Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Adverse Reactions to Facemasks in Health-Care Workers: A Cross-Sectional Survey
Authors Liu N, Ye M, Zhu Q, Chen D, Xu M, He J, Li Q, Li J
Received 16 March 2022
Accepted for publication 17 May 2022
Published 25 May 2022 Volume 2022:15 Pages 947—954
DOI https://doi.org/10.2147/CCID.S365390
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Ning Liu,1 Min Ye,2 Qinya Zhu,2 Dingchao Chen,3 Mingmin Xu,4 Jia He,5 Qian Li,4 Jie Li6
1Outpatient Department, Zhejiang Rongjun Hospital, Jiaxing, Zhejiang Province, 314000, People’s Republic of China; 2Nursing Department, Zhejiang Rongjun Hospital, Jiaxing, Zhejiang Province, 314000, People’s Republic of China; 3Medical Department, Zhejiang Rongjun Hospital, Jiaxing, Zhejiang Province, 314000, People’s Republic of China; 4Ultrasonic Department, Zhejiang Rongjun Hospital, Jiaxing, Zhejiang Province, 314000, People’s Republic of China; 5Department of Urology, Zhejiang Rongjun Hospital, Jiaxing, Zhejiang Province, 314000, People’s Republic of China; 6The Health Administration Center, Zhejiang Rongjun Hospital, Jiaxing, Zhejiang Province, 314000, People’s Republic of China
Correspondence: Jie Li, The Health Administration Center, Zhejiang Rongjun Hospital, Jiaxing, Zhejiang Province, 314000, People’s Republic of China, Email [email protected]
Background: Coronavirus disease 2019 (COVID-19) has developed into a worldwide pandemic, which presents several challenges for frontline health-care workers (HCWs). HCWs are highly prone to various skin diseases due to prolonged use of personal protective equipment (PPE). The most frequently used type of PPE is facemasks. To effectively control adverse skin reactions, there is an urgent need for a range of preventive practices.
Methods: This cross-sectional study was conducted at 12 hospitals in Zhejiang province, China. HCWs were invited to participate in the web survey. Data were extracted by two independent reviewers using a predesigned data collection form and analyzed with SPSS 20.0.
Results: A total of 1147 questionnaires were collected, and of these, 1090 (95.03%) were valid and returned. The incidence of chest tightness and shortness of breath and face eczema was significantly higher in HCWs wearing N95 facemasks (41.91%; 31.62%) than in the HCWs wearing medical facemasks (38.05%, P = 0.010; 21.91%, P = 0.012). The incidence of ear pain and indentation was significantly higher in HCWs wearing hang-facemasks (83.81%) than in HCWs wearing strains-facemasks (61.19%, P < 0.001). The incidence of ear pain and indentation was significantly higher in HCWs wearing undiscriminating size code facemasks (79.88%) than in the HCWs wearing discriminating size code facemasks (67.86%, P = 0.031). There was a significant reduction (P < 0.001) in the incidence of HCWs without adverse reactions (ADRs) with increasing time wearing facemasks.
Conclusion: Incidence of ADRs does not significantly increase with the durations of mask wear where wearing mask time exceeded 4 hours per day. The medical staff generally wore masks for more than 4 hours per day; therefore, we recommend taking 15 min of rest after 2 hours of mask-wearing. Results in this study support the conclusion that the type of strain-facemasks and discriminating size code facemasks has a lower incidence of ADRs than other type of medical facemasks.
Keywords: facemask, health care, COVID-19, coronavirus, dermatitis, skin care, protective equipment
Introduction
The new coronavirus creates a challenging environment for all frontline health-care workers (HCWs). To reduce the exposure of human populations to life-threatening diseases, personal protective equipment (PPE) is essential.1 HCWs are extremely vulnerable to various skin diseases due to skin friction, hyper-hydration effects, and contact reactions.2 Certain studies have indicated that HCWs are using PPE, for example, caps, goggles, face shields, surgical masks, gowns, and gloves, which have been related to the development of certain cutaneous manifestations.3,4 Recently, several related studies on the prevalence of skin injuries among medical staff wearing PPE have been published. Jiang et al5 found this prevalence rate to be 42.8%. In another report, the prevalence of skin damage was 97.0%, with the nasal bridge being the most commonly affected site (83.1%).6
Facemasks are one of the essential components of PPE for HCWs and civilians during the COVID-19 pandemic.7,8 Moreover, the applicability of facemasks has been validated for preventing the transmission of the human coronavirus and the influenza virus from symptomatic individuals.7,9,10 However, the prolonged wearing of facemasks can exacerbate the prevalence of adverse reactions (ADRs) of facial skin and potential skin disease;4,11–14 in particular, HCWs are more vulnerable than the general populace to the disruption of the skin barrier.15,16 Therefore, the aim of this research is to study the characteristics of the adverse reactions to facemasks in HCWs to provide a reference for facemask manufacturers and the government to formulate relevant measures to reduce the incidence of ADRs due to the prolonged wearing of facemasks.
