Back to Journals » Vascular Health and Risk Management » Volume 18
The Liverpool Heart And bRain Project (L-HARP): Protocol for an Observational Cohort Study of Cardiovascular Risk and Outcomes Following Stroke
Authors Harrison SL, Lane DA, Buckley BJR, Chatterjee K, Alobaida M ![]() , Shipley E
, Shipley E ![]() , Lip GYH
, Lip GYH
Received 11 January 2022
Accepted for publication 1 April 2022
Published 26 April 2022 Volume 2022:18 Pages 313—318
DOI https://doi.org/10.2147/VHRM.S357829
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Konstantinos Tziomalos
Video abstract of "L-HARP: post-stroke cohort study protocol" [ID 357829].
Views: 122
Stephanie L Harrison,1,2 Deirdre A Lane,1– 3 Benjamin JR Buckley,1,2 Kausik Chatterjee,4 Muath Alobaida,1,2,5 Emily Shipley,1,2 Gregory YH Lip1– 3
1Liverpool Centre for Cardiovascular Science, University of Liverpool, Liverpool, UK; 2Cardiovascular and Metabolic Medicine, Institute of Life Course and Medical Sciences, University of Liverpool, Liverpool, UK; 3Department of Clinical Medicine, Aalborg University, Aalborg, Denmark; 4Care of the Elderly Department, Countess of Chester Hospital NHS Foundation Trust, Chester, UK; 5Department of Basic Science, Prince Sultan Bin Abdulaziz College for Emergency Medical Services, King Saud University, Riyadh, Saudi Arabia
Correspondence: Stephanie L Harrison, Liverpool Centre for Cardiovascular Science, University of Liverpool, 6 West Derby Street, Liverpool, L7 8TX, UK, Email [email protected]
Abstract: Further research is needed to refine risk prediction models for adverse cardiovascular outcomes following stroke in contemporary clinical practice, such as incident atrial fibrillation (AF), recurrent stroke, and cognitive impairment and dementia. The aims of this study are to prospectively investigate cardiovascular outcomes and risk factors for incident cardiovascular disease in a post-stroke cohort, and to externally validate, refine and expand current risk prediction models for cardiovascular and cardiovascular-related outcomes. The study sample size was based on the development of post-stroke risk prediction models for AF and was calculated as 1222 participants. The study design is a multicentre, prospective, observational cohort study. Participants will be adult patients admitted for ischaemic stroke confirmed by stroke physician or transient ischaemic attack (TIA) confirmed by MRI. Routinely collected data will be used in addition to the completion of simple validated questionnaires by the participants. Follow-up will be undertaken 12-months from the date of admission to hospital, in addition to linkage to routinely collected follow-up hospitalisation and mortality data. The primary outcomes are cardiovascular outcomes (including incident AF, stroke, TIA and myocardial infarction) at 12-month follow-up, all-cause mortality and mortality from cardiovascular causes, and incident cognitive impairment and dementia. Secondary outcomes include changes in function, depression, anxiety, fatigue and quality of life. The study has received approval from the Health Research Authority Research Ethics Committee (21/WA/0209), and is registered on https://www.clinicaltrials.gov/ (Identifier NCT05132465). Recruitment for the study began in October 2021 with completion of recruitment at all participating centres anticipated by October 2022.
Keywords: stroke, risk prediction, epidemiology, cohort study
Introduction
Extensive research has been conducted to identify individuals at a high-risk of cardiovascular disease through the development of risk prediction models. This has led to the incorporation of risk models for cardiovascular disease into clinical practice guidelines to improve patient-centred care and decision-making.1,2 People with prior stroke are at a high-risk of adverse cardiovascular outcomes, including atrial fibrillation (AF), recurrent stroke, cognitive impairment and dementia. Several risk prediction models have examined cardiovascular and cardiovascular-related outcomes in people post-stroke, but further research is needed to refine these models and make recommendations for implementation to clinical practice.
