")
Back to Journals » Journal of Pain Research » Volume 17
The Emotion Regulation of Acupuncture in Chronic Low Back Pain: A Clinical Neuroimaging Protocol
Authors Lai P, Cheng S, Chen X, Cheng F, Cheng J, Xin M, Zhu D, Li Z, Wu X, Zeng F
Received 1 December 2023
Accepted for publication 23 February 2024
Published 1 March 2024 Volume 2024:17 Pages 817—825
DOI https://doi.org/10.2147/JPR.S450589
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Peng Lai,1,2,* Shirui Cheng,1,2,* Xingyao Chen,1 Fangdong Cheng,3– 5 Jun Cheng,3– 5 Ming Xin,3,4,6 Deliang Zhu,3,4,6 Zhengjie Li,1,2 Xi Wu,1 Fang Zeng1,2
1Acupuncture and Tuina School, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 2Acupuncture & Brain Research Center, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 3Geriatric Diseases Institute of Chengdu, Chengdu Fifth People’s Hospital (The Second Clinical Medical College, Affiliated Fifth People’s Hospital of Chengdu University of Traditional Chinese Medicine), Chengdu, Sichuan, People’s Republic of China; 4Cancer Prevention and Treatment Institute of Chengdu, Chengdu Fifth People’s Hospital (The Second Clinical Medical College, Affiliated Fifth People’s Hospital of Chengdu University of Traditional Chinese Medicine), Chengdu, Sichuan, People’s Republic of China; 5Department of Orthopedic, Chengdu Fifth People’s Hospital (The Second Clinical Medical College, Affiliated Fifth People’s Hospital of Chengdu University of Traditional Chinese Medicine), Chengdu, Sichuan, People’s Republic of China; 6Department of Rehabilitation, Chengdu Fifth People’s Hospital (The Second Clinical Medical College, Affiliated Fifth People’s Hospital of Chengdu University of Traditional Chinese Medicine), Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fang Zeng; Xi Wu, Email [email protected]; [email protected]
Introduction: Acupuncture is effective for patients with chronic low back pain (CLBP), which can relieve pain intensity and regulate negative emotional states such as pain-related anxiety and depression. Previous studies mainly discuss the analgesic mechanism of acupuncture treatment of CLBP, but there are multiple dimensions to pain, including sensation, emotion and cognition. Therefore, this study aims to investigate the central mechanism of acupuncture for CLBP from the perspective of emotional regulation by functional magnetic resonance imaging (fMRI).
Methods and Analysis: A total of 72 patients with CLBP will be recruited in the study and randomly assigned to the verum acupuncture group or the sham acupuncture group. The trail will last for 18 weeks including a 2-week baseline, a 4-week treatment and a 12-week for follow-up period. The primary outcomes are the visual analog scale (VAS) and the Japanese Orthopaedic Association Scores (JOA) score. The secondary outcomes are the 12-item short form health survey (SF-12), the state trait anxiety inventory (STAI), the self-rating anxiety scale (SAS) and self-rating depression scale (SDS). The VAS, JOA, STAI SAS and SDS will be collected at baseline, week 2, week 4, and after follow-up. The SF-12 will be evaluated at baseline, week 2 and week 4. Functional magnetic resonance imaging (MRI) data will be collected at baseline and the end of treatment. Emotion-related brain regions will be chosen as regions of interest (ROIs). The gray matter volume (GMV), amplitude of low-frequency fluctuation (ALFF), regional homogeneity (ReHo), functional connectivity (FC), and large-scale functional brain network based on these ROIs will be analyzed within and between the two groups.
Discussion: This study will verify the emotional regulation of acupuncture and explore the mechanism of acupuncture for emotion regulation in patients with CLBP.
Trial Registration Number: https://www.chictr.org.cn/showproj.html?proj=195486, identifier: ChiCTR2300070557.
