Back to Journals » Patient Related Outcome Measures » Volume 14
The Effect of Armed Conflict on Treatment Interruption, Its Outcome and Associated Factors Among Chronic Disease Patients in North East, Amhara, Ethiopia, 2022
Authors Mesfin B ![]() , Mersha Demise A, Shiferaw M
, Mersha Demise A, Shiferaw M ![]() , Gebreegziabher F
, Gebreegziabher F ![]() , Girmaw F
, Girmaw F ![]()
Received 16 May 2023
Accepted for publication 16 August 2023
Published 24 August 2023 Volume 2023:14 Pages 243—251
DOI https://doi.org/10.2147/PROM.S388426
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lynne Nemeth
Betelhem Mesfin,1 Alexander Mersha Demise,2 Mullu Shiferaw,3 Freweyni Gebreegziabher,1 Fentaw Girmaw2
1Department of Nursing, School of Nursing, College of Health Sciences, Woldia University, North Wollo, Amhara, Ethiopia; 2Department of Pharmacy, College of Health Sciences, Woldia University, North Wollo, Amhara, Ethiopia; 3School of Medicine, College of Health Sciences, Woldia University, North Wollo, Amhara, Ethiopia
Correspondence: Betelhem Mesfin, Email [email protected]
Background: The health services delivery system is debilitated in conflict setting areas due to damage of health facilities and attack on health care providers. Armed conflict is a complex phenomenon which causes a large amount of death and disability worldwide. However, there is lack of information towards treatment interruption among chronic disease patients in conflict areas. Hence, this study was conducted to assess the prevalence of armed conflict induced treatment interruption and its outcome among chronic disease patients.
Methods: A mixed cross sectional study design was conducted on a total of 399 sample size at North Wollo and Waghimra zone hospitals. To select study participants a consecutive sampling method was used. Multiple logistic regressions were computed to evaluate the association and thematic analysis was used to analyse qualitative data.
Results: From the total 399 study participants, 264 (64.6%) study participants interrupted their medication. Treatment interruption is significantly associated with poor service availability and perceived high stress.
Conclusion: War has detrimental health effects, both immediate and long term, on populations. Treatment interruptions due to armed conflict were caused by poor health care access, lack of medications and lack of transport and displacement of hospital staff, insecurity and fear. Treatment interruption results in morbidity, mortality, lifelong complications, disability, psychological and economic impact.
Keywords: armed conflict, chronic disease, treatment interruption
Background
Among different conflict prone countries, Ethiopia is one which is regarded as philosophical, ethical, moral, socio political and religious division. Conflict results in loss of life, destruction of infrastructure and drained growth and development of the country.1 The TPLF attack on Ethiopian federal forces on November 4, 2020, G.C. marked the beginning of the country’s ongoing wars, which currently encompass the northern region.2 Attacks and mistreatment of towns and villages in northern Amhara (such as Lalibela, Woldia, Debre Tabor and Adi Arka) and in Afar (Uwwa, Galikoma and Berhale towns) since July 2021 have resulted in hundreds of civilian deaths from shelling or massacres, and by mid-September 2021, more than 550,000 people had been evacuated.2
In addition to reports of a food scarcity, bloodshed and humanitarian disaster, the war obtained attention internationally.3 Armed conflicts are complex, unpredictable and multifaceted events that result in a great deal of death and disability globally, as well as the destruction of families, communities and the social infrastructure that underpins health systems.4 The depletion of resources, access to health care and general disruption to everyday life during times of armed conflict create excess stress and burdens, which increase deaths.5
Chronic diseases are defined as medical conditions that persist for three months or longer, progressing slowly over an extended period of time.6 Chronic diseases like heart disease, diabetes mellitus, cancer, stroke, hypertension, respiratory diseases, oral diseases, arthritis and obesity can lead to a reduced quality of life. In addition, it also causes long-term disability, hospitalization and death.7,8
For example, armed conflict can cause delays in ART and HIV treatment access because it interrupts health care systems. The potential outcomes include the development of drug resistance, increased illness and, ultimately, mortality. This might be due to a lack of infrastructure, insufficient drug supply, hazardous travel circumstances, or relocation brought on by violence or house damage.9