Methods
This cross-sectional study used an online survey distributed as a web link. The questionnaire was distributed to different hospitals in Zhejiang Province, China, using WhatsApp. The questionnaire was distributed between August and September 2021. A total of 1147 questionnaires were collected, and of these, 1090 (95.0%) were valid and returned.
The study was conducted in accordance with the Declaration of Helsinki and approved by the regional ethics committee (Zhejiang Rongjun Hospital, approval number: YAN 2020–033), and all participants provided informed consent.
Survey data was collected from HCWs, including doctors, nurses, pharmacists, technicians, and other hospital workers. Only individuals between 18 and 60 years of age and those wearing facemasks without underlying skin disease were included in the study. The voluntary, anonymous, cross-sectional survey we administered had three sections: (a) demographic information, including age, sex, occupation, hospital department, and medical institution level; (b) facemask use details, including types of facemasks, duration of wearing facemasks, and frequency of wearing facemasks; (c) questions about facemask wearing-related ADRs, including ADR symptoms and signs. Two experts in medical terminologies have annotated the questionnaire alongside plain language, for example, chest tightness and shortness refers to difficulty breathing, shortness of breath, or feeling like you cannot breathe enough air.
Data were analyzed by SPSS statistical software (version 20.0, IBM SPSS Inc, Chicago, IL, USA). Count data are expressed as percentages (%), while measurement data are presented as mean ± SD. Comparison of means between groups was performed by a Mann–Whitney U-test, Fisher’s exact test, or r × c chi-square test. α = 0.05 was the test level. Spearman correlation was calculated. The differences were considered significant at P values of less than 0.05.
Results