Keywords: acupuncture, chronic low back pain, emotion regulation, functional magnetic resonance imaging
Introduction
Chronic low back pain (CLBP) mainly refers to long-term pain that lasts for more than three months, usually accompanied by discomfort, tightness, or stiffness in the area below the ribs and above the buttocks.1,2 CLBP is second only to lung cancer and ischemic heart disease in terms of disability-adjusted life years,3 which impacts approximately 10–13% of the adult population, accounting for over 30 million people in the United States.4 It is a major health problem with significant economic and social implications, accounting for more than 80% of healthcare expenditure,5 with an average annual expenditure $34 billion.6
According to the clinical practice guideline of the American College of Physicians (ACP), current pharmacotherapies for CLBP include non-steroidal anti-inflammatory drugs (NSAIDs), opioid analgesics, nonopioid analgesics, tramadol, antidepressants, benzodiazepines, corticosteroids, antiepileptic drugs, and so on.2 However, pharmacological therapies are often accompanied by undesirable side effects.2,7–11 Acupuncture, a widely used complementary and alternative therapy, has been strongly recommended as initially select nonpharmacologic treatment for CLBP,2 which not only can reduce the pain intensity of patients with CLBP significantly,12–14 but also can improve the functions of lumbar CLBP patients.14
The central mechanism in patients with CLBP plays an important role in the overall pain state.15,16 Many neuroimaging studies have shown that patients with CLBP had increased gray matter volume in the primary somatosensory cortex,17 amygdala,18 and anterior cingulate cortex (ACC),19 and altered functional activity in insula, superior parietal lobes,20 cerebellum and parahippocampus.21 Acupuncture can decrease the gray matter volume of primary somatosensory cortex,17 and regulate the functional activities of the insula,21 and ventral tegmental area22 in CLBP patients. Current studies mainly discuss the analgesic mechanism of acupuncture treatment of CLBP.23–25 However, according to the International Association for the Study of Pain (IASP) definition of pain, pain encompasses multiple dimensions such as sensation, emotion, and cognition.26 The regulation of negative emotions through acupuncture significantly contributes to its analgesic effects.27 However, the central mechanisms of acupuncture for CLBP from the perspective of emotional regulation remain unknown. Hence, the objective of this study is to investigate the central mechanism of acupuncture for CLBP from the perspective of emotional regulation.
Function magnetic resonance imaging (fMRI) can generate a three-dimensional map of regional brain activity with sub-millimeter spatial resolution28 and can make precise spatial localization of brain activity. It is a commonly used technique to investigate the central mechanism of acupuncture for chronic pain.29,30 The fMRI technology mainly measures changes in the ratio of deoxyhemoglobin and oxygenated hemoglobin in the blood and has the advantages of non-invasiveness and high spatial and temporal resolution, which allows it to clearly observe these brain regions31 and provide insights into the cerebral emotional-regulation mechanisms underlying acupuncture treatment for CLBP.
Methods and Analysis
Study Design
A randomized parallel-group randomized clinical trial will be conducted at the Fifth People’s Hospital of Chengdu and Affiliated Hospital of Chengdu University of Traditional Chinese Medicine. Seventy-two eligible patients diagnosed with CLBP according to the clinical guideline of the ACP and the Chinese Association of Rehabilitation Medicine (CARM)32 will be enrolled. The study will be conducted over a total duration of 18 weeks, comprising a 2-week baseline period, a 4-week treatment period, and a 12-week follow-up period. Functional MRI data will be collected at the baseline and the end of treatment. The clinical outcomes will be evaluated after 2-week treatment, after 4-week treatment and the end of follow-up. The flow diagram of this study is displayed in Figure 1. Emotion-related brain regions, such as amygdala, insula, and ACC, will be chosen as regions of interest (ROIs). The gray matter volume (GMV), amplitude of low-frequency fluctuation (ALFF), regional homogeneity (ReHo), functional connectivity (FC), and large-scale functional brain network based on these ROIs will be analyzed.
