Back to Journals » International Journal of Women's Health » Volume 17
The Global Burden of Polycystic Ovary Syndrome in Women of Reproductive Age: Findings from the GBD 2019 Study
Authors Jiang B
Received 9 August 2024
Accepted for publication 5 December 2024
Published 25 January 2025 Volume 2025:17 Pages 153—165
DOI https://doi.org/10.2147/IJWH.S490836
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Bengui Jiang
Department of Gynecology and Obstetrics, Ningbo University’s Women’s and Children’s Hospital, Ningbo, Zhejiang, 315000, People’s Republic of China
Correspondence: Bengui Jiang, Department of Gynecology and Obstetrics, Ningbo University’s Women’s and Children’s Hospital, Ningbo, Zhejiang, 315000, People’s Republic of China, Email [email protected]
Purpose: Polycystic ovary syndrome (PCOS) is a prevalent endocrine disorder and the primary cause of anovulatory infertility among women aged 15– 49 years. Despite its significance, it has been largely overlooked in global health discussions, with persistently high prevalence and incidence rates. This public health challenge necessitates attention both domestically and internationally. Between 1990 and 2017, the age-standardized prevalence of female infertility and associated DALYs rose by 0.70% and 0.396%, respectively. Economically, addressing women’s endocrine and metabolic health can bolster the overall well-being of the female population using existing resources. For judicious utilization of available resources, data regarding the burden of PCOS is pivotal for comprehending women’s health status and for devising and refining policies related to women’s endocrine health. Consequently, this study scrutinizes and assesses the age-standardized PCOS incidence rate and DALYs for 1990 and 2019, traces the trends of these metrics from 1990 to 2019, examines the composition of various populations and diseases, and offers international comparisons. This aims to furnish critical insights for future health policy development and adjustments in the realm of female endocrine and metabolic health.
Patients and Methods: This study employed the Global Health Data Exchange to obtain PCOS burden data based on GBD 2019. It collected incidence, DALYs, and age-standardized rates (ASRs) from 1990 to 2019 across global, regional, national, and SDI quintile levels, spanning 21 regions and 204 countries. To analyze trends, ASRs and estimated annual percentage changes (EAPCs) were calculated, with standardization crucial for comparability. EAPC was derived using a generalized linear model with a Gaussian distribution.
Results: The global burden of PCOS increased significantly from 1990 to 2019, with estimated annual percentage change (EAPCs) of 0.56 for incidence and 0.83 for DALYs. The highest incidence rates were observed in the High-income Asia Pacific region, particularly in Japan and New Zealand, while the lowest rates were in Central Europe. Equatorial Guinea and Qatar exhibited the most pronounced increases in incidence and DALYs, attributed to urbanization and enhanced healthcare infrastructure. The incidence and DALYs of PCOS showed variation across SDI quintiles, with the greatest burden found in the middle-SDI quintile. Women between the ages of 20– 29 years had the highest incidence and DALYs, emphasizing the importance of targeted interventions during this critical period. In contrast, regions with lower SDI levels, such as Central and Eastern Europe, reported the lowest burdens of PCOS, likely due to underdiagnosis and limited healthcare resources.
Conclusion: From 1990 to 2019, there was a significant increase in the global burden of PCOS, with variations seen across regions and SDI quintiles. Countries such as Italy, Japan, New Zealand, and Australia had the highest burdens, while Central and Eastern Europe had the lowest. The age group most affected was women aged 20– 29 years, emphasizing the necessity for targeted interventions.
Keywords: reproductive age, polycystic ovary syndrome, incidence, disability-adjusted life-years, socio-demographic index
Introduction
Polycystic ovary syndrome (PCOS) is a common endocrine disorder and a major cause of anovulatory infertility in women aged 15 to 49 years.1,2 Women with PCOS are at an increased risk of developing glucose intolerance and type 2 diabetes, hepatic steatosis, metabolic syndrome, hypertension, dyslipidemia, vascular thrombosis, cerebrovascular accidents, and potential cardiovascular events. Additionally, they may experience low fertility, obstetric complications, endometrial dysplasia or cancer, and possible ovarian malignancy. Emotional and psychological disorders are also common among women with PCOS.3 The etiology of PCOS is complex, involving functional disorders of multiple physiological systems, including ovarian and adrenal hyperandrogenism, neuroendocrine and hypothalamic pituitary dysfunction, and peripheral insulin resistance disorders.4 Due to the high heterogeneity of clinical manifestations of PCOS, its exact pathogenesis remains unclear. It is speculated that there are complex relationships between PCOS and genetic, metabolic, environmental, and lifestyle factors. Genetic factors may increase susceptibility to PCOS, while metabolic abnormalities, environmental chemicals, and unhealthy lifestyle habits may exacerbate or trigger this condition.5,6 Diagnosing and managing PCOS is challenging due to the variability of symptoms with age and presentation, and the use of several different diagnostic criteria. The most commonly used Rotterdam criteria (2003) require the presence of two of the following three characteristics: hyperandrogenism and/or hyperandrogenism, oligomenorrhea/amenorrhea, and polycystic ovary morphology.7 Globally, the prevalence of PCOS is estimated to range between 5% and 15%.8 Research shows that women with PCOS are at a higher risk of obesity, dyslipidemia, impaired glucose tolerance, and long-term complications like diabetes, endometrial cancer, and cardiovascular disease.9,10
Historically, monitoring efforts for the PCOS epidemic have mainly focused on documenting disease prevalence.11–13 However, the annual incidence of PCOS, which measures the rate of new cases per year, provides a more precise representation of the epidemiological changes associated with this disorder.14 The disability-adjusted life-years (DALYs), a comprehensive metric that includes premature mortality and disability, serve as a useful measure for direct comparison across various geographical regions.15
From 1990 to 2017, the age-standardized prevalence of infertility and the corresponding DALYs among women increased annually by 0.370% and 0.396%, respectively.16 As PCOS is the main cause of anovulatory infertility in women,2 it is essential to gain a better understanding of the current burden of PCOS for the primary prevention of infertility. Furthermore, from an economic perspective, enhancing women’s endocrine and metabolic health can further elevate their well-being within the existing resource constraints. In the pursuit of rational utilization of available resources, data and information regarding the burden of PCOS are vital for grasping women’s health status and formulating or adjusting health policies aimed at women’s endocrine health.