General Characteristics
A total of 1147 questionnaires were collected; of these, 1090 (95.03%) were returned and valid. Of 1090 participants, more than half of the study participants (57.98%) were in the age range of 20–35 years, 857 (78.62%) participants were female, 636 (58.3%) participants were nurses, 489 (44.86%) participants worked in general wards, and 734 (66.42%) participants had a skin allergy history. More than half of the hospitals were ranked as secondary hospitals (60.46%), followed by tertiary hospitals (36.33%) and primary hospitals (3.21%). The vast majority of facemask types were surgical masks (98.26%), whereas only 1.74% were N95 masks; 79.91% of participants wore facemasks hanging over the ears, while the other (20.09%) wore strains; 94.86% of participants the facemasks discriminating a size code. In terms of duration, the highest proportion of participants wore facemasks for 6–8 hours (32.66%), followed by 4–6 hours (29.72%), 8–10 hours (23.85%), >12 hours (8.99%), and 10–12 hours (4.77%). There were significant differences in the incidence of ADRs across different occupations, departments, hospital ranks, facemask models, discriminating size codes, and durations of mask wear (P < 0.001, P = 0.013, P = 0.004, P = 0.007, P = 0.042, P < 0.001, respectively). There was no significant correlation between the incidence of ADRs and the durations of mask wear (Spearman test, r = 0.7, P = 0.188). Incidence of ADRs does not significantly increase with the durations of mask wear where wearing mask time exceeded 4 hours. The sociodemographic characteristics and facemasks of the participants are summarized in Table 1.
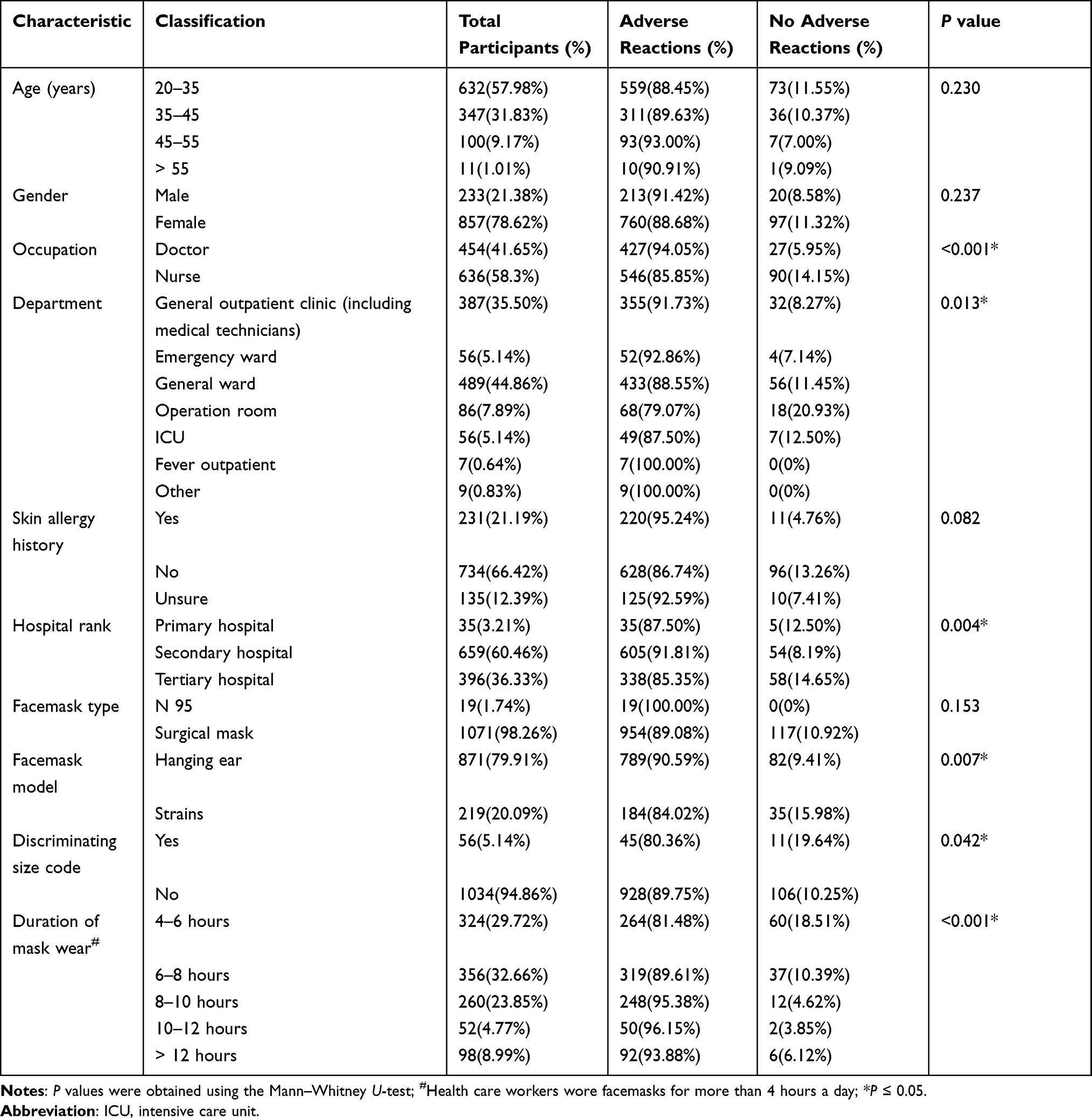 |
Table 1 The Sociodemographic Characteristics and Facemask Characteristics of the Participants (n = 1090) |
Associations Between Facemask Types and ADR Types
