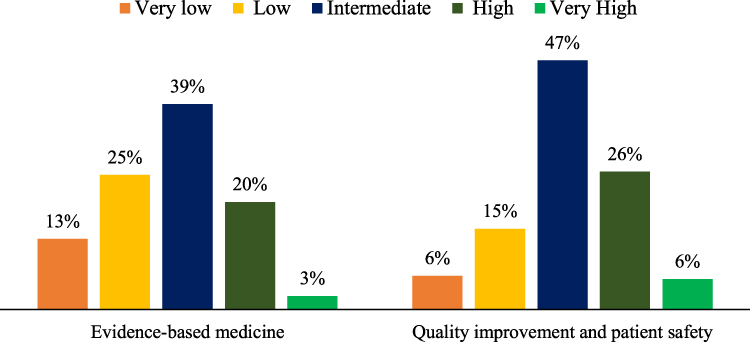 |
Figure 3 Perceived impact of the morning report on practice of evidence based medicine and quality improvement and patient safety. |
Discussion
This cross-sectional multicenter observational study explored the MR practice in the internal medicine residency training programs in the Eastern Province of Saudi Arabia. In addition, it addressed the resident’s perception of the MR contribution to their education, factors influencing their attendance and participation, and their motivation to participate.
The response rate in this study was 54.7% which is higher than the average reported response rate for published online survey studies of 44.1% as found in a recently published meta-analysis.27 It was also within the range of the response rate found by other graduate medical education studies using an online survey.28,29
MR was found to be a commonly practiced educational activity in internal medicine residency training programs in the eastern province of Saudi Arabia with variable frequencies; this finding is consistent with the practice elsewhere in the world.3–6,30
The frequency of MR (Table 1) was commonly 5 days per week on the weekdays (85.5%) which is consistent with the requirement of the training curriculum; however, only about half of the respondents (47.1%) implemented the expected MR duration of 45–60 minutes as per the curriculum.23 This MR frequency and duration are higher than the finding by a recent national survey of internal medicine residency program directors in the USA which was 31.7% and 33.6%, receptively.30
We found diversity in the MR format; however, the case-based discussion was predominant. The wide variation in MR among similar programs is well recognized, for example a recent prospective observational study in ten different Veterans Affairs (VA) academic medical centers in the USA found this variation and also found that case-based discussion was the predominant format, similar to our finding.19 The internal medicine residency training curriculum addresses this variation and emphasizes the case presentation for the purposes of residents’ education.23 Handover was also found to be practiced commonly, even though it was not specifically mentioned in the curriculum; instead, it was stated that “The team that has been on call the previous night briefly present and discuss all admitted patients with the audience” which can be interpreted as a handover.23 Handover in the morning report is well-established practice although its limitation to maintaining patients’ safety was questioned and the need for improvement has been recognized.31–33 Short case presentation, data interpretation, and a topic presentation were much less reported by the respondents (Table 1), although specifically included in the curriculum, on the other hand, we found utilization of MR for other activities not included specifically as a component of MR format including journal club presentation and exam preparation.23 Noteworthy, presenting journal club in the MR has been recognized in the literature.21
MR in this survey was reported to be facilitated (moderated) most commonly by consultants, while residents’ participation as facilitators was much less. This is in contrast with the finding of the survey from the USA mentioned above, in which the internal medicine MR was led by chief residents (61.9%), senior residents (29%), junior residents (14.3), and faculty (28%).30
The top reason reported by respondents for attending the MR regularly was mandatory attendance, on the contrary, a recently published survey about internal medicine residents’ perception of the MR found that the top reason for participation was clinical education (85%),34 while in our study educational benefit was reported by 41.9% (Table 2). The case discussion and MR facilitator (moderator) contributed also to the respondents’ motivation for MR attendance though to a lesser degree. The case and the running of the show which is the task of the facilitator were highlighted by a survey of internal medicine faculties at the University of Toronto, Canada, as important elements for successful MR facilitation.7 On the other hand, the top reported reason for not attending MR regularly in this study was “embarrassing questions”; consistent with this reason, it was shown previously that the MR environment can be a fearful place.35 In literature, “being busy with patient care” is cited to be the primary barrier to attending MR,34,36 however it was reported by a relatively small proportion of the respondents in this study (25.6%) (Table 2), which may reflect the education-protected time implemented by the programs. The facilitator (moderator) was also reported as the second reason for not attending MR regularly. This finding reflects the key role of the MR facilitator including skills in facilitating discussion, creating a learning environment, and respecting time which were suggested as important attributes for the facilitator to conduct successful facilitation.7
A lack of educational benefits was also reported as a reason for not attending by 23.3% (Table 2) which is slightly higher than the finding by the recently published medical residents’ perception study mentioned above in which only 16% reported MR as not good for the time.34
The respondents’ motivation for regular MR attendance and active participation (presenting, commenting, or asking questions) was predominantly intermediate; however, it was predominantly very low for taking a facilitator (moderator) role, and only 11% reported high/very high motivation for that (Figure 1). Motivation is an internal derive that sustains all human action.37 It can be defined as “a phenomenon originating in the perceptions that the student has of himself and his environment, which lead to his choosing to carry out the educational activity proposed, persevere and engage with it, with the aim of learning from it”.38 To our knowledge, no previous study has specifically assessed the internal medicine residents’ motivation to participate in MR as an educational activity and this limitation could be due to the assumption that residents as adult learners are highly motivated since “motivation” is one of the fundamental assumptions of adult learning theory.39
The perceived MR contribution to respondents’ role development was predominantly intermediate for medical experts, leaders, communicators, and professionals, on the other hand, it was predominantly very low/low for role development as a scholar.
