Back to Journals » Journal of Pain Research » Volume 11
The effect of diaphragm training on lumbar stabilizer muscles: a new concept for improving segmental stability in the case of low back pain
Authors Finta R ![]() , Nagy E
, Nagy E ![]() , Bender T
, Bender T ![]()
Received 27 July 2018
Accepted for publication 10 October 2018
Published 28 November 2018 Volume 2018:11 Pages 3031—3045
DOI https://doi.org/10.2147/JPR.S181610
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Michael Überall
Video abstract presented by Regina Finta.
Views: 1590
Regina Finta,1 Edit Nagy,1 Tamás Bender2
1Department of Physiotherapy, Faculty of Health Sciences, University of Szeged, Szeged, Hungary; 2Department of Orthopedics, Faculty of Medicine, Doctoral School of Clinical Medicine, University of Szeged, Szeged, Hungary
Purpose: The aim of this study was to assess the effects of diaphragm training on low back pain and thickness of stabilizer muscles of the lumbar spine.
Patients and methods: Fifty-two individuals were recruited with a history of chronic low back pain in our randomized controlled trial. The participants were divided randomly into two groups. One of the groups took part in a complex training program and completed with diaphragm training (DT group, n=26). The control (C) group took part only in the complex training (n=21). The thickness of transversus abdominis, diaphragm, and lumbar multifidus muscle was measured with ultrasonography in two positions: lying and sitting. All muscles were assessed in relaxed and in contracted state in the lying position and in a relatively relaxed (calm sitting) and relatively contracted state (during weightlifting) in the sitting position.
Results: After the training, severity of the pain was significantly reduced in both the groups. Regarding the thickness of the muscles, there were no changes in group C. The thickness of transversus abdominis increased significantly in relaxed and in relatively relaxed state, but there were no changes in contracted and relatively contracted state in group DT. As for the diaphragm muscle, there were significant increase in the state of supine position and in relatively contracted state, but there was no notable change in relatively relaxed state. With regard to the thickness of lumbar multifidus, a significant increase was only found in the left-sided muscle in relaxed, relatively relaxed, and relatively contracted state and in case of the right-sided one in relatively contracted state in group DT.
Conclusion: Our results suggest that diaphragm training has an effect also on the thickness of other active stabilizers of the lumbar spine, such as transversus abdominis and lumbar multifidus muscles.
Keywords: chronic low back pain, ultrasound assessment, lumbar stabilization, postural function
Introduction
Chronic low back pain (CLBP) is a very common problem in developed countries and affects the entire population from children to the elderly.1 Chronic pain has a negative effect on the individuals’ lives as well as on the whole society. This is the main cause of inactivity and job absenteeism.1 Low back pain is among the top ten high burden diseases and injuries, with the average number of disability-adjusted life years, higher than that of HIV, road injuries, tuberculosis, lung cancer, COPD, and preterm birth complications.1 Low back pain has been ranked as the greatest contributor to global disability.2 Based on the etiology, CLBP can be divided into two types: nonspecific and specific low back pain. If the pathological reason is known, it is called specific low back pain, but if the reason for the pain is not known, it is classified as nonspecific CLBP.1 The majority of low back pain cases are nonspecific CLBPs, which makes the treatment more complicated.3
One of the postulated reasons for nonspecific low back pain is the segmental instability of the lumbar spine.4 The concept of segmental instability has not yet been proven in vivo; experiments were performed in vitro on cadaveric lumbar spines.5 Several researchers have tried to define segmental spinal instability, but there is no accurate definition for the subtle forms of instability which are present when nonspecific low back pain occurs. This subtle instability may not be detected by radiological techniques or physical examination. One of the possible explanations for this instability is the “neutral zone concept” proposed by Panjabi.6 Based on the theoretical findings, the total range of motion (ROM) of a spinal motion segment may be divided into two zones: a neutral and an elastic one. The neutral zone is the initial part of the total ROM and spinal motion is produced against minimal internal resistance in this zone. The elastic zone is the portion nearer to the end-range of movement that is produced against significant internal resistance.6 Increased segmental laxity occurs when the size of the neutral zone increases.6 The expansion of the neutral zone may occur as a result of a decrease in the capacity of the stabilizing system of the spine.6 Therefore, the increased size of the neutral zone is a better indicator of lumbar instability than the increased total ROM of the lumbar segment. Based on this theory, segmental instability may be defined as a decrease in the capacity of the stabilizing system of the spine to maintain the spinal neutral zones within physiological limits.6
Three subsystems are responsible for maintaining stability, namely passive, neural, and active subsystems. The passive subsystem consists of the spine and parts of the spinal joints; the neural subsystem receives information from the structures of the passive and active subsystems, and it stabilizes the lumbar spine by controlling the function of the active subsystem, namely the muscles.4 The neural and active subsystems are primarily responsible for spinal stability in the neutral zone.5 The members of the active subsystem can be divided into two groups: global and local stabilizer muscles. The global stabilizer muscles play an important role in performing the movements of the trunk and the hips, while the unique function of the local stabilizer muscles is the stabilization of the segments in relation to each other.7 Generally local stabilizers include all the deep layer muscles such as lumbar multifidus, transversus abdominis, pelvic floor muscles, and diaphragm.8 The stabilizing function of these deep muscles can be realized in a variety of ways. Lumbar multifidus has an important role in the segmental control mainly during lifting and rotational movements.5 Transversus abdominis muscle attaches to the thoracolumbar fascia; therefore, it is capable of increasing the stiffness of the lumbar spine indirectly.9 The pelvic floor muscles and diaphragm are in synergism with transversus abdominis, and they are responsible for maintaining and increasing intra-abdominal pressure during several postural tasks.10 Hodges and Gandevia11 presumed in a previous study that a possible explanation for the mechanism of the stabilizing function of the diaphragm and pelvic floor muscles is the following: the activation of transversus abdominis prior to the initiation of an upper limb movement results in the displacement of the abdominal contents; hence, the consequential contraction of the diaphragm and pelvic floor muscles is necessary to restrain the shift of these abdominal structures. In their research, they assessed the activation of the diaphragm and transversus abdominis muscle during repetitive arm flexions in standing position. Contrary to their hypothesis, they found that the activation of diaphragm occurs prior to an arm movement and happens simultaneously with the activation of transversus abdominis.11 The exact role of diaphragm in trunk stabilization has been under investigation for >50 years, but the accurate mechanism still remains poorly understood.12 There have been several types of research which investigated the functioning of trunk stabilizer muscles during upper limb movement in standing position.13–16 However, there have been few research considering the sitting position.11,16
The importance of using non-pharmacological treatments, such as physical exercises, to reduce the intensity of low back pain is well known.17 However, to date, there has been no unitary exercise training program or any well-established complex solution to the problem, and there is a huge gap between evidence and practice.17 There is no consensus even in the national guidelines.17 Previous studies specified the impact of several types of training on CLBP, but a diaphragm strengthening training has not been tested yet as a solution to it. Ki et al18 measured the effect of forced breathing exercises on lumbar stability. They proved that forced breathing exercises may improve lumbar stability in case of low back pain,18 but the role of breathing exercises in the background of the mechanism of improved lumbar stability was not clarified by this study. Janssens et al19 proved that the postural stability of the trunk can be improved by strengthening the diaphragm muscle and suggest that pain intensity may be decreased by diaphragm training. They strengthened the diaphragm with a POWERbreathe device that provides resistance to inhalation. Their training program lasted for 8 weeks, and the displacement of the center of the pressure was assessed by using a force plate. Pain intensity was measured with the Oswestry Disability Index. They found that the 8-week-long intensive diaphragm training increased respiratory muscle strength, that proprioceptive use changed in a positive way, and that the participants reported a decrease in low back pain severity.19 They presumed that their training program had an effect on the muscles other than diaphragm as well and may have improved the stabilization of the trunk.19 However, the changes that may have occurred as a result of the diaphragm strengthening training in the musculature and the mechanisms that provided the improvement of lumbar stabilization were not identified in their research.
The aim of this study was to assess the effects of an 8-week-long diaphragm training on low back pain and not only on thickness of the diaphragm but also on that of other stabilizer muscles like transversus abdominis and lumbar multifidus muscle.
Materials and methods
Subjects
A total of 52 people participated voluntarily in our study with a history of chronic nonspecific low back pain while two of them withdrew their participation. The inclusion criterion was low back pain lasting for at least 3 months. Participants were asked not to have any other treatment during the time of the training, and they were required to be able to learn the usage of the diaphragm trainer and to be able to get to the location of the training. Exclusion criteria were the following: diagnosed specific causes of low back pain, balance problems of neurological origin, malignant tumors, serious organ diseases, respiratory diseases, previous surgical interventions affecting the trunk or the limbs and the subjects being uncooperative. The participants were asked to indicate immediately if an acute inflammatory disease occurred. Based on these exclusion criteria, three subjects were excluded. All participants gave their written informed consent. The study is in compliance with the principles of the Declaration of Helsinki and was approved by the National Medical Research Council (identification number: 21416-2/2017/EKU). The trial was registered on www.clinicaltrials.gov (identification number: NCT03600207).
Study design
Grouping
This study was a randomized controlled trial which took place from September to December 2017. The participants were divided (www.randomizer.org) into two groups randomly: diaphragm training group (DT, n=26) and control group (C, n=21). The members of group C took part only in a complex training, while the members of group DT performed the complex training enhanced by diaphragm training. A flowchart of the study design can be seen in Figure 1. There were no significant differences between the groups regarding age, body mass index, and the duration of low back pain. The comparison of the main characteristics of the groups are summarized in Table 1.
