")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
The Impact of Intermittent Fasting on Non-Alcoholic Fatty Liver Disease in Older Adults: A Review of Clinicaltrials.gov Registry
Received 15 July 2023
Accepted for publication 30 September 2023
Published 6 October 2023 Volume 2023:16 Pages 3115—3121
DOI https://doi.org/10.2147/DMSO.S430740
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Konstantinos Tziomalos
Nasser M Alorfi, Ahmed M Ashour
Pharmacology and Toxicology Department, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Nasser M Alorfi, Email [email protected]
Background: Non-alcoholic fatty liver disease (NAFLD) is a predominant health condition across the world due to its rising prevalence and association with various metabolic disorders. Intermittent fasting (IF) has attracted increasing attention as a dietary approach to addressing weight management and enhancing metabolic well-being, and its potential effects on NAFLD have been a topic of growing research interest.
Aim: This review aims to critically evaluate the current evidence on IF’s impact on NAFLD, including the mechanisms underlying the observed effects in older adults (65+).
Methods: A comprehensive search of Clinicaltrials.gov was conducted to identify relevant studies that investigated the effects of IF on NAFLD in older adults (65+). Data on study design, sample size, intervention details, and outcomes related to NAFLD were extracted and analyzed.
Results: As of April 12th, 2023, there were 1304 clinical trials on NAFLD. Most of these were interventional studies. The investigation focused on completed studies and found that limited clinical trials were identified with limited interventional measures. Only five out of the 1304 studies on NAFLD involved IF. Basic and advanced outcome measures were examined.
Conclusion: Although some studies suggest that IF may have potential benefits for NAFLD, the evidence is still limited and inconclusive.
Keywords: hepatology, intermittent fasting, metabolic disease, lifestyles, clinical trials
Introduction
Non-alcoholic fatty liver disease (NAFLD) is an escalating and concerning global health issue, and its incidence has undergone a substantial rise in the recent past. A recent meta-analysis study estimated that by the year 2040, more than 50% of the adult population would be diagnosed with NAFLD.1 NAFLD refers to the accumulation of hepatic steatosis in individuals who consume little or no alcohol.2 It encompasses a continuum of hepatic disorders spanning from uncomplicated fatty liver (steatosis) to non-alcoholic steatohepatitis (NASH), the latter holding the potential to advance to cirrhosis and, in more severe cases, hepatocellular carcinoma (HCC).3 The exact pathophysiology of NAFLD is complex and multifactorial, involving a combination of genetic, metabolic, and environmental factors.4 Resistance to insulin is a key characteristic of NAFLD;5 this induces heightened lipolysis within adipose tissue, consequently amplifying the transportation of free fatty acids to the liver, precipitating hepatic steatosis6 Over an extended duration, hepatic steatosis may advance to NASH, characterized by inflammatory processes, hepatocellular damage, and fibrotic changes, potentially culminating in cirrhosis and the development of HCC.7 NAFLD is often asymptomatic in its early stages and is incidentally detected during routine blood tests or imaging studies.8,9 Numerous factors can increase the risk of developing NAFLD. Obesity, especially visceral adiposity, is a significant risk factor for NAFLD, due to its propensity to cause insulin resistance and a rise in the release of free fatty acids from adipose tissue.10,11 NAFLD is also associated with several other risk factors, including metabolic syndrome, dyslipidemia, and Type 2 diabetes.12,13 Other risk factors include a sedentary lifestyle, poor diet, rapid weight loss and polycystic ovary syndrome (PCOS).14–16 Various researchers have reported that fasting may lead to improvements in liver function, potentially indicating a reduction in liver fat accumulation or inflammation.17–20 Additionally, total cholesterol levels, which are known to be associated with NAFLD, may also improve during this fasting period.
