Back to Journals » Journal of Inflammation Research » Volume 15
The Diagnostic Value of Various Inflammatory Biomarkers for Diagnosing Periprosthetic Joint Infection is Gender-Specific
Authors Shi W, Jiang Y, Wang Y, Zhang C, Yu T, Li T
Received 27 February 2022
Accepted for publication 11 July 2022
Published 14 July 2022 Volume 2022:15 Pages 3975—3982
DOI https://doi.org/10.2147/JIR.S364309
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monika Sharma
Weipeng Shi,1,2 Yaping Jiang,3 Yingzhen Wang,1 Cailong Zhang,1 Tengbo Yu,1 Tao Li1
1Department of Orthopaedic Surgery, The Affiliated Hospital of Qingdao University, Qingdao, People’s Republic of China; 2Medical Department of Qingdao University, Qingdao, Shandong, People’s Republic of China; 3Department of Oral Implantology, The Affiliated Hospital of Qingdao University, Qingdao, People’s Republic of China
Correspondence: Tao Li; Tengbo Yu, Department of Orthopaedic Surgery, The Affiliated Hospital of Qingdao University, Qingdao, People’s Republic of China, Email [email protected]; [email protected]
Objective: Previous studies have suggested that the diagnostic biomarkers of periprosthetic joint infection (PJI) are largely influenced by gender. In the present study, we aimed to evaluate the diagnostic value of traditional inflammatory biomarkers, fibrinolytic biomarkers (fibrinogen and D-dimer), and C-reactive protein (CRP)/albumin for PJI in different genders.
Methods: A single-center retrospective analysis was performed on revision total hip or knee arthroplasty between June 2013 to June 2021, and the study included 80 patients in the PJI group and 136 patients in the non-PJI group. PJI was diagnosed based on the International Consensus Meeting (ICM) in 2018. The levels of CRP, fibrinogen, erythrocyte sedimentation rate (ESR), D-dimer, and albumin count were determined. Receiver operating characteristic (ROC) curves and Youden’s index were used to evaluate the diagnostic ability of various biomarkers.
Results: The levels of CRP, fibrinogen, D-dimer, ESR, and CRP/albumin were significantly higher in the PJI group (P < 0.001). In PJI of females, the predictive value of CRP was the highest among the five biomarkers, with the area under the curve (AUC) of 0.98. The optimal predictive cut-off for CRP was 8.86 mg/L, with a sensitivity and specificity of 90.2% and 95.7%, respectively. When combined with the other four biomarkers, the AUC of CRP was 0.98, 0.99, 0.98, and 0.99, respectively. In PJI of males, the predictive value of ESR was the highest among the five biomarkers, with an AUC of 0.92. The optimal predictive cut-off for ESR was 14.50 mm/h, with a sensitivity and specificity of 84.6% and 86.6%, respectively. When combined with the other four biomarkers, the AUC of ESR was 0.95, 0.94, 0.93, and 0.97, respectively.
Conclusion: CRP and ESR were excellent biomarkers for diagnosing PJI in female and male patients, respectively, and their combined use with CPR/albumin could provide higher diagnostic value in different genders.
Keywords: gender, biomarkers, periprosthetic joint infection
Introduction
Periprosthetic joint infection (PJI) is a rare but severe complication after total joint infection (TJA), imposing a critical economic burden on society and families.1 Although many studies have reported the value of different biomarkers in the diagnosis of PJI, there exists no single gold standard for PJI. In 2011, the American Musculoskeletal Infection Society (MSIS) identified elevated serum C-reactive protein (CRP) and serum erythrocyte sedimentation rate (ESR) as secondary criteria for its diagnosis.2 CRP and ESR have long been used to detect infections. Although they are not specific to a particular disease and both are increased after TJA and have limited diagnostic utility in acute PJI, ESR and CRP are still considered to be the most routine inflammatory markers for the diagnosis of PJI.3
Accumulating evidence shows that gender can affect the levels of biomarkers, such as CRP, ESR, and so on,4,5 and further impair the accuracy of the diagnosis of PJI, which is attributed to the difference in fat distribution between males and females, the influence of sex hormones, and their effects on gene expression and immune system.6,7 Sex-based differences in immunity contribute to differences in infection susceptibility between men and women.8 In addition, there are also differences in fibrinogen and D-dimer levels between males and females.9,10 Moreover, it is also known that the infection rate after TJA is significantly higher in male patients (1.9%) compared with female patients (1.4%).11
The current diagnostic criteria of PJI do not take demographic variables (such as gender) of patients into account when calculating the positive threshold for biomarkers. Since biomarker levels are related to gender, it is reasonable to speculate that the cut-off values are sex-dependent as well. However, the area under the curve (AUC) and optimal predictive cut-off values reported by all the studies so far are unisex.
In the present single-center retrospective cohort study, we aimed to (1) determine the value of traditional inflammatory biomarkers (CRP and ESR), fibrinolytic biomarkers (fibrinogen and D-dimer), and CRP/albumin for diagnosing PJI in different genders; and (2) identify the most suitable combination of biomarkers for different genders.