No comprehensive quantitative estimates of the incidence of PCOS and the associated DALYs by age and socio-demographic index (SDI) across various countries and territories have been published to date. Therefore, the objective of this study was to provide a detailed estimate of the age- and SDI-stratified incidence of PCOS at global, regional, and national levels using data from 204 countries and territories collected during the Global Burden of Diseases. The report presents the estimated PCOS incidence and DALYs for women of reproductive age, the age-standardized PCOS incidence and DALYs for the years 1990 and 2019, and the trends observed in these variables from 1990 to 2019, aiming to provide crucial information for the formulation and adjustment of health policies in the field of women’s endocrine and metabolic health in the future.
Materials and Methods
Summary
The Global Burden of Disease (GBD) project, led by the Institute for Health Metrics and Evaluation (IHME), provides a comprehensive assessment of the descriptive epidemiology of diseases across 21 regions and 204 countries and territories from 1990 to 2019. This initiative utilizes global collaboration to leverage all available data, making it a crucial resource for understanding the global disease burden.17 Data for the project were obtained through direct queries and downloaded from the GBD results tool, with detailed methodological descriptions available on the database help page and other publications.18 GBD gathers health data from a variety of sources, including life records, registers, censuses, health surveys, population surveillance, scientific research, administrative reports, hospital discharge records, outpatient visits, and health insurance claims. These data are then processed using algorithms to estimate the disease burden. Disease estimates in GBD studies are generated by age, year, and location using the Bayesian meta-regression tool DisMod-MR 2.1, ensuring consistency in epidemiological parameters across the conditions studied.18
Data Source
Data on the global burden of PCOS was obtained from the Global Health Data Exchange query tool. This study collected information on the incidence, DALYs, and Age-Standardized Rates (ASRs) of PCOS worldwide, broken down by global, regional, national, and SDI quintiles from 1990 to 2019 using GBD 2019. The SDI, which categorizes 21 regions and 204 countries and territories into five levels (high, high-middle, middle, low-middle, and low), is determined by factors such as total fertility rate, per capita income, and average years of education, with values ranging from 0 to 1 where higher values indicate greater socioeconomic development. It is important to note that GBD regions are analytical groupings of countries and not actual geopolitical units. Cases of PCOS were identified using the International Classification of Diseases (ICD) codes, specifically ICD-10 code E28.2 and ICD-9 code E28.2. This study was approved by Ningbo University’s Women’s and Children’s Hospital and did not involve individual participants.
Statistical Analysis
ASR and estimated annual percentage change (EAPC) were computed to measure and compare trends in the incidence and DALYs of PCOS. Standardization is crucial in removing the impact of age distribution in the population, guaranteeing the comparability of research metrics. The formula for calculating ASR (per 100,000 population) is:
where  and
and  represent specific age ratios and the number of people (or body weight) in the same age subgroup of the selected reference standard population (where
represent specific age ratios and the number of people (or body weight) in the same age subgroup of the selected reference standard population (where  represents the
represents the  -th age group), respectively, and A is the number of age groups. EAPC quantifies the trend in ASR within the designation and is calculated using a generalized linear model with a Gaussian distribution. The regression line is fitted to the natural logarithmic rate,
-th age group), respectively, and A is the number of age groups. EAPC quantifies the trend in ASR within the designation and is calculated using a generalized linear model with a Gaussian distribution. The regression line is fitted to the natural logarithmic rate,  where
where  The formula for calculating EAPC is:
The formula for calculating EAPC is:

The 95% confidence interval of EAPC was derived from the linear model. A positive EAPC along with the lower bound of its 95% Confidence Interval suggests an increasing trend in ASR, whereas a negative EAPC along with the upper bound of its 95% CI indicates a decreasing trend. If neither of these conditions are met, the ASR is deemed stable over the specified time period. The reported data includes estimates with corresponding 95% Uncertainty Intervals (UIs) where applicable.
The relationship between EAPC and ASR at the national level was investigated to determine potential influencing factors of EAPC. Statistical analyses and graphing were conducted using R software (version 4.1.0). A p-value below 0.05 was deemed statistically significant.