Of the 1090 participants, 954 wore medical facemasks, while 136 wore N95 facemasks. The incidence of chest tightness and shortness of breath and face eczema was significantly higher in HCWs wearing N95 facemasks (41.91%; 31.62%) than in HCWs wearing medical facemasks (38.05%, P = 0.010; 21.91%, P = 0.012). There was no significant difference in ADR incidence for upper respiratory symptoms, nose pain or indentation, damaged skins on nose, ear pain or indentation, facial skin pain or indentation, or damaged facial skin (detailed data are shown depicted in Table 2).
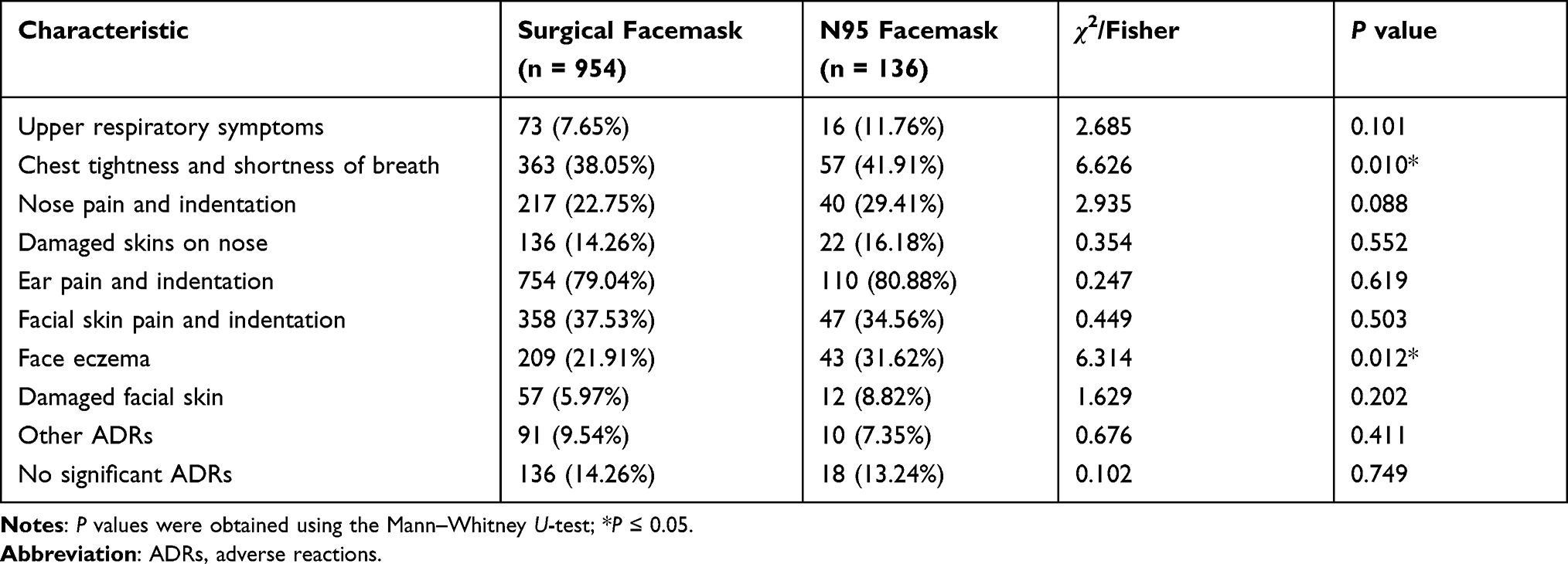 |
Table 2 Associations Between Facemask Types and ADRs Types |
Associations Between Facemask Models and ADR Types
Of the 1090 participants, 871 wore hang-facemasks, while 219 wore strain-facemasks. The incidence of ear pain and indentation was significantly higher in HCWs wearing hang-facemasks (83.81%) than in HCWs wearing strain facemasks (61.19%, P < 0.001). There was no significant difference in ADR incidence for upper respiratory symptoms, chest tightness and shortness of breath, nose pain or indentation, damaged skins on nose, facial skin pain or indentation, face eczema, or damaged facial skin (detailed data are shown in Table 3).
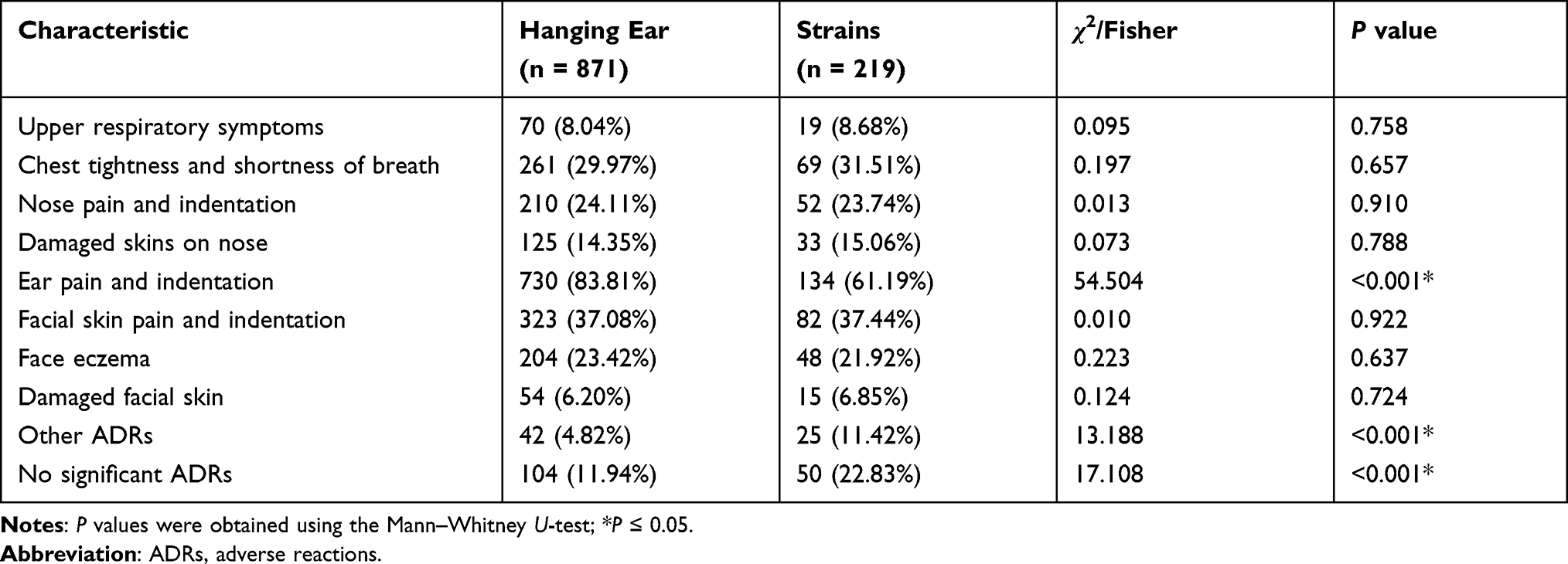 |
Table 3 Associations Between Facemask Models and ADRs Types |
Associations Between Facemask Discriminating Size Code and ADR Types
Of the 1090 participants, 1034 wore undiscriminating size code facemasks, and 56 wore discriminating size code facemasks. The incidence of ear pain and indentation was significantly higher in HCWs wearing undiscriminating size code facemasks (79.88%) than in HCWs wearing discriminating size code facemasks (67.86%, P = 0.031). There was no significant difference in ADR incidence for upper respiratory symptoms, chest tightness and shortness of breath, nose pain or indentation, damaged skins on nose, facial skin pain or indentation, face eczema, or damaged facial skin (detailed data are shown in Table 4).