The respondents’ perception of the MR contribution to their performance in the exam and overall education was also predominantly intermediate. We also found a predominant intermediate perception of MR impact on participants’ practice of EBM and QIPS. In contrast, previous studies showed that teaching EBM in the MR was highly regarded.34,40 Also, our previous single-center qualitative study found a gap in QIPS education in internal medicine residency training programs.41
Measuring the contribution of the MR to residents’ education is challenging,21 hence there are very limited published studies. However, the most recent survey from the USA about residents’ perception of the MR found it highly regarded educational activity.34 Also, a recent cross-sectional study from Pakistan found that the MR was rated as an effective teaching activity by 92% of the participants.42
The current study findings alert us about the importance of the MR quality of education, use of the protected time, and resident engagement with it; hence, further assessment of MR and intervention for improvement are justified. These findings could be due to a lack of a well-structured MR format linked to its objectives, skills to facilitate MR, and regular monitoring and feedback. In fact, there have been reports of interventions to improve the MR quality of education with positive outcomes, such interventions include changing MR format,6 implementing a toolkit,43 training residents to act as teachers,44 and providing consistent feedback.45
Limitations
This study has important limitations including, the limited generalizability since it was limited to one province of Saudi Arabia, although the response rate was acceptable (54%), the non-respondents may have different responses than the respondents. In addition, the perception of education may not reflect the actual gaining of knowledge because of educational activity.
Strengths
MR is a very ubiquitous educational activity in internal medicine residency training programs, hence assessing its practice, and contribution to trainees’ education, is crucial for improvement to make sure that the protected time spent regularly by the trainees and the educators is rewarded by educational benefits. To the best of our knowledge, this is the first multicenter cross-sectional study in Saudi Arabia that addresses the practice of MR and its educational aspects. In addition, it adds to the literature since there is a dearth of published similar studies from the internal medicine residents “perspectives”.
Conclusion
This cross-sectional multicenter study demonstrated that the traditional MR continued to be a commonly practiced educational activity in internal medicine residency training programs in the eastern province of Saudi Arabia. The case-based discussion was found to be the most frequent format consistent with the classic practice. The reported respondents’ motivation for engagement in MR was predominantly intermediate. In addition, we found a predominant intermediate perceived contribution of the MR to respondents’ education and role development and a similar perceived predominant intermediate impact of the MR on EBM and QIPS practice. These findings call for further research to examine the role of MRs in internal medicine residency training. Since this is the first study (up to our best knowledge) in Saudi Arabia, we hope the leaders in the field will find it helpful for further studies and improvement initiatives.
Acknowledgment
We wanted to thank all the internal medicine trainee residents in the Eastern Province of Saudi Arabia for participating in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Parrino TA, Villanueva AG. The principles and practice of morning report. JAMA. 1986;256(6):730–733. doi:10.1001/jama.1986.03380060056025
2. Dunbar-Yaffe R, Gold WL, Wu PE. Junior rounds: an educational initiative to improve role transitions for junior residents. BMC Res Notes. 2017;10(1):694. doi:10.1186/s13104-017-3027-5
3. Amin Z, Guajardo J, Wisniewski W, Bordage G, Tekian A, Niederman LG. Morning report: focus and methods over the past three decades. Acad Med. 2000;75(10 Suppl):S1–S5.
4. Das JP, Draman MS, Cormican L, O’Neill J. Morning report: a recommendation to improve medical handover. Ir Med J. 2012;105(2):59.
