Back to Journals » Clinical Epidemiology » Volume 14
The Interaction Effect Between Previous Stroke and Hip Fracture on Postoperative Mortality: A Nationwide Cohort Study
Authors Hjelholt TJ ![]() , Johnsen SP, Brynningsen PK, Pedersen AB
, Johnsen SP, Brynningsen PK, Pedersen AB ![]()
Received 8 February 2022
Accepted for publication 1 April 2022
Published 27 April 2022 Volume 2022:14 Pages 543—553
DOI https://doi.org/10.2147/CLEP.S361507
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eyal Cohen
Thomas J Hjelholt,1,2 Søren P Johnsen,3 Peter K Brynningsen,4 Alma B Pedersen1,2
1Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus N, DK-8200, Denmark; 2Department of Clinical Medicine, Aarhus University, Aarhus N, DK-8200, Denmark; 3Danish Center for Clinical Health Services Research, Department of Clinical Medicine, Aalborg University, Aalborg Ø, DK-9220, Denmark; 4Department of Geriatrics, Aarhus University Hospital, Aarhus N, DK-8200, Denmark
Correspondence: Thomas J Hjelholt, Department of Clinical Epidemiology, Aarhus University Hospital, Olof Palmes Alle 43-45, Aarhus N, DK-8200, Denmark, Tel +45 871 68219, Email [email protected]
Purpose: It remains uncertain how a history of stroke impacts the prognosis for patients with hip fracture. This study aimed to evaluate mortality following hip fracture surgery by comparing patients with and without a history of stroke.
Patients and Methods: All patients aged 65 years or above in Denmark receiving hip fracture surgery between 2010 and 2018. For every patient, 10 individuals from the general population without hip fracture were sampled. Comparators had a similar stroke history, age, and sex on the date of hip fracture surgery (index date). We established four cohorts: hip fracture patients with/without stroke and non-hip fracture patients with/without stroke. Outcomes were all-cause mortality at 0– 30 days, 31– 365 days and 1 to 5 years. Direct standardized mortality rates (MR) with 95% confidence intervals (CI) were computed. We calculated the interaction contrast to estimate excess absolute mortality among patients with both hip fracture and stroke. Through a Cox proportional hazards model, we estimated the hazard ratio (HR) and the attributable proportion as a measure of excess relative mortality attributable to interaction.
Results: Of the hip fracture patients, 8433 had a stroke history and 44,997 did not. Of the non-hip fracture patients, 84,330 had a stroke history and 449,962 did not. Corresponding 30-day MRs/100 person years were 148.4 (95% CI: 138.8– 158.7), 124.3 (95% CI: 120.7– 128.1), 14.3 (95% CI: 13.4– 15.2) and 8.4 (95% CI: 8.1– 8.7). The interaction contrast was 18.2 (95% CI: 7.5– 28.8), and the attributable proportion was 9.0% (95% CI: 2.9– 15.1). No interaction was present beyond 30 days.
Conclusion: We observed excess short-term mortality in patients with stroke and hip fracture, but the effect disappeared at later follow-up periods. Clinicians are encouraged to pay rigorous attention to early complications among hip fracture patients with stroke, as this may serve as a way to reduce mortality.
Keywords: hip fracture, interaction, mortality, prognosis, stroke
Plain Language Summary
Stroke and hip fracture are common conditions among elderly individuals and thus, 15% of patients have a history of stroke at the time of the accident causing a fractured hip. How this impacts the prognosis following hip fracture has been sparsely studied.
This project included all patients in Denmark above 65 years that was surgically treated for a hip fracture between 2010 and 2018. All patients were classified according to stroke history (yes/no). For each patient, we identified 10 individuals from the background population of same age, sex and stroke history but with no record of a hip fracture. Consequently, we obtained four groups: Hip fracture patients with/without stroke and non-hip fracture patients with/without stroke.
We compared the mortality risk in these four groups and found that patients with both hip fracture and stroke had a 9% excess mortality above what should be expected from the individual diseases. The excess mortality was only detectable during the early postoperative phase of 0–30 days, indicating that acute postoperative complications may be the explanation for the increase.
These results indicate that extra awareness of short-term complications in patients with hip fracture and stroke may be beneficial.
Introduction
Hip fracture and stroke are two of the most debilitating conditions among older people. Mortality is high – approximately 30% for both conditions within the first year1,2 and survivors experience increased disability.3,4 Stroke survivors have a 1.4 to 2 times elevated risk of sustaining a hip fracture due to impaired mobility and a high prevalence of osteoporosis.5–8 The highest risk is found among the most disabled patients and in those with recent stroke.9 Consequently, around 15% of patients with hip fracture have a history of stroke.10 Despite this knowledge, a previous report showed that stroke survivors were infrequently screened and treated for osteoporosis.11
Patients with previous stroke and affected physical or cognitive function would be expected to have increased mortality following hip fracture due to a higher risk of postoperative complications.12 Furthermore, hip fracture patients with stroke history may benefit less from rehabilitation,13 resulting in increased chronic disability following hip fracture, thereby increasing the risk of a poor long-term outcome, including higher mortality. However, only a few studies have examined how stroke history affects prognosis among patients with fracture5,13–16 and results are diverging. The existing studies are constrained by small and selected populations,5,13,14,16 short follow-up duration,15 or lack of adjustment for potential confounders.5,13,15,16 Thus, it remains to be established if hip fracture patients with stroke history have increased mortality during short and/or long-term follow-up. Furthermore, an investigation of whether stroke and hip fracture interact to increase mortality above the effect of each individual disease on mortality would provide important knowledge regarding possible areas accessible for intervention.
