Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
The Effects of a Nursing Program Applying Zinc Oxide Mixed with Petroleum Jelly and Centella Asiatica Mixed with Aloe Vera on Skin Indicators Among Older Patients in Semi-Intensive Care Units: A Pilot Study
Authors Chaisomsee S, Banharak S ![]() , Sommana C
, Sommana C ![]() , Tuntiyasawasdikul S, Sim-im S, Ransinyo K, Limpawattana P
, Tuntiyasawasdikul S, Sim-im S, Ransinyo K, Limpawattana P ![]() , Deesui W, Pimpun P, Somkamsri T, Seeharach O
, Deesui W, Pimpun P, Somkamsri T, Seeharach O
Received 26 March 2025
Accepted for publication 24 July 2025
Published 1 August 2025 Volume 2025:18 Pages 4561—4587
DOI https://doi.org/10.2147/JMDH.S527931
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jacqueline Dunbar-Jacob
Somphorn Chaisomsee,1 Samoraphop Banharak,2 Chakkarin Sommana,2 Sarunya Tuntiyasawasdikul,3 Supin Sim-im,1 Khanisorn Ransinyo,2 Panita Limpawattana,4 Waraporn Deesui,5 Porntip Pimpun,1 Teerawat Somkamsri,1 Orada Seeharach1
1Nursing Department, Srinagarind Hospital, Khon Kaen University, Khon Kaen, Thailand; 2Department of Gerontological Nursing, Faculty of Nursing, Khon Kaen University, Khon Kaen, Thailand; 3Center for Research and Development of Herbal Health Products, Faculty of Pharmaceutical Sciences, Khon Kaen University, Khon Kaen, Thailand; 4Department of Internal Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 5Department of Internal Medicine, Namphong Hospital, Khon Kaen, Thailand
Correspondence: Samoraphop Banharak, Email [email protected]
Abstract: Incontinence-associated dermatitis (IAD) is commonly observed in older patients admitted to intensive or semi-intensive care units, particularly those who are unable to perform daily activities independently or have restricted mobility. Once IAD occurs, it causes discomfort, pain, and loss of self-confidence, as well as increases the financial burden of treatment. This pilot study aimed to assess the feasibility of using a protective skin product to prevent and manage IAD in older patients. We applied a double-blind, randomized, block-controlled trial with a two-group pre-posttest design for this study. The study included 20 older patients admitted to a semi-intensive medical care unit. Ten participants received a nursing program that applied zinc oxide mixed with petroleum jelly, and another 10 received the same nursing program but with Centella Asiatica mixed with aloe vera. We measured the risk and severity of IAD, assessed skin moisturizer and skin pH, and analyzed data using both quantitative and qualitative methods. The results demonstrated that both tested products effectively prevented and managed IAD in older patients. They contributed to reducing the risk and severity of IAD, enhancing skin hydration, and maintaining a mildly acidic skin pH. The findings of this pilot study confirm the feasibility of using these products for older patients with incontinence. Additionally, the products were easy to apply, exhibited appropriate viscosity, created a protective barrier for the skin, reduced inflammation, and facilitated skin recovery from IAD. However, further studies with larger sample sizes and more rigorous research designs are needed to validate these findings comprehensively. Protocol Registration: TCTR20240910009 (September 10, 2024).
Keywords: incontinence associated dermatitis, aged, critical care, skin care, dermatitis
Introduction
Incontinence-associated dermatitis (IAD) refers to inflammation, irritation, or damage to the skin around the buttocks and genitals.1–3 It is a form of dermatitis caused by prolonged exposure to moisture, often from urine or feces.2 It is commonly caused by the inability to control bowel movements, leading to prolonged skin contact with urine or feces and irritation. Other contributing factors include harsh skin scrubbing or rubbing, bathing in too hot or too cold water, the use of inappropriate skin protection products, and a lack of knowledge or understanding about the prevention and care of incontinence-associated dermatitis, both by healthcare professionals and caregivers.2,4 Incontinence-associated dermatitis is widespread among older patients who are hospitalized.
The higher prevalence of this condition among older adults can be attributed to age-related changes in the skin. As individuals age, their skin undergoes various degenerative processes, such as thinning, a reduction in the underlying fat layer, diminished skin moisture, dry skin, and a decrease in the function of sweat and sebaceous glands, all of which contribute to skin dryness.5 Additionally, older adults exhibit key characteristics, often summarized as “RAMPS” which can be explained as follows: 1) Reduced body reserve: The skin of older adults becomes thinner and less resistant to irritation and friction. It also lacks moisture and protective barriers, which, along with a reduced ability to control excretion, increases the risk of incontinence-associated dermatitis. Furthermore, the immune response to detect and eliminate pathogens is slower, leading to delayed wound healing.5 2) Atypical presentation: It often leads to unclear dermatitis symptoms, making it challenging to distinguish from pressure ulcers, which require different causes and care approaches. 3) Multiple pathologies and 4) Polypharmacy: Older adults often face multiple health issues and require various medications for treatment. Many of these conditions, such as diabetes and high blood pressure, can hinder tissue recovery. In addition, the use of multiple medications can impact bodily functions. Diuretics, for example, can affect urinary control. At the same time, antibiotics, especially when taken in large doses or over prolonged periods, can lead to watery stools and disrupt bowel control, calling antibiotics inducing diarrhea. 5) Social adversity: Families and society often lack sufficient knowledge and understanding of how to care for older adults with incontinence-associated dermatitis. As a result, there is an increased risk of its occurrence, and when it does happen, it becomes difficult to manage, leading to delayed healing.6
Studies have identified several factors that increase the risk of developing IAD among older patients, namely excessively moist or dry skin, alkaline skin, fungal or bacterial infections, friction, aging, malnutrition (especially protein deficiency), watery stools or gastrointestinal infections, obesity, and poor oxygen and blood circulation.2,7 These factors place older patients in intensive or semi-intensive medical care units at a high risk of developing IAD. Since intensive or semi-intensive medical care units treat patients with severe conditions and perform life-saving procedures such as intubation, dialysis, high-risk medications, and sedatives, patients are often restricted in their mobility and ability to perform activities of daily living. These treatment conditions increase the incidence of IAD, particularly in older patients’ skin, which is more vulnerable when exposed to feces or urine with high alkalinity (pH greater than 8) and digestive enzymes found in feces that can damage the skin.8 Even brief exposure, as short as 10 to 15 minutes, can result in IAD.2
A survey on the prevalence of incontinence in older adults revealed rates ranging from 16% to 78%.2 When categorized by type, urinary incontinence in hospitals was found to have a prevalence of 60–70%, while fecal incontinence in intensive care units reached 36%.9 An assessment of the risk of IAD in older patients showed that one in four patients admitted to the ward was at very high risk.2,3 A survey on the incidence of IAD in hospitals found a range of 5.6% to 46%,7 with rates of 20.67% in semi-intensive care units10 and 22.8% in intensive care units.7 A study on the incidence of IAD revealed that it typically occurred on the fourth day of hospitalization (within 1–6 days).9 IAD can be categorized as mild to moderate in 5.2% of cases and severe in 2.4%.9 IAD has a wide range of impacts, affecting patients, caregivers, and hospitals. Physically, patients may experience pain, burning, bleeding, infection, and insomnia. Mentally, they may struggle with anxiety about wound healing, loss of self-image, and depression. For families, it can cause anxiety, increased caregiving responsibilities, and additional financial burdens. Hospitals are also impacted, including extended hospital stays, increased bed occupancy, higher overall hospitalization costs, and additional treatment expenses for IAD.11 Studies also found that older patients with IAD were 10 times more likely to develop pressure ulcers than those without dermatitis.2,4 Furthermore, they can face an increased risk of wound and bloodstream infections.12 Therefore, it is vital for healthcare professionals, especially nurses, to implement comprehensive care plans to prevent and effectively manage IAD in older patients.