The management of NAFLD involves a combination of lifestyle modifications, pharmacotherapy, and addressing the underlying risk factors.21 A recommended method for the management of the disease is losing weight by exercising, changing diet, and changing behaviour.22 Liver histology is reported to improve when losing >10% of total body weight, and the risk of disease progression decreases.23 As part of the management of NAFLD, it is recommended that a patients follow a well-balanced and calorie-restricted diet. This diet should emphasize a reduction in the intake of refined carbohydrates, saturated fats, and added sugars, while consuming more healthy fats, wholegrains, fruits and vegetables, and lean proteins.17,24
Moreover, numerous pharmacological agents have undergone scrutiny in the pursuit of effective interventions for the management of NAFLD. Although there is no specific FDA-approved medication for NAFLD, some medications have shown promise in certain situations. For example, NASH patients taking vitamin E, particularly those without diabetes, have been reported to show improved liver histology, although its long-term safety and efficacy need further evaluation.25–27 Studies on Pioglitazone, a thiazolidinedione, have shown that it can lead to improvements in liver histology in patients with concurrent diabetes and NASH.28–30 However, its utilization should be cautiously weighed, taking into account potential adverse effects such as an increase in weight, retention of fluid, and a greater risk of heart failure.29,31 Other pharmacological interventions, including statins, ursodeoxycholic acid, and obeticholic acid, are currently under investigation for their potential therapeutic role in the management of NAFLD.32,33 Furthermore, incretin mimetics (glucagon-like peptide-1 (GLP-1) receptor agonists), have been reported to be a potentially valuable therapeutic option for patients with fatty liver disease, NAFLD in particular.34,35 They reduce the accumulation of fat in the liver, as well as inflammation and fibrosis in these patients.36,37
Numerous researchers have explored the impact of IF on NAFLD utilizing both animal models and human participants. Findings from animal studies have demonstrated that IF possesses the capacity to mitigate hepatic steatosis, inflammatory responses, and fibrosis across a spectrum of NAFLD animal models.38–40 Promising results have also been published on how IF can positively impact NAFLD. A clinical study by Badran et al conducted with 98 NAFLD patients demonstrated that IF led to significant and noteworthy improvements in the ultrasonographic, biochemical, and anthropometric parameters associated with NAFLD, particularly in the early phases of the condition and among individuals at risk of developing diabetes.19 Another study by Faris et al found that Ramadan IF induced significant but subtle changes in liver function tests with aspartate transaminase, alkaline phosphatase and bilirubin demonstrating minor yet noteworthy enhancements, and gamma glutamyl transpeptidase exhibiting a more moderate improvement.18
Intermittent fasting holds paramount importance for older patients as it offers a multifaceted approach to addressing common age-related health challenges. It can improve metabolic health by enhancing insulin sensitivity and aiding weight management, crucial factors in preventing and managing conditions like diabetes and cardiovascular disease.41,42 This study will review and assess the impact of IF on NAFLD in older adults using data extracted from the ClinicalTrials.gov registry.
Methods
Search Strategy
On April 12th, 2023, ClinicalTrials.gov was searched for relevant studies, using the single search term “NAFLD” for the disease/condition, in conjunction with “intermittent fasting”.
Review Search Results
The identification of relevant clinical trials was based on the following inclusion and exclusion criteria: the inclusion criteria included NAFLD clinical trials that used IF as an observational measure, and other clinical trials were excluded.
Extracted Data
Data such as study title, study status, study type, intervention details, and outcome were extracted from the database.
Results
Number of Studies Returned by the Search
On April 12th, 2023, a total of 1304 clinical trials related to NAFLD were identified in the ClinicalTrial.gov registry. Only five studies included IF as an intervention.
Characteristics of the Clinical Trials
These five clinical trials examined mainly NAFLD along with obesity, diabetes mellitus, insulin resistance and gut microbiota. They included a total of 325 participants. The full details are shown in Table 1.
 |
Table 1 Characteristics of the Clinical Trials (from ClinicalTrials.gov 12.04.2023) |
Outcome Measures
Most of the clinical trials focused on taking basic measurements such as liver fat content, visceral adipose tissue content, dietary intake, body weight, blood glucose, fasting blood glucose, HbA1c levels, liver enzymes levels, total cholesterol, and triglyceride. The full list is provided in Table 2.
