Back to Journals » Patient Preference and Adherence » Volume 20
The Effect of Changes in Defecation Posture on Health-Related Quality of Life Among Elderly Habitual Squat-Toilet Users After Total Hip Arthroplasty for Femoral Neck Fracture
Authors Zhao Y, Guo D ![]() , Yan C, Dong Y, Li X
, Yan C, Dong Y, Li X ![]() , Zhang J
, Zhang J
Received 10 November 2025
Accepted for publication 8 January 2026
Published 17 January 2026 Volume 2026:20 575359
DOI https://doi.org/10.2147/PPA.S575359
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yue Zhao,1 Dongsheng Guo,2 Chen Yan,2 Yuefu Dong,2 Xin Li,2 Jian Zhang2
1Department of Nursing, Lianyungang Maternity and Child Health Hospital, Lianyungang, Jiangsu, People’s Republic of China; 2Department of Orthopedics, The Affiliated Lianyungang Hospital of Xuzhou Medical University / The First People’s Hospital of Lianyungang, Lianyungang, Jiangsu, People’s Republic of China
Correspondence: Xin Li, Department of Orthopedics, The Affiliated Lianyungang Hospital of Xuzhou Medical University / The First People’s Hospital of Lianyungang, Lianyungang, Jiangsu, People’s Republic of China, Email [email protected] Jian Zhang, Department of Orthopedics, The Affiliated Lianyungang Hospital of Xuzhou Medical University / The First People’s Hospital of Lianyungang, Lianyungang, Jiangsu, People’s Republic of China, Email [email protected]
Background: Elderly patients undergoing total hip arthroplasty (THA) for femoral neck fractures are commonly restricted from squatting postoperatively. In regions where squat toilets are widely used, older adults who are accustomed to squatting may be forced to transition to a sitting defecation posture, which can affect daily functioning and health-related quality of life (HRQoL), yet this culturally specific clinical issue remains insufficiently studied.
Methods: A total of 152 elderly patients with displaced intracapsular femoral neck fractures underwent primary cementless THA between January 2023 and July 2024. Defecation posture was evaluated using the 10-item Toilet Posture Score (TPS) preoperatively and at 1, 3, and 6 months after surgery. HRQoL was assessed with the EQ-5D-5L and EQ-VAS. Changes in TPS were examined across time points using repeated-measures ANOVA. Multivariable linear regression models were constructed to determine whether 6-month TPS improvement predicted 6-month HRQoL gains after adjustment for age, sex, body mass index, and Charlson Comorbidity Index.
Results: The mean age was 77.82 ± 7.11 years, and 72.4% were women. TPS decreased from 16.02 ± 2.37 preoperatively to 15.38 ± 2.61 at 1 month (P = 0.004), and further improved to 12.68 ± 2.49 and 11.22 ± 2.70 at 3 and 6 months (both P < 0.001). EQ-5D-5L increased from 0.61 ± 0.15 preoperatively to 0.82 ± 0.13 at 6 months (P < 0.001), and EQ-VAS increased from 55.10 ± 11.90 to 78.38 ± 12.31 (P < 0.001). Greater improvement in defecation posture independently predicted larger improvements in both EQ-5D-5L (B = − 0.037; 95% CI − 0.043 to − 0.032; P < 0.001) and EQ-VAS (B = − 1.319; 95% CI − 1.386 to − 1.252; P < 0.001) change scores at 6 months. Constipation requiring medical advice occurred in 36 patients (23.7%).
Conclusion: Elderly patients who are accustomed to squatting experience considerable restrictions in defecation posture after THA. The degree of postural improvement independently predicts HRQoL gains assessed by both EQ-5D-5L and EQ-VAS. Post-THA rehabilitation should include targeted toileting education and gradual posture retraining to facilitate a safe transition from squat toilets to sitting toilets while maintaining hip precautions.
