Back to Journals » Journal of Asthma and Allergy » Volume 19
Asthma in Individuals Over 60 Years: A Comparative Analysis Across Age Subgroups
Authors Miodońska M ![]() , Bożek A
, Bożek A ![]() , Urbaniec E, Sadowska D, Mitka A, Foks-Ciekalska A, Mućka S, Kwaśniak A, Zalejska-Fiolka J, Nittner-Marszalska M
, Urbaniec E, Sadowska D, Mitka A, Foks-Ciekalska A, Mućka S, Kwaśniak A, Zalejska-Fiolka J, Nittner-Marszalska M
Received 9 September 2025
Accepted for publication 10 December 2025
Published 31 January 2026 Volume 2026:19 561913
DOI https://doi.org/10.2147/JAA.S561913
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Martyna Miodońska,1 Andrzej Bożek,1 Ewa Urbaniec,2 Dominika Sadowska,1 Aleksandra Mitka,1 Aleksandra Foks-Ciekalska,1 Szymon Mućka,1 Anna Kwaśniak,1 Jolanta Zalejska-Fiolka,3 Marita Nittner-Marszalska4
1Clinical Department of Internal Diseases, Dermatology and Allergology, Medical University of Silesia in Katowice, Zabrze, Poland; 2Medical Center of Allergology and Laryngology, Łaziska Górne, Poland; 3Department of Biochemistry, Faculty of Medical Sciences in Zabrze, Medical University of Silesia in Katowice, Zabrze, Poland; 4Department of Internal Medicine, Pneumology and Allergology, Wroclaw Medical University, Wroclaw, Poland
Correspondence: Martyna Miodońska, Clinical Department of Internal Diseases, Dermatology and Allergology, Medical University of Silesia in Katowice, ul. Marii Skłodowskiej-Curie 10, Zabrze, 41-800, Poland, Email [email protected]
Purpose: Asthma is often not adequately treated in individuals over 60 years of age due to atypical symptom presentation, comorbidities that overlap with asthma symptoms, and difficulties with diagnostic testing. The aim of this study was to evaluate asthma control, its phenotypes, accompanying comorbidities and quality of life, as well as treatment patterns, in patients aged 60 years and older. The assessment also covered asthma treatment and control in specific age subgroups.
Patients and Methods: A multicenter, cross sectional study of 345 asthma patients over 60 years of age and 410 matched controls without obstructive lung disease was conducted. Spirometry, Forced Oscillation Technique (FOT) assessment, bronchodilator reversibility test, and patient-reported outcome data, including Asthma Control Test (ACT), Asthma Quality of Life Questionnaire (AQLQ), and 36-Item Short Form Survey (SF-36) data were analyzed.
Results: Severe asthma was present in 25% (n=87) of the study population. A total of 48% (n= 165) of all asthma patients presented the T2 phenotype. The FOT proved useful where spirometry was limited. The asthma patients had significantly higher rates of depression (p=0.02), cognitive decline (p=0.02), and multimorbidity (p=0.01) than the non-asthma patients did. The quality-of-life score (AQLQ) was consistently lower in the asthma group: 3.78 ± 0.91 (median ± interquartile range) vs 4.29 ± 1.81 in non-asthma group (p=0.01). In the analysis of subgroups, older patients over 80 years had significantly poorer asthma control, and reduced quality of life in SF-36 questionnaire (55.521 score in younger vs 46.991 in older, for p=0.01).
Conclusion: Asthma in older age is often associated with other comorbidities, which can have a significant impact on a person’s quality of life and general health. Patients are often undertreated, which results in poorer asthma control, particularly among the oldest patients.
Keywords: elderly, late-onset asthma, spirometry, FOT, asthma phenotypes, quality of life
Introduction
Bronchial asthma is a chronic inflammatory disease of the airways that is caused by interactions among different cells, cellular elements and cytokines.1 Chronic inflammation is associated with bronchial hyperresponsiveness and leads to bronchial remodelling. These processes result in recurrent symptoms of varying severity, such as wheezing, shortness of breath, chest tightness and cough. The described symptoms often occur at night, in the morning or after exercise and resolve spontaneously or with treatment.1
While these symptoms, alongside relevant laboratory test results, can easily lead doctors to a correct diagnosis in younger patients, a final diagnosis can sometimes be problematic in people over 60 years of age. It is believed that the number of asthma patients over 60 years of age is underestimated.2–4 Owing to the prevalence of these symptoms in many other age-related diseases, asthma is not usually the first condition a doctor considers. In 2021, 7.2% of adults aged 60–65 years and older in the United States (US) had a current diagnosis of asthma (2.3). Among the European Union (EU) population, the prevalence of asthma in people aged 65 and older varies from 1.8% to 10.9% across different countries. In 2022, the highest and lowest prevalence rates of self-reported asthma were reported in the United Kingdom (UK) (17.6%) and Bosnia and Herzegovina (1.3%), respectively.5,6
There are several reasons why asthma can be difficult to diagnose and treat in older patients. Elderly patients may underreport their symptoms, be misdiagnosed with chronic obstructive pulmonary disease (COPD) or have congestive heart failure, which can accompany and mimic asthma symptoms.4,7,8 In many cases, asthma that recurs in older patients after being present in childhood, adolescence or adulthood is misclassified as other diseases. When a differential diagnosis is made, it is important to consider late-onset asthma (LOA), which is characterized by a sudden onset and rapid decline in lung function.9 Notably, phenotyping asthma into T2 and low-T2 phenotypes is rarely carried out in older patients.10,11 Furthermore, allergies are often underdiagnosed, resulting in allergic asthma in a significant proportion of patients.12
Underdiagnosis of asthma can lead to inadequate treatment, which is a significant problem in this patient group. It is particularly important to be able to identify asthma in elderly individuals with multiple chronic conditions who are undergoing multiple drug therapies.4,12 Failure to treat all comorbidities comprehensively leads to treatment failure and poor quality of life.
Due to the ageing process and progressive multimorbidity, it appears that the group of patients over 60 years of age with asthma may not be homogeneous. Currently, there is no assessment of possible differences in the clinical course of asthma in subgroups aged 60–70, 70–80, and over 80. From a clinical medicine perspective, this is of great importance in the personalized treatment of the oldest patients with asthma.
This observational study aimed to characterize and phenotype a population of individuals over 60 years of age with confirmed asthma undergoing guided treatment. A secondary objective was to compare the progression of asthma in the following age groups: 60–70, 71–80, and over 80.
Materials and Methods
Study Design
This observational, multicenter, prospective study examined a population of people over 60 years of age who had been diagnosed and treated at allergy, geriatric and pulmonology outpatient clinics in southern Poland.
Patients
Participants were selected from a medical database based on the following International Classification of Diseases, Tenth Revision (ICD-10) codes: J45, J45.1, J45.8 and J45.13, from five centers.
