Back to Journals » Journal of Pain Research » Volume 16
The Impact of Hot Spring Hydrotherapy on Pain Perception and Dysfunction Severity in Patients with Chronic Low Back Pain: A Systematic Review and Meta-Analysis
Authors Mao S ![]() , Xiao K, Zhou W, Xu H, Zhang S
, Xiao K, Zhou W, Xu H, Zhang S ![]()
Received 7 October 2023
Accepted for publication 8 November 2023
Published 16 November 2023 Volume 2023:16 Pages 3925—3944
DOI https://doi.org/10.2147/JPR.S438744
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Sujie Mao,1 Kaiwen Xiao,1 Wensheng Zhou,2 Hong Xu,3 Shikun Zhang4
1Discipline Construction Office, Nanjing Sport Institute, NanJing, Jiangsu, People’s Republic of China; 2Department of Physical Education, Jiangsu Second Normal University, Nanjing, JiangSu, People’s Republic of China; 3Department of Physical Education, Nanjing Xiao-Zhuang University, Nanjing, JiangSu, People’s Republic of China; 4Department of Police Physical Education, Jiangsu Police Institute, Nanjing, JiangSu, People’s Republic of China
Correspondence: Shikun Zhang, Department of Police Physical Education, Jiangsu Police Institute, No. 48 Sangong, Shifo Temple, Pukou District, Nanjing, Jiangsu Province, People’s Republic of China, Email [email protected]
Background: Chronic Low Back Pain (CLBP) is a prevalent global health issue, leading to prolonged discomfort and functional limitations. Hot spring hydrotherapy, which utilizes mineral-rich, warm spring water, offers a unique physical therapy that holds promise in alleviating CLBP symptoms.
Objective: This meta-analysis aims to assess the effectiveness of hot spring hydrotherapy in improving CLBP symptoms, encompassing pain intensity, functional disability, quality of life, and medication usage.
Methods: A systematic review and meta-analysis were conducted by searching relevant literature in multiple databases. Included studies compared hot spring hydrotherapy with control interventions or other treatments. Standardized mean differences (SMD) with 95% confidence intervals (CI) were calculated for pain intensity, functional disability, medication usage, and quality of life.
Results: A total of 16 studies met the inclusion criteria, involving 1656 participants with chronic low back pain across various countries. The meta-analysis demonstrated that hot spring hydrotherapy was effective in reducing pain intensity (SMD = − 0.901, 95% CI [− 1.777, − 0.025], P < 0.05) and improving functional disability (SMD = − 3.236, 95% CI [− 4.898, − 1.575], P < 0.0001) in CLBP patients. Hot spring hydrotherapy also resulted in a significant reduction in medication usage (P < 0.05). Subgroup analysis showed that the effects of hot spring hydrotherapy were more pronounced in patients aged 60 and above, while no significant differences were observed in patients below 60 years of age, single hot Spring Hydrotherapy help improve patients’ quality of life.
Conclusion: Hot spring hydrotherapy is an effective intervention for improving CLBP symptoms, including pain intensity, functional disability, and medication usage. It is particularly beneficial for CLBP patients aged 60 and above. These findings support the integration of hot spring hydrotherapy into the treatment approach for CLBP, although further research is needed to determine its efficacy in younger patients and to explore the underlying mechanisms of its therapeutic effects.
Prospero Id: CRD42023430860.
Keywords: hydrotherapy, visual analog scale, impaired physical function, quality of life
Introduction
Chronic Low Back Pain (CLBP) is a persistent or recurring pain that extends from the lower edge of the rib cage to the baseline of the buttocks, with the pain duration being relatively long, and the course of the disease exceeding three months. It is a common type of lower back pain.1,2 CLBP patients usually suffer from persistent pain, muscle stiffness, joint movement limitations, and functional disorders, which severely affect the quality of life and work capacity.3 According to the Global Burden of Disease Study, chronic low back pain is one of the diseases that causes the most disability worldwide.4 The World Health Organization (WHO) estimates that about 60%-70% of adults worldwide experience low back pain at least once in their lives, and approximately 10% of people may develop chronic low back pain.5 Moreover, the recurrence rate of this disease is quite high, with 40%-50% of patients relapsing within a year.6 It not only has a profound impact on patients’ health but also puts tremendous pressure on the global healthcare system and workforce productivity. Therefore, seeking effective treatment and prevention strategies for chronic low back pain has become particularly important.
There are various ways to treat CLBP, aiming to alleviate pain, improve function, and enhance quality of life. Clinically, surgical treatment, drug therapy, and physical therapy methods are usually adopted to alleviate the symptoms related to CLBP.7 However, surgical treatment of CLBP is often accompanied by surgery-related complications, a long postoperative recovery period, and the risk of postoperative recurrence;8 prolonged medication use may lead patients to develop drug dependence and resistance, causing the effect of the drugs to gradually weaken. Furthermore, medications can typically only relieve pain and do not address the cause of low back pain.9 Therefore, patients may also opt for physical therapy to improve and recover from CLBP. This primarily includes methods such as exercise therapy, hot and cold compresses, massage, and traction.10
Hot spring hydrotherapy is a form of physical therapy that uses the unique therapeutic properties of natural hot spring water, including its mineral content and temperature, for physical and mental recuperation, offering a method of relief and recovery. It utilizes the physical properties of the hot spring (temperature, water flow, and buoyancy) to improve disease symptoms and promote recovery in CLBP patients.11 It is often used to relieve pain, reduce inflammation, relax muscles, increase blood circulation, and promote recovery. By soaking in hot spring water, undergoing hot spring jetting, and exercising in hot spring water, hot spring hydrotherapy can provide a unique physical therapy that helps to improve symptoms and functional disorders of diseases like chronic lower back pain.12 A large number of studies have shown that hot spring hydrotherapy can effectively improve the relevant symptoms of CLBP patients and can play an important role in their recovery.13–15 A past meta-analysis also indicated that hot spring hydrotherapy can effectively improve pain, relieve patient disability, enhance lumbar function, and increase joint mobility.16
However, there is some controversy regarding the effects of hot spring hydrotherapy on CLBP, including differences in the effects of interventions on patients of different age groups,17 whether singular hot spring hydrotherapy has a significant effect, and whether it needs to be combined with other treatments for better results.18 Whether hydrotherapy can improve functional disorders beyond pain is also in question, so there is much uncertainty about the impact of hot spring hydrotherapy on CLBP. This study conducts a systematic review and meta-analysis of randomized controlled trials of hot spring hydrotherapy for CLBP by searching through five databases, aiming to better evaluate and understand the mechanism of action and therapeutic effects of hot spring hydrotherapy on CLBP.
Methods
This systematic review and meta-analysis were conducted following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline19 and is registering in the International Prospective Register of Systematic Reviews (PROSPERO ID: CRD42023430860). Annex 1 contains the PRISMA 2009 checklist in PDF format.
Eligibility Criteria
Study Inclusion and Exclusion Criteria
Inclusion Criteria
The meta-analysis included studies that involved patients with a confirmed diagnosis of chronic low back pain lasting more than 12 weeks.
Exclusion Criteria
Patients with osteoporosis, severe comorbidities, significant physical immobility, and a history of previous spinal surgery were excluded from the study to ensure the homogeneity of the participant population.
Types of Studies
The meta-analysis included only high-quality randomized controlled trials (RCTs) to provide reliable evidence on the effectiveness of hot spring hydrotherapy for chronic low back pain.
Participant Characteristics
The participants in the included studies were adult individuals (age range not specified) who had been diagnosed with chronic low back pain, regardless of gender or other demographic factors.
Intervention and Comparison
The intervention of interest was hot spring hydrotherapy, which involved immersing patients in natural hot spring water as a therapeutic measure for chronic low back pain. The comparison group consisted of individuals who did not receive any form of spa intervention.
Outcome Measures
The outcome measures assessed in the included studies varied and may include pain intensity scores (VAS), functional disability assessments (ODI, RMDQ), health-related quality of life measures (SF-36), and medication usage for pain management. The specific outcome measures used in each study were extracted and synthesized to evaluate the overall effect of hot spring hydrotherapy on chronic low back pain.
Information Sources
In our pursuit to ensure thoroughness in the research, a well-rounded search strategy was adopted, making use of multiple databases. The databases were PubMed, the Web of Science Core Collection, EMBASE, the Cochrane Library, and EBSCO databases. These sources were chosen due to their comprehensive coverage of scientific literature across diverse research fields. The temporal scope of our search was defined from the inception of each database up to October 31, 2022.
To enhance the comprehensiveness of our retrieval strategy, we diligently reviewed the reference lists from previous studies. This supplementary step was crucial as it enabled us to unearth valuable studies that might not have been captured in our initial database searches. This search strategy ensured that all potentially relevant articles, regardless of their year of publication or database of origin, were considered for our research.
Search
The detailed search strategy for the meta-analysis on spa treatment for chronic low back pain involved the following steps:
Subject heading: Based on the PICOS principle, we determined the search terms related to “Low Back Pain”, “Chronic Pain” and “Hydrotherapy”. “Balneology”, “Hot Springs”, These terms were selected to ensure comprehensive retrieval of relevant studies. Table 1 provides a list of the finalized search terms.