Keywords: femoral neck fracture, total hip arthroplasty, toilet posture, quality of life, elderly
Introduction
Femoral neck fractures are common among the elderly and often lead to serious complications, including reduced mobility and increased mortality. For displaced fractures in older adults, total hip arthroplasty (THA) is generally preferred, offering better functional outcomes than hemiarthroplasty. Numerous studies have confirmed that THA significantly improves health-related quality of life (HRQoL) in patients with femoral neck fractures.1–4 Postoperative rehabilitation emphasizes early mobilization and dislocation prevention, with one critical precaution being the avoidance of hip flexion beyond 90 degrees—thereby prohibiting activities such as squatting.5–7 From a biomechanical perspective, deep squatting involves extreme hip flexion and altered spinopelvic motion, which can increase prosthetic impingement and reduce the functional safe zone of the acetabular component, thereby elevating the risk of dislocation.8
While this restriction is generally manageable in Western settings where sitting toilets are standard, it presents a substantial challenge in many Asian regions. In these areas, squat toilets are the cultural norm and are deeply ingrained in daily routines, particularly among older adults who have used them throughout their lives.9,10 A national survey of rural Chinese adults aged ≥55 years reported that 29.5% used indoor squatting toilets (vs 24.0% using indoor pedestal pans), and 42.1% still toileted outdoors, indicating that squat-type toileting remains common among older adults in these settings.11 This cultural discrepancy introduces a unique rehabilitation challenge: the forced transition from squatting to sitting defecation posture. Evidence from gastroenterology suggests that defecation posture can meaningfully influence anorectal mechanics and rectal sensory parameters, which may in turn affect evacuation efficiency and straining.12 For example, a forward-leaning “Thinker” posture has been reported to facilitate evacuation compared with standard sitting, and rectal sensory testing outcomes may differ across body positions including sitting and squatting.13 This provides a physiological rationale for constipation-related difficulties during the forced transition from squatting to sitting. Despite the potential impact of this transition on patients’ autonomy, bowel function, and psychological well-being, it has received little attention in the orthopedic literature. Recent studies have shown that constipation is highly prevalent among elderly patients following hip surgery, with rates exceeding 70% during hospitalization.14,15 This is often linked to reduced mobility, opioid use, and unfamiliar toileting environments. These findings highlight the need to consider bowel function as a relevant factor when evaluating the impact of toileting posture changes. Previous THA perioperative and rehabilitation literature has predominantly emphasized pain control and early mobilization with gait- and joint function–oriented outcomes, and commonly does not report toileting posture or squat-to-sit adaptation as a distinct functional domain.16–18 This reflects the outcome scope typically prioritized in prior protocols rather than a deficiency in study quality. To objectively assess toileting performance and posture adaptation, the Toilet Posture Score (TPS) has recently been developed as a simple, structured tool that quantifies patients’ ability to maintain defecation posture and level of dependence during toileting. Incorporating such a measure allows functional outcomes beyond mobility and pain to be captured in a standardized way.
This study aims to determine how changes in defecation posture, particularly the transition from squatting to sitting, influence postoperative quality of life following THA in elderly patients. By assessing defecation posture and HRQoL at different time points before and after surgery, the relationship between changes in defecation posture and HRQoL can be analysed. This study will help identify functional impairments that are easily overlooked during postoperative rehabilitation and provide a basis for developing more comprehensive and personalized rehabilitation guidance programs, thereby improving rehabilitation efficiency and overall patient satisfaction.
Methods
Study Design
This prospective cohort study was conducted at the First People’s Hospital of Lianyungang from January 2023 to July 2024, with ethical approval from the hospital’s Ethics Committee. All participants provided written informed consent, and procedures followed the Declaration of Helsinki. Patient privacy was protected, and postoperative pain was managed per standard protocols. The study adhered to STROBE guidelines.
Patient Selection
This study continuously enrolled patients who underwent surgical treatment during the study period. The inclusion criteria were as follows: (1) aged ≥ 65 years; (2) radiologically confirmed displaced intracapsular femoral neck fracture, classified as Garden type III or IV; (3) initial cementless THA performed via a standard posterolateral approach within 7 days of the injury; (4) good cognitive and communication abilities, able to understand the study content and voluntarily sign the informed consent form; (5) habitual use of squat toilets preoperatively, confirmed through patient interview at admission; and (6) first-time primary THA with no history of hip replacement on either side.
The exclusion criteria were as follows: (1) pathological fractures, such as those caused by tumours or severe osteoporosis accompanied by nontraumatic fractures; (2) cognitive impairment (Mini-Mental State Examination score < 24), unable to cooperate with relevant questionnaire assessments and follow-up; (3) a history of previous surgery on the same side of the hip joint; or (4) inability to complete at least 6 months of follow-up assessments due to severe medical conditions, limited mobility, living environment, or poor compliance.
Cementless THA was selected to standardize surgical technique and prosthesis type. Age ≥65 was chosen to capture a homogenous elderly cohort typically using squat toilets in our region.
The patient inclusion flow diagram is presented in Figure 1.
 |
Figure 1 Flow diagram of patient selection. |
Data Collection
Preoperative data were systematically collected at the time of patient enrolment to assess general health status and comorbidities. The demographic and clinical characteristics included age, sex, body mass index (BMI), and Charlson Comorbidity Index (CCI). The data were collected by trained research nurses who distributed questionnaires during outpatient visits or hospital stays. These nurses provided on-site guidance to ensure that patients understood the questionnaires. Postoperative follow-up data were obtained via outpatient assessments, telephone calls, or electronic questionnaires. All the data were double-entered to ensure accuracy. Follow-up assessments were conducted at 1, 3, and 6 months postoperatively. These assessments were mostly conducted during outpatient visits; for patients who were unable to visit the hospital, follow-up assessments were performed via telephone or video. Participants who could not be reached after at least three contact attempts were considered lost to follow-up, and their data at that time point were treated as missing.
Surgical Techniques and Postoperative Management
All patients underwent primary THA within 7 days after the fracture. The surgery was performed under general or combined spinal–epidural anaesthesia by orthopaedic physicians with extensive experience in hip replacement. A standardized posterolateral approach was uniformly used to implant standardized cementless acetabular and femoral stem prostheses, thus ensuring good prosthesis stability. During the operation, care was taken to protect the sciatic nerve and achieve strict haemostasis.