The aim of this study was to examine the interaction effect between stroke and hip fracture on mortality 30 days, 1- and 5 years following hip fracture surgery. To do so, we investigated mortality in four cohorts: Patients with hip fracture with/without previous stroke and non-hip fracture patients with/without previous stroke.
Patients and Methods
Design and Setting
We conducted a matched cohort study, using nationwide Danish medical registries. The Danish hospital system is 100% government funded, guaranteeing free and equal access to healthcare for all individuals.17
Data Sources
The Civil Registration System18 holds information on migrant and vital status, and provides a unique 10-digit identifier (CPR-number) for each person. The CPR number encodes date of birth and sex and allow for accurate individual-level linkage of registries.
The Danish Multidisciplinary Hip Fracture registry19 was used to identify patients with hip fracture. This clinical quality registry includes all surgically treated patients with hip fracture above age 65.
The Danish National Patient Registry20 was consulted for identifying patients’ history of stroke and other comorbidities. All hospital contacts are recorded in this registry, primary and secondary diagnoses are coded using the International Classification of Diseases, 10th revision (ICD-10).
The Danish Stroke Registry21 holds key information on all adults admitted to Danish hospitals with acute stroke since 2003.
The Danish National Prescription Registry22 was accessed to obtain information on prescription medicine for all individuals. The registry records all dispensings by community pharmacies, using the Anatomical Therapeutic Chemical classification codes (ATC-codes).
Selection of Patients for Hip Fracture and Comparison Cohorts
Patients undergoing surgery due to a first-time hip fracture between January 1st 2010 and December 31st 2018 were initially identified in the Danish Multidisciplinary Hip Fracture Registry. Patients were excluded if the time from admission to surgery was more than 72 hours, as this was considered a possible erroneous registration.
We sampled a comparison cohort of 10 individuals per hip fracture patient from a 2% random sample of the general population. These individuals were matched on age (+/- one month), sex, and history of stroke (lookback period 15 years, see Supplementary Table 1 and Supplementary Figure 1). Individuals were eligible for matching if they were alive and without a hip fracture diagnosis on the day of hip fracture operation (index date) of their matched case. Thus, we obtained four cohorts: hip fracture patients with/without stroke history and non-hip fracture patients with/without stroke history. Matching was done with replacement as this has proven to be the most robust method when persons were at a high risk of the outcome.23 Eight patients with hip fracture and high age (≥100 years) were excluded because no eligible matches were found.
Outcome
All-cause mortality was recorded from the Civil Registration System. The vital status is updated daily, enabling a precise date of death to be deducted. Follow-up was divided into three periods reflecting short, intermediate and long-term prognosis: 0–30 days, 31–365 days and 1–5 years.
Covariates
Diagnoses of comorbid diseases prior to index date were found in the National Patient Registry. To obtain a uniform measure of comorbidity, we used the Charlson Comorbidity Index (CCI) score.24 Because entry into two of the cohorts in this study was dependent on a stroke diagnosis, we modified the CCI score by excluding the variable “cerebrovascular disease” in the calculation. Comorbidity burden was classified using the modified CCI score categorized into low (CCI score = 0), moderate (CCI score = 1–2), or severe (CCI score = 3+).
The use of the following, frequently used, types of medication was included: antithrombotics, oral anticoagulants, lipid lowering drugs, antihypertensives, antidiabetics, antipsychotics, and antidepressants. As we wanted an indication of drug use at index date, we approximated current users as patients with at least one prescription redeemed within three months from index date. Furthermore, we included use of osteoporosis medication one year from index date as a baseline variable to obtain an indication of current osteoporosis treatment at baseline.
Stroke subtype was identified based on the ICD-10 code (hemorrhagic or ischemic), whereas stroke severity was obtained from the Danish Stroke registry, which records the Scandinavian Stroke Scale score25 on admission. Data were available for approximately 50% of stroke patients with equal distribution between the groups. Missing records were mainly related to strokes occurring before the time of routine registration. Patients were categorized into severe (≤29 points), moderate (30–44 points), or mild (≥45 points) stroke.
Statistical Analysis
Age, sex, comorbidity, medication use, and year of surgery/index date were tabulated across the four cohorts (hip fracture patients with/without stroke and non-hip fracture patients with/without stroke).
The cohorts were followed from the index date until a registration of mortality in the CRS, emigration or end of follow-up (five years after index date or end of study period (December 31st 2018)).
Measures of Association
Direct standardized mortality rates (MRs) per 100 person years (PYs) with 95% confidence intervals (CIs) were calculated. Standardization was performed using age, sex, and CCI score categories – both in the overall and in the stratified analyses (except for the variable that was stratified on).
A Cox proportional hazards regression analysis was performed to obtain a relative measure of association, the hazard ratio (HR) with 95% CIs. Analyses were adjusted for age (continuous), sex and CCI-score (continuous). The proportionality assumption was tested through log–log curves and found to be satisfactory.
