Back to Journals » Clinical Epidemiology » Volume 8
The Danish Nonmelanoma Skin Cancer Dermatology Database
Authors Lamberg AL, Sølvsten H, Lei U, Vinding GR, Stender IM, Jemec GB, Vestergaard T, Thormann H, Hædersdal M, Dam TN, Olesen AB
Received 17 November 2015
Accepted for publication 17 February 2016
Published 25 October 2016 Volume 2016:8 Pages 633—636
DOI https://doi.org/10.2147/CLEP.S99464
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor H Sorensen
Anna Lei Lamberg,1 Henrik Sølvsten,2 Ulrikke Lei,3 Gabrielle Randskov Vinding,3 Ida Marie Stender,4 Gregor Borut Ernst Jemec,5 Tine Vestergaard,6 Henrik Thormann,7 Merete Hædersdal,8 Tomas Norman Dam,9 Anne Braae Olesen10
1Dermatology Clinic, Grenaa, Central Denmark Region, 2Dermatology Clinic, Aalborg, North Denmark Region, 3Department of Dermato-Allergology, Gentofte Hospital, University of Copenhagen, Gentofte, 4Dermatology Clinic, Charlottenlund, Capital Region of Denmark, 5Department of Dermatology, Roskilde Hospital, Health Sciences Faculty, University of Copenhagen, Roskilde, Zealand Region, 6Department of Dermatology, Odense University Hospital, Odense, 7Dermatology Clinic, Vejle, Region of Southern Denmark, 8Department of Dermatology, Bispebjerg Hospital, University of Copenhagen, Copenhagen, Capital Region of Denmark, 9Dermatology Clinic, Nykøbing Falster, Zealand Region, 10Department of Dermatology, University Hospital of Aarhus, Aarhus, Central Denmark Region, Denmark
Aim of database: The Danish Nonmelanoma Skin Cancer Dermatology Database was established in 2008. The aim of this database was to collect data on nonmelanoma skin cancer (NMSC) treatment and improve its treatment in Denmark. NMSC is the most common malignancy in the western countries and represents a significant challenge in terms of public health management and health care costs. However, high-quality epidemiological and treatment data on NMSC are sparse.
Study population: The NMSC database includes patients with the following skin tumors: basal cell carcinoma (BCC), squamous cell carcinoma, Bowen's disease, and keratoacanthoma diagnosed by the participating office-based dermatologists in Denmark.
Main variables: Clinical and histological diagnoses, BCC subtype, localization, size, skin cancer history, skin phototype, and evidence of metastases and treatment modality are the main variables in the NMSC database. Information on recurrence, cosmetic results, and complications are registered at two follow-up visits at 3 months (between 0 and 6 months) and 12 months (between 6 and 15 months) after treatment.
Descriptive data: In 2014, 11,522 patients with 17,575 tumors were registered in the database. Of tumors with a histological diagnosis, 13,571 were BCCs, 840 squamous cell carcinomas, 504 Bowen's disease, and 173 keratoakanthomas.
Conclusion: The NMSC database encompasses detailed information on the type of tumor, a variety of prognostic factors, treatment modalities, and outcomes after treatment. The database has revealed that overall, the quality of care of NMSC in Danish dermatological clinics is high, and the database provides the necessary data for continuous quality assurance.
Keywords: nonmelanoma skin cancer, basal cell carcinoma, squamous cell carcinoma, epidemiology, treatment
Aim of database
The Danish Nonmelanoma Skin Cancer Dermatology Database is a publicly funded national clinical database. It was established in 2008 to monitor the quality of treatment for nonmelanoma skin cancer (NMSC) by dermatologists in office-based settings and provide the necessary data for quality assurance and improvement.