5. Quadri K, Jaffery T, Alam A, Rahim M. Preliminary experience with a new medicine morning report format incorporating multimedia and up-to-date. J Pak Med Assoc. 2007;57:320–321.
6. Daniels VJ, Goldstein CE. Changing morning report: an educational intervention to address curricular needs. J Biomed Educ. 2014;2014:830701. doi:10.1155/2014/830701
7. Devine L, Gold W, Page A, et al. Tips for facilitating morning report. Can J Gen Intern Med. 2017;12(1). doi:10.22374/cjgim.v12i1.206
8. Liederman Z, Patafio F, Green J, et al. The morning report iBook - a novel approach to the internal medicine morning report. Can J Gen Intern Med. 2016;11(12). doi:10.22374/cjgim.v11i2.144
9. Bowman J, Duran A, Duffy B, Gladding S, Baum K. Teaching high-value care: a novel morning report. Clin Teach. 2015;12(3):165–170. doi:10.1111/tct.12270
10. Banks DE, Shi R, Timm DF, et al. Decreased hospital length of stay associated with presentation of cases at morning report with librarian support. J Med Libr Assoc. 2007;95(4):381–387. doi:10.3163/1536-5050.95.4.381
11. Boushehri E, Khamseh ME, Farshchi A, Aghili R, Malek M, Ebrahim Valojerdi A. Effects of morning report case presentation on length of stay and hospitalisation costs. Med Educ. 2013;47(7):711–716. doi:10.1111/medu.12152
12. Renting N, Gans ROB, Borleffs JCC, Van Der Wal MA, Jaarsma ADC, Cohen-Schotanus J. A feedback system in residency to evaluate CanMEDS roles and provide high-quality feedback: exploring its application. Med Teach. 2016;38(7):738–745. doi:10.3109/0142159X.2015.1075649
13. Hassan IS, Kuriry H, Ansari LA, et al. Competency-structured case discussion in the morning meeting: enhancing CanMEDS integration in daily practice. Adv Med Educ Pract. 2015;6:353–358. doi:10.2147/AMEP.S79521
14. Ways M, Kroenke K, Umali J, Buchwald D. Morning report. A survey of resident attitudes. Arch Intern Med. 1995;155(13):1433–1437. doi:10.1001/archinte.1995.00430130127013
15. Rencic J, Trowbridge RL Jr, Fagan M, Szauter K, Durning S. Clinical reasoning education at US medical schools: results from a national survey of internal medicine clerkship directors. J Gen Intern Med. 2017;32(11):1242–1246. doi:10.1007/s11606-017-4159-y
16. Park YS, Hodges B, Tekian A. Evaluating the paradigm shift from time-based toward competency-based medical education. In: Implications for Curriculum and Assessment. Springer; 2016:411–425.
17. Shadid AM, Bin Abdulrahman AK, Bin Dahmash A, et al. SaudiMEDs and CanMEDs frameworks: similarities and differences. Adv Med Educ Pract. 2019;10:273–278. doi:10.2147/AMEP.S191705
18. Tekian AS, Al Ahwal MS. Aligning the SaudiMED framework with the national commission for academic accreditation and assessment domains. Saudi Med J. 2015;36(12):1496–1497. doi:10.15537/smj.2015.12.12916
19. Heppe DB, Beard AS, Cornia PB, et al. A multicenter VA study of the format and content of internal medicine morning report. J Gen Intern Med. 2020;35(12):3591–3596. doi:10.1007/s11606-020-06069-6
20. West CP, Kolars JC, Eggert CH, Kennedy CC, Ficalora RD. Changing morning report: evaluation of a transition to an interactive mixed-learner format in an internal medicine residency program. Teach Learn Med. 2006;18(4):330–335. doi:10.1207/s15328015tlm1804_10
21. McNeill M, Ali SK, Banks DE, Mansi IA. Morning report: can an established medical education tradition be validated? J Grad Med Educ. 2013;5(3):374–384. doi:10.4300/JGME-D-12-00199.1
22. Saudi Commission for Health Specialties. Saudi commission for health specialties; 2022. Available from: https://scfhs.org.sa/en/about-us.
23. Saudi Commission for Health Specialties. Saudi board internal medicine curriculum 2015; 2015. Available from: https://scfhs.org.sa/sites/default/files/2022-01/INTERNAL%20MEDICINE.pdf.
24. Arab M, Ghavami B, Akbari Lakeh M, Yaghmaie M, Hosseini-Zijoud S-M. Learning theory: narrative review. Int J Med Rev. 2015;2(3):291–295.