Measures of Interaction
It is recommended to report interactions on both the absolute and on the relative scale.26 On the absolute scale, the interaction effect was calculated using the interaction contrast (IC).27 The IC denotes the MR among patients with hip fracture and previous stroke that exceeds the expected MR based on addition from the three other cohorts (note that the MRnon hip fracture – stroke is a part of the MR in the other cohorts and is therefore subtracted):

To obtain a measure of interaction on the relative scale, we estimated the attributable proportion of the HR to the interaction between stroke and hip fracture. This can be viewed as a theoretical indication of how much the HR could be reduced if hip fracture patients were completely free from stroke.28
Sensitivity Analyses
We performed four sensitivity analyses:
To obtain information on whether the severity of the stroke affected our results, we repeated the analysis across strata of stroke severity.
Since the timing of the stroke before hip fracture might impact results, especially if stroke rehabilitation is incomplete and the level of function has not yet stabilized, we stratified patients in the two stroke cohorts based on time from stroke (less than 6 months or not) to index date.
As different stroke types might impact prognosis differently, we stratified the stroke cohorts according to whether strokes were classified as ischemic or hemorrhagic.
As a cerebrovascular event is likely to affect pharmacological treatment of the patient, we primarily observed medication use as a mediator of the association we were investigating. However, as some medications could also possibly confound the association, we repeated the analyses with baseline medication use included in the model as covariates.
The study is reported according to the REporting of Studies Conducted Using Observational Routinely‐Collected Data (RECORD) guidelines.29 All analyses were performed on the remote servers of Statistics Denmark using R version 4.0.2 (R Foundation for Statistical Computing).
Results
We included 53,430 patients with hip fracture, of which 8433 patients had a history of stroke (15.8%) and 534,292 individuals in the cohorts without hip fracture, including 84,330 with stroke. When matching was done with replacement, an individual from the general population was eligible for selection several times. Consequently, the comparison cohorts consisted of 348,077 unique individuals.