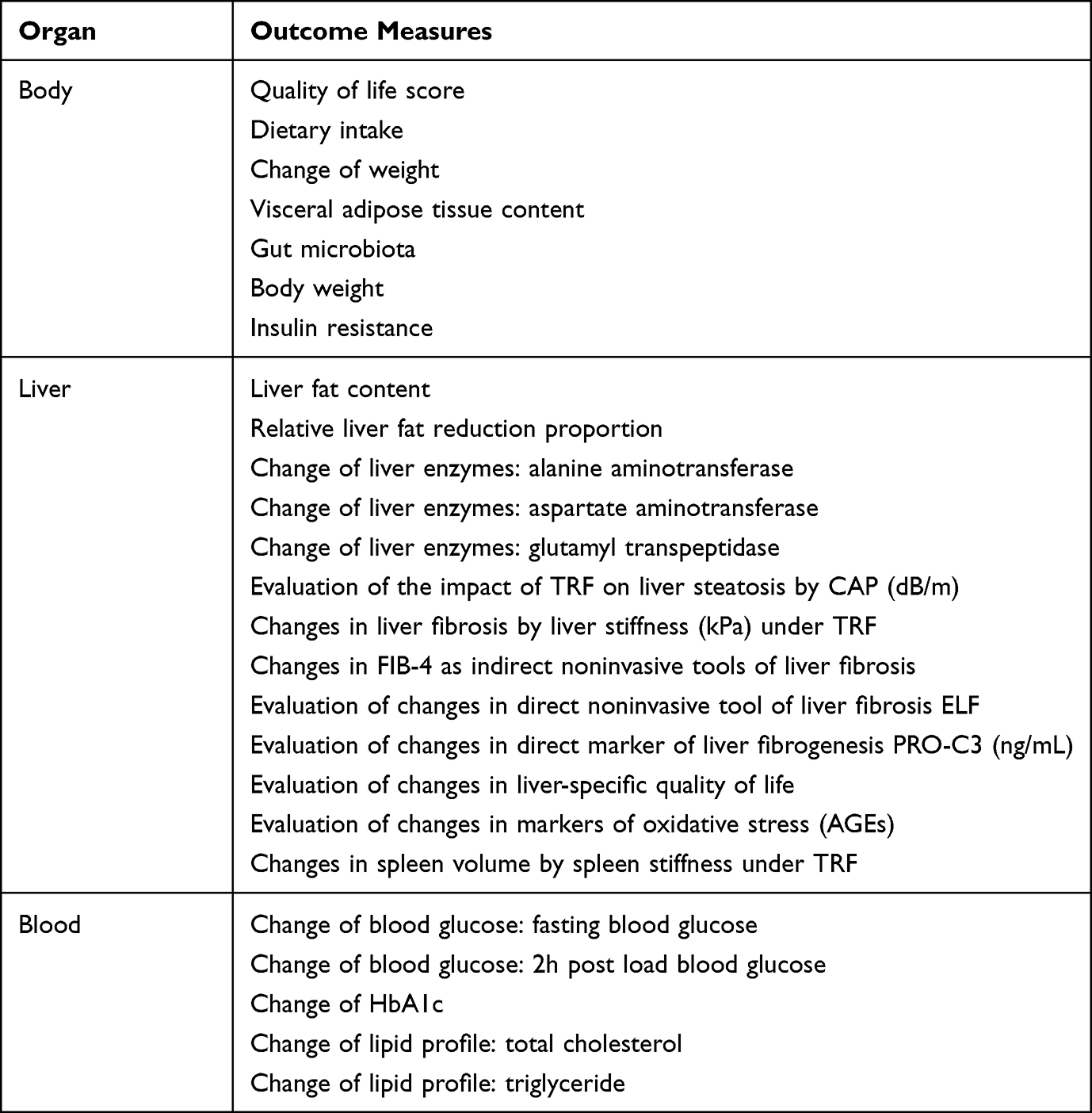 |
Table 2 Outcome Measures with NAFLD Using if |
Discussion
NAFLD is a prevalent liver disorder marked by excessive accumulation of fat in the liver, without excessive alcohol intake. NAFLD has a close link to obesity, insulin resistance, dyslipidemia, and other components of metabolic syndrome, and it has been subject to thorough investigation through clinical trials. In recent times, there has been a burgeoning interest in evaluating the prospective influence of IF on NAFLD, prompting the utilization of diverse approaches and methodologies to scrutinize IF’s impact on this ailment. Lifestyle modifications play a crucial role in the management of NAFLD.18 IF is a dietary regimen characterized by alternating periods of fasting and feeding. It encompasses diverse patterns such as time-restricted feeding, alternate day fasting, and periodic fasting practices, such as those observed during Ramadan.43,44
The main premise of IF is to create periods of energy restriction, which can lead to changes in metabolism and cellular responses, and potentially impact the development and progression of NAFLD.45 The mechanisms through which IF may impact NAFLD are complex and yet to be understood in full, but scholars have proposed a number of potential mechanisms. One of the most prominent of these is through improved glucose homeostasis and sensitivity to insulin. Intermittent fasting can induce changes in insulin signaling pathways, leading to improved insulin sensitivity, reduced hepatic gluconeogenesis, and increased glucose uptake in peripheral tissues, which may help to reduce hepatic fat accumulation. A study conducted by Gnanou et al demonstrated that Ramadan fasting in young, healthy individuals positively influences glucose homeostasis maintenance, accompanied by a reduction in adiponectin levels and significant weight loss.46 Another study on 27 healthy male participants found that IF practiced during Ramadan yielded favorable effects by enhancing insulin sensitivity, as well as promoting beneficial outcomes related to weight and fat reduction.20 The key factor underlying the metabolic