 |
Table 4 Associations Between Facemask Discriminating Size Code and ADRs Types |
Associations Between Durations of Mask Wear and ADR Types
The proportion of HCWs wearing facemasks for 4–6 hours, 6–8 hours, 8–10 hours, 10–12 hours, and >12 hours per day was 29.72%, 32.66%, 23.85%, 4.77%, and 8.99%, respectively. Significant differences were observed in ADRs for upper respiratory symptoms, chest tightness and shortness of breath, nose pain and indentation, damaged skins on nose, ear pain and indentation, facial skin pain and indentation, and face eczema. There was a significant reduction (P < 0.001) in the incidence of HCWs without ADRs with increasing time wearing facemasks (detailed data are shown in Table 5).
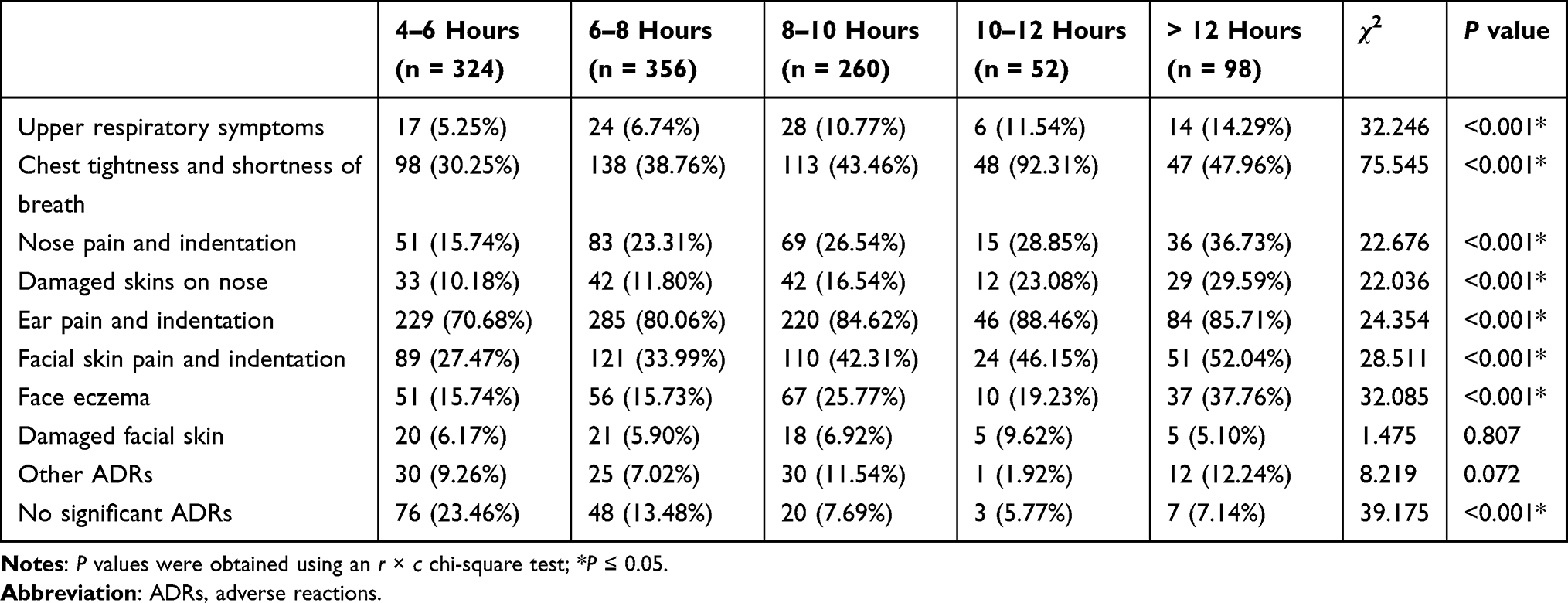 |
Table 5 Associations Between Durations of Mask Use and ADRs Types |
Discussion
“Facemasks” is a term used for a wide range of face protective equipment that can reduce the transmission of infectious droplets. The purpose of surgical masks is to protect patients with open wounds from possible surrounding infectious agents during surgery. The applicability of surgical masks for preventing the transmission of the human coronavirus and the influenza virus from symptomatic individuals has been confirmed.7,17,18
Therefore, experts, including the Centers for Disease Control and Prevention, have widely recommended that people wear facemasks to prevent the spread of COVID-19, especially in public.9,10,19 However, the prolonged wearing of facial PPE, especially tight-fitting PPE, can cause various skin injuries, such as contact dermatitis, urticaria, skin tears, blisters, and pressure ulcers.20 It is almost impossible for HCWs to avoid wearing masks for a long time; therefore, minimizing and treating ADRs is a challenge.