The age distributions were comparable between the four groups (Table 1). Patients with hip fracture and stroke were most comorbid, followed by non-hip fracture patients with stroke, hip fracture patients without stroke and finally, non-hip fracture patients without stroke. Osteoporosis medication was used by 9.5–13% of patients depending on the cohort, slightly more frequent by patients with hip fracture, and slightly less frequent by stroke patients. Cross-tabulation of individual comorbidities in the CCI score can be found in Supplementary Table 2.
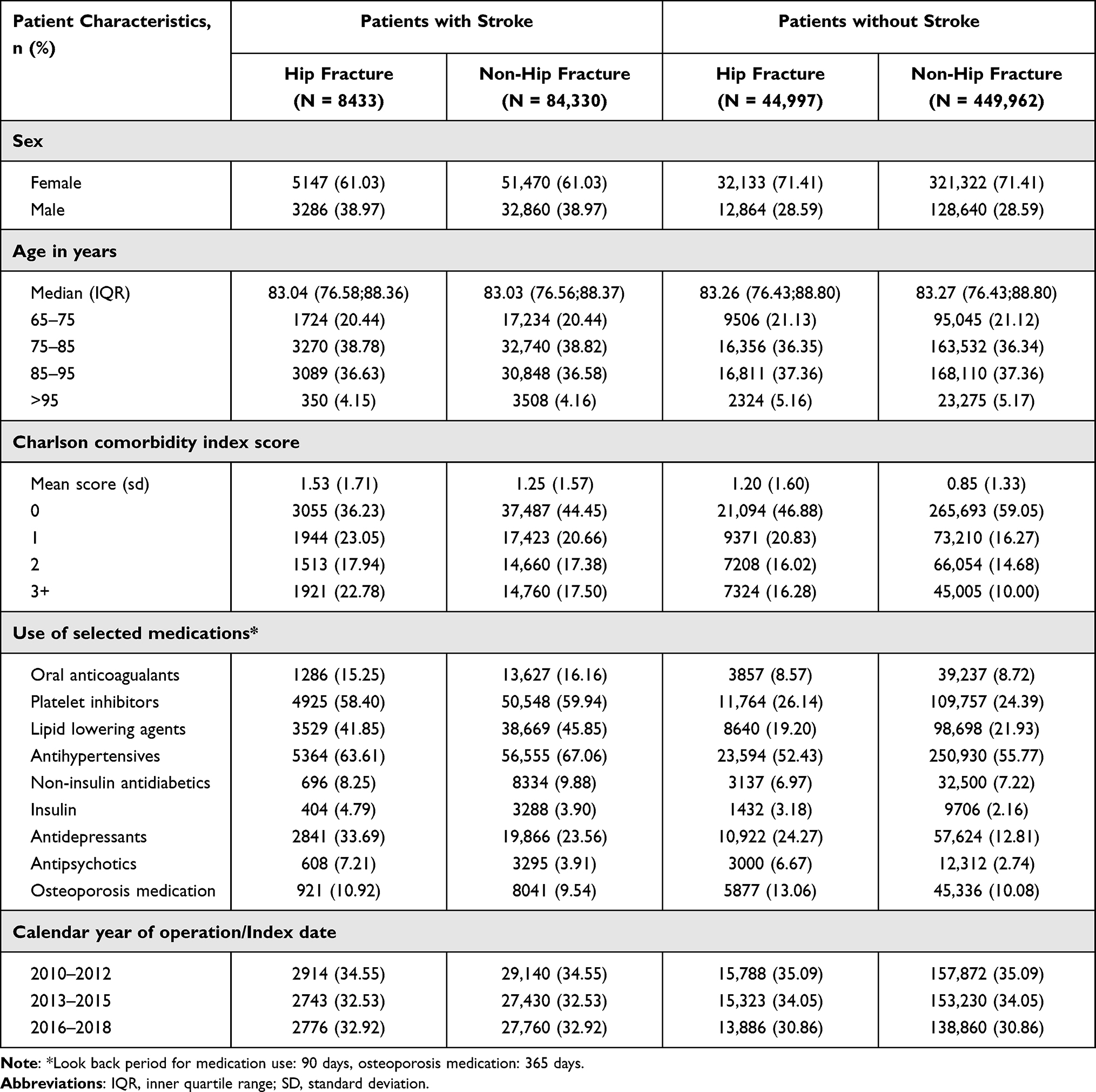 |
Table 1 Patient Characteristics at Index Date |
Mortality, Overall Cohorts
At 0–30-day follow-up, the MRs were markedly higher in the two hip fracture cohorts. Also, in both hip fracture and non-hip fracture patients, stroke further increased the MR from 8.4/100 PYs (95% CI: 8.1–8.7) to 14.3/100 PYs (95% CI: 13.4–15.2) in the non-hip fracture cohort and from 124.3/100 PYs (95% CI: 120.7–128.1) to 148.4/100 PYs (95% CI: 138.8–158.7) in the hip fracture cohort. See also Table 2 and Figure 1. Based on the absolute risks, we found an IC of 18.2/100 PYs, indicating an excess mortality among hip fracture patients with a history of stroke.
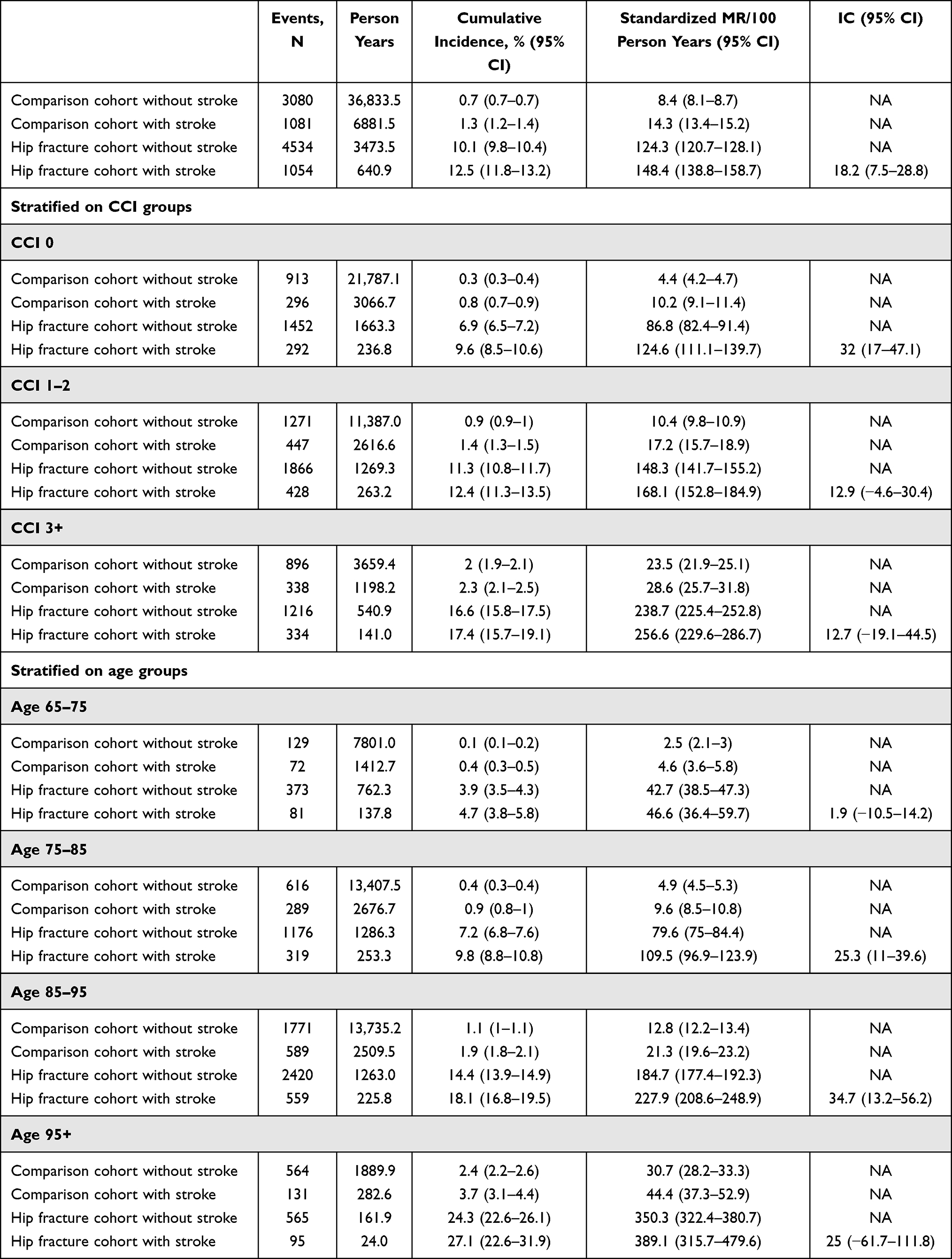 |
Table 2 0–30-Day Mortality in the Four Cohorts: Risks, Rates and Interaction Contrast (IC). Overall and Stratified on Comorbidity and Age |
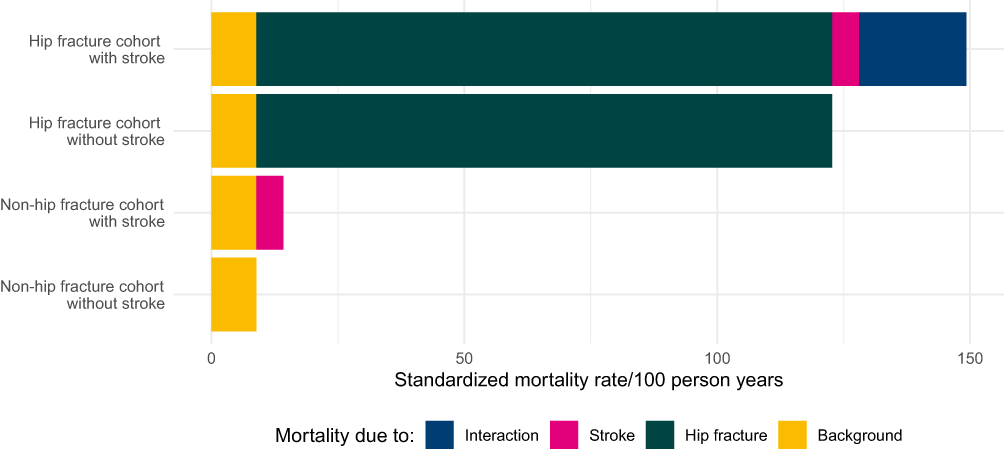 |
Figure 1 0–30 day standardized mortality rate in the four cohorts: Hip fracture with/without stroke and non-hip fracture with/without stroke. |
In the adjusted Cox proportional hazards analysis (Figure 2), using patients without hip fracture and without stroke as reference, we found the same pattern as for the absolute risks. We observed HRs of 1.7 (95% CI: 1.6–1.8) in the non-hip fracture cohort with stroke, 15.1 (95% CI: 14.4–15.8) in the hip fracture cohort without stroke, and 17.3 (95% CI: 16.1–18.6) in the hip fracture cohort with stroke. From the relative estimates, the AP was 9.0% (95% CI 2.9–15.1).
 |
Figure 2 0–30 day relative mortality: Hazard ratios (HR) and attributable proportion (AP) with 95% confidence intervals (CI). Overall and stratified on comorbidity and age. Abbreviations: CCI, Charlson Comorbidity Index; Adjusted for age, sex and CCI score. Notes: Forest plot indicating the hazard ratios for 0–30-day mortality, whiskers indicating 95% confidence intervals. Non-hip fracture patients without stroke are used as a reference. Cohort explanation: Non-hip – S; Non-hip fracture patients without stroke, Non-hip + S; Non-hip fracture patients with stroke, Hip – S; Hip fracture patients without stroke, Hip + S; Hip fracture patients with stroke. |