alterations in adipose tissue during fasting is most likely a decrease in insulin signaling. Another potential mechanism is the modulation of lipid metabolism.47 IF can lead to changes in lipid metabolism, including increased lipolysis, reduced lipogenesis, and increased β-oxidation of fatty acids, which can lead to a decrease in hepatic fat content.48,49 Additionally, IF can affect the gut microbiota, leading to changes in bile acid metabolism, which can impact lipid metabolism and hepatic steatosis.50 Furthermore, IF has been shown to induce autophagy.51 The activation of autophagy, which results in the reduction of hepatic triglyceride levels and improved liver function, holds potential as a therapeutic approach for treating NAFLD through the use of autophagy regulators.51–53 Moreover, IF has been shown to modulate oxidative stress and inflammation,54 which are both key contributors to the pathogenesis of NAFLD.55 Furthermore, IF has demonstrated its capacity to modulate oxidative stress and liver inflammation. A small body of research has indicated that IF may diminish indicators of oxidative stress, including reactive oxygen species (ROS) and malondialdehyde (MDA), while concurrently augmenting the activity of antioxidant enzymes such as superoxide dismutase (SOD) and glutathione peroxidase (GPx) in the liver. This, in turn, has the potential to alleviate oxidative stress.56,57 In addition, it has been shown that fasting during can decrease hepatic inflammation by reducing the levels of pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6), and by increasing the levels of anti-inflammatory cytokines such as interleukin-10 (IL-10).58,59
Conclusion
The studies in this review demonstrate that IF positively affects NAFLD through a number of different physiological pathways. These include improved insulin sensitivity and glucose homeostasis, modulation of lipid metabolism, induction of autophagy, modulation of oxidative stress and inflammation, and modulation of gut microbiota. However, it should be noted that the mechanisms underlying the effects of IF on NAFLD are complex and may involve other pathways as well.