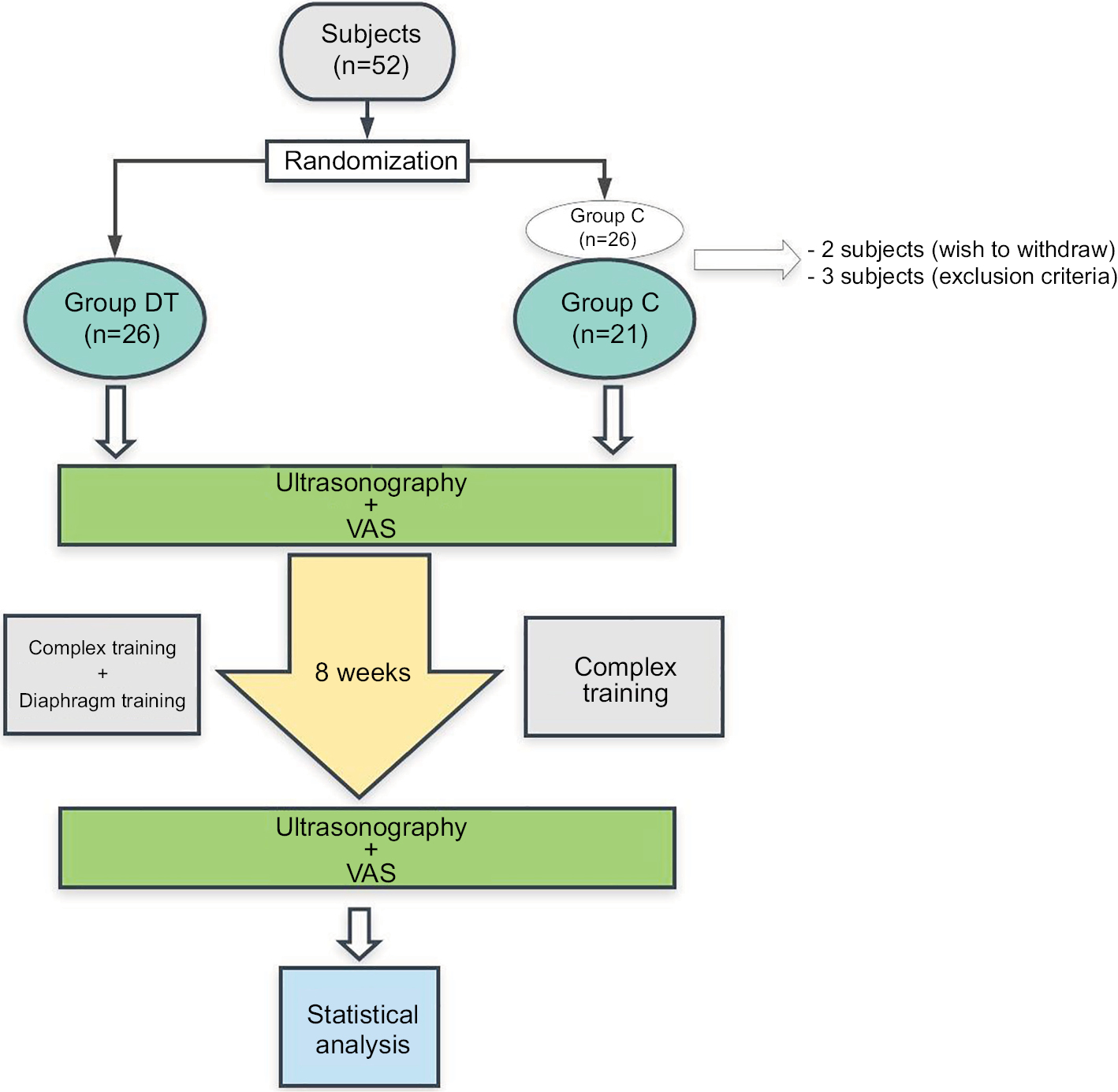 | Figure 1 Flowchart of the study design. Abbreviations: C, control group; DT, diaphragm training group; VAS, visual analog scale. |
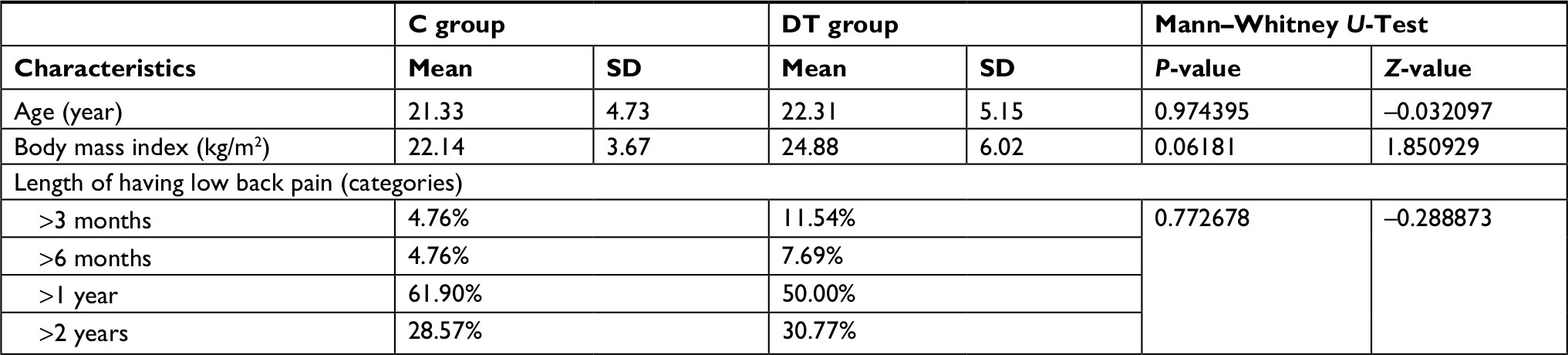 | Table 1 The main characteristics of the groups Abbreviations: C, control group; DT, diaphragm training group. |
The training method
Both the groups had an 8-week-long complex training, which was done twice per week, with 60 minutes duration (the details of the complex training are included in the Supplementary material). The members of groups C and DT participated in the same exercise program during the complex training. Besides this, group DT used a POWERbreathe Medic Plus (POWERbreathe Ltd, Warwickshire, UK) device twice a day at home, 30 inhalations per occasion, and with the speed of 15 inhalations/min in addition to the complex training. The device was also used when trunk muscle strengthening exercises were performed during trainings. Using this device, members of group DT inhaled against resistance. The subjects were educated about the proper use of the POWERbreathe Medic Plus device during the first session. Before the training, a baseline assessment was conducted in group DT: maximal inhalation pressure (MIP) was measured with a POWERbreathe KH2 (POWERbreathe Ltd) device to determine the magnitude of resistance during training. The resistance was set individually to the value of 60% of the MIP.
Measurements
Pain intensity was assessed with the visual analog scale (VAS).20 VAS is a unidimensional measure of pain intensity, which has been widely used in diverse adult populations.21 It is a continuous scale comprised of a horizontal line 10 cm in length. The scale is anchored by “no pain” (score of 0) and “worst imaginable pain” (score of 10). A higher score indicates greater pain intensity.21 Test–retest reliability is good (r=0.94, P<0.001).21 VAS scores are shown to correlate highly with other pain measure scores (r=0.62–0.91), and they are sensitive to measuring changes in pain associated with treatment or time.21
The thickness of the stabilizer muscles’ belly was measured with B-mode ultrasonography. By using a Zonare Z.One Ultrasound System (ZONARE Medical Systems, Inc., Mountain View, CA, USA; 2013), the thickness of transversus abdominis, lumbar multifidus, and diaphragm muscles were recorded in two different positions: in lying and in sitting positions (Figure 2). The positions of the transducers can be further seen in Figure 3. All the muscles were measured in two different states: in a relaxed and in a contracted state. When a clear image of the measured muscles was seen, it was frozen on the screen and saved. The thickness of the muscles’ belly was measured on the saved pictures. Three pictures of one muscle in one position and state were taken. A total of 48 pictures of each participant were taken before the training and also 48 pictures after the training program. To ensure the same setting for ultrasonography, the skin surface was constantly marked, and the measurement was carried out by the same person with experience in ultrasonography. Test–retest reliability was tested by calculation of intra-class correlation and the reliability coefficient. Both the high interclass correlations (0.991–1) and the small repeatability coefficients (0.008–0.095) showed good reliability.