The C2HEST score has been shown to perform well in discriminating risk of incident AF in people post-stroke (C index 0.73), which performed significantly better than the Framingham risk score (C index 0.72).3 However, there is no single model that is recommended for clinical practice which can stratify people by risk of AF following a stroke. The CHA2DS2-VASc score and the Essen Stroke Risk Score (ESRS) have shown to modestly predict risk of recurrent stroke in patients with ischaemic stroke (C-statistics approximately 0.55).4 The TRA2◦P (Thrombin Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events) score has previously shown a strong graded relationship with the rate of cardiovascular death, myocardial infarction (MI) and ischaemic stroke in patients with previous MI.5 However, similarly to the CHA2DS2-VASc and ESRS, the TRA2◦P score was also suggested to have low-moderate performance to predict overall cardiovascular risk in patients following stroke.4 Models have been developed to predict other important outcomes including function, dementia and mortality following ischaemic stroke.6,7 Although these existing models have potential utility in clinical practice, further external validation is required before they could be used to support decision-making.
In addition, identifying precise risk prediction models for cardiovascular disease and cardiovascular-related complications in people post-stroke is needed to target screening for conditions such as AF and recurrent stroke, and develop targeted population-specific intervention strategies.
The Liverpool-Heart and bRain Project (L-HARP) will establish a post-stroke cohort with aims to: 1) prospectively test risk factors for incident cardiovascular disease, including AF and recurrent stroke, and 2) externally validate, refine and expand current risk prediction models for cardiovascular disease, cognitive impairment and dementia and mortality.
Materials and Methods
Design
This study is a multicentre, prospective, observational cohort study of people following hospitalisation for ischaemic stroke or transient ischaemic attack (TIA) in England and Wales. The study plans to recruit a minimum of 1222 participants across the participating hospital sites. At enrolment, data collected as part of usual care will be recorded and some additional questions regarding the health of the participant will be elicited via questionnaires. Data will be inputted into an electronic case report form and a follow-up assessment will occur 12 months from the date of admission to the hospital, to repeat some of the questionnaires. The follow-up will be completed within two weeks before or within two weeks after the 12-month date. Where possible, follow-ups will be conducted remotely. Additionally, consent will be requested at baseline to link to the participant’s hospital episode statistics (HES) and mortality data for 12 months from the date of admission to the hospital, held by the National Health Service (NHS) Digital.