For later follow-up times (31–365 days and 1–5 years) the same pattern was observed with stepwise increase in MRs and HRs in the non-hip fracture cohort with stroke and further increase in hip fracture cohort without stroke and highest mortality in the hip fracture cohort with stroke. The excess mortality was not as profound as observed for the short follow-up, and we found no interaction, as indicated by an IC and AP around zero (Supplementary Tables 3, 4 and Supplementary Figures 2, 3).
Mortality, Stratified on CCI Score and Age
After stratifying the analysis according to CCI score categories, we found augmented 0–30-day MRs in all cohorts as the level of comorbidity increased (Table 2). In the Cox proportional hazards analysis, we observed decreasing HRs with increasing comorbidity, reflecting that the relative increase in mortality due to stroke and hip fracture was lower, when other comorbidities were present (Figure 2). Generally, the same pattern as described above was present between the cohorts in each stratum. The interaction was highest when no other comorbidities were present in the cohorts (CCI score 0: IC = 32.0/100 PYs (95% CI: 17.0–47.1), AP = 23.5% (95% CI: 13.9–33.1)), whereas the interaction faded in strata with higher comorbidity.
Stratification on age categories also showed increasing MRs by higher age in all cohorts (Table 2). On the relative scale, the HRs decreased slightly for each increase in age category (Figure 2). We found a positive interaction in the 75–85-year stratum and in the 85–95-year stratum (IC = 25.3/100 PYs (95% CI: 11.0–39.6) and 34.7/100 PYs (95% CI: 13.2–56.2), AP = 11% (95% CI: 0.0–22.0) and 10% (95% CI: 1.7–18.3)).
The stratified results for the later follow-up periods generally show the same consistency.
Sensitivity Analyses
1) When stratifying on severity of stroke, the excess mortality for patients with hip fracture and stroke was most evident among patients with high stroke severity. Patients with hip fracture and mild stroke had comparable MRs as patients with hip fracture-only. Both IC and AP estimates were close to zero and showed considerable uncertainty in the estimates (data not shown).