 | Figure 2 The applied postures during the ultrasonography: (A) supine position; (B) prone position; (C) quiet sitting; (D) weightlifting. |
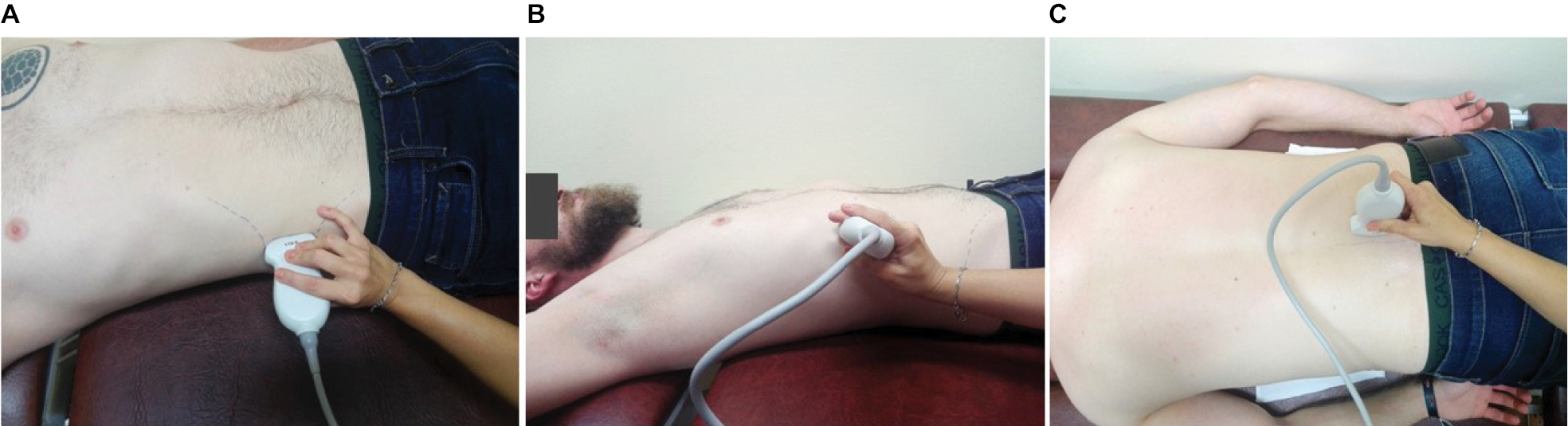 | Figure 3 The positions of the transducers: (A) transversus abdominis muscle; (B) diaphragm muscle; (C) lumbar multifidus muscle (right-sided). |
In case of transversus abdominis and diaphragm muscle, the subject was in a supine position with hips and knees flexed during the assessment (Figure 2A). Whereas in the case of the lumbar multifidus muscle, the subject was in a prone position with flexed knees and the lumbar spine was positioned into flexion by a small pillow placed under the abdomen (Figure 2B). Also, the knees were supported by a small pillow, providing ~30° flexion. All muscles were assessed in a sitting position as well: during holding the sitting posture (Figure 2C) and during a weightlifting task (Figure 2D). The subjects were sitting on a chair without back support with hips and knees flexed in 90° and their feet were on the floor. The neutral position of the trunk was set, and the participants were asked to hold this position during the examination. The subjects were sitting calmly but the stabilizer muscles were active to maintain the vertical position, so the so-called relaxed state was just a relatively relaxed state (Figure 2C). To achieve a more contracted state of the stabilizer muscles in the sitting position, a weightlifting activity was applied while holding the neutral position of the trunk. One dumbbell was used for the lifting procedure, and it was held with both hands (Figure 2D). The participants had to lift the weight forward to the height of the shoulders with extended elbows and maintain this position until the ultrasonography was performed (about 2 seconds) and repeat this maneuver as many times as was needed to assess the muscles. The patients were asked not to change the height of the lifting to ensure the same conditions.13 The weight to be lifted was chosen based on the subjective, perceived difficulty of the task: the subjects had to be able to lift it 13 times with short rests (about 5 seconds) between them. Thirteen repetitions were determined because the first lifting was a testing procedure when we could correct the height of the lifting and the posture of the trunk if that was necessary. Then three pictures of the assessed muscles were taken (three of transversus abdominis, three of the left- and three of the right-sided lumbar multifidus, and three of diaphragm muscle). When a neutral trunk posture was held in sitting position, it was defined as a relatively relaxed state, whereas lifting the weight in neutral trunk posture caused a relatively contracted state. Transversus abdominis muscle was assessed during tidal inhalation while diaphragm muscle was assessed during tidal exhalation to minimize the respiratory function of these muscles. The methodology of the ultrasound assessments is summarized in Table 2.
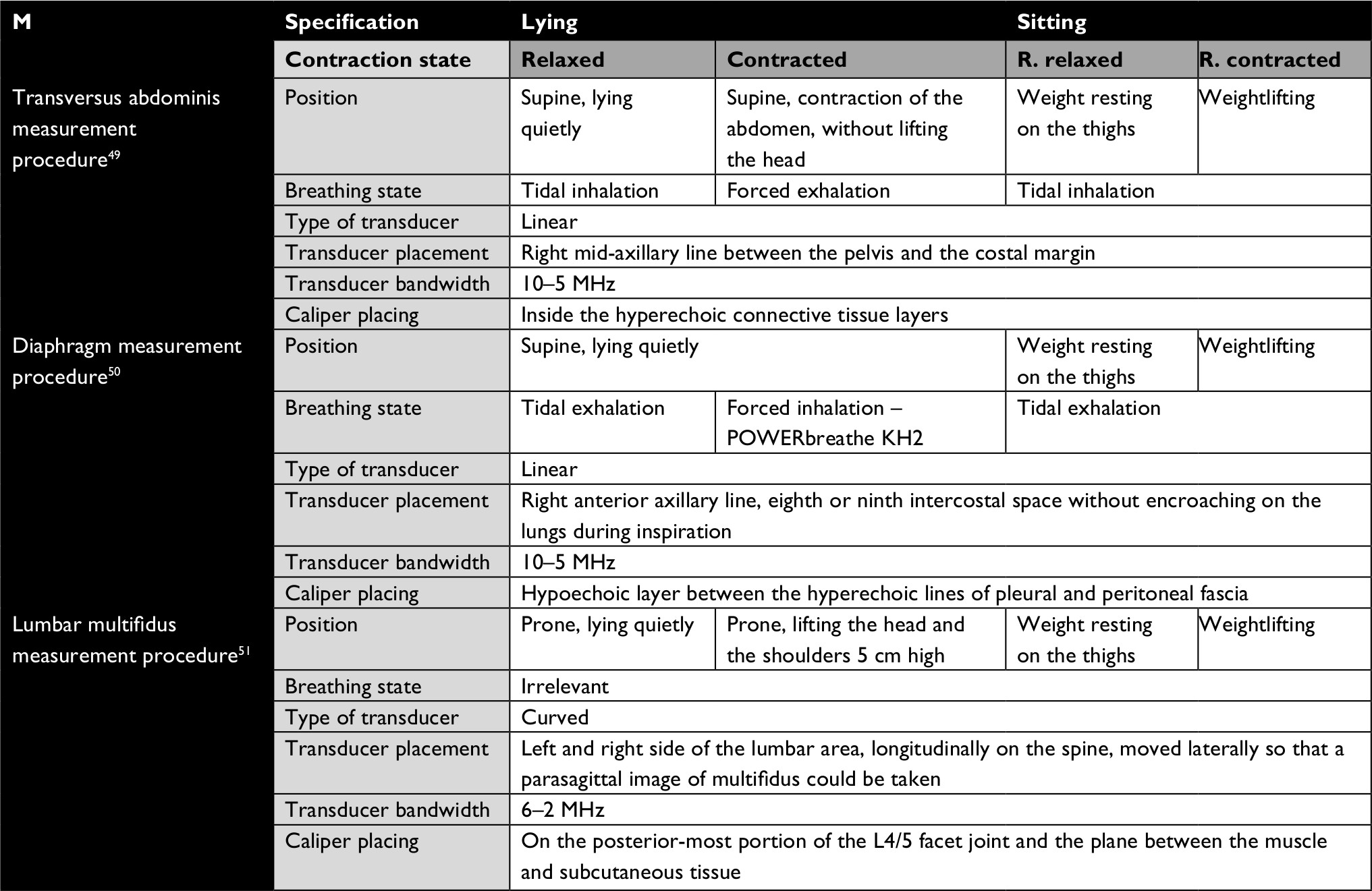 | Table 2 Measurement procedures of the ultrasound assessment Abbreviations: M, muscle; R., relatively. |
Data collection and analysis
When using the VAS, the participants had to mark the average severity of lumbar pain on a 10-cm-long line.20 The scale is anchored by “no pain” (score of 0) and “worst imaginable pain” (score of 10). The distance of their mark from the zero point in cm-s was defined as the severity of the pain.21 For the comparison of the pain intensity, average values were calculated by group (mean ± SD). To compare the change between the before and after data, Wilcoxon matched pairs test was used.
Ultrasound data analysis
Statistical calculations were performed with STATISTICA 13.1 (TIBCO Software Inc., Palo Alto, CA, USA) and IBM SPSS Statistics 24 software (IBM Corporation, Armonk, NY, USA). Test–retest reliability of the ultrasound imaging was checked by intra-class coefficients. The Shapiro–Wilk test was used as normality test. To compare the change between the before and after data, a two-way repeated measures ANOVA mixed model was performed where the three repetitions were also taken into account. Results are given as estimated marginal means with their standard errors. To avoid significant changes by occasion, individual P-values were corrected by the step-down Bonferroni.
Results
Severity of pain
Both the groups showed significant improvement (P<0.01) with regard to pain after the training. In group C, the average intensity of pain was 5.75 (±1.68) initially and after the training it changed to 2.14 (±1.9) (P=0.000219), which shows a 62% decrease. In the group DT, the average intensity of pain was 5.70 (±1.74) before the treatment, whereas after the 8-week-long training it was only 2.62 (±1.89) (P=0.000017), so the decrease is 54%.
Ultrasound assessment
The results of the statistical comparison are summarized in Table 3. The estimated means and standard errors of the ultrasound assessment data are shown in Figures 4–9.