However, it is crucial to acknowledge that the clinical evidence for IF in the context of NAFLD remains relatively sparse. Many of the existing studies are small in scale and lack long-term follow-up, making it challenging to draw decisive conclusions about its safety and efficacy. Additionally, the outcomes of these studies can vary widely depending on the specific fasting regimen employed, making it difficult to establish standardized guidelines for NAFLD management. Future research should be conducted to fully clarify the underlying mechanisms and to determine the optimal regimen of IF for the management of NAFLD. It should be noted that patients are strongly advised to consult with a healthcare professional before engaging in IF.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nguyen MH, Le MH, Yeo YH, et al. Forecasted 2040 global prevalence of nonalcoholic fatty liver disease using hierarchical bayesian approach. Clin Mol Hepatol. 2022;28(4):841. doi:10.3350/CMH.2022.0239
2. Smith BW, Adams LA. Non-alcoholic fatty liver disease. Crit Rev Clin Lab Sci. 2011;48(3):97–113. doi:10.3109/10408363.2011.596521
3. Burt AD, Lackner C, Tiniakos DG. Diagnosis and assessment of NAFLD: definitions and histopathological classification. Semin Liver Dis. 2015;35(03):207–220. doi:10.1055/S-0035-1562942/ID/JR00799-35
4. Carr RM, Oranu A, Khungar V. Non-alcoholic fatty liver disease: pathophysiology and management. Gastroenterol Clin North Am. 2016;45(4):639. doi:10.1016/J.GTC.2016.07.003
5. Utzschneider KM, Kahn SE. The role of insulin resistance in nonalcoholic fatty liver disease. J Clin Endocrinol Metab. 2006;91(12):4753–4761. doi:10.1210/JC.2006-0587
6. Kitade H, Chen G, Ni Y, Ota T. Nonalcoholic fatty liver disease and insulin resistance: new insights and potential new treatments. Nutrients. 2017;9(4):387. doi:10.3390/NU9040387
7. Mooli RGR, Ramakrishnan SK. Liver steatosis is a driving factor of inflammation. Cell Mol Gastroenterol Hepatol. 2022;13(4):1267. doi:10.1016/J.JCMGH.2022.01.007
8. Muhammad A. Non-alcoholic fatty liver disease, an overview. Integr Med a Clin J. 2019;18:42.
9. Muthiah MD, Cheng Han N, Sanyal AJ. A clinical overview of non-alcoholic fatty liver disease: a guide to diagnosis, the clinical features, and complications—what the non-specialist needs to know. Diabetes Obes Metab. 2022;24(S2):3–14. doi:10.1111/DOM.14521
10. Mirza MS. Obesity, visceral fat, and NAFLD: querying role of adipokines in the progression of nonalcoholic fatty liver disease. ISRN Gastroenterol. 2011;2011:1–11. doi:10.5402/2011/592404
11. Chung GE, Oh S, Ahn DW, et al. Effects of additive interactions among obesity, visceral adiposity, and sarcopenia on nonalcoholic fatty liver disease. Sci Rep. 2023;13:1–8. doi:10.1038/s41598-023-30833-3
12. Matsuzaka T, Shimano H. New perspective on type 2 diabetes, dyslipidemia and non‐alcoholic fatty liver disease. J Diabetes Investig. 2020;11(3):532. doi:10.1111/JDI.13258
13. Dharmalingam M, Yamasandhi PG. Nonalcoholic fatty liver disease and type 2 diabetes mellitus. Indian J Endocrinol Metab. 2018;22(3):421. doi:10.4103/IJEM.IJEM_585_17
14. Vassilatou E. Nonalcoholic fatty liver disease and polycystic ovary syndrome. World J Gastroenterol. 2014;20(26):8351. doi:10.3748/WJG.V20.I26.8351