2) Patients with stroke within six months from hip fracture had higher excess mortality than patients with stroke more than six months from hip fracture: Standardized MR among hip fracture with stroke: 173.5/100 PY (95% CI: 147.7–203.9) for recent stroke, 148.1/100 PY (95% CI: 137.3–159.8) for not-recent stroke. The IC and AP estimates were imprecise (data not shown).
3) 9344 patients (10.1%) had an intracerebral bleeding as their latest stroke event with equal distribution between the two stroke cohorts. We observed no difference between mortality – nor on interaction estimates based on the type of stroke (data not shown).
4) Baseline medication use is presented in Table 1 and described above. Including medication use as covariates in the Cox model (each type of medication as an independent variable) did not alter the results (data not shown).
Discussion
This study shows an interaction effect between stroke and hip fracture on the risk of 0–30-day mortality of 18.2 events per 100 PYs – more than double the mortality rate in the comparison cohort of patients without neither stroke nor hip fracture. No interaction was present at later follow-up times, indicating that short-term complications following hip fracture may be the reason for the excess mortality. The interaction was most pronounced among patients with no other comorbidities and patients aged 75–95 years.
Surprisingly, only 10.9% of patients with stroke had received osteoporosis treatment in the year prior to hip fracture. Combining the numerous reports of increased hip fracture risk among patients with stroke,7,30 with our results indicating a substantially increased risk of mortality in patients with stroke and hip fracture, makes the low prevalence of osteoporosis treatment even more alarming. Even though post-stroke osteoporosis is mentioned as a concern in current clinical guidelines for stroke management,31 more attention to screening for osteoporosis and consideration of antiresorptive treatment appears to be warranted during stroke rehabilitation.32,33
Based on the sensitivity analyses, our results indicate the excess mortality among hip fracture patients with stroke to be more pronounced if the stroke is of higher severity and if it has occurred within 6 months. These patients have previously been highlighted as the group with the highest risk of sustaining a hip fracture,9 emphasizing the importance of clinical attention on preventing falls and fractures in these subgroups of patients.
This is the first study to investigate in detail the impact of stroke history on mortality in patients with hip fracture. Previous studies with follow-up of 6 months13 or one year14,16 have found no difference. At least two of these studies are clearly underpowered (N = 862; 63 with stroke history,14 N = 548; 77 with stroke history16) with estimates pointing towards an association with increased mortality similar to the present findings. The third study13 included patients from 1987 to 2001; both hip fracture and stroke care have changed substantially since then. Other studies have found an increased risk of postoperative complications among hip fracture patients with previous stroke,15 and among stroke patients and hip fracture patients in general.12,34 Patients with stroke have a higher prevalence of poor prognostic factors, including cognitive deficits (including risk of postoperative delirium), nutritional problems and poor mobility. These factors all contribute to the observed effect of increased mortality and thus, they should be considered as mediators of the effect (Supplementary Figure 4). Considering such factors, it seems reasonable to expect hip fracture patients with stroke to be more susceptible to complications, such as cardiovascular events and infections – especially pneumonia. Early postoperative complications may explain the increased mortality and the interaction effect found in this study. The interaction effect was most pronounced in patients with no other comorbidities than stroke, whereas the effect was increasingly diluted in the presence of other comorbidities. The role of age was less clear; an interaction effect was observed in the two middle age categories only, but estimates were imprecise for the oldest category. Possibly, the results could be due to the increased frailty that inherently comes with age, although interpretations should be made with caution. Surprisingly, we observed no interaction effect on the later follow-up periods of 31–365 days and 1–5 years. Contrary to our hypothesis, it appears that stroke is insufficient to impact long-term mortality with an interaction effect.
Methodological Considerations
This nationwide cohort study included all patients receiving surgical treatment for their hip fracture in Denmark. This setup practically eliminates selection bias; hospital treatment is free for all and acute stroke and hip fracture care is exclusively carried out in public hospitals. Both stroke and hip fracture diagnosis codes have been validated, showing highly positive predictive values.35,36 Similarly, the codes used in the CCI have been validated satisfactorily.36 Although information about the severity of the included comorbidities as well as conditions treated exclusively by general practitioners were not available, we find no reason to believe that this should be unevenly distributed across the cohorts. Consequently, it would only introduce a bias towards the null. Similarly, patients may have had other injuries and fractures simultaneously with the hip fracture. It is, however, a relatively rare situation, and we have no reason to believe that this should affect our estimates or be unevenly distributed in the cohorts. We did not have information on delirium, nutritional problems, dysphagia, poor mobility, or low functional level. These factors are likely more prevalent among patients with stroke and a part of the causal pathway between stroke and increased mortality. Consequently, they are mediators in the association – not confounders (see Supplementary Figure 4). Although it would be interesting to analyze the contribution of these factors on mortality, we were not able to do this with the data available. Likewise, we considered baseline medication use as a mediator rather than a confounder of the association. We did, however, also perform an extra adjustment for baseline medication use in a sensitivity analysis to accommodate the fact that some medications might be confounders more than mediators – but this did not alter the results. Body mass index (BMI) and atrial fibrillation are other potential confounders of the observed association between stroke, hip fracture and mortality. We have previously observed that the absolute mortality risk is higher among patients with AF,37 although it is a relatively weak independent predictor when other confounders are considered simultaneously.38 The latter study also showed that high BMI is protective of mortality among patients with hip fracture,38 whereas increasing BMI is related to increased stroke risk. Thus, the associations point in opposite directions. In conclusion, it seems unlikely that BMI or atrial fibrillation would confound the observed association strongly.