Results
The PCOS Burden at the Global Level
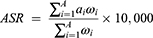
In 2019, the total number of DALYs attributed to PCOS in women of reproductive age was 28.09 million worldwide, with an EAPC of 0.83% (95% CI: 0.78 to 0.87)) (Table 1, Figure 1A and B). Additionally, there were 63.30 million incident cases of PCOS among women aged 15–49 globally, with a calculated EAPC of 0.56% (95% CI: 0.51 to 0.61) (Table 1, Figure 1C and D).
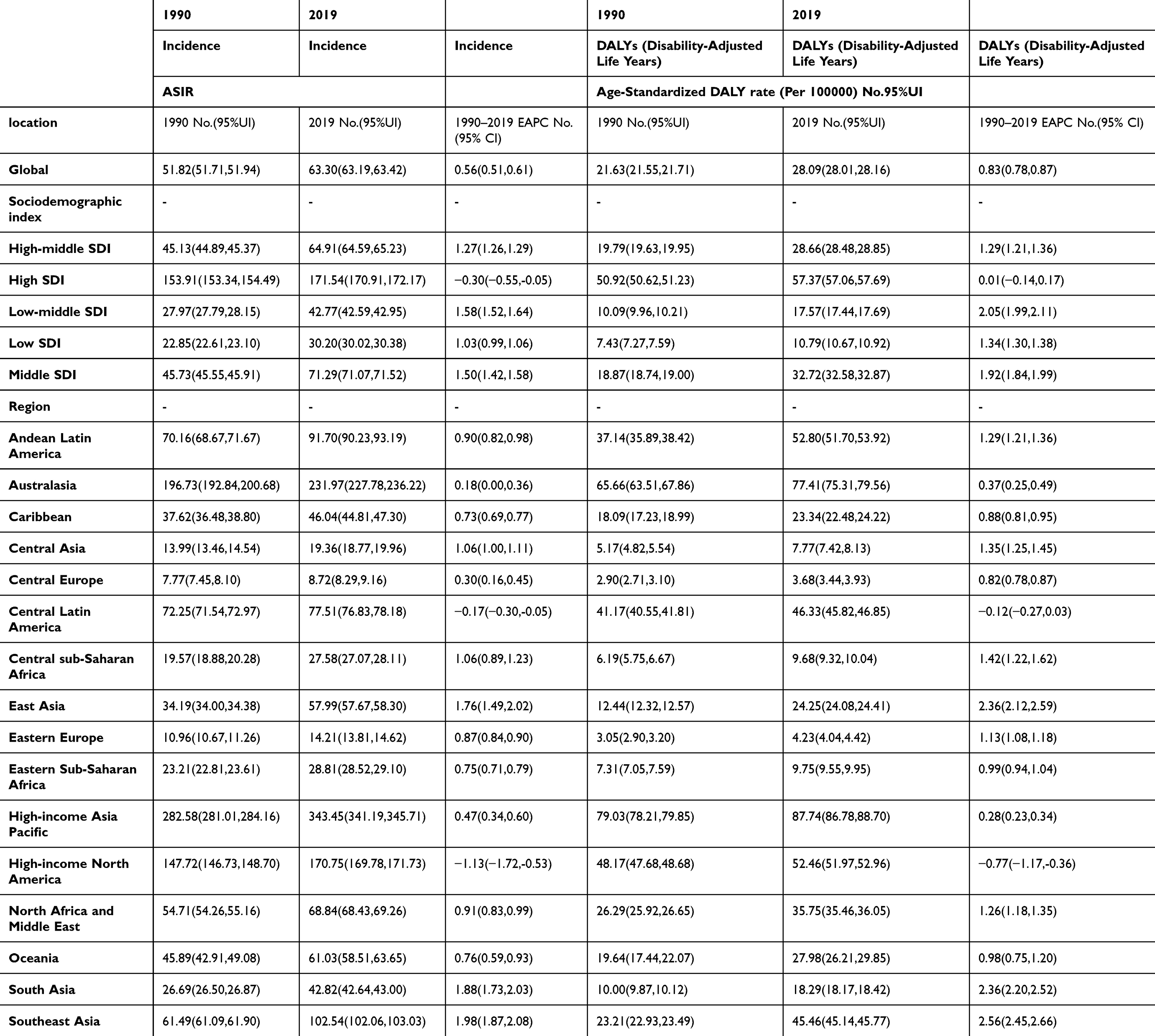 |
Table 1 Age-Standardized DALY Rate, DALYs of Polycystic Ovarian Syndrome in Women of Reproductive Age in 1990, 2019 and EAPC and Growth Proportion in DALYs Between 1990 and 2019 in Different Regions of the World |
 |
Figure 1 The ASRs and EAPC of Global Burden of PCOS by region: age-standardized DALY rate and ASIR in 2019. (A) Age-Standardized DALY Rate, (B) EAPC of Age-Standardized DALY Rate. (C) ASIR in 2019. (D) EAPC of ASIR. Abbreviations: ASIR, age-standardized Incidence rate; DALY, disability adjusted life-year; PCOS, polycystic ovary syndrome. |
The PCOS Burden at the Regional Level
In 2019, the regions with the highest age-standardized PCOS incidence rates were High-income Asia Pacific, with 343.45 (95% UI: 341.19 to 345.71) per 100,000 population, Australasia, with 231.97 (95% UI: 227.78 to 236.22) per 100,000 population, and High-income North America, with 170.75 (95% UI: 169.78 to 171.73) per 100,000 population. Conversely, Central Europe had the lowest age-standardized incidence rate, at 8.72 (95% UI: 8.29 to 9.16) per 100,000 population (Table 1; Table S1; Table S2, Figures 1C and S1B). The most significant increases in age-standardized incidence rates from 1990 to 2019 were observed in Southeast Asia, with an EAPC of 1.98 (95% CI: 1.87 to 2.08), East Asia, with an EAPC of 1.76 (95% CI: 1.49 to 2.02), and South Asia, with an EAPC of 1.88 (95% CI: 1.73 to 2.03) (Tables 1, S1 and S2; Figures 1D, S1ABE and S2ABE).