Patient Population - Inclusion and Exclusion Criteria
To facilitate the inclusion of people who are often excluded from clinical studies, the eligibility criteria are broad. Participants will be included if they are aged ≥18 years and have had an ischaemic stroke confirmed by a stroke physician or TIA confirmed by magnetic resonance imaging (MRI). Participants will be excluded if they are unable to provide informed consent or if they have no personal consultee available or the personal consultee does not think the person would want to participate, or they are receiving palliative or end-of-life care (Figure 1).
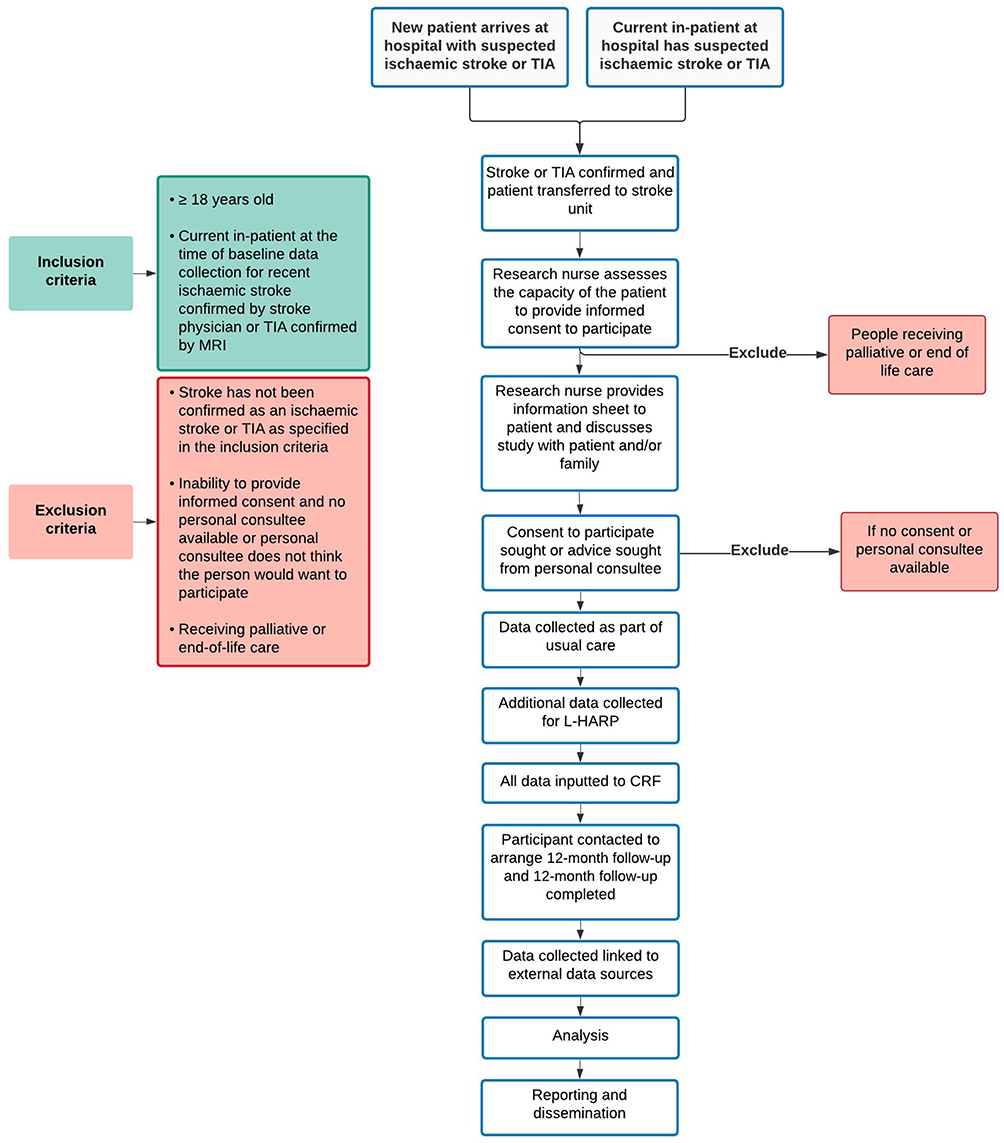 |
Figure 1 Flow diagram of the Liverpool-Heart and bRain Project (L-HARP) stroke cohort for participant recruitment, and inclusion and exclusion criteria. Abbreviations: TIA, transient ischaemic attack; MRI, magnetic resonance imaging; CRF, case report form. |
Often people living with cognitive impairment, dementia or aphasia are excluded from research studies without adequate reasoning. Consequently, in this study, the option to seek advice from a personal consultee (relative/friend/carer) has been included where informed consent is not possible, in line with the Mental Capacity Act 2005 in the United Kingdom. The study research nurse for the participating hospital will assess the capacity of each participant to provide consent in consultation with other healthcare professionals with a duty of care to the participant, as appropriate.
Treatment or Intervention
No intervention is planned. The participants will be treated in line with usual care practices at the participating hospitals.
Primary Outcomes
● Cardiovascular outcomes including AF, recurrent stroke, TIA, and myocardial infarction within 12 months from the index stroke determined from HES data or self-reported at the follow-up assessment.
● All-cause mortality and mortality from cardiovascular causes within 12 months from the index stroke.
● Cognitive decline as determined by changes in the Montreal Cognitive Assessment between baseline and follow-up assessments, and incident dementia within 12 months from the index stroke determined from HES data or self-reported at the follow-up assessment.
Secondary Outcomes
- Changes in function, depression, anxiety, fatigue and quality of life (questionnaires described in Supplementary Table 1)
Data Quality
The electronic case report form has been developed using Research Electronic Data Capture (REDCap; https://www.project-redcap.org). REDCap is a secure web application for building and managing online surveys and databases. Data quality will be monitored monthly by members of the University of Liverpool research team. A report detailing any missing data or inconsistencies in data will be provided to the participating sites and the local study teams will be asked to address the data queries and update the data collected accordingly.