The study on nursing processes for the prevention and care of IAD in older patients identified eight key activities: 1) providing knowledge on the prevention and care of IAD to healthcare personnel, older patients, and their caregivers, 2) assessing the risk of developing IAD in older patients, both for those who have not yet developed it and those who have, including assessing the severity of the condition, 3) identifying the underlying causes and risk factors for IAD in older patients and addressing these factors, which may involve a multidisciplinary team, including doctors, nurses, and pharmacists, 4) gently cleaning the skin using techniques suitable for older patients, such as avoiding excessive scrubbing and using mildly acidic cleaning products that are appropriate for their skin condition, 5) applying skin protection products that offer a barrier against waste, such as zinc oxide, petroleum jelly, or 3M Cavilon products, 6) repositioning the patient at least every two hours to minimize skin contact with waste and to promote ventilation, 7) promoting nutrition for older patients by providing a balanced diet that includes all five food groups, with a particular emphasis on protein to support wound healing, and 8) assessing outcomes, using criteria such as the incidence and severity of IAD, assessing the risk of IAD, checking the skin surface pH and moisture.2 From the literature review and practice, limited products are available on the market. The prices are also high compared to the product quantity. In addition, there is a lack of studies on the use of Thai herbs as potential treatments for IAD.
Research on the effectiveness of products in preventing IAD in hospitalized patients has been conducted. One study compared zinc oxide, petroleum jelly, and a combination of both, finding that the mixed formula was the most effective in preventing and treating IAD.13 Studies that compared zinc oxide with 3M Cavilon also found that 3M Cavilon was the most effective product for preventing and treating IAD.14,15 However, in practice, patients or their relatives must purchase skin protection products to prevent IAD, which are often expensive and difficult to find. Upon reviewing domestic and international literature, there is no evidence of using Thai herbs with skin-protecting and anti-inflammatory properties in the formulation of creams for preventing and treating IAD. The literature on Thai herbs known for their ability to protect the skin, increase moisture, reduce inflammation, and promote wound healing was reviewed. Aloe vera and centella asiatica possess these beneficial properties. Aloe vera, in particular, helps heal wounds and moisturize the skin. Moreover, studies have confirmed that Aloe vera possesses antifungal, antibacterial, and anti-inflammatory properties. It helps reduce swelling of wounds within 24 to 48 hours and promotes new skin regeneration within five to six days. The wound-healing benefits of Aloe vera are significant as it helps reduce the risk of infection.11,16 Centella Asiatica, on the other hand, contains triterpenoid glycosides, including Asiatic acid, asiaticoside, and Madecassoside,17 which help promote wound healing and reduce skin inflammation. Moreover, these compounds have been found to accelerate collagen production, further stimulating the wound-healing process.18 Both herbs possess properties that can prevent and treat IAD and improve skin moisture. Based on these evidences, we were motivated to investigate the effects of using the products to prevent and manage IAD in older patients. This study was conducted by a multidisciplinary team that focused on the development and feasibility of using the products to prevent and treat IAD in older patients admitted to semi-intensive medical care units.
Objective
This pilot study aimed to assess the feasibility of integrating nursing activities with skin protection and care products for incontinence-associated dermatitis in older patients by comparing centella asiatica mixed with aloe vera and zinc oxide mixed with petroleum jelly.
Research Methodology
Design
This was a double-blind, randomized pilot study with a block-controlled trial and a two-group pre-posttest design. Both the participants and the assessors were blinded to which group was the experimental group and which was the control group. Quantitative and qualitative data were collected to provide comprehensive insights into the findings, which reflect the feasibility of using and measuring the effectiveness of the products for the prevention and treatment of IAD in older patients.
Setting and Sampling
The samples were selected using the randomization block method from older patients admitted to the semi-intensive medical care unit of a super tertiary university hospital in the northeastern region of Thailand. The inclusion criteria were: 1) new patients aged 60 years and older, both male and female, admitted to the semi-intensive medical care unit, either through new admissions from the emergency department or transfers from other wards; 2) patients or first-degree relatives who could provide consent to participate in the study; 3) having urinary/fecal incontinence, with watery stools occurring at least three times within 24 hours;19 and 4) presence of IAD. The exclusion criteria were: 1) receiving palliative care; 2) patients with allergies to topical zinc oxide, petroleum jelly, Centella Asiatica, or Aloe vera. A 2-hour forearm test was conducted, and any cases of itching or rash led to exclusion from the study.
The allocation concealment was performed using colored stickers to differentiate the types of products, ensuring that both the older patients and the assessors were unaware of which product each participant received. The older patients were assessed based on the inclusion criteria and then randomly selected using the block randomization technique until 20 older patients were chosen (Figure 1).
 |
Figure 1 Consort diagram. |
Intervention
The nursing program for preventing and caring for IAD consisted of eight activities. The program’s validity was proved, yielding a content validity index (CVI) of 1.00 and an index of item-objective congruence (IOC) of 0.873. The eight activities were as follows.
The first activity was education and skill training on IAD management. This activity involves providing knowledge and practical training on preventing and managing IAD. It includes hands-on practice on assessment using standardized assessment tools, interpreting assessment results, IAD management, and secondary infection control. Additionally, participants were trained to recognize early signs of IAD and understand the importance of proper skin care to minimize the risk of IAD. The second activity was risk and severity assessment. We assessed the risk of IAD using the PAT-T scale while using the IADIT-T scale assessed severity. Skin hydration was evaluated using the SkinUp device, and the skin’s pH was measured using the Skin pH Meter HI981037. The third activity involved identifying causes, contributing factors, and management strategies. This activity focused on identifying and managing the causes and risk factors associated with IAD, then collaborated with attending physicians to address these factors and minimize risks. The fourth activity was skin cleansing. We cleaned the perineal and genital areas with two to three drops of pH-balanced baby liquid soap (pH 4.0–6.8) and rinsed with 0.9% normal saline solution (NSS). The skin was gently patted dry with a soft towel, avoiding rubbing or scrubbing to prevent irritation.
The fifth activity was the application of protective skin products. This activity was divided into two groups. Group one received standard nursing care and applied an herbal-based protective product containing Centella Asiatica and Aloe Vera. However, group two received standard nursing care with a protective product containing zinc oxide and petroleum jelly. Both groups apply the designated product twice daily (morning and evening). If patients experience urinary or fecal incontinence, skin cleansing is performed according to protocol, followed by reapplication of the protective products. The sixth activity was repositioning the patient. Patients were repositioned every two hours, alternating between the left and right lateral positions to minimize prolonged exposure to urine or feces and promote air circulation. We monitored bowel and bladder function every two hours. The seventh activity was nutritional support. This activity includes collaborating with the attending physician to assess patients’ nutritional needs, ensuring adequate high-protein intake to promote skin healing and recovery from IAD, administering enteral feeding slowly over 3–4 hours to prevent diarrhea, monitoring for potential milk protein allergies in older patients, and observing adverse reactions to oral or enteral electrolyte supplements, such as elixir KCl and phosphate mixture. The final activity was outcome evaluation. We evaluated outcomes on day 7th after completing the program using the PAT-T scale, IADIT-T scale, SkinUp, and Skin pH Meter HI981037.
Data Collection Instruments
Five experts, including a doctor, two nursing lecturers, and two nurses, validated the quality of the data collection instrument. The content validity index (CVI) for all instruments was 1.00.3 The instruments consisted of three parts, as follows:
Part 1: General information record form (7 items): This included gender, age, weight, height, BMI, education, and occupation.
Part 2: Illness record form (15 items). It included the date of hospital admission, date of admission to the semi-intensive medical care unit, date of conducting research, initial diagnosis, underlying conditions, APACHE II score, antibiotics use, laxatives use, anesthesia use, level of consciousness, albumin levels, malnutrition screening using SPENT, Nutrition Screening Tool and Nutrition Alert Form (NAF), ability to perform activities of daily living using Barthel Activities of Daily Living Scale, urinary/fecal continence, use of excretory support devices, and use of oxygen or ventilator.
Part 3: Skin indicators record form: The following instruments were used for assessing IAD risk, the severity of IAD, skin surface pH, and skin surface moisture levels:
3.1 Thai Version of Perineal Assessment Tool (PAT-T):10 It was used to assess the risk based on the following four factors: 1) the severity and concentration of the irritant, 2) the duration of absorbent change, 3) the condition of the skin in the pelvic area, and 4) contributing factors such as hypoalbuminemia, antibiotic use, tube feeding, or gastrointestinal infection. The score ranges from 4 to 12 points, with a score of 4 −7 points indicating low risk and 8 −12 points indicating high risk.
3.2 Thai Version of Incontinence-Associated Dermatitis Intervention Tool (IADIT-T):20 This tool was used to assess patients developing IAD, categorized into severity levels as high risk, early IAD, moderate IAD, severe IAD, and fungal-appearing rash.