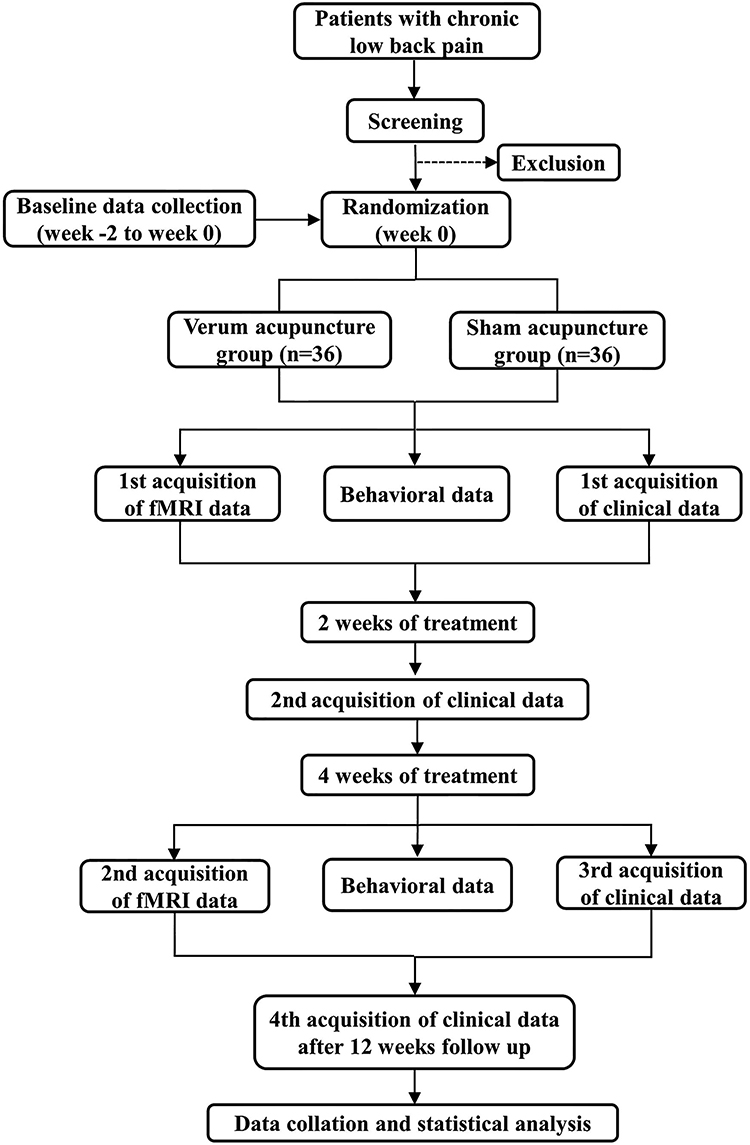 |
Figure 1 Study flowchart. |
This trial adheres to the Standard Protocol Recommendations for Interventional Trials (SPIRIT) guidelines33 (Table 1), and adheres to the principles outlined in the Comprehensive Standards for Trial Reports (CONSORT) and the Reporting Standards for Intervention Measures in Traditional Chinese Medicine Clinical Trials, as well as the Standard for Reporting Intervention Measures in Acupuncture Clinical Trials (STRICTA).34 The study has been approved by the Medical Ethics Committee of Affiliated Hospital of Chengdu University of Traditional Chinese Medicine (2023KL-120) and the Ethics Committee of the Fifth People’s Hospital of Chengdu (Ethics 2023–003 (Section) −01), which registered with on Chinese Clinical Trial Registry (registration no. ChiCTR2300070557). This trial will be conducted according to the Declaration of Helsinki.
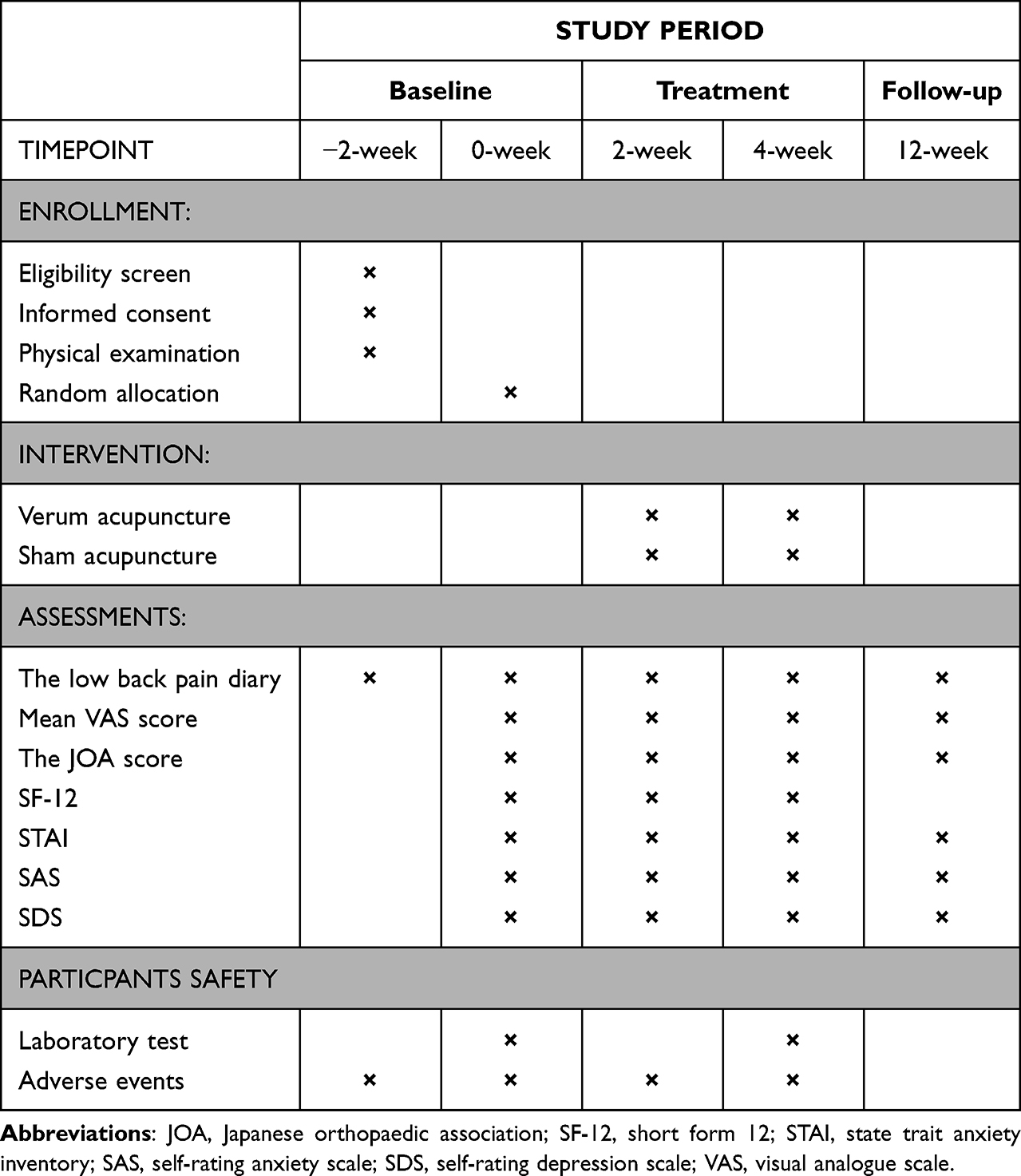 |
Table 1 Standard Protocol Items: Recommendations for Interventional Trails (SPIRIT) Schedule of the Trial |
Participant
Sample Size Considerations
The calculation for sample size is determined based on the changes in visual analogue scale (VAS) scores. An earlier study intervention on patients with CLBP found that the average improvement of VAS score in the experience group was −26.41 ± 19.06 (mean ± SD), while in the placebo group, the average improvement of VAS score was −12.83 ± 19.45 (mean ± SD).35 With a power of 0.90 and a two side of significance level of 0.05, the required sample size is 32 cases per group (the radio 1:1). Considering a dropout rate of 10%, this trial will require a total of 72 subjects.
Recruitment