Methods
Study Population
This study was approved by the institutional review board of our hospital, and the procedures used in this study complied with the Declaration of Helsinki. A total of 271 patients who underwent revision hip or knee arthroplasty in our institution from June 2013 to June 2021 were included in this single-center retrospective study. Patients diagnosed with a periprosthetic fracture or prosthetic dislocation (n = 28) were first excluded, as these were more likely to be related to trauma rather than infection. Moreover, 24 patients who had comorbidities, including autoimmune diseases (n = 5), malignancies (n = 3), and hematological diseases, and used anticoagulants (n = 16) were also excluded. In addition, patients with incomplete information (n = 3) were also excluded from the study cohort. Finally, there were 80 patients with a preoperative diagnosis of PJI, and 136 patients received treatment for aseptic revision TJA. PJI was defined according to the International Consensus Meeting (ICM) in 2018,11 and aseptic revisions were considered cases undergoing revision for aseptic loosening, joint instability, and unexplained pain.
Data Extraction
In the present study, all included patients were independently grouped by gender and then studied separately. The basic information of all patients, including age, gender, joint, comorbidities, and treatments, and the laboratory test results were extracted using the electronic medical record system of our institution. Fasting venous blood samples were collected on the following day of admission and sent to the clinical laboratory of our hospital within 1 h for blood routine examination and coagulation examination, including CRP, ESR, fibrinogen, D-dimer, and albumin.
The biomarker testing was performed as previously described.11 Briefly, the levels of CRP, ESR, fibrinogen, D-dimer, and albumin were assessed by nephelometric immunoassay, Westergren method, Clauss method, turbidimetric immunoassay, and colorimetry (Bromocresol Green, BCG), respectively. In addition, joint fluid/pus and periprosthetic tissues or bone were collected intraoperatively and then sent to the laboratory for aerobic and anaerobic cultures and histopathologic examination for patients with confirmed or suspected PJI.
Statistical Analyses
All statistical analyses were performed with the SPSS version 26.0 (IBM Inc., Armonk, NY, USA). The Kolmogorov–Smirnov test was used to assess whether continuous variables conformed to a normal distribution. Normally distributed data were expressed as mean ± standard deviation (SD) and were investigated using the independent-sample t-tests. If data did not follow a normal distribution, these data were expressed as median (interquartile range), and the log transformation was applied, followed by independent-sample t-tests. A P less than 0.05 was considered statistically significant. The receiver operating characteristic curves (ROC), AUC, and 95% confidence interval (CI) were used to determine the diagnostic value of CRP, fibrinogen, D-dimer, ESR, and CRP/albumin. The optimal cut-off value, positive predictive value (PPV), and negative predictive value (NPV) of biomarkers were determined using Youden’s index. The AUC values were categorized into excellent (0.900–1.000), good (0.800–0.899), fair (0.700–0.799), poor (0.600–0.699), and no diagnostic ability (0.500–0.599).14
Results
Demographic Characteristics of All Patients
Of the 216 included patients, there were 110 females and 106 males. In females, there was no significant difference in age between the PJI group (n=41) and the non-PJI group (n=69), while patients in the PJI group had a higher body mass index (BMI) and a more significant proportion of knees compared with the non-PJI group (P=0.032, P=0.003). In males, there were no significant differences in age and BMI between the PJI group (n=39) and the non-PJI group (n=67). Similar to females, the proportion of knees in the PJI group was also higher compared with the non-PJI group (P<0.001) (Table 1).
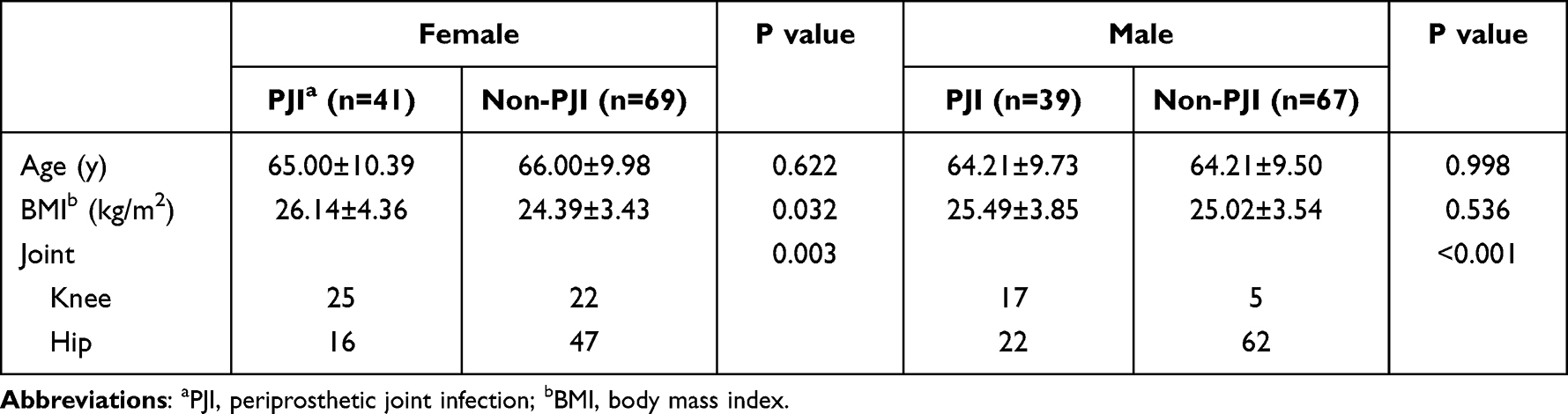 |
Table 1 Demographic Characteristics of All Patients |
Diagnostic Value of Biomarkers in Different Genders
Regardless of gender, biomarker levels and ratios (CRP/albumin) were significantly increased in the PJI group compared with the non-PJI group (P < 0.001) (Table 2). In females, Figure 1A and Table 3 show that the AUC (95% CI) of the five biomarkers was 0.98 (0.951, 1.000), 0.89 (0.826, 0.953), 0.79 (0.705, 0.879), 0.93 (0.882, 0.976), and 0.96 (0.914, 1.000), respectively. Based on the Youden’s index, the optimal cut-off for CRP was 8.86 mg/L with the highest sensitivity (90.2%) and specificity (95.7%) among the five biomarkers, and the PPV and NPV were 92.5% and 94.3%, respectively, while the sensitivity (65.9%) and specificity (79.7%) of D-dimer were the worst.