3.3 SkinUp:21 This tool was used to assess skin surface moisture, with 0–39% indicating dry skin, 40–60% indicating normal skin moisture, and 61–100% indicating excessive skin moisture.
3.4 Meter HI981037: An electrode was used to measure the skin surface pH directly. The instrument has a pH range of 0.00 to 12.00, with a resolution of 0.01 and an accuracy of ±0.05 pH, as tested by Neonics Co., Ltd. A pH less than 7 indicates an acidic environment, a pH of 7 indicates a neutral environment and a pH greater than 7 indicates an alkaline environment.
3.5 Daily bowel record form: This form was used to record the assessment of the frequency of bowel movements, the frequency of changing absorbent products, the amount of stool, and the characteristics of the stool using the Bristol Stool Chart.
Research Ethics
This study complied with the Declaration of Helsinki and was reviewed and approved by the Human Research Ethics Committee of Khon Kaen University, under the approval number: HE 671267, on August 27, 2024. The protocol registration was completed in the TCTR database, with registration number TCTR20240910009, on September 10, 2024. A clear explanation of the research topic, objectives, procedures, data collection timeline, and potential study benefits was provided during data collection. The older patients or their first-degree relatives with decision-making authority independently consent or refuse participation voluntarily. They were also informed that they could withdraw from the study without impacting their treatment. Photographs of selected case studies were taken before and after the interventions to document skin changes and healing. Only the perineal and buttocks areas were captured, ensuring patient anonymity and preserving privacy. The different characteristics of patients and severity levels of IAD among ICU patients were considered for providing various skin conditions and care strategies. Participants received study information and decided to participate in this study by signing the informed consent. Moreover, the patients consented to their cases being published. All collected data were kept confidential, and the overall research results were presented.
Data Collection Process
After obtaining ethics approval and completing the protocol registration, a letter was submitted to the ward administrator requesting permission to collect data. A meeting was held with the head nurse and registered nurses to clarify the data collection process, ensuring mutual understanding and compliance. The nurses responsible for caring for the samples were trained in the program and completed the training following the program for seven days. The initial assessments were carried out by a research assistant who was not involved in the ward’s daily operations. The assessments included risk assessment, severity of IAD, skin surface pH, and skin surface moisture. Additionally, the participants received all eight activities outlined in the program. The nurse lead of each shift assessed the progress using a checklist.
Data Analysis
In this pilot study, quantitative data were collected from 20 case studies. The data analysis was conducted and divided into three parts. Part 1: General information was analyzed using descriptive statistics, including percentage, mean, standard deviation, median, minimum, and maximum values. Differences in enumerated data were compared using the Chi-square test or Fisher’s exact test. Part 2: Continuous variables, including the risk scores for incontinence-associated dermatitis, skin surface pH, and skin surface moisture, were analyzed using non-parametric statistics. The comparison within groups before and after receiving the program was performed using the Wilcoxon signed-rank test. In contrast, the comparison between groups was conducted using the Mann–Whitney U-test. Part 3: The group variable, the incidence of incontinence-associated dermatitis, was analyzed using McNemar’s test. The severity was further analyzed using descriptive statistics, and the results were presented in tables and discussed. In addition, qualitative data were analyzed from 10 case studies (five cases from Experiment 1 and the other five from Experiment 2). The results were discussed to highlight differences in experimental results, with comparative images presented before and after the experiment.
Results
Possibility of Using the Nursing Program and IAD Products
The results of this pilot study confirmed the effectiveness of using Centella Asiatica mixed with Aloe vera product in treating IAD in older patients. The product’s properties were thoroughly examined, revealing that the Centella Asiatica mixed with Aloe vera product had the ideal viscosity, remained stable without separation, was white, and maintained an appropriate pH with low acidity. It also provided adequate moisture. When applied to the skin, it adhered well, was easy to clean, and could be stored at room temperature. In terms of efficacy, Centella Asiatica mixed with Aloe vera product was found to protect the skin from waste, reduce inflammation and irritation, lessen the severity of the condition, and alleviate IAD. The skin surface pH remained slightly acidic, and skin surface moisture increased to levels comparable to those achieved by the zinc oxide mixed with petroleum jelly product. However, the effectiveness of treating IAD was complemented by the 8-activity program, which contributed to the effective management of the condition.
“The Centella Asiatica mixed with Aloe vera has a moisturizing thick, white, colorless cream texture, making it ideal for skin protection. It effectively treats IAD in older patients and is easy to rinse off” RN01031024.
“The Centella Asiatica mixed with Aloe vera is easy and convenient to use, providing enough amount for 5-7 days of use. It has a non-sticky cream texture that spreads easily, enhances skin moisture, protects the skin, and helps reduce inflammation and redness” RN02151024.
Quantitative Study Results
General Characteristics of the Sample Group
The sample consisted of 20 participants, evenly distributed between males and females, with a mean age of 75.35±7.17 years. The majority were aged between 70 and 79 years (50%). Most participants had a normal body mass index (65%) and were retired government officers (60%). The primary reasons for hospital admission were respiratory diseases (60%) and bloodstream infections (60%), with 70% classified as severe cases. The most common comorbid conditions were hyperlipidemia (65%) and diabetes mellitus (60%), with no significant differences between the two groups (Table 1).
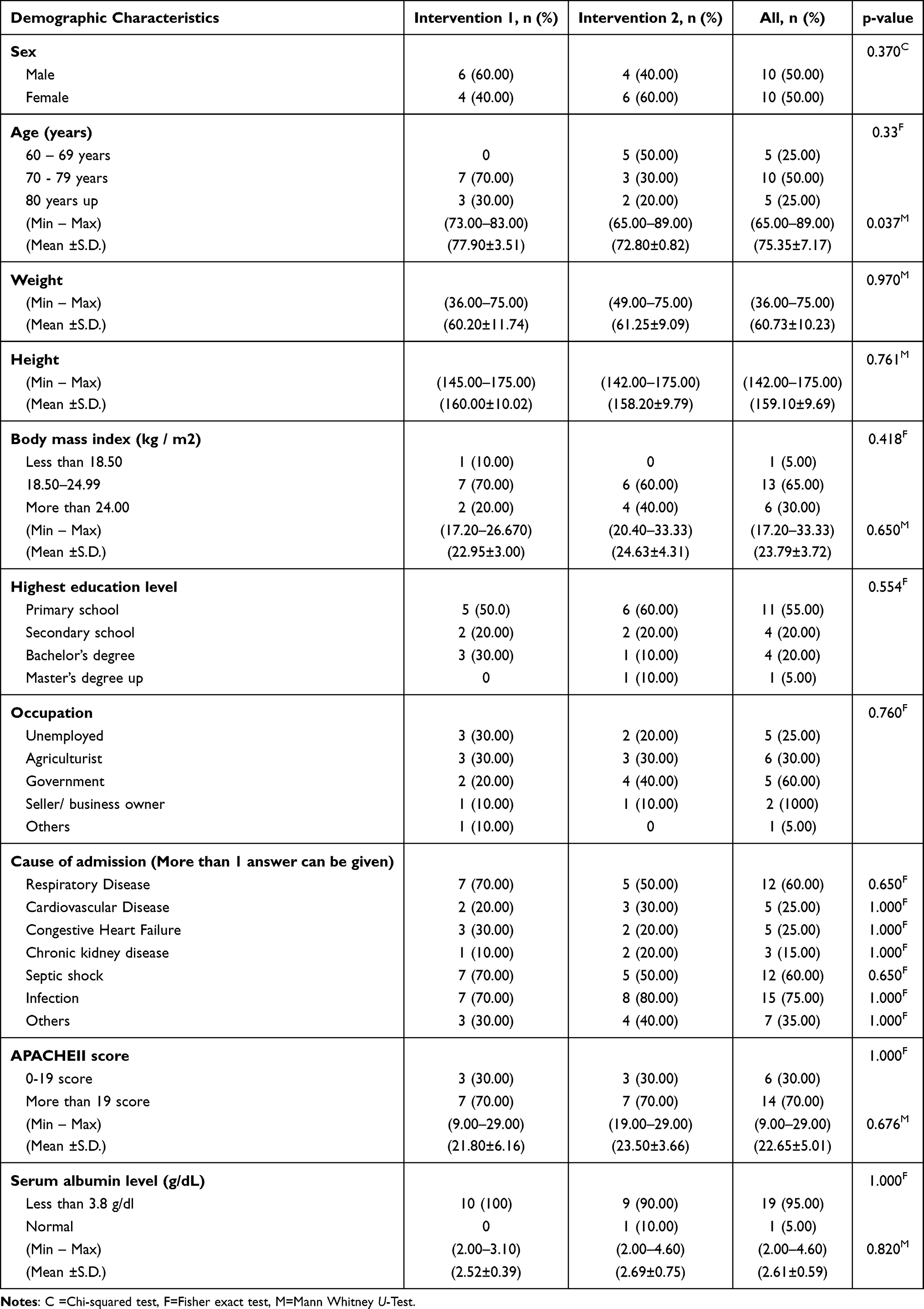 |
Table 1 Demographic Characteristics Among Older Patients (n=20) |
The Risk Factors for IAD in Older Patients
Most participants exhibited moderate levels of consciousness (80%) with an average Glasgow Coma Scale (GCS) score of 11.20±2.07. Most of the sample did not use sedatives (95%). Regarding bowel and bladder function, most received laxatives (70%) and antibiotics (90%), with 70% receiving two or more types. The Barthel Activities of Daily Living (ADL) assessment yielded an average score of 1.15±2.03. Nutritional risk assessment indicated that all participants were at risk of malnutrition (100%), with 80% experiencing severe malnutrition. Additionally, 80% of participants required oxygen therapy, 40% using a tracheostomy, and 40% using an endotracheal tube. Most participants were physically restrained (80%) and used disposable diapers for excretion management (100%). There were no significant differences between the two groups (Table 2).