The delivery of health services, continuity of treatment and the provision of appropriate care for patients with NCDs have all been made more difficult as a result of the rise in targeted attacks on medical facilities and medical personnel in conflict-ridden areas.10 Delays in care and treatment may result in poorly managed health issues, possible consequences and much comorbidity. Chronic illnesses require ongoing care, coordination and treatment.11
Achieving adequate glycaemic control might be challenging if a drug regimen is interrupted during therapy, as could happen in diabetes mellitus. Interruptions in treatment can lead to the formation of disorders including diabetes microangiopathy (retinopathy, nephropathy and neuropathy) and also raise the risk of diabetic complications.12 On the other side, stopping or interrupting antiretroviral medication might lead to clinical advancement, drug resistance, immunological decompensation, viral rebound and drug resistance.13
The study conducted in Kenya stated that among 1605 study participants, the prevalence of treatment interruption was 71% and similarly the study conducted in Yemen stated that the prevalence of armed conflict induced treatment interruption is 8.4% among DM patients.14,15 Even though different African countries have stated the prevalence of treatment interruption in conflict setting areas, there is limited information. Therefore, the purpose of this study was to evaluate how armed conflict affected the interruption of treatment for patients with chronic illnesses in North Wollo and Waghimra zone hospitals in the Amhara region.
The study finding may be helpful in providing preliminary information for an interventional program. In addition, little is known about the optimal health sector response to chronic diseases in poor, post-conflict countries. As a consequence, the findings of this study can serve as a baseline for other studies that are relevant to it and they will create baseline data about the effect of armed conflict on treatment interruption among patients with chronic diseases.
Methods
Study Area
This study was conduct at North Wollo and Waghimra zone hospitals. North Wollo zone and Waghimra zone are found in Amhara regional state with the capital city of Woldia which is 521 km away from Addis Ababa and 360 km from Bahirdar. In these two zones there are around seven governmental hospitals: Mersa Primary Hospital, Meket Primary Hospital, Kobo Primary Hospital, Kone Primary Hospital, Lalibela General Hospital, Tefera Hailu Memorial Hospital and Woldia Comprehensive Specialized Hospital.
Study Design and Study Population
A hospital-based mixed cross sectional study design was conducted. Study populations were those chronic disease patients in the North Wollo and Waghimra zone hospitals who were present during the data collection period. Since this study aim was to assess the prevalence of armed conflict induced treatment interruption, its outcome and associated factors, we recruited those participants who had follow up before the war and came to chronic OPD during the data collection period. Among those chronic disease patients newly diagnosed (after war) patients and mentally ill patients were excluded from the study, respectively.
Sample Size Determination and Sampling Techniques
The sample size was determined by using a single population proportion formula by assuming a 5% margin of error, and a proportion (p) of 50% and 95% confidence interval and 5% non-response rate. Since there were fewer than 10,000 patients with chronic diseases overall, the adjustment formula was employed, and the 5% non-response rate was also taken into account. Based on this the actual sample size was 399.
Mersa Primary Hospital, Meket Primary Hospital, Kobo Primary Hospital, Lalibela General Hospital, Tefera Hailu Memorial Hospital and Woldia Comprehensive Specialized Hospital were chosen among the governmental hospitals in the North Wollo and Waghimra zone. Following a list of all chronic illness patients (including those with diabetes, heart disease, HIV/AIDS and hypertension), the entire sample size was proportionally divided among the populations of each institution (ie n×total population of sources in each hospital/total population of sources over the whole research region). The appropriate sample size was enrolled using the consecutive sampling procedure.
Measurement
Quantitative data were collected through kobo toolbox application. A checklist consisting of socio-demographic, personal and other possible information adopted from different literature had been used. Focus group discussions and a questionnaire about chronic disease and the effects of war, which included questions about displacement, the death of a relative and home destruction, were used to gather qualitative data. Patients who visited the hospital during the war as well as health care professionals were also asked to respond. Patients with chronic diseases who were comparable to the research population but were excluded from the actual study were used as pre-test subjects for the questionnaire. For one day, data collectors received instruction on the study’s goal and data gathering methods.