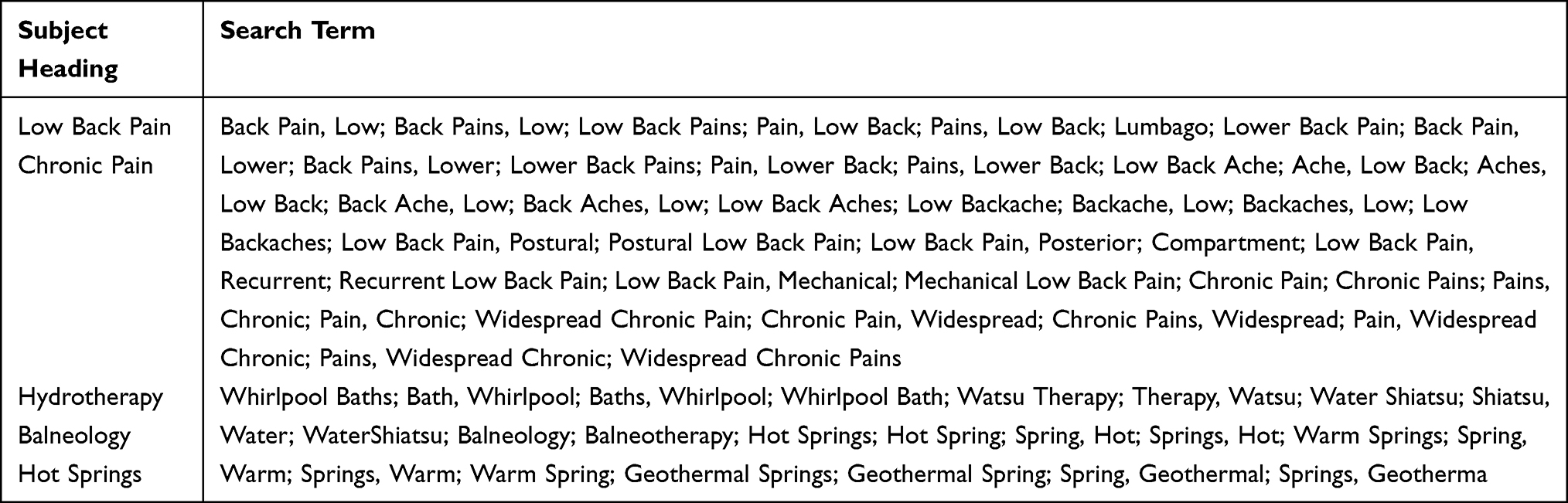 |
Table 1 Search Terms for Hot Spring Hydrotherapy in the Treatment of Chronic Low Back Pain |
Search Strategy for Each Database: The search strategy was customized for each database to maximize the retrieval of relevant literature. The databases searched included PubMed, Embase, Web of Science, EBSCO, and Cochrane Library. The specific search strategies for each database are outlined in Annex 2, providing the detailed syntax and combination of search terms used for each database.
To ensure a comprehensive search, no restrictions were applied regarding the control group, outcome indicators, or literature type. This approach aimed to retrieve as many relevant studies as possible. The search strategies employed aimed to capture all relevant literature available in the selected databases.
Study Selection
Initial Screening
KWX and HX independently screened the titles and abstracts of all the identified studies from the search. This initial screening was done to eliminate studies that were clearly irrelevant, based on the eligibility criteria. Any study that either reviewer believed could potentially meet the inclusion criteria was retained for full-text review.
Full-Text Review
Both reviewers independently reviewed the full text of the remaining studies to assess their eligibility for inclusion. This detailed review was done to determine whether the studies met all the inclusion criteria and none of the exclusion criteria. The reviewers recorded their decisions and the reasons for exclusion of ineligible studies.
Any disagreements between the two reviewers, either at the initial screening stage or the full-text review stage, were resolved by discussion and consensus. If a consensus could not be reached, the disputed item was arbitrated by a third reviewer, SKZ, who made the final decision.
This method of involving two independent reviewers and using a third reviewer for arbitration reduces the potential for bias and error in the study selection process. It also increases the reliability of the systematic review and meta-analysis. The entire process was conducted following the guidelines of the PRISMA statement.
Data Collection Process
The data extraction process was carried out by two independent reviewers, kW and HX, who divided the selected studies between them. Each reviewer was responsible for extracting relevant data from their assigned studies.
The following information was extracted from each study:
Study Characteristics
This included details such as authors, year of publication, country where the study was conducted, study design (randomized controlled trial, observational study, etc.), and the sample size.
Participant Characteristics
Number, age, gender, diagnosis, severity of low back pain.
Intervention Details
Here, we gathered information on the spa therapy used, including the description of the therapy, its duration, frequency, any comparison treatments used, and the setting in which the therapy was provided.
Outcome Measures
Measures of pain relief using the Visual Analog Scale (VAS), disability using the Oswestry Disability Index (ODI) and the Roland-Morris Disability Questionnaire (RMDQ), quality of life, and analgesic dosage. For each measure, the timepoints of measurement and the results, including measures of effect and measures of uncertainty (confidence intervals), were recorded.
Results
Data for each outcome measure, including measures of effect and measures of uncertainty (confidence intervals).
A standardized data extraction form was used to ensure consistency in data collection. The form was pilot-tested on a small number of studies and refined as necessary before being used for full data extraction.
Any disagreements between the two reviewers during the data extraction process were resolved through discussion and consensus. If consensus could not be reached, a third expert, SKZ, was consulted to resolve the dispute.
These data items were selected for extraction as they provide comprehensive and necessary information to fulfill the objectives of our systematic review and meta-analysis.
This systematic and thorough data extraction process was designed to capture all relevant data from the included studies, minimizing the potential for bias and errors, and ensuring the reliability and validity of the systematic review and meta-analysis.
Risk of Bias in Individual Studies
The risk of bias for each study was systematically assessed using the Risk of Bias 2.0 (ROB 2.0) tool20 developed by the Cochrane Collaboration. This instrument addresses five domains: Randomization process, deviations from intended interventions, missing outcome data, Measurement of the outcome, selection of reported results.
Each study was independently evaluated by two reviewers (KWX and HX), with each domain classified as “Low”, “High”, or “Unclear” risk. Discrepancies were resolved through discussion, and if consensus was not achieved, adjudication involved a third reviewer (WSZ). This rigorous bias assessment strategy ensured the reliability of the findings from our systematic review and meta-analysis.
Summary Measures
Primary outcome measures in our systematic review and meta-analysis were the Visual Analog Scale (VAS) for pain relief, the Oswestry Disability Index (ODI), and the Roland-Morris Disability Questionnaire (RMDQ) for disability evaluation. We also included quality of life and analgesic dosage as secondary outcome measures.
To aggregate the data from the studies, we used mean values and standard deviations (SD) for both primary and secondary outcomes. In instances where studies reported median values and range or interquartile ranges, we employed established statistical methods to calculate the corresponding mean values and standard deviations.
Such standardization of summary measures ensured a consistent approach in our quantitative synthesis, thus facilitating an accurate assessment of the overall effects of spa therapy on low back pain.
Synthesis of Results
For the synthesis of outcomes, both fixed-effects and random-effects models were implemented based on the I² statistic; a fixed-effects model was used when I² was less than 50%, denoting low heterogeneity, and a random-effects model was applied when I² was 50% or greater, signaling moderate to high heterogeneity. In this meta-analysis, the effect sizes were calculated using the Standardized Mean Difference (SMD) when the units of measurement were inconsistent across the included studies. When the units of measurement were consistent among the studies, the Weighted Mean Difference (WMD) was used to calculate the pooled effect sizes.
In the handling of missing data, a systematic approach was adopted. Initially, GetData software was utilized to retrieve data from figures.21 If data remained to get, correspondence with the respective authors was pursued. In the event of non-obtainability of data, the particular study was excluded from the meta-analysis to uphold the stringent standards of our research.
We use the sensitivity analysis was conducted to ascertain the robustness of our findings. Individual studies were sequentially omitted from the pooled analysis to assess the influence of each on the overall effect size. This approach facilitated the identification of any studies disproportionately influencing the collective results.
Results
Literature Search results
This study conducted a literature search following the PRISMA guidelines. The flowchart in Figure 1 illustrates the search strategy and screening process.
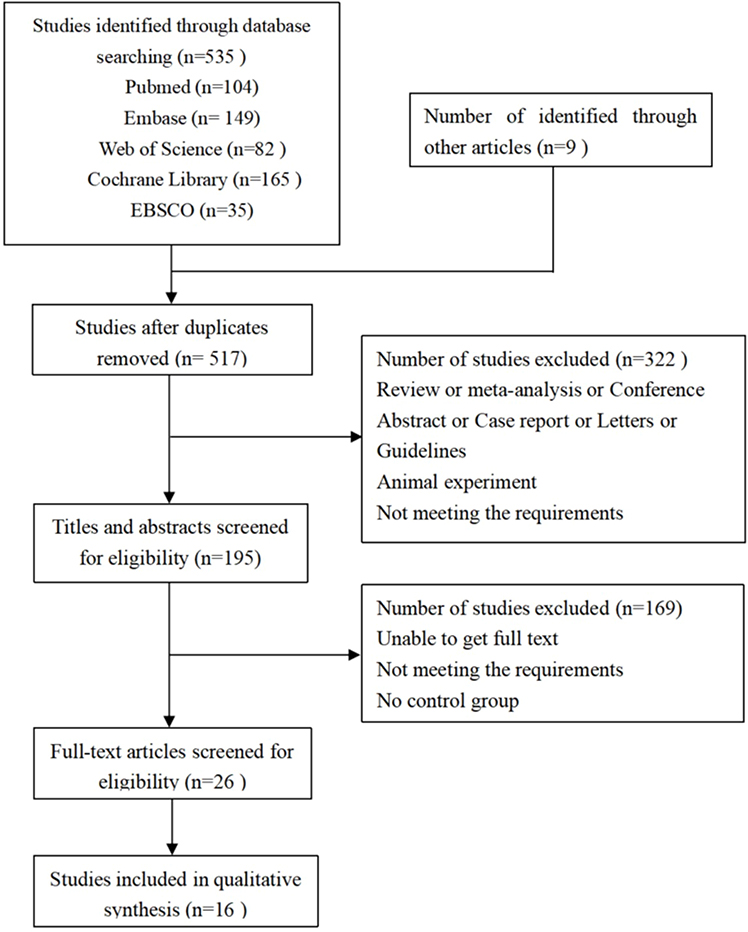 |
Figure 1 Document retrieval flow chart. |
Five databases, including PubMed, Web of Science, EMBASE, Cochrane Library, and EBSCO, were searched in the preliminary phase, resulting in a total of 535 documents. After deduplicating the database records, the retained literature underwent a detailed assessment during the full-text review. Additionally, the reference lists of included studies were checked, and a manual search was performed. Following the initial screening and subsequent re-screening, a total of 16 research papers were ultimately included in the analysis.