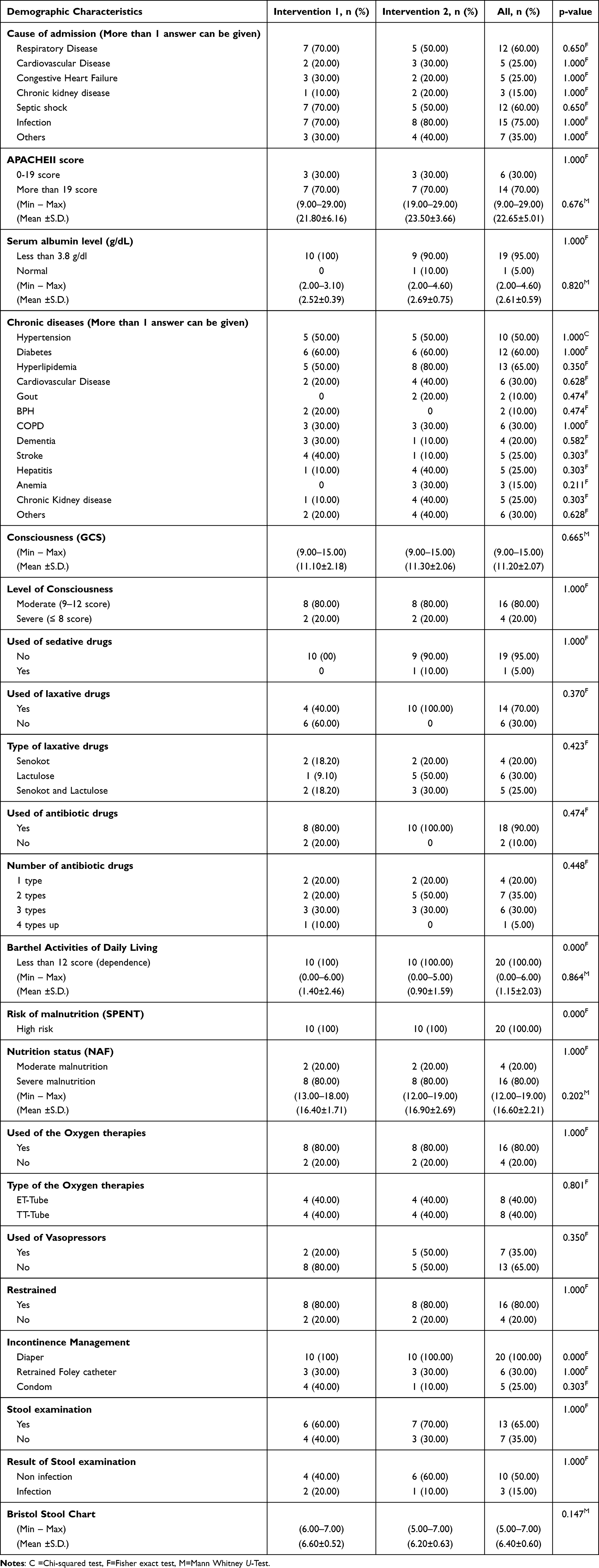 |
Table 2 History of Illness and Risk Factor of Older Patients (n=20) |
The Skin Indicators Within Group Comparison Before and After Intervention
Group Using Centella Asiatica Mixed with Aloe Vera
Before the intervention, participants exhibited a high risk of developing IAD (9.00±0.91). After the intervention, the risk significantly decreased to a lower level (6.20±0.91) (p=0.004). The initial skin pH was within the neutral range (7.57±0.39), which shifted to a mildly acidic level post-intervention (6.84±0.28) (p=0.005). Skin moisture levels improved from a low value (10.15±0.29) before the intervention to a higher level (13.06±1.29) after the intervention (p=0.005) (Table 3).
 |
Table 3 The Comparison Risks of Incontinence-Associated Dermatitis and Biomarkers Before and After Receiving Interventions Within Group Comparison Among Older Patients (n=20) |
Group Using Zinc Oxide Mixed Petroleum Jelly
Initially, the risk of developing IAD was high (10.03±1.06), which significantly reduced to a lower level post-intervention (6.30±1.42) (p=0.004). The initial skin pH was neutral (7.40±0.32), which shifted to a mildly acidic level (6.27±0.14) (p=0.005). Skin moisture levels improved from a low value (10.13±0.14) before the intervention to a higher level (12.73±0.60) after the intervention (p=0.005) (Table 3).
The Skin Indicators Between Groups Comparison Before and After Intervention
The Risk assessment for IAD revealed no significant difference between the two groups before the intervention (p=0.221), and both groups demonstrated lower risk levels post-intervention with no significant difference (p=0.803). Similarly, initial skin pH levels showed no difference between the groups (p=0.427). For post-intervention, both groups exhibited a shift to mildly acidic skin pH with no significant difference (p=0.075). Initial skin moisture levels also showed no significant difference (p=0.563), and both groups exhibited increased moisture levels post-intervention without significant differences (p=0.940) (Table 4).
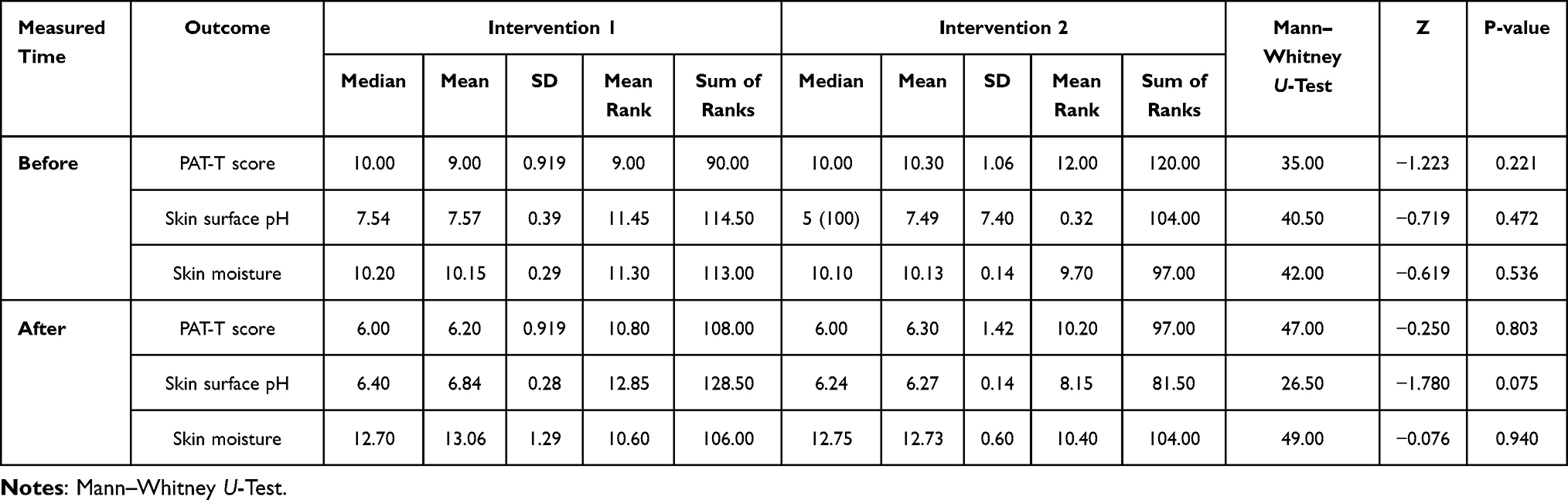 |
Table 4 The Comparison of IAD Risks and Biomarkers Before and After Receiving Interventions Between Groups Comparison Among Older Patients (n=20) |
The Result of IAD Incidence Within Group Comparison Before and After Intervention
The group using Centella Asiatica mixed with aloe vera had IAD (100%) prior to the intervention. However, the incidence of IAD decreased to 80% after intervention (p=0.500). The group using Zinc oxide mixed with petroleum jelly initially had IAD (100%). However, the incidence decreased to 60% (p=0.125) after intervention (Table 5).