A survey found that over one-quarter of children experienced breathing discomfort attributed to facemasks.21 Accordingly, we found that 38.53% of HCWs wearing facemasks for over 4 hours experienced chest tightness and shortness of breath, and the incidence of chest tightness and shortness of breath was significantly higher in HCWs wearing N95 facemasks (41.91%) than in HCWs wearing medical facemasks (38.05%). It is possible that the air and water vapor transmittance of N95 masks higher than surgical masks.22 The microclimate conditions inside and outside of N95 facemasks and surgical masks may be different. Compared to N95 masks, the outer surface temperature and humidity of surgical masks are higher, while the inner surface temperature and humidity are lower.23
It has been reported that N95 masks may cause more facial ADRs and higher levels of discomfort compared to other masks.24 Additionally, Zuo et al24 pointed out that N95 masks are the least breathable and cause more pressure than other types of masks, which may increase the number of facial ADRs, including acne, pruritus, and skin rash. Moreover, N95 masks have been reported to create a closer, moister, and warmer environment; consequently, skin microbial populations associated with facial skin disease may increase ADRs.25
Wearing a facemask has also been shown to lead to increased sebum production in areas not touched by the mask.26 The occlusion of the pilosebaceous unit by a tight facemask may trigger acne.27 Additionally, facemasks may contain rubber bands, glue, or metal clips that may cause irritation or allergic contact dermatitis.13,15,28 We found a similar result in this study. The incidence of face eczema was significantly higher in HCWs wearing N95 masks (31.62%) than in HCWs wearing medical facemasks (21.91%). Daye et al29 found significant acne in HCWs using N95 masks, whereas surgical masks did not contribute significantly to its development.
Since all facemasks do not have the same size and shape, we investigated the relationships of facemask models and discriminating size codes with ADR types. The incidence of ear pain and indentation was significantly higher in HCWs wearing hang-facemasks (83.81%) and undiscriminating size code facemasks (79.88%) than in HCWs wearing strain-facemasks (61.19%) and discriminating size code facemasks (67.86%). This might be because of the hang-facemasks’ and discriminating size code facemasks’ inability to regulate the degree of tightness, resulting in those with larger heads being more prone to ear pain and indentation.
Li et al23 found that N95 masks resulted in more significant ADRs than surgical masks, but this phenomenon was not found in this survey, which may be caused by the following reasons: the wearing time was the cumulative daily wearing time; the medical staff wore masks for more than 4 hours per day. The question of whether N95 masks lead to a higher incidence of ADRs than surgical masks with prolonged wear needs further experimental confirmation. However, the prolonged use of facemasks can lead to excessive maceration and disruption of the skin barrier.4 Long-term use of facemasks, as well as a lack of appropriate cleaning and relief of skin stress, may also exacerbate underlying skin conditions and potentially spread bacteria.14
With the deepening of the research, the description of ADRs associated with face mask wearing is more detailed and accurate. Yaqoob et al30 found that oily-skinned female HCWs wearing N-95 masks most prone to acne eruption on cheeks.
Based on our results, some measures should be taken to prevent and control ADRs. The World Health Organization guidelines and instructions on the proper use of facemasks, such as encouraging HCWs to be aware of and follow CDC-recognized protocols for mask-wearing, can minimize ADRs.31 Moreover, we have several recommendations for reducing the incidence of adverse reactions: 1) taking 15 min of rest after 2 hours of mask-wearing; 2) ensuring proper cleaning, including hand washing or sanitizing with water and soap, before putting on and removing the mask;32 and 3) using a moisturizer after face wash, keeping skin makeup-free, choosing the right facemask size code,33 and avoiding usage of moisturizer multiple times per day.14
Limitations
The clinical signs and severity of ADRs in this study were all intuitive and not assessed by any dermatologist. The participants with underlying diseases but not skin disease were not excluded from the study. In addition, this study did not evaluate the protective effect of different types of facemasks. However, the literature on the protective effects of different types of facemasks is disputable Loeb et al34 reported that surgical masks were non-inferior in preventing laboratory-confirmed influenza compared with N95 masks, but their findings were criticized for various study limitations.35,36 Conversely, another study using a cluster-randomized clinical trial found that medical masks led to twice the infection rate of N95 masks.37 Therefore, the protective effects of different types of facemasks need to be confirmed by further research.
Conclusions
Incidence of ADRs does not significantly increase with the durations of mask wear where wearing mask time exceeded 4 hours per day. The medical staff generally wore masks for more than 4 hours per day; therefore, we recommend taking 15 min of rest after 2 hours of mask-wearing. Results in this study support the conclusion that the type of strain-facemasks and discriminating size code facemasks has a lower incidence of ADRs than other type of medical facemasks.