Literature Characteristics
In this meta-analysis, 16 studies were included, involving 1656 participants with chronic low back pain across various countries. These studies had diverse sample sizes and age ranges, representing a wide range of populations. The treatment and control groups utilized different intervention methods. The treatment group received hot spring therapy, either alone or in combination with other interventions, while the control group mainly underwent traditional or physical therapy. The timing, frequency, and duration of interventions varied among the studies.
The studies assessed multiple endpoints, including pain intensity (Visual Analog Scale), functional impairment (Oswestry Disability Index and Roland-Morris Disability Questionnaire), quality of life (Short Form 36 questionnaire), medication usage, daily activities, and pain-related fear avoidance beliefs (Fear-Avoidance Beliefs Questionnaire).For more detailed information on the study characteristics, please consult Table 2.
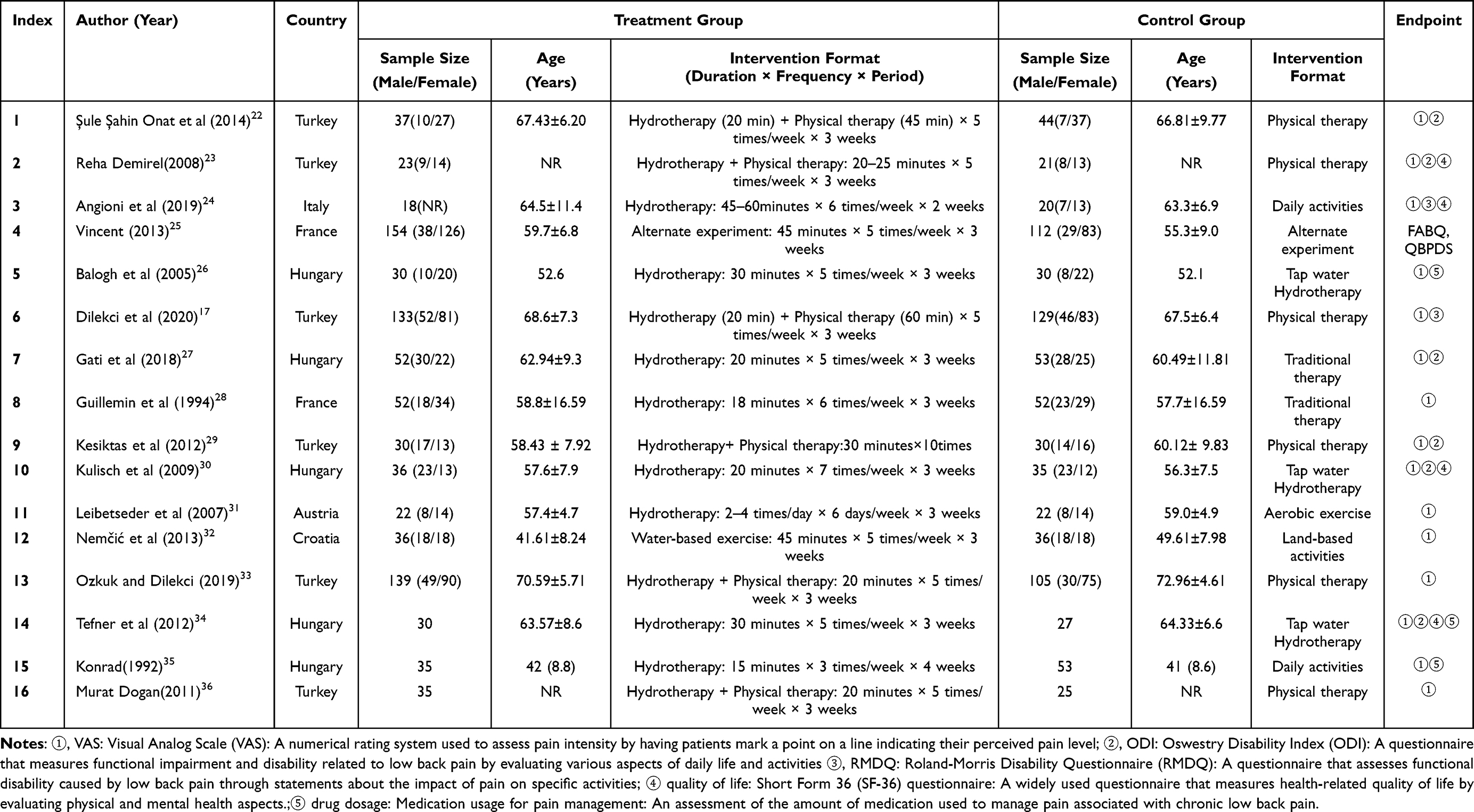 |
Table 2 Feature List of Included Documents |
Quality Evaluation
This meta-analysis on 16 studies indicates a low overall bias risk. However, deviations from interventions, missing data, outcome measurements, and selection of reported results raise concerns. The randomized process risk was low in 88.2% of the studies. High-risk biases were identified: deviations from interventions (35.3%), missing data (64.7%), outcome measurements (17.6%), and reported results (47.1%). Overall, 41.2% of studies had a high bias risk. These findings emphasize careful scrutiny of potential biases when interpreting meta-analysis results. The risk of bias maps, depicted in Figure 2 (Literature Risk of Bias Map) and Figure 3 (Literature Risk of Bias Summary Map), provide visual aids that illustrate the distribution and summary of bias risks across the literature.
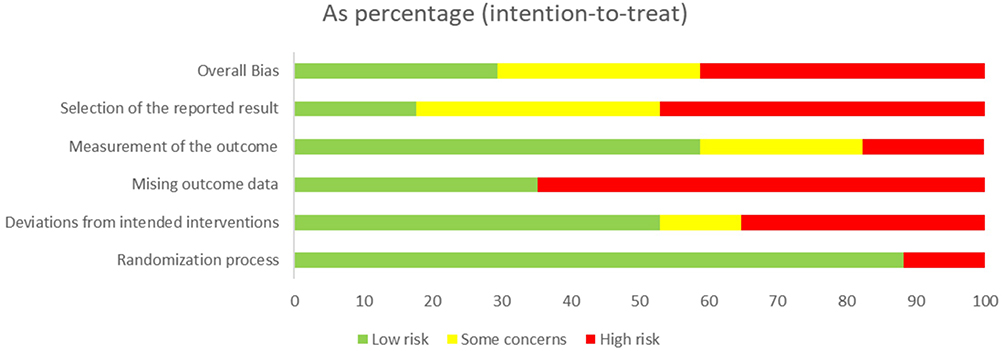 |
Figure 2 Risk of bias map. |
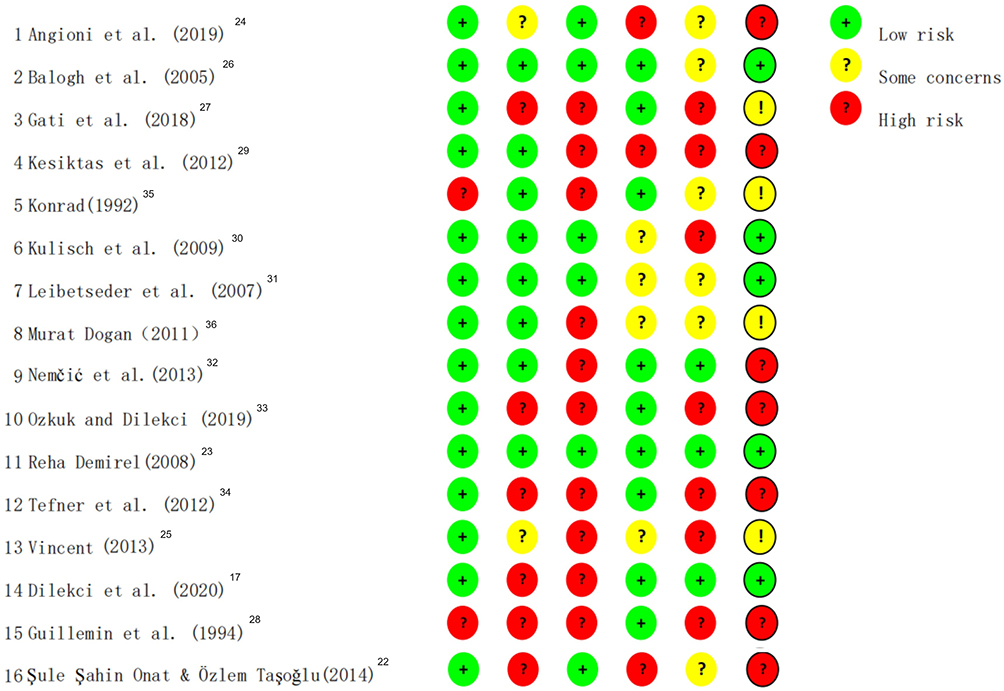 |
Figure 3 Literature Risk of Bias Summary Map. |
Meta-Analysis Results
Impact of Hot Spring Therapy on Pain Perception in Patients with Chronic Low Back Pain
In our meta-analysis examining the efficacy of hot spring hydrotherapy on pain in patients suffering from chronic low back pain, we analyzed a total of 21 studies comparing the intervention and control groups. Utilizing the Visual Analog Scale (VAS) as a measurement tool for pain intensity, we observed a significant reduction in reported pain for the intervention group, as evidenced by the SMD=−0.901 (95% CI [−1.777, −0.025], P=0.044). This outcome indicates a favorable response to hot spring hydrotherapy, denoting an improvement in pain scores. Nevertheless, a high level of heterogeneity was detected among the studies (I²=98.20%), suggesting varying outcomes across the analyzed studies (Figure 4, Pain Index Combined Effect Size Forest Plot).