The concept of NMSC primarily refers to basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). These tumors are the most common malignancies in Denmark as well as in other Western countries.1,2 In spite of its low mortality, the high prevalence of NMSC makes it a significant challenge in terms of health management and health care costs.3 Care for NMSC is complex, with treatments provided in both hospitals and office-based settings. Several medical specialties may be involved in the treatment of NMSC, but the primary care providers are dermatologists, often within an office-based setting.3,4
A wide range of different treatments are used in the management of NMSC, eg, Mohs micrographic surgery, excision, cryotherapy, curettage, curettage combined with cautery, cryotherapy or laser, photodynamic therapy, radiotherapy, and imiquimod. Guidelines have been published by several organizations.5–8
The cost of treatment depends on treatment modality and setting (hospital or office based).3 However, little is known about the effectiveness of the most commonly used treatment modalities for SCC and BCC.7–10 The current knowledge comes predominantly from selected patient groups in studies often performed in single hospital centers.7–10 The management of NMSC differs between countries, and compared to other countries, curettage is used more frequently in Denmark10 and Mohs micrographic surgery is less often performed.
Detailed data on NMSC and its treatment in routine clinical practice are important for surveillance, assessment of prognosis, quality assurance, and improvements.2,11,12 Such data can only be obtained from clinical databases, which are an attractive resource for epidemiological research.11,12
The NMSC database contains detailed data on NMSC diagnosed by the participating dermatologists, providing the necessary data for quality assurance and improvement. The aim of the NMSC database is to collect data on NMSC treatment and improve the treatment of NMSC in Denmark.
Study population
The NMSC database includes patients with the skin tumors BCC, SCC, Bowen’s disease, and keratoacanthoma diagnosed by the participating office-based dermatologists in Denmark.
Between January 2008 and January 2011, the NMSC database was a regional database, incorporating data on NMSC patients diagnosed and treated at dermatology clinics in the Central and North Denmark Regions, which have a combined population of 1.8 million people that accounts for ~30% of the Danish population. After approval by the Danish National Board of Health, the database started operating at a national (5.6 million people) level since February 2011.
Collecting prospective data highly increases the workload of the registering clinics. In 2014, 11,522 patients with 17,575 tumors were registered in the database, and >72,000 tumors are now registered in the database.
Completeness can be difficult to estimate precisely, because not all cases are sent for histopathology or registered in other registries. However, using the Danish Pathology Registry as a gold standard, the overall data completeness is 62%. Some clinics do not register. The completeness of the clinics registering in the database is 75%. The completeness of the individual variables is high, with only a few (median 2%) missing data (Table 1).
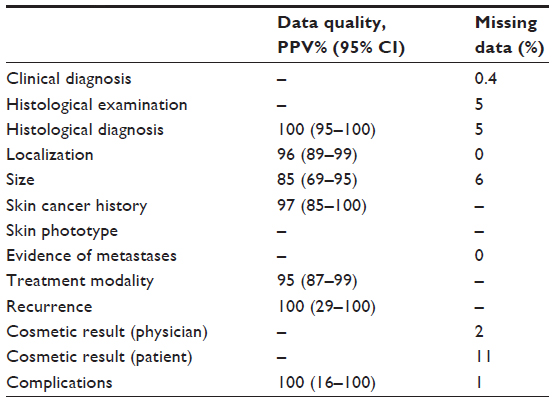 | Table 1 Main variables in the Danish Nonmelanoma Skin Cancer Dermatology Database |
A new online registration system is under construction. This system will have a special data capture technique, enabling an NMSC database reminder when an NMSC patient is in the clinic. Higher completeness will make the database a strong research tool. Extra efforts will be taken to enroll the clinics not registering in the database.
Main variables
Content of the NMSC database
The NMSC database operates via an Internet-based online registration system. A common interface form ensures standardized data collection. Data are entered into a computer-based data management system using the civil personal registry number (a unique ten-digit number assigned to each Danish citizen at birth or immigration).
For each patient, the treating dermatologist enters detailed information on tumor, treatment, and evaluation after treatment. The exact localization of the tumor is marked on an anatomical position sketch.
On the day of treatment, the treating dermatologist completes a questionnaire with detailed information on prognostic and treatment-related variables: clinical and histological diagnoses, clinical BCC subtype, localization, size, skin cancer history, skin phototype, evidence of metastases, and treatment modality. The histology report is added when it is received. If the patients have new tumors or recurrences later in life, these are added to the anatomical position sketch.
