Back to Journals » Journal of Pain Research » Volume 14
The Efficacy and Safety of Local Anesthetic Techniques for Postoperative Analgesia After Cesarean Section: A Bayesian Network Meta-Analysis of Randomized Controlled Trials
Authors Wang J, Zhao G, Song G ![]() , Liu J
, Liu J ![]()
Received 6 April 2021
Accepted for publication 21 May 2021
Published 2 June 2021 Volume 2021:14 Pages 1559—1572
DOI https://doi.org/10.2147/JPR.S313972
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Jian Wang,1 Ge Zhao,2 Guang Song,3 Jing Liu2
1Department of Anesthesiology, The First Affiliated Hospital of China Medical University, Shenyang, People’s Republic of China; 2Department of Obstetrics, The First Affiliated Hospital of China Medical University, Shenyang, People’s Republic of China; 3Department of Ultrasound, Shengjing Hospital of China Medical University, Shenyang, People’s Republic of China
Correspondence: Jing Liu
Department of Obstetrics, The First Affiliated Hospital of China Medical University, No. 155 Nanjing North Street, Heping District, Shenyang, Liaoning Province, 110001, People’s Republic of China
Tel +86 24 8328 2599
Email [email protected]
Objective: Cesarean section (CS) is one of the most frequently performed major surgical interventions. Local anesthetic techniques, a universal component of perioperative multimodal analgesia, are reportedly effective in reducing pain scores and opioid requirements. However, the optimal local anesthetic technique for postoperative CS pain remains unclear.
Methods: Six databases were searched, and a Bayesian network meta-analysis was performed. The outcomes included cumulative morphine consumption and pain scores at four time points, time to first analgesic request, postoperative nausea and vomiting, pruritus, and sedation.
Results: Sixty-eight studies with 5039 pregnant women were included. Six local anesthetic techniques were involved, including transversus abdominis plane block (TAPB), ilioinguinal and iliohypogastric nerve block, quadratus lumborum blocks, transversalis fascia plane block, erector spinae block, and wound infiltration. Compared to inactive controls, TAPB reduced cumulative morphine consumption at 6, 12, 24, and 48 h, pain scores at 6, 12, and 24 h (with the exception of 24 h at rest), the risk of postoperative nausea and vomiting, and sedation. Compared with inactive controls, ilioinguinal and iliohypogastric nerve block reduced cumulative morphine consumption at 6 and 24 h and pain scores at 6, 12, and 24 h during movement. Compared with inactive controls, quadratus lumborum blocks reduced cumulative morphine consumption at 24 and 48 h and pain scores at 6 and 12 h and lengthened the time to first analgesic request. Compared with inactive controls, wound infiltration reduced cumulative morphine consumption at 12 and 24 h, pain scores at 12 and 24 h during movement, and risk of sedation. Compared with inactive controls, erector spinae block reduced pain scores at 6 and 12 h. Transversalis fascia plane block was found to have similar outcomes to inactive controls.
Conclusion: TAPB is the most comprehensive local anesthetic technique for postoperative CS analgesia in the absence of intrathecal morphine.
Keywords: Cesarean section, postoperative pain, network meta-analysis, local anesthesia
Introduction
Cesarean section (CS) is one of the most frequently performed major surgical interventions. In 2012, 23 million CS were performed worldwide.1 Although CS has some benefits, such as lowering the risk of birth injuries (eg, asphyxia, shoulder dystocia, fractures2), it can cause moderate to severe postoperative pain.3 This pain must be taken seriously and treated in a timely manner because it may delay recovery, affect daily activities, and impact maternal psychological well-being.4 Furthermore, insufficient treatment may cause pain to become persistent5 and chronic.6 Optimizing analgesic regimens is a crucial aspect of pain management and can be a cost-effective way to improve postoperative outcomes and patient satisfaction.
Although opioids are commonly used for relief of postoperative pain after CS, opioid-related adverse effects such as nausea, vomiting, sedation, itching, and risk of delayed maternal respiratory depression can lead to other problems for new mothers, such as delayed initiation of breastfeeding and impairment of mother-infant bonding,7 all of which reduce overall patient satisfaction.7,8 Many scholars have studied the safety and efficacy of interventions for postoperative CS pain management and have suggested that various local anesthetic techniques, such as transversus abdominis plane block (TAPB), ilioinguinal and iliohypogastric nerve block (IIIH), quadratus lumborum blocks (QLB), transversalis fascia plane block (TFBP), erector spinae block (ESB), and wound infiltration (WI), are effective in reducing pain scores and opioid requirements. Given that the potential side effects of these local analgesic techniques are limited, they are frequently recommended. However, to date, no randomized controlled trial (RCT) has directly compared the six methods. Hence, uncertainty exists among clinicians concerning the best method for postoperative CS pain management.
In the absence of an RCT directly comparing all interventions of interest, a network meta-analysis (NMA) provides the best evidence on the most effective intervention.9 NMA allows for indirect pairwise comparisons of interventions through the use of a common comparison group and subsequent ranking of the interventions. To date, this method has not been applied to the study of the six available interventions for postoperative CS pain management. Thus, our aim was to determine which of these six interventions is the ideal method of pain relief after CS.
Methods
This NMA was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for NMA guidelines (Supplemental Table S18). A review protocol (number: CRD42021225699) was registered in the PROSPERO database (https://www.crd.york.ac.uk/PROSPERO). The Grading of Recommendations Assessment, Development and Evaluation (GRADE) system was utilized to assess the certainty of the evidence using four levels (high, moderate, low, and very low).10
Search Strategy
On December 12, 2020, two examiners independently searched for relevant studies in the following databases; PubMed, MEDLINE, Web of Science, EMBASE, ClinicalTrials.gov, and Cochrane Library. Search words included “cesarean section” (“transversus abdominis plane block,” or “ilioinguinal and iliohypogastric nerve block,” or “quadratus lumborum blocks,” or “transversalis fascia plane block,” or “erector spinae block,” or “wound infiltration”) and “postoperative pain.” The details of the search strategy are shown in Table S1. At the same time, we searched the references of identified articles to find additional literature that met the inclusion criteria.
Data Extraction
Original studies were eligible if they met the following criteria: (I) was an RCT study; (II) full text available in English; and (III) assessed the efficacy and safety of local anesthetic techniques for postoperative analgesia after cesarean delivery in the absence of intrathecal morphine (ITM) or other long-acting neuraxial opioids.11 Original studies were ineligible if they were (I) reviews, observational studies, case-control studies, abstracts, letters, or case reports; (II) studies involving combination blocks (ie, TAPB and rectus sheath); (III) studies with adjuncts; or (IV) laboratory animal literature. In the case of several publications from the same study, the study with the greatest number of cases and most relevant information was included.
For eligible studies, the first author, year of publication, anesthesia technique, groups and number of participants in each group, drug and dose, postoperative analgesia, and outcomes were extracted. Numeric data were gathered directly from tables or, when presented in graph form only, were inferred by digitizing the figure with GetData Graph Digitizer 2.26.12
Outcomes
Cumulative morphine consumption and pain scores were the primary outcomes of this NMA. Four time points (6, 12, 24, and 48 h postoperatively) were chosen. Any opiate drugs other than intravenous morphine were converted to morphine equivalents.13 Pain scores reported using visual analogue scales, verbal analogue scales, or numerical rating scores were converted to a standardized 0–100-point score (where 0 = no pain and 100 = worst pain imaginable) for quantitative evaluations. Time to first analgesic request (min), postoperative nausea and vomiting (PONV), pruritus, and sedation were chosen as secondary outcomes.
Statistical Analysis
Prior to analysis, the risk of trial bias was assessed for the included studies using the Cochrane Collaboration’s tool. Mean difference (MD) and 95% confidence interval (CI) were used to report cumulative morphine consumption, pain scores, and time to first analgesic request. Odds ratios (ORs) were used to report the risk of PONV, pruritus, and sedation. We evaluated the efficacy and safety of local anesthetic techniques for postoperative CS analgesia using an NMA. In this Bayesian NMA, random-effects and consistency models were used to analyze data and carry out the NMA (four chains, 50,000 iterations, 20,000 per chain). We assessed inconsistencies using the node-splitting method, and inconsistencies are reported by their Bayesian P values. An overall grading of the quality of evidence was conducted using the GRADE system. We analyzed symmetry of comparison-adjusted funnel plots to evaluate possible small sample effects. All analyses were conducted using the “gemtc” package of R version 4.0.2 (R Foundation, Vienna, Austria) and Stata version 16.0 (StataCorp, College Station, TX, USA).