All potential CLBP patients will be recruited by the outpatient of Rehabilitation Department and Pain Department of Chengdu Fifth People’s Hospital and Affiliated Hospital of Chengdu University of Traditional Chinese Medicine from November 2023 to September 2025. All participants will sign the informed consent forms at the beginning of this trial and meet all the following inclusion criteria will be recruited in this study: (1) have a diagnosis of CLBP according to the guidelines of ACP 2007 and CARM 2016; (2) fall within the age range of 18 to 55 years old (including 18 and 55 years old); (3) are right-handed; (4) have a minimum VAS score of 4 points; (5) have signed the informed consent form.
If participants who meet any of the following criteria will be excluded: (1) have taken any medication or received any non-pharmaceutical therapies within the past month; (2) have suffered from lumbar spinal stenosis, lumbar spondylolisthesis, purulent spondylitis, intervertebral disc infection, spinal trauma; (3) have metabolic diseases, urinary system diseases, neurological disorders, vascular diseases, psychogenic diseases; (4) have contraindications to magnetic resonance imaging, such as metal dentures, claustrophobia.
Randomization and Blinding
Seventy-two random sequence numbers will be generated by using a computer according to the random number table method. All eligible participants will be randomly assigned to the verum acupuncture group or the sham acupuncture group. Since it is difficult to blind acupuncture therapists in this study, we will implement blinding measures for the participants. Study assessments and statistical analysis will be performed by an independent assessor and a statistician who are unaware of the group allocation.
