Back to Journals » Clinical Interventions in Aging » Volume 20
Nursing Program Applying Lithospermum Oil for Incontinence-Associated Dermatitis Care Among Older Patients in Intensive Care Units: A Randomized Controlled Trial
Authors Qiao G, Banharak S ![]() , Panpanit L, Sae-Sia W, Promnoi C
, Panpanit L, Sae-Sia W, Promnoi C
Received 28 April 2025
Accepted for publication 18 August 2025
Published 28 August 2025 Volume 2025:20 Pages 1401—1415
DOI https://doi.org/10.2147/CIA.S535087
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Guojin Qiao,1 Samoraphop Banharak,2 Ladawan Panpanit,2 Wipa Sae-Sia,3 Chantra Promnoi4
1Nursing Department, Affiliated Hospital of Guizhou Medical University, Guiyang, Guizhou, People’s Republic of China; 2Department of Gerontological Nursing, Faculty of Nursing, Khon Kaen University, Meaung, Khon Kaen Thailand; 3Department of Adult and Gerontological Nursing in Surgery, Faculty of Nursing, Prince of Songkla University, Hat Yai, Songkhla Thailand; 4Department of Fundamental Nursing Profession, Faculty of Nursing, Prince of Songkla University, Hat Yai, Songkhla Thailand
Correspondence: Samoraphop Banharak, Department of Gerontological Nursing, Faculty of Nursing, Khon Kaen University, 123 Moo 16 Friendship Road, Mueang, Khon Kaen, 40002, Thailand, Tel +6661-930-8118, Fax +6643-424-809, Email [email protected]
Background: Incontinence-associated dermatitis affects patients admitted to the intensive care unit, especially older adults, physically, mentally, and emotionally. Therefore, nursing activities to prevent and care for incontinence-associated dermatitis are important and necessary for healthcare staff and caregivers. This study aimed to explore the effectiveness of a nursing prevention and care program involving the application of Lithospermum Oil on the risk, severity, and incidence rate of incontinence-associated dermatitis among older adult intensive care unit patients.
Methods: This randomized controlled trial was conducted from July 2023 to October 2023. Sixty-eight samples were recruited by systematic random sampling and equally divided into two groups by simple random sampling. The experimental group received a nursing prevention and care program that involved applying Lithospermum Oil for five days; however, a control group received routine care.
Results: After attending the program, the risk level of IAD in the experimental group was no different from that before the application or from the control group. However, after the experiment, the incidence of IAD in the experimental group was significantly lower than in the control group. Finally, the severity of IAD in the experimental group before the experiment did not significantly differ from that after the experiment or from the control group.
Conclusion: This study’s findings indicate that the intervention effectively reduces the incidence of IAD but does not significantly impact its risk or severity. Nursing prevention and care programs and Lithospermum Oil should be integrated into routine clinical practice to enhance patient care and minimize skin-related complications.
Plain Language Summary: Incontinence-associated dermatitis (IAD) is skin damage that can lead to physical, mental, and emotional issues while also contributing to severe skin problems like pressure ulcers, prolonged hospital stays, and increased treatment costs.Older adults, especially those in the intensive care unit, often experience incontinence, a significant cause of IAD.Patients with IAD are ten times more likely to develop pressure ulcers compared to those without IAD.A systematic review provided the eight nursing strategies for IAD prevention and care; however, Chinese herbs, such as Lithospermum oil, are not included.This study proved that a prevention and care program involving the application of Lithospermum oil can reduce the number of cases developing IAD.
Keywords: aged, critical care, dermatitis, herb, intensive care, skin care
Introduction
Incontinence-associated dermatitis (IAD) is a significant problem among older adults who are hospitalized, especially those in intensive care units.1,2 Mostly, IAD leads to sores in the groin and genital areas3 and can occur in both males and females. Additionally, older adults with this condition often experience pain at the wound site, burning, itching, insomnia, and may even develop depression.4 The primary cause is the loss of bowel control.5 Risk factors include improper cleaning, friction, inappropriate cleaning products, and prolonged periods of lying in the same position.3 Older adults, in particular, are at a higher risk due to the body’s degenerative processes, which cause the skin to thin and lose moisture. This decline related to aging makes them more susceptible to IAD than other age groups.1–3 When IAD occurs, there is a high risk of complications, such as infected wounds and pressure ulcers, which are ten times more likely to develop in older adults compared to other age groups.1,2 A study on the prevention and care of IAD in older adults found that Lithospermum oil is widely used in China. Research on its properties indicates that it penetrates the skin, protects it from waste, and reduces inflammation and redness.6,7 Furthermore, the nursing process is a crucial tool that enables nurses to provide standardized care to patients. This process includes assessment, diagnosis, planning, implementation, and evaluation.8 Integrating interventions related to the nursing process, combined with Lithospermum oil, could provide effective management of IAD among older ICU patients.
Background
IAD is the most prevalent skin condition among incontinent individuals, characterized by inflammation and skin deterioration in the perianal and perineal regions. This dermatitis is caused by chemical irritation from prolonged exposure to urine and feces in individuals with urinary and fecal incontinence.3,4 It commonly affects the perineum, buttocks, groin, scrotum, labia, inner thighs, and lower back. IAD often leads to severe itching, prompting frequent scratching, which can worsen skin damage and increase the risk of complications such as pressure ulcers and secondary infections.3
Skin damage is a sensitive quality indicator closely related to patient safety, posing significant challenges in clinical practice.9 IAD patients often feel very uncomfortable and experience pain, burning, itching, or tingling in the inflamed skin area.4 Skin lesions associated with IAD are susceptible to infection due to impaired barrier function. In addition, IAD may prolong a patient’s hospital stay, increase medical costs and the workload of caregivers, as well as reduce the patient’s quality of life.1
The primary risk factor for IAD is incontinence, so the prevention, treatment, and management of incontinence are crucial for the prevention and care of IAD.5 When urine and feces are in contact for a long time, not only does overhydration of the skin occur, but the skin pH, which is usually acidic, can also become alkaline,3 resulting in an inflammatory skin reaction. Therefore, when the patient’s skin is contaminated, the skin should be cleaned immediately. Friction in cleaning removes the skin cuticle and thins the skin,10 especially for older adults. Older adults have more fragile skin than other age groups since they experience an aging process, so caregivers should choose soft wipes to clean the skin.
Gray and Giuliano investigated the prevalence of IAD in 36 states of the United States in 2018, and they found that the overall prevalence of IAD was 21.3% (1140/5342), and the prevalence of IAD in incontinence patients was 45.7% (1140/2492).11 Campbell et al12 reported that the incidence of IAD in hospitalized patients was 19–50%, the incidence of incontinence dermatitis in stroke was 5.6–50%, the mean age of the patients was 62 years, and the rate of incontinence was higher in female than in male. In the ICU, the incidence of IAD can be as high as 45%;13 the mean age of the patients was 65.1 years, and 67% was male, so it had an even higher incidence among older patients in the ICU. A Chinese study of 11 hospitals in Zhejiang province found that the incidence of IAD in the ICU was 35.1%.14 According to the data, it can be found that the ICU ward is a place where elderly critically ill patients are concentrated, and the incidence of IAD is at a high level.