In 2019, the regions with the highest age-standardized DALY rates were High-income Asia Pacific (87.74 per 100,000 population), Australasia (77.41 per 100,000 population), and Andean Latin America (52.80 per 100,000 population). On the other hand, Central Europe had the lowest rate at 3.68 per 100,000 population. (Tables 1, S1 and S2; Figures 1A and S1D). The most significant increases in age-standardized DALY rates from 1990 to 2019 were seen in Southeast Asia, East Asia, and South Asia. In contrast, High-income North America and Central Latin America experienced decreasing trends in age-standardized DALY rates during the same period (Tables 1, S1 and S2; Figures 1, S1CDF and S2CDF).
Countries with the Highest PCOS Burdens in 2019
In 2019, Japan had the highest age-standardized incidence rate (ASIR) of PCOS at 413.50 per 100,000 people, followed by New Zealand at 255.20 per 100,000 people, and Brunei Darussalam at 242.43 per 100,000 people. Conversely, the lowest ASIRs were observed in Bosnia and Herzegovina (7.99 per 100,000 people), Albania (7.99 per 100,000 people), and North Macedonia (8.15 per 100,000 people) (Tables S3 and S4; Figures 3A, S1B and S2B).
In 2019, Italy had the highest age-standardized DALY rates for PCOS at 131.63 per 100,000 people, followed by Japan at 106.46 per 100,000 people, and New Zealand at 90.15 per 100,000 people. Conversely, the countries with the lowest age-standardized DALY rates were Bosnia and Herzegovina (3.09 per 100,000 people), Albania (3.14 per 100,000 people), and North Macedonia (3.15 per 100,000 people) (Tables S4 and S5; Figures 3B, S1D and S2D).
The incidence of PCOS cases showed the highest increases from 1990 to 2019 in Equatorial Guinea, recording an EAPC of 7.43. This was followed by Angola with an EAPC of 5.05, and Benin with an EAPC of 4.94. Conversely, countries with the smallest increases in incidence were Latvia with an EAPC of 0.67, Italy with an EAPC of 0.60, and Poland with an EAPC of 0.57 (Tables S3 and S4; Figures S1ABE and S2ABE).
From 1990 to 2019, the most significant increases in DALY cases attributed to PCOS were documented in Equatorial Guinea, exhibiting an EAPC of 8.94. Following closely were Qatar with an EAPC of 6.85 and the United Arab Emirates with an EAPC of 6.45. Conversely, the smallest increases were recorded in Latvia with an EAPC of 0.87, Japan with an EAPC of 0.85, and Italy with an EAPC of 0.84 (Tables S4 and S5; Figures S1CDF and S2CDF).
PCOS Burden by Age Group and Country
Incidence rates of PCOS varied across different countries, with Japan, New Zealand, and Brunei Darussalam showing the highest rates, particularly among women aged 20–24 years and 25–29 years. Japan had a particularly high incidence rate exceeding 400 per 100,000 population in the 20–24 age group. Australia, the United States, and Saudi Arabia also had high rates, with peaks in the 25–29 and 30–34 age groups. On the other hand, countries like Bosnia and Herzegovina, Albania, and North Macedonia consistently reported the lowest rates, below 20 per 100,000 population. The incidence of PCOS typically peaks in the 20–29 age range in most countries, highlighting a critical period for the onset of this condition. Incidence rates decline in older age groups (35–49 years), reflecting the diagnostic and clinical patterns of PCOS, which often manifest during the early reproductive years (Tables S3, S4 and S6; Figures 2A and 3A).