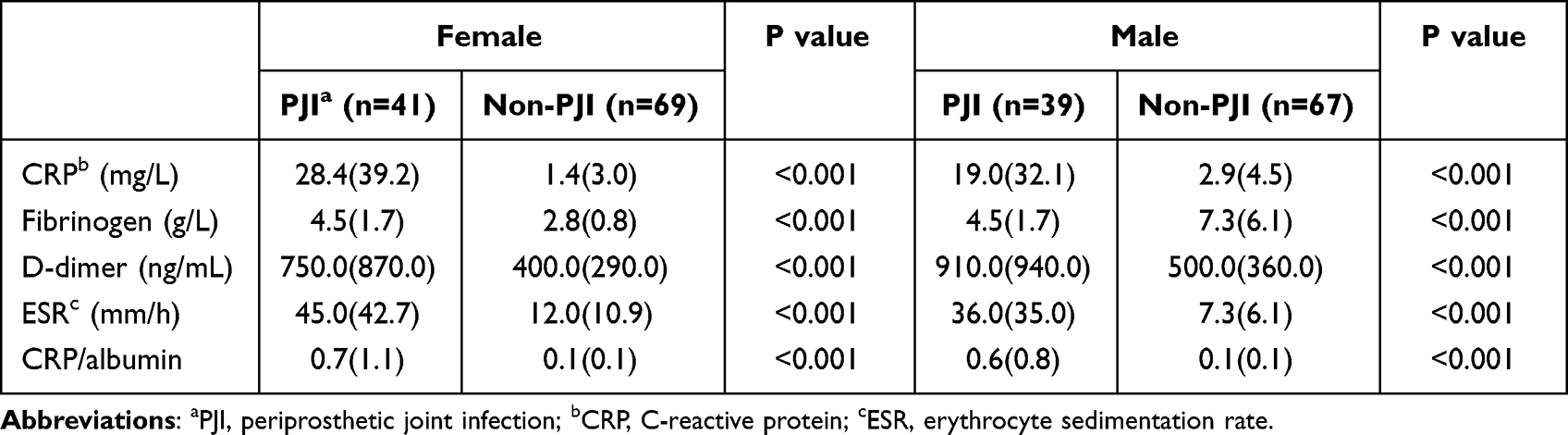 |
Table 2 Comparison of the Levels of Biomarkers in Different Genders |
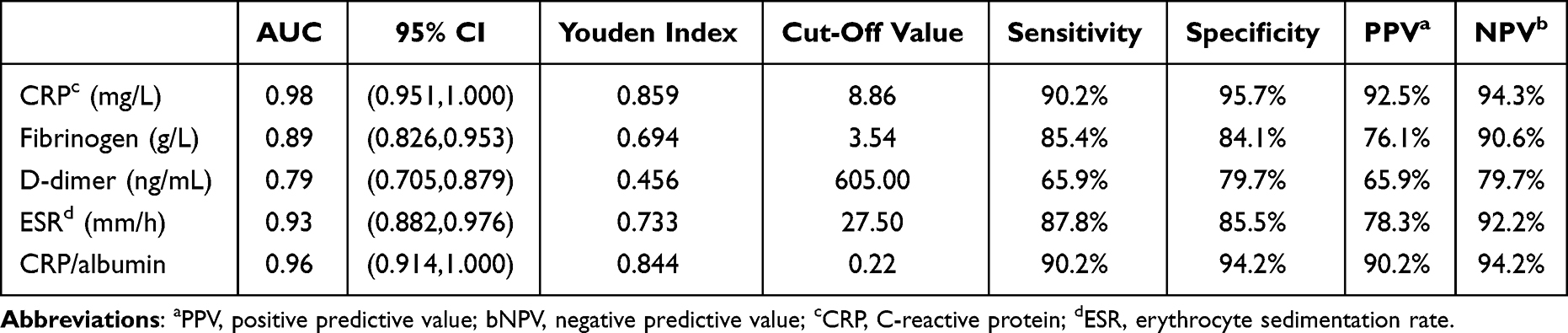 |
Table 3 The Diagnostic Value of Biomarkers in Female PJI |
 |
Figure 1 The ROC curves of plasma CRP, fibrinogen, D-dimer, ESR, and CRP/albumin in female PJI. Among the biomarkers, the AUC of CRP was the largest, and that of D-dimer was the smallest (A). CRP+ CRP/albumin had the best ability to diagnose PJI, while CRP+ESR was the worst (B). |
In males, Figure 2A and Table 4 show that the AUC (95% CI) of two traditional inflammatory biomarkers (CRP and ESR) was 0.83 (0.824, 0.959) and 0.92 (0.874, 0.974), respectively. The AUC of CRP/albumin (0.91) was the second-highest and only slightly lower than ESR. Additionally, the AUC of fibrinogen and D-dimer was 0.87 (0.799, 0.937) and 0.76 (0.662, 0.862), respectively. The optimal cut-off for ESR was 14.50 mm/L, with considerable sensitivity, specificity, PPV, and NPV values of 84.6%, 86.6%, 94.7%, and 75.9%, respectively. The sensitivity of ESR was the highest, followed by CRP/albumin (82.1%), while D-dimer had a sensitivity of only 46.2%. Surprisingly, the specificity of D-dimer (97.0%) was better compared with the other four biomarkers.
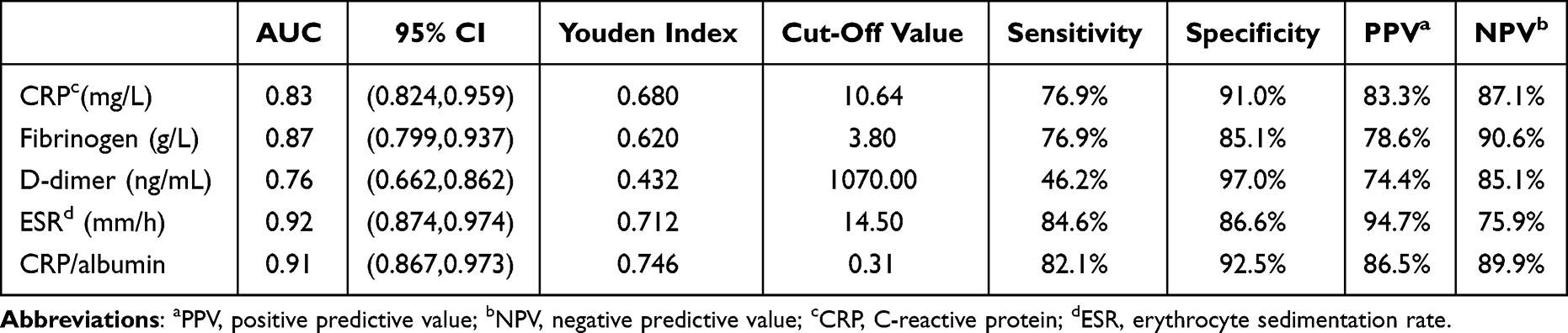 |
Table 4 The Diagnostic Value of Biomarkers in Male PJI |
 |