Sample Size Estimates
One of the main aims of this study is to examine post-stroke risk prediction models for AF and therefore this has been used to determine the sample size. Post-stroke prevalence of AF has been estimated at approximately 24% using eight different diagnostic methods up to a mean 74.8 days following stroke or TIA.8 A more precise estimate of AF diagnosed within 12 months following stroke based on routine care only within the UK is not available, and there will be variation in the level of monitoring received as part of routine care if AF is suspected in this cohort during the follow-up time. Based on this estimate, the approach by Riley et al, to calculate sample size for developing a risk prediction model was followed using an online calculator available at https://riskcalc.org/pmsamplesize/.9 The number of candidate predictor values for potential inclusion in the model was set at 12 as this is the maximum number of variables included in previous AF prediction models (Supplementary Table 2), and the level of shrinkage was set to the recommended small amount of desired shrinkage (≤10%) during model development.9 From this, it was calculated that a minimum sample size of 1019 would be required for the model. The study aims to recruit these participants plus an additional 20% to account for potential loss to follow-up, resulting in a minimum target recruitment of 1222 participants.
Statistical Analyses
All data collected will be quantitative. Cox proportional hazard models adjusted for potential confounding factors will be used to examine associations between risk factors and cardiovascular outcomes and mortality. Risk models identified in previous studies for AF and cardiovascular-related outcomes, including cardiovascular disease, physical function, cognitive impairment and dementia, quality-of-life, and all-cause and cardiovascular mortality, will be examined in the L-HARP stroke cohort. Receiver operating characteristic curves will be constructed, and Harrell C indexes (ie area under the curve) will be estimated as a measure of model performance and compared using the DeLong test. Calibration of the models will be assessed by plotting the estimated risk against observed incidence.10 Calibration slopes will be compared, and a slope >1 overestimates risk and a slope <1 underestimates risk.11
In addition to traditional epidemiological approaches to risk prediction modelling, machine learning methodologies will also be used. Machine learning has been shown to produce comparable results to traditional cardiovascular disease risk prediction scores, but with advantages such as examining all available data in an unbiased approach which could lead to the discovery of new relationships among data. Traditional machine learning techniques, including k-Nearest Neighbours, random forest, and decision tree, will be utilised rather than deep learning techniques, which are usually applied to larger datasets. A subset of the data (two-thirds) will be used for model training, with the remainder (one-third) used for model evaluation. The accuracy, specificity, sensitivity, positive and negative predictive values of the models will be compared.
Study Organisation and Funding
The study is co-ordinated by academic researchers and clinical collaborators at the Liverpool Centre for Cardiovascular Science (LCCS). The study steering committee provides overall governance for the project.
The study has received the approval from Health Research Authority Research Ethics Committee (21/WA/0209), and the University of Liverpool is the sponsor for the project (UoL001512). The study is supported with part-funding from Bristol-Myers Squibb, as well as a National Institute for Health Research (NIHR) Senior Investigator grant to Professor Lip.
Discussion
The L-HARP is important to determine optimal risk prediction models for outcomes in individuals following a stroke that are feasible to use as part of patient care pathways. The study plans to use routinely collected data and some additional questionnaires at the time of the ischaemic stroke or TIA and examine outcomes at 12 months following stroke. In this prospective cohort study, novel prediction models for important outcomes for patients following stroke including recurrent stroke, cardiovascular disease, AF and mortality will be developed and compared to previously developed models.
There will be variation in the amount of surveillance individuals will receive for certain outcomes including AF as part of routine care. For this study, there was no further funding available to perform additional clinical monitoring of the participants and the study aims to use routinely collected data as much as possible. The risk prediction models will reflect a “real-world” approach, but this may limit the accuracy of the risk models for AF.
Recruitment for the L-HARP opened in October 2021. Opening of sites is ongoing as sites have varied in the time to process local approvals and complete the required study training. As of 8th March 2022, 18 participating hospitals had begun recruitment for the study and 293 participants had been recruited. On this date, a further 10 hospitals were processing local approvals before commencing recruitment. A map showing the location of the participating hospitals is shown in Supplementary Figure 1.