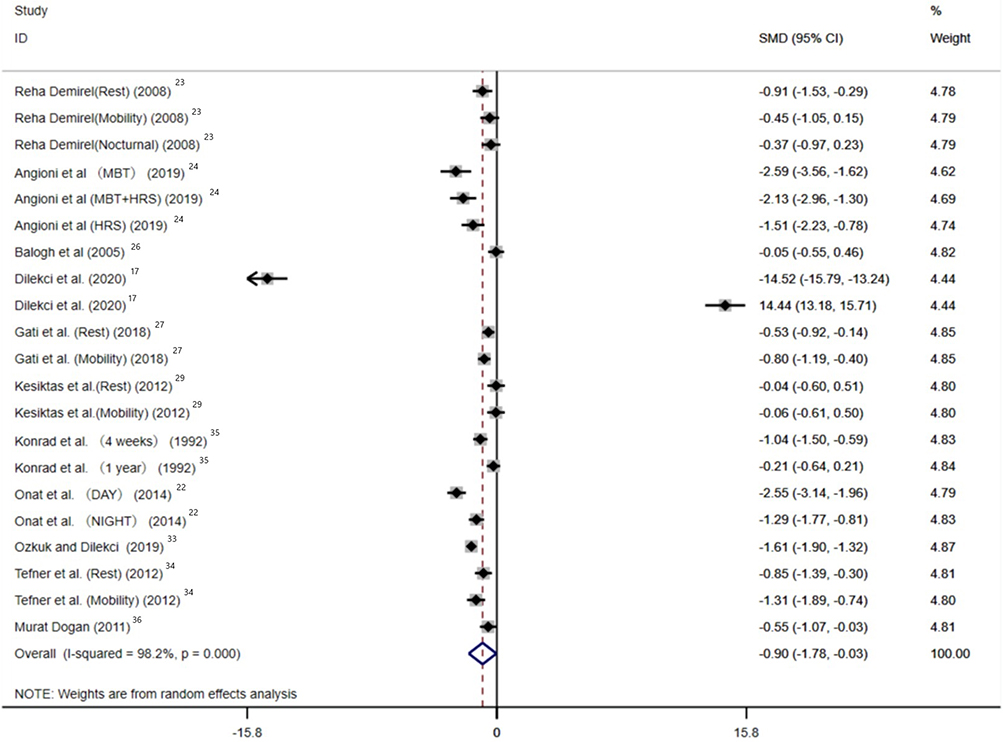 |
Figure 4 Forest plot of combined effect size of pain indicators. |
In our meta-analysis evaluating the impact of hot spring hydrotherapy on chronic low back pain, a subgroup analysis was conducted to further interpret observed heterogeneity. Considering age-based subgroups, older participants (≥60 years) showed a more substantial response to the therapy with a high degree of heterogeneity. Intervention types, both combination therapy and single hot spring hydrotherapy, demonstrated effectiveness, again with high heterogeneity.
From the perspective of regional subgroup analysis, the heterogeneity was particularly notable Studies conducted in Turkey showed extreme heterogeneity, while those from Italy and Hungary presented moderate to high levels of heterogeneity.
The high heterogeneity observed across different subgroups highlights the diverse therapeutic outcomes of hot spring hydrotherapy in varying contexts (Annex 3). Given these findings, future research should delve deeper into the specific factors leading to the substantial heterogeneity observed, enhancing our understanding and utilization of hot spring hydrotherapy in various contexts and demographics.
Hot Spring Therapy and Its Role in Modulating Dysfunction Severity in Patients with Chronic Low Back Pain
The functional impairment severity, as assessed by the Oswestry Disability Index (ODI) and Roland Morris Disability Questionnaire (RMDQ), was evaluated in a total of nine randomized controlled trials to examine the combined effect size of hot spring hydrotherapy on dysfunction severity in patients with chronic low back pain. The analysis revealed a significant and substantial effect, the SMD= −3.236 (95% CI [−4.898, −1.575], P<0.0001). This substantial SMD suggests a notable reduction in dysfunction severity among patients undergoing hot spring hydrotherapy. Nonetheless, it is crucial to acknowledge the high heterogeneity observed among the included studies (I²=98.4%), indicating potential variations in therapeutic outcomes (Figure 5 Modulating Dysfunction index combined effect size result forest plot).
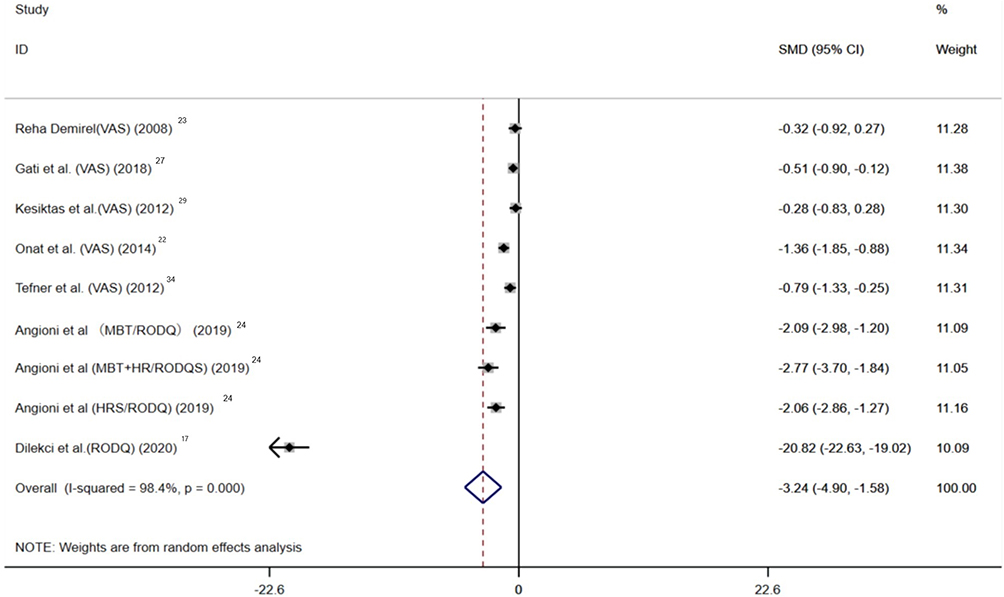 |
Figure 5 Modulating Dysfunction index combined effect size result forest plot. |
By subgroup analysis it was found that among patients aged 60 years and above, hot spring hydrotherapy significantly reduced dysfunction severity. Both combination therapy and single hot spring hydrotherapy demonstrated significant effects. However, in patients below 60 years, the therapy did not show a significant effect on dysfunction severity. In terms of intervention type, both combination therapy and single hot spring hydrotherapy yielded significant reductions in dysfunction severity.
In terms of regional subgroups, Studies conducted in Turkey exhibited high heterogeneity in dysfunction severity outcomes. In contrast, studies from Hungary and Italy showed low heterogeneity (Annex 3). These regional variations in heterogeneity suggest that the effectiveness of hot spring hydrotherapy in reducing dysfunction severity may be influenced by geographic factors or differences in study design and patient characteristics. Further research is needed to better understand the underlying reasons for these regional discrepancies and to determine how they may impact the therapeutic outcomes of hot spring hydrotherapy for chronic low back pain.
These subgroup analyses suggest that hot spring hydrotherapy can effectively reduce dysfunction severity in patients with chronic low back pain, particularly in older patients, and when using either combination therapy or single hot spring hydrotherapy. However, further research is needed to explore the variability observed in the subgroups based on age and country.
Exploring the Effect of Hot Spring Therapy on the Quality of Life in Individuals Suffering from Chronic Low Back Pain
In our meta-analysis, comprising 11 studies that compared the intervention and control groups, we examined the combined effect size of hot spring hydrotherapy on Quality of Life outcomes in patients with chronic low back pain (CLBP). The analysis revealed a small effect size, with a SMD=0.104 (95% CI [−0.397,0.606], P=0.683). Significantly, there was a notable level of heterogeneity among the studies (I²=86.30%). Our findings indicate that hot spring hydrotherapy may not yield significant improvements in Quality of Life for CLBP patients when compared to the control groups. Further research is needed to identify the sources of heterogeneity and gain deeper insights into the impact of hot spring therapy on the Quality of Life of patients with CLBP (Figure 6 The forest plot of the combined effect size results of quality of life indicators).
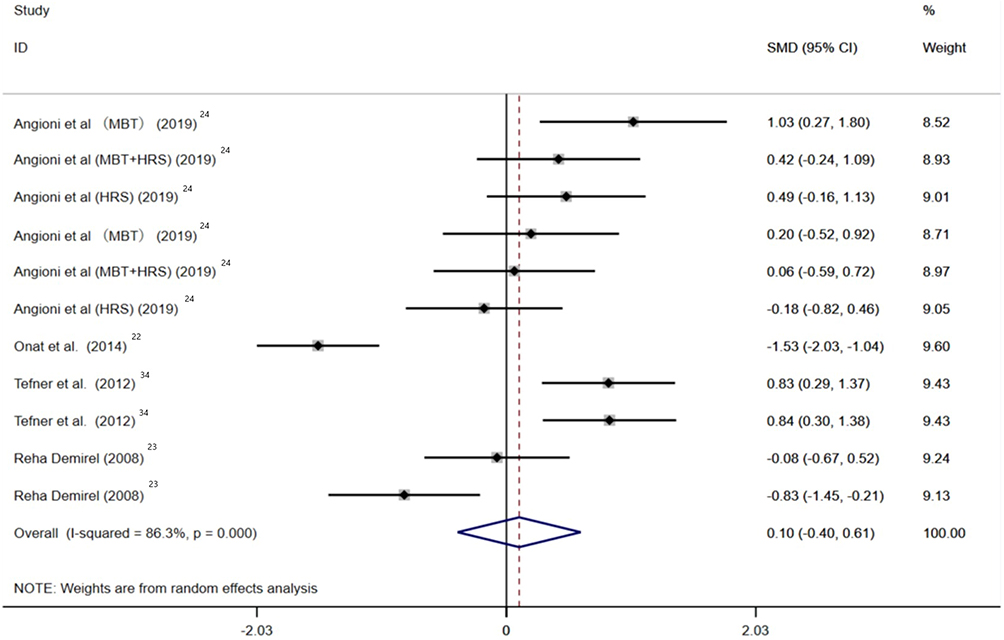 |
Figure 6 The forest plot of the combined effect size results of quality of life indicators. |
Among different age subgroups, patients aged 60 years and above demonstrated a potential positive effect on Quality of Life, while the subgroup with patients in other age groups did not show a statistically significant effect. In terms of intervention types, combination therapy showed a potential negative effect, whereas single hot spring hydrotherapy indicated a potential positive effect on Quality of Life (Annex 3).