Figure 2 The ROC curves of plasma CRP, fibrinogen, D-dimer, ESR, and CRP/albumin in male PJI. Among the biomarkers, the AUC of ESR was the largest, and that of D-dimer was the smallest (A). ESR+ CRP/albumin had the best ability to diagnose PJI, while ESR+D-dimer was the worst (B). |
Results of Multiple Combinatorial Tests for Traditional Biomarkers
In addition, to further improve sensitivity and specificity, we performed multiple combinatorial tests of traditional biomarkers according to the above research results, including serial and parallel tests. The results showed that two traditional biomarkers (CRP and ESR) could provide higher diagnostic value in different genders when combined with CRP/albumin, and all AUC values of combinatorial tests achieved “excellent”. In females, the AUC value of CRP in combination with CRP/albumin (0.99) was the highest, and CRP in combination with ESR had the lowest AUC value (0.98) (Figure 1B). In males, ESR in combination with CRP/albumin had the best ability to diagnose PJI (0.97), while ESR in combination with D-dimer was the worst (0.93) (Figure 2B). Tables 5 and 6 show the sensitivity, specificity, PPV, and NPV of combinatorial tests for PJI in different genders. Serial tests increased specificity and decreased sensitivity, and parallel tests increased sensitivity and decreased specificity. Notably, in females, the specificity of D-dimer was improved from the worst (79.7%) for a single biomarker to the best (100%) for a combined biomarker (with CRP).