Data Management and Analysis
Every day, the collected data were examined for completeness. Disclosure of the identities or any other personal information ensured confidentiality. Before data entry began, questions that were not completed were removed. Epi Info software version 4.2.0.0 was used to validate, code and input the data before it was exported and analysed using SPSS software version 24. Frequencies and percentages from the data displayed in the tables and graphs were utilized. The quantitative data were described using the mean, SD and 95% CI. The relationship was assessed using multiple logistic regressions, and thematic analysis was used to analyse the qualitative data.
Results
Socio-Demographic Characteristics
A total of 399 questionnaires were distributed through kobo toolbox application to the study participants with a response rate of 99.2% (396). From the total of 396 respondents, 204 (51.1%) were female and 192 (48.1%) were in the age range between 20 and 86 years. The mean ages of the participants were 48.36 ± 14.0 years. Study participants from Lalibela General Hospital constituted the largest proportion, 100 (25.3%), of the study population. With respect to their marital status, the majority 236 (59.6) of the respondents were married and 52 (13.1%) of the participants were single (Table 1).
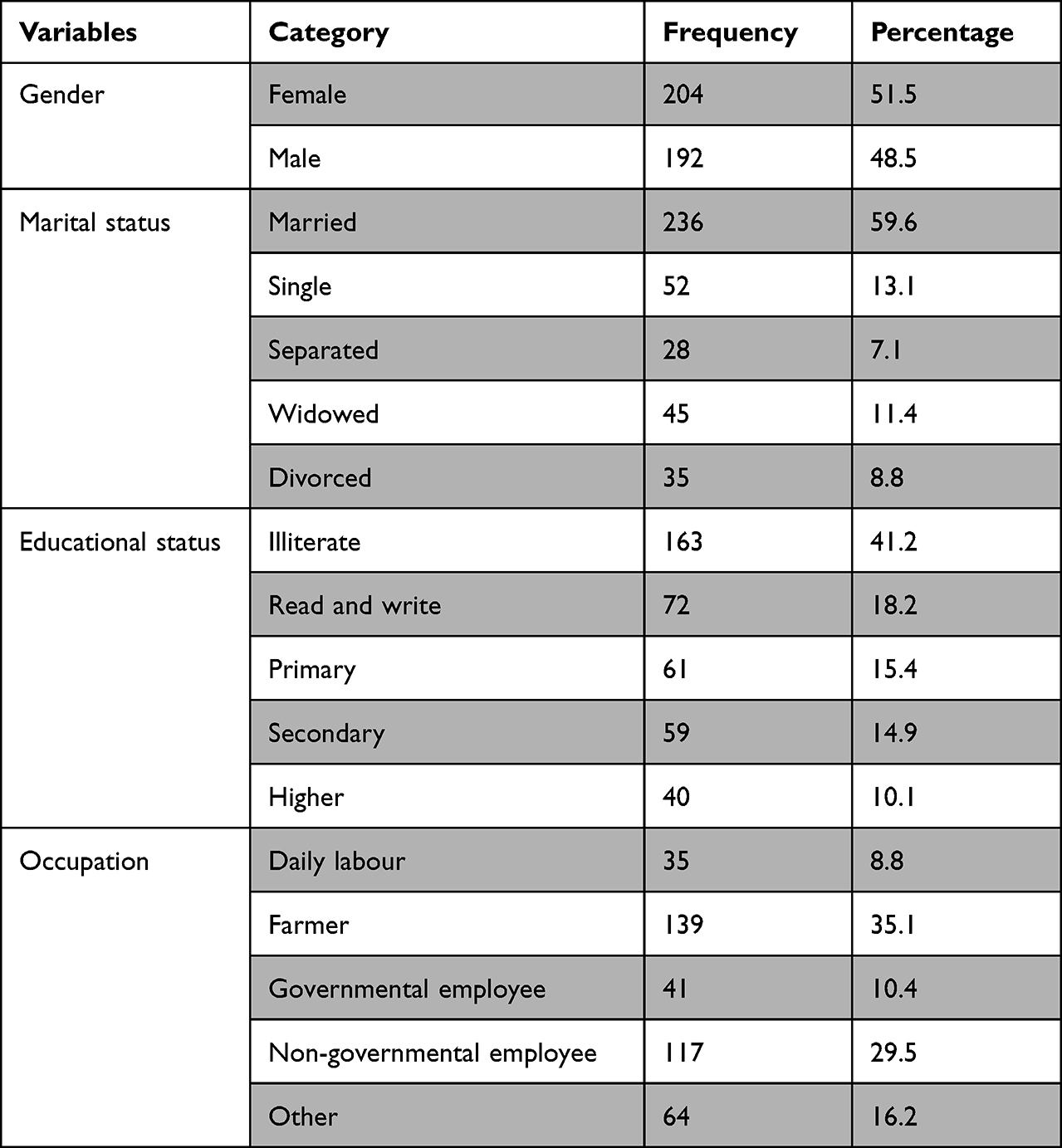 |