These findings suggest that the impact of hot spring hydrotherapy on Quality of Life outcomes in CLBP patients is influenced by factors such as age, intervention type, and country. However, further research is needed to understand the underlying reasons for these variations and to establish more robust conclusions regarding the effectiveness of hot spring hydrotherapy on Quality of Life in patients with chronic low back pain.
The Impact of Hot Spring Hydrotherapy on Drug Dosage in Patients with Chronic Low Back Pain
The impact of hot spring hydrotherapy on drug dosage was examined in our meta-analysis, which included six studies comparing the intervention and control groups. The analysis revealed a significant effect, with a negative Standardized Mean Difference of −0.471 (95% CI[−0.922, −0.020], P=0.041). This indicates that hot spring hydrotherapy is associated with a reduction in drug dosage among patients with chronic low back pain. However, a moderate level of heterogeneity was observed among the included studies (I²=70.70%). Further research is warranted to explore the sources of heterogeneity and gain a better understanding of the specific factors influencing the effect of hot spring hydrotherapy on drug dosage in patients with chronic low back pain (Figure 7 Forest plot of combined effect size results of drug dosage indicators).
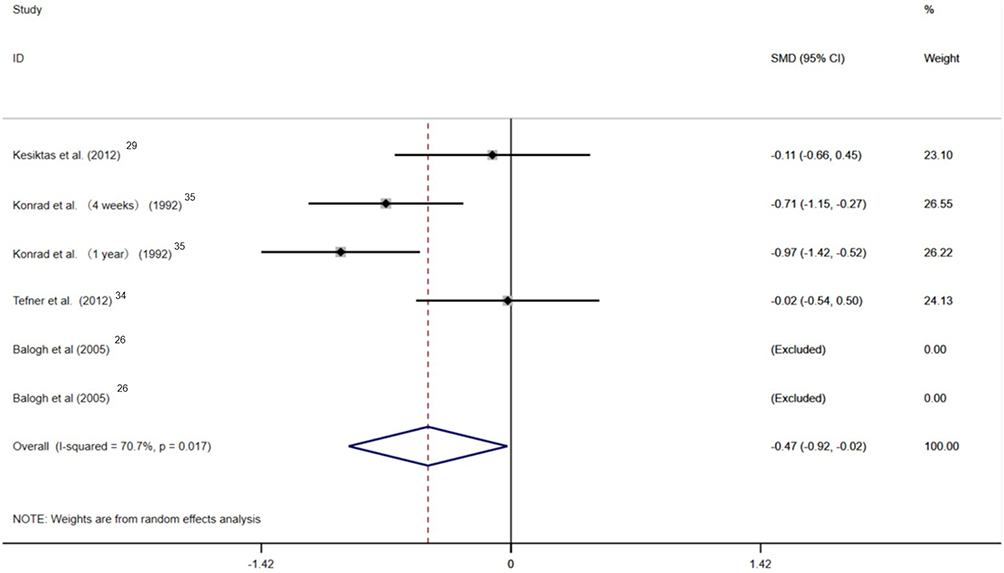 |
Figure 7 Forest plot of combined effect size results of drug dosage indicators. |
In our meta-analysis examining the impact of hot spring hydrotherapy on chronic low back pain, a subgroup analysis was conducted to gain further insights into the observed heterogeneity. Regarding age-based subgroups, older participants (≥60 years) showed a notable response to the therapy, despite a low number of studies available. The efficacy in the subgroup of patients below 60 years varied, with a negative effect size indicating a reduction in drug dosage, albeit with moderate heterogeneity. When considering the intervention types, both combination therapy and single hot spring hydrotherapy demonstrated effectiveness in reducing drug dosage, with moderate to high levels of heterogeneity.
From a regional perspective, the heterogeneity was particularly evident. Studies conducted in Hungary revealed a negative effect size, indicating a reduction in drug dosage with moderate heterogeneity. Conversely, the single study from Turkey showed a different pattern, with a non-significant effect size and no heterogeneity observed (Annex 3).
The high heterogeneity observed across the age and intervention type subgroups, as well as the regional differences, underscores the diverse therapeutic outcomes of hot spring hydrotherapy in different contexts. Future research should focus on identifying the specific factors contributing to the observed heterogeneity, thereby enhancing our understanding and utilization of hot spring hydrotherapy in various demographic and regional settings.
Publication Bias Analysis
Publication bias analysis was conducted for the VAS index and quality of life index. Due to the limited number of studies (less than 10) on functional impairment and drug dosage, no publication bias analysis was performed for these variables.
The Egger’s test was conducted to assess publication bias across the examined variables. The results showed no significant evidence of publication bias for the variables analyzed, which included VAS slope (coef. −1.01174, t=−0.71, P=0.488), VAS bias (coef. 0.4210571, t=0.08, P=0.938), Quality of Life slope (coef. −2.607475, t=−1.29, P=0.231), and Quality of Life bias (coef. 8.534173, t=1.31, P=0.221). These findings indicate that the included studies demonstrate no notable bias in reporting the effects of hot spring hydrotherapy on the examined variables (Figure 8. Publication bias plot of hydrotherapy for chronic low back pain).
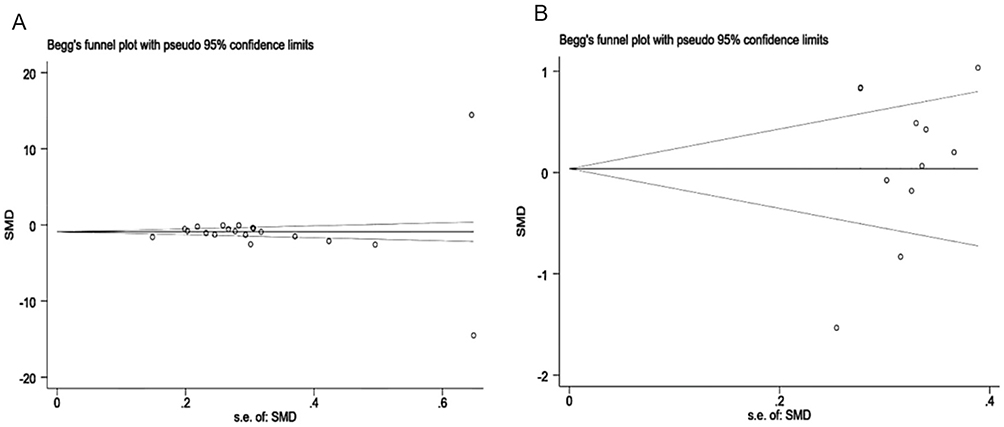 |
Figure 8 (A) Publication Bias Analysis graph of pain index in CLBP patients. (B) Publication Bias Analysis graph of quality of life in CLBP patients. |
Sensitivity Analysis
In order to assess the robustness of our systematic review and meta-analysis investigating the effectiveness of hot spring hydrotherapy on pain and functionality in patients with chronic low back pain, we conducted four sensitivity analyses. These analyses involved the inclusion/exclusion of specific studies and evaluated the impact on the overall effect sizes and conclusions of our findings. The results indicated that the inclusion or exclusion of individual studies did not substantially alter the overall results, providing confidence in the robustness of our findings. For a visual representation of the sensitivity analyses, please refer to Figure 9, which illustrates the sensitivity analysis chart depicting the effect of spa treatment on chronic low back pain.
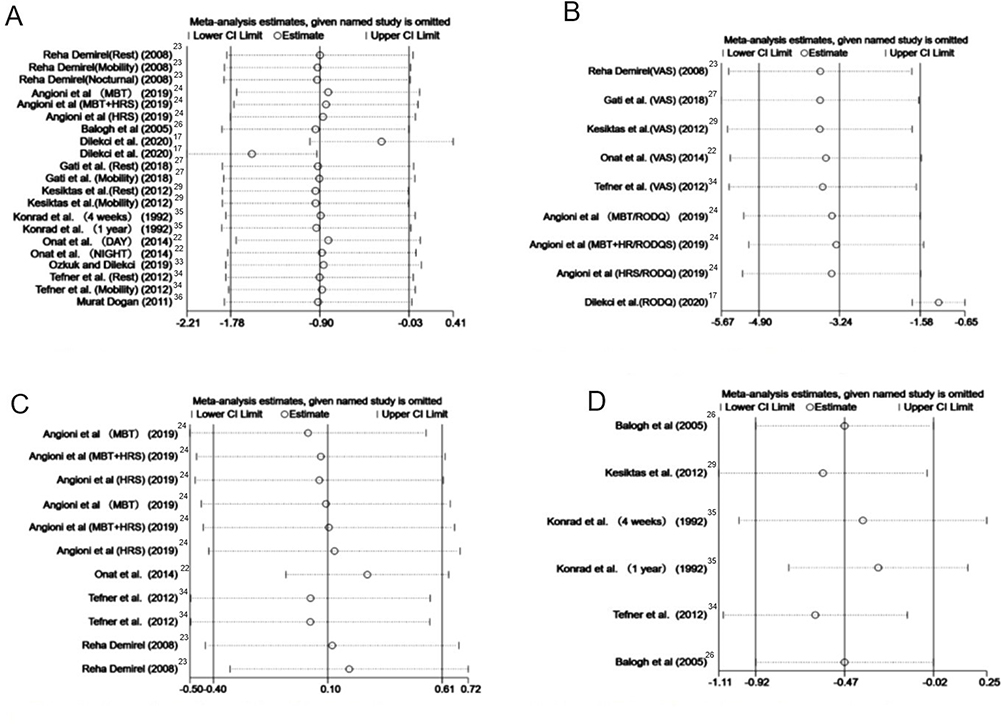 |
Figure 9 (A) Sensitivity analysis of pain indicators. (B) Sensitivity analysis of functional impairment indicators. (C) Sensitivity analysis of quality of life indicators. (D) Sensitivity analysis of drug dosage indicators. |
Discussion
Patients with Chronic Lower Back Pain are accompanied by various uncomfortable symptoms. Past research has confirmed that aquatic activities can effectively improve the related symptoms in CLBP patients, but there remains a great deal of uncertainty about the effectiveness of hot spring hydrotherapy in improving CLBP.37 Through the meta-analysis of the included literature in this study, it was found that compared with the control group, symptoms of chronic lower back pain and functional disorders in patients over 60 years old, as well as the reduction in the use of analgesics, were significantly improved (P < 0.05). However, no significant difference was found for the population over 60 years old (P≥0.05). Compared with combining hot spring hydrotherapy with other interventions, the single treatment method of hot spring hydrotherapy has a better improvement effect on functional disorders and can effectively improve the quality of life of CLBP patients. Currently, the therapeutic effect of hot spring hydrotherapy on CLBP patients over 60 years old remains uncertain.