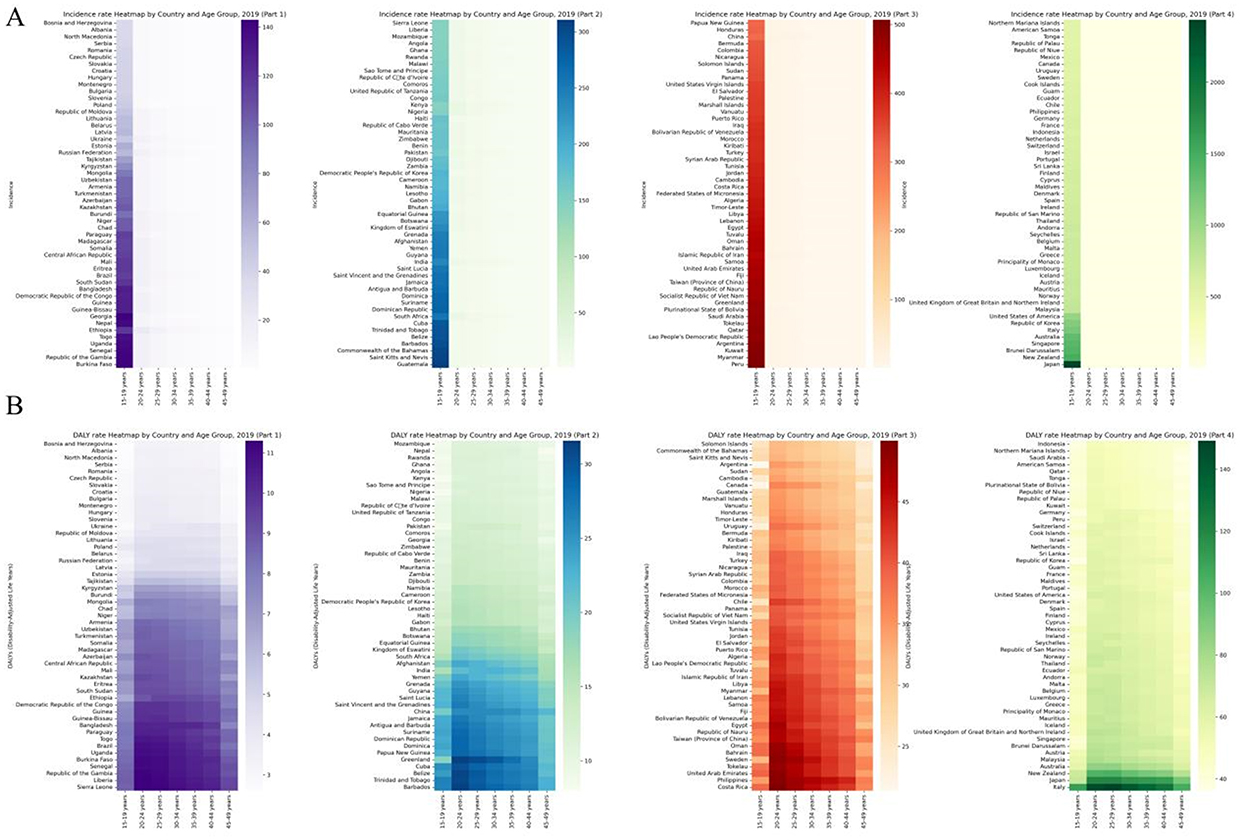 |
Figure 2 Global Heatmap of PCOS 2019 by Country and Age Group: (A) ASIR, (B) Age-Standardized DALY Rate. Abbreviations: DALY, Disability-Adjusted Life-Year; ASIR, Age-Standardized Incidence Rate; PCOS, polycystic ovary syndrome. |
 |
Figure 3 The ASIR and age-standardized DALY rate of Global Burden of PCOS in 2019 by 204 countries. (A) ASIR, (B) Age-Standardized DALY Rate. Abbreviations: ASIR, age-standardized Incidence rates; SDI, Socio-demographic Index; DALY, Disability-Adjusted Life-Year; ASRs, Age-standardized rates; PCOS, polycystic ovary syndrome. |
For DALY rates, the highest were observed in Japan, Italy, and New Zealand, particularly in the 20–24 and 25–29 age groups. Japan exhibited DALY rates exceeding 140 per 100,000 population in the 20–24 age group. Countries such as Qatar, United Arab Emirates, and Kuwait also showed high DALY rates, indicating a substantial burden of health loss related to PCOS. On the other hand, Bosnia and Herzegovina, Albania, and North Macedonia consistently reported the lowest DALY rates across all age groups, with rates below 10 per 100,000 population. The peak in DALY rates aligning with the incidence rates in the 20–29 age groups highlights the significant impact of PCOS during these reproductive years. The decrease in DALY rates in older age groups (35–49 years) suggests that the disability and health loss associated with PCOS may diminish with age or be less acknowledged and documented in older women (Tables S4, S5 and S7; Figures 2B and 3B).
The PCOS Burden at the SDI Quintile Level
The incidence cases and DALYs of PCOS showed an upward trend globally from 1990 to 2019, across all SDI subarea (Table S1, Figure S2). In 2019, the high-SDI quintile had the highest ASIR of 171.54 (95% UI: 170.91 to 172.17) per 100,000 population, while the low-SDI quintile had the lowest ASIR at 30.20 (95% UI: 30.02 to 30.38) per 100,000 population. Throughout the study period, there was an increase in ASIR among women of reproductive age in all SDI quintiles. The middle-SDI quintile experienced the highest rise in ASIR, with an (EAPC of 1.50 (95% CI: 1.42 to 1.58) from 1990 to 2019 (Tables 1 and S1, Figure 1C and D).
In 2019, the highest age-standardized DALY rate was found in the high-SDI quintile at 57.37 (95% UI: 57.06 to 57.69) per 100,000 population, while the lowest rate was observed in the low-SDI quintile at 10.79 (95% UI: 10.67 to 10.92) per 100,000 population. The age-standardized DALY rates increased across all SDI quintiles during the study period, with the most significant rise seen in the low-middle SDI quintile, displaying an EAPC of 2.05 (95% CI: 1.99 to 2.11) (Tables 1 and S1, Figure 1A and B).