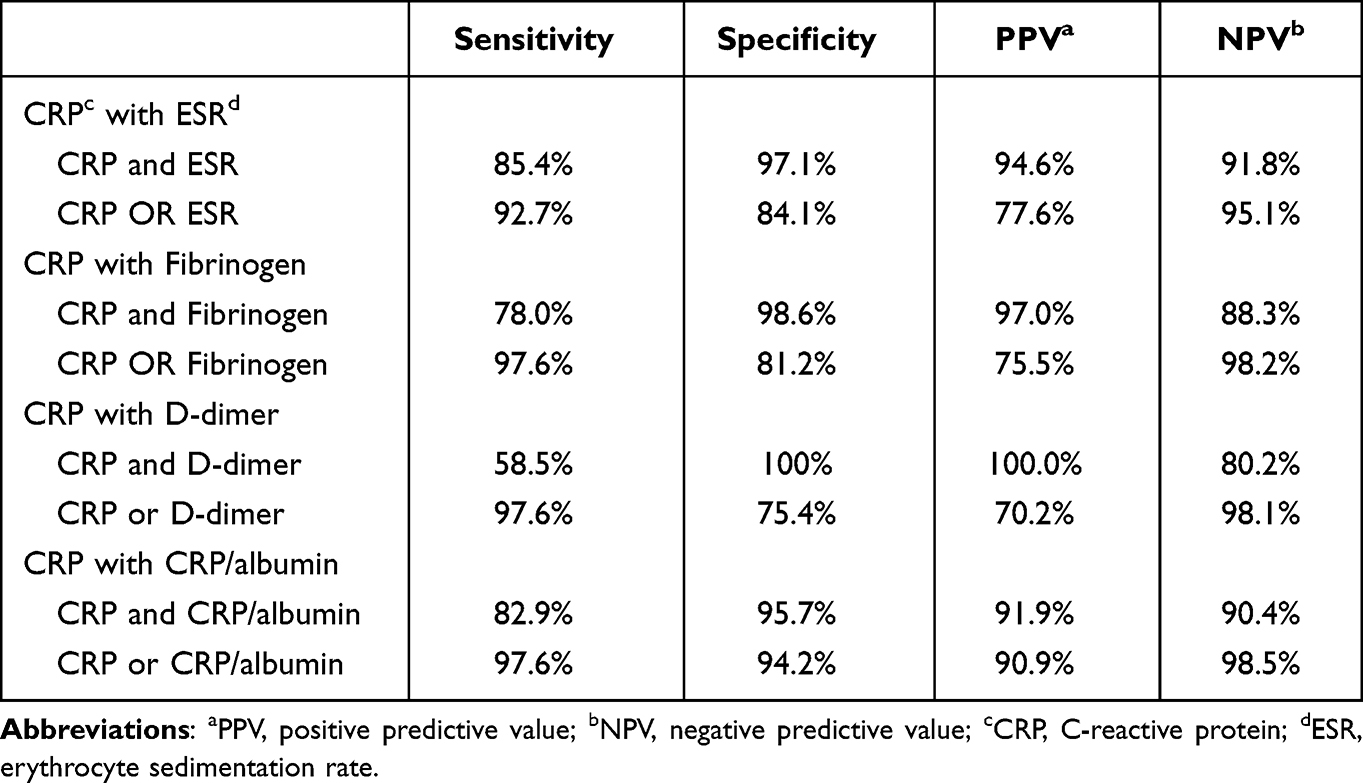 |
Table 5 The Comparison of Sensitivity and Specificity Between Biomarkers in Female PJI |
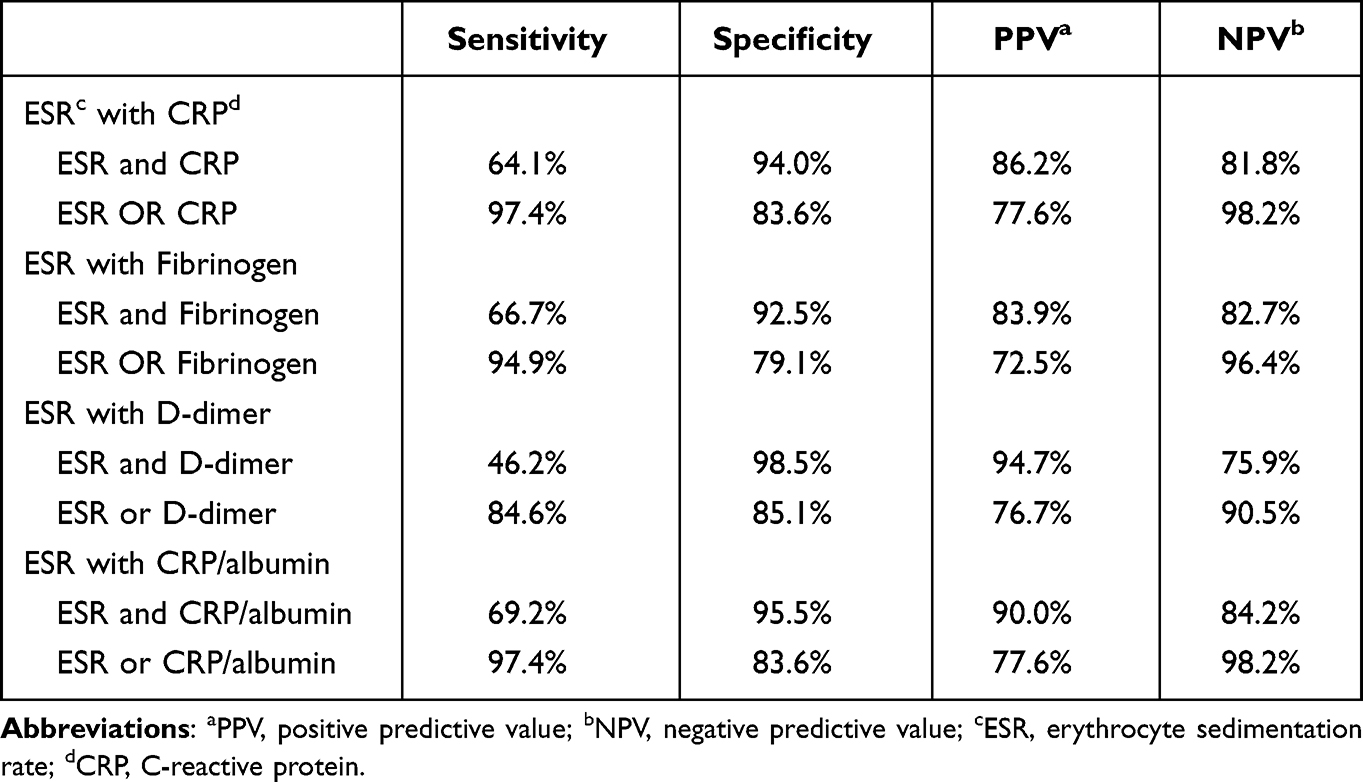 |
Table 6 The Comparison of Sensitivity and Specificity Between Biomarkers in Male PJI |
Discussion
In this single-center retrospective study, we compared the diagnostic value of traditional biomarkers (CRP and ESR), fibrinolytic biomarkers (fibrinogen and D-dimer), and a new biomarker CRP/albumin identified in our previous study for PJI in different genders. To the best of our knowledge, it is the first time to evaluate the diagnostic value of biomarkers by gender of patients. In the present study, CRP and ESR appeared to be excellent biomarkers for diagnosing PJI in female and male patients, respectively. These two traditional biomarkers could further improve the diagnostic value when combined with other markers, especially CRP/albumin.
Likely explanations for the different biomarker levels in females and males are discussed below. The first factor is the gender difference in fat distribution. Females have more subcutaneous fat than males, who deposit fat in the abdominal cavity.15 Moreover, increased central fat accumulation may produce more significant differences in proinflammatory levels between men and women, which may partly explain the difference in CRP levels between different genders.16 In addition, inflammatory markers are significantly elevated in subjects with abnormal BMI, and such a difference is more pronounced in women.15 Obesity is associated with a higher susceptibility to infection, which may lead to elevated CRP.17 Second, higher estrogen levels are associated with higher CRP levels in women. In general, estrogen enhances the immune response, while