Interventions
The acupuncture procedures will be administered by two licensed acupuncturists with a minimum of five-year clinical experience. Bilateral Shenshu (BL23), bilateral Dachangshu (BL25), Mingmen (GV4), Yaoyangguan (GV3), and two Ashi acupoints will be chosen as acupuncture prescription. The Ashi point will be detected from the low back region. If the patient does not have Ashi acupoint, the bilateral Yaoyan (EX-B7) will be used as a substitute. Each participant will undergo a total of 12 acupuncture sessions, scheduled three times a week over a period of 4 weeks. The detailed information regarding the location of the acupoints is presented in Figure 2.
 |
Figure 2 Locations of acupoints. Shenshu (BL23): On the back, 1.5 cun lateral to the lower border of the spinous process of the 2nd lumbar vertebra. Dachangshu (BL25): On the back, 1.5 cun lateral to the lower border of the spinous process of the 4th lumbar vertebra. Mingmen (GV4): In the lumbar region, on the posterior median line, in the depression below the spinous process of the 2nd lumbar vertebra. Yaoyangguan (GV3): On the lumbar region, on the posterior median line, in the depression below the spinous process of the 4th lumbar vertebra. Yaoyan (EX-B7): On the lower back, in the depression 3.5 cun lateral to the lower border of the spinous process of the 1st lumbar vertebra. |
Verum Acupuncture Group
The verum acupuncture procedure will be performed as follows: First, the skin will be thoroughly disinfected. The acupuncturist will remove the skin-facing adhesive ring from the Park Sham placebo Acupuncture Device (PSD; Suzhou, China), insert a disposable sterile filiform needles (0.25mm × 40mm; Hwatuo, Suzhou, China) and fix the plastic cannula to the skin of the acupuncture point. During the insertion, the needles will be inserted for 0.5–1.5 cun and manipulated using uniform twirling, lifting and thrusting to elicit a deqi sensation.36 The twisting angle is 90–360 degrees, and the rotation frequency is 120–160 times per minute. The needles will be kept for 30 minutes, with additional manipulation performed twice for 10–15 seconds every 10 minutes during this period.
Sham Acupuncture Group
In the sham acupuncture group, the treatment procedure and duration are the same as in the verum acupuncture group. However, when the needles (0.25mm × 40mm; blunt tip, Womeida Medical Equipment Technology Co., Ltd., China) touch the skin, it will leverage force to retract into the hollow plastic sheath, preventing penetration into the skin, and no manipulation will be performed to elicit a deqi sensation. The needles will be kept for 30 minutes.
Medications
During the trial period, it is recommended that participants avoid using any additional medications as much as possible. If participants experience intolerable low back pain, they can temporarily take NSAIDS such as ibuprofen (approval number: GYZZ H10900089, manufacturer: Sino-US Tianjin Shike Pharmaceutical Co., Ltd.)
Functional MRI Data Acquisition
The MRI data of participants will be collected at the Chengdu Fifth People’s Hospital using a 3.0 Tesla magnetic resonance scanner (Siemens, Munich, Germany). During the scanning process, each patient needs to keep their head still, close their eyes, avoid thinking about anything, relax their body, and remain calm.
Three-dimensional T1-weighted (3D-T1) structural imaging: Before conducting a resting state scan, all participants will complete a 3D-T1 structural imaging scanning. The scanning parameters are as follows: repeat time (TR) = 1900ms, echo time (TE) = 2.74ms, and field of view (FOV) = 256 × 256mm2, matrix = 256 × 256.
Blood oxygen-level-dependent functional magnetic resonance imaging (BOLD fMRI): Gradient Echo Planar Imaging (GRE-EPI) sequence will be used during the resting state scan. Scanning parameters: TR = 2000ms, TE = 30ms, flip angle (FA) = 90°, number of layers = 32, layer thickness = 5mm, FOV = 240 × 240mm2, matrix = 64 × 64.
Outcome Measurements
Primary Outcome
Visual Analogue Scale will be used to assess the pain intensity of each patient.37 A score of 0 represents painlessness, and 10 represents the most severe unbearable pain. Japanese Orthopaedic Association (JOA) score with a maximum score of 29 points will be used to elevate the lumbar spine function of patients with CLBP.38
Secondary Outcome
Twelve-item short form health survey (SF-12), including 12 items and 8 dimensions, will be used to evaluate the relevant quality of life of patients. State trait anxiety inventory (STAI), consisting of a state anxiety inventory and a trait anxiety inventory, will be used to calculate the cumulative scores of the state anxiety and trait anxiety scales separately. The self-rating anxiety scale (SAS)39 and self-rating depression scale (SDS)40 are often used to assess the anxiety41 and depression symptoms42 of CLBP patients.