Results
Baseline Characteristics of Included Studies
A total of 602 potentially relevant publications were retrieved from six databases using our exhaustive search strategy (Supplemental Table S1). After screening, the full texts of 78 articles were reviewed. Finally, 68 RCTs were included in our final analysis (Figure 1).14–81
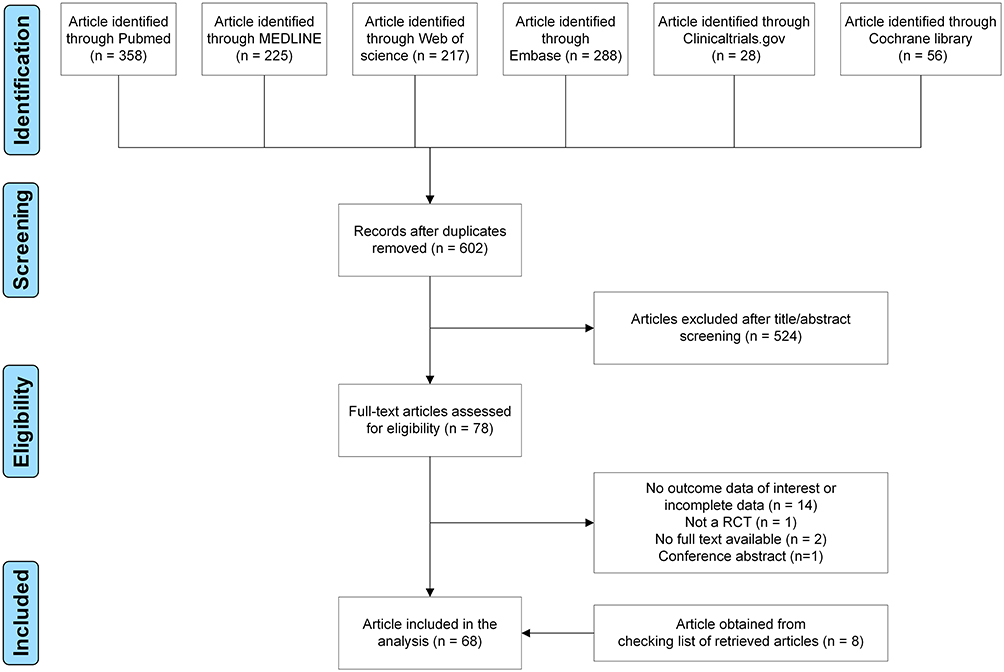 |
Figure 1 Flow-chart of study selection. |
The 68 RCTs were conducted between 1991 and 2021 and involved 5039 patients (Table 1). Six local anesthetic techniques were assessed in these studies, including ESB, IIIH, QLB, TAPB, TFPB, and WI (Figure 2). In total, 77.9% (53/68) involved spinal anesthesia; others involved general anesthesia or epidural anesthesia (3/68). Sixty-five were two-arm studies, and three were three-arm studies. A total of 21 studies compared WI with a control; 17 studies compared TAPB with a control; ten studies compared IIIH with a control; seven studies compared QLB with a control; and two studies compared TFPB with a control. No study compared ESB with a control. TAPB was compared with all other local anesthetic techniques. Drugs and dose, postoperative analgesia, and outcomes are shown in Table 1. Evaluation of bias risk for all RCTs is presented in Supplemental Figures S1 and S2.
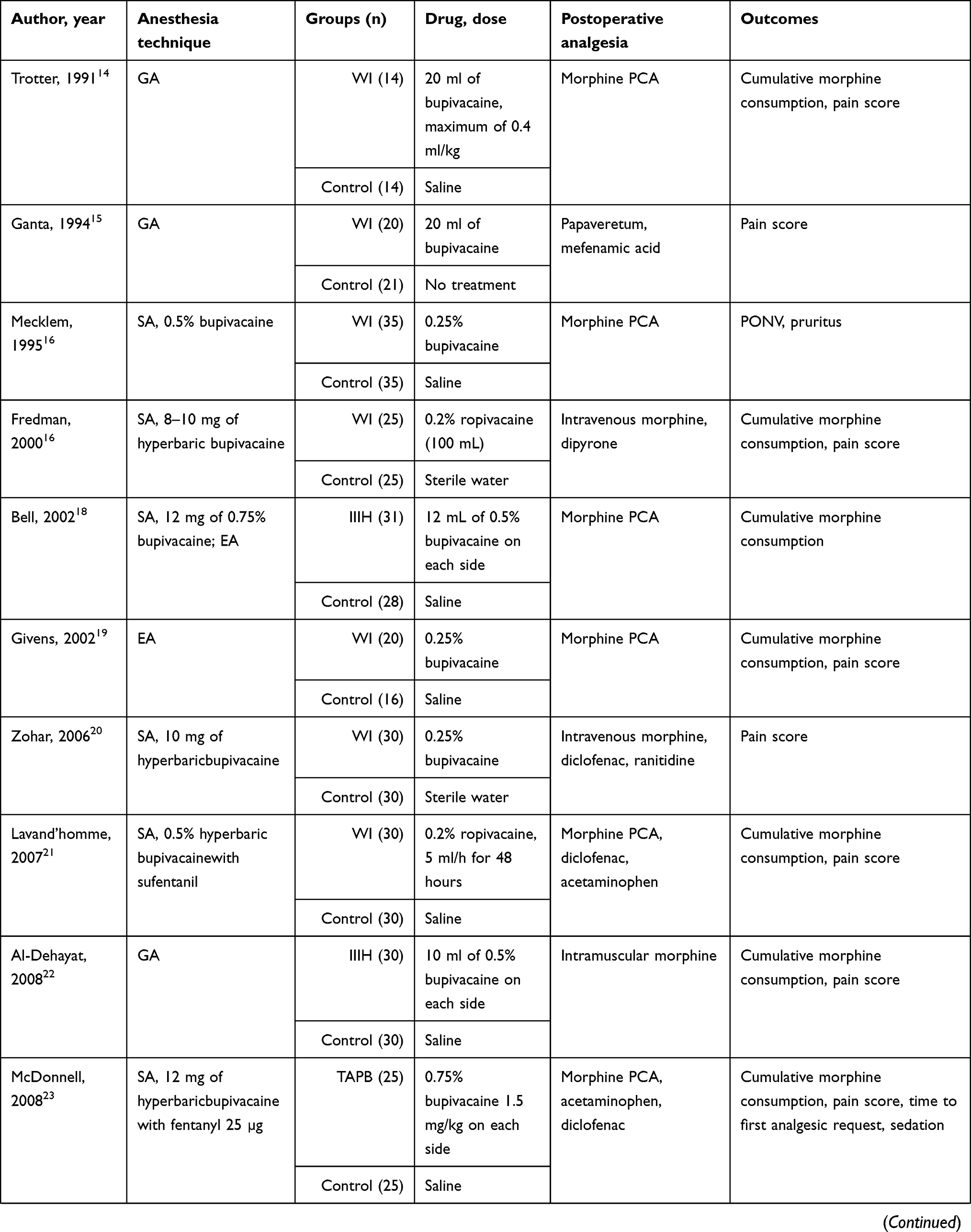 | 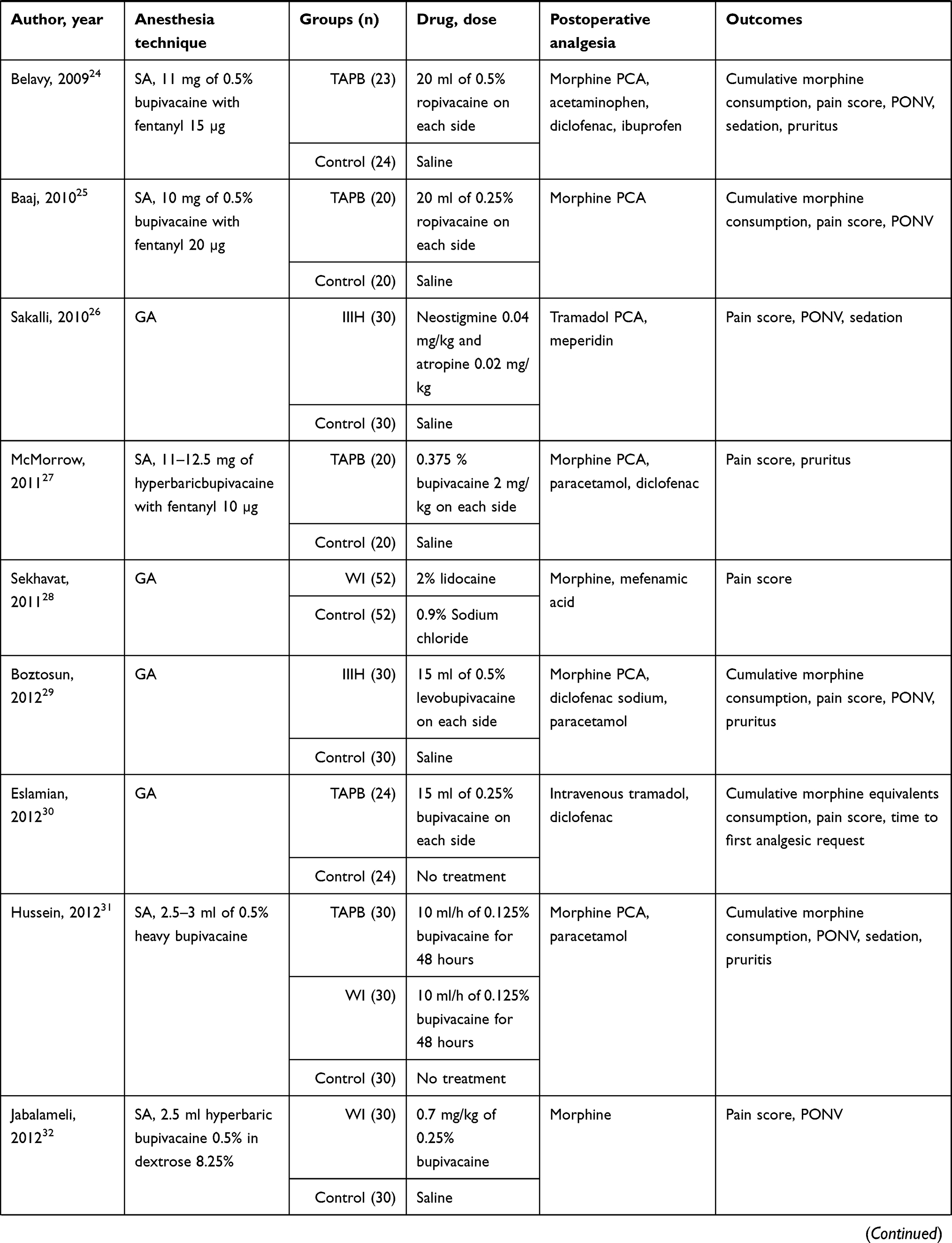 | 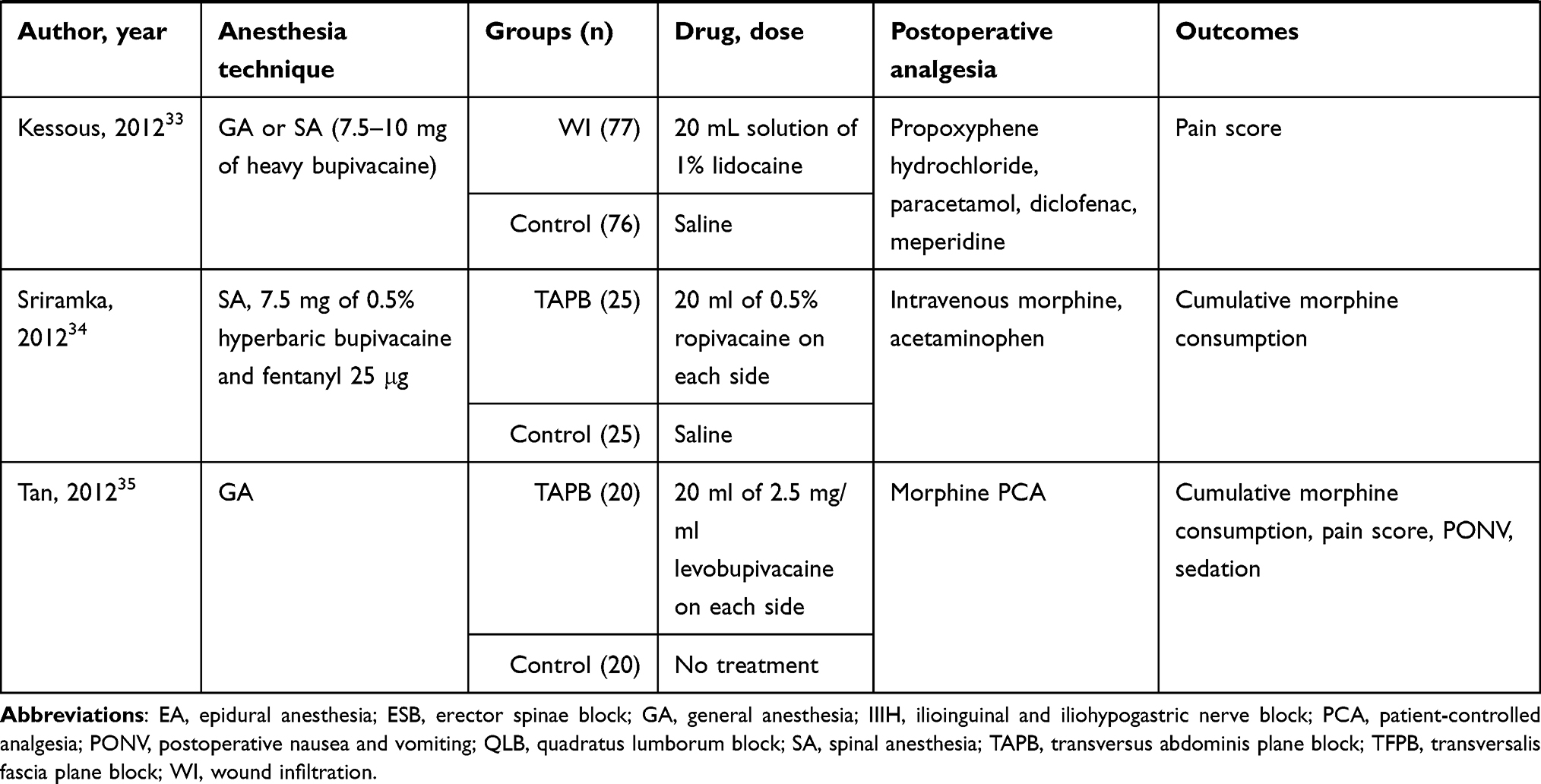 |
Table 1 Characteristics of Included Studies |
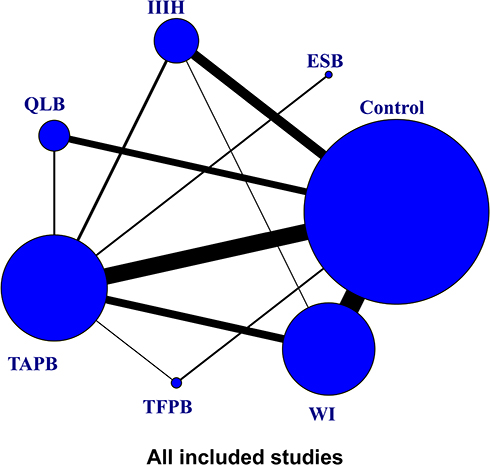 |