testosterone reduces the immune response.7 Estrogens modulate both innate and acquired immune function and may contribute to resistance to infection.18 Estrogen levels are also positively correlated with BMI in women,19 so estrogen is indirectly associated with elevated biomarker levels from obesity-related infections. Third, leptin is a hormone produced by adipose tissue, the association of leptin with CRP is independent of other measures of obesity, and such a relationship is only seen in women, suggesting that sex differences in CRP are mediated by leptin in part.20 Fourth, women have significantly higher arachidonic acid (AA) values than men, and the higher AA levels can produce more robust inflammatory and immune responses to bacterial infections.21,22 Fifth, the β-fibrinogen-455A allele is associated with erythrocyte hyper-aggregation in males, which may be regulated by increased fibrinogen concentrations, but not in females.23
Since biomarker levels are associated with gender, it is not difficult to infer that their optimal cut-off value and efficiency for predicting PJI should be sex-dependent. The AUC for each biomarker and cut-off value were different between males and females when the PJI patients were grouped based on gender. Introducing gender-specific AUCs and cut-off values can improve screening results and increase the diagnostic accuracy of PJI. It is not easy to accurately diagnose PJI, and the higher values for sensitivity and specificity reflect a better diagnostic value. Although high sensitivity may lead to unnecessary testing and higher cost for non-PJI patients, it can ensure fewer misdiagnosed patients. CRP and ESR, as traditional inflammatory biomarkers, showed the best single-marker diagnostic value in our study.