Patients were included if they met the following criteria:
- An age over 60 years.
- A confirmed diagnosis of bronchial asthma made according to the Global Initiative for Asthma (GINA) criteria, with at least one year of treatment documented. Asthma severity was classified also according to the GINA: based on the level of treatment required to control symptoms and prevent exacerbations.
- A positive bronchial reversibility test (an increase of at least 12% and/or 200 mL in forced expiratory volume in 1 second (FEV1) of predicted value and/or a decrease of at least 40% in R19 resistance in the FOT examination) or -partial reversibility (ΔFEV1 <12% and/or <200 mL) when severe asthma was diagnosed (GINA criteria).1
The exclusion criteria were as follows:
- Obstructive respiratory diseases.
- The presence of another systemic respiratory disease that affects respiratory efficiency.
- A condition of cardiac failure that necessitates therapeutic intervention.
- Failure to cooperate with the respiratory function tests.
The patient inclusion process is illustrated in Flow Diagram (Figure 1). Ultimately, 345 patients from 451 were randomly selected (by the use of computer program Access Microsoft) for further analysis and inclusion in the study.
 |
Figure 1 Flow diagram of study patients. |
At the same time, a non-asthmatic group of participants (as controls) aged over 60 was formed by excluding those with obstructive respiratory diseases (without a diagnosis of asthma and/or COPD), based on correct spirometry results and the absence of specific asthma or COPD therapy. Participants were recruited from the same centers and also randomly selected to further procedures: perform a spirometry test and a FOT.
Procedures
Interview. Medical Examination. Analysis of Medical Records
The presence of multimorbidity was accounted for in the analysis, incorporating data on asthma treatment and coexisting conditions over the 12 months prior to the start of the study. The analysis included other chronic diseases identified using ICD-10 codes, documented treatment for at least one year and any other diagnostic tests that supplemented the diagnosis. Furthermore, the findings of allergy diagnostics, including skin tests, allergen-specific IgE levels, and total IgE levels in blood serum, were examined. If necessary, detailed data from the interviews conducted during the visits were included. Patients from the study group who had doubts about whether they had COPD, as indicated by a physical examination or treatment, were excluded from the analysis.
Questionnaire Assessment
All patients with asthma also completed the Asthma Control Test (ACT), as well as the Asthma Quality of Life Questionnaire (AQLQ) and 36-Item Short Form Survey (SF-36) questionnaires.13–15 The latter were also completed in the control group.
Asthma Control Test (ACT)
The ACT is a patient-administered tool for identifying individuals with poorly controlled asthma. The total score ranges from 5 (poor asthma control) to 25 (complete asthma control), with higher scores reflecting greater control. An ACT score greater than 19 indicates well-controlled asthma.
Asthma Quality of Life Questionnaire (AQLQ)
The AQLQ is a disease-specific health-related quality of life instrument that measures the physical and emotional effects of asthma. This questionnaire contains the following categories: Symptoms (11 items); Activity Limitations (12 items, five of which are individualized); Emotional Functioning (five items); and Environmental Exposure (four items). The total score ranges from 1 to 7, with higher scores indicating better quality of life.
36-Item Short Form Survey (SF-36)
The SF-36 is a well-researched, self-reported outcome measure instrument that is often used in research. The SF-36 stems from a study called the Medical Outcomes Study, which aims to objectively measure quality of life. SF-36 scores are obtained by standardizing the scales using a scoring algorithm or SF-36v2 scoring software, resulting in a total score ranging from 0–100. Higher scores indicate better health status, and a mean score of 50 was established as the normative value for all scales.
Spirometry
Certain medications were discontinued (if they were used) prior to testing: short-acting β2-agonists and ipratropium bromide were stopped eight hours before testing, whereas long-acting theophylline and long-acting inhaled β2-agonists (formoterol and salmeterol) were stopped for 24 hours. The bronchial flow test was performed in accordance to American Thoracic Society and European Respiratory Society (ATS/ERS) guidelines, with the Lungtest 1000 (MES, Cracow, Poland).16 FOT was performed 15 min before spirometry only in patients with asthma (study group). Patients with severe airflow limitations (FEV1 <30%) were excluded from the analysis in accordance with the inclusion criteria, as significant obstruction could influence FOT measurements.
Forced Oscillation Technique (FOT)
The FOT assessment measures changes in airflow in response to an external pressure wave (a sinusoidal signal with a defined frequency and amplitude) generated by a loudspeaker while not interfering with normal breathing. The resulting respiratory impedance comprises both resistance (airway patency) and reactance (the elasticity and inertia of the respiratory system). Low-frequency signals (eg, 5 or 8 Hz) are used to assess the entire bronchial tree.17 In patients with obstructive diseases, resistance is increased, and reactance decreases due to peripheral airway obstruction. In patients with interstitial lung disease, reduced compliance also causes lower reactance.
The Resmon Pro device (Restech SRL, Milan, Italy) was used in accordance with ATS/ERS guidelines.17,18 The software automatically assessed the validity of the 5 Hz measurements using a coherence function. At least three valid measurements were analyzed. The predicted resistance values at 5 Hz were calculated on the basis of sex-specific reference standards.18
Bronchodilator Reversibility Testing
Bronchodilator reversibility testing was performed for all asthmatic patients during the visit. After baseline spirometry, the participants were given 400 μg of salbutamol (a short-acting β2 agonist) via a metred-dose inhaler and spacer (Aerochamber Plus, Trudell Medical International, London, Ontario, Canada). Spirometry was repeated 15 minutes later. A positive response to bronchodilator administration was defined as an improvement of at least 200 mL and 12% in FEV1 and/or forced vital capacity (FVC), respectively.16
Statistical Analysis
Statistical analysis was conducted using Statistica 8.2 software (StatSoft, Poland). The Shapiro–Wilk test was performed to determine whether the data were normally distributed. Nonparametric tests were used because the studied parameters were not normally distributed. The data are expressed as the median (Me), as well as the minimum (Min) and maximum (Max) parameter values. Mann–Whitney or chi-square tests were performed to compare two independent samples, especially when comparing age subgroups. For dependent samples, Wilcoxon or McNemar tests were performed. Spearman’s test was used to analyse the correlations between variables. A p value of less than 0.05 was considered to indicate statistical significance for all tests.
Results
Phenotyping of Asthma
Data from 345 patients who met the study criteria were used for the final analysis. The detailed data are shown in Table 1. The distributions of asthma control and treatment levels across age subgroups in the studied asthmatic population are shown in Figure 2.