Figure 2 A network plot of eligible comparisons among different local anesthetic techniques. Notes: Circles represent the intervention as a node in the network, lines represent direct comparisons using randomized controlled trials and the thickness of lines corresponds to the number of randomized controlled trials included in each comparison.Abbreviations: ESB, erector spinae block; IIIH, ilioinguinal and iliohypogastric nerve block; QLB, quadratus lumborum blocks; TAPB, transversus abdominis plane block; TFBP, transversalis fascia plane block; WI, wound infiltration. |
Primary Outcomes
Eleven studies reported cumulative morphine consumption at 6 h. Cumulative morphine consumption at 6 h was significantly lower for TAPB and IIIH than for controls (MD = −9.37, 95% CI: −14.52 to −4.11; MD = −15.29, 95% CI: −26.95 to −3.63, respectively). Fourteen studies reported cumulative morphine consumption at 12 h. Cumulative morphine consumption at 12 h was significantly lower for TAPB and WI than for controls (MD = −13.62, 95% CI: −21.59 to −5.54; MD = −13.36, 95% CI: −24.74 to −2.05, respectively). Thirty-five studies reported cumulative morphine consumption at 24h. Cumulative morphine consumption at 24h was significantly lower for TAPB, QLB, IIIH, and WI than for controls (Figure 3). Twelve studies reported cumulative morphine consumption at 48 h. Cumulative morphine consumption at 48 h was significantly lower for TAPB and QLB than for controls (MD = −24.81, 95% CI: −48.92 to −2.36; MD = −25.28, 95% CI: −48.82 to −1.78, respectively).