In PJI of females, the sensitivity and specificity of CRP at 8.86 mg/L reached 90.2% and 95.7%, respectively, with the AUC of 0.97, which was the highest among the five tested biomarkers. It appeared to be a promising biomarker for diagnosing PJI, closely followed by CRP/albumin. Compared with the excellent results of CRP, D-dimer performed poorly. We found that D-dimer at 605 ng/mL had a sensitivity and specificity of 65.9% and 79.7%, respectively, making it the worst biomarker. Our study had similar results to previous reports.24 Shahi et al have reported that D-dimer is a better marker than CRP and ESR (sensitivity and specificity are 89% and 93%, respectively) because that study includes autoimmune diseases (Rheumatoid Arthritis, Systemic Lupus Erythematosus, and so on), which may cause significant bias in the results. In addition, race (Asian vs European) may also lead to differences in results.25
In PJI of males, ESR emerged as the best-performing marker, with the AUC, sensitivity, and specificity of 0.92, 84.6%, and 86.6%, respectively. Based on our results, the AUC for CRP/albumin (0.91) was only slightly lower compared with ESR, and it also showed good sensitivity (82.1%) and specificity (92.5%) for diagnosing PJI, which was similar to our previous findings.13 As one of the traditional inflammatory biomarkers, ESR is often used as a reference for evaluating other new biomarkers. In 2011, MSIS first identified elevated serum CRP and serum ESR as secondary criteria for diagnosis.13 In the newest modification of the ICM criteria, even though the diagnostic value of D-dimer for PJI still remains controversial, it is given two points, while ESR is given lower points.12 In the present study, ESR received attention for its excellent diagnostic value in PJI of males. However, there are three points that need to note. First, the specificity of D-dimer in PJI was the highest among the five markers (97.0%) in males, while the sensitivity was only 46.2%, indicating that D-dimer in males was a low-sensitivity marker and should be given attention as an exclusive marker rather than a diagnostic marker. D-dimer did not appear to have this effect in female PJI. Second, the optimal predictive cut-off of ESR in male PJI was only 14.5 mm/h, lower than reported in previous studies. This discrepancy might be attributed to the fact that few patients receive antibiotic treatment. However, we could not determine one by one due to limited clinical information. Moreover, the previous study does not distinguish between men and women, while the physiological ESR of women is higher compared with men, resulting in a significantly higher final result than our study. Third, the diagnostic value of CRP/albumin ranked second in both female and male PJI patients, just slightly lower than CRP or ESR, proving that CRP/albumin had a promising prospect as a new biomarker for the diagnosis of PJI.
Despite the advantages of the present study, there are several limitations. First, none of the current diagnostic criteria could achieve 100% sensitivity and specificity. Therefore, patients might be misclassified. Second, this study was a single-center retrospective study, and the inherent bias of the data was unavoidable. Moreover, the sample size was small, and the conclusions needed to be verified in a large-sample, multi-center, prospective study. Third, due to limited clinical information, no subgroup analysis was conducted to assess the effects of confounding factors, such as antibiotic use, causative microorganisms, and comorbidities, on the results of the current study, which was the most significant limitation of our study and would also be the focus of our subsequent research.
Conclusions
Taken together, compared with fibrinolytic biomarkers, traditional inflammatory biomarkers (CRP and ESR) were more reliable for the diagnosis of PJI in different genders, and their combined use with CPR/albumin could further improve their diagnostic value.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board (IRB) Affiliated Hospital of Qingdao University. All personal details were erased before analysis to cover patient data confidentiality and comply with the Declaration of Helsinki.
Consent for Publication
The co-authors agreed on the final version of the manuscript.
Funding
Qingdao Traditional Chinese Medicine Science and Technology Project; Grant number: 2021-zyym28; Science and technology Development Project of Shandong Geriatric Society; Grant number: LKJGG2021W082.
Disclosure
The authors declare they have no financial and or non finanicial interests.
References
1. Kurtz SM, Lau E, Watson H, et al. Economic burden of periprosthetic joint infection in the United States. J Arthroplasty. 2012;27(8 Suppl):61–65. doi:10.1016/j.arth.2012.02.022
2. Workgroup Convened by the Musculoskeletal Infection Society. New definition for periprosthetic joint infection. J Arthroplasty. 2011;26(8):1136–1138. doi:10.1016/j.arth.2011.09.026
3. Shohat N, Bauer T, Buttaro M, et al. Hip and knee section, what is the definition of a Periprosthetic Joint Infection (PJI) of the knee and the hip? Can the same criteria be used for both joints?: Proceedings of International Consensus on Orthopedic Infections. J Arthroplasty. 2019;34(2S):S325–S327. doi:10.1016/j.arth.2018.09.045
