Back to Journals » Clinical Epidemiology » Volume 8
The Danish Stroke Registry
Authors Johnsen SP, Ingeman A, Hunborg HH, Schaarup SZ, Gyllenborg J
Received 5 January 2016
Accepted for publication 7 March 2016
Published 25 October 2016 Volume 2016:8 Pages 697—702
DOI https://doi.org/10.2147/CLEP.S103662
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor H Sorensen
Søren Paaske Johnsen,1 Annette Ingeman,1,2 Heidi Holmager Hundborg,1 Susanne Zielke Schaarup,3 Jesper Gyllenborg4
1Department of Clinical Epidemiology, Aarhus University Hospital, 2Registry Support Center of Clinical Quality & Health Informatics (West), The Danish Clinical Registries, Aarhus, 3Department of Neurology, Bispebjerg Hospital, Copenhagen, 4Department of Neurology, Zealand University Hopital, Roskilde, Denmark
Aim of database: The aim of the Danish Stroke Registry is to monitor and improve the quality of care among all patients with acute stroke and transient ischemic attack (TIA) treated at Danish hospitals.
Study population: All patients with acute stroke (from 2003) or TIA (from 2013) treated at Danish hospitals. Reporting is mandatory by law for all hospital departments treating these patients. The registry included .130,000 events by the end of 2014, including 10,822 strokes and 4,227 TIAs registered in 2014.
Main variables: The registry holds prospectively collected data on key processes of care, mainly covering the early phase after stroke, including data on time of delivery of the processes and the eligibility of the individual patients for each process. The data are used for assessing 18 process indicators reflecting recommendations in the national clinical guidelines for patients with acute stroke and TIA. Patient outcomes are currently monitored using 30-day mortality, unplanned readmission, and for patients receiving revascularization therapy, also functional level at 3 months poststroke.
Descriptive data: Sociodemographic, clinical, and lifestyle factors with potential prognostic impact are registered.
Conclusion: The Danish Stroke Registry is a well-established clinical registry which plays a key role for monitoring and improving stroke and TIA care in Denmark. In addition, the registry is increasingly used for research.
Keywords: stroke, transient ischemic attack, quality improvement
Background and aim of the database
A stroke is a medical emergency and can cause permanent neurological damage, complications, and death. Stroke is of major importance for public health internationally as stroke is the second most common cause of death globally and is a major cause of disability worldwide.1,2 The 30-day case-fatality among patients with stroke has dropped in recent decades but remains overall between 10% and 20% in most Western populations.
Monitoring the quality of stroke care has a high international priority. The World Health Organization (WHO) Cardiovascular Disease Program aims at developing standards of care as well as feasible surveillance methods to monitor prevention and control initiatives for cardiovascular diseases, including stroke. Furthermore, a number of countries monitor the quality of stroke care at a national level in established stroke registries, for example, Sweden, the US, Germany, and Austria. Denmark first launched national clinical guidelines for the acute treatment and care of patients with stroke in 2003, and they have since been updated regularly. These guidelines recommend early initiation of treatment, care, and rehabilitation, and are in line with international consensus guidelines from the American Heart Association and the European Stroke Organisation.
The Danish Stroke Registry (DSR) was established in 2003 as part of the Danish National Indicator Project, which was a national quality improvement initiative aimed at monitoring and improving quality of care using evidence-based quality of care indicators.3 The DSR is now a nationwide clinical registry and part of The Danish Clinical Registries – a national improvement program, which is an umbrella organization encompassing clinical registries in Denmark. The activities of the registry are coordinated by a multidisciplinary steering group, including physicians, nurses, physiotherapists, and occupational therapists. The members of the steering groups have been appointed by the relevant scientific societies and stakeholders.
Setting
All Danes (total population, aged 18 or older by January 2016: 3,964,146) are provided tax-supported health care by the Danish health care system allowing free access to hospital care and general practitioners. Patients with acute medical conditions, including stroke, are exclusively admitted to public hospitals. All hospitals’ departments regularly treating patients with acute stroke and transient ischemic attack (TIA) are required by law to report data to the DSR. Staff members responsible for data collection have been appointed at all participating departments. Data are collected prospectively and reported to the DSR using a web-based interface.