Table 1 Socio-Demographic Characteristics of Study Participants at North Wollo and Wagehemra Zone Hospitals (n=396) |
Personal Information of the Study Participants
Among all those who took part in the research (396), 126 (31.8%) patients live with HIV/AIDS, 121 (30.6%) patients with diagnosed hypertension, 91 (23.0%) diagnosed diabetes mellitus and 20 (5.1%) of the participants diagnosed congestive heart failure. Likewise, 24 (5.22%) of the patients were diagnosed with comorbid disease like 0.3% diagnosed with CHF and HTN, and 4.3% of the patients diagnosed DM and HTN. The mean duration of the disease was 4 years (SD: 4 years), in the range between 0.83 and 22 years (Table 2).
Availability of Health Service During the War
The patients were questioned regarding the availability of health service during the war. The result showed that 59.1% answered that there was no health service during the war and 40.9% answered that there was available health service during the war. Among 234 (59.1%) study participants, 105 (26.5%) of the participants had follow up at the time of the war and 57 (14.4%) of the participants had no follow up during the war.
Availability of Medication During the War
Among the total study participants, 149 (37.6%) stated that there was medication during the war and 247 (62.4%) stated that there was no treatment during the war. Among the total participants, 140 (35.4) had taken their medications regularly (Table 2).
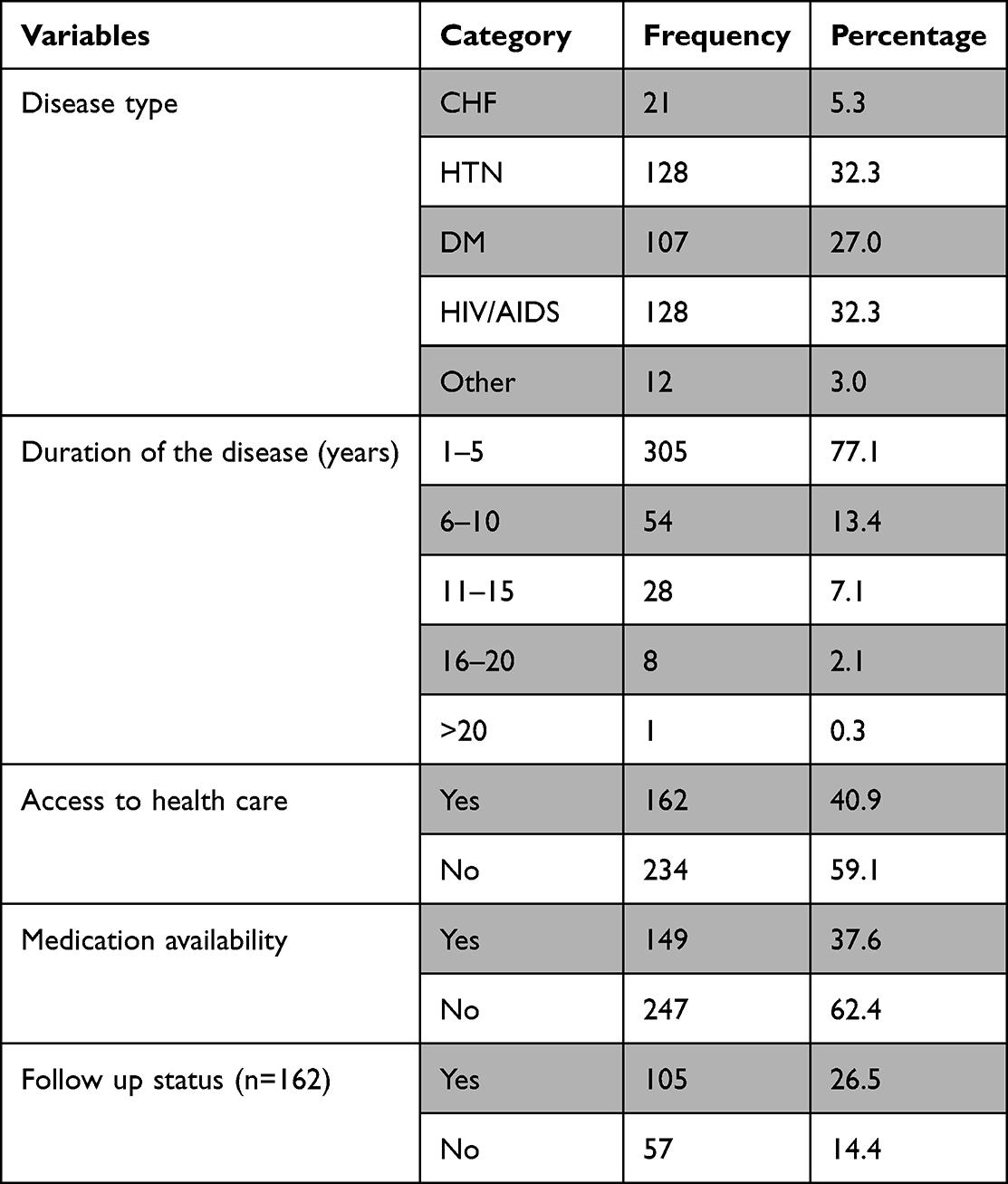 |