All patients received a standardized postoperative rehabilitation protocol. From postoperative day 1, patients performed a standardized bedside exercise program under therapist supervision and within hip precautions, typically 2–3 sessions per day. Each session included ankle pumps and quadriceps/gluteal isometric contractions (10–20 repetitions each) and gentle hip abduction within precautions (10 repetitions × 2 sets); sitting training was initiated for 10–15 minutes per bout, 2–3 times per day and progressed to 20–30 minutes per bout as tolerated. Within 48 hours postoperatively, partial weight-bearing exercises involving standing and short-distance walking (with the assistance of a walker) were initiated. For the first 12 weeks after surgery, there were strict restrictions regarding hip flexion beyond 90 degrees, adduction beyond the midline, and internal rotation movements to prevent prosthesis dislocation. Posterior precautions were lifted at 12 weeks, allowing gradual attempts at squatting under supervision.
Among these restrictions, prohibiting squatting during defecation was the core focus of education and behavioural intervention at this stage. Nursing staff and rehabilitation therapists provided patients with guidance regarding defecation posture after surgery; recommended the use of a sitting toilet or raised toilet seat device; and educated patients on proper sitting toilet techniques. Moreover, patients received professional rehabilitation assessments during hospitalization, and individualized home rehabilitation plans were developed to ensure gradual functional postoperative recovery and to prevent complications.
All patients received a standardized postoperative bowel regimen, including a high-fiber diet, adequate hydration, and early mobilization. Dietary guidance was provided once daily during hospitalization by nursing staff and reinforced with written home-care instructions at discharge. An osmotic laxative was routinely initiated according to our institutional protocol (lactulose oral solution, 15 mL twice daily, starting on postoperative day 1). If no bowel movement occurred within 48 hours, the regimen was escalated by adding a rectal micro-enema (glycerin enema, 10 mL per dose, as needed) while continuing the osmotic agent. Bowel activity was monitored daily during hospitalization.
Toilet Posture Score and Scoring Criteria
To evaluate toileting function, the TPS was developed through a structured process. First, an initial item pool was generated based on a targeted literature review and clinical experience relevant to toileting after THA. Second, an expert panel (n = 9) comprising orthopaedic surgeons (n = 3), rehabilitation therapists/physiotherapists (n = 3), and nursing specialists (n = 3) evaluated item relevance, clarity, and feasibility in older adults. Feedback was incorporated through two iterative rounds, including wording refinement, consolidation of overlapping items, and clarification of the three-level scoring anchors to improve scoring consistency. Third, the draft TPS was pilot-tested in a preliminary cohort of elderly patients after THA (n = 25) to assess comprehensibility and practicality during follow-up; minor modifications were made based on feedback, and the final 10-item TPS was confirmed. The scale demonstrated good content validity through expert review. Internal consistency was high (Cronbach’s alpha = 0.84), construct validity was supported by a moderate negative correlation with EQ-5D-5L (r = –0.41, P < 0.01), and responsiveness was confirmed by significant score changes over time (P < 0.001).
The TPS is a 10-item questionnaire, with each item scored on a three-point Likert scale from 0 to 2. Total scores range from 0 to 20, with higher scores indicating greater reliance on traditional squatting and poorer adaptation to sitting toilets; thus, a reduction in TPS over time reflects improved toileting adaptation. The full item list and scoring criteria are shown in Table 1. The TPS was administered preoperatively and at 1, 3, and 6 months postoperatively by trained assessors during outpatient visits or remote follow-up.
 |
Table 1 Toilet Posture Score (TPS) Items and Scoring Criteria |
Outcome Measures
HRQoL was evaluated using the EuroQol 5 Dimensions 5 Levels Questionnaire (EQ-5D-5L) and the EuroQol Visual Analogue Scale (EQ-VAS) preoperatively and at 1, 3, and 6 months postoperatively. In this study, changes in defecation posture, quantified using the 10-item TPS, were examined as a key predictor variable to assess their association with HRQoL outcomes.
The EQ-5D-5L includes five dimensions, namely, mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, each of which is scored with five levels.19 EQ-5D-5L utility scores range from 0 (equivalent to death) to 1 (perfect health), as per the national valuation algorithm. A previous study reports an MCID of 0.05–0.54 for the EQ-5D-5L in musculoskeletal populations, suggesting that the observed changes are clinically meaningful.20 The EQ-VAS is a visual analogue scale with scores ranging from 0 to 100. This scale evaluates patients’ self-assessment of their current overall health status, with higher scores indicating better quality of life.21
Sample Size Estimation
G*Power 3.1 was used to estimate the sample size. For TPS scores assessed across four time points, a repeated-measures ANOVA assuming a medium effect size (f = 0.25), an α level of 0.05, and a power of 0.80 required a minimum of 24 participants. To evaluate the predictive effect of TPS improvement on health-related quality-of-life outcomes using multiple linear regression with five predictors (medium effect size f2 = 0.15, α = 0.05, power = 0.80), a sample size of 92 participants was required. Considering potential attrition, missing data across follow-up, and the need to ensure stable estimates for multivariable analyses, a total of 152 patients were enrolled.
Adverse Events Monitoring
Postoperative adverse events were systematically monitored and recorded throughout the 6-month follow-up period. Data on complications such as hip dislocation, surgical-site infection, deep vein thrombosis (DVT), pulmonary embolism, periprosthetic fracture, and constipation requiring medical attention were collected through clinical assessments during outpatient visits, patient self-reports via telephone follow-up, and review of hospital records. All reported events were verified by the clinical research team and categorized according to standardized diagnostic criteria. Only events occurring within 6 months postoperatively were included in the analysis.