Study population
All patients (≥18 years) admitted to Danish hospitals with acute stroke, as defined by WHO criteria, that is, an acute disturbance of focal or global cerebral function with symptoms lasting more than 24 hours or leading to death of presumed vascular origin, are eligible for inclusion in the DSR. Only patients with symptom onset within the last week are included. This includes patients with intracerebral hemorrhage and ischemic stroke (International Classification of Diseases tenth edition: I63, infarction; I61, hemorrhage; and I64, unspecified). In addition, patients with TIA (ie, patients with symptoms lasting up to 24 hours) are included. Patients with subarachnoidal or epidural hemorrhage, subdural hematoma, retinal infarct, and infarct caused by trauma, infection, or an intracranial malignant process are excluded. Patients with diffuse symptoms, such as isolated vertigo or headache, and asymptomatic patients with infarct detected only by computed tomography or magnetic resonance imaging scan are also excluded.
The registry included >130,000 events by the end of 2014, including 10,822 strokes and 4,227 TIAs registered in 2014. The sensitivity and predictive value of the registration of patients in the DSR was estimated to be >90% in 2009.4 Although it cannot entirely be excluded that the completeness of the registration and regular assessments of the validity of the registration is always to be recommended in clinical registries, there is no indication based on the number of registered patients and the diagnostic work up of the patients that the registration practice has changed substantially over time.
Quality indicators