From 1990 to 2019, the ASIR and DALY rates of PCOS exhibited diverse trends across different SDI quintiles. The high-SDI quintile showed fluctuations in both incidence and DALYs, whereas the middle-SDI quintile consistently had the highest ASIR and DALY rates. In contrast, the low-SDI quintile consistently maintained the lowest rates throughout the entire period (Tables 1 and S1), Among the top five countries of incidence cases and DALYs of PCOS, there is an increasing trend with the increase of SDI value, incidence cases correlation coefficient is 0.68 and DALYs correlation coefficient is 0.65, highly correlated.(Table S8, Figure 4A and B).
 |
Figure 4 Correlation in PCOS of all ages incident cases /DALYs, and SDI in only the country names for the top five in ASIR/ASDR, in 2019. (A) incident cases in 2019 by top five countries. (B) DALYs in 2019 by top five countries. Abbreviations: ASIR, age-standardized Incidence rates; SDI, Socio-demographic Index; DALY, Disability-Adjusted Life-Year; PCOS, polycystic ovary syndrome. |
Discussion
This study provides a comprehensive report on the overall and age-standardized incidence rates of PCOS and the associated DALYs among women of reproductive age globally, regionally, and nationally from 1990 to 2019. In 2019, there were 63.30 million new cases of PCOS and 28.09 million associated DALYs worldwide. In this study, we found that the age-standardized incidence rate and DALY rate increased slightly during the study period. The EAPCs were 0.56 and 0.83, respectively, and the increase was more pronounced in the middle SDI quintile group and women aged 20–29 years. Furthermore, the burden of PCOS varied greatly across countries and regions. Italy, Japan, New Zealand, and Australia had the highest burden of PCOS, while Central and Eastern Europe had a lower burden of PCOS. Previous research has not thoroughly examined the prevalence of PCOS. Various epidemiological studies have shown conflicting results, possibly because of differences in inclusion criteria, sample sizes, ethnicities, study designs, and geographic regions.12
The clinical manifestations of PCOS are markedly diverse, encompassing hyperandrogenism, infrequent or absent ovulation, and various metabolic abnormalities such as insulin resistance, obesity, type 2 diabetes, dyslipidemia, and an elevated risk of cardiovascular disease.19–21 This symptomatic heterogeneity in polycystic ovary syndrome is likely attributable to its multifaceted etiology and pathogenesis, which encompass genetic predispositions, epigenetic influences, and a range of environmental factors including race, diet, living conditions, lifestyle, and psychological determinants.22 The slight rise in PCOS prevalence could be linked to population growth, aging, and changes in diagnostic criteria over the years. The adoption of the Rotterdam criteria, a widely used diagnostic standard,23,24 led to a significant increase in PCOS cases. The escalating rates of obesity also contribute, as studies have shown a higher prevalence of PCOS among obese women.25 It is noteworthy that a considerable number of PCOS cases go undiagnosed despite multiple medical visits,13 suggesting that the true incidence of this condition might be underestimated.12
Our analysis reveals significant heterogeneity of PCOS across the globe, particularly between different SDI quintile intervals and geographic regions. The middle-SDI quintile showed the highest increase in PCOS incidence, while the low-middle SDI quintile had the highest increase in DALYs. These findings suggest better detection rates, advanced healthcare infrastructure, and greater availability of primary healthcare services in these regions. Conversely, the low-SDI quintile had the lowest age-standardized rates of PCOS incidence and DALYs, indicating lower detection rates.26 For instance, ultrasonography, a common diagnostic tool for PCOS, faces limitations in availability and affordability in Africa.27 It is crucial to enhance health resource allocation in resource-limited regions.
Regionally, the Asia Pacific region with high-income countries had the highest age-standardized PCOS incidence and DALYs, with Japan and New Zealand making significant contributions. The presence of comprehensive health service systems in these nations, coupled with the adoption of updated diagnostic criteria and extensive utilization of healthcare services, played a key role in these elevated rates. In contrast, Central Europe recorded the lowest age-standardized incidence and DALYs, potentially attributable to limited healthcare accessibility and lower rates of detection.26
Notably, the burden of PCOS also shows time-series heterogeneity across countries and regions. Countries like Equatorial Guinea and Qatar experienced substantial increases in PCOS incidence and DALYs between 1990 and 2019, driven by factors such as urbanization, lifestyle modifications, and enhanced healthcare infrastructure.28 Conversely, countries like Latvia and Italy displayed minimal increases, likely due to the stability of their healthcare systems and less pronounced changes in lifestyle factors.28 Urbanization often leads to lifestyle changes such as decreased physical activity and increased consumption of calorie-dense foods, both of which are risk factors for obesity and metabolic disorders like PCOS. Improved healthcare infrastructure and increased availability of diagnostic facilities in these countries have likely led to higher detection rates of PCOS, reflecting a shift in disease burden recognition. Conversely, countries like Latvia and Italy showed minimal increases. In Latvia, the stability may be due to a combination of stable healthcare systems and less significant lifestyle changes.28 The healthcare systems in these countries might already be adept at managing PCOS, resulting in a consistent but not rapidly increasing detection rate. Additionally, public health initiatives aimed at managing obesity and promoting healthy lifestyles could have mitigated potential increases in PCOS prevalence. Italy, despite its advanced healthcare system, showed minimal increases, potentially due to effective public health policies and a well-established healthcare infrastructure that has been consistently managing PCOS over the years. Additionally, Italy’s Mediterranean diet, which is high in fruits, vegetables, and healthy fats, might contribute to lower obesity rates, thereby indirectly affecting the prevalence of PCOS.