Statistical Analysis
All statistical analyses were performed using SPSS 27.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as the mean ± standard deviation (SD), and categorical variables are presented as frequencies and percentages. Normality of continuous variables was assessed using the Shapiro–Wilk test together with visual inspection of Q–Q plots; the main outcomes were considered approximately normally distributed, supporting the use of parametric summaries and models. Changes in TPS, EQ-5D-5L, and EQ-VAS over time were evaluated using repeated-measures ANOVA. Sphericity was assessed using Mauchly’s test; when sphericity was violated, the Greenhouse–Geisser correction was applied.
To evaluate whether improvement in defecation posture predicted improvements in HRQoL, multivariable linear regression models were constructed with 6-month changes in EQ-5D-5L and EQ-VAS as dependent variables and 6-month changes in TPS (ΔTPS = TPS_6mo − TPS_preop) as the main independent variable. Covariates included age, sex, BMI, and CCI. Unstandardized regression coefficients (B) with 95% confidence intervals (CIs) were reported. A two-sided P value <0.05 was considered statistically significant.
Results
Patient Characteristics
All 152 enrolled patients underwent THA. The mean age was 77.82 ± 7.11 years, 72.4% were female, the mean BMI was 24.60 ± 3.80 kg/m2, and the mean CCI score was 3.22 ± 1.27 (Table 2).
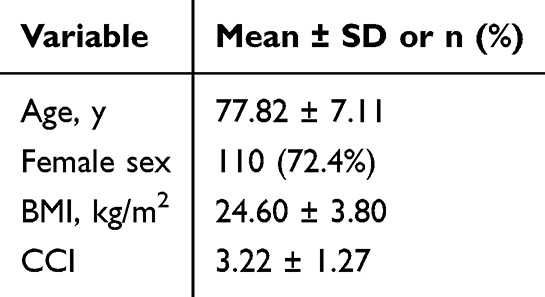 |
Table 2 Preoperative Demographic and Clinical Characteristics |
Changes in Toilet Posture and HRQoL
At 1 month postoperatively, the mean TPS declined from 16.02 ± 2.37 preoperatively to 15.38 ± 2.61, and this change was statistically significant (P = 0.004). Further improvements were observed at 3 months (12.68 ± 2.49; P < 0.001 vs preoperative) and 6 months (11.22 ± 2.70; P < 0.001 vs preoperative). Overall, TPS decreased by 4.80 points from baseline to 6 months, indicating progressive adaptation to sitting toileting over time (Table 3).
 |
Table 3 All Reported Improvements in EQ-5D-5L and EQ-VAS Scores Reflect Comparisons with Preoperative Values |
The EQ-5D-5L utility index increased from 0.61 ± 0.15 preoperatively to 0.70 ± 0.14 at 1 month (P < 0.001), 0.78 ± 0.13 at 3 months (P < 0.001), and 0.82 ± 0.13 at 6 months (P < 0.001). Similarly, EQ-VAS scores improved from 55.10 ± 11.90 preoperatively to 64.82 ± 13.79 at 1 month (P < 0.001), 72.52 ± 12.61 at 3 months (P < 0.001), and 78.38 ± 12.31 at 6 months (P < 0.001), demonstrating sustained gains in HRQoL throughout follow-up (Table 3).
Association Between Changes in the TPS and Improvements in HRQoL
In multivariable linear regression models adjusting for age, sex, BMI, and CCI, greater improvement in defecation posture was independently associated with larger improvements in HRQoL at 6 months. Specifically, each 1-point decrease in ΔTPS was associated with a 0.037 increase in the EQ-5D-5L change score (B = −0.037; 95% CI −0.043 to −0.032; P < 0.001) and a 1.319-point increase in the EQ-VAS change score (B = −1.319; 95% CI −1.386 to −1.252; P < 0.001). Higher CCI independently predicted smaller improvements in both the EQ-5D-5L change score (B = −0.014; 95% CI −0.024 to −0.004; P = 0.007) and the EQ-VAS change score (B = −1.092; 95% CI −1.213 to −0.971; P < 0.001) (Tables 4–5).