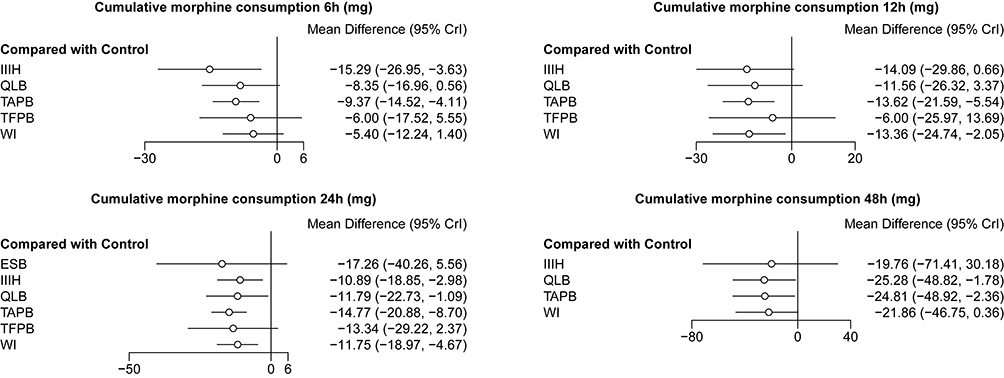 |
Figure 3 Forest plots of network meta-analysis of all trials for cumulative morphine consumption at each time point. Abbreviations: ESB, erector spinae block; IIIH, ilioinguinal and iliohypogastric nerve block; QLB, quadratus lumborum blocks; TAPB, transversus abdominis plane block; TFBP, transversalis fascia plane block; WI, wound infiltration. |
Pain scores at 6 and 12 h both at rest and during movement and at 24 h during movement were lower for TAPB both than for controls (Figure 4). Pain scores were lower for ESB and QLB at 6 and 12 h both at rest and during movement than for controls (Figure 4). Pain scores were lower for IIIH at 6, 12, and 24 h during movement than for controls (Figure 4). Pain scores were lower for WI at 12 and 24 h during movement than for controls (Figure 4). Pain scores were similar between TFPB and controls (Figure 4). Pairwise comparisons are shown in Supplemental Tables S2-S13.
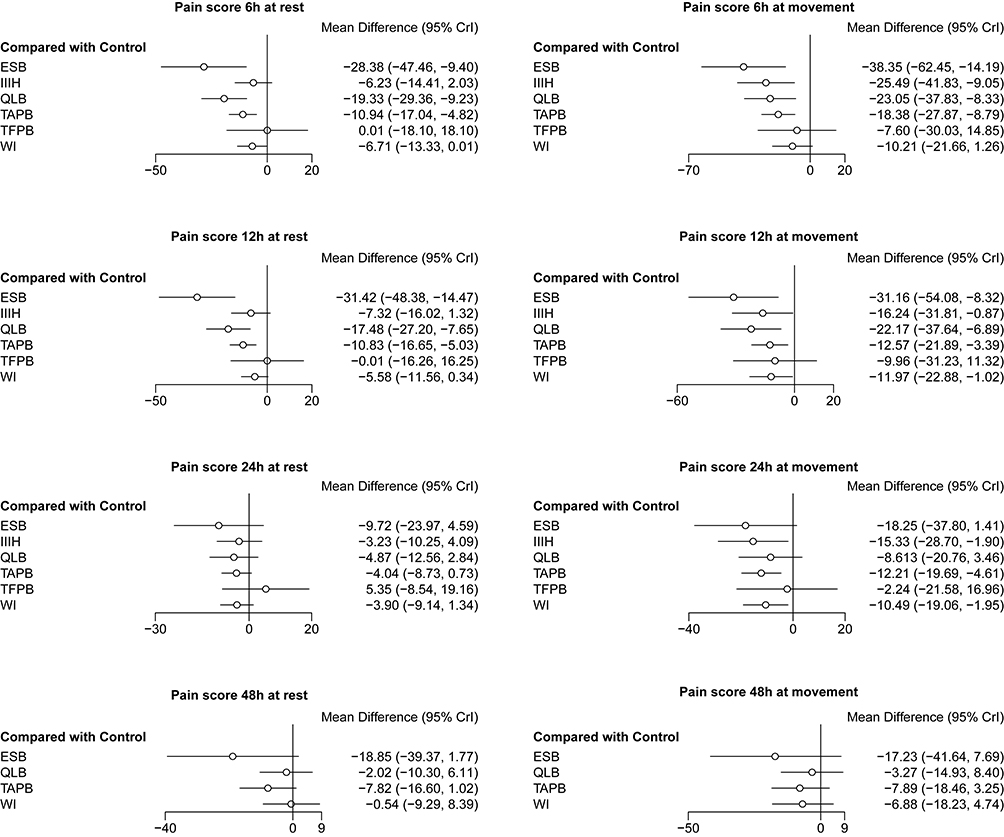 |
Figure 4 Forest plots of network meta-analysis of all trials for pain scores at each time point. Abbreviations: ESB, erector spinae block; IIIH, ilioinguinal and iliohypogastric nerve block; QLB, quadratus lumborum blocks; TAPB, transversus abdominis plane block; TFBP, transversalis fascia plane block; WI, wound infiltration. |
Secondary Outcomes
QLB lengthened the time to first analgesic request compared with controls (MD = 966.76, 95% CI: 262.82–1662.52). TAPB reduced the risk of PONV compared with controls (OR = 0.37, 95% CI: 0.15–0.86). TAPB and WI reduced the risk of sedation compared with controls (OR = 0.19, 95% CI: 0.05–0.58; OR = 0.17, 95% CI: 0.03–0.69, respectively, Figure 5). Pairwise comparisons are shown in Supplemental Tables S14-S17.
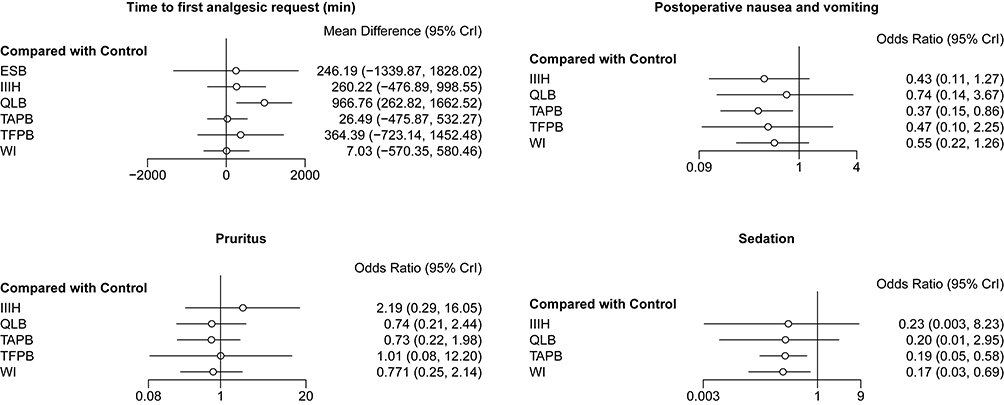 |
Figure 5 Forest plots of network meta-analysis of all trials for secondary outcomes. Abbreviations: ESB, erector spinae block; IIIH, ilioinguinal and iliohypogastric nerve block; QLB, quadratus lumborum blocks; TAPB, transversus abdominis plane block; TFBP, transversalis fascia plane block; WI, wound infiltration. |
Inconsistencies, Certainty of Evidence, and Publication Bias
Evaluations of inconsistencies for all outcomes are presented in Supplemental Figures S3–S5. We noted a significance level of P > 0.05 for most cases, which indicates that inconsistencies were not sufficient to influence the conclusions of this NMA. We used the GRADE system to evaluate the certainty of evidence (Table 2). No significant asymmetry was found in the funnel plots of major primary and secondary outcomes.