The relationship between SDI and PCOS burden suggests that as SDI increases, the incidence cases and DALYs initially increase, This linear correlation underscores the intricate interplay between socioeconomic factors and disease burden. Enhanced healthcare access and improved diagnostic capabilities are likely contributing factors to the higher detection rates of PCOS with increasing SDI.29
The stability of the global age-standardized PCOS incidence and DALYs over time suggests that the epidemiology of PCOS has not drastically changed. However, the variability and inconsistency between different diagnostic criteria pose significant challenges to accurately estimating PCOS incidence. As PCOS manifests differently across ethnic groups, establishing ethnicity-specific guidelines is crucial for enhancing screening, diagnostic outcomes, management priorities, and treatment responses.
This study represents the first comprehensive assessment of PCOS incidence and DALYs globally, regionally, and nationally using data from GBD 2019. The use of DALYs enables direct comparisons across diverse regions and countries. Additionally, PCOS incidence and DALYs were estimated based on the SDI, which was refined in GBD 2019 to provide a more accurate reflection of each country’s development status. Exploring the heterogeneity of disease burden across different countries and regions aids public health policymakers in more precisely allocating medical resources and formulating prevention and control strategies, thereby mitigating the overall societal burden of PCOS. Furthermore, through enhanced international cooperation and exchange, we can collectively address this global health challenge.
The GBD 2019 study aimed to collect all available data, but some regions had limited data availability, leading to widely estimated UIs. The study also relied on increased hospital medical records, potentially introducing selection bias towards individuals accessing healthcare services. Evaluating the PCOS phenotype is complex and involves various procedures such as clinical and laboratory assessments, pelvic ultrasonography, and multiple clinic visits, which could result in underestimating PCOS incidence. Detection bias may inflate PCOS incidence estimates in regions with better healthcare access and health awareness, cautioning resource allocation in these “high-risk” areas. Furthermore, the evolving diagnostic criteria contribute to inconsistencies in determining PCOS incidence.
Conclusion
From 1990 to 2019, the global disease burden of PCOS increased, with incident cases, DALYs, and corresponding ASRs all showing an upward trend. This rise was particularly pronounced in the middle-SDI quintile and among women aged 20–29 years, underscoring the importance of targeted interventions during these reproductive years. Countries like Italy, Japan, New Zealand, and Australia had the highest PCOS burdens, reflecting advanced healthcare systems and improved diagnostic practices. In contrast, Central and Eastern Europe reported lower PCOS burdens, possibly due to underdiagnosis and limited healthcare resources. The significant disparities in PCOS incidence and DALYs between regions highlight the need for tailored health interventions and better resource allocation. Future research should concentrate on regions with the most severe PCOS burdens to identify the contributing factors. Standardizing diagnostic criteria and enhancing global healthcare access are essential steps in managing and reducing the burden of PCOS.
Data Sharing Statement
This data is publicly available at the GBD 2019 (https://vizhub.healthdata.org/gbd-results/).
Ethics Approval and Consent to Participate
This study was approved by Ningbo University’s Women’s and Children’s Hospital and did not involve individual participants.
Acknowledgments
We thank all authors for their contributions to the article.
Funding
This study was supported by Ningbo Clinical Medical Research Centre for Gynaecological Diseases (2024L002).
Disclosure
The author reports no conflicts of interest in this work.
References
1. Szilágyi A, Szabó I. Endocrine characteristics of polycystic ovary syndrome (PCOS). Indian J Exp Biol. 2003;41(7):694–700.