Data quality
We have previously examined the accuracy of the registrations in the NMSC database using medical record review as a gold standard. However, for the variable “histological diagnosis,” the Danish Pathology Registry was used as a gold standard.13
Overall, the accuracy of variables registered in the NMSC database was high.13 Positive predictive value (PPV) of histologically verified diagnoses was 100% using the Danish Pathology Registry as a gold standard. The PPV was 96% for localization, 85% for size, and 91% for the date of treatment. The PPV of treatment modality registered was 95%13 (Table 1).
Treatment quality
In order to monitor and facilitate improvement of treatment, six quality indicators have been chosen related to diagnosis, surveillance, and outcome of the treatment of NMSC, Bowen’s disease, and keratoacanthoma (Table 2).
 | Table 2 Quality indicators in the Danish Nonmelanoma Skin Cancer Dermatology Database |
A report is published annually with data from the database showing data on all six quality indicators, with comments from both an epidemiologist and the steering committee of the NMSC database.
Follow-up
NMSC patients are scheduled for two follow-up visits, one at ~3 months (between 0 and 6 months) and one at ~12 months (between 6 and 15 months) after treatment. At these visits, information on recurrence, cosmetic result, and complications are entered in the database.
In 2014, 54% of the patients were registered in the database at the first follow-up visit and 38% at the second follow-up visit.
Examples of research
The database was developed as a part of a PhD study.14 A validation study was conducted as a part of the PhD study.13
Data in the NMSC database are available for clinical research. It is possible to apply for data at the Danish Clinical Registries. The dermatologists registering in the database also have to apply for data for clinical research.
Using the civil personal registry number, data on patients can be linked to other Danish medical and population-based databases. The Civil Registration System stores information from 1968 to present, including date of birth, change of address, date of emigration, and exact date of death.15
Currently, three studies are in process:
- regional variations in the treatment of NMSC;
- recurrence rate after treatment of NMSC in Denmark; and
- characteristics and treatments of keratoacanthoma.
The management of NMSC differs not only between countries but also nationally. Study 1 describes the regional differences in the management of treatment. A wide range of treatments can be used in the treatment of a low-risk tumor according to national and international guidelines.5–8 Study 2 investigates the recurrence rates, providing real-world data to the understanding of recurrence risk associated with the available different treatment modalities adjusted for clinical characteristics of the tumors. Study 3 provides epidemiological data on keratoacanthomas, increasing our understanding of these tumors that resemble SCCs clinically and histologically but are self-limiting and benign.
Administrative issues and funding
Organization
The NMSC database was initiated in cooperation with the Danish Dermatological Society and the Danish Dermatologists’ Organization in 2007. The organization of the NMSC database consists of a steering committee of dermatologists from both hospitals and office-based clinics, as well as representatives from the Central Denmark Region administration. Currently, the steering committee of NMSC database has 12 members who administer the database.
The development of the database was funded by the Danish Regional Collaboration of Specialists “Fonden for Faglig Udvikling af Speciallægepraksis” and “Aage Bangs Foundation.”
The NMSC database is approved as a national clinical quality database. Patient privacy is ensured by encryption and password protection. The dermatologists only have access to their own data.
The Danish Regional Funding for Clinical Databases funds the daily operation of the NMSC database. The database is operated by DAK-E (Danish Quality Unit of General Practice), and in future, DAK-E will fund the daily operation.
Conclusion
The NMSC database encompasses detailed information on the type of tumor, a variety of prognostic factors, treatment modality, and outcomes after treatment. The main strength of the NMSC database is the very detailed registration and the high accuracy of the registrations.13 To the best of our knowledge, comparable NMSC data have previously been registered only in smaller cohorts of patients for limited time periods. The value of the Danish NMSC database may prove to be even greater than NMSC databases of other countries because of the unique opportunity to link it with other Danish population-based and medical data sources.