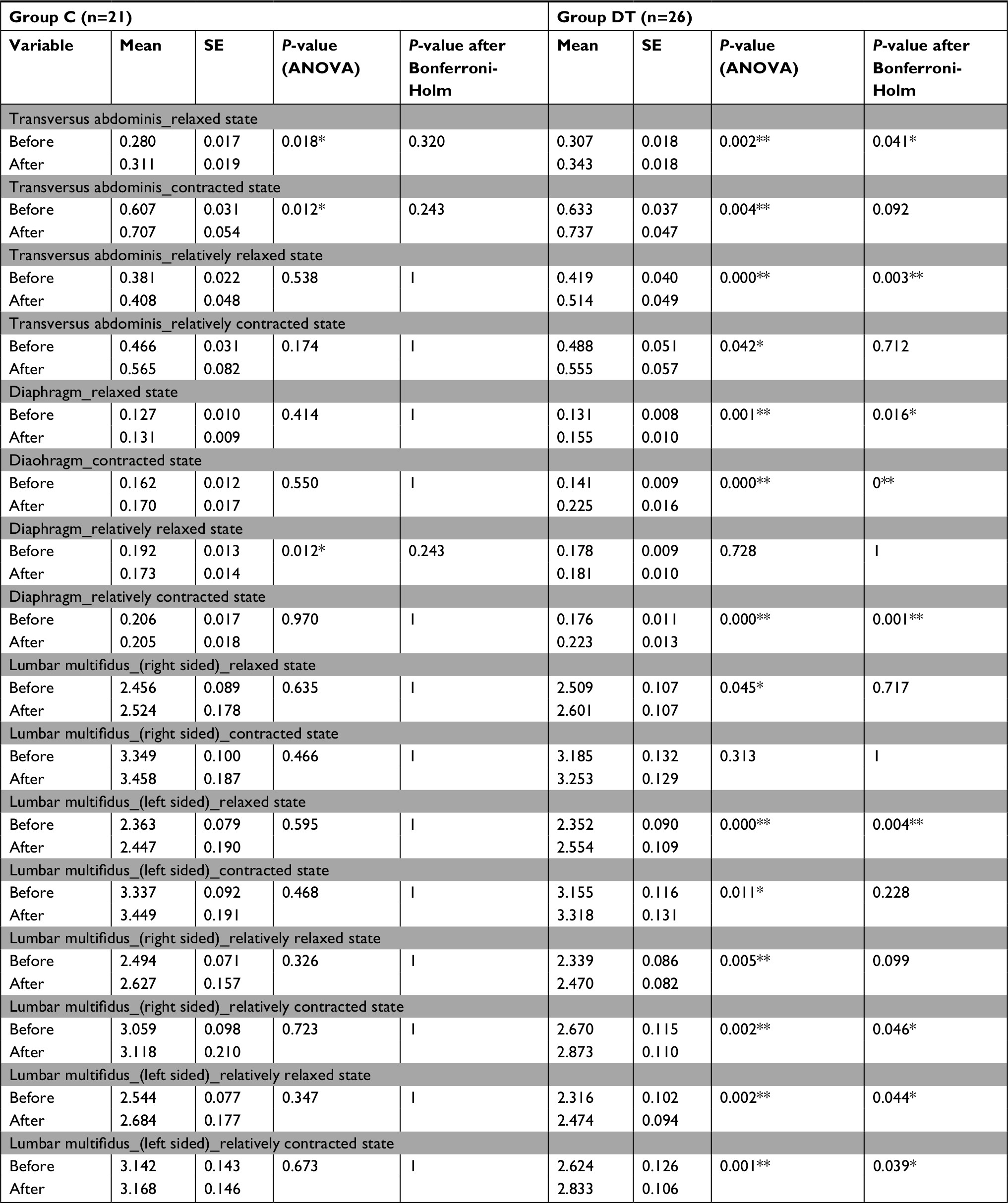 | Table 3 The results of the statistical comparison Notes: *P<0.05; **P<0.01. Abbreviations: C, control; DT, diaphragm training; SE, standard error. |
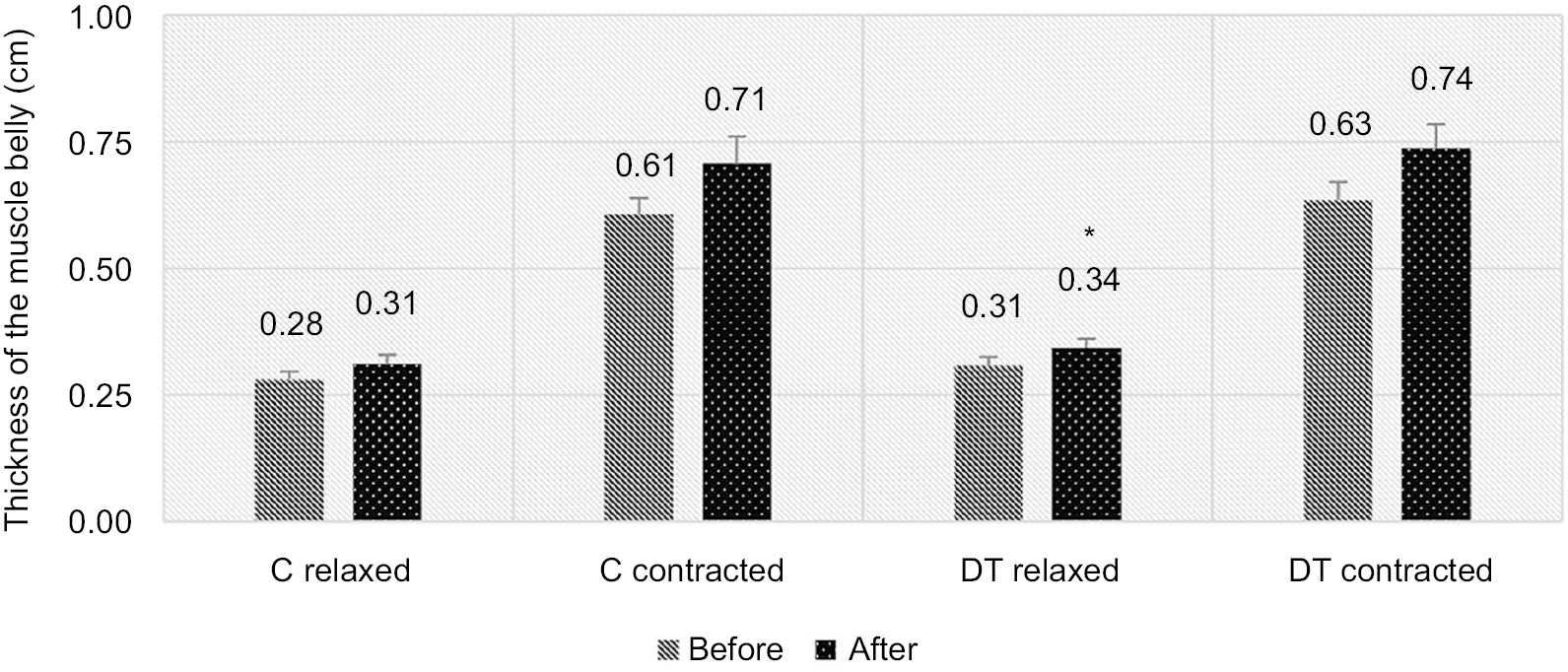 | Figure 4 Changes in the thickness of transversus abdominis muscle in supine position, in the relaxed and in the contracted states (mean ± SE). Note: *P<0.05. Abbreviations: C, control group; DT, diaphragm training group; SE, standard error. |
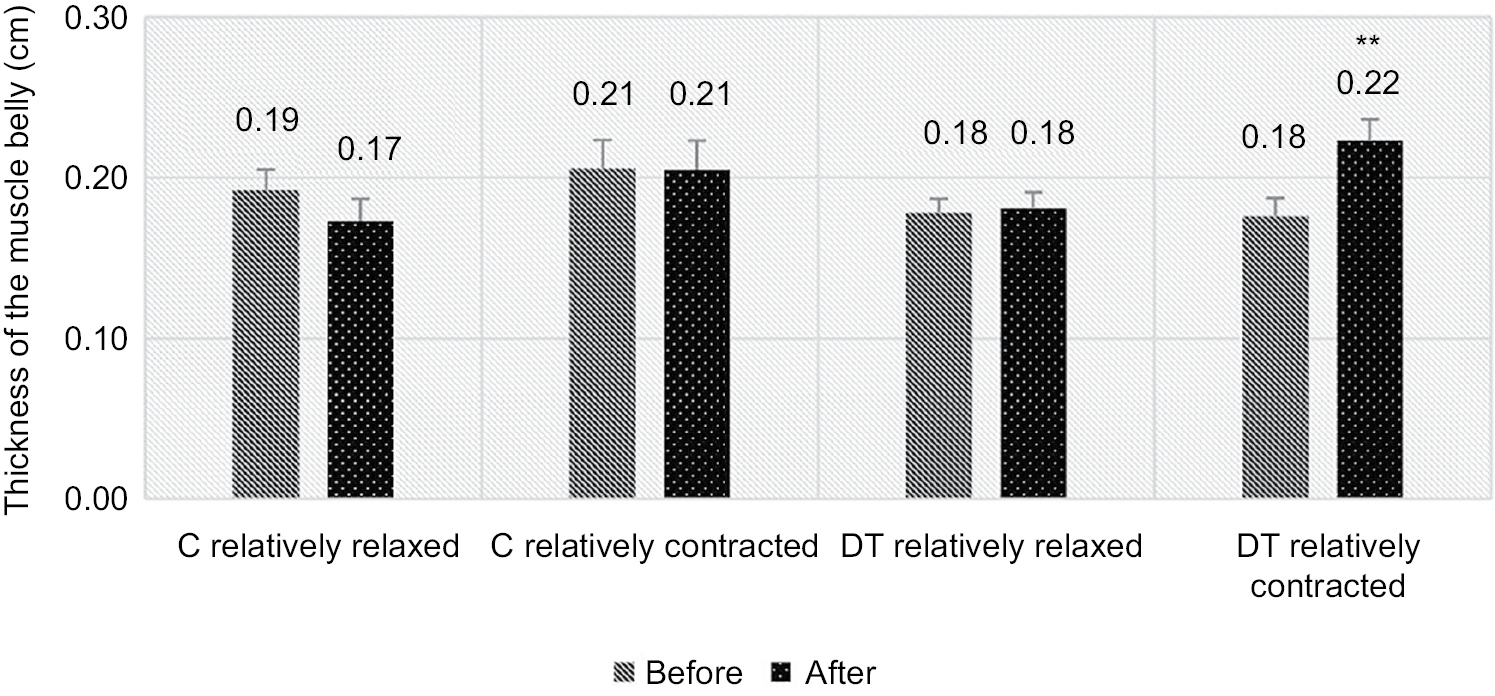
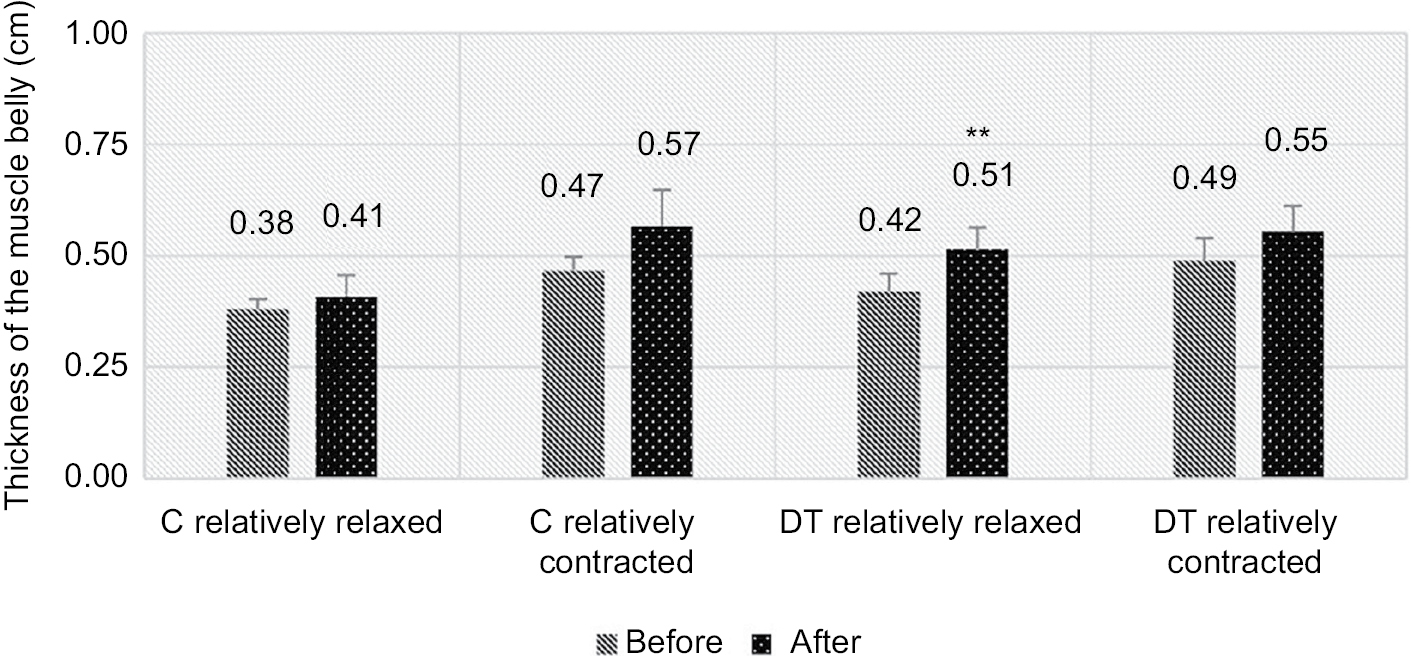 | Figure 5 Changes in the thickness of transversus abdominis muscle in a functional, sitting position in the relatively relaxed and in the relatively contracted state (mean ± SE). Note: **P<0.01. Abbreviations: C, control group; DT, diaphragm training group; SE, standard error. |
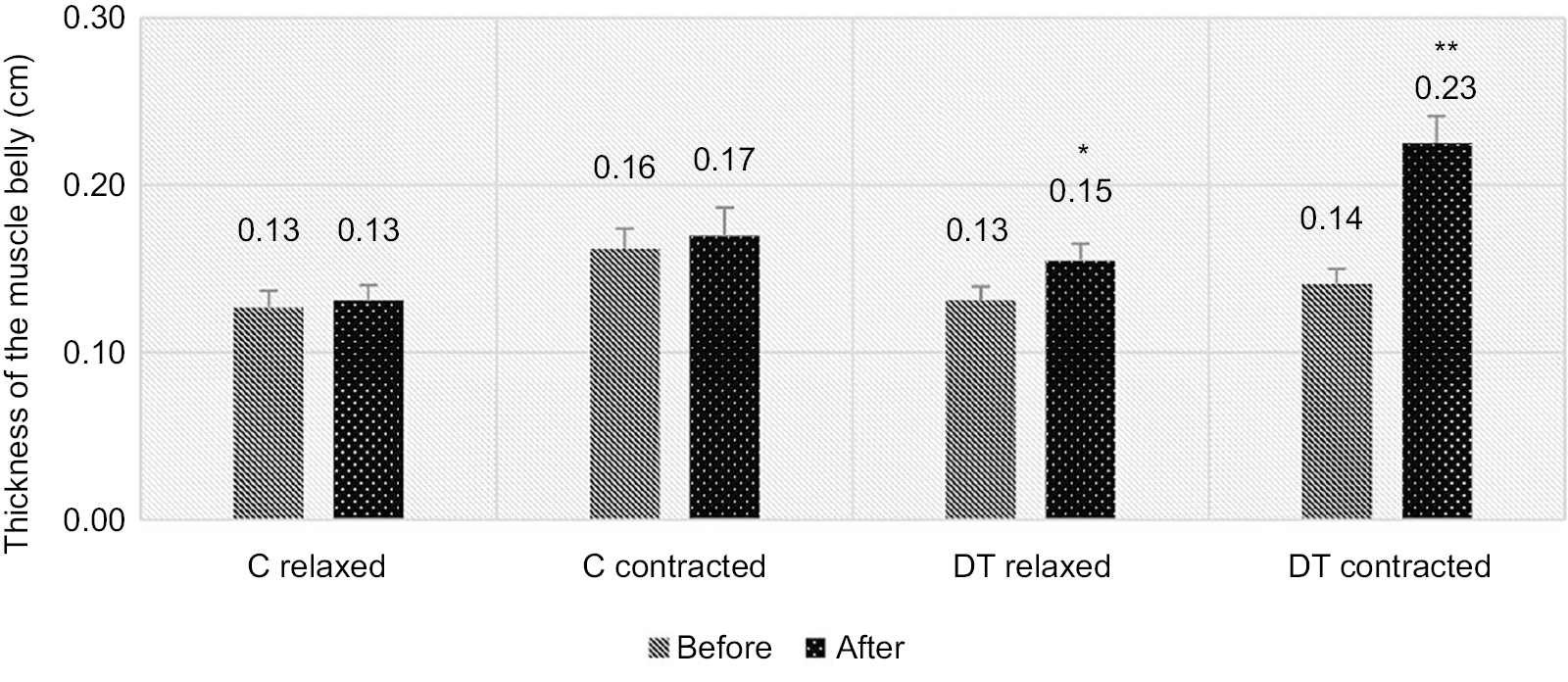 | Figure 6 Changes in the thickness of diaphragm muscle in supine position in the relaxed and in the contracted state (mean ± SE). Notes: *P<0.05; **P<0.01. Abbreviations: C, control group; DT, diaphragm training group; SE, standard error. |
 | Figure 7 Changes in the thickness of diaphragm muscle in the functional, sitting position in the relatively relaxed and in the relatively contracted state (mean ± SE). Note: **P<0.01. Abbreviations: C, control group; DT, diaphragm training group; SE, standard error. |
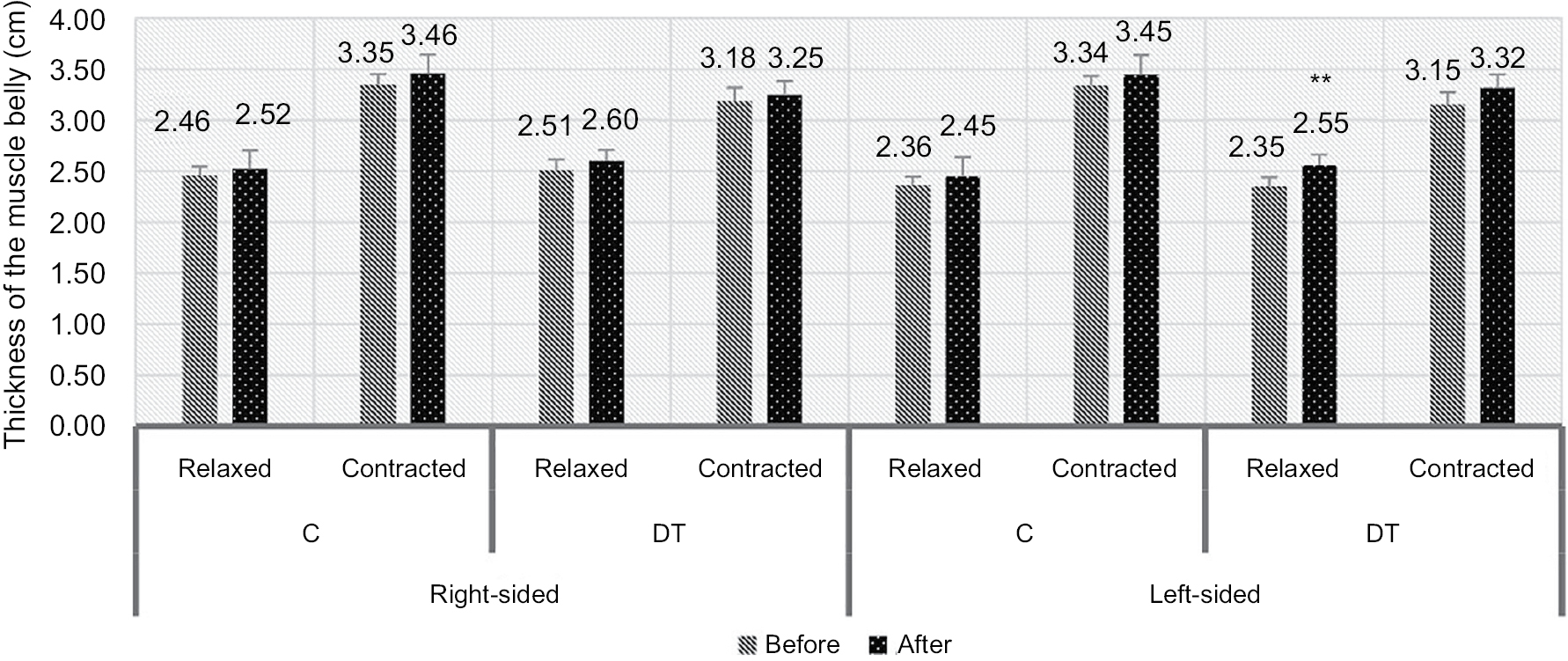 | Figure 8 Lumbar multifidus muscle thickness in the prone position (mean ± SE). Note: **P<0.01. Abbreviations: C, control group; DT, diaphragm training group; SE, standard error. |
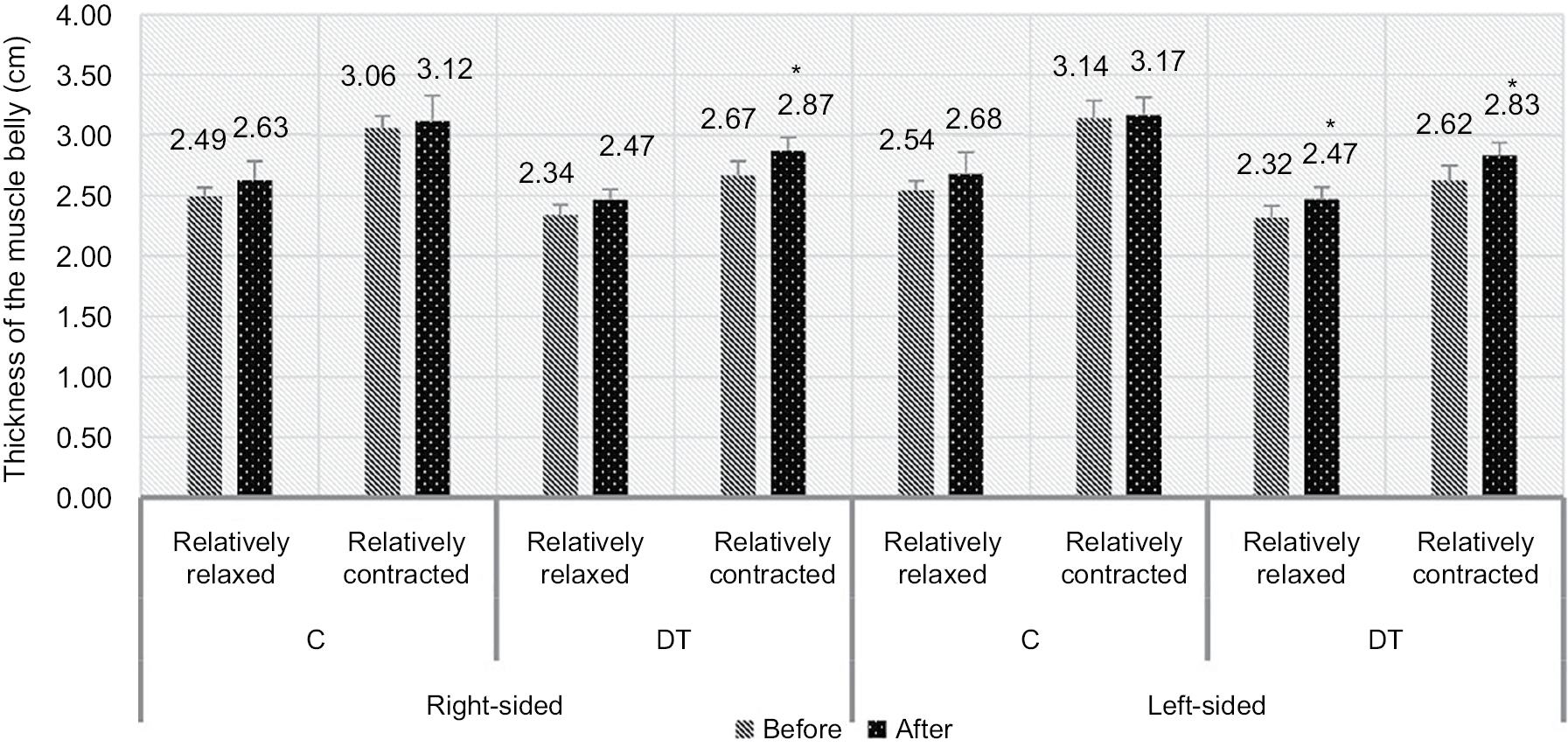 | Figure 9 Lumbar multifidus muscle thickness during sitting (mean ± SE). Note: *P<0.05. Abbreviations: C, control group; DT, diaphragm training group; SE, standard error. |
The results of the ultrasound assessment for the transversus abdominis muscle showed no significant differences in group C in supine position during relaxed and contracted state. In case of group DT, significant increase in thickness was found in the relaxed state (P<0.05), but there were no significant changes in the contracted state in supine position (Figure 4).
In sitting position, there were no differences between the before and after data in group C. On the contrary, in case of group DT, the thickness of transversus abdominis muscle increased significantly in the relatively relaxed state (P<0.01). However, there were no significant changes in the relatively contracted state (Figure 5).