Skin protectors, or moisture-proof or occluding moisturizers, provide a protective membrane that protects the skin from chemical irritants and pathogens in feces and urine.15 The standard skin protectant has a petroleum jelly matrix, dimethyl silicone oil matrix, zinc oxide matrix, and oily and liquid acrylate film. Vaseline matrix can effectively avoid skin irritation, but the moisturizing effect is moderate; the moisturizing effect of dimethyl silicone oil matrix is good, but the concentration of dimethyl silicone oil will affect its skin protection effect. Zinc oxide matrix has a good skin protection effect but is not easy to clean. Oily skin protectants can form a protective film after application, avoid being impregnated by urine, feces, and other impurities, and reduce skin friction. The main skin products are skin moisturizer, camellia oil, and Lithospermum oil. Powder mainly produces absorption; for example, after smear, it can absorb the water in urine or stool, but the powder may produce particles due to water. The use of powder needs to increase the frequency of cleaning, and the nursing workload, so the use of powder is not much in clinical practice; oil is more convenient for clinical use. Lithospermum oil is widely used in infants with red buttocks, skin eczema, and IAD; it is a traditional Chinese medicine that is mainly used to block the contact of excreta and skin, promote blood circulation on the skin surface, promote epidermal growth, and inhibit the growth of bacteria on the wound.6,7
The nursing process is a tool for nurses to provide standard care for the patient. This process includes assessment, diagnosis, planning, implementation, and evaluation.8 In the IAD prevention and care process, the nursing process assessment includes the patient’s risk factors and the severity of IAD. According to the assessment results, the risk degree of IAD, whether the patient has IAD, and the severity of IAD patients can be diagnosed. According to the nursing diagnosis of patients, corresponding nursing plans were made, such as the prevention strategy of Lithospermum oil for high-risk IAD patients and the nursing intervention strategy for severe IAD patients. The nursing process is a program construct, and Lithospermum oil is added to promote skin care. The intervention was implemented according to the care plan, and the patient’s outcome was finally evaluated.
In conclusion, research has highlighted the high incidence of IAD among older patients with incontinence in ICU, along with its increased severity, associated discomfort, higher healthcare costs, and more significant nursing workload.4,11,13 Despite the need for effective preventive and management interventions, ICU nurses often do not prioritize IAD care. Additionally, there is no standardized nursing protocol for managing IAD in older ICU patients, nor have there been reports on the use of Lithospermum oil for reducing IAD incidence in this population. However, previous studies have demonstrated the effectiveness of Lithospermum oil in managing skin dermatitis. Therefore, further research is required to address these gaps. This study aims to develop and evaluate the effectiveness of a nursing prevention and care program incorporating Lithospermum oil for older ICU patients, particularly vulnerable to IAD, to contribute to advancing nursing research in this field.
Aims
To explore the effectiveness of nursing prevention and care programs by applying Lithospermum oil on levels of risk, severity, and incidence rate of IAD among older intensive care unit patients.
Conceptual Framework
This study applied the nursing process (Figure 1) as a conceptual framework to manage the skin of older ICU patients with incontinence, which has five stages: assessment, diagnosis, planning, implementation, and evaluation.16
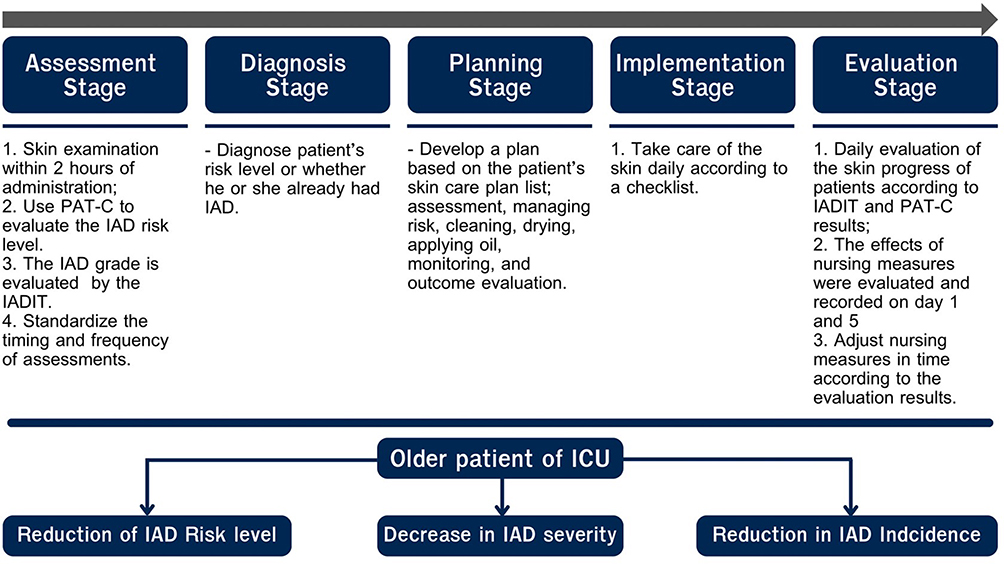 |
Figure 1 Conceptual Framework. |
Methods
Design
This study applied the randomized controlled trial design to explore the effectiveness of nursing prevention and care with applying Lithospermum oil on levels of risk, severity, and incidence rate of IAD among older intensive care unit patients.
Setting
The settings were wards A and B at the university hospital, a class III Grade a general hospital located in Guiyang, Guizhou Province. Considering that the number of beds in Ward A and Ward B was the same, at 17 beds each, there was no significant difference in the severity of the patients admitted, and there was no crossover between the nursing staff in the two wards. By randomization, Ward A was the control group, and Ward B was the experimental group. Patients who met the inclusion criteria were included in the study using systematic random sampling after obtaining consent. The cases were collected from July 2023 to October 2023 (Figure 2).
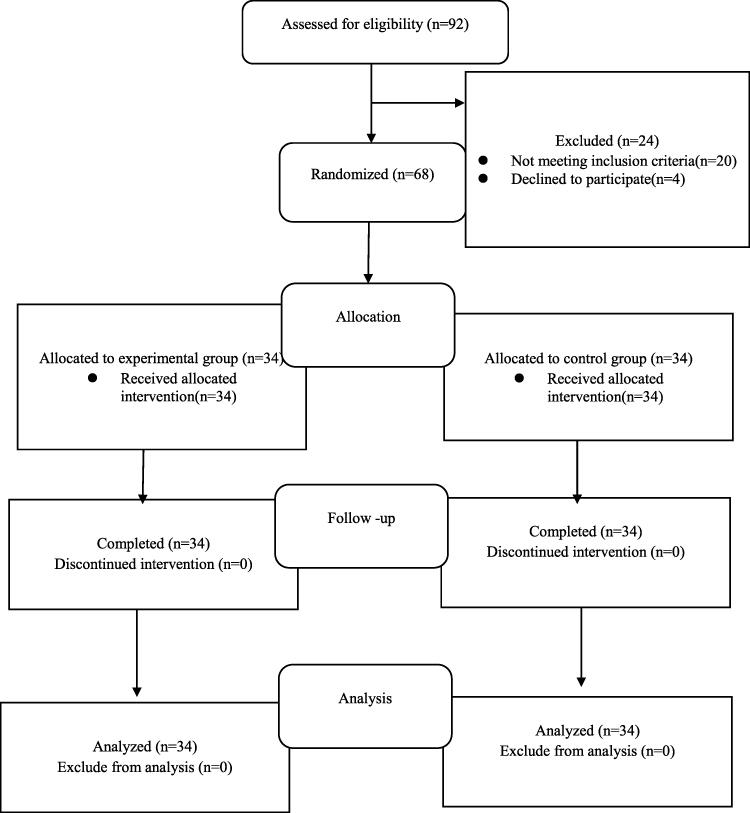 |
Figure 2 Sample sampling flow chart (CONSORT Diagram). Notes: CONSORT figure adapted from Schulz KF, Altman DG, Moher D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010;7(3): e1000251. Copyright: © 2010 Schulz et al. Creative Commons Attribution License.17 |
Sampling
The population in this study was incontinence patients aged 60 years and older. The sample in this study was admitted to the comprehensive ICU of the university hospital in Guiyang City, Guizhou Province, China, from July 2023 to October 2023. GPower 3.1 software was used to calculate the study’s sample size. The study set one tail of alpha level as α=0.05, power (1-β) =0.8, and medium of effect size=0.3. The sample size calculated is 64; however, a possible 5% dropout was added. The total number of participants in this study was 68. There were 34 patients in the experimental group and 34 in the control group. The inclusion criteria were: 1) ICU incontinence patients, fecal incontinence, urinary incontinence, or double incontinence; 2) Males and females age ≥60; 3) Willing to participate in this study by signing the consent form themselves or their family members. The Exclusion criteria were: 1) Patient has pressure injury and skin injury in the sacrococcygeal region; 2) perianal abscess; 3) severe cachexia such as edema; and 4) be discharged or transferred before finishing the program (within five days).