The care of NMSC is multidisciplinary, and a limitation of the database is that only dermatology clinics currently register in the database. A future goal is to cooperate with hospital departments in dermatology, plastic surgery, and oncology.
So far the database has revealed that the overall quality of care of NMSC in Danish dermatological clinics is high, and the database will provide the necessary data for continuous quality assurance and improvement.
Acknowledgments
The steering committee of NMSC database acknowledges the important effort of dermatologists registering data in the NMSC database, despite their high workload and the time-consuming registration procedure. This article was funded by the Program for Clinical Research Infrastructure established by the Lundbeck Foundation and the Novo Nordisk Foundation, and administered by the Danish Regions.
Disclosure
The authors report no conflicts of interest in this work.
References
Diepgen TL, Mahler V. The epidemiology of skin cancer. Br J Dermatol. 2002;146(suppl 61):1–6. | |
Trakatelli M, Ulrich C, del MV, Euvard S, Stockfleth E, Abeni D. Epidemiology of nonmelanoma skin cancer (NMSC) in Europe: accurate and comparable data are needed for effective public health monitoring and interventions. Br J Dermatol. 2007;156(suppl 3):1–7. | |
Chen JG, Fleischer AB Jr, Smith ED, et al. Cost of nonmelanoma skin cancer treatment in the United States. Dermatol Surg. 2001; 27(12):1035–1038. | |
Smith ES, Feldman SR, Fleischer AB Jr, Leshin B, McMichael A. Characteristics of office-based visits for skin cancer. Dermatologists have more experience than other physicians in managing malignant and premalignant skin conditions. Dermatol Surg. 1998;24(9):981–985. | |
Danish Dermatological S. Guidelines for Treatment of Basal Cell Carcinoma. 2009. Available from: www.dds.nu/wp-content/uploads/2012/08/Basocellulært-carcinom.pdf. Accessed April 2, 2016. | |
Danish Dermatological S. Guidelines for Treatment of Sqaumous Cell Carcinoma. 2009. Available from: www.dds.nu/wp-content/uploads/2012/08/Spinocellulær-hudcancer-SCC.pdf. Accessed April 2, 2016. | |
Motley R, Kersey P, Lawrence C; British Association of Dermatologists; British Association of Plastic Surgeons; Royal College of Radiologists, Faculty of Clinical Oncology. Multiprofessional guidelines for the management of the patient with primary cutaneous squamous cell carcinoma. Br J Dermatol. 2002;146(1):18–25. | |
Telfer NR, Colver GB, Morton CA; British Association of Dermatologists. Guidelines for the management of basal cell carcinoma. Br J Dermatol. 2008;159(1):35–48. | |
Bath-Hextall F, Perkins W, Bong J, Williams H. Interventions for basal cell carcinoma of the skin. Cochrane Database Syst Rev. 2007;(1):CD003412. | |
Veien K, Veien NK, Hattel T, Laurberg G. Non-melanom hudkræft behandlet i en dermatologisk speciallægepraksis: en kvalitetskontrolundersøgelse [Non-melanoma skin cancer treated in a dermatologic practice. A quality control study]. Ugeskr Laeger. 2002;164(37):4293–4295. Danish. | |
Mainz J. Defining and classifying clinical indicators for quality improvement. Int J Qual Health Care. 2003;15(6):523–530. | |
Sõrensen HT. Regional administrative health registries as a resource in clinical epidemiology. Int J Risk Saf Med. 1997;10(1):1–22. | |
Lamberg AL, Cronin-Fenton D, Olesen AB. Registration in the Danish Regional Nonmelanoma Skin Cancer Dermatology Database: completeness of registration and accuracy of key variables. Clin Epidemiol. 2010;2:123–136. | |
Lamberg AL. The Use of New and Existing Data Sources in Non-Melanoma Skin Cancer Research [PhD dissertation]. Aarhus: Faculty of Health Sciences, Aarhus University; 2011. | |
Schmidt M, Pedersen L, Sorensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.