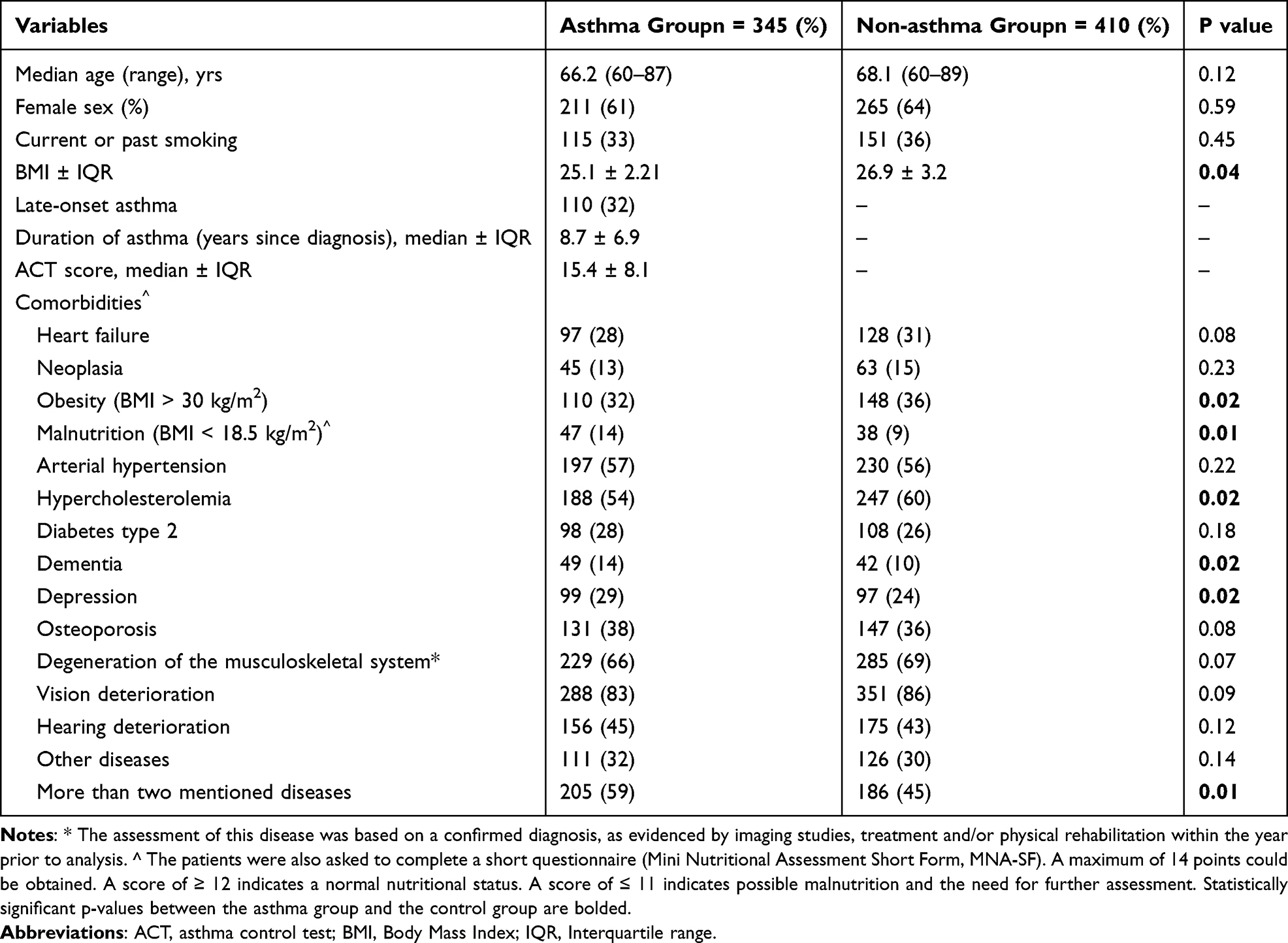 |
Table 1 Characteristics of the Clinical Outcomes of the Asthma Group Compared with the Non-Asthma Group |
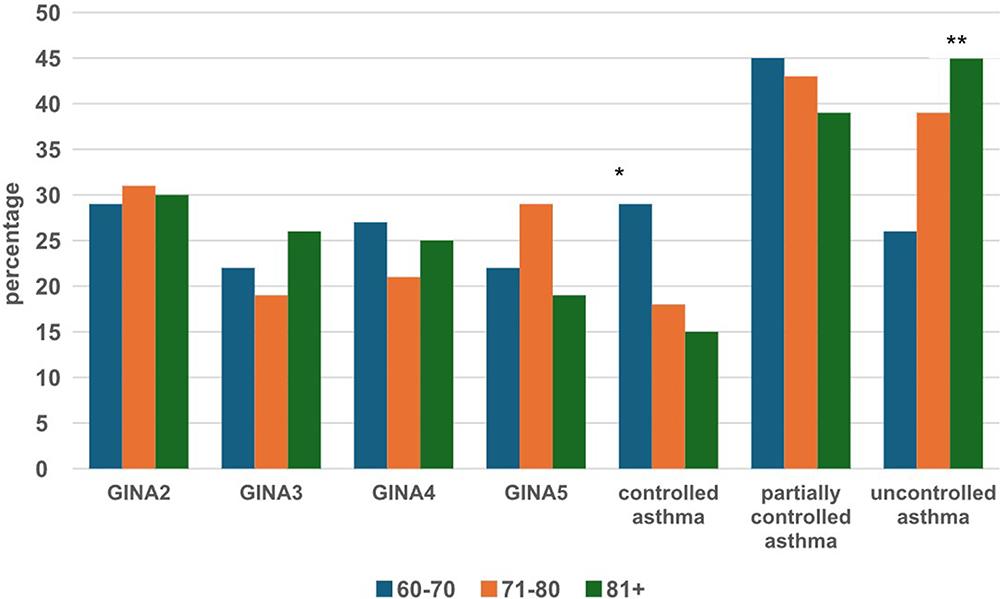 |
Figure 2 Characteristics of asthma patients in different age groups (60–70, 71–80, and 81+ years). GINA2-GINA5: Asthma treatment steps to maintain disease control, depending on disease severity, according to the Global Initiative for Asthma (2023). *Controlled asthma was significantly more common in the youngest subgroup (p =0.01). ** Uncontrolled asthma was significantly more common in the older subgroups (p =0.01). |
Phenotyping for T2 asthma was performed for the included patients on the basis of biomarker analysis (eosinophilia (>150/μL), FeNO (>20 ppm), IgE level (70 kU/L)) and a good response to inhaled and oral steroids, as well as the presence of clinical features of allergic diseases. Low T2 asthma was confirmed when blood eosinophils were <150 cells/µL, FeNO was <25 ppb and total IgE was normal or low, as well as there being a poor response to corticosteroids. Mixed-type asthma (T2-high/T2-low overlap) was defined by the following criteria: blood eosinophils of 150–300 cells/µL, FeNO of 25 ppb or more, and often elevated total IgE, as well as a partial response to corticosteroids.