 |
Table 5 The Comparison of the Incidence of Incontinence-Associated Dermatitis Cases Before and After Receiving Interventions Within Group Comparison Among Older Patients (n=20) |
The Comparison of IAD Incidence and Severity Between Groups Before and After Intervention
Post-intervention, the incidence of IAD did not differ significantly between the two groups (p=0.680) (Table 6). However, within the Centella Asiatica mixed with the Aloe Vera group, 20% of participants recovered from IAD, and the severity of the condition decreased from severe and moderate levels to mild (80%). In the zinc oxide mixed petroleum jelly group, 40% recovered from IAD, and the severity reduced from severe to mild (50%) and moderate (10%) (Table 7). These findings suggest that both formulations effectively reduced the risk and severity of IAD in older patients, with no significant difference between the two interventions.
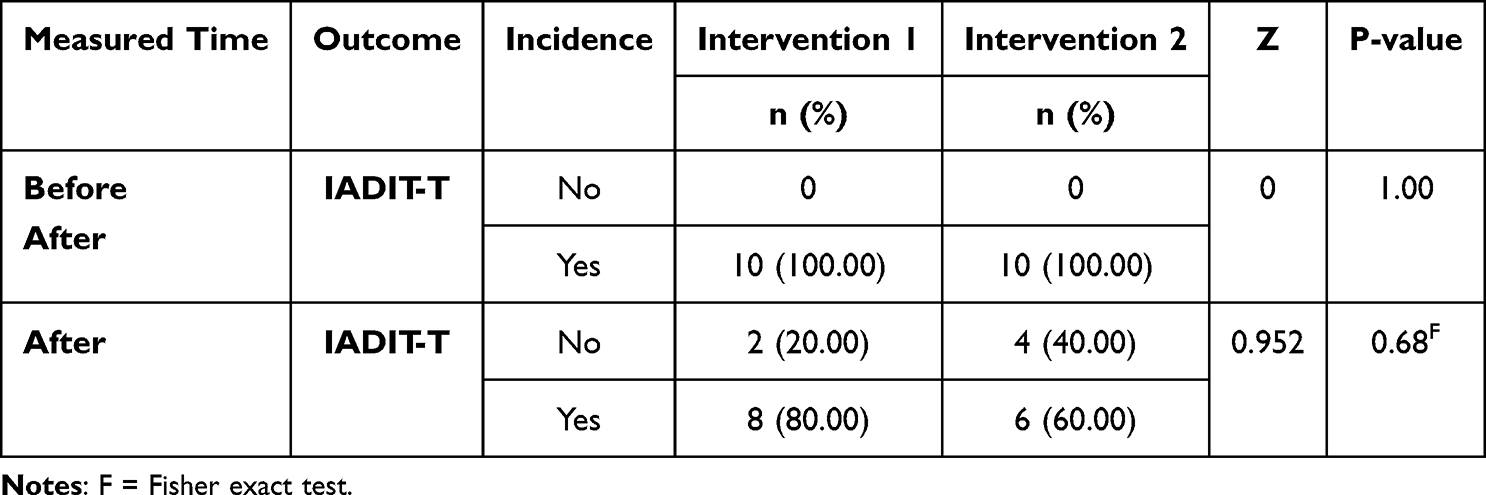 |
Table 6 The Comparison of the Incidence of IAD Before and After Receiving Interventions Between Groups Comparison Among Older Patients (n=20) |
 |
Table 7 The Comparison of the Severity of Incontinence-Associated Dermatitis Cases Before and After Receiving Interventions Among Older Patients (n=20) |
Qualitative Study Results
Intervention 1 The Centella Asiatica Mixed with Aloe Vera Group
Case Study 1
A 65-year-old female patient was admitted with pneumonia and septic shock, presenting with severe disease severity (APACHE II score = 22 points). The patient was at high risk for developing IAD (PAT-T score = 11 points), with contributing factors including: 1) overweight status (BMI = 31.22 kg/m²), 2) watery stools (Bristol stool chart type 7), 3) treatment with ATB Tazocin, 4) a lower albumin level (albumin = 2.3), 5) neutral skin pH of 7.98, and 6) low skin moisture (10.10). These factors led to moderate IAD. After seven days of treatment, the patient showed improvement, with the IAD starting to recover by day five. The risk assessment was reduced to low (PAT-T score = 6 points). The Centella Asiatica mixed with Aloe vera product resolved the underlying causes of IAD, increasing skin moisture to 13.10 and restoring a slightly acidic pH of 6.40 (Figures 2 and 3).
 |
Figure 2 Skin lesion of case 1 before receiving the program. |
 |
Figure 3 Skin lesion of case 1 after receiving the program. |
Case Study 2
A 76-year-old female patient was admitted with congestive heart failure with UTI with septic shock and bedridden status, presenting with severe disease severity (APACHE II score = 29 points). The patient was at high risk for developing IAD (PAT-T score = 12 points), with contributing factors including: 1) overweight status (BMI = 26.32 kg/m²), 2) watery stools (Bristol stool chart type 7), 3) treatment with ATB Augmentin, 4) a lower albumin level (albumin = 2.0), 5) neutral skin pH of 8.15, and 6) low skin moisture (9.10). These factors led to severe IAD. After seven days of treatment, the patient showed improvement, with early/mild IAD. The risk assessment was reduced to low (PAT-T score = 5 points). Centella Asiatica mixed with Aloe vera product resolved the underlying causes of IAD, increasing skin moisture to 12.32 and restoring a slightly acidic pH of 6.32 (Figures 4 and 5).
 |
Figure 4 Skin lesion of case 2 before receiving the program. |
 |
Figure 5 Skin lesion of case 2 after receiving the program. |
Case Study 3
A 73-year-old male patient was admitted with chronic obstructive pulmonary disease with acute exacerbation with pneumonia, presenting with severe disease severity (APACHEII score = 20 points). The patient was at high risk for developing IAD (PAT-T score = 10 points), with contributing factors including: 1) watery stools (Bristol stool chart type 6–7), 2) treatment with ATB Tazocin, 3) a lower albumin level (albumin = 2.1), 4) neutral skin pH of 7.13, and 6) low skin moisture (10.05). These factors led to moderate IAD. After seven days of treatment, the patient showed improvement, with early/mild IAD. The risk assessment was reduced to low (PAT-T score = 5 points). The Centella Asiatica mixed with Aloe vera product resolved the underlying causes of IAD, increasing skin moisture to 12.20 and restoring a slightly acidic pH of 6.62 (Figures 6 and 7).
 |
Figure 6 Skin lesion of case 3 before receiving the program. |
 |
Figure 7 Skin lesion of case 3 after receiving the program. |
Case Study 4
A 69-year-old male patient was admitted with acute kidney injury on top of chronic kidney disease with septic encephalopathy, presenting with severe disease severity (APACHE II score = 22 points). The patient was at high risk for developing IAD (PAT-T score = 10 points), with contributing factors including: 1) watery stools (Bristol stool chart type 7), 2) treatment with ATB Tazocin and Ceftazidime, 3) a lower albumin level (albumin = 2.0), 4) unconsciousness, 5) neutral skin pH of 7.42, and 6) low skin moisture (10.00). These factors led to moderate IAD. After seven days, the patient showed improvement, with the IAD starting to recover by day six. The risk assessment was reduced to low (PAT-T score = 5 points). The Centella Asiatica mixed with Aloe vera product resolved the underlying causes of IAD, increasing skin moisture to 12.42 and restoring a slightly acidic pH of 6.71 (Figures 8 and 9).