Intervention
The experimental group adopted the nursing process to manage the patients’ skin. The skin of ICU patients with incontinence was managed in five stages: assessment, diagnosis, planning, implementation, and evaluation. Specific management methods are as follows (Figure 3):
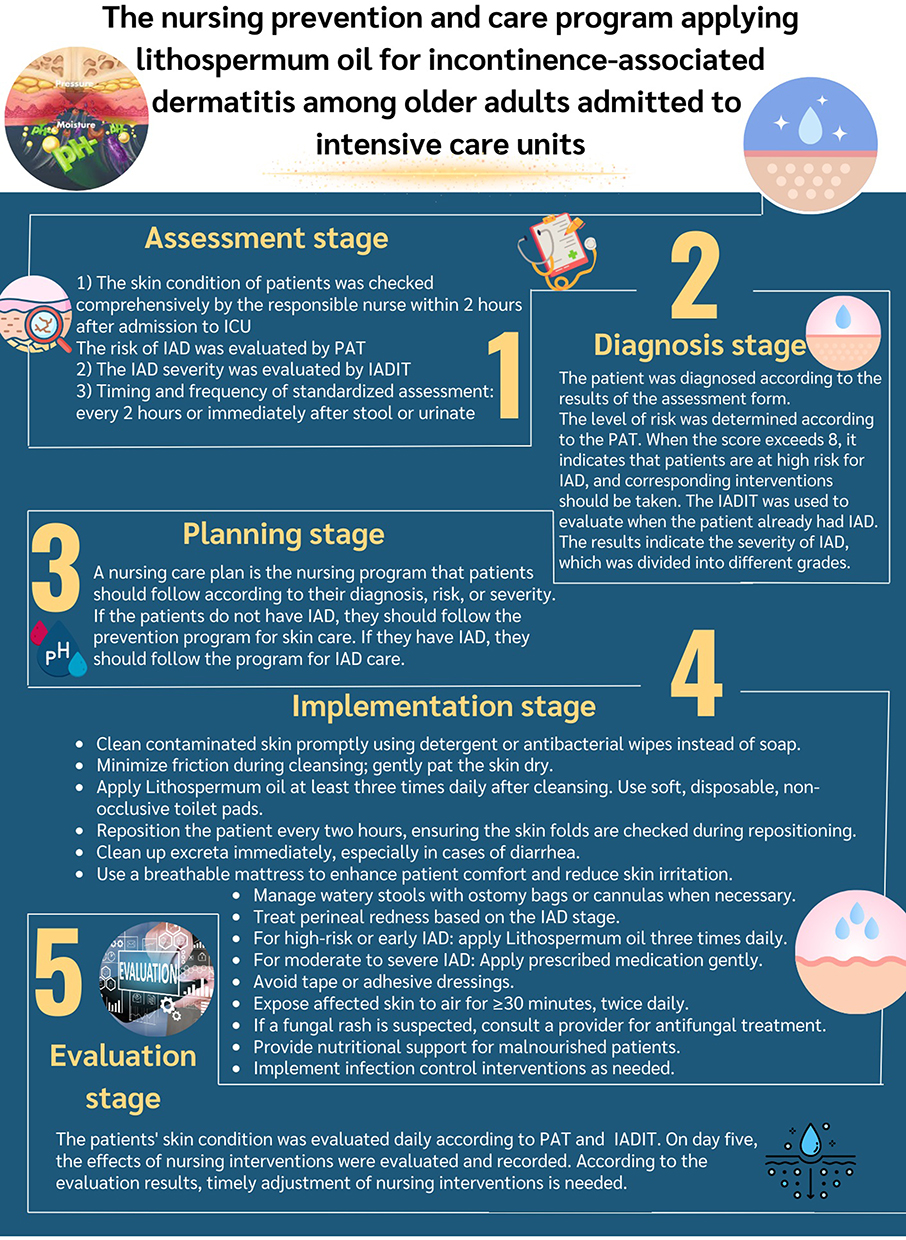 |
Figure 3 Nursing Interventions. |
Assessment Stage
The main content was to eliminate the hidden danger of skin injury and reduce the possibility and harmfulness of the risk. The main measures were as follows: 1) The skin condition of patients was checked comprehensively by the responsible nurse within two hours after admission to the ICU; 2) The perineal assessment tool (PAT-C) was used to assess the risk of IAD from four aspects: type and intensity of stimulation (formed stool, liquid stool, urine); The duration of skin exposure to the irritation; perineal skin condition; factors associated with increased risk of diarrhea; 3) IADIT evaluated IAD grade; and 4) Timing and frequency of standardized assessment: IADIT and PAT-C were used for initial assessment within two hours after admission, high-risk patients were evaluated after each stool, and other patients were evaluated in each shift, and the risk factors were reassessed in time.
Diagnosis Stage
The patient was diagnosed according to the assessment form results. The level of risk factors of patients was determined according to the PAT-C assessment results. When the score exceeds eight, it indicates that patients have high-risk factors for IAD, and corresponding interventions should be taken. The IADIT was used to evaluate when the patient already had IAD. The evaluation form required a second person to review the score to ensure the accuracy of the diagnosis.
Planning Stage
Plan the nursing program that patients should follow according to the diagnosis results. If the patients do not have IAD, follow the prevention program for skin care. If the patients have IAD, management should be implemented.
Implementation Stage
The steps are as follows: Clean contaminated skin promptly, use detergent or antibacterial wipes instead of soap, minimize friction on the skin surface when cleaning, and gently pat the skin dry. Apply Lithospermum Oil at least three times a day after cleansing. Toilet pads should be non-closed, disposable, and soft cotton pads. The patients were turned over every two hours. When turning over, pay attention to opening the crease of the skin to check the skin. When there is excrement, it must be cleaned in time or no later than 15 minutes. A breathable mattress provides a safe and comfortable medical environment for patients. Formed and soft stools require prompt cleaning, and watery stools require stool management for the patient, such as collecting stools as an ostomy bag or cannula. When the skin of the perineum is red, it must be treated according to the stage. After cleaning the skin of high-risk and early IAD, apply Lithospermum oil three times a day. For moderate IAD and severe IAD, apply the medicine as the doctor recommends and place it gently on the injured skin to avoid rubbing, and do not use tape or other adhesive dressings. Damaged skin was exposed to air for 30 minutes or more at least twice daily. For fungal-appearing rash, need to ask the primary care provider to order an anti-fungal powder or ointment. Patients with malnutrition need to choose the appropriate way to increase nutrition according to the patient’s situation, and patients with infection need to control infection.
Evaluation Stage
The patients’ skin condition was evaluated daily according to IADIT and PAT-C results, and the effect of nursing measures was evaluated and recorded on the fifth day. Based on the evaluation results, the researcher made timely adjustments to nursing interventions.
Data Collection Instruments
The following forms were used to collect patient information as required by the study. The Chinese version of these forms, which have been used in hospitals for many years, was used in the study.
1) Patient general data collection form: The form includes the patient’s number, gender, age, chief complaint, diagnoses, health problems, medication uses, and incontinence status. The patient’s transfer time out of the ICU unit should be recorded. Basic information collected from patients can be used to compare basic information and guide adjustment analysis in cases where the basic information between groups differs.
2) Patient clinical data collection form: The form includes infection indicators (white blood cell count, neutrophil count, and daily maximum body temperature), blood gas analysis indicators, nutritional risk, IAD information (risk score and severity level), and transfer time of the patient out of the ICU unit should be recorded. Patient clinical data can be used to compare and guide for adjusted analysis in cases where the information between groups is different.