4. Pieroni L, Bastard JP, Piton A, et al. Interpretation of circulating C-reactive protein levels in adults: body mass index and gender are a must. Diabetes Metab. 2003;29(2 Pt 1):133–138. doi:10.1016/s1262-3636(07)70019-8
5. Padua FG, Yayac M, Parvizi J. Variation in inflammatory biomarkers among demographic groups significantly affects their accuracy in diagnosing periprosthetic joint infection. J Arthroplasty. 2021;36(4):1420–1428. doi:10.1016/j.arth.2020.10.036
6. Festa A, D’Agostino
7. McClelland EE, Smith JM. Gender specific differences in the immune response to infection. Arch Immunol Ther Exp (Warsz). 2011;59(3):203–213. doi:10.1007/s00005-011-0124-3
8. Yee MK, Goldsmith E, Watson NB, et al. Differential sensitivity to IL-12 drives sex-specific differences in the CD8+ T cell response to infection. Immunohorizons. 2019;3(4):121–132. doi:10.4049/immunohorizons.1800066
9. Danesh J, Danesh J, Lewington SG, et al. Plasma fibrinogen level and the risk of major cardiovascular diseases and nonvascular mortality: an individual participant meta-analysis. JAMA. 2005;294(14):1799–1809. doi:10.1001/jama.294.14.1799
10. Rudnicka AR, Rumley A, Lowe GDO, et al. Diurnal, seasonal, and blood-processing patterns in levels of circulating fibrinogen, fibrin D-dimer, C-reactive protein, tissue plasminogen activator, and von Willebrand factor in a 45-year-old population. Circulation. 2007;115(8):996–1003. doi:10.1161/CIRCULATIONAHA.106.635169
11. Brown MJ, Koh NP, Bell SW, et al. Age and gender related differences in infection, thromboembolism, revision and death in knee arthroplasty in a Scottish population. Scott Med J. 2020;65(3):89–93. doi:10.1177/0036933020936282
12. Parvizi J, Tan TL, Goswami K, et al. The 2018 definition of periprosthetic hip and knee infection: an evidence-based and validated criteria. J Arthroplasty. 2018;33(5):1309–1314. doi:10.1016/j.arth.2018.02.078
13. Shi W, Wang Y, Zhao X, et al. CRP/Albumin has a promising prospect as a new biomarker for the diagnosis of periprosthetic joint infection. Infect Drug Resist. 2021;14:5145–5151. doi:10.2147/IDR.S342652
14. Xu H, Xie J, Yang J, et al. Plasma fibrinogen and platelet count are referable tools for diagnosing periprosthetic joint infection: a single-center retrospective cohort study. J Arthroplasty. 2020;35(5):1361–1367. doi:10.1016/j.arth.2019.12.015
15. Cohen E, Margalit I, Shochat T, et al. Markers of chronic inflammation in overweight and obese individuals and the role of gender: a cross-sectional study of a large cohort. J Inflamm Res. 2021;14:567–573. doi:10.2147/JIR.S294368
16. Hermsdorff HH, Volp AC, Puchau B, et al. Contribution of gender and body fat distribution to inflammatory marker concentrations in apparently healthy young adults. Inflamm Res. 2012;61(5):427–435. doi:10.1007/s00011-011-0429-z
17. Ishii S, Karlamangla AS, Bote M, et al. Gender, obesity and repeated elevation of C-reactive protein: data from the CARDIA cohort. PLoS One. 2012;7(4):e36062. doi:10.1371/journal.pone.0036062
18. Klein SL. Hormonal and immunological mechanisms mediating sex differences in parasite infection. Parasite Immunol. 2004;26(6–7):247–264. doi:10.1111/j.0141-9838.2004.00710.x
19. Lukanova A, Lundin E, Zeleniuch-Jacquotte A, et al. Body mass index, circulating levels of sex-steroid hormones, IGF-I and IGF-binding protein-3: a cross-sectional study in healthy women. Eur J Endocrinol. 2004;150(2):161–171. doi:10.1530/eje.0.1500161
20. Abdullah SM, Khera A, Leonard D, et al. Sex differences in the association between leptin and CRP: results from the Dallas Heart Study. Atherosclerosis. 2007;195(2):404–410. doi:10.1016/j.atherosclerosis.2006.10.022
21. Rondanelli M, Klersy C, Perna S, et al. Effects of two-months balanced diet in metabolically healthy obesity: lipid correlations with gender and BMI-related differences. Lipids Health Dis. 2015;14:139. doi:10.1186/s12944-015-0131-1
22. Furman D, Hejblum BP, Simon N, et al. Systems analysis of sex differences reveals an immunosuppressive role for testosterone in the response to influenza vaccination. Proc Natl Acad Sci USA. 2014;111(2):869–874. doi:10.1073/pnas.1321060111
23. Ben AE, Bova I, Berliner S, et al. Gender differences in the expression of erythrocyte aggregation in relation to B beta-fibrinogen gene polymorphisms in apparently healthy individuals. Thromb Haemost. 2006;95(3):428–433. doi:10.1160/TH05-08-0578
24. Xu H, Shang G, Wang Y, et al. Plasma fibrinogen is a reliable marker for diagnosing periprosthetic joint infection and determining the timing of second-stage revision. Int J Infect Dis. 2021;108:220–225. doi:10.1016/j.ijid.2021.05.068
25. Shahi A, Kheir MM, Tarabichi M, et al. Serum d-dimer test is promising for the diagnosis of periprosthetic joint infection and timing of reimplantation. J Bone Joint Surg Am. 2017;99(17):1419–1427. doi:10.2106/JBJS.16.01395
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Clinical Impact of Metagenomic Next-Generation Sequencing for the Diagnosis of Periprosthetic Joint Infection
Li H, Niu E, Fu J, Huang Y, Gao Y, Chai W, Chen J
Infection and Drug Resistance 2023, 16:6521-6533
Published Date: 2 October 2023