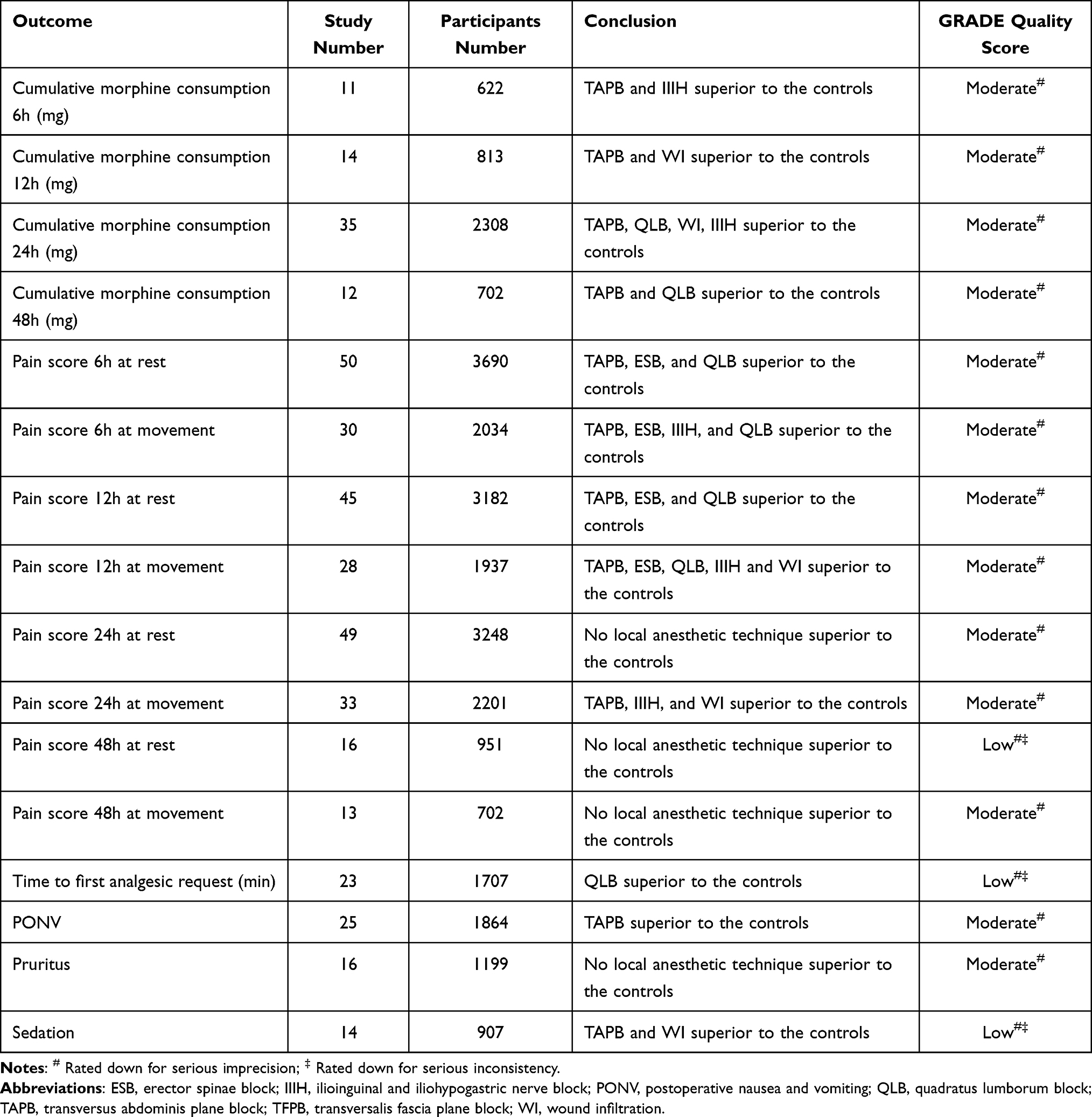 |
Table 2 Summary of the Results of NMA and GRADE Quality Score Assessment for the Outcomes |
Discussion
This NMA is the largest review assessing the efficacy and safety of local anesthetic techniques after CS. A total of 68 RCTs involving 5039 patients were included. Our analysis provided the opportunity to both explore the network of evidence and combine all data available for treatment comparisons. In this first comprehensive NMA, we found that TAPB had many advantages, including reduced cumulative morphine consumption at 6, 12, 24, and 48 h, reduced pain scores at 6, 12, and 24 h, reduced risk of PONV, and reduced risk of sedation compared with inactive controls. IIIH, QLB, ESB, and WI each had their own limited advantages. However, TFPB was found to have similar outcomes to inactive controls. Using this fairly new method for comparing these six interventions for postoperative CS pain management, TAPB appeared to be the most comprehensive option.
Opioid use has risen dramatically in the past three decades. ITM and intrathecal diamorphine are currently considered the gold standard for analgesia following elective CS in the USA and United Kingdom, respectively.82 However, opioid overdose has become a leading cause of unintentional deaths, surpassing motor vehicle accidents in the USA.83 In the last decades, doctors have begun to reduce opioid use during and after CS. Because operations such as CS are a vulnerable time when most patients are first exposed to opioids, utilizing a different local anesthetic technique could play a large role in decreasing opioid exposure.
Various local anesthetic techniques, which are a universal component of any perioperative multimodal analgesia, have been explored in the last two decades.82 TAPB, WI, IIIH, and QLB are the most widely used local anesthesia techniques, and recently an increasing number of doctors have employed ESB and TFPB for postoperative analgesia after CS. These six local anesthetic techniques can also be used together with non-opioid medications. Thus, patients may be able to remain opioid-free in the first few hours after CS.
Safety-related outcomes of local anesthetic techniques may include opioid-related side effects (ie, PONV, pruritus, sedation, respiratory depression, hypotension, and urinary retention), block-related complications (ie, hematoma, organ injury, local anesthetic systemic toxicity, and block failure), and effects on breastfeeding or mother-infant interaction.84–86 Respiratory depression,14,37,51,78 hypotension,32,37,38,53 urinary retention,31,37,68,72 effects on breastfeeding or mother-infant interaction,43,65,77 and block-related complications37,39,41,43,50,73,80 were rarely reported in the involved study. Therefore, we selected PONV, pruritus, and sedation as the safety outcomes of this NMA. Although their incidence is low, block-related complications, especially local anesthetic systemic toxicity, deserve attention, as pregnant women have increased cardiac output and reduced α1-acid glycoprotein levels, which can increase perfusion speed at injection sites, enhance local anesthetic absorption, and increase peak free local anesthetic concentrations.87
The efficacy outcomes of local anesthetic techniques usually include cumulative morphine consumption, pain scores, and time to first analgesic request. In this NMA, cumulative morphine consumption and pain scores were the primary outcomes. Time to first analgesic request, also called the duration of the local anesthetic technique, was also assessed. The results revealed that QLB lengthened the time to first analgesic request compared with TAPB, WI, and controls. QLB also effectively reduced pain scores 12 h after CS, which was consistent with the results of previous studies.86,88,89 A recently published study revealed that QLB not only reduced acute pain scores (with similar efficacy to TAPB during the acute phase) but also reduced the severity of persistent postoperative pain months after CS (with better efficacy than TAPB during the chronic phase).90 More RCTs are needed to confirm these findings. The durations of other local anesthetic techniques were similar.
TAPB was first described by Rafi et al in 200191 and has rapidly gained popularity in the study of local anesthesia for CS. TAPB is useful as a primary mode of analgesia in women undergoing CS who are not receiving neuraxial morphine for any reason.92 TAPB is also quite useful for opioid-tolerant patients, who often have poorly controlled postoperative pain. The major disadvantage of TAPB is that it does not provide visceral analgesia. This omission likely explains why multiple studies have failed to show that TAPB is superior to standard multimodal analgesia with ITM and why TAPB has not been shown to offer any additional analgesic benefits in the presence of ITM. In the present NMA, all included studies were conducted in the absence of ITM.