3) Perirectal Skin Assessment Tool (PAT): PAT was used to assess the risk level of IAD and was assessed at least once a day during the study. PAT consists of four parts: stimulus type, stimulation time, perineal skin condition, and influencing factors. The score of each subscale was rated as 1–3 from low to high, with the total lowest score of 4 and the highest score of 12. The higher the score, the higher the risk of IAD. Moreover, the total score was summarized and divided into low and high-risk groups, using eight at a cutting point, 4–7 indicating low risk, and 8–12 indicating high risk. The levels of risk used for both between and within group comparison.18
4) IAD Assessment Intervention Tool (IADIT): IADIT was used to assess the severity of IAD. It was assessed at least twice a day during the study and again when the patient’s skin condition changed. The IADIT evaluated IAD in terms of skin color, rash, and skin damage and classified the severity of IAD into five grades: high risk, early IAD, moderate IAD, severe IAD, and Fungal-appearing rash.
Data Collection Procedure
1) The study plans were submitted to the research ethics committee. After receiving consent from Khon Kaen University IRB, the researcher informed the participants about this research project; this study was started when the researcher received consent from the participants or their representatives. Before the study, the researchers trained the registered nurses on IAD knowledge and skills of IAD prevention and care to ensure consistency in all operations. The training content for nursing staff included assessment and recording of skin integrity, skin cleansing, skin protection measures, nutritional implementation for patients, and outcome evaluation aimed at improving the knowledge, skills, abilities, and attitudes necessary for nursing staff in IAD care. According to the skin care operation list and the observed data, interventions in the study were recorded in the general data questionnaire, and clinical data collection was in the table Finally, the obtained data were analyzed.
2) This study started with program development and pilot study. Firstly, the researchers conducted a literature search and analysis, established a research plan, started a pre-experiment on five cases, and improved and modified the existing and possible problems according to the pre-experiment results.19
3) For this RCT study, when a new patient was transferred to Ward A and B, the researchers assessed the newly transferred older incontinence patients aged ≥60 to determine whether they met the inclusion criteria.
4) Patients who met the inclusion criteria were systematically randomized into this study. A sign was hung at the patient’s bedside, and the general data collection form and clinical information collection form were filled out. All investigators were informed of the patient grouping and the subsequent intervention.
5) Ward A was the control group, and Ward B was the experimental group. Patients in Ward A were nursed according to routine skin care methods as follows: after patients had stool and urine, nurses wiped the stool with tissue or wipes, replaced nursing pads and contaminated bed sheets and quilt covers, and kept the bed sheets clean and tidy. The nurses took a bath once a day for the patients, avoided using soap when cleaning the skin, and refrained from wiping. After cleaning the stool, check the skin condition around the anus. If the skin is damaged, notify the doctor to take treatment measures. In contrast, patients in Ward B were nursed by nurses trained with IAD-related knowledge for nursing prevention and implementing a nursing prevention and care program by applying Lithospermum oil.
6) Patient assessment: All patients enrolled in the study had IAD assessments performed at 8:00 a.m. and 8:00 p.m. every day during the routine nursing shift, and the assessment results were recorded on the nursing record sheet. The results of the patient’s assessment were recorded every day, and results were compared on days 1 and 5 of the patient’s transfer. When the patient has IAD, the patient’s skin condition should be recorded with photos and words on the nursing record sheet to be ready for data management and analysis.
Ethical Considerations
We conducted this study in accordance with the ethical principles outlined in the Declaration of Helsinki, which governs research involving human participants and ensures respect for their rights, safety, and well-being. The Center for Ethics in Human Research, Khon Kaen University committee approved this study before starting data collection. The approval date was 12 July 2023, and the approval number was HE662113. While gathering data, the researchers informed older persons and/or their family members, in case the older have no conscious or could not decide by themselves, about the study’s topic, goals, methods, schedule, and possible advantages. Participants could leave the study anytime without repercussions and were fully informed of their freedom to consent or voluntarily deny participation. All information was kept private, and participants signed the informed consent form when they gave their informed agreement. In the case of older people who have no conscious or cannot decide by themselves, their family members sign instead of them. Then, the researcher collected data, and the results were analyzed. Finally, results were presented anonymously.
Data Analysis
The researchers used the Statistical Package for the Social Sciences (SPSS) version 28.0.1.0 under the university license to analyze the data and confirm its completeness and accuracy. Descriptive statistics such as percentage and frequency were used to analyze basic population information statistics. The Wilcoxon Sign Rank Test was used to compare the risk of IAD evaluation results and IADIT scores of the experimental and control groups on the first and fifth days since non-normal distributions were found. The Mann–Whitney U-Test was used to analyze the PAT and IADIT evaluation results of the experimental and the control groups on the fifth day because of the non-normal distribution of the score. The chi-square test was used to compare the IAD incidence between the two groups. Finally, the adjusted analysis, which used statistics to explore the actual effect of the intervention when some demographics or baseline outcomes were different between the experimental and control groups, was conducted. For this study, binary logistic regression was used to explore the actual effectiveness of the intervention, as we found that the participants’ basic and clinical information, types of incontinence, stool characteristics, and white blood cell counts differed between the two groups.
Validity, Reliability, and Rigors
This study has proven highly beneficial in preventing and improving IAD. The application of Lithospermum oil as a skin protectant was systematically evaluated, demonstrating its effectiveness in reducing both the incidence and severity of IAD in clinical settings. The study group comprised 13 nurses with over 10 years of experience working in the Intensive Care Unit (ICU). At least two trained personnel were on duty during each shift to ensure effective intervention. The research team was responsible for investigating, monitoring, and providing guidance on skin issues in incontinent patients daily while identifying skin quality management challenges. The team leader and data collectors oversaw the implementation and ensured the accuracy of collected information. Before the study commenced, all nursing staff underwent comprehensive training, including theoretical and practical components. Additionally, a pilot study was conducted with five cases to assess the feasibility and acceptability of the program. Based on recommendations from the pilot phase, necessary revisions were made before proceeding with the actual study. A checklist was used to standardize nursing procedures in patient care, ensuring consistency and minimizing errors. A second individual reviewed all collected data for accuracy. Data collectors were not involved in patient care to prevent bias, and all information was digitized during analysis for efficient statistical evaluation. To maintain the integrity of the study, nurses assigned to the control and experimental groups remained fixed in their respective wards. Additionally, patient bed transfers between ICU wards were strictly prohibited to prevent data variability. This study followed a well-structured research methodology and can serve as a valuable reference for improving the management and care of patients risking or suffering from IAD.
Results
The Participant’s Demographic Characteristics
The total sample consisted of 68 patients, predominantly male (70.60%), with a mean age of 73.16 years (SD = 7.38). The mean length of hospital stay was 10.00 days (SD =7.52). The main reasons for admission to the intensive care unit were respiratory failure and pneumonia (54.40%). There were no significant differences in age, sex, length of hospital stay, and diagnosis among the participants between experimental and control groups (Table 1).