2. Balen AH, Morley LC, Misso M, et al. The management of anovulatory infertility in women with polycystic ovary syndrome: an analysis of the evidence to support the development of global WHO guidance. Hum Reprod Update. 2016;22(6):687–708. doi:10.1093/humupd/dmw025
3. Azziz R. Polycystic ovary syndrome. Obstetrics Gynecol. 2018;132(2):321–336. doi:10.1097/AOG.0000000000002698
4. Glueck CJ, Goldenberg N. Characteristics of obesity in polycystic ovary syndrome: etiology, treatment, and genetics. Metabolism. 2019;92:108–120. doi:10.1016/j.metabol.2018.11.002
5. Rosenfield R, Ehrmann DA. The pathogenesis of polycystic ovary syndrome(PCOS):the hypothesis of PCOS as functional ovarian hyperandrogenism revisited[J]. Endocr Rev. 2016;37:467–520. doi:10.1210/er.2015-1104
6. Bellver R-TL, Robles A, Robles A. et al. Polycystic ovary syndrome throughout a woman’s life. J Assist Reprod Genet. 2018;35:25–39. doi:10.1007/s10815-017-1047-7
7. Huffman AM, Rezq S, Basnet J, Romero DG. Biomarkers in polycystic ovary syndrome. Curr Opin Physiol. 2023;36:100717. doi:10.1016/j.cophys.2023.100717
8. Azziz R. Introduction: determinants of polycystic ovary syndrome. Fertil Steril. 2016;106(1):4–5. doi:10.1016/j.fertnstert.2016.05.009
9. Lim SS, Davies MJ, Norman RJ, Moran LJ. Overweight, obesity and central obesity in women with polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod Update. 2012;18(6):618–637. doi:10.1093/humupd/dms030
10. Wild RA. Dyslipidemia in PCOS. Steroids. 2012;77(4):295–299. doi:10.1016/j.steroids.2011.12.002
11. Yildiz BO, Bozdag G, Yapici Z, Esinler I, Yarali H. Prevalence, phenotype and cardiometabolic risk of polycystic ovary syndrome under different diagnostic criteria. Hum Reprod. 2012;27(10):3067–3073. doi:10.1093/humrep/des232
12. Ding T, Hardiman PJ, Petersen I, Wang FF, Qu F, Baio G. The prevalence of polycystic ovary syndrome in reproductive-aged women of different ethnicity: a systematic review and meta-analysis. Oncotarget. 2017;8(56):96351–96358. doi:10.18632/oncotarget.19180
13. Wolf WM, Wattick RA, Kinkade ON, Olfert MD. Geographical prevalence of polycystic ovary syndrome as determined by region and Race/Ethnicity. Int J Environ Res Public Health. 2018;15(11):2589. doi:10.3390/ijerph15112589
14. Dicker RC, Heisey-Grove D, Beach M, Dicker RC, Matyas BT. Principles of epidemiology. Epidemiol Infect. 2006;134:935–941. doi:10.1017/S0950268805005832
15. Capone A. Towards an effective assessment of the sustainability of health interventions. Ig Sanita Pubbl. 2019;75(3):189–199.
16. Sun H, Gong TT, Jiang YT, Zhang S, Zhao YH, Wu QJ. Global, regional, and national prevalence and disability-adjusted life-years for infertility in 195 countries and territories, 1990–2017: results from a global burden of disease study, 2017. Aging. 2019;11(23):10952–10991. doi:10.18632/aging.102497
17. Murray, Abbafati C, Abbas KM, et al. Five insights from the global burden of disease study 2019. Lancet. 2020;396(10258):1135–1159. doi:10.1016/s0140-6736(20)31404-5
18. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/s0140-6736(20)30925-9
19. Witchel SF, Teede HJ, Peña AS. Curtailing PCOS. Pediatr Res. 2020;87(2):353–361. doi:10.1038/s41390-019-0615-1
20. Zeng X, Xie YJ, Liu YT, Long SL, Mo ZC. Polycystic ovarian syndrome: correlation between hyperandrogenism, insulin resistance and obesity. Clin Chim Acta. 2020;502:214–221. doi:10.1016/j.cca.2019.11.003
21. Bahri Khomami M, Teede HJ, Joham AE, Moran LJ, Piltonen TT, Boyle JA. Clinical management of pregnancy in women with polycystic ovary syndrome: an expert opinion. Clin Endocrinol. 2022;97(2):227–236. doi:10.1111/cen.14723
22. Wang J, Wu D, Guo H, Li M. Hyperandrogenemia and insulin resistance: the chief culprit of polycystic ovary syndrome. Life Sci. 2019;236:116940. doi:10.1016/j.lfs.2019.116940
23. Eshre. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Sterility. 2004;81(1):19–25. doi:10.1016/j.fertnstert.2003.10.004
24. Miazgowski T, Martopullo I, Widecka J, Miazgowski B, Brodowska A. National and regional trends in the prevalence of polycystic ovary syndrome since 1990 within Europe: the modeled estimates from the global burden of disease study 2016. Arch Med Sci. 2021;17(2):343–351. doi:10.5114/aoms.2019.87112
25. Mu L, Zhao Y, Li R, Lai Y, Chang HM, Qiao J. Prevalence of polycystic ovary syndrome in a metabolically healthy obese population. Int J Obstet Gynaecolo. 2019;146(2):164–169. doi:10.1002/ijgo.12824
26. Motlagh Asghari K, Nejadghaderi SA, Alizadeh M, et al. Burden of polycystic ovary syndrome in the Middle East and North Africa region, 1990–2019. Sci Rep. 2022;12(1):7039. doi:10.1038/s41598-022-11006-0
27. Safiri S, Noori M, Nejadghaderi SA, et al. Prevalence, incidence and years lived with disability due to polycystic ovary syndrome in 204 countries and territories, 1990-2019. Hum Reprod. 2022;37(8):1919–1931. doi:10.1093/humrep/deac091
28. Liu J, Wu Q, Hao Y, et al. Measuring the global disease burden of polycystic ovary syndrome in 194 countries: global burden of disease study 2017. Hum Reprod. 2021;36(4):1108–1119. doi:10.1093/humrep/deaa371
29. Wan Z, Zhao J, Ye Y, et al. Risk and incidence of cardiovascular disease associated with polycystic ovary syndrome. Eur J Prev Cardiol. 2024. doi:10.1093/eurjpc/zwae066
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Global Burden of Appendicitis in 204 Countries and Territories from 1990 to 2019
Yang Y, Guo C, Gu Z, Hua J, Zhang J, Qian S, Shi J
Clinical Epidemiology 2022, 14:1487-1499
Published Date: 13 December 2022