A total of 165 (48%) patients had T2 asthma, 114 (33%) patients had low-T2 asthma, and 66 (19%) patients had a mixed phenotype. An additional analysis of 87 patients with severe asthma according to GINA (for whom all the necessary data were available) revealed that 49 patients had the T2 type, 17 patients had the mixed type, and 21 patients had the low T2 type on the basis of the same criteria. Additionally, 21 patients were confirmed to have aspirin-induced asthma on the basis of their medical history and/or an oral provocation test result.
Patients with asthma were found to have a higher prevalence of multimorbidity, as well as significantly higher rates of depression and/or cognitive impairment. However, the remaining disease profiles were similar between the asthma group and the control group of patients without obstructive disease in the same age range.
A final diagnosis of asthma, COPD, or both conditions simultaneously could not be confirmed in 24 patients. Therefore, these individuals were not included in the analysis.
The analysis of data on concomitant allergic diseases and allergy test results is presented in Table 2. Notably, most eligible patients were not eligible for biological treatment at the time of data evaluation.
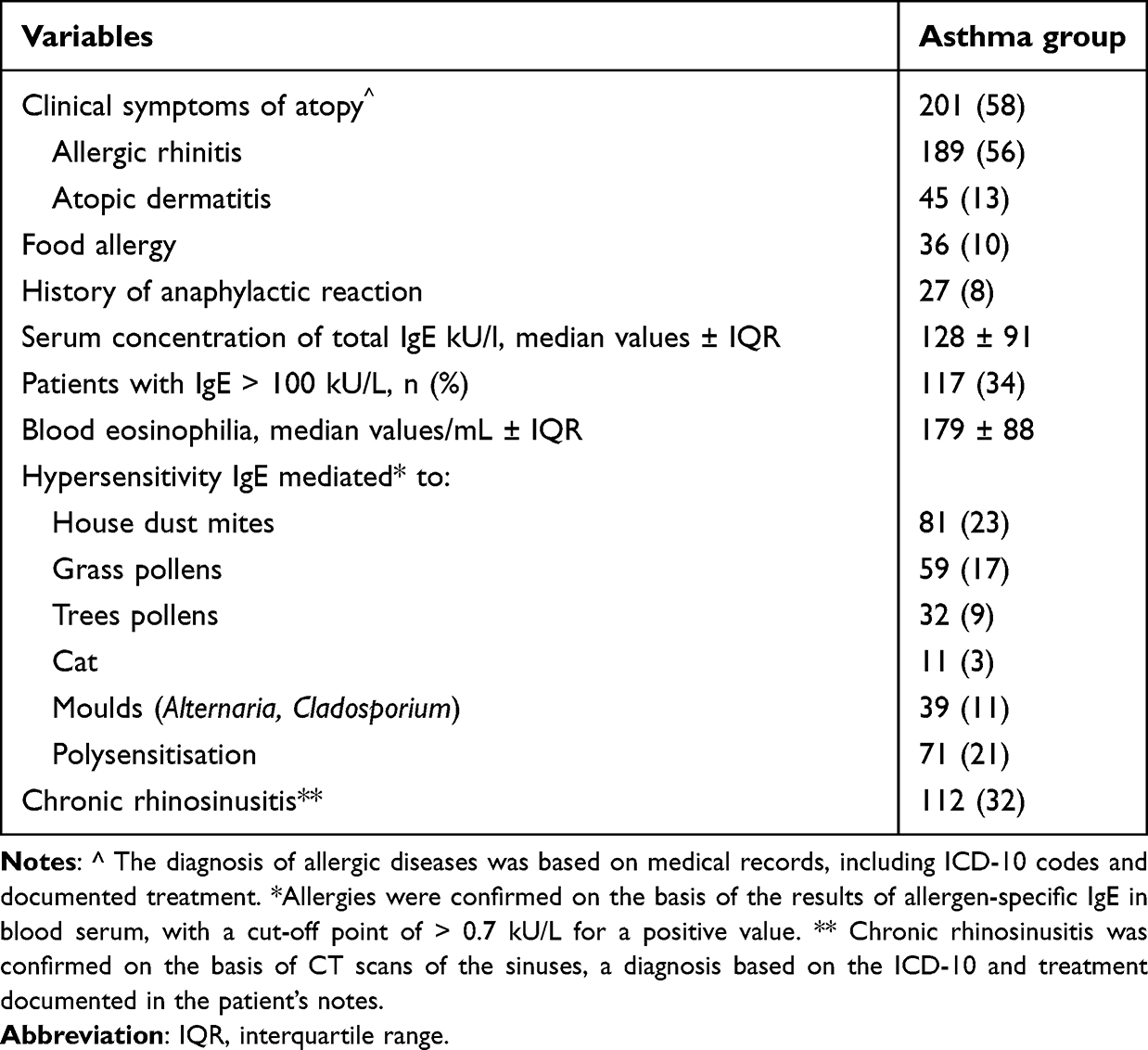 |
Table 2 Allergic Characteristics of the Studied Asthma Population (n = 345) |
Respiratory Function Tests
The results of functional tests in the form of expected FEV1 percentages and R5 values for the different age groups are presented in Figures 3 and 4. The median FEV1 values for the entire asthma population were 81% ± 20.8% (IQR) and 1.89 L/s ± 0.79 (IQR). For R5, the values were 129% ± 27.1% and 0.88 ± 0.51 cmH2O/L/s. Patients over 80 years of age achieved their age-appropriate FEV1 less frequently than younger patients did. No such differences were observed in R5 resistance in the FOT study (see Figure 4).