We found that TAPB decreased cumulative morphine consumption at each time point studied and reduced pain scores within 24 h. In addition, opioid-related side effects, such as PONV and risk of sedation, were also reduced, which may be related to the reduction in opioid consumption after TAPB. Although TAPB did not show an overwhelming advantage over the other five local anesthetic techniques in pairwise comparisons, the benefits of TAPB were clear, and we conclude that this is the most comprehensive local anesthetic technique. This is in agreement with previous meta-analysis studies.11,93
We found that IIIH reduced pain scores at 6, 12, and 24 h during movement, and WI reduced pain scores at 12 and 24 h during movement. However, neither IIIH nor WI showed greater benefits in relieving resting pain. Due to the absence of a study directly comparing ESB and controls, the results of indirect comparisons showing that ESB reduced pain scores at 6 and 12 h need to be further confirmed.74,76 Finally, we found that TFPB was not superior to controls for all outcomes we analyzed.
NMA can be used to estimate relative effects, even in the absence of pairwise clinical trials, through the use of a common comparator. Therefore, NMA is a particularly useful tool for decision-makers. Using NMA, we were able to compare six local anesthetic techniques. Altogether, the best available evidence suggests that TAPB is the most effective and safest local anesthetic technique for postoperative CS analgesia when ITM is not possible or desired, such as when general anesthesia is required for cesarean delivery.85
Limitations
First, in some cases, the same intervention was performed in several different ways, but we pooled the different techniques into a single group for analysis. For example, two approaches to TAPB, lateral and posterior, were employed, and QLB could be divided into QLB 1, QLB 2, and QLB 3.82 However, unlike previous studies, we could not perform subgroup analysis.11,94 Second, the drugs and doses used were not consistent across different studies of the same intervention, which limited the results of this NMA. Third, some included studies were single-center trials with limited sample sizes, which may have reduced the reliability of the results and conclusions of those studies.
Conclusion
The present NMA suggests that TAPB is the most comprehensive local anesthetic technique for postoperative CS analgesia in the absence of ITM.
Abbreviations
CI, confidence interval; CS, cesarean section; ESB, erector spinae block; GRADE, Grading of Recommendations Assessment, Development and Evaluation; IIIH, ilioinguinal and iliohypogastric nerve block; ITM, intrathecal morphine; MD, mean difference; NMA, network meta-analysis; OR, odds ratio; PONV, postoperative nausea and vomiting; QLB, quadratus lumborum blocks; RCT, randomized controlled trial; TAPB, transversus abdominis plane block; TFBP, transversalis fascia plane block; WI, wound infiltration.
Ethical Publication Statement
We confirm that we have read the journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Author Contributions
All authors contributed to data analysis and drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Molina G, Weiser TG, Lipsitz SR, et al. Relationship between cesarean delivery rate and maternal and neonatal mortality. JAMA. 2015;314(21):2263–2270. doi:10.1001/jama.2015.15553
2. Mylonas I, Friese K. Indications for and risks of elective cesarean section. Dtsch Arztebl Int. 2015;112(29–30):489–495.
3. Roofthooft E, Joshi GP, Rawal N, et al. PROSPECT guideline for elective caesarean section: updated systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2021;76(5):665–680.
4. Gamez BH, Habib AS. Predicting severity of acute pain after cesarean delivery: a narrative review. Anesth Analg. 2018;126(5):1606–1614.
5. Kainu JP, Sarvela J, Tiippana E, Halmesmaki E, Korttila KT. Persistent pain after caesarean section and vaginal birth: a cohort study. Int J Obstet Anesth. 2010;19(1):4–9.
6. Weibel S, Neubert K, Jelting Y, et al. Incidence and severity of chronic pain after caesarean section: a systematic review with meta-analysis. Eur J Anaesthesiol. 2016;33(11):853–865.
7. Bell EA, Jones BP, Olufolabi AJ, et al. Iliohypogastric-ilioinguinal peripheral nerve block for post-Cesarean delivery analgesia decreases morphine use but not opioid-related side effects. Can J Anaesth. 2002;49(7):694–700.
8. Li X, Zhou M, Shi X, et al. Local anaesthetic wound infiltration used for caesarean section pain relief: a meta-analysis. Int J Clin Exp Med. 2015;8(6):10213–10224.
9. Salanti G, Higgins JP, Ades AE, Ioannidis JP. Evaluation of networks of randomized trials. Stat Methods Med Res. 2008;17(3):279–301.
10. Puhan MA, Schunemann HJ, Murad MH, et al. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ. 2014;349(sep24 5):g5630. doi:10.1136/bmj.g5630
11. Sultan P, Patel SD, Jadin S, Carvalho B, Halpern SH. Transversus abdominis plane block compared with wound infiltration for postoperative analgesia following Cesarean delivery: a systematic review and network meta-analysis. Can J Anaesth. 2020;67(12):1710–1727.
12. Li SM, Kang MT, Wu SS, et al. Studies using concentric ring bifocal and peripheral add multifocal contact lenses to slow myopia progression in school-aged children: a meta-analysis. Ophthalmic Physiol Opt. 2017;37(1):51–59.
13. Centers for Medicare Medicaid Services. Opioid morphine equivalent conversion factors. 2019. https://www.cms.gov/medicare/prescription-drug-coverage/prescriptiondrugcovcontra/downloads/opioid-morphine-eq-conversion-factors-March-2016.pdf.
14. Trotter TN, Hayes-Gregson P, Robinson S, Cole L, Coley S, Fell D. Wound infiltration of local anaesthetic after lower segment caesarean section. Anaesthesia. 1991;46(5):404–407.
15. Ganta R, Samra SK, Maddineni VR, Furness G. Comparison of the effectiveness of bilateral ilioinguinal nerve block and wound infiltration for postoperative analgesia after caesarean section. Br J Anaesth. 1994;72(2):229–230.
16. Mecklem DWJ, Humphrey MD, Hicks RW. Efficacy of bupivacaine delivered by wound catheter for post-caesarean section analgesia. Austr N Z J Obstetrics Gynaecol. 1995;35(4):416–421.
17. Fredman B, Shapiro A, Zohar E, et al. The analgesic efficacy of patient-controlled ropivacaine instillation after Cesarean delivery. Anesth Analg. 2000;91(6):1436–1440.
18. Bell EA, Jones BP, Olufolabi AJ, et al. Iliohypogastric-ilioinguinal peripheral nerve block for post-Cesarean delivery analgesia decreases morphine use but not opioid-related side effects. Can J Anaesthesia. 2002;49(7):694–700.
19. Givens VA, Lipscomb GH, Meyer NL. A randomized trial of postoperative wound irrigation with local anesthetic for pain after cesarean delivery. Am J Obstet Gynecol. 2002;186(6):1188–1191.
20. Zohar E, Shapiro A, Eidinov A, Fishman A, Fredman B. Postcesarean analgesia: the efficacy of bupivacaine wound instillation with and without supplemental diclofenac. J Clin Anesth. 2006;18(6):415–421.
21. Lavand’homme PM, Roelants F, Waterloos H, De Kock MF. Postoperative analgesic effects of continuous wound infiltration with diclofenac after elective cesarean delivery. Anesthesiology. 2007;106(6):1220–1225.
22. Al-Dehayat G, Al-Momany M. Ilioinguinal-iliohypogastric peripheral nerve block for analgesia after caesarean section. J Ramanujan Math Soc. 2008;15(2):70–72.
23. McDonnell JG, Curley G, Carney J, et al. The analgesic efficacy of transversus abdominis plane block after cesarean delivery: a randomized controlled trial. Anesth Analg. 2008;106(1):186–191, table of contents.
24. Belavy D, Cowlishaw PJ, Howes M, Phillips F. Ultrasound-guided transversus abdominis plane block for analgesia after Caesarean delivery. Br J Anaesth. 2009;103(5):726–730.
25. Baaj JM, Alsatli RA, Majaj HA, Babay ZA, Thallaj AK. Efficacy of ultrasound-guided transversus abdominis plane (TAP) block for post-cesarean section delivery analgesia: a double-blind, placebo-controlled, randomized study. Middle East J Anesthesiol. 2010;20(6):821–826.
26. Sakalli M, Ceyhan A, Uysal HY, Yazici I, Başar H. The efficacy of ilioinguinal and iliohypogastric nerve block for postoperative pain after caesarean section. J Res Med Sci. 2010;15(1):6–13.
27. Rcn M, Ni Mhuircheartaigh RJ, Ahmed KA, et al. Comparison of transversus abdominis plane block vs spinal morphine for pain relief after Caesarean section. Br J Anaesth. 2011;106(5):706–712.
28. Sekhavat L, Behdad S. Preoperative analgesia with local lidocaine for cesarean delivery pain relief. J Matern Fetal Neonatal Med. 2011;24(7):891–893.