Table 2 Personal Information of Chronic Disease Patients (n=396) |
Treatment Interruption Prevalence and Outcome
Among the study participants, 64.6% (95% CI: 0.00–0.009) did not take their treatment, 21.35% stated that they had stopped all their treatments for 1-month duration, 22.1% had stopped all their medications for 2 months, 14.1% for 3 months, 5.8% for 4 months and 1.3% for 5 months. Among 64.6% patients who had their treatment interrupted, 42.9% developed negative consequences related to treatment interruption and the rest 21.7% did not develop any negative consequences (Figure 1).
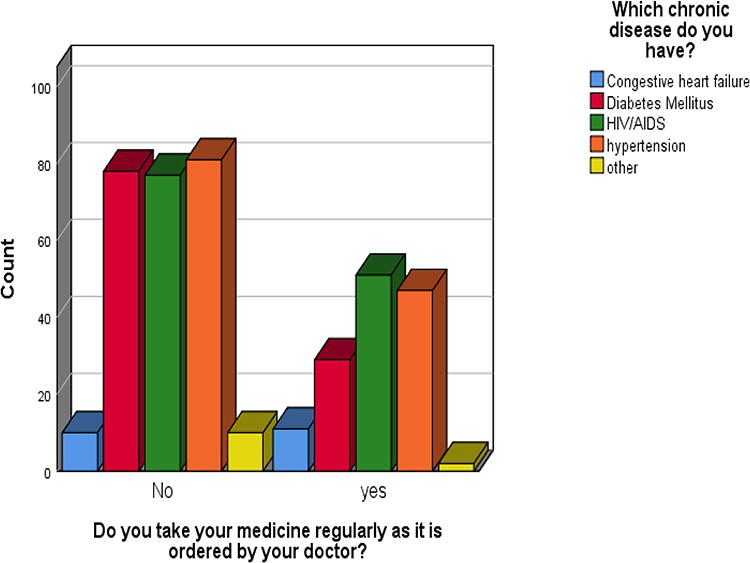 |
Figure 1 Prevalence of treatment interruption among chronic disease patients in North Wollo and Wagemra zone hospitals (n=256). |
Factors Associated with Armed Conflict Induced Treatment Interruption
Findings from the binary logistic regression analysis noted that treatment interruption is significantly associated with being a farmer (p value: 0.002, OR: 3.116, 95% CI, 1.364–8.688), service availability (p value: 0.028, OR: 0.2, 95% CI: 0.048–0.839), follow up status and perceived high stress (p value; 0.02, OR; 0.95, 95% CI, 0.021–0.424). However, in the multivariable logistic regression analysis, only health service availability and perceived high stress (AOR: 4.724, 95% CI, 2.175–10.262) remained significantly associated with increased occurrence of treatment interruption.
