Back to Journals » Clinical Epidemiology » Volume 8
The Danish Schizophrenia Registry
Authors Baandrup L ![]() , Cerqueira C, Haller L, Korshoej L, Voldsgaard I, Nordentoft M
, Cerqueira C, Haller L, Korshoej L, Voldsgaard I, Nordentoft M
Received 15 November 2015
Accepted for publication 19 January 2016
Published 25 October 2016 Volume 2016:8 Pages 691—695
DOI https://doi.org/10.2147/CLEP.S99488
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor H Sorensen
Lone Baandrup,1 Charlotte Cerqueira,2 Lea Haller,3 Lene Korshøj,3 Inge Voldsgaard,4 Merete Nordentoft5
1Centre for Neuropsychiatric Schizophrenia Research (CNSR) and Centre for Clinical Intervention and Neuropsychiatric Schizophrenia Research (CINS), Mental Health Centre Glostrup, Copenhagen University Hospital, Glostrup, 2Registry Support Centre (East) – Epidemiology and Biostatistics, Research Centre for Prevention and Health, Capital Region of Denmark, Copenhagen, 3The Danish Clinical Registries, Registry Support Centre for Health Quality and Informatics (KCKS-West), Aarhus, 4Psychosis Ward, Section P, Aarhus University Hospital, Risskov, 5Mental Health Centre Copenhagen, Mental Health Services in the Capital Region of Denmark, University of Copenhagen, Copenhagen, Denmark
Aim of database: To systematically monitor and improve the quality of treatment and care of patients with schizophrenia in Denmark. In addition, the database is accessible as a resource for research.
Study population: Patients diagnosed with schizophrenia and receiving mental health care in psychiatric hospitals or outpatient clinics. During the first year after the diagnosis, patients are classified as incident patients, and after this period as prevalent patients.
Main variables: The registry currently contains 21 clinical quality measures in relation to the following domains: diagnostic evaluation, antipsychotic treatment including adverse reactions, cardiovascular risk factors including laboratory values, family intervention, psychoeducation, postdischarge mental health care, assessment of suicide risk in relation to discharge, and assessment of global functioning.
Descriptive data: The recorded data are available electronically for the reporting clinicians and responsible administrative personnel, and they are updated monthly. The registry publishes the national and regional results of all included quality measures in the annual audit reports. External researchers may obtain access to the data for use in specific research projects by applying to the steering committee.
Conclusion: The Danish Schizophrenia Registry represents a valuable source of informative data to monitor and improve the quality of care of patients with schizophrenia in Denmark. However, continuous resources and time devoted is necessary to maintain the integrity of the registry and the validity of the data.
Keywords: schizophrenia, national registry, quality of care, antipsychotic, adverse reactions, family intervention
Aim
To systematically monitor and annually audit the quality of the diagnostic evaluation, treatment, and care of patients with schizophrenia in Denmark. A further aim is to improve and facilitate progress and research in schizophrenia mental health care.
Study population
The Danish Schizophrenia Registry was founded in 2003. The registry comprises patients diagnosed with schizophrenia and receiving mental health care in psychiatric hospitals or outpatient clinics. All psychiatric treatment and care is public and financed by taxes. Data on both inpatient and outpatient care are collected and transferred from the National Patient Registry.1 In the year 2014, 14,324 patients were recorded in the Danish Schizophrenia Registry via the National Patient Registry. During the first year after the diagnosis, patients are classified as incident patients, and after this period reported as prevalent patients. General practitioners and private psychiatrists do not report to the registry due to national convention. If treated within these settings, the patients will, for the most part, present with only mild symptom severity or be in remission. Thus, patients with only mild symptom severity are not routinely recorded in the registry and thus are not available for quality monitoring or research.
Main clinical quality measures
Introduction
The registry currently contains 21 clinical quality measures in relation to the following domains: diagnostic evaluation, antipsychotic treatment including adverse reactions, cardiovascular risk factors including laboratory values, family intervention, psychoeducation, postdischarge mental health care, assessment of suicide risk in relation to discharge, and assessment of global functioning. The registry contains quality measures in relation to performance of a specific task or intervention (processes of care), as well as quality measures recorded and reported as numerical results (results of care). The core of the quality measures has been consistent since the registry was established in 2003, but new quality measures have been added by the steering committee of the registry. The quality measures have mainly been collected by manual registration into an electronic registry, but in recent years, several of the quality measures have been harvested from nationwide administrative registries to reduce the burden of registration. This includes information on antipsychotic treatment (from 2014), laboratory values (expected from 2015), and postdischarge psychiatric follow-up (from 2012). However, due to administrative difficulties, the process of linkage between the relevant registries has not proven as efficient as expected, and a delay has been introduced regarding the electronic harvesting of some of these data.