29. Boztosun A, Duger C, Kosar MI, et al. Abdominal blockage of iliohypogastric and ilio-inguinal nerves for management of post-caesarean pain: a novel method. S Afr J Obstet Gynaecol. 2012;18(1):23–27.
30. Eslamian L, Jalili Z, Jamal A, Marsoosi V, Movafegh A. Transversus abdominis plane block reduces postoperative pain intensity and analgesic consumption in elective cesarean delivery under general anesthesia. J Anesth. 2012;26(3):334–338.
31. Hussein M, Youssef K, Hassan MJLSJ. Comparative Study between Continuous transversus abdominis plane block and ON-Q anesthetic pump for postoperative analgesia following caesarean section. Life Sci J. 2012;9(1s):179–183.
32. Jabalameli M, Safavi M, Honarmand A, Saryazdi H, Moradi D, Kashefi P. The comparison of intraincisional injection tramadol, pethidine and bupivacaine on postcesarean section pain relief under spinal anesthesia. Adv Biomed Res. 2012;1:53.
33. Kessous R, Wiznitzer A, Polachek H, et al. Preoperative analgesia with local lidocaine infiltration for post cesarean delivery pain management. J Matern Fetal Neonatal Med. 2012;25(7):1131–1134.
34. Sriramka B, Sahoo N, Panigrahi S. Analgesic efficacy of ultrasound-guided transversus abdominis plane block following caesarean section. Int J Perioperative Ultrasound Appl Technol. 2012;1(1):5–8.
35. Tan TT, Teoh WHL, Woo DCM, Ocampo CE, Shah MK, Sia ATH. A randomised trial of the analgesic efficacy of ultrasound-guided transversus abdominis plane block after caesarean delivery under general anaesthesia. Eur J Anaesthesiol. 2012;29(2):88–94.
36. Demiraran Y, Albayrak M, Yorulmaz IS, Ozdemir I. Tramadol and levobupivacaine wound infiltration at cesarean delivery for postoperative analgesia. J Anesth. 2013;27(2):175–179.
37. Eldaba AA, Amr YM, Sobhy RA. Effect of wound infiltration with bupivacaine or lower dose bupivacaine/magnesium versus placebo for postoperative analgesia after cesarean section. Anesth Essays Res. 2013;7(3):336–340.
38. Aydogmus MT, Sinikoglu SN, Naki MM, Ocak NB, Sanli N, Alagol A. Comparison of analgesic efficiency between wound site infiltration and ultrasound- guided transversus abdominis plane block after cesarean delivery under spinal anaesthesia. Hippokratia. 2014;18(1):28–31.
39. Chandon M, Bonnet A, Burg Y, et al. Ultrasound-guided Transversus Abdominis plane block versus continuous wound infusion for post-caesarean analgesia: a randomized trial. PLoS One. 2014;9(8):e103971.
40. Pekmezci A, Cesur M, Aksoy M, Ince I, Aksoy AN. The effect of ilioinguinal-iliohypogastric block with or without intravenous paracetamol for pain relief after caesarean delivery. Acta Med Mediterr. 2014;30(6):1183–1188.
41. Raoofi Z, Karimi MB, Parvar SP, Parvar SP. Ilioinguinal and iliohypogastric nerve block with anatomical landmark and direct visualization technique. Bangladesh J Obstetrics Gynecol. 2014;29(2):83–86.
42. Blanco R, Ansari T, Girgis E. Quadratus lumborum block for postoperative pain after caesarean section: a randomised controlled trial. Eur J Anaesthesiol. 2015;32(11):812–818.
43. Jolly C, Jathieres F, Keita H, Jaouen E, Guyot B, Torre A. Cesarean analgesia using levobupivacaine continuous wound infiltration: a randomized trial. Eur J Obstet Gynecol Reprod Biol. 2015;194:125–130.
44. Larsen KR, Kristensen BB, Rasmussen MA, et al. Effect of high-volume systematic local infiltration analgesia in Caesarean section: a randomised, placebo-controlled trial. Acta Anaesthesiol Scand. 2015;59(5):632–639.
45. Srivastava U, Verma S, Singh TK, et al. Efficacy of trans abdominis plane block for post cesarean delivery analgesia: a double-blind, randomized trial. Saudi J Anaesth. 2015;9(3):298–302.
46. Telnes A, Skogvoll E, Lonnee H. Transversus abdominis plane block vs. wound infiltration in Caesarean section: a randomised controlled trial. Acta Anaesthesiol Scand. 2015;59(4):496–504.
47. Blanco R, Ansari T, Riad W, Shetty N. Quadratus lumborum block versus transversus abdominis plane block for postoperative pain after cesarean delivery: a randomized controlled trial. Reg Anesth Pain Med. 2016;41(6):757–762.
48. Klasen F, Bourgoin A, Antonini F, et al. Postoperative analgesia after caesarean section with transversus abdominis plane block or continuous infiltration wound catheter: a randomized clinical trial. TAP vs. infiltration after caesarean section. Anaesth Crit Care Pain Med. 2016;35(6):401–406.
49. Ahmad M, Furqan A, Adnan M, Waris S, Yousuf M. Transversus abdominis plane block offers prolonged postoperative analgesia than surgical incision infiltration by bupivacaine in cesarean section patients. Anaesthesia Pain Intensive Care. 2017;21(3):312–316.
50. Gorkem U, Kocyigit K, Togrul C, Gungor T. Comparison of bilateral transversus abdominis plane block and wound infiltration with bupivacaine for postoperative analgesia after cesarean delivery. J TurkishGerman Gynecol Assoc. 2017;18(1):26–32.
51. Kahsay DT, Elsholz W, Bahta HZ. Transversus abdominis plane block after Caesarean section in an area with limited resources. Southern Afr J Anaesthesia Analgesia. 2017;23(4):90–95.
52. Kiran LV, Sivashanmugam T, Kumar VRH, Krishnaveni N, Parthasarathy S. Relative efficacy of ultrasound-guided ilioinguinal-iliohypogastric nerve block versus transverse abdominis plane block for postoperative analgesia following lower segment Cesarean section: a prospective, randomized observer-blinded trial. Anesth Essays Res. 2017;11(3):713–717.
53. Lalmand M, Wilwerth M, Fils JF, Van der Linden P. Continuous ropivacaine subfascial wound infusion compared with intrathecal morphine for postcesarean analgesia: a prospective, randomized controlled, double-blind study. Anesth Analg. 2017;125(3):907–912.
54. Niazi RHK, Dodhy AA, Sultana B, Akram MA. Effectiveness of Transversus Abdominis Plane (TAP) block for pain management after caesarean section. Pak J Med Health Sci. 2017;11(3):1060–1062.
55. Nigatu Y, Gebremedhn E, Tawuye H, Gebreegzi AJ. Analgesic efficacy of bilateral ilioinguinal and iliohypogastric nerve block for post caesarean delivery under spinal anaesthesia, 2016. double blind randomized study. J Anesth Clin Res. 2017;8(751):2.
56. Poudel A, Dutta PK. A comparative study of bilateral ilioinguinal and iliohypogastric nerve block for postoperative analgesia in lower segment cesarean section. J Soc Anesthesiologists Nepal. 2017;4(2):81–86.
57. Tawfik MM, Mohamed YM, Elbadrawi RE, Abdelkhalek M, Mogahed MM, Mohamed H. Transversus Abdominis Plane Block Versus Wound Infiltration for Analgesia After Cesarean Delivery: a Randomized Controlled Trial. Anesth Analg. 2017;124(4):1291–1297.
58. Ahemed SA, Denu ZA, Getinet Kassahun H, Yilikal Fentie D. Efficacy of bilateral transversus abdominis plane and ilioinguinal-iliohypogastric nerve blocks for postcaesarean delivery pain relief under spinal anesthesia. Anesthesiol Res Pract. 2018;2018:1948261.
59. Jadon A, Jain P, Chakraborty S, et al. Role of ultrasound guided transversus abdominis plane block as a component of multimodal analgesic regimen for lower segment caesarean section: a randomized double blind clinical study. BMC Anesthesiol. 2018;18(1):53.
60. Krohg A, Ullensvang K, Rosseland LA, Langesaeter E, Sauter AR. The analgesic effect of ultrasound-guided quadratus lumborum block after cesarean delivery: a randomized clinical trial. Anesth Analg. 2018;126(2):559–565.