Poor Availability of Health Service Related to War
Even though there was no health care service during the time, the drugs collected through different means were distributed for the participants by the health care workers who were there during the time. The condition was described as:
… When arriving at the hospital there was nothing to get service, unfortunately I had got health care worker and he gave me some medications. But I was not comfortable with them and asked repeatedly about the correctness of the drug. He clearly described about the drug type. (Participant 1)
We couldn’t get medications in hospital due to poor service availability even if medications were available in some private pharmacy but we couldn’t buy it due to increased price of medication it was so expensive related to previous price … (Participant 2)
The reason behind for treatment interruption was mentioned by some of the participants:
… during the conflict there was no one who could help me to get to the hospital and there was no transportation. I also heard people were taking drugs out of the hospitals pharmacy without the doctor’s permission so I did not want to take unprescribed medication so I chose to stay at home. (Participant 3)
Another participant stated:
I visited the hospital to be treated but I didn’t get any help and there was no insulin by the time. So I started to ask in the private pharmacies but I could not find any. (Participant 4)
War and Treatment Interruption Outcome
One participant explained his lived experience regarding the outcome of treatment interruption:
… because I run out of medication for my pressure I started using herbal medicine like Garlic, honey “Feto”, Black Cumin which I heard they are important for health from some medias. And as it is known hypertension is a killer so I do not think I would develop complication. Those herbal medicines helped me to stay healthy. (Participant 5)
Other participants stated:
I had headache, fatigue and visual problem … (Participant 6)
There were patients who died due to many factors one to be listed was medication unavailability; some patients came with complications for example paralysis and high viral load which was assessed immediately after the war. There were 21 patients with high viral load which was many comparing to past … (Participant 7)
Another participant stated that:
… stroke was one of the complications which were found among few patients … (Participant 12)
Other participants explained:
… all most all patients had good clinical outcome except one female patient who develop Steven Johnson syndrome … (Participant 13)
Among the study participants one of the participants said that:
because of medication unavailability, I was developed infections on my legs and I was unable to walk from one place to the other. (Participant 8)
Another participant tells us:
… because of treatment interruption, she lost her child because of abortion and she lost her husband. (Participant 9)
A health care professional who was working at an ART clinic stated that:
… patients switch their treatment regimen from 1st line to 2nd line and vice versa in addition 9 patients among patients with ART died because of medication unavailability. (Health care professional 1)
Discussion
This study assessed the prevalence of armed conflict induced treatment interruption among chronic disease patients and the treatment interruption outcome as well as associated factors related to treatment interruption. Around 399 participants were involved in the study. The prevalence of armed conflict induced treatment interruption among chronic disease patients was 64.6%.