Funding
This study was supported by the Jiaxing Science and Technology Innovation and People’s Livelihood Science and Technology Plan (Grant no. 2021AD30060).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang JV, Parish LC. Dermatologic manifestations of the 1918–1919 influenza pandemic. SKINmed. 2019;17(5):296–297.
2. Kantor J. Behavioral considerations and impact on personal protective equipment use: early lessons from the coronavirus (COVID-19) pandemic. J Am Acad Dermatol. 2020;82(5):1087–1088. doi:10.1016/j.jaad.2020.03.013
3. Masood S, Tabassum S, Naveed S, Jalil P. COVID-19 pandemic & skin care guidelines for health care professionals. Pak J Med Sci. 2020;36(COVID19–S4):S115.
4. Lan J, Song Z, Miao X, et al. Skin damage among health care workers managing coronavirus disease-2019. J Am Acad Dermatol. 2020;82(5):1215–1216.
5. Jiang Q, Song S, Zhou J, et al. The prevalence, characteristics, and prevention status of skin injury caused by personal protective equipment among medical staff in fighting COVID-19: a Multicenter, Cross-Sectional Study. Adv Wound Care. 2020;9(7):357–364. doi:10.1089/wound.2020.1212
6. Elston DM. Occupational skin disease among health care workers during the coronavirus (COVID-19) epidemic. J Am Acad Dermatol. 2020;82(5):1085–1086. doi:10.1016/j.jaad.2020.03.012
7. Leung NHL, Chu DKW, Shiu EYC, et al. Author correction: respiratory virus shedding in exhaled breath and efficacy of face masks. Nat Med. 2020;26(6):981. doi:10.1038/s41591-020-0946-9
8. Cowling BJ, Chan KH, Fang VJ, et al. Facemasks and hand hygiene to prevent influenza transmission in households: a cluster randomized trial. Ann Intern Med. 2009;151(7):437–446. doi:10.7326/0003-4819-151-7-200910060-00142
9. Liu Y, Leachman SA, Bar A. Proposed approach for reusing surgical masks in COVID-19 pandemic. J Am Acad Dermatol. 2020;83(1):e53–e54. doi:10.1016/j.jaad.2020.04.099
10. Esposito S, Principi N, Leung CC, Migliori GB. Universal use of face masks for success against COVID-19: evidence and implications for prevention policies. Eur Respir J. 2020;55(6):45.
11. Kosasih LP. MASKNE: mask-induced acne flare during coronavirus disease-19. what is it and how to manage it? Open Access Maced J Med Sci. 2020;8(T1):411–415. doi:10.3889/oamjms.2020.5388
12. Szepietowski JC, Matusiak Ł, Szepietowska M, Krajewski PK, Białynicki-Birula R. Face mask-induced itch: a self-questionnaire study of 2315 responders during the COVID-19 pandemic. Acta Derm Venereol. 2020;100(10):adv00152. doi:10.2340/00015555-3536
13. Maliyar K, Sachdeva M, Mufti A, Yeung J. Reply to: “Skin damage among health care workers managing coronavirus disease 2019”. J Am Acad Dermatol. 2020;83(2):e169–e170. doi:10.1016/j.jaad.2020.05.037
14. Desai SR, Kovarik C, Brod B, et al. COVID-19 and personal protective equipment: treatment and prevention of skin conditions related to the occupational use of personal protective equipment. J Am Acad Dermatol. 2020;83(2):675–677.
15. Foo CC, Goon AT, Leow YH, Goh CL. Adverse skin reactions to personal protective equipment against severe acute respiratory syndrome–a descriptive study in Singapore. Contact Dermatitis. 2006;55(5):291–294. doi:10.1111/j.1600-0536.2006.00953.x
16. Bhoyrul B, Lecamwasam K, Wilkinson M, et al. A review of non-glove personal protective equipment-related occupational dermatoses reported to EPIDERM between 1993 and 2013. Contact Dermatitis. 2019;80(4):217–221. doi:10.1111/cod.13177
17. Offeddu V, Yung CF, Low MSF, Tam CC. Effectiveness of masks and respirators against respiratory infections in healthcare workers: a systematic review and meta-analysis. Clin Infect Dis. 2017;65(11):1934–1942. doi:10.1093/cid/cix681
18. Panovska-Griffiths J, Kerr CC, Waites W, et al. Modelling the potential impact of mask use in schools and society on COVID-19 control in the UK. Sci Rep. 2021;11(1):8747. doi:10.1038/s41598-021-88075-0