61. Kupiec A, Zwierzchowski J, Kowal-Janicka J, et al. The analgesic efficiency of transversus abdominis plane (TAP) block after caesarean delivery. Ginekol Pol. 2018;89(8):421–424.
62. Mieszkowski MM, Mayzner-Zawadzka E, Tuyakov B, et al. Evaluation of the effectiveness of the Quadratus Lumborum Block type I using ropivacaine in postoperative analgesia after a cesarean section - a controlled clinical study. Ginekol Pol. 2018;89(2):89–96.
63. Rahimzadeh P, Faiz SHR, Imani F, Jahromi MR. Comparison between ultrasound guided transversalis fascia plane and transversus abdominis plane block on postoperative pain in patients undergoing elective cesarean section: a randomized clinical trial. Iran Red Crescent Med J. 2018;20(9):7.
64. Wagner-Kovacec J, Povalej-Brzan P, Mekis D. Efficacy of continuous in-wound infusion of levobupivacaine and ketorolac for post-caesarean section analgesia: a prospective, randomised, double-blind, placebo-controlled trial. BMC Anesthesiol. 2018;18(1):165.
65. Buluc H, Ar AY, Turan G, Karadogan F, Sargin MA, Akgun N. The efficacy of transversus abdominis plane block for post-operative analgesia after the cesarean section performed under general anesthesia. North Clin Istanb. 2019;6(4):368–373.
66. Hansen CK, Dam M, Steingrimsdottir GE, et al. Ultrasound-guided transmuscular quadratus lumborum block for elective cesarean section significantly reduces postoperative opioid consumption and prolongs time to first opioid request: a double-blind randomized trial. Reg Anesth Pain Med. 2019;44(9):896–900.
67. Li Y, Ballard H, Carani JL, et al. Transversus abdominis plane block in parturients undergoing intrapartum cesarean delivery. J Anesthesia Perioperative Med. 2019;6(1):15–22.
68. Nasir F, Sohail I, Sadiq H, Habib M. Local wound infiltration with ropivacaine for postoperative pain control in caesarean section. Cureus. 2019;11(9):e5572.
69. Tamura T, Yokota S, Ando M, Kubo Y, Nishiwaki K. A triple-blinded randomized trial comparing spinal morphine with posterior quadratus lumborum block after cesarean section. Int J Obstet Anesth. 2019;40:32–38.
70. Verma K, Malawat A, Jethava D, Das jethava D. Comparison of transversus abdominis plane block and quadratus lumborum block for post-caesarean section analgesia: a randomised clinical trial. Indian J Anaesth. 2019;63(10):820–826.
71. Abiy S, Ayalew N, Eshete A, et al. Comparison of bilateral ilioinguinal-iliohypogastric nerve block versus transverses abdominis nerve block for postoperative pain management for parturient undergoing elective cesarean section in Dilla University Referral Hospital, Ethiopia. A randomized controlled trial. Int J SurgOpen. 2020;26:22–29.
72. Aydin ME, Bedir Z, Yayik AM, et al. Subarachnoid block and ultrasound-guided transversalis fascia plane block for caesarean section: a randomised, double-blind, placebo-controlled trial. Eur J Anaesthesiol. 2020;37(9):765–772.
73. Bavarsadkarimi M, Raoufi Z, Koohpayehzadeh J. Evaluation of the efficacy of ilioinguinal and iliohypogastric blocks on postoperative pain relief and use of opioids after lower segment caesarean section. Med Sci. 2020;24(102):855–860.
74. Boules ML, Goda AS, Abdelhady MA, et al. Comparison of analgesic effect between erector spinae plane block and transversus abdominis plane block after elective cesarean section: a prospective randomized single-blind controlled study. J Pain Res. 2020;13:1073–1080.
75. Krishnegowda S, Pujari VS, Doddagavanahalli SRC, Bevinaguddaiah Y, LHJJoOA P, Care C. A randomized control trial on the efficacy of bilateral ilioinguinal-iliohypogastric nerve block and local infiltration for post-cesarean delivery analgesia. J Obstet Anaesthesia Crit Care. 2020;10(1):32.
76. Malawat A, Verma K, Jethava D, Jethava DD. Erector spinae plane block and transversus abdominis plane block for postoperative analgesia in cesarean section: a prospective randomized comparative study. J Anaesthesiol Clin Pharmacol. 2020;36(2):201–206.
77. Rosetti J, Francotte J, Noel E, Drakopoulos P, Rabbachin N, de Brucker M. Continuous ropivacaine subfascial wound infusion after cesarean delivery in pain management: a prospective randomized controlled double-blind study. Int J Gynaecol Obstet. 2020;17.
78. Salama ER. Ultrasound-guided bilateral quadratus lumborum block vs. intrathecal morphine for postoperative analgesia after cesarean section: a randomized controlled trial. Korean J Anesthesiol. 2020;73(2):121–128.
79. Serifsoy TE, Tulgar S, Selvi O, et al. Evaluation of ultrasound-guided transversalis fascia plane block for postoperative analgesia in cesarean section: a prospective, randomized, controlled clinical trial. J Clin Anesth. 2020;59:56–60.
80. Yoshida K, Tanaka S, Watanabe K, Obara S, Murakawa M. The effectiveness of the intramuscular quadratus lumborum block in postoperative analgesia after cesarean section with vertical incision: a randomized, double-blinded placebo-controlled study. J Anesth. 2020;34(6):849–856.
81. Yu Y, Gao S, Yuen VM, Choi SW, Xu X. The analgesic efficacy of ultrasound-guided transversus abdominis plane (TAP) block combined with oral multimodal analgesia in comparison with oral multimodal analgesia after caesarean delivery: a randomized controlled trial. BMC Anesthesiol. 2021;21(1):7.
82. Patel SD, Sharawi N, Sultan P. Local anaesthetic techniques for post-caesarean delivery analgesia. Int J Obstet Anesth. 2019;40:62–77.
83. Koepke EJ, Manning EL, Miller TE, Ganesh A, Williams DGA, Manning MW. The rising tide of opioid use and abuse: the role of the anesthesiologist. Perioper Med (Lond). 2018;7:16.
84. Novikova N, Cluver C. Local anaesthetic nerve block for pain management in labour. Cochrane Database Syst Rev. 2012;(4):CD009200.
85. Mitchell KD, Smith CT, Mechling C, Wessel CB, Orebaugh S, Lim G. A review of peripheral nerve blocks for cesarean delivery analgesia. Reg Anesth Pain Med. 2019.
86. Hussain N, Brull R, Weaver T, Zhou M, Essandoh M, Abdallah FW. Postoperative analgesic effectiveness of quadratus lumborum block for cesarean delivery under spinal anesthesia. Anesthesiology. 2021;134(1):72–87.
87. El-Boghdadly K, Pawa A, Chin KJ. Local anesthetic systemic toxicity: current perspectives. Local Reg Anesth. 2018;11:35–44.
88. Xu M, Tang Y, Wang J, Yang J. Quadratus lumborum block for postoperative analgesia after cesarean delivery: a systematic review and meta-analysis. Int J Obstet Anesth. 2020;42:87–98.
89. Tan HS, Taylor C, Weikel D, Barton K, Habib AS. Quadratus lumborum block for postoperative analgesia after cesarean delivery: a systematic review with meta-analysis and trial-sequential analysis. J Clin Anesth. 2020;67:110003.
90. Borys M, Zamaro A, Horeczy B, et al. Quadratus lumborum and transversus abdominis plane blocks and their impact on acute and chronic pain in patients after cesarean section: a randomized controlled study. Int J Environ Res Public Health. 2021;18(7):3500.
91. Rafi AN. Abdominal field block: a new approach via the lumbar triangle. Anaesthesia. 2001;56(10):1024–1026.
92. Carvalho B, Butwick AJ. Postcesarean delivery analgesia. Best Pract Res Clin Anaesthesiol. 2017;31(1):69–79.
93. Ng SC, Habib AS, Sodha S, Carvalho B, Sultan P. High-dose versus low-dose local anaesthetic for transversus abdominis plane block post-Caesarean delivery analgesia: a meta-analysis. Br J Anaesth. 2018;120(2):252–263.
94. El-Boghdadly K, Desai N, Halpern S, et al. Quadratus lumborum block vs. transversus abdominis plane block for caesarean delivery: a systematic review and network meta-analysis. Anaesthesia. 2021;76(3):393–403.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.