With regard to the diaphragm muscle’s thickness, in supine position, there were no notable changes in case of group C in either state. On the other hand, for group DT, significant increase was found in the thickness of the muscle belly both in the relaxed (P<0.05) and in the contracted states (P<0.01) after the training (Figure 6).
For the functional sitting position, there were no notable changes in the relatively relaxed and the relatively contracted state in group C, with regard to the thickness of diaphragm. In contrast, group DT showed a significant increase in the relatively contracted state (P<0.01) but not in the relatively relaxed state (Figure 7).
In case of the relaxed and contracted states of the left- and right-sided lumbar multifidus, there were no substantial changes found in group C in prone position. For group DT, significant increase was only found in the left-sided muscle in the relaxed state (P<0.01). There were no notable changes either in the relaxed and or the contracted states of the right-sided multifidus or in the contracted state of the left-sided lumbar multifidus muscle (Figure 8).
In the sitting position, there were no significant differences between the before and after data in group C in any states of lumbar multifidus muscle. For group DT, significant increases were found in the relatively contracted states (P<0.05) in bilateral lumbar multifidus muscles as well as in the left-sided multifidus in the relatively relaxed state (P<0.05). Regarding the right-sided multifidus muscle in the relatively relaxed state, there were no notable changes in the thickness of the muscle in the sitting position with regard to group DT (Figure 9).
Discussion
The main finding of the study is that complex training completed with diaphragm training increased the thickness not only of the diaphragm but also of the other stabilizer muscles such as transversus abdominis and multifidus muscle. The significant increase in diaphragm muscle thickness in supine position indicates the effectiveness of diaphragm training22 in a position where the other stabilizers are relaxed. Both of the applied training methods resulted in significant improvement in pain. However, it was more significant in case of group C whose members participated only in the complex training. With regard to the thickness of the lumbar stabilizer muscles in group C, there were no significant changes in any of the muscles resulting from the 8-week-long intervention, which suggests that diaphragm strengthening training can provide extra benefits.