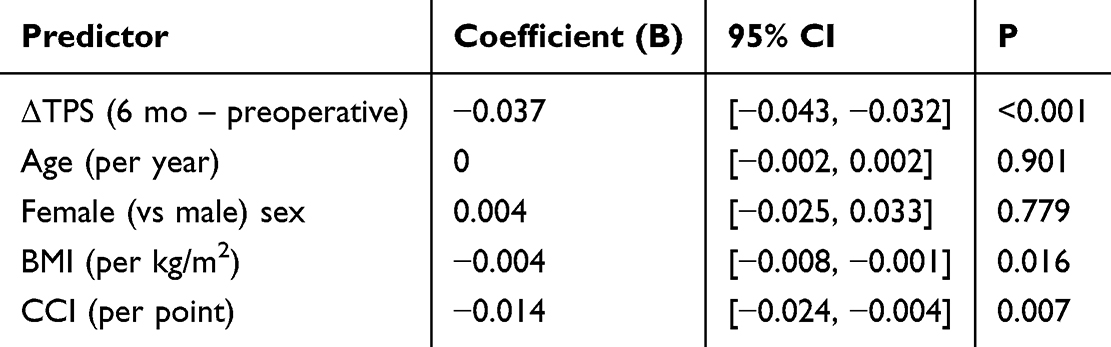 |
Table 4 Multivariable Linear Regression Predicting Changes in EQ-5D-5L Scores at 6 Months |
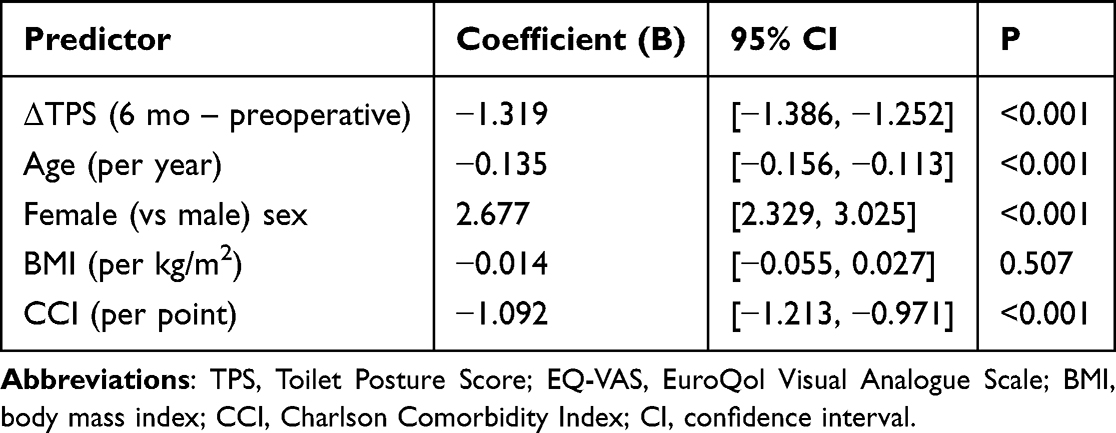 |
Table 5 Multivariable Linear Regression Predicting Changes in EQ-VAS Scores at 6 Months |
Adverse Events
Adverse events within 6 months are summarized in Table 6. No hip dislocations were observed. Problematic constipation (requiring medical advice) was reported in 36 patients (23.7%), which was more frequent than surgical-site infection, venous thromboembolism, or periprosthetic fracture. This incidence is lower than the >70% reported during acute hospitalization in previous hip fracture cohorts, likely because our definition captured clinically significant constipation over a 6-month period rather than any inpatient constipation episode.
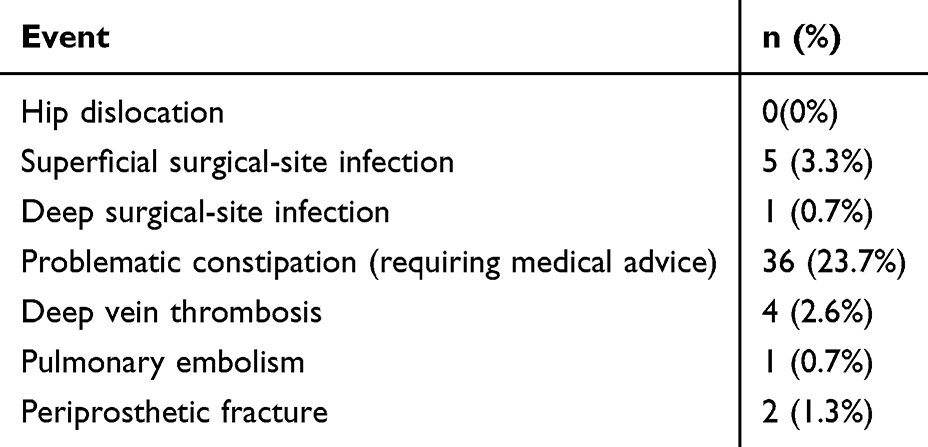 |
Table 6 Postoperative Adverse Events Within Six Months |
Discussion
This study examined how changes in defecation posture after THA affect quality of life in elderly patients with femoral neck fractures who were accustomed to squatting toilets. The results showed early postoperative difficulty maintaining squatting posture, followed by gradual improvement in defecation posture over time. Both EQ-5D-5L and EQ-VAS scores improved significantly. Notably, improvements in the TPS were independently associated with greater improvements in both EQ-5D-5L and EQ-VAS at 6 months. These findings highlight the importance of toileting function in postoperative recovery and support including toilet posture training in rehabilitation programs.
During the early phase after THA, TPS decreased modestly at 1 month, and this early reduction was already statistically significant, suggesting that patients began adapting to sitting toileting soon after surgery despite the limited magnitude of change. The main reasons for these challenges may include limited postoperative hip joint mobility, pain, unfamiliarity with using a sitting toilet, and concerns about postoperative dislocation.7,22,23 In this study, some patients were observed to attempt maintaining a posture similar to squatting or required assistance during toileting due to toilet seat instability or difficulty with transfers, which likely contributed to the limited improvement in TPS during the early postoperative period. Over time, the TPS significantly improved, indicating gradual restoration of defecation posture. This positive change can be attributed to the synergistic effects of multiple factors. First, the gradual relief of postoperative pain increases patients’ willingness and ability to engage in activities.24 Second, hip joint mobility and lower limb muscle strength gradually recover due to systematic rehabilitation training, thus enhancing the ability to perform toilet-related behaviours.25,26 Patients gradually developed toilet-related habits such as using sitting toilets or raised toilet stools during rehabilitation, overcoming psychological discomfort and fear of the unknown.