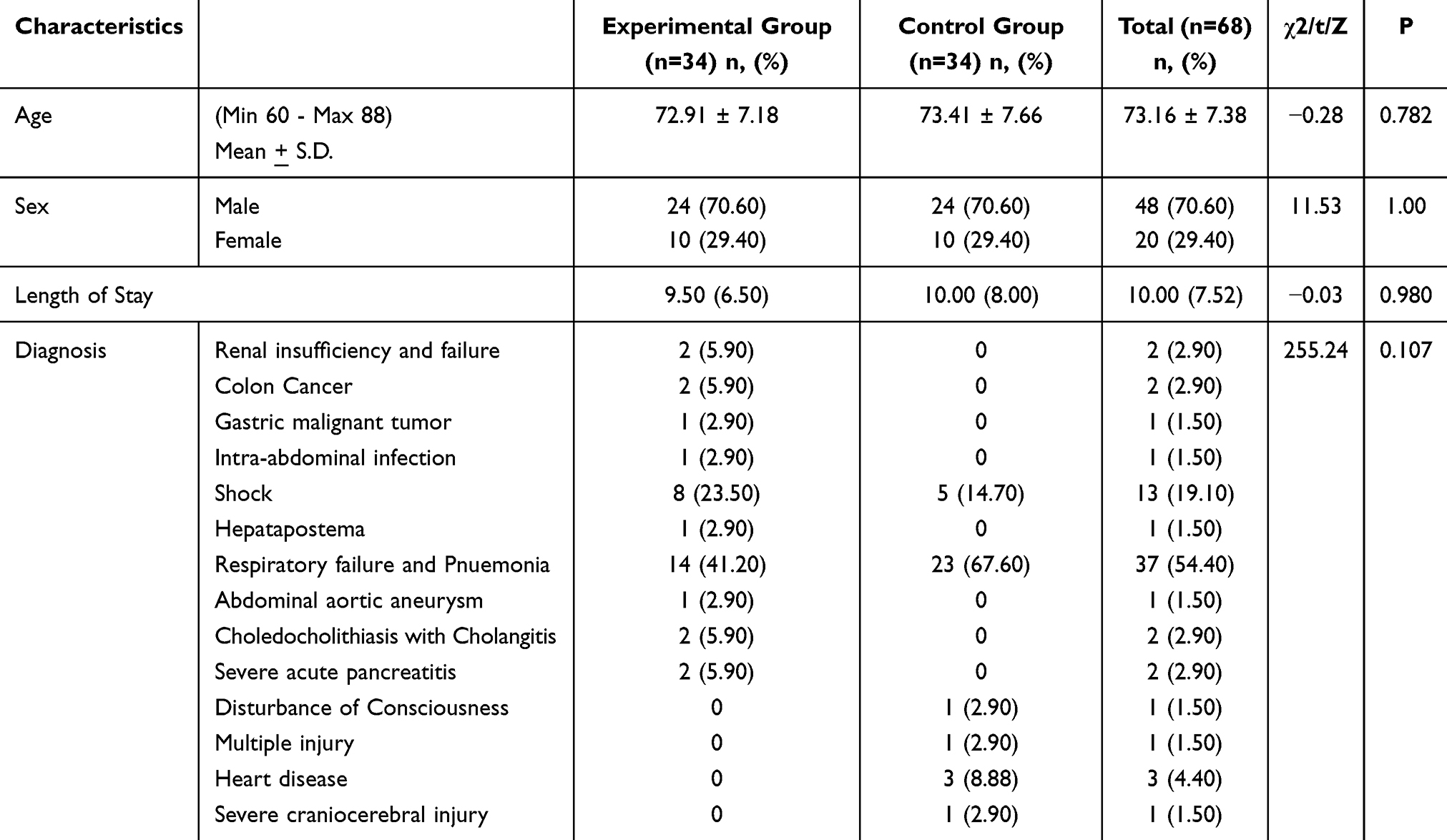 |
Table 1 The Participant’s Demographic Characteristics |
The Clinical Data of Participants
Data on the severity of illness among the participants between the two groups revealed that their PaO2 was about 75.00 (SD=37.61), NRS2002 was about 1.00 (SD=1.2), BMI was 22.50 (SD=3.82), and the APACHE II was about 24.00 (SD = 5.82) which no difference was found between the two groups. However, a difference was found for the white blood cell (p-value < 0.05) between the intervention and control groups (Table 2).
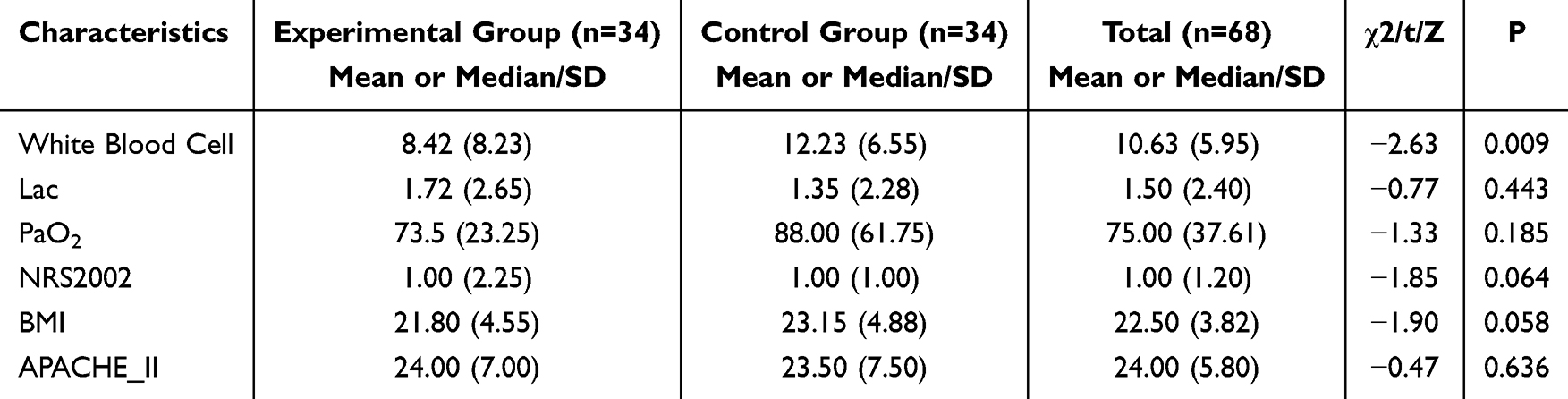 |
Table 2 The Clinical Data of Participants |
The Incontinence Data of Participants
The bowel frequency was once a day. Most participants had urinary incontinence 60.30%, fecal incontinence accounted for 4.40%, and participants with double incontinence accounted for 35.30%. The stool characteristics were formed at 60.30, followed by loos at 38.20 and water at 1.50. There were differences between types of incontinence and stool characters between the experimental and the control group (P<0.05) (Table 3).
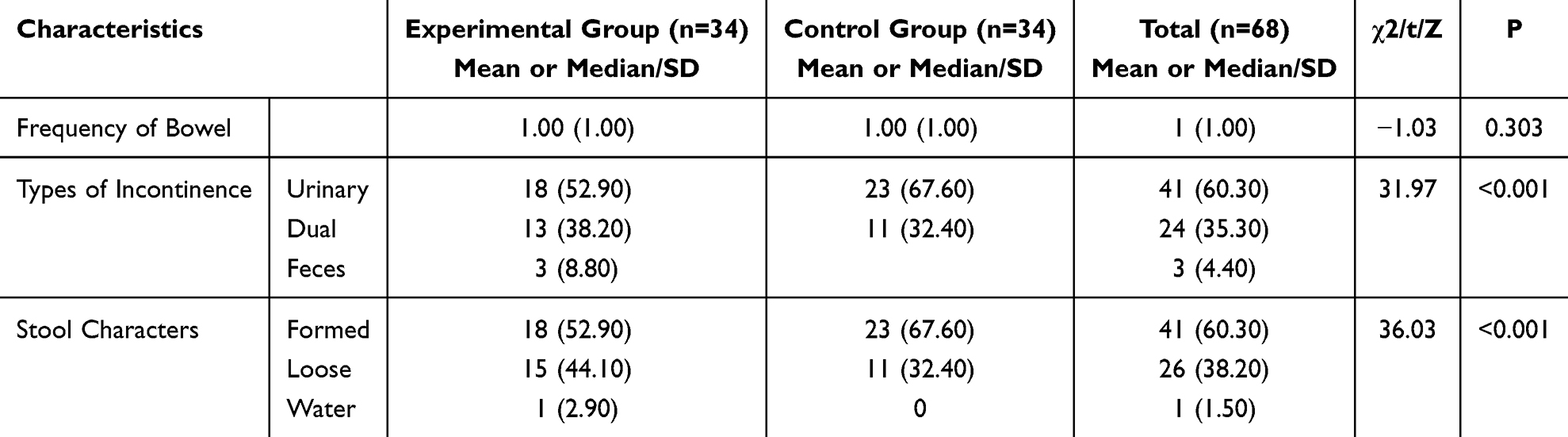 |
Table 3 The Incontinence Data of Participants |
The Risk and Severity of IAD (within Group Comparison)
The Wilcoxon Sign Rank Test was used to compare the risk of IAD evaluation results of the experimental group on the first day and the fifth day. The result showed that the PAT score increased from before 7.65 (SD = 0.73) to after 7.79 (SD = 0.95). However, the different PAT scores were nonstatistically significant (p = 0.059). The patient did not suffer from IAD before the intervention. However, after implementing intervention for five days, we found four cases experiencing IAD, of which three were early IAD and one was moderate IAD. The severity score assessed by IADIT before was 1.0 (SD =1.0), and after was 1.0 (SD = 1.15), which was nonstatistically significant (p = 0.059) (Table 4).