The collection of data into the registry has changed within recent years. Before 2012, data were collected using a registration form with detailed written instructions. After January 1, 2012, data have been recorded in parallel with the collection of administrative data in the large national health care registries, which has required another set of registration procedures to be implemented. The change in recording procedures was mainly driven by a wish to reduce the amount of double registration, but it has proven more difficult to implement than first expected and data quality dropped substantially with the change in registration. However, the registry is on its way to reestablish itself, reinforced by the updating of electronic medical records that will better support the recording of the defined quality measures. Overall, the experience from this registry shifting from manual to electronic data collection emphasizes the importance of user-friendly interfaces with an easily available patient overview to facilitate electronic collection and recording of data.
For each quality measure, a desired absolute level (a standard) has been decided upon by the steering committee to reflect what is considered necessary to provide high quality service during diagnostic evaluation, treatment, and care of patients with schizophrenia. The quality measures with respective standards are listed in Table 1. The standard regarding assessment of cognitive functioning does not reflect a consideration of the optimum level of quality of care. Instead, it reflects the role of the registry to support the development and improvement of schizophrenia treatment and care.
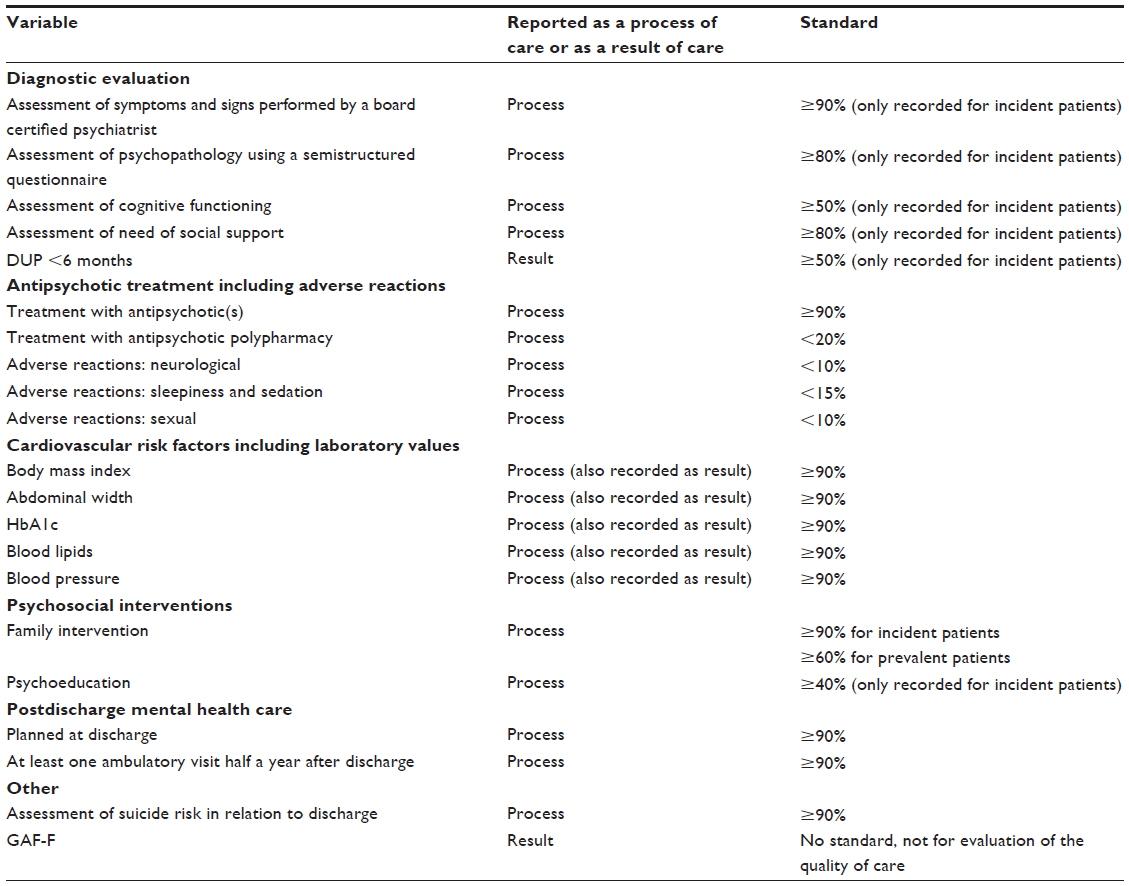 | Table 1 Summary of the variables (including standards to define high quality treatment and care) in the Danish Schizophrenia Registry |
The steering committee is comprised of representatives from different geographic regions and relevant professional societies. Across the years, it has been the responsibility of the steering committee to select which quality measures to include. From the beginning, it was decided to keep the number of quality measures at a minimum to limit the burden of registration and to increase data completeness.