Regarding the intensity of pain, both the training methods resulted in significant improvement although it was more significant in group C. The members of the groups took part in the same complex training with the same exercises. However, the members of group DT faced a more difficult situation: they had to do the strengthening exercises parallel with the diaphragm strengthening training. Pain perception is highly subjective, which is influenced by several psychological and emotional factors.23,24 Intensive strengthening exercises taken for a short period of time are not always very effective in reducing pain intensity.25 Many factors (fear, structural abnormality, pain, posture reduction, etc) maintain the vicious cycle in CLBP; if intervention is capable of reducing one of the maintaining factors, the vicious cycle may be broken.26,27 Both the trainings decreased pain significantly and the complex training completed with diaphragm training increased the thickness of stabilizer muscles generating change in the condition of transversus abdominis, diaphragm, and lumbar multifidus muscles. Based on our results, it can be stated that pain perception seems to have been influenced positively by the interventions, so it can be a possible way to influence the vicious cycle underlying CLBP.
The exercises of our complex training program were the same in the two study groups. The training consisted of static and dynamic strengthening exercises for the trunk and hip muscles as well as proprioceptive training. All strengthening exercises were performed using external resistance (dumbbells, resistance bands, and medicine ball) or body weight. A double-blind, randomized controlled trial proved earlier that both motor control and general exercises increase the thickness of lumbar multifidus and transversus abdominis muscle significantly in the case of low back pain patients as a result of an 8-week-long training program.28 A previous study also showed that the thickness of diaphragm muscle increases as a consequence of a 4-week-long diaphragm training.22 Based on the abovementioned findings and considering our results, we can conclude that our complex training completed with a diaphragm strengthening training is a possible way to increase the thickness of transversus abdominis, diaphragm, and lumbar multifidus muscles.