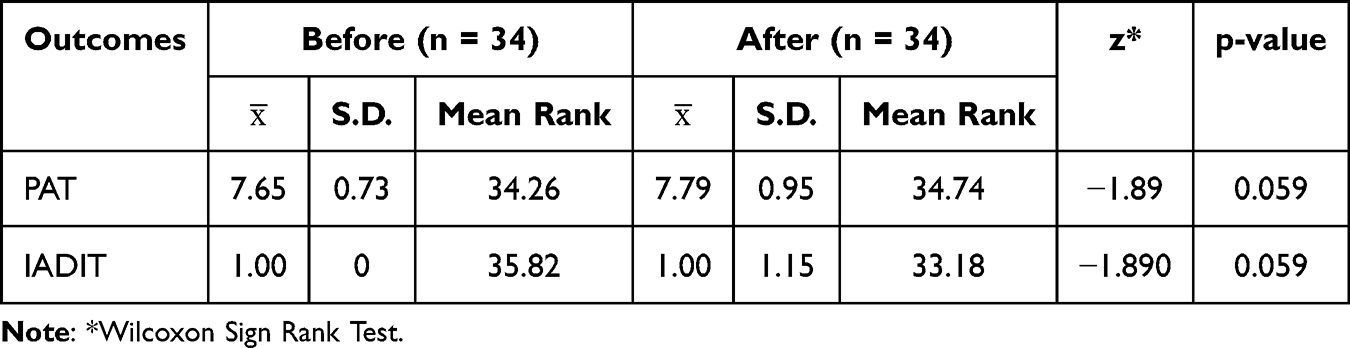 |
Table 4 PAT (Risk) and IADIT (Severity) Scores in the Experimental Group Before and After Attending the Program |
The Risk and Severity of IAD Five Days After Attending the Program (Between Groups Comparison)
After applying the standardized prevention and care program with Lithospermum oil for five days, the PAT score in the experimental group was 7.79 (SD = 0.95), and in the control group was 7.82 (SD = 1.07); however, there was no significant difference in the results (p = 0.92). The data analysis found that the IADIT score in the experimental group was 1.15 (SD = 0.44), while the IADIT score in the control group was 1.56 (SD = 1.28); there was also no significant difference in the severity of IAD between the two groups (p = 0.37) (Table 5).
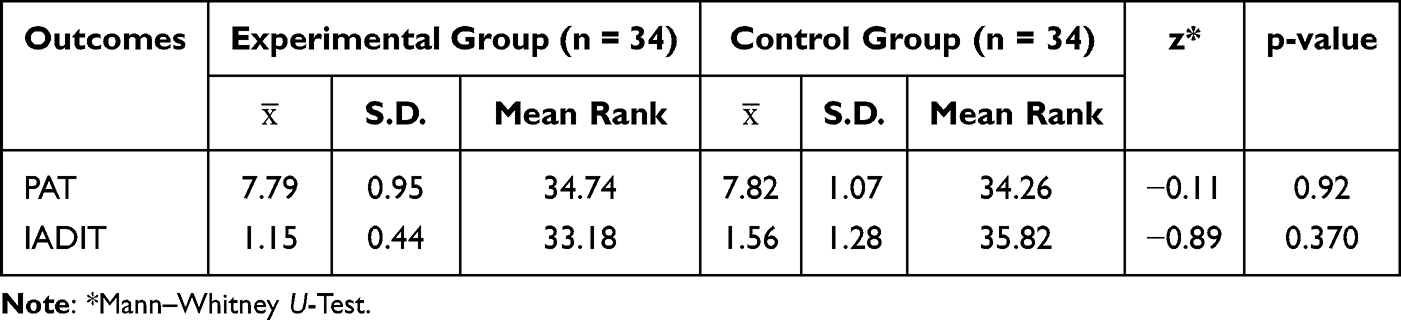 |
Table 5 PAT (Risk) and IADIT (Severity) Scores Between Experimental and Control Groups on Five days After Attending Intervention |
The Incidence of IAD Between the Experimental and the Control Groups
The incidence rate of IAD was four cases (11.80%) in the experimental group and nine cases (26.47%) in the control group. These incidences were statistically different (p < 0.01). The intervention in the experimental group could effectively reduce the incidence of IAD (Table 6). To confirm this conclusion, we applied adjusted analysis because this study found some general information differences between the participants in experimental and control groups regarding types of incontinence, stool characteristics, and white blood count. Finally, the adjusted analysis was used to explore the actual effect of the intervention. A binary logistic regression analysis, controlling for three variables (types of incontinence, stool characteristics, and white blood cell counts), was conducted. Finally, we still found the difference in the incidence rate between the experimental and control groups (p = 0.04), demonstrating that this intervention can actually reduce the incidence rate of IAD (Table 7).
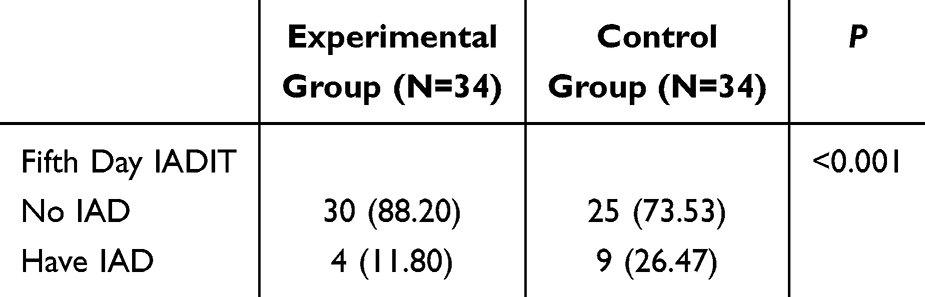 |
Table 6 Number of IAD Cases Comparison After Five days Attending Interventions Between Experimental and Control Groups |
 |
Table 7 Comparison Number of IAD Cases After Receiving the Program by the Adjusted Binary Logistic Regression Analysis |
Discussion
This study found that most patients were male, accounting for 70.6%. This finding is consistent with the study by Sommana et al,2 which examined the IAD prevention program in older patients in the intensive care unit. The results showed that most of the patients were male, as male patients tend to engage in health-risk behaviors such as alcohol consumption, smoking, and lack of exercise. When they become ill, they tend to be more severely affected than females.20 The age of the participants in the study ranged from 60 to 88 years old; the average age of the experimental group was 72.9, and the average age of the control group was 73.4. In previous studies, the age of the subjects mainly was adult (> 18 years old) patients.4,12,21,22 It was found that the incidence of IAD increased with age,23 indicating that the incidence of IAD was higher in older patients, which was consistent with the subjects and objectives of this study. The participating ICU unit was a comprehensive ICU unit in which the majority of patients were diagnosed with severe pneumonia, and the disease had no specific effect on incontinence. In terms of length of hospital stay, because the duration of the etiology varied, only the first five days of data were extracted in this study, as IAD typically occurs 3–4 days after admission. The extended length did not affect study data collection, especially since the mean length of stay of this study was 10 days, which covered the duration of this study.