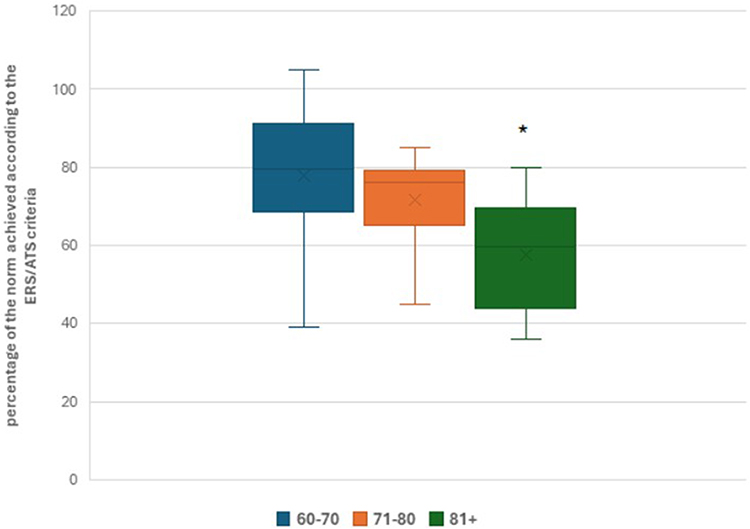 |
Figure 3 Average percentage of the FEV1 norm achieved in different age groups (60–70, 71–80, and 81+ years). The interpretation of the results was based on ERS/ATS standards (ETS-European Respiratory. Society, ATS – American Thoracic Society). * Patients over 80 years of age achieved a significantly lower percentage of the FEV1 norm than younger patients did (p=0.01). |
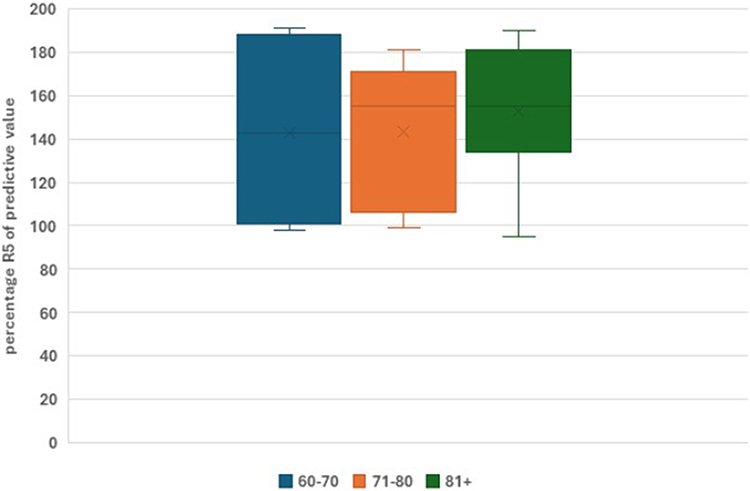 |
Figure 4 Comparison of the average percentages obtained for the R5 resistance norm in the study of forced respiratory oscillations in different age groups (60–70, 71–80, and 81+ years). No significant differences were observed among the age groups. |
Asthma Therapy
The average daily use of inhaled steroids is presented in Figure 5. Significant differences were observed in the form of lower inhaled steroid use in the older subgroups. The median daily dose of ICS (budesonide equivalent) for the entire examined asthma population was 605 ± 275 μg (± interquartile range=IQR).
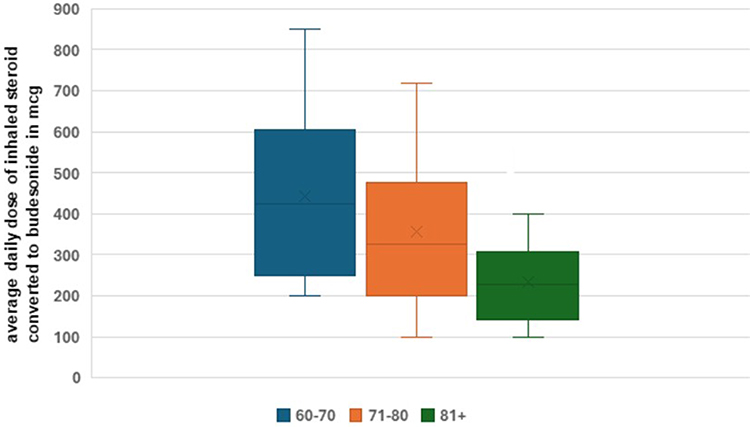 |
Figure 5 Average daily doses of inhaled steroids converted to budesonide in different age groups (60–70, 71–80, and 81+ years). The graph shows the average daily dose, the standard deviation and the median. The average daily dose of inhaled steroids was significantly lower in the older subgroup than in the younger subgroups (p = 0.01). |
The details of antiasthmatic drug use are presented in Table 3. Biological treatment was rarely used by the patients in this study, whereas a large proportion of patients had chronic oral steroid use.
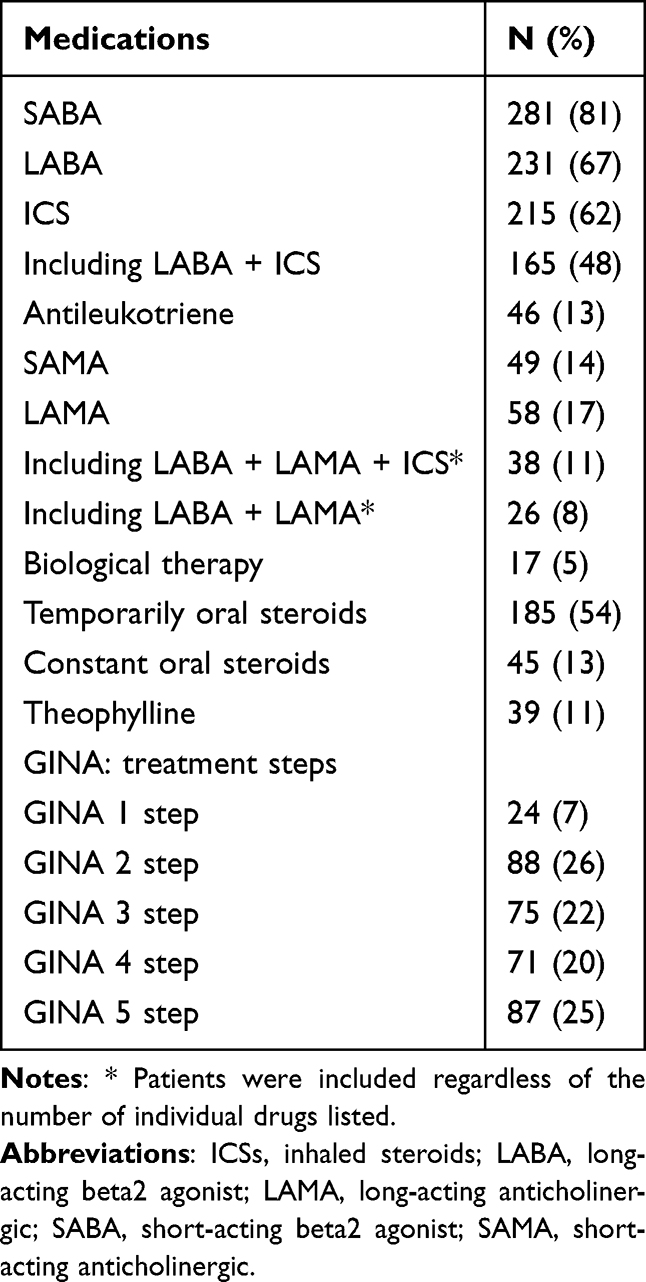 |
Table 3 Antiasthmatic Drugs Used by the Patients in the Study (n = 345) |
Quality of Life
The average total AQLQ score obtained by the asthma group during the visit was 3.78 ± 0.91 (median ± IQR), which was significantly lower than that obtained by the non-asthmatic group (4.29 ± 1.81, p =0.01).