A total of 18 process and four result indicators covering the early phase of stroke have been identified by the steering group (Table 1). The process indicators reflect key recommendations from the national clinical guidelines and the DSR consequently monitors the implementation of these guidelines at Danish hospitals. Patients are classified as eligible or noneligible for the specific processes of care depending on whether the stroke team or physician treating the patient identifies contraindications; for example, severe dementia in a patient with ischemic stroke and atrial fibrillation precluding oral anticoagulant therapy or rapid spontaneous recovery of motoric symptoms, making early assessment by a physiotherapist and an occupational therapist irrelevant.
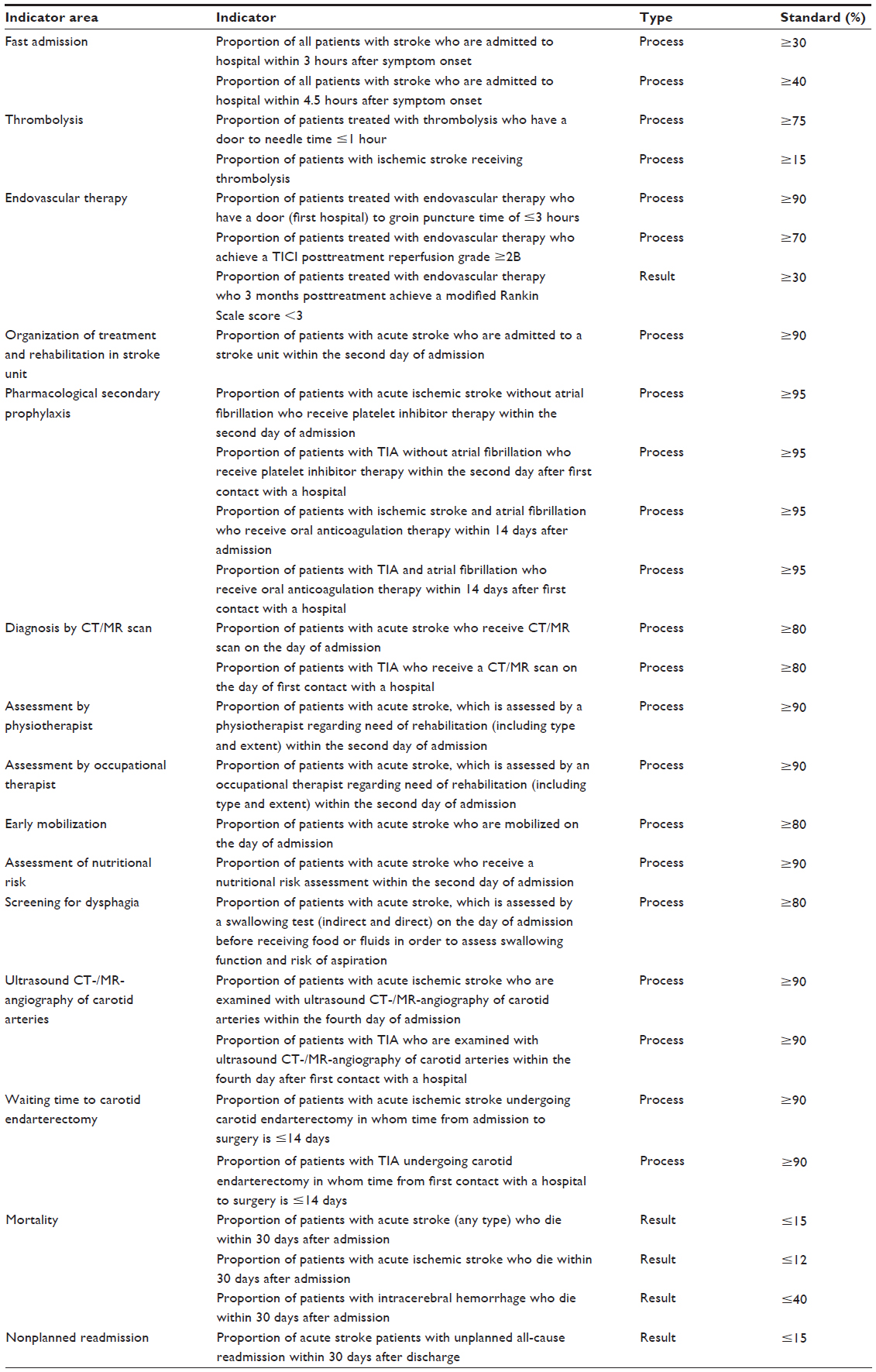 | Table 1 Indicators and standards in the Danish Stroke Register |
A structured audit process is carried out regularly (every year) on a national, regional, and local basis to assess critically the quality of the dataset and results. After the audit process is completed, the data are released publicly with department-level data, including comments on the results from the audit groups and recommendations on how to improve quality of care.5 Improvements over the years have been observed for all quality indicators and for some process indicators the improvements have been dramatic, for example, the proportion of relevant patients fulfilling the indicator has doubled or even tripled.
Main variables
Selected key variables in the DSR are presented in Table 2. Besides the variables used to assess the quality indicators, the DSR also includes data on a range of prognostic factors. These factors are used to characterize the included patients and to take differences in case-mix into account when benchmarking departments or when comparing the same department over time. In addition, supplementary data on intravenous thrombolysis and endovascular therapy are obtained in order to characterize the provided treatments.