Data Analysis
All data will undergo statistical analysis employing SPSS software (version 25.0, IBM SPSS, New York, USA). The significance level will be set at α < 0.05, using a two-sided test. Categorical variable will be expressed as rates or proportions, while continuous variables will be represented as mean ± standard deviation (SD). The distribution of continuous variables will be initially assessed using the Kolmogorov–Smirnov test. For normally distributed data, a paired t-test will be employed to compare the pre- and post-treatment within each group, and a one-way analysis of variance (ANOVA) will be used for comparisons between different groups. Additionally, for non-normally distributed data, non-parametric tests will be performed to compare the pre- and post-treatment differences within each group, and multiple non-parametric tests for independent samples will be used to for between-group comparisons. The chi-square test will be used for categorical data.
Functional MRI Data Preprocessing and Analysis
Imaging data will be processed using SPM12 (http://www.fil.ion.ucl.ac.uk/spm) on MATLAB (2018, The Math-Works Inc. Natick, MA, USA). All functional images will go through slice time correction, realignment, and registration with their mean image. Then, the functional volumes will be aligned to the standardized Montreal Neurological Institute (MNI) template for spatial normalization. Moreover, the acquired data will be smoothed using an isotropic Gaussian kernel with a Full Width at Half Maximum (FWHM) of 8 mm.
The amygdala, prefrontal cortex (PFC), and anterior cingulate cortex (ACC) will be chosen as regions of interest (ROIs). The gray matter volume (GMV), amplitude of low-frequency fluctuation (ALFF), regional homogeneity (ReHo), functional connectivity (FC), and large-scale functional brain network based on these ROIs will be analyzed within and between the two groups. The relationship between brain structural and functional alterations and clinical variables will be evaluated using Pearson’s correlation analysis.
Discussion
The regulation of functional activities of various emotion-related brain regions, including the amygdala, insula, ACC, medial prefrontal cortex, hippocampus, and other brain regions might be one of the underlying mechanisms of acupuncture.21,22,43 Previous studies have established that acupuncture exerts a positive impact on negative emotional states in individuals suffering from chronic neck or shoulder pain.44,45 Hence, this study will be designed to verify the emotional regulation of acupuncture in patients with CLBP, and explore the underlying mechanism of acupuncture based on emotion-related brain regions using the fMRI technology.
Limitation
This study exists a few limitations. First, we are unable to blind acupuncturists, so we adopted the principle of separating researchers, evaluators, and analysis groups. Second, ensuring consistent application of acupuncture techniques poses a formidable challenge for different acupuncturists. Hence, both acupuncturists will undergo rigorous and standardized acupuncture manipulation training prior to this trial.
Trial Status
This clinical trial has been registered on the Chinese Clinical Trial Registry (https://www.chictr.org.cn) on April 17, 2023 (registration no. ChiCTR2300070557); protocol version no. 1.0). Patient recruitment was started on November 20, 2023.
Ethics Statement
This study was reviewed and approved by Review Boards and Medical Ethics Committee of Affiliated Hospital of Chengdu University of Traditional Chinese Medicine (2023KL-120) and Ethics Committees of Chengdu Fifth People’s Hospital (Ethics 2023-003 (Section) −01).
Acknowledgments
Peng Lai and Shirui Cheng are co-first authors for this study. The authors thank Yucai Luo and Zilei Tian for study protocol design assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is financially supported by the National Natural Science Foundation of China (No. 82205288), China Postdoctoral Science Foundation (No. 2021MD703796), Sichuan Science and Technology Program (No. 2022NSFSC0856), Medical Technology Project of Health Commission of Sichuan Province (No. 21PJ110). The funders did not play any role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368–2383. doi:10.1016/s0140-6736(18)30489-6
2. Qaseem A, Wilt TJ, McLean RM, et al. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American college of physicians. Ann Intern Med. 2017;166(7):514–530. doi:10.7326/m16-2367
3. Mokdad AH, Ballestros K, Echko M, et al. The state of US health, 1990–2016: burden of diseases, injuries, and risk factors among US states. JAMA. 2018;319(14):1444–1472. doi:10.1001/jama.2018.0158
4. Shmagel A, Foley R, Ibrahim H. Epidemiology of chronic low back pain in US adults: data from the 2009–2010 national health and nutrition examination survey. Arthritis Care Res. 2016;68(11):1688–1694. doi:10.1002/acr.22890
5. Maher CG. Effective physical treatment for chronic low back pain. Orthop Clin North Am. 2004;35(1):57–64. doi:10.1016/s0030-5898(03)00088-9
6. Institute of Medicine Committee on Advancing Pain Research C, Education. The National Academies Collection: reports funded by National Institutes of Health. In: Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. National Academy of Sciences; 2011.