The results of this study revealed that elderly patients with femoral neck fractures who underwent THA experienced significant improvements in HRQoL, as scores on the EQ-5D-5L and EQ-VAS were markedly better after the surgery than preoperatively. This trend is consistent with the findings of previous studies, indicating that THA can effectively relieve pain and improve joint function, serving as an important method for increasing HRQoL among elderly patients.27–29 This finding suggests that the recovery of toilet posture function not only affects physical function but also affects patients’ overall perceived health. Furthermore, improving the TPS also alleviates psychological burden and anxiety by decreasing dependence on others, thereby promoting overall multidimensional health, as measured by the EQ-5D; these findings reflect the key role of defecation posture in postoperative functional rehabilitation.30,31 Although EQ-VAS is a single-item, subjective measure and may be influenced by factors beyond specific functional changes, the observed independent association suggests that toileting adaptation may also contribute to patients’ overall perceived health status.32,33
Previous studies have largely emphasized major functional domains after THA—such as walking ability, balance, and stair climbing—and therefore toileting posture or squat-to-sit adaptation is rarely assessed or reported as a distinct outcome.34–36 Our longitudinal findings extend this literature by demonstrating that toileting posture adaptation represents a meaningful, culturally relevant functional domain after THA and is independently associated with improvements in HRQoL.
While previous rehabilitation protocols after THA have focused largely on mobility, gait, and joint function, our results suggest that toileting posture should also be considered a key component of functional recovery—especially in populations accustomed to squatting. Given the independent association between improved TPS scores and better EQ-5D-5L and EQ-VAS outcomes, postoperative care should include structured support for toileting adaptation. This includes preoperative education about toileting restrictions, training in the use of sitting toilets or assistive devices, and gradual posture retraining. Examples of accessible aids include raised toilet seats, toilet safety frames or grab bars to facilitate safe transfers, and a stable low footstool to elevate the feet and enable a forward-leaning sitting posture, which may partially reproduce the defecatory mechanics of squatting while respecting hip precautions. By integrating toilet posture transition into rehabilitation programs, clinicians can better support patients’ independence, reduce toileting-related distress, and enhance overall quality of life following surgery.
This study has several limitations. First, this was a single-centre observational study, and future multicentre studies are needed to assess generalizability. Second, the follow-up period was limited to 6 months, which captures early postoperative recovery, and longer follow-up is warranted to evaluate the durability of toileting adaptation and HRQoL changes. Third, although 152 patients were included, the sample size may limit precision and increase the risk of type II error, particularly for analyses involving EQ-VAS, and larger cohorts are needed for confirmation. Finally, given the observational design, causality cannot be inferred for the association between TPS improvement and HRQoL. Residual confounding and reverse causality are possible. Unmeasured factors such as caregiver support intensity and the home toileting environment or renovation status may influence both toileting adaptation and quality of life and may lead to an overestimation of the predictive effect.
Conclusion
This study revealed that elderly patients with femoral neck fractures who habitually used squat toilets before surgery experienced significant limitations in defecation posture after THA but exhibited gradual postoperative improvements. The degree of improvement in defecation posture independently predicted improvements in HRQoL assessed by both EQ-5D-5L and EQ-VAS. These results highlight that the recovery of toilet ability not only affects self-care ability but is also important for improving postoperative HRQoL. These findings highlight the need for rehabilitation programs to address toilet behavior transitions through preoperative education, practical training, and individualized support. Future research should explore how these interventions can be adapted across different cultural and healthcare settings, to evaluate broader applicability. Larger, multicentre studies with longer follow-up are also needed to confirm long-term outcomes.
Ethics Approval and Informed Consent
This study was reviewed and approved by the Research Ethics Committee of the First People’s Hospital of Lianyungang (No. LW-20251225001). All procedures involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Written informed consent was obtained from all individual participants included in the study.
Acknowledgments
We would like to thank all of the doctors who participated in this study for their cooperation.