Conclusion
In conclusion, we observed an interaction effect of stroke and hip fracture on 0–30-day mortality, but the effect had disappeared at later follow-up periods. Clinicians are encouraged to pay rigorous attention to early complications among hip fracture patients with stroke, as this may serve as a way to reduce the excess short-term mortality. Furthermore, the low prevalence of osteoporosis prophylaxis among stroke survivors indicates room for improvement, with the potential to reduce hip fracture incidence.
Data Sharing Statement
To protect the privacy of patients, individual-level data are not allowed to be publicly disclosed. The statistical code can be made available upon reasonable request.
Ethics Approval
The study was reported to the Danish Data Protection Agency through registration at Aarhus University (record number: AU-2016-051-000001, sequential number 880). Non-interventional registry-based research projects that do not involve human biological material and are based on pure data such as numbers do not require notification to the Danish Scientific Ethics Committee.39
Acknowledgments
The authors wish to thank the surgeons, physicians and other health care professionals for their cooperation in submitting high-quality clinical data to the national registries.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Novo Nordisk Foundation [Grant number NNF170C0029800] and Aase and Ejnar Danielsen’s Foundation, Denmark. The funders had no influence on the study design, collection, analysis, and interpretation of data, writing of the report, or decision to submit the paper for publication.
Disclosure
SPJ has received speaker honoraria from Bayer, Bristol-Myers Squibb, and Pfizer, has participated in advisory board meeting for Bayer, Bristol-Myers Squibb, and Pfizer and received research grants from Bristol-Myers Squibb and Pfizer. The authors report no other conflicts of interest in this work.
References
1. Pedersen AB, Ehrenstein V, Szepligeti SK, et al. Thirty-five-year trends in first-time hospitalization for hip fracture, 1-year mortality, and the prognostic impact of comorbidity: a Danish Nationwide Cohort Study, 1980–2014. Epidemiology. 2017;28(6):898–905. doi:10.1097/EDE.0000000000000729
2. Schmidt M, Jacobsen JB, Johnsen SP, Botker HE, Sorensen HT. Eighteen-year trends in stroke mortality and the prognostic influence of comorbidity. Neurology. 2014;82(4):340–350. doi:10.1212/WNL.0000000000000062
3. Keene GS, Parker MJ, Pryor GA. Mortality and morbidity after hip fractures. BMJ. 1993;307(6914):1248–1250. doi:10.1136/bmj.307.6914.1248
4. Donnan GA, Fisher M, Macleod M, Davis SM. Stroke. Lancet. 2008;371(9624):1612–1623. doi:10.1016/S0140-6736(08)60694-7
5. Ramnemark A, Nilsson M, Borssen B, Gustafson Y. Stroke, a major and increasing risk factor for femoral neck fracture. Stroke. 2000;31(7):1572–1577. doi:10.1161/01.STR.31.7.1572
6. Laroche M, Moulinier L, Leger P, Lefebvre D, Mazieres B, Boccalon H. Bone mineral decrease in the leg with unilateral chronic occlusive arterial disease. Clin Exp Rheumatol. 2003;21(1):103–106.
7. Salehi Omran S, Murthy SB, Navi BB, Merkler AE. Long-term risk of hip fracture after ischemic stroke. Neurohospitalist. 2020;10(2):95–99. doi:10.1177/1941874419859755
8. Dennis MS, Lo KM, McDowall M, West T. Fractures after stroke - frequency, types, and associations. Stroke. 2002;33(3):728–734. doi:10.1161/hs0302.103621
9. Northuis CA, Crandall CJ, Margolis KL, Diem SJ, Ensrud KE, Lakshminarayan K. Association between post-stroke disability and 5-year hip-fracture risk: the Women’s Health Initiative. J Stroke Cerebrovasc Dis. 2020;29(8):104976. doi:10.1016/j.jstrokecerebrovasdis.2020.104976
10. Pedersen AB, Ehrenstein V, Szepligeti SK, Sorensen HT. Excess risk of venous thromboembolism in hip fracture patients and the prognostic impact of comorbidity. Osteoporos Int. 2017;28(12):3421–3430. doi:10.1007/s00198-017-4213-y
11. Kapoor E, Austin PC, Alibhai SMH, et al. Screening and treatment for osteoporosis after stroke. Stroke. 2019;50(6):1564–1566. doi:10.1161/STROKEAHA.118.024685
12. Ingeman A, Andersen G, Hundborg HH, Svendsen ML, Johnsen SP. In-hospital medical complications, length of stay, and mortality among stroke unit patients. Stroke. 2011;42(11):3214–3218. doi:10.1161/STROKEAHA.110.610881
13. Penrod JD, Litke A, Hawkes WG, et al. The association of race, gender, and comorbidity with mortality and function after hip fracture. J Gerontol Series A. 2008;63(8):867–872. doi:10.1093/gerona/63.8.867