The Impact of Hot Spring Hydrotherapy on Pain in Patients with Chronic Lower Back Pain
The Visual Analogue Scale (VAS) is a commonly used pain assessment tool primarily employed for evaluating the degree of pain in patients with chronic lower back pain. It involves patients self-assessing their pain intensity, usually on a continuous range from no pain (0 points) to extreme pain (10 points). Numerous studies have confirmed that VAS scores can effectively reflect pain intensity and response to treatment, and closely correlate with indicators such as quality of life, functional disorders, and psychological conditions in patients with chronic lower back pain.38 According to the “Guidelines for the Assessment and Treatment of Chronic Pain (2012)”, the ideal state for VAS scoring is as close to 0 points as possible to reflect the minimum sensation of pain and the best quality of life.39
The results of this meta-analysis show that hot spring hydrotherapy can effectively improve the VAS indicators of CLBP patients. This might be related to the higher baseline level of VAS among the subjects in this study. This differs from a recent study by Maccarone (2023), which, through balneotherapy rehabilitation of 160 patients with degenerative or postoperative musculoskeletal diseases, found that compared to other hydrotherapies, balneotherapy demonstrated limited effectiveness in relieving various forms of pain, Moreover, it exhibited a relatively weak correlation with regard to the reduction of scores across various parameters.40 This study aligns with the findings of a previous meta-analysis, Ruixue (2019) found in a meta-analysis study that included 12 papers that after hot spring hydrotherapy, VAS indicators were significantly reduced, MD=16.07, 95% CI [9.57, 22.57].41 At the same time, Bai (2019) also proved through a meta-study that hot spring hydrotherapy significantly improved the pain of CLBP patients with degenerative joint diseases and spinal diseases during loading and rest, with SMD=−0.747 (P<0.05) for pain indicators during loading and SMD=−0.783 (P<0.05) for pain indicators during rest.16 Moreover, in the subgroup analysis of this study, it was found that compared with the control group, the impact of hot spring hydrotherapy on pain is more significant in elderly CLBP patients (age≥60), while for CLBP patients with age<60, its SMD=−0.561 (P=0.885, not significant).
The phenomenon that hot spring hydrotherapy can improve the pain symptoms of CLBP patients may involve multiple mechanisms. One potential mechanism could be the thermal effect of the hot springs. Under higher temperatures (generally 33–37 degrees Celsius), the heat can trigger a response in the skin’s thermoreceptors.42 These thermoreceptors then relay information to the central nervous system, which initiates physiological responses such as vasodilation, muscle relaxation, and pain reduction. It can also increase blood circulation, alleviate muscle fatigue, improve body balance, and promote the body’s natural healing process.43 Additionally, minerals in the hot spring water (such as sulfur, magnesium, calcium) are absorbed through the skin and may have antioxidant effects on the body, resulting in anti-inflammatory and analgesic effects.29 Balneotherapy has multiple positive effects on musculoskeletal disorders, including pain relief, reduced inflammation, improved mobility, suppression of matrix-degrading enzymes, and the expression of oxidative stress markers. Different types of balneotherapy positively impact these effects. It can reduce various systemic pro-inflammatory mediators such as prostaglandin E2, leukotriene B4, and interleukin-1β, which play a role in inflammation and cartilage degradation in rheumatic diseases. Additionally, balneotherapy helps in regulating the balance between oxidants and antioxidants, lowering oxidative stress levels. It reduces serum/plasma levels of malondialdehyde, increases total antioxidant capacity, and has a beneficial impact on patients with rheumatoid arthritis, fibromyalgia, and osteoarthritis.44 Treatment with hydrogen sulfide (H2S) donors exhibits anti-inflammatory and antioxidant properties in an animal cell culture model of osteoarthritis. This therapy restricts the activation of the MAPK/ERK and NF-kB pathways and reduces the production of osteoarthritis-related factors, including IL-6, IL-8, NO, PGE2, and MMP-13. This indicates that balneotherapy can reduce the levels of inflammatory mediators in joint tissues while simultaneously increasing cortisol concentration, enhancing monocyte chemotaxis to damaged tissues, and promoting an anti-inflammatory phenotype.45 At the same time, the buoyancy generated during hot spring hydrotherapy can relieve the gravitational burden on the spine and joints. This makes it easier for patients to perform flexibility and strength training in the water. It also helps to improve body posture and reduce back pain, which contributes to the alleviation of pain symptoms in CLBP patients.46
The fact that hot spring therapy can significantly improve pain in CLBP patients aged 60 and over, while there is no significant difference for those under 60, may be due to various physiological changes in the body as it ages. These changes include degenerative joint disease, degenerative spine disease,47 and other chronic diseases (such as hypertension, diabetes, heart disease, etc.). These diseases, which may affect pain perception, are more common in older adults.48 These conditions can cause chronic lower back pain, and hot spring hydrotherapy has been proven to alleviate these symptoms, thus improving pain symptoms.49 At the same time, older adults tend to have a more pronounced perception and threshold for pain. This could result in older adults having a stronger perception of the pain-relieving effects produced by hot spring hydrotherapy.50 Furthermore, due to age-related changes in metabolism and endocrine function, the body’s hormone levels may change, causing older adults to have a stronger response to the minerals and other beneficial ingredients in hot spring hydrotherapy.51
Impact of Hot Spring Hydrotherapy on Functional Disability in Patients with Chronic Low Back Pain
The Oswestry Disability Index (ODI) and Roland-Morris Disability Questionnaire (RMDQ) are crucial tools for assessing functional disability resulting from chronic low back pain (CLBP).52 These instruments quantify the impact of CLBP on everyday life, measuring the effect of pain on patients’ quality of life and functional capabilities. They primarily focus on how CLBP affects patients’ daily activities, including walking, sleeping, personal care, social activities, and work. The ODI comprises ten items, and the RMDQ contains 24 questions. A higher score assessed on these scales indicates a more severe functional disability. Both the ODI and RMDQ have been widely used in clinical research and practice, proving their reliability and validity in evaluating functional disability in CLBP patients.
The results of the present study indicate that hot spring hydrotherapy can effectively alleviate functional disability symptoms in patients with CLBP. This suggests that hot spring hydrotherapy can effectively improve functional disability in CLBP patients. These findings are consistent with the outcomes of some previous studies on aquatic exercises. Zhang (2018) reported in a meta-analysis of 11 articles that physical activities in water could significantly enhance physical functional activity in CLBP patients, with an SMD of 0.63 (95% CI [0.17, 1.09], P < 0.05).53 Zhang (2021) stated in a meta-analysis that activities in water could effectively improve functional disability symptoms in CLBP patients (ODI) (SMD = −2.07, 95% CI: [−3.19, −0.96], P < 0.00001).54 However, our subgroup analysis revealed a similar result to the combined effect size for pain indices. Compared with the control group, hot spring hydrotherapy can effectively reduce the functional disability index in older CLBP patients (SMD=−1.515, 95% CI [−2.163, −0.867], P < 0.001), with no significant improvement observed in patients aged under 60.
There are multiple factors contributing to the improvement of functional disability in CLBP patients through hot spring hydrotherapy. One factor may be the stimulation of the nervous system by hot spring hydrotherapy. The temperature and pressure stimulation of hot spring hydrotherapy can impact the sensory nerve endings in the skin, and this information is transmitted to the spinal cord and brain. In the brain, this information is processed and interpreted.55 Subsequently, motor commands are sent through descending neural pathways, leading to improved coordination of body movements, enhanced precision, and fluency of actions, thus improving functional impairments.56 Furthermore, hot spring hydrotherapy can improve muscle function and joint mobility through the temperature and buoyancy of the water. It helps reduce muscle pain and stiffness and increases the range of joint motion, thereby achieving improvements in functional disability symptoms. When engaging in activities in the water, the human body requires a greater sense of body awareness and balance to control movements. This type of training may contribute to improving body awareness and balance, further enhancing motor coordination, and ultimately improving functional disability in CLBP patients.57
Hot spring hydrotherapy has been shown to effectively improve functional disability in elderly CLBP patients, while there is no significant effect observed in CLBP patients below the age of 60. The reasons behind this phenomenon may lie in the physiological differences between patients aged 60 and above and those below 60. Elderly individuals typically experience age-related changes, including degenerative changes in muscles, bones, and joints.58 Hot spring hydrotherapy can partially alleviate these symptoms, leading to an improvement in functional disability among elderly CLBP patients. Additionally, older individuals often experience a decline in muscle mass and function, decreased bone density, and an increased prevalence of joint diseases. These factors may make older individuals more sensitive to treatment methods, particularly those related to muscles, bones, and joints.59 Hot spring hydrotherapy helps improve muscle strength, joint mobility, and pain perception in the elderly. However, for younger CLBP patients (age < 60), who may have more stable physiological conditions, CLBP may be more related to other factors such as posture and activity patterns. Therefore, the effects of hot spring hydrotherapy may not be as pronounced for this age group. Furthermore, hot spring hydrotherapy effectively promotes joint lubrication, leading to more significant improvements in functional disability. It is possible that CLBP patients below the age of 60 are influenced by other factors, which may result in less noticeable effects of hot spring hydrotherapy for them.60
The Impact of Hot Spring Hydrotherapy on the Quality of Life and Medication Dosage in Patients with Chronic Low Back Pain
Meta-analysis findings suggest that single-session hot spring hydrotherapy can contribute to the improvement of the quality of life in patients with chronic low back pain. The SF-36 scale is widely used as a tool for evaluating the quality of life.61 Therefore, it can be observed that in this study, single-session hot spring hydrotherapy effectively improves the quality of life in CLBP patients. This improvement can be attributed to the alleviation of pain and discomfort, leading to reduced stress and anxiety levels, thereby positively influencing psychological well-being and emotional state.62 However, it is worth noting that potential biases may arise due to differences in sample size, study design, follow-up duration, and study quality among the included studies. Additionally, the heterogeneity of the CLBP patients included in the study, such as age, gender, severity of the disease, and duration, may influence the treatment outcomes, resulting in differences in the effectiveness of various hot spring hydrotherapy interventions. Consistent with the pain outcomes, CLBP patients aged 60 and above experienced pain relief, which consequently led to a reduction in the dosage of pain medication.