 |
Figure 8 Skin lesion of case 4 before receiving the program. |
 |
Figure 9 Skin lesion of case 4 after receiving the program. |
Case Study 5
A 72-year-old female patient was admitted with aspirate pneumonia with septic shock, presenting with severe disease severity (APACHE II score = 20 points). The patient was at high risk for developing IAD (PAT-T score = 11 points), with contributing factors including 1) watery stools (Bristol stool chart type 6–7), 2) treatment with ATB Meropenem and Levofloxacin, 3) a lower albumin level (albumin = 2.4), 4) Gastrointestinal infection, 5) neutral skin pH of 7.98, and 6) low skin moisture (10.10). These factors led to moderate IAD. After seven days of treatment, the patient showed improvement, with the IAD starting to recover by day six. The risk assessment was reduced to low (PAT-T score = 6 points). The Centella Asiatica mixed with Aloe vera product resolved the underlying causes of IAD, increasing skin moisture to 12.81 and restoring a slightly acidic pH of 6.61 (Figures 10 and 11).
 |
Figure 10 Skin lesion of case 5 before receiving the program. |
 |
Figure 11 Skin lesion of case 5 after receiving the program. |
Intervention 2 Zinc Oxide Mixed Petroleum Jelly
Case Study 6
A 65-year-old male patient was admitted with hepatic encephalopathy, presenting with severe disease severity (APACHE II score = 25 points). The patient was at high risk for developing IAD (PAT-T score = 12 points), with contributing factors including: 1) watery stools (Bristol stool chart type 7), 2) treatment with ATB ceftriaxone, 3) a lower albumin level (albumin = 2.0), 4) unconsciousness, 5) neutral skin pH of 8.10, and 6) low skin moisture (10.00). These factors led to moderate IAD. After seven days of treatment, the patient showed improvement, with the IAD starting to recover by day seven. The risk assessment was reduced to low (PAT-T score = 5 points). The Zinc oxide mixed petroleum jelly product resolved the underlying causes of IAD, increasing skin moisture to 11.79 and restoring a slightly acidic pH of 6.91 (Figures 12 and 13).
 |
Figure 12 Skin lesion of case 6 before receiving the program. |
 |
Figure 13 Skin lesion of case 6 after receiving the program. |
Case Study 7
A 75-year-old male patient was admitted with aspirate pneumonia with septic shock, presenting with severe disease severity (APACHE II score = 20 points). The patient was at high risk for developing IAD (PAT-T score = 10 points), with contributing factors including: 1) watery stools (Bristol stool chart type 6–7), 2) treatment with ATB Ceftazidime and Tazocin, 3) a lower albumin level (albumin = 2.3), 4) neutral skin pH of 7.56, and 5) low skin moisture (10.00). These factors led to moderate IAD. After seven days, the patient showed improvement, with early/mild IAD. The risk assessment was reduced to low (PAT-T score = 6 points). Using Zinc oxide mixed with petroleum jelly products resolved the underlying causes of IAD, increasing skin moisture to 11.69 and restoring a slightly acidic pH of 6.81 (Figures 14 and 15).
 |
Figure 14 Skin lesion of case 7 before receiving the program. |
 |
Figure 15 Skin lesion of case 7 after receiving the program. |
Case Study 8
An 81-year-old female patient was admitted with a urinary tract infection with septic shock, presenting with severe disease severity (APACHE II score = 22 points). The patient was at high risk for developing IAD (PAT-T score = 10 points), with contributing factors including: 1) watery stools (Bristol stool chart type 6–7), 2) treatment with ATB Meropenem and Levofloxacin, 3) a lower albumin level (albumin = 2.3), 4) neutral skin pH of 7.76, and 5) low skin moisture (10.10). These factors led to moderate IAD. After seven days of treatment, the patient showed improvement, with the IAD starting to recover by day six. The risk assessment was reduced to low (PAT-T score = 6 points). Using Zinc oxide mixed with petroleum jelly products resolved the underlying causes of IAD, increasing skin moisture to 12.10 and restoring a slightly acidic pH of 6.73 (Figures 16 and 17).
 |
Figure 16 Skin lesion of case 8 before receiving the program. |
 |
Figure 17 Skin lesion of case 8 after receiving the program. |
Case Study 9
A 70-year-old female patient was admitted with a hypertensive emergency with aspirate pneumonia with septic shock, presenting with severe disease severity (APACHE II score = 20 points). The patient was at high risk for developing IAD (PAT-T score = 10 points), with contributing factors including: 1) watery stools (Bristol stool chart type 6–7), 2) treatment with ATB Meropenem and Ceftazidime, 3) a lower albumin level (albumin = 2.2), 4) neutral skin pH of 8.13, and 5) low skin moisture (9.89). These factors led to severe IAD. After seven days of treatment, the patient showed improvement, with early/mild IAD. The risk assessment was reduced to low (PAT-T score = 6 points). Using zinc oxide mixed with petroleum jelly resolved the underlying causes of IAD, increasing skin moisture to 12.30 and restoring a slightly acidic pH of 6.65 (Figures 18 and 19).
 |
Figure 18 Skin lesion of case 9 before receiving the program. |
 |
Figure 19 Skin lesion of case 9 after receiving the program. |
Case Study 10
A 76-year-old female patient was admitted with aspirate pneumonia with septic shock, presenting with severe disease severity (APACHE II score = 22 points). The patient was at high risk for developing IAD (PAT-T score = 10 points), with contributing factors including: 1) watery stools (Bristol stool chart type 6–7), 2) treatment with ATB Tazocin, 3) a lower albumin level (albumin = 2.4), 4) neutral skin pH of 7.82, and 5) low skin moisture (10.10). These factors led to the severity of IAD. After seven days, the patient showed improvement, with early/mild IAD. The risk assessment was reduced to low (PAT-T score = 6 points). Using Zinc oxide mixed with petroleum jelly products resolved the underlying causes of IAD, increasing skin moisture to 12.10 and restoring a slightly acidic pH of 6.79 (Figures 20 and 21). The graphs demonstrated the changes and improvements in skin indicators for 20 participants were demonstrated (Figures 22–25).
 |
Figure 20 Skin lesion of case 10 before receiving the program. |
 |
Figure 21 Skin lesion of case 10 after receiving the program. |
 |
Figure 22 The changes in risk of IAD before and after receiving the program. |
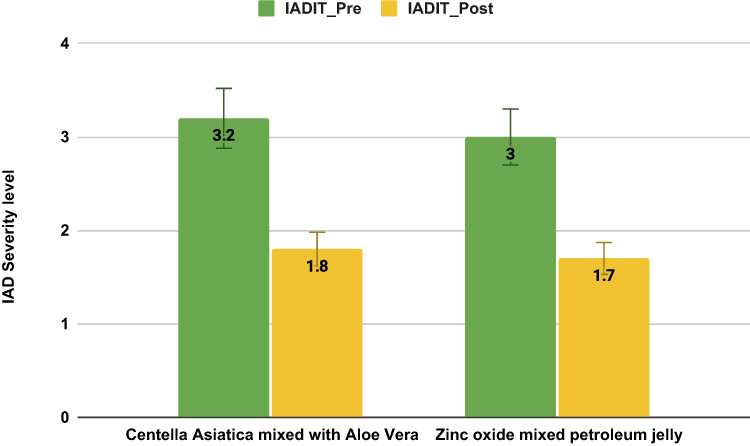 |
Figure 23 The changes in the severity of IAD before and after receiving the program. |
 |
Figure 24 The changes in skin pH before and after receiving the program. |
 |
Figure 25 The changes in moisture before and after receiving the program. |
Discussion
IAD is a common problem among older patients admitted to intensive or semi-intensive care units.2,22 This condition is caused by prolonged exposure to urine and feces, leading to skin erosion, swelling, inflammation, and discomfort, such as pain and burning. These symptoms significantly affect the quality of life for hospitalized patients. After applying the product containing Centella Asiatica mixed with Aloe vera to areas affected by IAD, the skin showed improvement after seven days, with reduced inflammation, diminished redness, and increased moisture. The Centella Asiatica mixed with Aloe vera formulation helps form a protective barrier on the skin, shielding it from waste such as urine and feces.23 Centella extract has known properties to reduce skin inflammation, promote wound healing, relieve pain, and stimulate collagen production, all contributing to increased skin surface moisture.18 Aloe vera is lightweight on the skin and is known for its ability to soothe inflammation, reduce redness from irritation and burns, and enhance skin hydration.11,16 These results align with the findings of Stepán et al (2014),24 investigating the effectiveness of herbal extract cream in the treatment of pressure ulcers. The study demonstrated that herbs can reduce inflammation, promote wound healing, and accelerate recovery. Similarly, Winkfield et al (2024)25 examined the keratin-based topical cream containing protein components that enhance skin surface moisture. This study revealed that the cream effectively treated burning and radiation dermatitis in breast cancer patients. The study above highlights that when developing creams or products, it is crucial to consider the specific purpose and properties of the ingredients to ensure their suitability for the intended use. Our pilot study, which tested the use of the product combining Centella Asiatica mixed with Aloe Vera, demonstrated that such a formulation effectively treated IAD.