Similar trends were observed for each analyzed domain: environmental exposure (4.21 ± 0.95 vs 5.08 ± 1.16), emotional function (4.45 ± 0.78 vs 4.91 ± 0.97) and activity (3.01 ± 0.59 vs 4.0.8 ± 0.83). The quality-of-life score was significantly correlated with better asthma control, as determined by the ACT (Spearman’s rank correlation test, R = 0.77, p=0.02). However, the AQLQ score was not correlated with the spirometric value (FEV1).
Analysis of the AQLQ scores revealed no significant differences in quality of life among the age subgroups.
Compared with the non-asthmatic group, the asthma group had significantly poorer results in all domains. These data are presented in Table 4. Moreover, the average SF-36 scores were significantly worse for the asthma group over 80 years of age than for the younger groups in terms of general perceptions (53.521 vs 46.991, p=0.01).
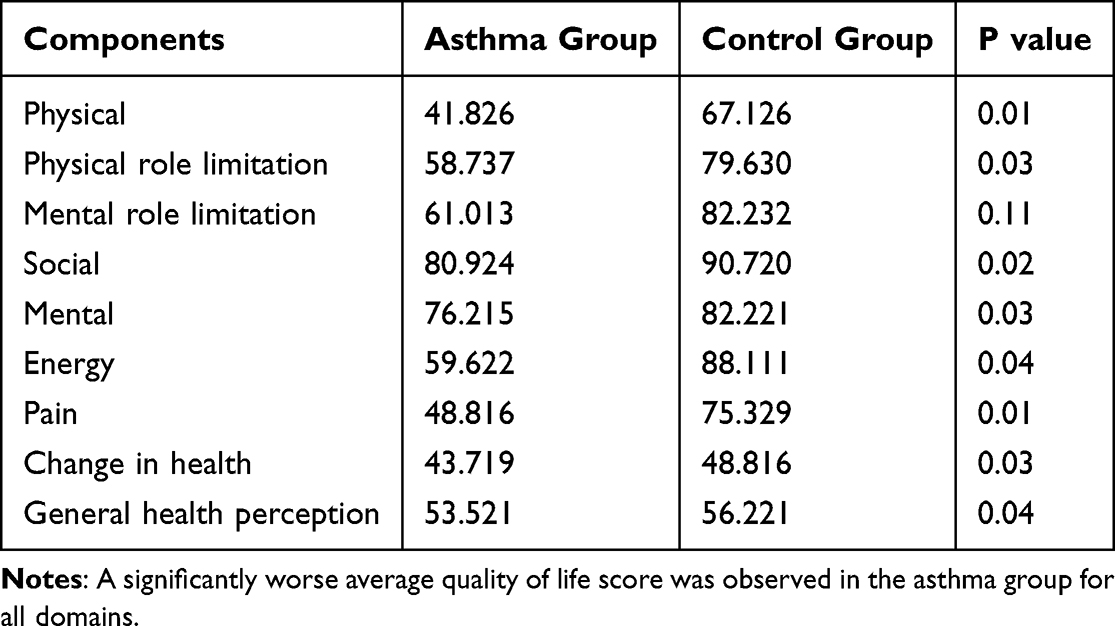 |
Table 4 Detailed Results of the SF-36 Questionnaire Organised by Domain |
Discussion
Asthma is estimated to affect approximately 7–10% of people older than 60–65 years, aligns with global estimates reported by Gibson et al (2010) and Hanania et al (2011), who also highlighted diagnostic problem of asthma and comorbidities in this age group.7,19 Similarly, local data from Central and Eastern Europe confirmed a comparable observations in asthmatic older people.12
The diagnosis of asthma in older adults presents several unique challenges due to physiological changes associated with ageing, symptoms that overlap with those of other diseases, and atypical presentations of the disease.19–21
The comorbidity in patients with asthma presented here has the effect of either masking or mimicking asthma itself. Notably, the observed differences in the disease profiles of patients with and without asthma may be key. The higher prevalence of dementia and depression episodes, as well as the presence of more comorbidities, in asthma patients may suggest that they find it more difficult to verbalize health problems, including asthma itself. Our results regarding the coexistence of cognitive disorders and poorer asthma control are in line with Bozek and Jarzab (2011), who found that appropriate asthma management improved mental and physical function in elderly patients with Alzheimer’s disease.22 This highlights the importance of comprehensively evaluating asthma patients and defining comprehensive treatment plans. However, it should be noted that diseases such as type 2 diabetes and osteoporosis were not significantly more prevalent in the entire asthma population than in the non-asthmatic group, which is consistent with other studies.23,24 However, these observations do not apply to patients with severe asthma who use oral steroids and experience various complications as it was confirmed by other authors.24 The typical changes associated with ageing undoubtedly affect the prevalence of asthma and other respiratory diseases. For example, normal ageing causes decreased lung elasticity and chest wall compliance, as well as reduced respiratory muscle strength.25 These changes can obscure the typical spirometry results used to diagnose asthma. This is particularly common in the oldest subgroup, in which malnutrition and sarcopenia, which are typical of seniors, are also observed most frequently.25,26
Another problem that needs to be emphasized is the difficulty of performing functional respiratory tests in seniors with suspected obstructive diseases of the respiratory system. Reliable spirometry can be difficult because of physical frailty, poor coordination and even cognitive impairment.27–30 The authors report that in approximately one-third of the examined patients, reversibility testing (the response to bronchodilators) was less clear or less powerful. In some seniors, the subsequent exercise helped generate reliable results owing to the merit of the right medical staff. These observations were confirmed by other authors.28–30 However, too little attention is still given to other methods of assessing respiratory capacity that are easier for patients to cooperate with.
The use of the FOT as an easier method is understandable for this group of patients.31 The added value of the FOT, particularly in diagnosing asthma in children, has been demonstrated by numerous studies and endorsed in ERS/ATS recommendations.32,33 The value of the bronchial reversibility test using the FOT has also been confirmed in other international studies involving the prediction of such a test using spirometry.34,35 However, data evaluating the definitive value of this test in diagnosing asthma in older people are still lacking. The obtained resistance values were found to be significantly correlated with the FEV1 values obtained for patients with mild and moderate asthma, as well as for some patients with severe asthma.34,36 Further research that accounts for both patient age and initial bronchial obstruction is needed. Nevertheless, the FOT appears to be a valuable tool for diagnosing patients who are unable to cooperate with spirometry.