Tognolo (2022) conducted a comprehensive review of 14 studies on balneotherapy, clearly indicating its positive impact on patients with conditions such as osteoarthritis and fibromyalgia. This impact includes pain relief, enhanced functionality, and improved quality of life. The combination of balneotherapy with rehabilitation interventions effectively improves various indicators in patients with rheumatic diseases. These effects are likely the result of the combined mechanical, thermal, and chemical actions of different balneotherapy approaches. Immersion in thermal waters helps alleviate the burden on degenerative and/or inflammatory joints. Furthermore, temperature stimulation may trigger the release of cortisol, adrenocorticotropic hormone, prolactin, and β-endorphins, providing significant analgesic and immune-suppressive effects, thereby improving symptoms, reducing mechanical hypersensitivity, and neuropathic pain. Additionally, the positive social atmosphere in the balneotherapy environment contributes to the treatment of chronic diseases, reduces psychological stress, and enhances overall quality of life.63 Scanu (2021) demonstrated the immunomodulatory effects and the therapeutic use of hydrogen sulfide (H2S) donors exhibiting anti-inflammatory and antioxidant activities. This treatment restricts the activation of the MAPK/ERK and NF-kB pathways and reduces the generation of various factors associated with OA. They propose that balneotherapy has beneficial effects on the immune system, exerting inhibitory effects on inflammation and oxidative stress, thereby reducing the levels of inflammatory mediators, increasing cortisol concentrations, and improving pain, functionality, and quality of life.64
Limitation
- Language Limitation: The research only includes studies published in English, leading to a potential language bias and ignoring findings presented in other languages.
- Heterogeneity: There is considerable heterogeneity across studies due to differences in research design, methodologies, and patient populations, which makes it difficult to aggregate data and draw firm conclusions. To enhance the quality of future research, standardization of patient selection criteria is recommended, including factors such as age, severity of CLBP, and duration of the condition.
- Lack of Long-Term Studies: Most studies focus on the short-term effects of spa therapy, and there is a lack of research investigating the long-term efficacy and sustainability of the benefits. Researchers should consider conducting long-term studies to evaluate the sustainability of the benefits of hot spring hydrotherapy, allowing for an in-depth exploration of the long-term effectiveness of this treatment. Researchers should prioritize the consistency of control group composition and study design to ensure adequate matching, thereby facilitating the attainment of reliable results.
- Insufficient High-Quality Trials: The field lacks a substantial number of high-quality randomized controlled trials, which limits the strength of the evidence supporting the effectiveness of spa therapy for chronic low back pain.
Conclusion
The findings of this meta-analysis study indicate that hot spring hydrotherapy has a positive impact on pain and functional disability symptoms in patients with chronic low back pain (CLBP), and it reduces the use of pain medication. Single-session hot spring hydrotherapy effectively improves the quality of life in CLBP patients. Subgroup analysis revealed that the effects of hot spring hydrotherapy are more pronounced in CLBP patients aged 60 and above, with a reduction in pain scores by 1.43, a decrease in functional disability scores by 1.52, and a decrease in medication dosage by 0.018 g/day. Single-session hot spring hydrotherapy improves the quality of life score by 0.83. However, due to heterogeneity and potential biases in the included studies, as well as differences in study designs, the therapeutic effects of hot spring hydrotherapy on CLBP patients aged below 60 cannot be determined conclusively, and further research is needed.
Acknowledgments
We would like to express our gratitude to the authors of the primary studies included in this systematic review and meta-analysis. We also thank the editorial boards, reviewers, and our research team for their contributions. We appreciate the support and input from our colleagues and peers, as well as the funding agencies that supported this research. Their efforts have advanced our understanding of the effectiveness of hot spring hydrotherapy for chronic low back pain.
Disclosure
The authors declare that they have no conflicts of interest related to this research study.
References
1. Markman JD, Czerniecka-Foxx K, Khalsa PS, et al. AAPT Diagnostic Criteria for Chronic Low Back Pain. J Pain. 2020;21(11–12):1138–1148. doi:10.1016/j.jpain.2020.01.008
2. Last AR, Hulbert K. Chronic low back pain: evaluation and management. Am Fam Physician. 2009;79(12):1067–1074.
3. Childs JD, Cleland JA, Elliott JM, et al. Neck pain: clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Orthopedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2008;38(9):A1–a34. doi:10.2519/jospt.2008.0303
4. Hurwitz EL, Randhawa K, Yu H, Côté P, Haldeman S. The Global Spine Care Initiative: a summary of the global burden of low back and neck pain studies. Eur Spine J. 2018;27(Suppl 6):796–801. doi:10.1007/s00586-017-5432-9
5. WHO. The burden of musculoskeletal conditions at the start of the new millennium. World Health Organ Tech Rep Ser. 2003;919:1–218.
6. Hoy D, Brooks P, Blyth F, Buchbinder R. The Epidemiology of low back pain. Best Pract Res Clin Rheumatol. 2010;24(6):769–781. doi:10.1016/j.berh.2010.10.002
7. Shipton EA. Physical Therapy Approaches in the Treatment of Low Back Pain. Pain Ther. 2018;7(2):127–137. doi:10.1007/s40122-018-0105-x
8. Wang X, Borgman B, Vertuani S, Nilsson J. A systematic literature review of time to return to work and narcotic use after lumbar spinal fusion using minimal invasive and open surgery techniques. BMC Health Serv Res. 2017;17(1):446. doi:10.1186/s12913-017-2398-6
9. Yabuki S, Tam CK, et al. Evidence-Based Recommendations on the Pharmacological Management of Osteoarthritis and Chronic Low Back Pain: an Asian Consensus. Asian J Anesthesiol. 2019;57(2):37–54. doi:10.6859/aja.201906_57(2).0003
10. Meroni R, Piscitelli D, Ravasio C, et al. Evidence for managing chronic low back pain in primary care: a review of recommendations from high-quality clinical practice guidelines. Disabil Rehabil. 2021;43(7):1029–1043. doi:10.1080/09638288.2019.1645888
11. Yolgösteren E, Külekçioğlu S. The effectiveness of balneotherapy and thermal aquatic exercise in postoperative persistent lumbar pain syndrome. Int J Biometeorol. 2021;65(12):2137–2145. doi:10.1007/s00484-021-02176-z
12. Bernetti A, Mangone M, Alviti F, et al. Spa therapy and rehabilitation of musculoskeletal pathologies: a proposal for best practice in Italy. Int J Biometeorol. 2020;64(6):905–914. doi:10.1007/s00484-019-01731-z
13. Kamioka H, Tsutani K, Yamada M, et al. Effectiveness of music therapy: a summary of systematic reviews based on randomized controlled trials of music interventions. Patient Prefer Adherence. 2014;8:727–754. doi:10.2147/ppa.S61340
14. Magrey MN, Danve AS, Ermann J, Walsh JA. Recognizing Axial Spondyloarthritis: a Guide for Primary Care. Mayo Clin Proc. 2020;95(11):2499–2508. doi:10.1016/j.mayocp.2020.02.007
15. Serra R, Ielapi N, Bitonti A, et al. Efficacy of a Low-Dose Diosmin Therapy on Improving Symptoms and Quality of Life in Patients with Chronic Venous Disease: randomized, Double-Blind, Placebo-Controlled Trial. Nutrients. 2021;13(3). doi:10.3390/nu13030999
16. Bai R, Li C, Xiao Y, Sharma M, Zhang F, Zhao Y. Effectiveness of spa therapy for patients with chronic low back pain: an updated systematic review and meta-analysis. Medicine. 2019;98(37):e17092. doi:10.1097/md.0000000000017092
17. Dilekçi E, Özkuk K, Kaki B. The short-term effects of balneotherapy on pain, disability and fatigue in patients with chronic low back pain treated with physical therapy: a randomized controlled trial. Complement Ther Med. 2020;54:102550. doi:10.1016/j.ctim.2020.102550
18. Fikri-Benbrahim K, Houti A, El Ouali Lalami A, et al. Main Therapeutic Uses of Some Moroccan Hot Springs’ Waters. Evid Based Complement Alternat Med. 2021;2021:5599269. doi:10.1155/2021/5599269
19. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
20. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
21. Gheibi S, Mahmoodzadeh A, Kashfi K, Jeddi S, Ghasemi A. Data Extraction from Graphs Using Adobe Photoshop: applications for Meta-Analyses. Int J Endocrinol Metab. 2019;17(4):e95216. doi:10.5812/ijem.95216
22. Onat Ş, Taşoğlu Ö, Güneri FD, Özişler Z, Safer VB, Özgirgin N. The effectiveness of balneotherapy in chronic low back pain. Clin Rheumatol. 2014;33(10):1509–1515. doi:10.1007/s10067-014-2545-y
23. Demirel R, Ucok K, Kavuncu V, et al. Effects of balneotherapy with exercise in patients with low back pain. J Back Musculoskelet Rehabil. 2008;21(4):263–272.