15. Kelley CE, Brown AJ, Diehl AM, Setji TL. Review of nonalcoholic fatty liver disease in women with polycystic ovary syndrome. World J Gastroenterol. 2014;20(39):14172. doi:10.3748/WJG.V20.I39.14172
16. Tsai JH, Ferrell LD, Tan V, Yeh MM, Sarkar M, Gill RM. Aggressive non-alcoholic steatohepatitis following rapid weight loss and/or malnutrition. Mod Pathol. 2017;30(6):834. doi:10.1038/MODPATHOL.2017.13
17. Aliasghari F, Izadi A, Gargari BP, Ebrahimi S. The effects of ramadan fasting on body composition, blood pressure, glucose metabolism, and markers of inflammation in NAFLD patients: an observational trial. J Am Coll Nutr. 2017;36(8):640–645. doi:10.1080/07315724.2017.1339644
18. Faris MAI, Jahrami H, Abdelrahim D, Bragazzi N, BaHammam A. The effects of ramadan intermittent fasting on liver function in healthy adults: a systematic review, meta-analysis, and meta-regression. Diabetes Res Clin Pract. 2021;178:108951. doi:10.1016/J.DIABRES.2021.108951
19. Badran H, Elsabaawy M, Sakr A, et al. Impact of Intermittent fasting on laboratory, radiological, and anthropometric parameters in NAFLD patients. Clin Exp Hepatol. 2022;8(2):118. doi:10.5114/CEH.2022.115056
20. Prasetya G, Sapwarobol S. Intermittent fasting during ramadan improves insulin sensitivity and anthropometric parameters in healthy young Muslim men. Am J Lifestyle Med. 2018;15(2):200–206. doi:10.1177/1559827618815430
21. Arab JP, Candia R, Zapata R, et al. Management of nonalcoholic fatty liver disease: an evidence-based clinical practice review. World J Gastroenterol. 2014;20(34):12182. doi:10.3748/WJG.V20.I34.12182
22. Papandreou D, Andreou E. Role of diet on non-alcoholic fatty liver disease: an updated narrative review. World J Hepatol. 2015;7(3):575. doi:10.4254/WJH.V7.I3.575
23. Glass LM, Dickson RC, Anderson JC, et al. Total body weight loss of ≥ 10 % is associated with improved hepatic fibrosis in patients with nonalcoholic steatohepatitis. Dig Dis Sci. 2015;60(4):1024–1030. doi:10.1007/S10620-014-3380-3
24. Kargulewicz A, Stankowiak-Kulpa H, Grzymisałwski M. Dietary recommendations for patients with nonalcoholic fatty liver disease. Przeglad Gastroenterol. 2014;9:18. doi:10.5114/PG.2014.40845
25. Amanullah I, Khan YH, Anwar I, Gulzar A, Mallhi TH, Raja AA. Effect of vitamin e in non-alcoholic fatty liver disease: a systematic review and meta-analysis of randomised controlled trials. Postgrad Med J. 2019;95(1129):601–611. doi:10.1136/POSTGRADMEDJ-2018-136364
26. El Hadi H, Vettor R, Rossato M. Vitamin E as a treatment for nonalcoholic fatty liver disease: reality or myth? Antioxidants. 2018;7(1). doi:10.3390/ANTIOX7010012
27. Bril F, Biernacki DM, Kalavalapalli S, et al. Role of vitamin E for nonalcoholic steatohepatitis in patients with type 2 diabetes: a randomized controlled trial. Diabetes Care. 2019;42(8):1481–1488. doi:10.2337/DC19-0167
28. Della Pepa G, Russo M, Vitale M, et al. Pioglitazone even at low dosage improves NAFLD in type 2 diabetes: clinical and pathophysiological insights from a subgroup of the TOSCA. IT randomised trial. Diabetes Res Clin Pract. 2021;178:108984. doi:10.1016/J.DIABRES.2021.108984