Conclusion
Although several risk models for cardiovascular and cardiovascular-related outcomes have been examined in patients following stroke, moderate accuracy has often been observed and further research is needed to refine these models or develop models with higher accuracy which can be implemented in routine clinical practice. The Liverpool-Heart and bRain Project is a large multicentre prospective study aiming to utilise routinely collected data and limited additional data from patients to improve prediction of cardiovascular and cardiovascular-related outcomes following stroke. Good feasibility to recruit the target number of patients has been demonstrated during the first five months of study recruitment.
Disclosure
SLH reports grants from Bristol Myers Squibb (BMS) during the conduct of the study. DAL reports grants from BMS and personal fees from Boehringer Ingelheim and BMS/Pfizer outside the submitted work; received investigator-initiated educational grants from BMS, has been a speaker for Bayer, Boehringer Ingelheim, and BMS/Pfizer, and has consulted for BMS and Boehringer Ingelheim. BJRB: received funding from BMS/Pfizer. KC, MA and ES report no conflicts of interest. GYHL reports being a consultant for Bayer/Janssen, BMS/Pfizer, Medtronic, Boehringer Ingelheim, Novartis, Verseon and Daiichi-Sankyo and speaker for Bayer, BMS/Pfizer, Medtronic, Boehringer Ingelheim, and Daiichi-Sankyo. The authors report no other potential conflicts of interest for this work.
References
1. Goff DC
2. Usher-Smith JA, Silarova B, Schuit E, Moons KG, Griffin SJ. Impact of provision of cardiovascular disease risk estimates to healthcare professionals and patients: a systematic review. BMJ Open. 2015;5(10):e008717. doi:10.1136/bmjopen-2015-008717
3. Sposato LA, Cipriano LE, Saposnik G, Ruiz Vargas E, Riccio PM, Hachinski V. Diagnosis of atrial fibrillation after stroke and transient ischaemic attack: a systematic review and meta-analysis. Lancet Neurol. 2015;14(4):377–387. doi:10.1016/S1474-4422(15)70027-X
4. Georgiopoulos G, Ntaios G, Stamatelopoulos K, et al. Comparison of risk scores for the prediction of the overall cardiovascular risk in patients with ischemic stroke: the Athens stroke registry. J Stroke Cerebrovasc Dis. 2019;28(12):104415. doi:10.1016/j.jstrokecerebrovasdis.2019.104415
5. Bohula EA, Bonaca MP, Braunwald E, et al. Atherothrombotic risk stratification and the efficacy and safety of vorapaxar in patients with stable ischemic heart disease and previous myocardial infarction. Circulation. 2016;134(4):304–313. doi:10.1161/CIRCULATIONAHA.115.019861
6. Fahey M, Crayton E, Wolfe C, Douiri A. Clinical prediction models for mortality and functional outcome following ischemic stroke: a systematic review and meta-analysis. PLoS One. 2018;13(1):e0185402. doi:10.1371/journal.pone.0185402
7. Lim JS, Oh MS, Lee JH, et al. Prediction of post-stroke dementia using NINDS-CSN 5-minute neuropsychology protocol in acute stroke. Int Psychogeriatr. 2017;29(5):777–784. doi:10.1017/S1041610216002520
8. Li YG, Bisson A, Bodin A, et al. C2 HEST score and prediction of incident atrial fibrillation in poststroke patients: a French nationwide study. J Am Heart Assoc. 2019;8(13):e012546. doi:10.1161/JAHA.119.012546
9. Riley RD, Ensor J, Snell KIE, et al. Calculating the sample size required for developing a clinical prediction model. BMJ. 2020;368:m441. doi:10.1136/bmj.m441
10. Van Calster B, McLernon DJ, van Smeden M, et al. Calibration: the Achilles heel of predictive analytics. BMC Med. 2019;17(1):230. doi:10.1186/s12916-019-1466-7
11. Khurshid S, Kartoun U, Ashburner JM, et al. Performance of atrial fibrillation risk prediction models in over 4 million individuals. Circ Arrhythm Electrophysiol. 2021;14(1):e008997. doi:10.1161/CIRCEP.120.008997
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.