7. Enthoven WT, Roelofs PD, Deyo RA, van Tulder MW, Koes BW. Non-steroidal anti-inflammatory drugs for chronic low back pain. Cochrane Database Syst Rev. 2016;2(2):CD012087. doi:10.1002/14651858.CD012087
8. Machado GC, Maher CG, Ferreira PH, Day RO, Pinheiro MB, Ferreira ML. Non-steroidal anti-inflammatory drugs for spinal pain: a systematic review and meta-analysis. Ann Rheum Dis. 2017;76(7):1269–1278. doi:10.1136/annrheumdis-2016-210597
9. Baldo BA. Opioid analgesic drugs: misuse, toxicity, and hypersensitivity. J Allergy Clin Immunol Pract. 2017;5(6):1607–1608. doi:10.1016/j.jaip.2017.04.028
10. Chaparro LE, Furlan AD, Deshpande A, Mailis-Gagnon A, Atlas S, Turk DC. Opioids compared to placebo or other treatments for chronic low-back pain. Cochrane Database Syst Rev. 2013;(8):Cd004959. doi:10.1002/14651858.CD004959.pub4
11. Baldo BA. Toxicities of opioid analgesics: respiratory depression, histamine release, hemodynamic changes, hypersensitivity, serotonin toxicity. Arch Toxicol. 2021;95(8):2627–2642. doi:10.1007/s00204-021-03068-2
12. Cho YJ, Song YK, Cha YY, et al. Acupuncture for chronic low back pain: a multicenter, randomized, patient-assessor blind, sham-controlled clinical trial. Spine. 2013;38(7):549–557. doi:10.1097/BRS.0b013e318275e601
13. Leibing E, Leonhardt U, Köster G, et al. Acupuncture treatment of chronic low-back pain -- a randomized, blinded, placebo-controlled trial with 9-month follow-up. Pain. 2002;96(1–2):189–196. doi:10.1016/s0304-3959(01)00444-4
14. Weiss MD, Wasdell MB, Bomben MM, Rea KJ, Freeman RD. Sleep hygiene and melatonin treatment for children and adolescents with ADHD and initial insomnia. J Am Acad Child Adolesc Psychiatry. 2006;45(5):512–519. doi:10.1097/01
15. Roussel NA, Nijs J, Meeus M, Mylius V, Fayt C, Oostendorp R. Central sensitization and altered central pain processing in chronic low back pain: fact or myth? Clin J Pain. 2013;29(7):625–638. doi:10.1097/AJP.0b013e31826f9a71
16. Meints SM, Mawla I, Napadow V, et al. The relationship between catastrophizing and altered pain sensitivity in patients with chronic low-back pain. Pain. 2019;160(4):833–843. doi:10.1097/j.pain.0000000000001461
17. Kim H, Mawla I, Lee J, et al. Reduced tactile acuity in chronic low back pain is linked with structural neuroplasticity in primary somatosensory cortex and is modulated by acupuncture therapy. Neuroimage. 2020;217:116899. doi:10.1016/j.neuroimage.2020.116899
18. Lin JC, Chu LF, Stringer EA, et al. One month of oral morphine decreases gray matter volume in the right amygdala of individuals with low back pain: confirmation of previously reported magnetic resonance imaging results. Pain Med. 2016;17(8):1497–1504. doi:10.1093/pm/pnv047
19. Dagenais S, Caro J, Haldeman S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. 2008;8(1):8–20. doi:10.1016/j.spinee.2007.10.005
20. Medrano-Escalada Y, Plaza-Manzano G, Fernández-de-Las-Peñas C, Valera-Calero JA. Structural, functional and neurochemical cortical brain changes associated with chronic low back pain. Tomography. 2022;8(5):2153–2163. doi:10.3390/tomography8050180
21. Xiang A, Chen M, Qin C, et al. Frequency-specific blood oxygen level dependent oscillations associated with pain relief from ankle acupuncture in patients with chronic low back pain. Front Neurosci. 2021;15:786490. doi:10.3389/fnins.2021.786490
22. Yu S, Ortiz A, Gollub RL, et al. Acupuncture treatment modulates the connectivity of key regions of the descending pain modulation and reward systems in patients with chronic low back pain. J Clin Med. 2020;9(6):1719. doi:10.3390/jcm9061719
23. Kasch R, Truthmann J, Hancock MJ, et al. Association of lumbar MRI findings with current and future back pain in a population-based cohort study. Spine. 2022;47(3):201–211. doi:10.1097/brs.0000000000004198
24. Alshelh Z, Brusaferri L, Saha A, et al. Neuroimmune signatures in chronic low back pain subtypes. Brain. 2022;145(3):1098–1110. doi:10.1093/brain/awab336
25. Kolar P, Sulc J, Kyncl M, et al. Postural function of the diaphragm in persons with and without chronic low back pain. J Orthop Sports Phys Ther. 2012;42(4):352–362. doi:10.2519/jospt.2012.3830
26. Raja SN, Carr DB, Cohen M, et al. The revised international association for the study of pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
27. Ma C, Cao M, Zou Y, Ye Y, Yan X. Psychology factors in correlation to acupuncture analgesia effect. J Traditional Chin Med. 2021;62(01):27–31. doi:10.13288/j.11-2166/r.2021.01.007