29. Blazina I, Selph S. Diabetes drugs for nonalcoholic fatty liver disease: a systematic review. Syst Rev. 2019;8(1):1–13. doi:10.1186/S13643-019-1200-8/TABLES/4
30. Wise J. Pioglitazone seems safe and effective for patients with fatty liver disease and diabetes. BMJ. 2016;353. doi:10.1136/BMJ.I3435
31. Lian J, Fu J. Pioglitazone for NAFLD patients with prediabetes or type 2 diabetes mellitus: a meta-analysis. Front Endocrinol. 2021;12. doi:10.3389/FENDO.2021.615409
32. Kulkarni AV, Tevethia HV, Arab JP, et al. Efficacy and safety of obeticholic acid in liver disease—a systematic review and meta-analysis. Clin Res Hepatol Gastroenterol. 2021;45(3):101675. doi:10.1016/J.CLINRE.2021.101675
33. Makri E, Cholongitas E, Tziomalos K. Emerging role of obeticholic acid in the management of nonalcoholic fatty liver disease. World J Gastroenterol. 2016;22(41):9039. doi:10.3748/WJG.V22.I41.9039
34. Alorfi NM, Algarni AS. Clinical impact of semaglutide, a glucagon-like peptide-1 receptor agonist, on obesity management: a review. Clin Pharmacol. 2022;14:61–67. doi:10.2147/CPAA.S374741
35. Nevola R, Epifani R, Imbriani S, et al. GLP-1 receptor agonists in non-alcoholic fatty liver disease: current evidence and future perspectives. Int J Mol Sci. 2023;24(2):24. doi:10.3390/IJMS24021703
36. Mantovani A, Targher G. Glucagon-like peptide-1 receptor agonists for treatment of nonalcoholic steatohepatitis: new insights from subcutaneous semaglutide. Hepatobiliary Surg Nutr. 2021;10(4):518. doi:10.21037/HBSN-2021-13
37. Wong C, Lee MH, Yaow CYL, et al. Glucagon-like peptide-1 receptor agonists for non-alcoholic fatty liver disease in type 2 diabetes: a meta-analysis. Front Endocrinol. 2021;12:609110. doi:10.3389/FENDO.2021.609110/BIBTEX
38. Zhao J, Bai M, Wei S, Li C, Lv Q, Chen Y. Improvement of non-alcoholic fatty liver disease in mice by intermittent use of a fasting-mimicking diet. Mol Nutr Food Res. 2021;65(23). doi:10.1002/MNFR.202100381
39. Memel ZN, Wang J, Corey KE. Intermittent fasting as a treatment for nonalcoholic fatty liver disease: what is the evidence? Clin Liver Dis. 2022;19(3):101. doi:10.1002/CLD.1172
40. Xu Z, Qin Y, Lv B, Tian Z, Zhang B. Intermittent fasting improves high-fat diet-induced obesity cardiomyopathy via alleviating lipid deposition and apoptosis and decreasing M6A Methylation in the heart. Nutrients. 2022;14. doi:10.3390/NU14020251
41. Yuan X, Wang J, Yang S, et al. Effect of intermittent fasting diet on glucose and lipid metabolism and insulin resistance in patients with impaired glucose and lipid metabolism: a systematic review and meta-analysis. Int J Endocrinol. 2022;2022:1–9. doi:10.1155/2022/6999907
42. Teong XT, Liu K, Vincent AD, et al. Intermittent fasting plus early time-restricted eating versus calorie restriction and standard care in adults at risk of type 2 diabetes: a randomized controlled trial. Nat Med. 2023;29(4):963–972. doi:10.1038/s41591-023-02287-7
43. Vasim I, Majeed CN, DeBoer MD. Intermittent fasting and metabolic health. Nutrients. 2022;14(3):631. doi:10.3390/NU14030631
44. Ravussin E, Gilmore LA, Redman LM. Calorie restriction in humans: impact on human health. Mol Basis Nutr Aging a Vol Mol Nutr Ser. 2016;677–692. doi:10.1016/B978-0-12-801816-3.00048-0