Treatment and Pharmacotherapy
The asthma treatment strategy used for most of the analyzed patients was in line with the GINA standards.1 Approximately 25% of the patients changed their inhaled treatment regimen due to problems with adherence to specific medications (these data were not published). There was also an underestimation or reduction in the daily dose of inhaled steroids, impacting asthma control, particularly in the oldest age subgroup.1 When comparing pharmacological management, the underuse of inhaled corticosteroids (ICS) and the overreliance on oral corticosteroids and short-acting beta-agonists (SABA) in our cohort mirrors the findings of Tomasello et al (2024) and Hung et al (2024), who reported similar trends in the US and Italian populations.37,38
Another negative trend observed in the presubmitted study was the relatively large number of patients with periodic oral steroid use and the very small number of patients who qualified for biologic treatment.39 Despite the availability of programs for biological drugs, this phenomenon is underpinned by the need to maintain a treatment regimen and cooperate with other therapies due to multimorbidity, as well as the lack of stereotypical exclusion of seniors owing to age and diagnostic concerns.
Conversely, long-acting beta2 agonist (LABA), combination drugs and short-acting beta2 agonist (SABA) abuse were also common in the younger age groups included in this study.
In many cases, conflicts due to a lack of therapeutic synchronization have been observed, eg, the use of nonselective beta-blockers in patients with arrhythmia and asthma, which significantly worsened ventilatory parameters in the absence of patient observation.40
In conclusion, asthma treatment should be personalized for all patients, especially those with asthma, on the basis of the GINA criteria, the patient’s ability to conduct and maintain therapy, and the other necessary therapies, which should be properly combined.
Quality of Life in the Elderly Population
Asthma can significantly reduce the quality of life of older adults.19 Age-related changes in lung function, alongside other chronic illnesses, exacerbate symptoms such as shortness of breath, coughing and wheezing, making these symptoms more challenging to manage. This can lead to reduced physical activity, fatigue and dependence on others.
Psychologically, asthma can lead to anxiety, depression and sleep disturbances, particularly when symptoms occur at night. Socially, elderly individuals may withdraw from activities because of a fear of asthma attacks, which can lead to isolation. The financial burden of treatment can also cause stress.41
The reduced quality of life (QoL) reported by our participants, particularly in the oldest subgroup, corroborates previous global studies (Gibson et al, 2010; Dyer et al, 1999),19,42 which also demonstrated that aging, comorbidities, and poorer asthma control are closely linked to functional decline.19,37,42
However, the limitations of the study may have affected the results in many cases. These include partially retrospective data, not all of which could be updated at the time of the visit, and a relatively large group of patients with obstructions who were ineligible for the study owing to diagnostic concerns. This particularly applies to patients with advanced bronchial obstructions for whom the correct bronchial reversal procedure has not been performed. A separate management consensus is needed for this group to avoid the misdiagnosis of asthma as COPD or an overlapping syndrome. Currently, such data are in preparation for publication.
Conclusion
In older adults, asthma remains undertreated despite its significant effects on health and quality of life. This study revealed that elderly patients often present with multimorbidity, poorer asthma control, reduced lung function and limited access to advanced therapies such as biologics. The lower ICS doses in older subgroups and the frequent use of oral steroids indicate a need for more personalized and age-adjusted treatment strategies. Patients over the age of 80 have worse asthma control more frequently as a result of insufficient treatment.
Data Sharing Statement
The datasets used in this study can be obtained from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Bioethical Committee of the Medical University of Silesia (No: BNW/NWN/0052/KB1/17/ I/23 13 June 2023; Katowice, Poland). All participants in the study gave their informed consent to participate in the study. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Medical University of Silesia, Poland (grant: nr UDA-FESL.10.25-IŻ.01.05/FB/23-00).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Global Initiative for Asthma (GINA). GINA Strategy Report 2025; 2025. https://ginasthma.org/2025-gina-strategy-report/.
2. Skloot GS, Busse PJ, Braman SS, et al. An official American Thoracic Society workshop report: evaluation and management of asthma in the elderly. Ann Am Thorac Soc. 2016;13(11):2064–13. doi:10.1513/AnnalsATS.201608-658ST
3. Battaglia S, Benfante A, Spatafora M, Scichilone N. Asthma in the elderly: a different disease? Breathe. 2016;12(1):18–28. doi:10.1183/20734735.002816
4. Benfante A, Tomasello A, Gianquinto E, Cicero MN, Scichilone N. Diagnostic and therapeutic approaches for elderly asthma patients: the importance of multidisciplinary and multidimensional management. Expert Rev Respir Med. 2023;17(6):459–468. doi:10.1080/17476348.2023.2215432
5. National Center for Environmental Health. Asthma Surveillance in the United States, 2001–2021; 2023.
6. Wecker H, Tizek L, Ziehfreund S, et al. Impact of asthma in Europe: a comparison of web search data in 21 European countries. World Allergy Organ J. 2023;16(8):100805. doi:10.1016/j.waojou.2023.100805
7. Hanania NA, King MJ, Braman SS, et al. Asthma in the elderly: current understanding and future research needs—a report of a National Institute on Aging (NIA) workshop. J Allergy Clin Immunol. 2011;128(3 Suppl):S4–S24. doi:10.1016/j.jaci.2011.06.048
8. Baptist AP, Busse PJ. Asthma over the age of 65: all’s well that ends well. J Allergy Clin Immunol Pract. 2018;6(3):764–773. doi:10.1016/j.jaip.2018.02.007
9. Dunn RM, Busse PJ, Wechsler ME. Asthma in the elderly and late-onset adult asthma. Allergy. 2018;73(2):284–294. doi:10.1111/all.13258
10. Gonzalez-Uribe V, Romero-Tapia SJ, Castro-Rodriguez JA. Asthma phenotypes in the era of personalized medicine. J Clin Med. 2023;12(19):6207. doi:10.3390/jcm12196207
11. Ge YY, Zuo R, Xi HX, et al. Multimorbidity patterns of asthma exacerbation in an older cohort: prognostic implications. J Allergy Clin Immunol Pract. 2025;S2213-198(25):00312.