Variables to assess the diagnostic evaluation
The quality measures related to the diagnostic evaluation comprise assessment of symptoms and signs performed by a board certified psychiatrist, assessment of psychopathology using a semistructured questionnaire (eg, the Present State Examination), assessment of cognitive functioning, assessment of need of social support, and duration of untreated psychosis (DUP). Except for DUP, these quality measures are recorded and reported as processes of care, that is, indicating the proportion of patients having received these examinations as part of the diagnostic evaluation. As regards DUP, this variable is recorded as a categorical variable (DUP <3 months, DUP 3–6 months, DUP >6 months) to facilitate recording since clinicians have reported to the steering committee that they find it difficult to give an exact estimation of the onset of psychosis. The standard of this quality measure is DUP <6 months, which was chosen pragmatically to indicate a DUP markedly below what is usually seen in clinical trials (eg, mean length of DUP is reported to be 61.3 weeks in a recent review2). DUP has been considered important to evaluate by the steering committee since long DUP is associated with a poor general symptomatic and global outcome.2 Consequently, proper first episode treatment services should be available to reduce, in general, DUP in the society.
Variables to assess the pharmacological treatment
The quality measures related to the pharmacological treatment comprise treatment with antipsychotics, number of different antipsychotics used, and antipsychotic adverse reactions. The latter includes neurological side effects, sleepiness and sedation, and sexual side effects.
Variables to assess cardiovascular risk factors
The quality measures related to cardiovascular risk factors include body mass index, abdominal width, glycosylated hemoglobin (HbA1c), blood lipids, and blood pressure. The cardiovascular risk factors are recorded both as processes of care, that is, the fraction of schizophrenia patients who have these measures recorded, and as results of care, that is, the mean value of HbA1c among recorded patients or the fraction of patients with increased levels. The evaluation of these quality measures as processes of care was driven by an aim to focus on the cardiovascular risk factors among patients with schizophrenia, because there is an urgent need to intervene against the excess cardiovascular mortality among patients with schizophrenia.3 With this focus, each recording inpatient or outpatient treatment unit can follow their own improvements in obtaining and recording these measures. The task of improving the absolute values of the cardiovascular risk measurements is a much more difficult one, which includes implementation of various interventions (eg, increased physical activity and pharmacological interventions) in a model of shared care with general practice. Evaluation of these indicators as results of care will follow after the recording of the data has been optimized. Thus, the current focus is mainly on increasing the proportion of patients for whom the cardiovascular risk factors are measured and recorded. When this is in place, the focus will shift to the absolute values of the cardiovascular risk factors and how these can be improved.
Other variables
The remainder of the quality measures encompasses family intervention, psychoeducation, postdischarge mental health care, assessment of suicide risk in relation to discharge, and assessment of global functioning using the Global Assessment of Functioning Scale (split GAF-F). The GAF-F is recorded as the numerical value, but it is not reported along with the other quality measures and there is no fixed standard. It is primarily collected as an indicator of illness severity for use in registry-derived analyses and research.
Validity
A study from 2012 investigated the validity of the quality of care data in the registry as compared with data extracted from the respective medical records.4 The results indicated substantial variability across the quality measures in the registry: sensitivity ranged from 11% to 96%, specificity ranged from 11% to 100%, and the ranges of the positive and negative predictive values were, respectively, 44%–100% and 5%–100%. The authors noted that the results were limited by incomplete documentation of care in a high proportion of the examined medical records, which were considered the gold standard of recording.