In case of group DT, the thickness of transversus abdominis muscle increased significantly in the relaxed state (calm lying) but not in the contracted state when the subjects were asked to contract their abdominal muscles in supine position. We found similar muscle changes in the sitting position where the thickness of transversus abdominis muscle increased significantly in the relatively relaxed state when the sitting position was held, but there were no notable changes during the weightlifting task in the relatively contracted state. The increase of the thicknesses in relaxed and relatively relaxed states may have occurred due to the effect of our intervention.28 The unchanged thickness parameter of the contracted state in the supine position maybe due to the limitation of our measurement procedure: the participants were asked to contract their abdominal muscles voluntarily without lifting their head or shoulders from the bed. This kind of contraction seems to be more dependent on the compliance of the participants.29,30 Moreover, this movement was not practiced during our program; therefore, the quality of the performance may have been diverse30 and may not have been sufficient enough to show the effectiveness of the training. In addition, transversus abdominis muscle is a local stabilizer whose main function is more of stabilization and not implementation of movements,8,9 and in supine position, the demand for stabilization is minimal.31,32 There was no significant change in the thickness of transversus abdominis in the relatively contracted state either when the weightlifting was performed. It is well known that lifting tasks activate mainly the extensor group.16,33 Our results provide further evidence that lumbar multifidus has a more enhanced role in performing a weightlifting task, than transversus abdominis muscle. Therefore, the applied weightlifting task may not be the most appropriate postural task to show the enhanced stabilizer function of transversus abdominis muscle.
The increased thickness of diaphragm muscle in relaxed and in contracted states in the supine position may show the effectiveness of the diaphragm strengthening training.22 The results show that the only condition where we could not find any increase in the thickness of diaphragm after the training was the relatively relaxed state in sitting position. This finding may be explained by the neutral vertical position of the trunk which was held only against gravity in this case. This posture does not require more enhanced stabilization from diaphragm muscle.10,34 Significant increase occurred in the thickness of diaphragm muscle when the weightlifting was performed, in the relatively contracted state. Movements of the upper limb challenge the diaphragm muscle as a stabilizer muscle more contrary to the simple tasks to maintain vertical position.10 In a previous study, Hodges et al assessed the functioning of diaphragm during a rapid movement of the arm. Their findings proved that increased activity of diaphragm occurs during this motion.10 The diaphragm of low back pain patients has an altered postural function compared to healthy subjects when isometric flexion against resistance of the upper or lower limb was applied.35 In our training program, several resistance exercises were performed by the upper limb when the vertical posture of the trunk needed to be held, and the participants used the POWERbreathe device in parallel with upper limb exercises. Our results show that there is an increased thickness of diaphragm during the lifting task after training which may suggest that the role of diaphragm muscle has improved in maintaining trunk stability during upper limb activities as a result of the applied 8-week-long training. Our findings are in line with a previous study of Dülger et al36 They found that as a result of a stabilization exercise program, the thickness of diaphragm increased as well as the stability of the lumbar spine.36
Considering lumbar multifidus muscle in prone position, significant increase was found only in case of the left-sided one in the relaxed state. There were no significant changes in case of contracted states of the left-sided muscle or in both states of the right-sided multifidus. Like in case of transversus abdominis, the main function of lumbar multifidus is not implementation of movements but the segmental stabilization of the lumbar spine as it produces compression with minimal movement torque.33 This may be the reason for the unchanged thickness in the contracted state, when the patients were asked to lift their head and shoulders from the bed. The role of lumbar multifidus muscle in stabilization is highlighted in rotational movements and therefore in movements of the contralateral limb.37 Every participant was right-handed in our study which might have influenced the training effects: our results revealed that in prone position, the left-sided (contralateral to the dominant arm) muscle thickness improved significantly in the relaxed state. The resistance exercises were probably more effectively performed with the dominant (right-sided) arm.38 In sitting position, the thickness of both the left- and right-sided multifidus muscle increased in the relatively contracted state (during weightlifting) and the left-sided lumbar multifidus muscle thickness also increased in the relatively relaxed state as well (while holding the vertical position of the trunk). Contrary to the prone position when sitting, the postural demand is enhanced and lumbar multifidus muscle can act directly on the lumbar vertebral column producing the anti-flexion (extension) moment.37 During weightlifting (relatively contracted state), this anti-flexion moment of bilateral multifidus muscle is more important.33 The increased thickness possibly occurred as a result of our training method. The only unchanged thickness in sitting position was found in the right-sided (ipsilateral to the dominant arm) lumbar multifidus muscle in relatively relaxed state. The unchanged thickness may be explained by the influence of right-handedness on the training and/or on the testing procedure. In case of our testing procedure, one dumbbell was lifted with both the hands; therefore, it is possible that the dominant arm had a bigger contribution in the exercise.38 Further investigations using two dumbbells are needed to support this hypothesis.
The differences between groups DT and C in the change of the thickness of the stabilizer muscles indicate that diaphragm training has an extra advantage compared to a conventional complex training program. Further investigations are warranted to explore the mechanism behind the changes, but some possible assumptions can be made.
The effect of deep abdominal muscle exercises on respiratory function was assessed in a previous study.39 Deep abdominal muscles and diaphragm play an important role in maintaining and increasing the intra-abdominal pressure by their co-contraction.40,41 The finding of this research shows that enhanced diaphragmatic function achieved via deep abdominal muscle strengthening exercises did not only increase respiratory volume but also enhanced the stability of the lumbar spine through the co-contraction of transversus abdominis.39 Contrary to their above-mentioned training method, we have placed emphasis on the diaphragm muscle strengthening in our training program, but as a consequence, transversus abdominis muscle may be strengthened in this alternative, indirect way.
People with CLBP have a higher diaphragm position, a smaller diaphragm excursion, and greater diaphragm fatigability,35,42 which is compensated by increased lung volume to provide an adequate increase in intra-abdominal pressure.42 Diaphragm strengthening training is a viable method to enhance the excursion of the diaphragm and increase the mobility of the muscle.43,44 We assumed that a higher excursion of the diaphragm occurred due to the diaphragm strengthening training which further influenced the function of the diaphragm muscle during breathing and postural stabilization.19 Significant increases were found in the diaphragm thickness when the weightlifting task was performed in sitting position. The increased thickness during weightlifting suggests that the role of diaphragm muscle in maintaining trunk stability may have been improved.
Previous studies suggested that increase in the respiratory output causes an increased excursion of the body in space.45,46 Another previous study reported that normal inhalation is linked to the extension of the lumbar spine in standing posture.47 Significant changes in posture and significant enhancement occurs in the activation of erector spinae muscle when the inspiration effort increases.48 The fact that our training combined exercises in vertical positions with forced inhalation exercises can explain the training effects especially the increase in the thickness of lumbar multifidus muscle in sitting posture.
Limitations
A limitation of this study is that by using ultrasonography we could not discriminate between the increase of muscle thickness as result of the changes of the tone and activation pattern and muscle hypertrophy which occurred as a result of the strengthening training. Another limitation of this study is the presumption that the compliance of the subjects was on the same level but it could not be controlled by objective methods. To assess transversus abdominis muscle in contraction in supine position, the patients were asked to contract their abdominal muscles voluntarily. This exercise needs a more developed understanding of the movement; therefore, we could not be sure that everyone performed the contraction on the same level.29,30 This procedure would have been better if we had allowed the flexion of the trunk to a specified extent. In case of sitting positions, the subjects were asked to hold the neutral position of the trunk which was controlled by a physiotherapist but not with objective methods. Therefore, some inclination of the trunk may have happened during the ultrasound measurement procedure. For further studies, the vertical position should be controlled in a more objective manner.
Conclusion
In our randomized controlled study, the training effects of a complex training and a complex training completed with diaphragm training were examined. Based on our results, we suggest that the applied complex training completed with diaphragm strengthening training is an effective and viable way to increase the thickness of the stabilizer muscles of the lumbar spine such as transversus abdominis, diaphragm, and lumbar multifidus muscles. We can say that this training method is effective in reducing the severity of lumbar pain. However, complex training alone was more efficient taking the results of VAS into consideration. The results suggest that our complex training enhanced with diaphragm strengthening may be a viable therapeutic approach in the complex treatment of chronic nonspecific low back pain. Our findings clearly show that our intervention can have an influence on the diaphragm’s postural function during upper limb lifting tasks. The mechanisms behind the effects of diaphragm training need to be understood more clearly; therefore, additional investigations are necessary. We suggest a further consideration focusing on whether diaphragm training alone would be a new therapeutic approach for those who are not capable of performing conventional exercises.
Acknowledgment
Edit Nagy and Tamás Bender share senior authorship.
Disclosure
The authors report no conflicts of interest in this work.