Funding
This research was supported by the Medical Technology Support Program of the First People’s Hospital of Lianyungang (YK202306) and the Key Research and Development Program of the First People’s Hospital of Lianyungang (No. ZG004).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Su Y, Li R, Ren X, et al. The health-related quality of life for hemiarthroplasty and total hip arthroplasty in the elderly: a meta-analysis. Front Med. 2023;10:1022584. doi:10.3389/fmed.2023.1022584
2. Rogmark C, Leonardsson O. Hip arthroplasty for the treatment of displaced fractures of the femoral neck in elderly patients. Bone Joint J. 2016;98-B(3):291–10. doi:10.1302/0301-620X.98B3.36515
3. Bartels S, Kristensen TB, Gjertsen JE, et al. Total hip arthroplasty leads to better results after low-energy displaced femoral neck fracture in patients aged 55 to 70 years: a randomized controlled multicenter trial comparing internal fixation and total hip arthroplasty. J Bone Joint Surg. 2022;104(15):1341–1351. doi:10.2106/JBJS.21.01411
4. Bartels S, Gjertsen JE, Frihagen F, Rogmark C, Utvåg SE. High failure rate after internal fixation and beneficial outcome after arthroplasty in treatment of displaced femoral neck fractures in patients between 55 and 70 years: an observational study of 2,713 patients reported to the Norwegian Hip Fracture Register. Acta Orthopaedica. 2018;89(1):53–58. doi:10.1080/17453674.2017.1376514
5. Kostewicz M, Szczęsny G, Tomaszewski W, Małdyk P. Narrative review of the mechanism of hip prosthesis dislocation and methods to reduce the risk of dislocation. Med Sci Monit. 2022;28. doi:10.12659/MSM.935665
6. Harada S, Hamai S, Gondo H, Higaki H, Ikebe S, Nakashima Y. Squatting after total hip arthroplasty: patient-reported outcomes and in vivo three-dimensional kinematic study. J Arthroplasty. 2022;37(4):734–741. doi:10.1016/j.arth.2021.12.028
7. Kim Y, Vergari C, Shimizu Y, Tokuyasu H, Takemoto M. The impact of hip mobility on lumbar and pelvic mobility before and after total hip arthroplasty. JCM. 2022;12(1):331. doi:10.3390/jcm12010331
8. McKnight BM, Trasolini NA, Dorr LD. Spinopelvic motion and impingement in total hip arthroplasty. J Arthroplasty. 2019;34(7S):S53–S56. doi:10.1016/j.arth.2019.01.033
9. Chen YL, Sari RK, Liao YH, Lin WC. Optimal span between feet of public squat toilet based on anthropometric data and squatting stability assessment. Healthcare. 2021;9(1):42. doi:10.3390/healthcare9010042
10. Buldukoğlu OÇ, Öcal S, Atar GE, Harmandar FA, Çekin AH. Sit or squat? Toilet type is a determinant of diverticulosis development. Turk J Gastroenterol. 2024;35(6):475–480. doi:10.5152/tjg.2024.23652
11. Liu C, Fong JH, Hoh JWT, et al. Bathing and toileting difficulties of older adults in rural China: the role of environment. BMC Geriatr. 2020;20(1):533. doi:10.1186/s12877-020-01919-8
12. Xiao CF, Li YF, Sun YY, et al. Influence of the examination position and distension medium on the rectal sensory test in patients with functional constipation. BMC Gastroenterol. 2024;24(1):238. doi:10.1186/s12876-024-03309-5
13. Takano S, Sands DR. Influence of body posture on defecation: a prospective study of “The Thinker” position. Tech Coloproctol. 2016;20(2):117–121. doi:10.1007/s10151-015-1402-6
14. Celik B, Bilik Ö. Postoperative constipation incidence and effects of selected risk factors on constipation development in elderly patients with hip fracture. Orthop Nurs. 2022;41(6):397–405. doi:10.1097/NOR.0000000000000896
15. Görler H, Yılmaz FT, Bekmez F. A common complication in orthopedic patients: postoperative constipation and related risk factors. J PeriAnesthesia Nurs. 2023;38(5):e15–e20. doi:10.1016/j.jopan.2023.05.004
16. Anger M, Valovska T, Beloeil H, et al. PROSPECT guideline for total hip arthroplasty: a systematic review and procedure‐specific postoperative pain management recommendations. Anaesthesia. 2021;76(8):1082–1097. doi:10.1111/anae.15498
17. Zachodnik J, Geisler A. Short-term and long-term pain after total hip arthroplasty: a prospective cohort study. Pain Manage Nurs. 2022;23(2):225–230. doi:10.1016/j.pmn.2021.04.004
18. Frassanito L, Vergari A, Nestorini R, et al. Enhanced recovery after surgery (ERAS) in hip and knee replacement surgery: description of a multidisciplinary program to improve management of the patients undergoing major orthopedic surgery. Musculoskelet Surg. 2020;104(1):87–92. doi:10.1007/s12306-019-00603-4
19. Feng YS, Kohlmann T, Janssen MF, Buchholz I. Psychometric properties of the EQ-5D-5L: a systematic review of the literature. Qual Life Res. 2021;30(3):647–673. doi:10.1007/s11136-020-02688-y
20. Clement ND, Afzal I, Peacock CJH, et al. Mapping analysis to predict the associated EuroQol five-dimension three-level utility values from the Oxford Knee Score: a prediction and validation study. Bone Joint Open. 2022;3(7):573–581. doi:10.1302/2633-1462.37.BJO-2022-0054.R1
21. Chuang LH, Kind P, Kohlmann T, Feng YS. Exploring the origin and conceptual framework of the EQ VAS. Qual Life Res. 2025;34:2163–2173. doi:10.1007/s11136-025-03947-6
22. Reisinger L, Cozowicz C, Poeran J, et al. Trends in comorbidities and complications among patients undergoing elective total hip and knee arthroplasty in the USA. Anaesthesia. 2025;80(5):543–550. doi:10.1111/anae.16529
23. Shinonaga A, Matsumoto H, Uekawa M, Kuramoto A, Mitani S, Hagino H. Relationship between preoperative Hip range of motion and anxiety about dislocation after total hip arthroplasty. J Joint Surg Res. 2023;1(1):152–157. doi:10.1016/j.jjoisr.2023.07.001
24. Sergooris A, Verbrugghe J, Bonnechère B, et al. Inter-individual differences in early post-operative pain, cognitions, and emotions after total hip arthroplasty: a longitudinal cohort study. Clin Rehabil. 2025:2692155251333537. doi:10.1177/02692155251333537
25. Meng Y, Deng B, Liang X, et al. Effectiveness of self-efficacy-enhancing interventions on rehabilitation following total Hip replacement: a randomized controlled trial with six-month follow-up. J Orthop Surg Res. 2022;17(1):225. doi:10.1186/s13018-022-03116-2
26. Pollet J, Pullara R, Bianchi LNC, Falso MV, Gobbo M, Buraschi R. Gait improvements in the early post-surgery rehabilitation phase in subjects receiving a total knee or hip arthroplasty: a prospective study. Gait Posture. 2025;120:25–33. doi:10.1016/j.gaitpost.2025.03.024
27. Ayers DC, Yousef M, Zheng H, Yang W, Franklin PD. Do patient outcomes vary by patient age following primary total hip arthroplasty? J Arthroplasty. 2022;37(7):S510–S516. doi:10.1016/j.arth.2022.03.032
28. Li F, Zhu L, Geng Y, Wang G. Effect of hip replacement surgery on clinical efficacy, VAS score and Harris hip score in patients with femoral head necrosis. Am J Transl Res. 2021;13(4):3851–3855.