25. Abela J. Adult learning theories and medical education: a review. Malta Med J. 2009;21:1.
26. Harden RM, Grant J, Buckley G, Hart IR. BEME guide no. 1: best evidence medical education. Med Teach. 1999;21(6):553–562. doi:10.1080/01421599978960
27. M-j W, Zhao K, Fils-Aime F. Response rates of online surveys in published research: a meta-analysis. Comput Hum Behav Rep. 2022;7:100206. doi:10.1016/j.chbr.2022.100206
28. Marshall AL, Jenkins S, Oxentenko AS, et al. Internal medicine trainees’ knowledge and confidence in using the American society of hematology choosing wisely guidelines in hemostasis, thrombosis, and non-malignant hematology. PLoS One. 2018;13(5):e0197414.
29. Yarger JB, James TA, Ashikaga T, et al. Characteristics in response rates for surveys administered to surgery residents. Surgery. 2013;154(1):38–45. doi:10.1016/j.surg.2013.04.060
30. Lessing JN, McGarry K, Schiffman F, et al. The state of morning report in the current healthcare landscape: a National Survey of Internal Medicine Program Directors. J Gen Intern Med. 2022;37(7):1665–1672. doi:10.1007/s11606-021-07010-1
31. Devlin MK, Kozij NK, Kiss A, Richardson L, Wong BM. Morning handover of on-call issues: opportunities for improvement. JAMA Intern Med. 2014;174(9):1479–1485. doi:10.1001/jamainternmed.2014.3033
32. Donnelly S, Dinesh D, Dew K, Stubbe M. The handover room: a qualitative enquiry into the experience of morning clinical handover for acute medical teams. Intern Med J. 2019;49(5):607–614. doi:10.1111/imj.14142
33. Rourke L, Amin A, Boyington C, Ao P, Frolova N. Improving residents’ handovers through just-in-time training for structured communication. BMJ Qual Improv Rep. 2016;5(1). doi:10.1136/bmjquality.u209900.w4090
34. Albert TJ, Redinger J, Starks H, et al. Internal medicine residents’ perceptions of morning report: a multicenter survey. J Gen Intern Med. 2021;36(3):647–653. doi:10.1007/s11606-020-06351-7
35. Khajeali N, Ahmady S, Karimi P, Hamedanchi A. A study on the challenges of morning report in clinical education: a phenomenological study. Biosci Biotechnol Res Asia. 2016;13(4):2201–2206. doi:10.13005/bbra/2384
36. Albert TJ, Bradley J, Starks H, et al. Internal medicine residents’ perceptions of virtual morning report: a multicenter survey. J Gen Intern Med. 2022;37(6):1422–1428. doi:10.1007/s11606-021-06963-7
37. Simpson EH, Balsam PD. The behavioral neuroscience of motivation: an overview of concepts, measures, and translational applications. Curr Top Behav Neurosci. 2016;27:1–12. doi:10.1007/7854_2015_402
38. Pelaccia T, Viau R. Motivation in medical education. Med Teach. 2017;39(2):136–140. doi:10.1080/0142159X.2016.1248924
39. Misch DA. Andragogy and medical education: are medical students internally motivated to learn? Adv Health Sci Educ Theory Pract. 2002;7(2):153–160. doi:10.1023/A:1015790318032
40. Tariq M, Abid S, Jafri W. Morning report is an effective teaching activity: residents and faculty perspectives. J Surg Pak Int. 2004;9:38.
41. Al Qarni A, Al-Nasser S, Alzahem A, Mohamed TA. Quality improvement and patient safety education in internal medicine residency training program: an exploratory qualitative study. Adv Med Educ Pract. 2021;12:499–506. doi:10.2147/AMEP.S300266
42. Tariq M, Vaqar M, Abid S, Jafri W. Morning report improves residents. Diagnostic competence and clinical problem-solving ability. medRxiv. 2022;2022:2022.
43. Luciano GL, Carter BL, Garb JL, Rothberg MB. Residents-as-teachers: implementing a toolkit in morning report to redefine resident roles. Teach Learn Med. 2011;23(4):316–323. doi:10.1080/10401334.2011.611762
44. James MT, Mintz MJ, McLaughlin K. Evaluation of a multifaceted “Resident-as-teacher” educational intervention to improve morning report. BMC Med Educ. 2006;6(1):20. doi:10.1186/1472-6920-6-20
45. Lawrence CB, Moore M, Painter AB, Zwemer E. 67. Does providing consistent feedback improve the perceived quality of morning report? Acad Pediatr. 2020;20(7):e32. doi:10.1016/j.acap.2020.06.088
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.