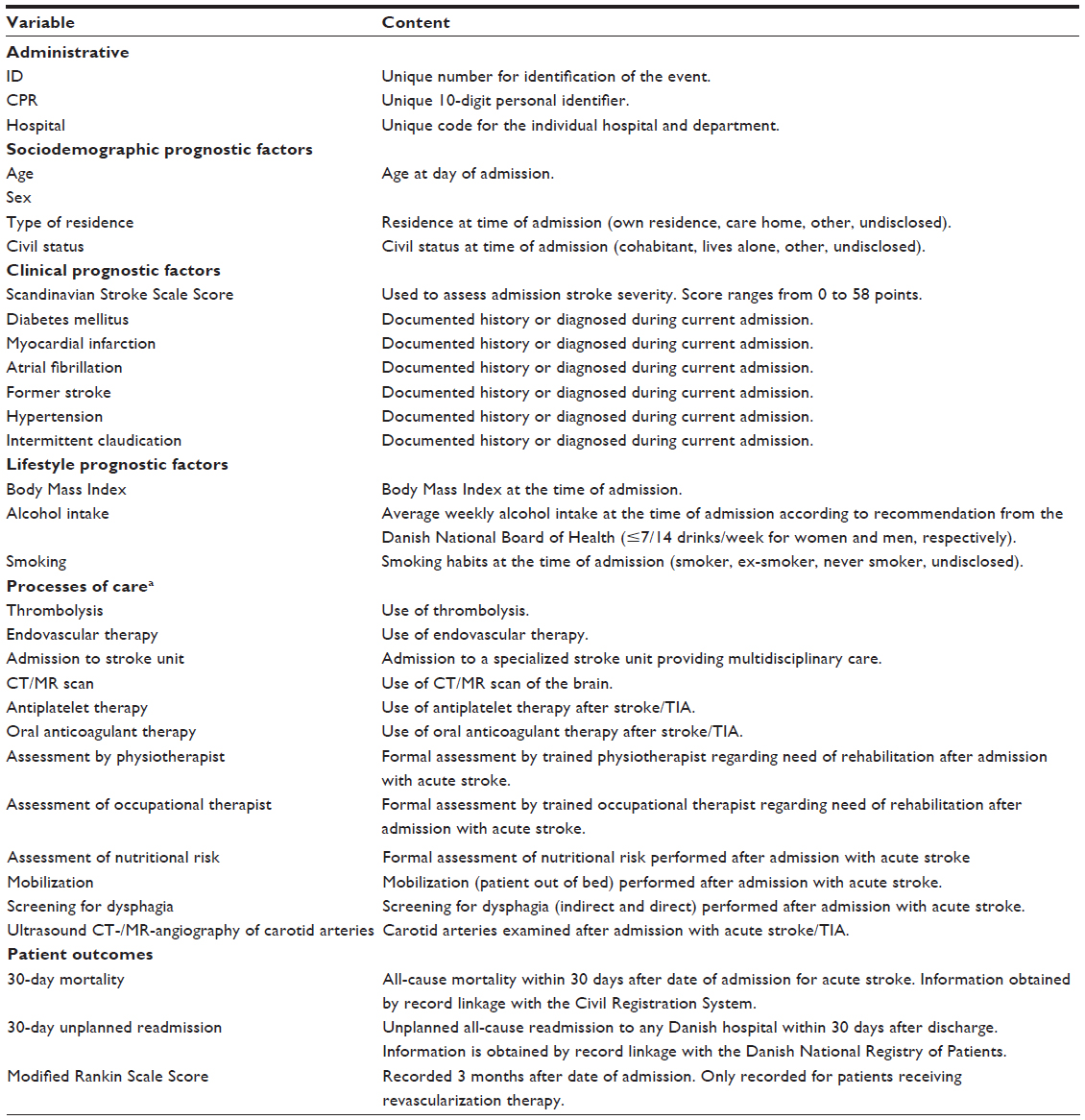 | Table 2 Key variables registered in the Danish Stroke Registry |
Formal validation studies on the registered data have not been conducted; however, the overall quality of the recorded data is most likely high since detailed instructions, including explicit data definitions, are available and data recording practices are examined and discussed by representatives of the hospitals departments reporting to the registry at the yearly audits.
Follow-up
All patients are followed up by individual-level record linkage to other public registries using the civil registry number, which is unique to every Danish citizen and enables unambiguous linkages.
Information on mortality is obtained from the Danish Civil Registration System, which stores daily updated electronic records of all changes in vital status and migration for the entire Danish population, including changes in address, date of emigration, and the exact date of death, since 1968.6
Information on unplanned readmissions are obtained from the Danish National Registry of Patients, which is an administrative nationwide public registry that covers all discharges from somatic hospitals in Denmark since January 1, 1977.7 The data include the dates of admission and discharge and up to 20 diagnoses for every discharge classified, since 1994, according to the Danish version of the International Classification of Diseases tenth edition.
Information on functional level 3 months after the day of admission with acute stroke is assessed using the modified Rankin Score for all patients receiving revascularization therapy (intravenous thrombolysis or endovascular therapy) and recorded directly in the DSR.