The comparison between the Centella Asiatica mixed with Aloe vera product and the zinc oxide mixed with petroleum jelly product revealed that both were feasible for patients to use in a clinical setting and effectively treated IAD in older patients. No significant differences were observed between the two groups in this study, as both had similar contexts, general characteristics, and health conditions. Therefore, the Centella Asiatica mixed with Aloe vera product was as effective as the zinc oxide mixed with petroleum jelly in protecting and treating IAD in older patients. Zinc oxide mixed with petroleum jelly is a well-established treatment in modern and standard medicine for IAD in critically ill patients.13 Based on the feedback from the nurse who applied the two products for this pilot study, Zinc oxide mixed with petroleum jelly has an appropriate viscosity, is moisturizing, easy to apply, and simple to clean, allowing for clear skin assessment, similar to the developed product was made from Thai herbal plants. Additionally, Thai herbal plants have properties that help reduce inflammation, decrease redness, increase moisture, and promote faster wound healing.11,18 As locally available plants, it enhances the use of Thai herbs in treating IAD. This finding aligns with Brunner et al’s (2012)26 and Pather et al (2017)22 research, examining the products designed to protect skin from IAD. These products demonstrated key properties: 1) forming a protective layer on the skin, 2) being lightweight and easy to apply, allowing for practical skin assessment, and 3) increasing skin surface moisture. Therefore, with its anti-inflammatory, moisturizing, and skin-barrier properties, Centella Asiatica mixed with Aloe vera is a practical and effective treatment for IAD in older patients, serving as a modern standard treatment, similar to zinc oxide mixed with petroleum jelly.
Our product contains coconut oil, beeswax, lanolin, shea butter, Aloe vera, and Centella Asiatica. These ingredients increase skin moisture and provide the appropriate viscosity to protect the skin from waste. Centella Asiatica contains triterpenoid glycosides, asiatic acid, asiaticoside, and madecassic acid (also known as Madecassol).17 It has properties that promote wound healing and reduce skin inflammation, while Aloe vera is effective in killing fungi and bacteria and reducing inflammation. Aloe vera helps reduce swelling of wounds within 24 to 48 hours, and new skin forms by days 5–6. Accelerating wound healing is beneficial in preventing infection.16 The results of this study were consistent with previous findings, showing that after the intervention, the experimental group experienced a reduction in the severity and incidence of IAD, inflammation, and redness. Patients reported feeling more comfortable, with burning and pain alleviated within seven days. Compared with zinc oxide mixed with petroleum jelly, the experimental product was equally effective in protecting the skin and treating IAD in older patients.13 This result is in line with the study by Kon et al (2017),27 which compared the 3M Cavilon product to standard nursing care in older female patients and found that the experimental group, using 3M Cavilon, had better skin protection than the group receiving standard care. Like the product used in this study, 3M Cavilon cream can protect the skin from waste contact, increase skin moisture, reduce inflammation, and promote wound healing. This study also indicated that the Centella Asiatica mixed with Aloe vera product helped increase skin surface moisture, adjusted the skin surface pH to a more suitable level, and was quickly absorbed into the skin, further enhancing wound healing and promoting faster recovery.
A study indicates that healthy skin typically has a slightly acidic pH ranging from 4.1 to 5.8.8 In this study, the product developed by the researcher team contained ingredients with a slightly acidic pH, which is ideal for maintaining skin balance. This pH level supports faster wound healing and inhibits the growth of bacteria and microorganisms, thus preventing skin infections.8 Moreover, the study revealed that the samples did not experience recurrent infections and successfully recovered from IAD. These results are consistent with findings from Glass et al (2021)12 and Kone et al (2017),27 investigating the effectiveness of 3M Cavilon products in critically ill patients with IAD. The 3M Cavilon products’ skin-coating properties can protect the skin from highly alkaline waste. The study demonstrated that the product effectively balanced the skin surface pH to a slightly acidic, facilitating faster wound healing and preventing skin infections. Sommana et al (2024)3 explored the feasibility of using the nursing program to prevent IAD by applying zinc oxide and petroleum jelly skin protection products among older patients. Zinc oxide mixed with petroleum jelly coats the skin and prevents waste from penetrating. After the experiment, the results showed that the products effectively protected the skin. It adjusted the skin surface pH to a slightly acidic level, which was well-suited to the skin condition and prevented the development of associated dermatitis in older patients.
However, for the prevention and management of associated dermatitis in older patients, alongside using the skin protection product developed by the researcher team, which was Centella asiatica mixed with Aloe vera, it is essential to implement eight comprehensive nursing activities, including: 1) providing knowledge, 2) conducting assessments, 3) identifying causes and risk factors, and addressing them, 4) performing proper cleaning, 5) applying skin protection products, 6) repositioning patients, 7) promoting nutrition, and 8) evaluating outcomes. These eight activities were derived from a systematic literature review by Banharak et al (2021).2 This study’s control and experimental groups followed the same program, and their demographic characteristics were comparable. However, the fifth activity differed, as the experimental group received Centella asiatica mixed with Aloe vera. In contrast, the control group was given zinc oxide mixed with petroleum jelly, a widely accepted treatment for IAD. The results showed that the effectiveness of treating IAD in older patients was not different between the two groups suggesting that the program, combined with the use of Centella asiatica mixed with Aloe vera, is effective in preventing and treating IAD in older patients when compared with standard product. This finding aligns with the research of Qiao & Banharak (2023),4 which conducted a literature review and tested the use of these eight activities among ICU older patients, finding that they effectively protected the skin and managed IAD in older patients. Similarly, the study by Sommana et al (2024)3 examined the feasibility of using the nursing program to prevent IAD in older patients and found that the eight nursing activities, when used together with skin protection products, were effective in caring for and preventing IAD. If the nurse expects the same results in practice, the products should be applied to the eight nursing activities.
Limitations
This pilot study had a small sample size, which limited the statistical power and reduced the reliability of the findings. Consequently, the generalizability of the study results is constrained.
Recommendations
Future studies should increase the sample size to enhance statistical power, enable a more comprehensive analysis, and improve research credibility. Although the history of illness and risk factors were not different between the two groups, these factors might affect the healing of IAD, and this point should be a concern for future studies. Additionally, rigorous research designs, such as randomized controlled trials (RCTs), should be employed to ensure the reliability and validity of nursing interventions and the efficacy of products.
Conclusion
This pilot study evaluated the feasibility of using Centella asiatica mixed with Aloe vera to treat IAD in older patients in the semi-intensive medical care unit. The registered nurse reflected on the acceptability and feasibility of using this local Thai herb product in the clinical setting. The product was practical and relied on nursing interventions and critical care contexts. Moreover, the results showed that the product can effectively protect the skin and treat IAD in older patients. It can also help heal wounds, reduce skin inflammation, increase skin moisture, and adjust the skin surface pH to a slightly acidic level, which is suitable for the skin condition. As a result, it can promote faster recovery from IAD and yield results comparable to those of zinc oxide mixed with petroleum jelly, a current standard treatment for IAD.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to prohibited laws (and/or rules, regulations, and contracts). However, they are available from the corresponding author upon reasonable request.