14. Youm T, Aharonoff G, Zuckerman JD, Koval KJ. Effect of previous cerebrovascular accident on outcome after hip fracture. J Orthop Trauma. 2000;14(5):329–334. doi:10.1097/00005131-200006000-00004
15. Fisher A, Srikusalanukul W, Davis M, Smith P. Poststroke hip fracture: prevalence, clinical characteristics, mineral-bone metabolism, outcomes, and gaps in prevention. Stroke Res Treat. 2013;2013:641943. doi:10.1155/2013/641943
16. Nho JH, Lee YK, Kim YS, Ha YC, Suh YS, Koo KH. Mobility and one-year mortality of stroke patients after hip-fracture surgery. J Orthop Sci. 2014;19(5):756–761. doi:10.1007/s00776-014-0593-4
17. Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–591. doi:10.2147/CLEP.S179083
18. Schmidt M, Pedersen L, Sorensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
19. Kristensen P, Röck N, Christensen H, Pedersen A. The Danish multidisciplinary hip fracture registry 13-year results from a population-based cohort of hip fracture patients. Clin Epidemiol. 2020;12:9–21. doi:10.2147/CLEP.S231578
20. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
21. Johnsen SP, Ingeman A, Hundborg HH, Schaarup SZ, Gyllenborg J. The Danish stroke registry. Clin Epidemiol. 2016;8:697–702. doi:10.2147/CLEP.S103662
22. Pottegård A, Schmidt SAJ, Wallach-Kildemoes H, Sørensen HT, Hallas J, Schmidt M. Data resource profile: the Danish National Prescription Registry. Int J Epidemiol. 2016;dyw213. doi:10.1093/ije/dyw213
23. Heide-Jørgensen U, Adelborg K, Kahlert J, Sørensen HT, Pedersen L. Sampling strategies for selecting general population comparison cohorts. Clin Epidemiol. 2018;10:1325–1337. doi:10.2147/CLEP.S164456
24. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
25. Lindenstrøm E, Boysen G, Waage Christiansen L, Rogvi Hansen B, Würtzen Nielsen P. Reliability of Scandinavian neurological stroke scale. Cerebrovasc Dis. 1991;1(2):103–107. doi:10.1159/000108825
26. Knol MJ, Vanderweele TJ. Recommendations for presenting analyses of effect modification and interaction. Int J Epidemiol. 2012;41(2):514–520. doi:10.1093/ije/dyr218
27. Vanderweele TJ. On the distinction between interaction and effect modification. Epidemiology. 2009;20(6):863–871. doi:10.1097/EDE.0b013e3181ba333c
28. VanderWeele TJ, Tchetgen Tchetgen EJ. Attributing Effects to Interactions. Epidemiology. 2014;25(5):711–722. doi:10.1097/EDE.0000000000000096
29. Benchimol EI, Smeeth L, Guttmann A, et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015;12(10):e1001885. doi:10.1371/journal.pmed.1001885
30. Pouwels S, Lalmohamed A, Leufkens B, et al. Risk of hip/femur fracture after stroke. Stroke. 2009;40(10):3281–3285. doi:10.1161/STROKEAHA.109.554055
31. Winstein CJ, Stein J, Arena R, et al. Guidelines for adult stroke rehabilitation and recovery. Stroke. 2016;47(6):e98–e169. doi:10.1161/STR.0000000000000098
32. Carda S, Cisari C, Invernizzi M, Bevilacqua M. Osteoporosis after stroke: a review of the causes and potential treatments. Cerebrovasc Dis. 2009;28(2):191–200. doi:10.1159/000226578
33. Poole KES, Reeve J, Warburton EA. Falls, fractures, and osteoporosis after stroke. Stroke. 2002;33(5):1432–1436. doi:10.1161/01.STR.0000014510.48897.7D
34. Lawrence VA, Hilsenbeck SG, Noveck H, Poses RM, Carson JL. Medical complications and outcomes after hip fracture repair. Arch Intern Med. 2002;162(18):2053–2057. doi:10.1001/archinte.162.18.2053
35. Hjelholt TJ, Edwards NM, Vesterager JD, Kristensen PK, Pedersen AB. The positive predictive value of hip fracture diagnoses and surgical procedure codes in the Danish multidisciplinary hip fracture registry and the Danish National Patient Registry. Clin Epidemiol. 2020;12:123–131. doi:10.2147/CLEP.S238722
36. Thygesen SK, Christiansen CF, Christensen S, Lash TL, Sorensen HT. The predictive value of ICD-10 diagnostic coding used to assess Charlson comorbidity index conditions in the population-based Danish National Registry of Patients. BMC Med Res Methodol. 2011;11:83. doi:10.1186/1471-2288-11-83
37. Hjelholt TJ, Johnsen SP, Brynningsen PK, Pedersen AB. Association of CHA2 DS2 -VASc score with stroke, thromboembolism, and death in hip fracture patients. J Am Geriatr Soc. 2020;68(8):1698–1705. doi:10.1111/jgs.16452
38. Hjelholt TJ, Johnsen SP, Brynningsen PK, Knudsen JS, Prieto-Alhambra D, Pedersen AB. Development and validation of a model for predicting mortality in patients with hip fracture. Age Ageing. 2022;51(1). doi:10.1093/ageing/afab233
39. Ludvigsson J, Håberg S, Knudsen GP, et al.. Ethical aspects of registry-based research in the Nordic countries. Clin Epidemiol. 2015;491. doi:10.2147/CLEP.S90589
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.