Examples of research
The DSR has been used in numerous studies covering a broad range of topics, including traditional clinical epidemiological studies on prognosis8–10 as well as studies on effectiveness of care,11–13 disparities of care,14,15 and health economics.16 The registry has been linked extensively with other public registries in many of these studies.
Administrative issues and funding
The DSR is an approved clinical quality database by the State Serum Institute and the Danish Data Protection Agency. It is funded by the Danish Regions and receives administrative, epidemiological, and biostatistical support from the Danish Clinical Registries. Aggregated data at regional level will be reported annually in a published report, and data will be provided monthly to the regions for use in each region’s information system.
Conclusion
The DSR is a national clinical registry which plays an important role as an information source and quality improvement instrument for stroke and TIA care in Denmark.
Acknowledgment
This paper was funded by the Program for Clinical Research Infrastructure (PROCRIN) established by the Lundbeck Foundation and the Novo Nordisk Foundation and administered by the Danish Regions.
Disclosure
SPJ, AI, and HHH are employees of Department of Clinical Epidemiology, Aarhus University Hospital, which receives funding from the Danish Clinical Registries, Danish Regions, for running the DSR. The authors report no other conflicts of interest in this work.
References
Donnan GA, Fisher M, Macleod M, Davis SM. Stroke. Lancet. 2008; 371:1612–1623. | |
Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367(9524):1747–1757. | |
Mainz J, Krog BR, Bjornshave B, Bartels P. Nationwide continuous quality improvement using clinical indicators: The Danish National indicator project. Int J Qual Health Care. 2004;16 (Suppl 1):i45–i50. | |
Wildenschild C, Mehnert F, Thomsen RW, et al. Registration of acute stroke: validity in the Danish Stroke Registry and the Danish National Registry of Patients. Clin Epidemiol. 2014;6:27–36. | |
Danish Stroke Registry, annual report 2015. Available from: https://www.sundhed.dk/sundhedsfaglig/kvalitet/kliniske-kvalitetsdatabaser/hjerte-kar-sygdomme/apopleksi-nip. Accessed April 11, 2016. | |
Schmidt M, Pedersen L, Sørensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29:541–549. | |
Andersen TF, Madsen M, Jorgensen J, Mellemkjoer L, Olsen JH. The Danish National Hospital Register. A valuable source of data for modern health sciences. Dan Med Bul. 1999;46:263–268. | |
Andersen KK, Olsen TS. The obesity paradox in stroke: lower mortality and lower risk of readmission for recurrent stroke in obese stroke patients. Int J Stroke. 2015;10:99–104. | |
Dehlendorff C, Andersen KK, Olsen TS. Sex disparities in stroke: Women have more severe strokes but better survival than men. J Am Heart Assoc. 2015;4:e001967. | |
Ingeman A, Andersen G, Hundborg HH, Svendsen ML, Johnsen SP. In-hospital medical complications, length of stay, and mortality among stroke unit patients. Stroke. 2011;42:3214–3218. | |
Ingeman A, Pedersen L, Hundborg H, et al. Quality of care and mortality among patients with stroke: a nationwide population-based follow-up study. Med Care. 2008;46:63–69. | |
Svendsen ML, Ehlers LH, Andersen G, Johnsen SP. Quality of care and length of hospital stay among patients with stroke. Med Care. 2009;47:575–582. | |
Ingeman A, Andersen G, Hundborg HH, et al. Processes of care and medical complications in patients with stroke. Stroke. 2011;42:167–172. | |
Palnum KD, Petersen P, Sørensen HT, et al. Older patients with acute stroke in Denmark: quality of care and short-term mortality. A nationwide follow-up study. Age Ageing. 2008;37:90–95. | |
Langagergaard V, Palnum KH, Mehnert F, et al. Socioeconomic differences in quality of care and clinical outcome after stroke: a nationwide population-based study. Stroke. 2011;42:2896–2902. | |
Svendsen ML Ehlers LH, Hundborg HH, Ingeman A, Johnsen SP. Processes of early stroke care and hospital costs. Int J Stroke. 2014;9:777–782. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.