19. Prevention CfDCa. How to protect yourself and others; 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html.
20. Yap KK, Murali M, Tan Z, Zhou X, Li L, Masen MA. Wax-oil lubricants to reduce the shear between skin and PPE. Sci Rep. 2021;11(1):11537. doi:10.1038/s41598-021-91119-0
21. Assathiany R, Salinier C, Béchet S, et al. Face masks in young children during the COVID-19 pandemic: parents’ and pediatricians’ point of view. Front Pediatr. 2021;9:676718. doi:10.3389/fped.2021.676718
22. Li Y, Wong T, Chung J, et al. In vivo protective performance of N95 respirator and surgical facemask. Am J Ind Med. 2006;49(12):1056–1065. doi:10.1002/ajim.20395
23. Li Y, Tokura H, Guo YP, et al. Effects of wearing N95 and surgical facemasks on heart rate, thermal stress and subjective sensations. Int Arch Occup Environ Health. 2005;78(6):501–509. doi:10.1007/s00420-004-0584-4
24. Zuo Y, Hua W, Luo Y, Li L. Skin reactions of N95 masks and medial masks among health-care personnel: a self-report questionnaire survey in China. Contact Dermatitis. 2020;83(2):145–147. doi:10.1111/cod.13555
25. Donovan J, Skotnicki-Grant S. Allergic contact dermatitis from formaldehyde textile resins in surgical uniforms and nonwoven textile masks. Dermatitis®. 2007;18(1):40–44.
26. Hua W, Zuo Y, Wan R, et al. Short-term skin reactions following use of N95 respirators and medical masks. Contact Dermatitis. 2020;83(2):115–121. doi:10.1111/cod.13601
27. Tan KT, Greaves MW. N95 acne. Int J Dermatol. 2004;43(7):522–523. doi:10.1111/j.1365-4632.2004.02338.x
28. Yu J, Chen JK, Mowad CM, et al. Occupational dermatitis to facial personal protective equipment in health care workers: a systematic review. J Am Acad Dermatol. 2021;84(2):486–494. doi:10.1016/j.jaad.2020.09.074
29. Daye M, Cihan FG, Durduran Y. Evaluation of skin problems and dermatology life quality index in health care workers who use personal protection measures during COVID-19 pandemic. Dermatol Ther. 2020;33(6):e14346. doi:10.1111/dth.14346
30. Yaqoob S, Saleem A, Jarullah FA, Asif A, Essar MY, Emad S. Association of acne with face mask in healthcare workers amidst the COVID-19 outbreak in Karachi, Pakistan. Clin Cosmet Investig Dermatol. 2021;14:1427–1433. doi:10.2147/CCID.S333221
31. CDC. Covid-19 and your health. Centers for disease control and prevention; 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/about-face-coverings.html.
32. Desai AN, Mehrotra P. Medical masks. JAMA. 2020;323(15):1517–1518. doi:10.1001/jama.2020.2331
33. 9 ways to prevent face mask skin problems. Available from: https://www.aad.org/public/everyday-care/skin-care-secrets/face/prevent-face-mask-skin-problems.
34. Loeb M, Dafoe N, Mahony J, et al. Surgical mask vs N95 respirator for preventing influenza among health care workers: a randomized trial. JAMA. 2009;302(17):1865–1871. doi:10.1001/jama.2009.1466
35. Clynes N. Surgical masks vs N95 respirators for preventing influenza. JAMA. 2010;303(10):
36. Finkelstein Y, Schechter T, Freedman SB. Surgical masks vs N95 respirators for preventing influenza. JAMA. 2010;303(10):
37. MacIntyre CR, Wang Q, Cauchemez S, et al. A cluster randomized clinical trial comparing fit-tested and non-fit-tested N95 respirators to medical masks to prevent respiratory virus infection in health care workers. Influenza Other Respi Viruses. 2011;5(3):170–179. doi:10.1111/j.1750-2659.2011.00198.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Pre-Existing Comorbidities with Disease Severity Among COVID-19 Patients in Eastern Ethiopia
Merga BT, Ayana GM, Raru TB, Alemu A, Negash B, Bekana M, Birhanu A, Dessie Y
Infection and Drug Resistance 2022, 15:2825-2834
Published Date: 1 June 2022
COVID-19 Case Fatality Rate and Factors Contributing to Mortality in Ethiopia: A Systematic Review of Current Evidence
Girma D, Dejene H, Adugna L, Tesema M, Awol M
Infection and Drug Resistance 2022, 15:3491-3501
Published Date: 4 July 2022
Impact of the COVID-19 Pandemic on Breastfeeding Support Services and Women’s Experiences of Breastfeeding: A Review
Lubbe W, Niela-Vilén H, Thomson G, Botha E
International Journal of Women's Health 2022, 14:1447-1457
Published Date: 6 October 2022
Assessment of the Prevalence and Incidence of COVID-19 in Saudi Arabia
Alyahyawi HE, Alharbi RA, Alatawi SK, Ahmed WAM, Almalki SSR
Journal of Multidisciplinary Healthcare 2023, 16:227-236
Published Date: 24 January 2023
Re-Emerging COVID-19: Controversy of Its Zoonotic Origin, Risks of Severity of Reinfection and Management
Chala B, Tilaye T, Waktole G
International Journal of General Medicine 2023, 16:4307-4319
Published Date: 20 September 2023