References
Duthey B. Lower back pain; 2013. Available from: http://www.who.int/medicines/areas/priority_medicines/BP6_24LBP.pdf. Accessed November 9, 2017. | ||
Hoy D, March L, Brooks P, et al. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73(6):968–974. | ||
Deyo RA, Weinstein JN. Low back pain. N Engl J Med. 2001;344(5):363–370. | ||
Panjabi MM. Clinical spinal instability and low back pain. J Electromyogr Kinesiol. 2003;13(4):371–379. | ||
Fritz JM, Erhard RE, Hagen BF. Segmental Instability of the Lumbar Spine. Phys Ther. 1998;78(8):889–896. | ||
Panjabi MM. The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis. J Spinal Disord. 1992;5397(4):390–397 discussion. | ||
Hodges PW, Moseley GL. Pain and motor control of the lumbopelvic region: effect and possible mechanisms. J Electromyogr Kinesiol. 2003;13(4):361–370. | ||
Bruno P. The use of “stabilization exercises” to affect neuromuscular control in the lumbopelvic region: a narrative review. J Can Chiropr Assoc. 2014;58(2):119–130. | ||
Macintosh JE, Bogduk N, Gracovetsky S. The biomechanics of the thoracolumbar fascia. Clin Biomech. 1987;2(2):78–83. | ||
Hodges PW, Butler JE, Mckenzie DK, Gandevia SC. Contraction of the human diaphragm during rapid postural adjustments. J Physiol. 1997;505 (Pt 2):539–548. | ||
Hodges PW, Gandevia SC. Activation of the human diaphragm during a repetitive postural task. J Physiol. 2000;522(Pt 1):165–175. | ||
Kolar P, Sulc J, Kyncl M, et al. Stabilizing function of the diaphragm: dynamic MRI and synchronized spirometric assessment. J Appl Physiol. 2010;109(4):1064–1071. | ||
Ning X, Zhou J, Dai B, Jaridi M. The assessment of material handling strategies in dealing with sudden loading: the effects of load handling position on trunk biomechanics. Appl Ergon. 2014;45(6):1399–1405. | ||
Zhou J, Dai B, Ning X. The assessment of material handling strategies in dealing with sudden loading: influences of foot placement on trunk biomechanics. Ergonomics. 2013;56(10):1569–1576. | ||
Sweeney N, O’Sullivan C, Kelly G. Multifidus muscle size and percentage thickness changes among patients with unilateral chronic low back pain (CLBP) and healthy controls in prone and standing. Man Ther. 2014;19(5):433–439. | ||
Yates JW, Karwowski W. An electromyographic analysis of seated and standing lifting tasks. Ergonomics. 1992;35(7–8):889–898. | ||
Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368–2383. | ||
Ki C, Heo M, Kim HY, Kim EJ. The effects of forced breathing exercise on the lumbar stabilization in chronic low back pain patients. J Phys Ther Sci. 2016;28(12):3380–3383. | ||
Janssens L, Mcconnell AK, Pijnenburg M, et al. Inspiratory muscle training affects proprioceptive use and low back pain. Med Sci Sports Exerc. 2015;47(1):12–19. | ||
Huskisson EC. Measurement of pain. Lancet. 1974;304(7889):1127–1131. | ||
Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP. Arthritis Care Res. 2011;63(Suppl 11):S240–S252. | ||
Vasconcelos T, Hall A, Viana R. The influence of inspiratory muscle training on lung function in female basketball players - a randomized controlled trial. Porto Biomed J. 2017;2(3):86–89. | ||
Williamson A. Issues in clinical nursing Pain: A Review of Three Commonly Used Pain Rating Scales. Available from: https://onlinelibrary.wiley.com/doi/pdf/. Accessed September 15, 2018. | ||
Feuerstein M, Beattie P. Biobehavioral factors affecting pain and disability in low back pain: mechanisms and assessment. Phys Ther. 1995;75:267–280. | ||
Dellve L, Ahlstrom L, Jonsson A, et al. Myofeedback training and intensive muscular strength training to decrease pain and improve work ability among female workers on long-term sick leave with neck pain: a randomized controlled trial. Int Arch Occup Environ Health. 2011;84(3):335–346. | ||
Langevin HM, Sherman KJ. Pathophysiological model for chronic low back pain integrating connective tissue and nervous system mechanisms. Med Hypotheses. 2007;68(1):74–80. | ||
Bonica JJ. Management of myofascial pain syndromes in general practice. J Am Med Assoc. 1957;164(7):732. | ||
Akbari A, Khorashadizadeh S, Abdi G. The Effect of Motor Control Exercise versus General Exercise on Lumbar Local Stabilizing Muscles Thickness: Randomized Controlled Trial of Patients with Chronic Low Back Pain. Journal of Back and Musculoskeletal Rehabilitation. 2008;21(2):105–112. | ||
Lima PO de P, de Oliveira RR, de Moura Filho AG, Raposo MCF, Costa LOP, Laurentino GEC. Reproducibility of the pressure biofeedback unit in measuring transversus abdominis muscle activity in patients with chronic nonspecific low back pain. J Bodyw Mov Ther. 2012;16(2):251–257. | ||
Storheim K, Bø K, Pederstad O, Jahnsen R. Intra-tester reproducibility of pressure biofeedback in measurement of transversus abdominis function. Physiother Res Int. 2002;7(4):239–249. | ||
Rasouli O, Arab AM, Amiri M, Jaberzadeh S. Ultrasound measurement of deep abdominal muscle activity in sitting positions with different stability levels in subjects with and without chronic low back pain. Man Ther. 2011;16(4):388–393. | ||
Hodges PW. Is there a role for transversus abdominis in lumbo-pelvic stability? Man Ther. 1999;4(2):74–86. | ||
Moseley GL, Hodges PW, Gandevia SC. Deep and Superficial Fibers of the Lumbar Multifidus Muscle Are Differentially Active During Voluntary Arm Movements. Vol 27. Available from: https://www.bodyinmind.org/wp-content/uploads/Moseley-et-al-2002-Spine-DM-SM-LM-arm-movement.pdf. Accessed September 17, 2018. | ||
Kolar P, Neuwirth J, Sanda J, et al. Analysis of diaphragm movement during tidal breathing and during its activation while breath holding using MRI synchronized with spirometry. Physiol Res. 2009;58(3):383–392. | ||
Kolář P, Sulc J, Kyncl M, et al. Postural function of the diaphragm in persons with and without chronic low back pain. J Orthop Sports Phys Ther. 2012;42(4):352–362. | ||
Dülger E, Bilgin S, Bulut E, et al. The effect of stabilization exercises on diaphragm muscle thickness and movement in women with low back pain. J Back Musculoskelet Rehabil. 2018;31(2):323–329. | ||
Macintosh JE, Bogduk N. The biomechanics of the lumbar multifidus. Clin Biomech. 1986;1(4):205–213. | ||
Li KW, Wang CW, Yu R. Modeling of predictive muscular strength for sustained one-handed carrying task. Work. 2015;52(4):911–919. | ||
Kim E, Lee H. The effects of deep abdominal muscle strengthening exercises on respiratory function and lumbar stability. J Phys Ther Sci. 2013;25(6):663–665. | ||
Hodges P, Kaigle Holm A, Holm S. Intervertebral stiffness of the spine is increased by evoked contraction of transversus abdominis and the diaphragm. Spine VivoPorcineStudies, editor. Vol. 28(23). Phila Pa 1976; 2003:2594–2601. | ||
Cholewicki J, Ivancic PC, Radebold A. Can increased intra-abdominal pressure in humans be decoupled from trunk muscle co-contraction during steady state isometric exertions? Eur J Appl Physiol. 2002;87(2):127–133. | ||
Janssens L, Brumagne S, Mcconnell AK, Hermans G, Troosters T, Gayan-Ramirez G. Greater diaphragm fatigability in individuals with recurrent low back pain. Respir Physiol Neurobiol. 2013;188(2):119–123. | ||
Rezkallah SF, Abd El-Hady AA, Hamid A, Botros FF. Sonographic Response of Diaphragmatic Excursion to Threshold Inspiratory Muscle Trainer in Elderly. Vol 85; 2017. Available from: www.medicaljournalofcairouniversity.net. Accessed September 16, 2018. | ||
Haytham HM, Azza AE, E.S M. NEG. Response of Diaphragmatic Excursion to Inspiratory Muscle Trainer Post Thoracotomy. Int J Med Heal Sci. 2016;10(1):15–18. | ||
Caron O, Fontanari P, Cremieux J, Joulia F. Effects of ventilation on body sway during human standing. Neurosci Lett. 2004;366(1):6–9. | ||
Kuczyński M, Wieloch M. Effects of accelerated breathing on postural stability. Hum Mov. 2009;9(2):107–110. | ||
Lewit K. Relation of faulty respiration to posture, with clinical implications. J Am Osteopath Assoc. 1980;79(8):525–529. | ||
Hodges PW, Gurfinkel VS, Brumagne S, Smith TC, Cordo PC. Coexistence of stability and mobility in postural control: evidence from postural compensation for respiration. Exp Brain Res. 2002;144(3):293–302. | ||
Rankin G, Stokes M, Newham DJ. Abdominal muscle size and symmetry in normal subjects. Muscle Nerve. 2006;34(3):320–326. | ||
Harper CJ, Shahgholi L, Cieslak K, Hellyer NJ, Strommen JA, Boon AJ. Variability in diaphragm motion during normal breathing, assessed with B-mode ultrasound. J Orthop Sports Phys Ther. 2013;43(12):927–931. | ||
Kiesel KB, Uhl TL, Underwood FB, Rodd DW, Nitz AJ. Measurement of lumbar multifidus muscle contraction with rehabilitative ultrasound imaging. Man Ther. 2007;12(2):161–166. |
Supplementary material
Details of the complex training program
The complex training can be divided into three parts: warm-up, main part, and cool-down sections.
- Warm-up: The training started with a 10 minutes warm-up section. The warm-up consisted of breathing exercises and dynamic exercises for all joints and muscles in standing position.
- Main part: The training method was a circuit training with five sections and with 3 minutes of exercising in one section, altogether in 40 minutes duration. There were 1 minute breaks between the sections while the participants took their places at the next section.
i.Strengthening exercises of the hip muscles: combined static and dynamic strengthening of the hip muscles
ii.Balancing exercise: static balance exercises (holding a position) on an unstable training tool in vertical posture (standing, kneeling)
iii.Strengthening exercises of the extensor muscles of the trunk: combined static and dynamic strengthening of extensors using limb activities with dynamic resistance
iv.Strengthening exercise of the abdominal muscles: combined static and dynamic strengthening of abdominal muscles using limb activities with dynamic resistance
v.Balancing exercise: dynamic reactive balance exercises: walking on unstable surfaces.
- Cool down: The training ended with a cool-down section of 10 minutes duration. This part of the training consisted of light aerobic, stretching, and breathing exercises.
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.