The prevalence of armed conflict induced treatment interruption among DM and HIV/AIDS patients was almost similar, which is 19.7% and 19.4% respectively. Compared with other studies, our finding is higher than that of 8.4% in Yemen which is a cross sectional study conducted to assess the effect of war on diabetes control.15
However, the finding is lower than a study done in Nairobi, Kenya (71%) which was conducted on the effect of war on treatment interruption among HIV/AIDS patients.14 This may be due to difference in sample size. Compared with the study conducted in Congo 7.57% of prevalence of ART interruption which is lower than our finding, the sample size may be the cause of the variation.16
The study revealed that more than half of the participants (59.1%) did not get access to health care which is due to lack of transportation, lack of available medication and displacement of hospital staff, which is supported by the studies conducted in Congo and Sarajevans as the study stated that armed conflict causes poor health care services to many populations which is due to distance and insecurity and drug supply chain interruptions; in addition to this, lack of transportation options can significantly hinder access to care.9,16,17
In this study 42.9% participants developed negative consequences related to treatment interruption. As the study showed that treatment interruption affects physiological like mortality, develop complications like stroke, hypoglycaemia, infections and generalized symptoms, psychological, due to discontinuation of the medications they feel like they died early and had stress, economic and social conditions of the participant. This finding supported by the study conducted in Sarajevans which stated that, nearly half of the subjects18 reported hypoglycaemic attacks, two patients were hospitalized because of hypoglycaemic coma and 10 reported severe attacks requiring medical intervention.17
Regarding the pattern of treatment interruption this study showed that some participants switch their medications from first line to second line and vice versa; in addition they take their neighbours' medications which might cause drug resistance. This finding is supported by the study conducted in South Africa which stated that conflict-related unplanned treatment interruptions in ART have negative effects on HIV treatment interruption outcomes including increased morbidity and mortality, as well as development of drug resistance with serious implications for future treatment.18
Male gender was associated with 1.37 times greater odds of treatment interruption (95% CI, 1.07–1.76), and travel times of three or more hours were associated with 1.86 times greater odds of treatment interruption compared to the referent group (95% CI, 1.28–2.71) in the Nairobi study. Travel time to clinic and length of time on ART are also factors associated with treatment interruptions. While travel distance to the clinic and the length of time on ART were factors leading to treatment interruptions in our research, they were also factors in the Nairobi trial. Gender, however, was not substantially linked with treatment interruption.
Our study showed that some participants lost their family member due to treatment interruption. This finding is supported by the study conducted in Yemen which stated that 10% of the participants had lost a 1st or 2nd degree relative from war induced treatment interruption.15
Strength and Limitation of the Study
Our study’s strength was the use of both quantitative and qualitative study approaches. As a shortcoming, it did not evaluate the research participant’s pre-war setting or the absence of comparable unaffected groups. As a result, it did not compare the health care delivery system in pre- and post-war environments. Due to facility damage from the conflict, it was also challenging to get data from various offices.
Conclusion
This study aimed to assess the prevalence of armed conflict induced treatment interruption and its outcome and associated factors. It was discovered that armed conflict increased the prevalence of treatment interruption; it was high (64.6% or 264) among 399 study participants. Poor access to health care, medication unavailability, lack of transportation and lack of follow up are the variable identified as factors which increase the treatment interruption prevalence related to armed conflict. Furthermore, treatment interruption has poor outcome which results in morbidity, mortality, lifelong complications, disability, psychological and economic impact. Therefore, all concerned bodies like governmental or non-governmental institutions make policies and programs to support the unique needs of conflict-affected individuals in North Wollo and Waghimra zone hospitals that address barriers to treatment and care. North Wollo and Waghimra zone hospitals should provide psychosocial support for individuals who were affected by conflict and health care professionals should initiate a treatment regime for those who interrupt their medication related to conflict.
Abbreviations
ART, Anti-retroviral Treatment; DM, Diabetes Mellitus; CHF, Congestive Heart Failure; HIV/AIDS, Human Immuno Virus/Acquired Immuno Deficiency Syndrome; HTN, Hypertension; NCD, Non-Communicable Disease.
Data Sharing Statement
The dataset used and analysed for the current study is available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from Woldia University, College of Health Sciences, Research and Community Service Review Committee (RCSRC). A formal letter for permission and support was written to RHB from Woldia University and finally to selected health facilities. All the study participants were informed about the purpose of the study, and their right to refuse. Written and signed voluntary informed consent was obtained from study subjects prior to distributing the questionnaire. The respondents were informed that the information obtained from them was treated with complete confidentiality and does not cause any harm on them as well as the study participants were informed that the result of the study will be published for the scientific community and the informed consent include publication of anonymized responses. This study was also complying with the Declaration of Helsinki.