45. Rynders CA, Thomas EA, Zaman A, Pan Z, Catenacci VA, Melanson EL. Effectiveness of intermittent fasting and time-restricted feeding compared to continuous energy restriction for weight loss. Nutrients. 2019;11(10):2442. doi:10.3390/NU11102442
46. Gnanou JV, Caszo BA, Khalil KM, Abdullah SL, Knight VF, Bidin MZ. Effects of ramadan fasting on glucose homeostasis and adiponectin levels in healthy adult males. J Diabetes Metab Disord. 2015;14(1). doi:10.1186/S40200-015-0183-9
47. Antoni R, Johnston KL, Collins AL, Robertson MD. Effects of intermittent fasting on glucose and lipid metabolism. Proc Nutr Soc. 2017;76(3):361–368. doi:10.1017/S0029665116002986
48. Ebrahimi S, Gargari BP, Aliasghari F, Asjodi F, Izadi A. Ramadan fasting improves liver function and total cholesterol in patients with nonalcoholic fatty liver disease. Int J Vitam Nutr Res. 2020;90(1–2):95–102. doi:10.1024/0300-9831/A000442
49. Kersten S. The impact of fasting on adipose tissue metabolism. Biochim Biophys Acta Mol Cell Biol Lipids. 2023;1868(3):159262. doi:10.1016/J.BBALIP.2022.159262
50. Khan MN, Khan SI, Rana MI, Ayyaz A, Khan MY, Imran M. Intermittent fasting positively modulates human gut microbial diversity and ameliorates blood lipid profile. Front Microbiol. 2022;13:2931. doi:10.3389/FMICB.2022.922727/BIBTEX
51. Lavallee CM, Bruno A, Ma C, Raman M. The role of intermittent fasting in the management of nonalcoholic fatty liver disease: a narrative review. Nutr. 2022;14:4655. doi:10.3390/NU14214655
52. Khambu B, Yan S, Huda N, Liu G, Yin XM. Autophagy in non-alcoholic fatty liver disease and alcoholic liver disease. Liver Res. 2018;2(3):112–119. doi:10.1016/J.LIVRES.2018.09.004
53. Urooj A, Kotebagilu NP, Shivanna LM, Anandan S, Thantry AN, Siraj SF. Effect of ramadan fasting on body composition, biochemical profile, and antioxidant status in a sample of healthy individuals. Int J Endocrinol Metab. 2020;18(4):107641. doi:10.5812/IJEM.107641
54. Yin C, Li Z, Xiang Y, et al. Effect of intermittent fasting on non-alcoholic fatty liver disease: systematic review and meta-analysis. Front Nutr. 2021;8:709683. doi:10.3389/FNUT.2021.709683/FULL
55. Monserrat-Mesquida M, Quetglas-Llabrés M, Abbate M, et al. Oxidative stress and pro-inflammatory status in patients with non-alcoholic fatty liver disease. Antioxidants. 2020;9(8):1–16. doi:10.3390/ANTIOX9080759
56. Hardiany NS, Karman AP, Calista ASP, et al. The effect of fasting on oxidative stress in the vital organs of New Zealand white rabbit. Reports Biochem Mol Biol. 2022;11:190. doi:10.52547/RBMB.11.2.190
57. Mohr AE, McEvoy C, Sears DD, Arciero PJ, Sweazea KL. Impact of intermittent fasting regimens on circulating markers of oxidative stress in overweight and obese humans: a systematic review of randomized controlled trials. Adv Redox Res. 2021;3:100026. doi:10.1016/J.ARRES.2021.100026
58. Faris MAIE, Kacimi S, Al-Kurd RA, et al. Intermittent fasting during ramadan attenuates proinflammatory cytokines and immune cells in healthy subjects. Nutr Res. 2012;32(12):947–955. doi:10.1016/J.NUTRES.2012.06.021
59. Mushtaq R, Akram A, Mushtaq R, Khwaja S, Ahmed S. The role of inflammatory markers following ramadan fasting. Pakistan J Med Sci. 2019;35:77. doi:10.12669/PJMS.35.1.95
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.