Back to Journals » Clinical Epidemiology » Volume 8
The Danish National Penile Cancer Quality database
Authors Jakobsen JK, Öztürk B ![]() , Søgaard M
, Søgaard M
Received 26 November 2015
Accepted for publication 13 February 2016
Published 25 October 2016 Volume 2016:8 Pages 589—594
DOI https://doi.org/10.2147/CLEP.S99513
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor H Sorensen
Jakob Kristian Jakobsen,1 Buket Öztürk,2 Mette Søgaard2
1Department of Urology, 2Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus Nord, Denmark
Aim of database: The Danish National Penile Cancer Quality database (DaPeCa-data) aims to improve the quality of cancer care and monitor the diagnosis, staging, and treatment of all incident penile cancer cases in Denmark. The aim is to assure referral practice, guideline adherence, and treatment and development of the database in order to enhance research opportunities and increase knowledge and survival outcomes of penile cancer.
Study population: The DaPeCa-data registers all patients with newly diagnosed invasive squamous cell carcinoma of the penis in Denmark since June 2011.
Main variables: Data are systematically registered at the time of diagnosis by a combination of automated data-linkage to the central registries as well as online registration by treating clinicians. The main variables registered relate to disease prognosis and treatment morbidity and include the presence of risk factors (phimosis, lichen sclerosus, and human papillomavirus), date of diagnosis, date of treatment decision, date of beginning of treatment, type of treatment, treating hospital, type and time of complications, date of recurrence, date of death, and cause of death.
Descriptive data: Registration of these variables correlated to the unique Danish ten-digit civil registration number enables characterization of the cohort, individual patients, and patient groups with respect to age; 1-, 3-, and 5-year disease-specific and overall survival; recurrence patterns; and morbidity profile related to treatment modality. As of August 2015, more than 200 patients are registered with ~65 new entries per year.
Conclusion: The DaPeCa-data has potential to provide meaningful, timely, and clinically relevant quality data for quality maintenance, development, and research purposes.
Keywords: penile cancer, squamous cell carcinoma of the penis, clinical quality, national database, epidemiology, treatment
Introduction
Penile cancer is rare, and in Denmark, it has traditionally been diversely managed in dermatology, surgery, urology, and oncology without management guidelines and systematic quality monitoring. In 2009, a centralization of service to two university hospitals and two specialties, urology and oncology, favored continuous prospective data collection and initiated several quality improvements. The purpose of this study is to describe the Danish National Penile Cancer Quality database (DaPeCa-data).
Aim of database
The DaPeCa-data is a nationwide clinical cancer database with prospective data collection since June 2011 (Table 1). By the means of the Danish Civil Registration System, the database enables individual data collection and holds potential for a large number of data-linkage opportunities to existing and longstanding national registries on, for example, socioeconomic and pharmacological parameters. To our knowledge, within penile cancer registries, this possibility is only matched by the Swedish penile cancer registry enabling DaPeCa-data to supply important population-based data on this rare entity. DaPeCa-data is affiliated with the Danish National Penile Cancer Quality group (DaPeCa-group), which consists of clinical and paraclinical experts from the specialties oncology, pathology, and urology. The group is responsible for developing national clinical guidelines for the staging, treatment, and follow-up of penile cancer in Denmark and decides on quality indicators and indicator standards based on experience and available literature.1