29. Patel I, Nham F, Zalikha AK, El-Othmani MM. Epidemiology of total hip arthroplasty: demographics, comorbidities and outcomes. Arthroplasty. 2023;5(1):2. doi:10.1186/s42836-022-00156-1
30. Assmann SL, Keszthelyi D, Breukink SO, Kimman ML. Living with faecal incontinence: a qualitative investigation of patient experiences and preferred outcomes through semi-structured interviews. Qual Life Res. 2024;33(11):3121–3129. doi:10.1007/s11136-024-03756-3
31. Bischof AY, Steinbeck V, Kuklinski D, et al. What is the association between gender and self-perceived health status when controlling for disease-specific conditions? A retrospective data analysis of pre- and post-operative EQ-5D-5L differences in total hip and knee arthroplasty. BMC Musculoskelet Disord. 2023;24(1):914. doi:10.1186/s12891-023-07026-0
32. Cheng LJ, Tan RLY, Luo N. Measurement properties of the EQ VAS around the globe: a systematic review and meta-regression analysis. Value Health. 2021;24(8):1223–1233. doi:10.1016/j.jval.2021.02.003
33. Lin DY, Cheok TS, Samson AJ, et al. A longitudinal validation of the EQ-5D-5L and EQ-VAS stand-alone component utilising the Oxford Hip Score in the Australian hip arthroplasty population. J Patient Rep Outcomes. 2022;6(1):71. doi:10.1186/s41687-022-00482-7
34. Abd-Eltawab AE, Elsherbini DMA, El Nashar EM, et al. Bilateral hip stability variation in the functional ambulation and kinetic parameters after total hip arthroplasty during leveled walking. Front Bioeng Biotechnol. 2024;12:1415645. doi:10.3389/fbioe.2024.1415645
35. Kim Y, Kim SY, Shim SR, Hyun JK. Predictive factors for gait recovery in patients undergoing total hip arthroplasty: a propensity score weighting analysis. JCM. 2025;14(6):1979. doi:10.3390/jcm14061979
36. Rivera RJ, Karasavvidis T, Pagan C, et al. Functional assessment in patients undergoing total Hip arthroplasty: a systematic review of the literature. Bone Joint J. 2024;106-B(8):764–774. doi:10.1302/0301-620X.106B8.BJJ-2024-0142.R1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Continuous Fascia Iliaca Compartment Block on Early Quality of Recovery After Total Hip Arthroplasty in Elderly Patients: A Randomized Controlled Trial
Gao Y, Li H, Hu H, Xu Y, Zhou J, Liu Y
Journal of Pain Research 2022, 15:1837-1844
Published Date: 28 June 2022
Changes in Anxiety and Depression After THA in Patients with Ankylosing Spondylitis and the Affecting Factors
Qian H, Wang X, Wang P, Zhang G, Liu J, Dang X, Guo J, Liu R
Therapeutics and Clinical Risk Management 2023, 19:675-684
Published Date: 15 August 2023
Use of Oral Celecoxib Preoperatively Reduces Risk of Delirium and Favors Functional Recovery in Elderly Patients with Femoral Neck Fracture: A Propensity Score-Matched Analysis
Ju M, Han X, He L, Jiang J, Wang M, Lin W, Liu Y
Journal of Pain Research 2025, 18:709-717
Published Date: 15 February 2025
Effect of Opioid-Free Anesthesia on the Quality of Early Recovery After Total Hip Arthroplasty in Elderly Patients (Aged 65-80 Years) as Assessed by the QoR-15 Score: A Randomized Controlled Trial
Su Y, Qin Z, Li X, Zhang X, Tong F, Wu L, Kong M
Drug Design, Development and Therapy 2025, 19:9127-9136
Published Date: 7 October 2025
Asthma in Individuals Over 60 Years: A Comparative Analysis Across Age Subgroups
Miodońska M, Bożek A, Urbaniec E, Sadowska D, Mitka A, Foks-Ciekalska A, Mućka S, Kwaśniak A, Zalejska-Fiolka J, Nittner-Marszalska M
Journal of Asthma and Allergy 2026, 19:561913
Published Date: 31 January 2026