12. Bozek A, Rogala B, Asthma BP. COPD and comorbidities in elderly people. J Asthma. 2016;53(9):943–947. doi:10.3109/02770903.2016.1170139
13. Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113(1):59–65. doi:10.1016/j.jaci.2003.09.008
14. Juniper EF, Buist AS, Cox FM, Ferrie PJ, King DR. Validation of a standardized version of the asthma quality of life questionnaire. Chest. 1999;115(5):1265–1270. doi:10.1378/chest.115.5.1265
15. Ware JE, Keller SD, Hatoum HT, Kong SX. The SF-36 arthritis-specific health index (ASHI):I. Development and cross-validation of scoring algorithms. Med Care. 1999;37(5 Suppl):MS40–MS50. doi:10.1097/00005650-199905001-00004
16. Graham BL, Steenbruggen I, Miller MR, et al. Standardization of spirometry 2019 update: an official American Thoracic Society and European Respiratory Society technical statement. Am J Respir Crit Care Med. 2019;200(8):e70–e88. doi:10.1164/rccm.201908-1590ST
17. Brashier B, Salvi S. Measuring lung function using sound waves: role of the forced oscillation technique and impulse oscillometry system. Breathe. 2015;11(1):57–65. doi:10.1183/20734735.020514
18. King GG, Bates J, Berger KI, et al. Technical standards for respiratory oscillometry. Eur Respir J. 2020;55(2):1900753. doi:10.1183/13993003.00753-2019
19. Gibson PG, McDonald VM, Marks GB. Asthma in older adults. Lancet. 2010;376(9743):803–813. doi:10.1016/S0140-6736(10)61087-2
20. Zeki AA, Jarjour NN. The asthma-chronic obstructive pulmonary disease overlap syndrome: a new take on an old concept. Ann Am Thorac Soc. 2016;13(9):1440–1442. doi:10.1513/AnnalsATS.201606-493ED
21. Cazzola M, Hanania NA, Rogliani P, Matera MG. Cardiovascular disease in asthma patients: from mechanisms to therapeutic implications. Kardiol Pol. 2023;81(3):232–241. doi:10.33963/KP.a2023.0038
22. Bozek A, Jarzab J. Improved activity and mental function related to proper antiasthmatic treatment in elderly patients with Alzheimer’s disease. Allergy Asthma Proc. 2011;32(5):341–345. doi:10.2500/aap.2011.32.3459
23. Lin HH, Hsu HY, Tsai MC, Hsu LY, Chien KL, Yeh TL. Association between type 2 diabetes and osteoporosis risk: a representative cohort study in Taiwan. PLoS One. 2021;16(7):e0254451. doi:10.1371/journal.pone.0254451
24. Rogala B, Bożek A, Gluck J. Is there a relationship between asthma and diabetes? J Asthma. 2020;57(12):1332–1338. doi:10.1080/02770903.2019.1652642
25. Oyarzún GM. Pulmonary function in aging. Rev Med Chil. 2009;137(3):411–418.
26. Benz E, Trajanoska K, Schoufour JD, et al. Sarcopenia in older people with chronic airway diseases: the Rotterdam study. ERJ Open Res. 2021;7(1):00522–2020. doi:10.1183/23120541.00522-2020
27. Braman SS. Asthma in the elderly. Clin Geriatr Med. 2003;19(1):57–75. doi:10.1016/S0749-0690(02)00052-6
28. Boutou AK, Zafeiridis A, Pitsiou G, Dipla K, Kioumis I, Stanopoulos I. Cardiopulmonary exercise testing in chronic obstructive pulmonary disease: an update on its clinical value and applications. Clin Physiol Funct Imaging. 2020;40(4):197–206. doi:10.1111/cpf.12627
29. Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005;26(5):948–968. doi:10.1183/09031936.05.00035205
30. Rudell K, Hareendran A, Bonner N, Arbuckle R, Burbridge C, Abetz L. Patients’ experience of asthma control and clinical guidelines: perspectives from a qualitative study. Respir Med. 2012;106(6):909–911. doi:10.1016/j.rmed.2011.08.024
31. Inoue H, Niimi A, Takeda T, et al. Pathophysiological characteristics of asthma in the elderly: a comprehensive study. Ann Allergy Asthma Immunol. 2014;113(5):527–533. doi:10.1016/j.anai.2014.08.002
32. Oostveen E, MacLeod D, Lorino H, et al. The forced oscillation technique in clinical practice: methodology, recommendations and future developments. Eur Respir J. 2003;22(6):1026–1041. doi:10.1183/09031936.03.00089403
33. Stanojevic S, Kaminsky DA, Miller MR, et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur Respir J. 2022;60(1):2101499. doi:10.1183/13993003.01499-2021
34. Desiraju K, Agrawal A. Impulse oscillometry: the state-of-art for lung function testing. Lung India. 2016;33(4):410–416. doi:10.4103/0970-2113.184875
35. Miodońska M, Bożek A, Urbaniec E, Mitka A, Wasilewska E. The usefulness of the forced oscillation technique in the diagnosis of bronchial asthma in seniors. Expert Rev Respir Med. 2025;19(2):175–182. doi:10.1080/17476348.2025.2461229
36. Zhou X, Yi D, Wu Y, et al. Expression of diaphragmatic myostatin and correlation with apoptosis in rats with chronic obstructive pulmonary disease. Exp Ther Med. 2018;15(3):2295–2300. doi:10.3892/etm.2018.5686
37. Tomasello A, Benfante A, Lisotta A, et al. Polypharmacy in older patients with asthma: hidden risks and opportunities for improvement. Expert Rev Respir Med. 2024;18(12):1047–1059. doi:10.1080/17476348.2024.2444331
38. Hung CT, Hung YC, Suk CW, et al. Polypharmacy among adults with asthma in the United States, 2005–2020. J Am Pharm Assoc. 2024;64(5):102154. doi:10.1016/j.japh.2024.102154
39. Moreno NVL, Herrera Sánchez DA, Larenas-Linnemann D. Diagnosis and management of asthma in the elderly. Clin Exp Allergy. 2022;52(9):1015–1017. doi:10.1111/cea.14190
40. Radenne F, Verkindre C, Tonnel AB. L’asthme du sujet âgé [Asthma in the elderly]. Rev Mal Respir. 2003;20(1 Pt 1):95–103.
41. Connolly MJ, Yohannes AM. The impact of depression in older patients with chronic obstructive pulmonary disease and asthma. Maturitas. 2016;92:9–14. doi:10.1016/j.maturitas.2016.07.005
42. Dyer CA, Hill SL, Stockley RA, Sinclair AJ. Quality of life in elderly subjects with a diagnostic label of asthma from general practice registers. Eur Respir J. 1999;14(1):39–45. doi:10.1034/j.1399-3003.1999.14a09.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effect of Changes in Defecation Posture on Health-Related Quality of Life Among Elderly Habitual Squat-Toilet Users After Total Hip Arthroplasty for Femoral Neck Fracture
Zhao Y, Guo D, Yan C, Dong Y, Li X, Zhang J
Patient Preference and Adherence 2026, 20:575359
Published Date: 17 January 2026
The Impact of Nursing Education Innovation on the Quality of Care for Elderly Hospitalized Patients: A Systematic Review Based on Student Competency Development
Cui H, Luo M
Journal of Multidisciplinary Healthcare 2026, 19:575875
Published Date: 4 February 2026
Exercise, Ethnicity, and Quality of Life in Older Adults with Persistent Nonvalvular Atrial Fibrillation: A Multicenter Cross-Sectional Study
Xu Y, Zhao X, Zheng X, Shi S, Lv F, Dong R, Liu K
Clinical Interventions in Aging 2026, 21:599331
Published Date: 15 May 2026