28. Huettel SA, Song AW, McCarthy G. Functional Magnetic Resonance Imaging.
29. Liu J, Mu J, Liu Q, Dun W, Zhang M, Tian J. Brain structural properties predict psychologically mediated hypoalgesia in an 8-week sham acupuncture treatment for migraine. Hum Brain Mapp. 2017;38(9):4386–4397. doi:10.1002/hbm.23667
30. Cao J, Tu Y, Orr SP, et al. Analgesic effects evoked by real and imagined acupuncture: a neuroimaging study. Cereb Cortex. 2019;29(8):3220–3231. doi:10.1093/cercor/bhy190
31. Bresler DE, Kroening RJ. Three essential factors in effective acupuncture therapy. Am J Chin Med. 1976;4(1):81–86. doi:10.1142/s0192415x76000123
32. Chen BH, Chen QX, Chen YZ, et al. Expert consensus on acute/chronic nonspecific low back pain in China. Chin J Spin Spinal Cord. 2016;26:12.
33. Chan AW, Tetzlaff JM, Gøtzsche PC, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013:346:e7586. doi:10.1136/bmj.e7586
34. Hugh M, Altman DG, Hammerschlag R, et al. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): extending the CONSORT statement (Chinese version). Zhong Xi Yi Jie He Xue Bao. 2010;8(9):804–818. doi:10.3736/jcim20100902
35. Lee SH. Randomized double blinded clinical trial of ojeoksan products extracted through different methods for low back pain. Seoul: Kyung Hee University Graduate School Thesis for the Degree of Master of KoreanMedicine; 2010:1–51.
36. Hui KK, Nixon EE, Vangel MG, et al. Characterization of the ”deqi” response in acupuncture. BMC Complement Altern Med. 2007;7:33. doi:10.1186/1472-6882-7-33
37. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011;63(11):S240–52. doi:10.1002/acr.20543
38. Oshima Y, Takeshita K, Kato S, et al. Comparison Between the Japanese Orthopaedic Association (JOA) Score and Patient-Reported JOA (PRO-JOA) score to evaluate surgical outcomes of degenerative cervical myelopathy. Global Spine J. 2022;12(5):795–800. doi:10.1177/2192568220964167
39. Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi:10.1016/s0033-3182(71)71479-0
40. Zung WW. A SELF-RATING DEPRESSION SCALE. Arch Gen Psychiatry. 1965;12:63–70. doi:10.1001/archpsyc.1965.01720310065008
41. Dunstan DA, Scott N. Norms for zung’s self-rating anxiety scale. BMC Psychiatry. 2020;20(1):90. doi:10.1186/s12888-019-2427-6
42. Dunstan DA, Scott N, Todd AK. Screening for anxiety and depression: reassessing the utility of the Zung scales. BMC Psychiatry. 2017;17(1):329. doi:10.1186/s12888-017-1489-6
43. Lin LL, Li HP, Yang JW, et al. Acupuncture for psychological disorders caused by chronic pain: a review and future directions. Front Neurosci. 2020;14:626497. doi:10.3389/fnins.2020.626497
44. Kligler B, Nielsen A, Kohrherr C, et al. Acupuncture therapy in a group setting for chronic pain. Pain Med. 2018;19(2):393–403. doi:10.1093/pm/pnx134
45. Cheng SR, Li ZJ, Zhou J, et al. Effect of acupuncture on clinical symptoms and serum levels of patients with knee osteoarthritis β- Effect of endorphin level. Moderniz Tradit Chin Med Mater Mat. 2021;23(01):217–224.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.