Follow-up
The recorded data is available electronically for the reporting clinicians and responsible administrative personnel, and it is updated monthly. The registry publishes the national and regional results of all included quality measures in the annual audit report. The steering committee meets once a year to audit the results of the preceding year and decides on the contents of the annual audit report with recommendations for future practice. The annual audit process is focused on evaluating whether the defined levels of high quality of care (the standards for each quality measure) are fulfilled, which is reported on a national level, on a regional level, on a hospital level, and on the level of individual departments of a certain size. At these meetings, it is decided whether any changes to the quality measures are warranted. Questions from clinicians or administrative staff in between the annual audits are discussed within a smaller group consisting of the national leadership and representatives from the Registry Support Centre of Clinical Quality and Health Informatics (West) and the Registry Support Centre of Epidemiology and Biostatistics (East).
Examples of research
Researchers may obtain access to the data in the registry for use in specific research projects by applying to the steering committee. Throughout the years, several studies have been published based on data from the Danish Schizophrenia Registry. It has been shown that the number of in-hospital processes of care received was associated with a lower risk of criminal behavior after discharge in patients with schizophrenia.5 Another study documented an increase in systematic suicide risk assessment in relation to discharge after initiation of the registry.6 The Danish Schizophrenia Registry is the only Danish nationwide registry that contains a measure of functional ability (GAF-F), which is not the case for other Danish registries because they are structured around collection of data with an administrative purpose. Among others, an intervention study to reduce the frequency of antipsychotic polypharmacy used GAF-F data from the registry to characterize the subjects in the intervention and control area regarding functional abilities.7 A recent study documented that quality of care improved with the implementation of the registry and the systematic monitoring program, but also that a high degree of variation between the hospitals remains.8
Administrative issues and funding
The registry is administered by the Danish Clinical Registries (RKKP), and the registry is managed by regional support centers specialized in epidemiology and biostatistics.
The registry is publicly funded by the RKKP for 3-year periods, which have been successively extended since the foundation of the registry in 2003.
Conclusion
The Danish Schizophrenia Registry represents an important source for improving psychiatric care for patients with schizophrenia. The value of the registry lies in the collection of clinical data that are not otherwise available. Furthermore, the registry provides an essential source of data for research purposes, in particular when linking with other central national registries. The collection of data regarding cardiovascular risk factors will eventually be a valuable source for further examinations of the link between metabolic side effects and the excess mortality among schizophrenia patients.
Acknowledgments
This paper was funded by the Program for Clinical Research Infrastructure (PROCRIN) established by the Lundbeck Foundation and the Novo Nordisk Foundation and administered by the Danish Regions.
Disclosure
The authors report no conflicts of interest in this work.
References
Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health. 2011;39(7 Suppl):30–33. | |
Penttilä M, Jääskeläinen E, Hirvonen N, Isohanni M, Miettunen J. Duration of untreated psychosis as predictor of long-term outcome in schizophrenia: systematic review and meta-analysis. Br J Psychiatry. 2014;205(2):88–94. | |
De HM, Correll CU, Bobes J, et al. Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry. 2011;10:52–77. | |
Pedersen CG, Gradus JL, Johnsen SP, Mainz J. Challenges in validating quality of care data in a schizophrenia registry: Experience from the Danish national Indicator Project. Clin Epidemiol. 2012;4(1):201–207. | |
Pedersen CG, Jensen SOW, Johnsen SP, Nordentoft M, Mainz J. Processes of in-hospital psychiatric care and subsequent criminal behaviour among patients with schizophrenia: A national population-based, follow-up study. Can J Psychiatry. 2013;58(9):515–521. | |
Pedersen CG, Jensen SOW, Gradus J, Johnsen SP, Mainz J. Systematic suicide risk assessment for patients with schizophrenia: A national population-based study. Psychiatr Serv. 2014;65(2):226–231. | |
Baandrup L, Allerup P, Lublin H, Nordentoft M, Peacock L, Glenthoj B. Evaluation of a multifaceted intervention to limit excessive antipsychotic co-prescribing in schizophrenia out-patients. Acta Psychiatr Scand. 2010;122(5):367–374. | |
Jørgensen M, Mainz J, Svendsen M, et al. Improving quality of care among patients hospitalized with schizophrenia: A nationwide initiative. BJPsych Open. 2015;1(1):48–53. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.