Funding
This study was financially supported by the Faculty of Medicine, Khon Kaen University, Thailand (Grant Number IN68010). We extend our appreciation to the research fund for making this study possible.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Beeckman D, Verhaeghe S, Defloor T, Schoonhoven L, Vanderwee K. A 3-in-1 perineal care washcloth impregnated with dimethicone 3% versus water and pH neutral soap to prevent and treat incontinence-associated dermatitis: a randomized, controlled clinical trial. Journal of Wound, Ostomy, and Continence Nursing: Official Publication of the Wound, Ostomy and Continence Nurses Society. 2011;38(6):627–634. doi:10.1097/WON.0b013e31822efe52
2. Banharak S, Panpanit L, Subindee S, et al. Prevention and Care for Incontinence-Associated Dermatitis among Older Adults: a Systematic Review. Journal of Multidisciplinary Healthcare. 2021;14:2983–3004. doi:10.2147/JMDH.S329672
3. Sommana C, Banharak S, Sim-Im S, Ransinyo K. Effects of Nursing Program in Preventing Incontinence-Associated Dermatitis by Applying Zinc Oxide and Petroleum Jelly Skin Protection Products Among Older Patients in Semi-Intensive Medical Care Units: a Pilot Study. Journal of Multidisciplinary Healthcare. 2024;17:3619–3636. doi:10.2147/JMDH.S469276
4. Qiao G, Banharak S. Incontinence-Associated Dermatitis in Older Intensive Care Patients: a Review and Case Report. Journal of Multidisciplinary Healthcare. 2023;16:3299–3308. doi:10.2147/JMDH.S434275
5. Khalid KA, Nawi AFM, Zulkifli N, Barkat MA, Hadi H. Aging and Wound Healing of the Skin: a Review of Clinical and Pathophysiological Hallmarks. Life. 2022;12(12):2142. doi:10.3390/life12122142
6. Limpawattana P. Geriatric Syndromes and Interesting Health Issues.
7. Kayser SA, Phipps L, VanGilder CA, Lachenbruch C. Examining Prevalence and Risk Factors of Incontinence-Associated Dermatitis Using the International Pressure Ulcer Prevalence Survey. Journal of Wound, Ostomy, and Continence Nursing: Official Publication of the Wound, Ostomy and Continence Nurses Society. 2019;46(4):285–290. doi:10.1097/WON.0000000000000548
8. Proksch E. pH in nature, humans and skin. J Dermatol. 2018;45(9):1044–1052. doi:10.1111/1346-8138.14489
9. Johansen E, Bakken LN, Duvaland E, et al. Incontinence-Associated Dermatitis (IAD): prevalence and Associated Factors in 4 Hospitals in Southeast Norway. Journal of Wound, Ostomy & Continence Nursing. 2018;45(6):527–531. doi:10.1097/WON.0000000000000480
10. Simim S, Banharak S, Panpanit L, et al. Translation, psychometric testing and implementation of the perineal assessment tool for assessing incontinence-associated dermatitis risk in semi-intensive care patients. Sci Rep. 2024;14(1):29787. doi:10.1038/s41598-024-81577-7
11. Ghanadi A, Salami M. Anti-inflammatory properties of Aloe vera gel on skin. Eur J Pharmacol. 2017;815:94–103.
12. Glass Jr GF, Goh CCK, Cheong RQ, Ong ZL, Khong PCB, Chan EY. Effectiveness of skin cleanser and protectant regimen on incontinence-associated dermatitis outcomes in acute care patients: a cluster randomised trial. Int Wound J. 2021;18(6):862–873. doi:10.1111/iwj.13588
13. Phungsiri P. The Effect of Utilizing Work Instruction for Incontinence Associated Dermatitis in High-Risk Patient. Journal of Public Medical. 2016;30:59–67.
14. Baatenburg de Jong H, Admiraal H. Comparing cost per use of 3M Cavilon No Sting Barrier Film with zinc oxide oil in incontinent patients. J Wound Care. 2004;13(9):398–400. doi:10.12968/jowc.2004.13.9.27264
15. Shaw SZ, Nien HH, Wu CJ, Lui LT, Su JF, Lang CH. 3M Cavilon No-Sting Barrier Film or topical corticosteroid (mometasone furoate) for protection against radiation dermatitis: a clinical trial. Journal of the Formosan Medical Association = Taiwan Yi Zhi. 2015;114(5):407–414. doi:10.1016/j.jfma.2013.04.003
16. Gupta A, Yadav L. Aloe vera: a miraculous plant for skin care. Int J Herbal Med. 2013;1(5):10–15.
17. Choi H, Shin HS. Centella Asiatica: a Comprehensive Review of Its Phytochemistry and Therapeutic Applications. Phytother Res. 2019;33(5):1060–1081. doi:10.1002/ptr.6348
18. Sur, et al. Wound Healing Properties of Centella asiatica: a Review. Pharm Biol. 2020;58(1):10–17. doi:10.1080/13880209.2020.1848242
19. Bliss DZ, Mathiason MA, Gurvich O, et al. Incidence and predictors of incontinence-associated skin damage in nursing home residents with new-onset incontinence. J Wound Ostomy Cont Nurs. 2017;44(2):165–171. doi:10.1097/WON.0000000000000313
20. Supin Simim. 2023. Translation, Psychometric Test and Implementation of Perineal Assessment Tool (PAT) and Incontinence - Associated Dermatitis Intervention Tool (IADIT) Among Patients in Semi Intensive Medical Care Units. Master of Nursing Science Thesis in Gerontological Nursing, Graduate School, Khon Kaen University.
21. Westermann TVA, Viana VR, Berto Junior C, Detoni da Silva CB, Carvalho ELS, Pupe CG. Measurement of skin hydration with a portable device (SkinUp® Beauty Device) and comparison with the Corneometer®. Skin Research and Technology: Official Journal of International Society for Bioengineering and the Skin (ISBS) [And] International Society for Digital Imaging of Skin (ISDIS) [And] International Society for Skin Imaging (ISSI). 2020;26(4):571–576. doi:10.1111/srt.12833
22. Pather P, Hines S, Kynoch K, Coyer F. Effectiveness of topical skin products in the treatment and prevention of incontinence-associated dermatitis: a systematic review. JBI Database of Systematic Reviews and Implementation Reports. 2017;15(5):1473–1496. doi:10.11124/JBISRIR-2016-003015
23. Baskaran R, Priya LB, Sathish Kumar V, Padma VV. Tinospora cordifolia extract prevents cadmium-induced oxidative stress and hepatotoxicity in experimental rats. J Ayurveda Integr Med. 2018;9(4):252–257. doi:10.1016/j.jaim.2017.07.005
24. Stepán J, Ehrlichova J, Hladikova M. Therapieergebnisse und Anwendungssicherheit von Symphytum-Herba-Extrakt-Creme in der Behandlung von Dekubitus [Efficacy and safety of Symphytum herb extract cream in the treatment of pressure ulcers]. Zeitschrift fur Gerontologie und Geriatrie. 2014;47(3):228–235. doi:10.1007/s00391-013-0522-8
25. Winkfield KM, Hughes RT, Brown DR, et al. Randomized Pilot Study of a Keratin-based Topical Cream for Radiation Dermatitis in Breast Cancer Patients. Technology in Cancer Research & Treatment. 2024;23:15330338231222137. doi:10.1177/15330338231222137
26. Brunner M, Droegemueller C, Rivers S, Deuser WE. Prevention of incontinence-related skin breakdown for acute and critical care patients: comparison of two products. Urol Nurs. 2012;32(4):214–219. doi:10.7257/1053-816X.2012.32.4.214
27. Kon Y, Ichikawa-Shigeta Y, Iuchi T, et al. Effects of a Skin Barrier Cream on Management of Incontinence-Associated Dermatitis in Older Women: a Cluster Randomized Controlled Trial. J Wound Ostomy Cont Nurs. 2017;44(5):481–486. doi:10.1097/WON.0000000000000353
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Adverse Reactions to Facemasks in Health-Care Workers: A Cross-Sectional Survey
Liu N, Ye M, Zhu Q, Chen D, Xu M, He J, Li Q, Li J
Clinical, Cosmetic and Investigational Dermatology 2022, 15:947-954
Published Date: 25 May 2022
Nursing Program Applying Lithospermum Oil for Incontinence-Associated Dermatitis Care Among Older Patients in Intensive Care Units: A Randomized Controlled Trial
Qiao G, Banharak S, Panpanit L, Sae-Sia W, Promnoi C
Clinical Interventions in Aging 2025, 20:1401-1415
Published Date: 28 August 2025