Among the 68 patients who participated in the study, the most stool character was loose stool, consistent with the previous study that loose and watery stools were more likely to form IAD than formed stools.11 A study reported that fecal irritation is the pathological factor of IAD, and stool frequency and characteristics are the main risk factors of IAD.10 Clinical experience also shows that loose and watery stools are more destructive to the skin than formed stool.1 However, watery stool is more likely to arouse the vigilance of clinical nursing staff to use more effective stool collection methods, such as anal bags. This situation can explain why patients with stool frequency and loose and watery stool in this study did not develop IAD. The APACHE II score is currently the most widely used and authoritative critical illness evaluation system in ICU Wards, which can be used to predict patients’ prognosis and mortality risk. A study by Bliss et al24 found through regression analysis that the APACHE II score is one of the risk factors for IAD in critically ill patients. The APACHE II score in this study ranged from 15 to 41 (SD =24). Based on the above data, we can see that there are many risk factors for IAD in patients with fecal incontinence in this study. Effective IAD prevention and care interventions are critical when these factors cannot or are difficult to change.
PAT was used to assess the patient risk level on the first and fifth day of hospitalization. According to the PAT, assessment results on the fifth day showed no significant difference between the two groups, representing that the intervention and routine care are effective in preventing the risk of IAD for older ICU patients. This finding is consistent with the study by Sommana et al,2 which examined the effects of a program to prevent incontinence-associated dermatitis in older patients. A pilot study conducted over five days found that the PAT-T score assessment results before and after the trial were not significantly different between the experimental and control groups. The intervention of a nursing prevention and care program by applying Lithospermum oil can improve skin irritation and time of excreta and reduce the risk of IAD.6,7 Skin irritation from excreta is reduced by visiting and cleaning excreta during nursing procedures, exposing the skin to air for more than 30 minutes per day, and using Lithospermum oil to separate excreta from skin contact.1,19 Contributing factors need to improve the general condition of patients in order to reduce the risk, which requires medical interventions. Based on a comparison of the risk of IAD evaluation results before and after the program in the experimental group showed no statistical significance; this means nursing can reduce or maintain the influencing factors and improve the physical state of patients by strengthening communication with doctors and jointly formulating the patient’s digestive tract management and nutrition plan. These factors lead to the limitation of nurses to control the risk factors of IAD. Nurses can protect patients’ skin through the intervention of nursing procedures, and at the same time, they should work with the medical staff to reduce the risk level of IAD.
According to the study results, the severity of IAD between the two groups on day five was higher in the control group than in the experimental group. Although the statistics did not show significance, the control group was higher than the experimental group when looking at the number of actual IAD cases. Nursing prevention and care protocols using Lithospermum oil can be used to prevent the occurrence of IAD and protect the skin. In the study by Park et al,25 interventions were shown to reduce the severity of IAD in patients. Fungal rashes occurred in three patients in the control group but not in the experimental group. All three patients who experienced fungal rashes had significant itching symptoms, making it difficult to sleep at night and affecting their rest. Lithospermum oil can form a protective layer on the skin surface of the patient and separate the skin from the pad, preventing the pad from sticking tightly to the skin and causing the skin to become infected with a fungal rash.26,27
This study showed that the incidence of IAD was 11.8% in the experimental group and 26.5% in the control group. The number of IAD cases in the experimental group was significantly lower than in the control group, and the difference was statistically significant. Findings from the study were consistent with previous studies that the incidence of IAD in the experimental group was 8.1%, and the control group was 27.1%, with a statistically significant difference.3 Montague et al28 also used standardized nursing tools in their study to help nurses clarify their thinking and care for patients; the incident rate of IAD decreased after that. This study proved that although routine care can be used to maintain a level of risk, it is not enough to provide better outcomes like preventing or reducing the number of cases developed IAD after admission.
IAD emphasizes prevention as the main focus, and this study constructs a nursing prevention and care program by applying Lithospermum oil to conduct a detailed evaluation of patients based on their general situation, fecal incontinence, and IAD risk. Banharak et al1 reported that healthcare providers can use strategies for prevention and care for IAD among older adults, including assessment, causative factors management, cleansing, applying medical products, body positioning, nutrition promotion, health education and training, and outcome evaluation to prevent and care for IAD. Moreover, Lithospermum oil is often used for skin prevention and care in China, especially among infants with red buttocks.27,29 Then, both nursing strategies and applying Lithospermum oil can be used for skin care improvement, especially in decreasing the incidence rate of IAD among older ICU patients. The focus is on strengthening the implementation of standardized nursing and prevention interventions for patients and the standardized use of the skin protector Lithospermum oil. Researchers should start with patients and intervene to clean, moisturize, and protect the skin; conduct personnel training; observe and record skin conditions in each shift; strengthen medical and nursing cooperation; manage bowel movements reasonably; and avoid soaking the skin with excreta. Thus, the purpose of observing and protecting the patient’s skin is achieved, which can effectively reduce the occurrence of IAD. ICU patients have a critical condition with multiple diagnostics and treatment measures, and there are also many risk factors for IAD. This study strengthened the structured intervention training for the experimental group nurses, described the risks and severity of IAD, developed a skincare checklist, and promptly took different interventions based on the specific situation of the patient’s skin to achieve the best outcomes.
Limitations
The risk scores from PAT and the severity levels from IADIT measurement were narrow, such as 1–5, and this ICU still provides standard care and quick action when skin problems are found. Then, only the incidence rate of IAD between the control and experimental groups was statistically different; however, risk scores and severity levels could not prove a significant difference in this study. Other risk factors for IAD have not been included in this study, such as the allocation of human resources, hypoproteinemia, and antibiotics used. Then these variables should be explored for future study. Seasonal factors were not considered in the study. During hot summer weather, patients sweat more, and their skin is damp, which increases the likelihood of developing dermatitis. Finally, the research on this topic is limited to the comprehensive ICU of this university hospital. It does not cover other specialized ICUs such as medical, surgical, cardiac, trauma, and burns intensive care units. There may be differences in the effectiveness of synchronous use in specialized ICU wards.
Conclusion and Recommendation
As a result, after applying the standardized prevention and care program with Lithospermum in the experimental group, the risk level of IAD was not different compared to that before the application. After implementing the intervention, this risk level was also not different between the experimental and control groups. The same finding was also found in the severity level evaluated by IADIT. Finally, the number of incidences of IAD in the experimental group was lower than in the control group. These proved that the intervention measures in this study effectively reduced the incidence rate of IAD.
A standardized nursing prevention and care program can help regulate nursing behavior, guide clinical work, and improve care for incontinence patients. Incorporating these procedures into daily practice can reduce skin problems. Lithospermum oil, an easily accessible over-the-counter skin protector, has been proven effective in preventing IAD. It is recommended for early use in high-risk patients based on PAT scores. Since the data collection period for this study was relatively short, future research should extend the timeframe to assess the long-term effectiveness of the prevention and care program. Researchers should also expand the sample size and conduct studies in other types of ICU to enhance generalizability and improve skin care outcomes for older ICU patients. Further studies should explore effective incontinence management strategies to help control IAD. Additionally, future research should measure and evaluate other factors, such as skin quality, acid-base balance, and moisture levels, to obtain more reliable data.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to prohibited laws (and/or rules, regulations, and contracts). However, they are available from the corresponding author upon reasonable request.
Acknowledgments
We extend our sincere gratitude to all individuals who contributed to this study. In particular, we express our deep appreciation to the hospitalized older patients at high risk of or experiencing incontinence-associated dermatitis, as well as their caregivers, for their participation. Additionally, we acknowledge the invaluable support of the hospital staff who contributed to the study. This study was registered with the Thai Clinical Trials Registry (TCTR20230808004).
Funding
This research was supported by The Development of Health Promotion for Prevention of Non Communicable Disease for Working All Aged People, funded by the Fundamental Fund of Khon Kaen University from the National Science, Research and Innovation Fund or NSRF (Grant Number NSRF68-001), Thailand. We sincerely appreciate this funding support, which made the research possible.