24. Angioni MM, Denotti A, Pinna S, et al. Spa therapy induces clinical improvement and protein changes in patients with chronic back pain. Reumatismo. 2019;71(3):119–131. doi:10.4081/reumatismo.2019.1200
25. Gremeaux V, Benaïm C, Poiraudeau S, Hérisson C, Dupeyron A, Coudeyre E. Evaluation of the benefits of low back pain patients’ education workshops during spa therapy. Joint Bone Spine. 2013;80(1):82–87. doi:10.1016/j.jbspin.2011.12.014
26. Balogh Z, Ordögh J, Gász A, Német L, Bender T. Effectiveness of balneotherapy in chronic low back pain -- a randomized single-blind controlled follow-up study. Forsch Komplementarmed Klass Naturheilkd. 2005;12(4):196–201. doi:10.1159/000086305
27. Gáti T, Tefner IK, Kovács L, Hodosi K, Bender T. The effects of the calcium-magnesium-bicarbonate content in thermal mineral water on chronic low back pain: a randomized, controlled follow-up study. Int J Biometeorol. 2018;62(5):897–905. doi:10.1007/s00484-017-1491-1
28. Guillemin F, Constant F, Collin JF, Boulange M. Short and long-term effect of spa therapy in chronic low back pain. Br J Rheumatol. 1994;33(2):148–151. doi:10.1093/rheumatology/33.2.148
29. Kesiktas N, Karakas S, Gun K, Gun N, Murat S, Uludag M. Balneotherapy for chronic low back pain: a randomized, controlled study. Rheumatol Int. 2012;32(10):3193–3199. doi:10.1007/s00296-011-2163-9
30. Kulisch A, Bender T, Németh A, Szekeres L. Effect of thermal water and adjunctive electrotherapy on chronic low back pain: a double-blind, randomized, follow-up study. J Rehabil Med. 2009;41(1):73–79. doi:10.2340/16501977-0291
31. Leibetseder V, Strauss-Blasche G, Marktl W, Ekmekcioglu C. Does aerobic training enhance effects of spa therapy in back pain patients? A randomized, controlled clinical trial. Forsch Komplementmed. 2007;14(4):202–206. doi:10.1159/000104686
32. Nemcić T, Budisin V, Vrabec-Matković D, Grazio S. Comparison of the effects of land-based and water-based therapeutic exercises on the range of motion and physical disability in patients with chronic low-back pain: single-blinded randomized study. Acta Clin Croat. 2013;52(3):321–327.
33. Özkuk K, Dilekçi E. The effects of balneotherapy in elderly patients with chronic low back pain treated with physical therapy: a pilot study. J Istanbul Faculty Med. 2019;82(4):186–192.
34. Tefner IK, Németh A, Lászlófi A, Kis T, Gyetvai G, Bender T. The effect of spa therapy in chronic low back pain: a randomized controlled, single-blind, follow-up study. Rheumatol Int. 2012;32(10):3163–3169. doi:10.1007/s00296-011-2145-y
35. Konrad K, Tatrai T, Hunka A, Vereckei E, Korondi I. Controlled trial of balneotherapy in treatment of low back pain. Ann Rheum Dis. 1992;51(6):820–822. doi:10.1136/ard.51.6.820
36. Dogan M, Sahin O, Elden H, Hayta E, Kaptanoglu E. Additional therapeutic effect of balneotherapy in low back pain. South Med J. 2011;104(8):574–578. doi:10.1097/SMJ.0b013e318224644f
37. Ma J, Zhang T, He Y, Li X, Chen H, Zhao Q. Effect of aquatic physical therapy on chronic low back pain: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2022;23(1):1050. doi:10.1186/s12891-022-05981-8
38. Tagliaferri SD, Miller CT, Owen PJ, et al. Domains of Chronic Low Back Pain and Assessing Treatment Effectiveness: a Clinical Perspective. Pain Pract. 2020;20(2):211–225. doi:10.1111/papr.12846
39. Hoydonckx Y, Kumar P, Flamer D, et al. Quality of chronic pain interventional treatment guidelines from pain societies: assessment with the AGREE II instrument. Eur J Pain Apr. 2020;24(4):704–721. doi:10.1002/ejp.1524
40. Maccarone MC, Magro G, Albertin C, et al. Short-time effects of spa rehabilitation on pain, mood and quality of life among patients with degenerative or post-surgery musculoskeletal disorders. Int J Biometeorol. 2023;67(1):29–36. doi:10.1007/s00484-022-02381-4
41. Bender T, Bálint G, Prohászka Z, Géher P, Tefner IK. Evidence-based hydro- and balneotherapy in Hungary--a systematic review and meta-analysis. Int J Biometeorol Apr. 2014;58(3):311–323. doi:10.1007/s00484-013-0667-6
42. Benarroch EE. Physiology and Pathophysiology of the Autonomic Nervous System. Continuum. 2020;26(1):12–24. doi:10.1212/con.0000000000000817
43. Devereux K, Robertson D, Briffa NK. Effects of a water-based program on women 65 years and over: a randomised controlled trial. Aust J Physiother. 2005;51(2):102–108. doi:10.1016/s0004-9514(05)70038-6
44. Cheleschi S, Tenti S, Seccafico I, Gálvez I, Fioravanti A, Ortega E. Balneotherapy year in review 2021: focus on the mechanisms of action of balneotherapy in rheumatic diseases. Environ Sci Pollut Res Int. 2022;29(6):8054–8073. doi:10.1007/s11356-021-17780-0
45. Cheleschi S, Gallo I, Tenti S. A comprehensive analysis to understand the mechanism of action of balneotherapy: why, how, and where they can be used? Evidence from in vitro studies performed on human and animal samples. Int J Biometeorol. 2020;64(7):1247–1261. doi:10.1007/s00484-020-01890-4
46. Dubois O, Salamon R, Germain C, et al. Balneotherapy versus paroxetine in the treatment of generalized anxiety disorder. Complement Ther Med. 2010;18(1):1–7. doi:10.1016/j.ctim.2009.11.003
47. Fehlings MG, Tetreault L, Nater A, et al. The Aging of the Global Population: the Changing Epidemiology of Disease and Spinal Disorders. Neurosurgery. 2015;77(Suppl 4):S1–5. doi:10.1227/neu.0000000000000953
48. Vetrano DL, Foebel AD, Marengoni A, et al. Chronic diseases and geriatric syndromes: the different weight of comorbidity. Eur J Intern Med. 2016;27:62–67. doi:10.1016/j.ejim.2015.10.025
49. Sukthana Y, Lekkla A, Sutthikornchai C, Wanapongse P, Vejjajiva A, Bovornkitti S. Spa, springs and safety. Southeast Asian J Trop Med Public Health. 2005;36(Suppl 4):10–16.
50. Tinnirello A, Mazzoleni S, Santi C. Chronic Pain in the Elderly: mechanisms and Distinctive Features. Biomolecules. 2021;11(8). doi:10.3390/biom11081256
51. Antonelli M, Donelli D, Veronesi L, Vitale M, Pasquarella C. Clinical efficacy of medical hydrology: an umbrella review. Int J Biometeorol. 2021;65(10):1597–1614. doi:10.1007/s00484-021-02133-w
52. Mohan A, Sharma R, Ghai B, Kumar V, Makkar JK, Jain A. Cross-cultural Adaptation and Validation of Hindi Version of Roland Morris Disability Questionnaire for Chronic Low Back Pain in Indian Population. Spine. 2023;48(5):364–370. doi:10.1097/brs.0000000000004472
53. Shi Z, Zhou H, Lu L, et al. Aquatic Exercises in the Treatment of Low Back Pain: a Systematic Review of the Literature and Meta-Analysis of Eight Studies. Am J Phys Med Rehabil. 2018;97(2):116–122. doi:10.1097/phm.0000000000000801
54. Zhang SK, Yang Y, Gu ML, Mao SJ, Zhou WS. Effects of Low Back Pain Exercises on Pain Symptoms and Activities of Daily Living: a Systematic Review and Meta-Analysis. Percept Mot Skills. 2022;129(1):63–89. doi:10.1177/00315125211059407
55. Stanton-Hicks M, Salamon J. Stimulation of the central and peripheral nervous system for the control of pain. J Clin Neurophysiol. 1997;14(1):46–62. doi:10.1097/00004691-199701000-00004
56. Athukorala RP, Jones RD, Sella O, Huckabee ML. Skill training for swallowing rehabilitation in patients with Parkinson’s disease. Arch Phys Med Rehabil. 2014;95(7):1374–1382. doi:10.1016/j.apmr.2014.03.001
57. Oujamaa L, Relave I, Froger J, Mottet D, Pelissier JY. Rehabilitation of arm function after stroke. Ann Phys Rehabil Med Apr. 2009;52(3):269–293. doi:10.1016/j.rehab.2008.10.003
58. Wong AYL, Karppinen J, Samartzis D. Low back pain in older adults: risk factors, management options and future directions. Scoliosis Spinal Disord. 2017;12:14. doi:10.1186/s13013-017-0121-3
59. Chodosh J, Solomon DH, Roth CP, et al. The quality of medical care provided to vulnerable older patients with chronic pain. J Am Geriatr Soc. 2004;52(5):756–761. doi:10.1111/j.1532-5415.2004.52214.x
60. Brandt KD, Dieppe P, Radin EL. Etiopathogenesis of osteoarthritis. Rheum Dis Clin North Am. 2008;34(3):531–559. doi:10.1016/j.rdc.2008.05.011
61. Osborne RH, Hawthorne G, Lew EA, Gray LC. Quality of life assessment in the community-dwelling elderly: validation of the Assessment of Quality of Life (AQoL) Instrument and comparison with the SF-36. J Clin Epidemiol. 2003;56(2):138–147. doi:10.1016/s0895-4356(02)00601-7
62. Keegan L. Therapies to reduce stress and anxiety. Crit Care Nurs Clin North Am. 2003;15(3):321–327. doi:10.1016/s0899-5885(02)00103-x
63. Tognolo L, Coraci D, Fioravanti A, et al. Clinical Impact of Balneotherapy and Therapeutic Exercise in Rheumatic Diseases: a Lexical Analysis and Scoping Review. Applied Sciences-Basel. 2022;12(15):7379. doi:10.3390/app12157379
64. Scanu A, Tognolo L, Maccarone MC, Masiero S. Immunological Events, Emerging Pharmaceutical Treatments and Therapeutic Potential of Balneotherapy on Osteoarthritis. Front Pharmacol. 2021;12681871. doi:10.3389/fphar.2021.681871
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.