Acknowledgment
We would like to thank Woldia University for giving us the chance to prepare this research. We would also like to express our gratitude to study participants, data collectors, supervisors and North Wollo and Waghemra zone health bureau. We also thank Mr. Addisu Getie for his support during manuscript revision.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Geda A, Degefe B. Conflict, Post-Conflict and Economic Performance in Ethiopia. In: Fosu AK, Collier P, editors. Post-Conflict Economies in Africa. International Economic Association Series. London: Palgrave Macmillan; 2005. doi:10.1057/97802305227328
2. Abbink J. The Politics of Conflict in Northern Ethiopia, 2020–2021: a study of war-making, media bias and policy struggle, African Studies Centre Leiden the Netherlands, ASCL Working Paper 152/2021; 2021.
3. Ploch Blanchard L. Ethiopia’s Transition and the Tigray Conflict; 2021.
4. Victor WS, Barry SL. the health impact of war. Int J Inj Contr Saf Promot. 2008;15(4):189–195. doi:10.1080/17457300802404935
5. Poole D; Daniel poole. indirect health consequences of war. Int J Sociol. 2012;42(2):90–107. doi:10.2753/IJS0020-7659420205
6. National cancer institute glossary of cancer terms. Available from: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/chronic-disease.
7. Comlossy M. Chronic disease prevention and management.
8. The power of prevention: chronic disease the public health challenge of the 21st century. Available from: www.cdc.gov/chronicdisease/pdf/2009-Power-of-Prevention.pdf.
9. Marita Mann MNL, Kimaiyo S, Kantor R. Effects of political conflict induced treatment interruptions on HIV drug resistance. NIH. 2013;15(1):15–24.
10. Bendavid E, Boerma T, Akseer N, Langer A. The effects of armed conflict on the health of women and children. Women’s Children’s Health Conflict Settings. 2021;397(10273):522–532.
11. Omar SM, Musa IR, Idrees MB, Adam I. Prevalence risk factor and glycemic control of type 2 diabetes mellitus in eastern Sudan; a community based study. SAGE J. 2019;21(1):1–8.
12. Navneet A, Ambrish S, Seema R. Factors affecting treatment interruption and its correlation with days off with the treatment in diabetes. ERWEJ. 2021;1(2):81–95. doi:10.54136/ERWEJ-0101-10009
13. Prevett M. Chronic non-communicable diseases in Ethiopia-a hidden burden. Ethiop J Health Sci. 2012;22(S):1–2.
14. Pyne-Mercier LD, John-Stewart GC, Richardson BA, et al. The consequences of post-election violence on antiretroviral HIV therapy in Kenya. AIDS Care. 2011;23(5):562–568. doi:10.1080/09540121.2010.525615
15. Al-Sharafi BA, Al-Tahami BA. The effect of war on the control of diabetes in patients with type 2 diabetes mellitus in Yemen: a cross-sectional study. Endocrinol Metab Syndr. 2017;6:270. doi:10.4172/2161-1017.1000270
16. Culbert H, Tu D, O’Brien DP, et al. HIV treatment in a conflict setting: outcomes and experiences from Bukavu, Democratic Republic of the Congo. PLoS Med. 2007;4(5):e129. doi:10.1371/journal.pmed.0040129
17. Kulenovic I, Robertson A, Grujic M, Suljevic E, Smajkic A. The impact of war on Sarajevans with non-insulin-dependent diabetes mellitus. Eur J Public Health. 1996;6(4):252–256. doi:10.1093/eurpub/6.4.252
18. Veenstra N, Whiteside A, Lalloo D, Gibbs A. Unplanned antiretroviral treatment interruptions in Southern Africa: how should we be managing these? Global Health. 2010;6:4. doi:10.1186/1744-8603-6-4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.