Disclosure
There is no conflict of interest in conducting this study.
References
1. Banharak S, Panpanit L, Subindee S, et al. Prevention and care for incontinence-associated dermatitis among older adults: a systematic review. J Multidisciplinary Healthcare. 2021;14:2983–3004. doi:10.2147/JMDH.S329672
2. Sommana C, Banharak S, Sim-Im S, Ransinyo K. Effects of nursing program in preventing incontinence-associated dermatitis by applying zinc oxide and petroleum jelly skin protection products among older patients in semi-intensive medical care units: a pilot study. J Multidisciplinary Healthcare. 2024;17:3619–3636. doi:10.2147/JMDH.S469276
3. Beeckman D. A decade of research on incontinence-associated dermatitis (IAD): evidence, knowledge gaps and next steps. J Tissue Viability. 2017;26(1):47–56. doi:10.1016/j.jtv.2016.02.004
4. Chianca TC, Gonçales PC, Salgado PO, Machado BO, Amorim GL, Alcoforado CL. Incontinence-associated dermatitis: a cohort study in critically ill patients. Dermatite associada à incontinência: estudo de coorte em pacientes críticos. Rev Gaucha Enferm. 2017;37(spe):e68075. doi:10.1590/1983-1447.2016.esp.68075
5. Beele H, Smet S, Van Damme N, Beeckman D. Incontinence-associated dermatitis: pathogenesis, contributing factors, prevention and management options. Drugs Aging. 2018;35(1):1–10. doi:10.1007/s40266-017-0507-1
6. Zhang LY, Li YW, Chi Q, Wang L, Xiao F. Experimental study on the antibacterial effect of compound Arnebia root Oil in vitro. World Trad Chinese Med. 2019;14(5):1133–1138.
7. Shen J, Zhu YP, Yang ZB, Ma Q. Effects of arnebia root oil on the expression of metalloproteinase-9 and vascular endothelial growth factor in rat wound tissue. J Ningxia Med University. 2018;40(9):1010–1013.
8. Adamy EK, Zocche DAA, Almeida MA. Contribution of the nursing process for the construction of the identity of nursing professionals. Rev Gaucha Enferm. 2019;41(spe):e20190143. doi:10.1590/1983-1447.2020.20190143
9. Micheal JCJ, Chander M, D’Cruz J, Braganza V, Mascarenhas V, Cruz P. Effect of nursing interventions in prevention and healing of incontinence-associated dermatitis among critical care patients. Nursing J India. 2020;111(1):17–20.
10. Beeckman D, Campbell J, Campbell K, et al. Incontinence-Associated Dermatitis: Moving Prevention Forward. London: Wounds International; 2015.
11. Gray M, Giuliano KK. Incontinence-associated dermatitis, characteristics and relationship to pressure injury: a multisite epidemiologic analysis. J Wound Ostomy Continence Nursing. 2018;45(1):63–67. doi:10.1097/WON.0000000000000390
12. Campbell JL, Coyer FM, Osborne SR. Incontinence-associated dermatitis: a cross-sectional prevalence study in the Australian acute care hospital setting. Int Wound J. 2016;13(3):403–411. doi:10.1111/iwj.12322
13. Beeckman D, Van Lancker A, Van Hecke A, Verhaeghe S. A systematic review and meta-analysis of incontinence-associated dermatitis, incontinence, and moisture as risk factors for pressure ulcer development. Res Nursing Health. 2014;37(3):204–218. doi:10.1002/nur.21593
14. Zheng YQ, Zhang HJ, Zhou YY. ICU patients with incontinent dermatitis correlation status investigation and risk factor analysis. J Nursing Manag China. 2018;17(4):488–492. doi:10.1016/j.jechem.2024.10.046
15. Doughty D, Junkin J, Kurz P, et al. Incontinence-associated dermatitis: consensus statements, evidence-based guidelines for prevention and treatment, and current challenges. J Wound Ostomy Continence Nursing. 2012;39(3):303–317. doi:10.1097/WON.0b013e3182549118
16. De la Cuesta C. The nursing process: from development to implementation. J Adv Nurs. 1983;8(5):365–371. doi:10.1111/j.1365-2648.1983.tb00459.x
17. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. PLoS Med. 2010;7(3):e1000251. doi:10.1371/journal.pmed.1000251
18. Nix DH. Validity and reliability of the perineal assessment tool. Ostomy/Wound Manag. 2002;48(2):43–49.
19. Qiao G, Banharak S. Incontinence-associated dermatitis in older intensive care patients: a review and case report. J Multidisciplinary Healthcare. 2023;16:3299–3308. doi:10.2147/JMDH.S434275
20. Coyer F, Campbell J, Doubrovsky A. Efficacy of incontinence-associated dermatitis intervention for patients in intensive care: an open-label pilot randomized controlled trial. Adv Skin Wound Care. 2020;33(7):375–382. doi:10.1097/01.ASW.0000666904.35944.a3
21. Al Kiyumi MH, Al Belushi ZI, Jaju S, Al Mahrezi AM. Urinary incontinence among Omani women: prevalence, risk factors and impact on quality of life. Sultan Qaboos University Med J. 2020;20(1):e45–e53. doi:10.18295/squmj.2020.20.01.007
22. Coyer F, Miles S, Gosley S, et al. Pressure injury prevalence in intensive care versus non-intensive care patients: a state-wide comparison. Australian Crit Care. 2017;30(5):244–250. doi:10.1016/j.aucc.2016.12.003
23. Holroyd S. Incontinence-associated dermatitis: identification, prevention and care. British J Nursing. 2015;24(9):S37–S43. doi:10.12968/bjon.2015.24.Sup9.S37
24. Bliss DZ, Savik K, Harms S, Fan Q, Wyman JF. Prevalence and correlates of perineal dermatitis in nursing home residents. Nursing Res. 2006;55(4):243–251. doi:10.1097/00006199-200607000-00004
25. Park KH, Kim KS. Effect of a structured skin care regimen on patients with fecal incontinence: a comparison cohort study. J Wound Ostomy Continence Nursing. 2014;41(2):161–167. doi:10.1097/WON.0000000000000005
26. Guo SH, Hao XY, Zhuang TF. Effect of epidermal growth factor combined with arnebia root oil on the treatment and nursing of neonates with severe red buttock. Chinese J Eugenics Genetics. 2021;29(1):131–134.
27. Zeng YM, Xiao SG, Xie YM. Homemade radix arnebiae seu lithospermi tea oil application in neonatal red buttock. J Med Equipment. 2020;21:121–122.
28. Montague M, Karafa M, Albert NM. Assessment and documentation of incontinence-associated dermatitis after implementation of a standardised instrument: a comparative study. J Wound Care. 2019;28(Sup9):S4–S11. doi:10.12968/jowc.2019.28.Sup9.S4
29. Li S, Ellis R, Zhu Y. The associations between cognitive ability and L2 development under five different instructional conditions. Applied Psycholinguistics. 2019;40(3):693–722. doi:10.1017/S0142716418000796
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Adverse Reactions to Facemasks in Health-Care Workers: A Cross-Sectional Survey
Liu N, Ye M, Zhu Q, Chen D, Xu M, He J, Li Q, Li J
Clinical, Cosmetic and Investigational Dermatology 2022, 15:947-954
Published Date: 25 May 2022
The Effects of a Nursing Program Applying Zinc Oxide Mixed with Petroleum Jelly and Centella Asiatica Mixed with Aloe Vera on Skin Indicators Among Older Patients in Semi-Intensive Care Units: A Pilot Study
Chaisomsee S, Banharak S, Sommana C, Tuntiyasawasdikul S, Sim-im S, Ransinyo K, Limpawattana P, Deesui W, Pimpun P, Somkamsri T, Seeharach O
Journal of Multidisciplinary Healthcare 2025, 18:4561-4587
Published Date: 1 August 2025