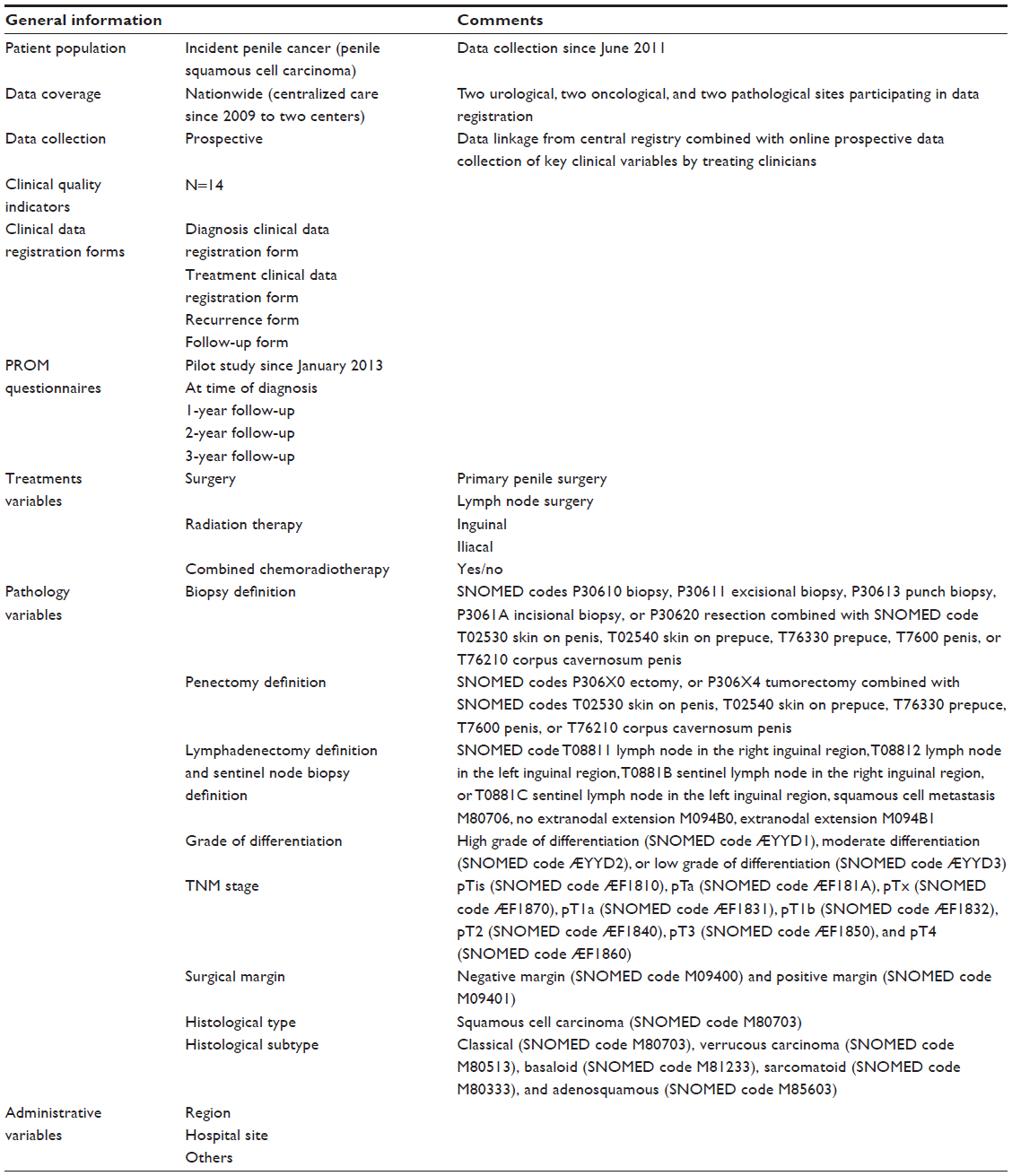 | Table 1 Overview of DaPeCa-data |
The overall aim of DaPeCa database and DaPeCa-group is to improve the quality of cancer care for penile cancer patients in Denmark. More specifically, the purpose of DaPeCa-data is to systematically collect key clinical variables on all incident penile cancer patients in Denmark for quality improvement and research.
The DaPeCa-data monitors clinical management of penile cancer. Penile cancer care in Denmark is centralized to two university centers.2 The DaPeCa-data monitors referral practice from regional hospitals and private practices within surgery/urology, dermatology, and general practice and monitors guideline adherence at the treating centers. The DaPeCa-data aims to assure modern staging and treatment of patients with penile cancer and to provide data for development of the research field.
Study population
Penile cancer is a rare disease with an incidence in developed countries in the range of 0.5–2.5/100,000 population/year.3 The incidence in Denmark is estimated to be 0.8/100,000 population/year, and the mean age at diagnosis is 65 years.4 Data on ~65 patients are entered into the database each year, which has currently accumulated to more than 200 entries. Due to the rarity of the disease, it is a high priority of the DaPeCa-group and DaPeCa-data to collaborate with other databases in Scandinavia and in other Northern European countries with comparable populations. Currently, an application for a common Scandinavian database is under preparation with the success of the common Scandinavian childhood cancer databases as a model.5
Inclusion criteria and exclusion criteria
The DaPeCa-data registers all patients with newly diagnosed invasive squamous cell carcinoma of the penis in Denmark.
Patients with penile tumors with nonsquamous cell carcinoma histopathological features, such as sarcoma, melanoma, lymphoma, and metastases, from other cancers are not registered in the DaPeCa-data since each of these entities are covered by other national databases. Tumors of the distal urethra (navicular fossa) are registered if they involve external aspects of penile anatomy. Other primary urethral tumors are not registered.
Inclusion in the database is based on registration of a patient in the Danish Pathology Registry6 with relevant Systematized Nomenclature of Human Medicine (SNOMED) codes or registration in the Danish National Patient Registry and the Danish Cancer Registry with relevant ICD codes (DC609, DC609J, DC609K, DC609L, DC609M, DC609N, DC609P, DC609Q, DC609R, DC609S, DC609T, DC609U, and DC609Z).7
Main variables and data quality
The variables currently collected via the online registration interface are listed in Table 2. Online registration by the urologist responsible for treatment has the advantage of a high level of data quality and variable validity. On the other hand, the registration interface is extensive and difficult to handle in daily practice. Ongoing validation projects of data accumulating via the Danish pathology and Danish patient registries aim to move a considerable part of the data registration toward automated data extraction and validation from these registries by treating clinicians via patient interview and examination or medical record verification. The annual reports published so far have been based mainly on this type of data, and it has turned out that continuous validation and interaction between clinicians and statisticians are of great importance in order to produce a valid and meaningful report. A solid framework for continuous validation algorithms and iterative data checking has to be designed and validated to speed this process up in order to meet the demand of the political visions of close-to real-time quality data production. This process is currently in an early phase, and limited resources are a main challenge.
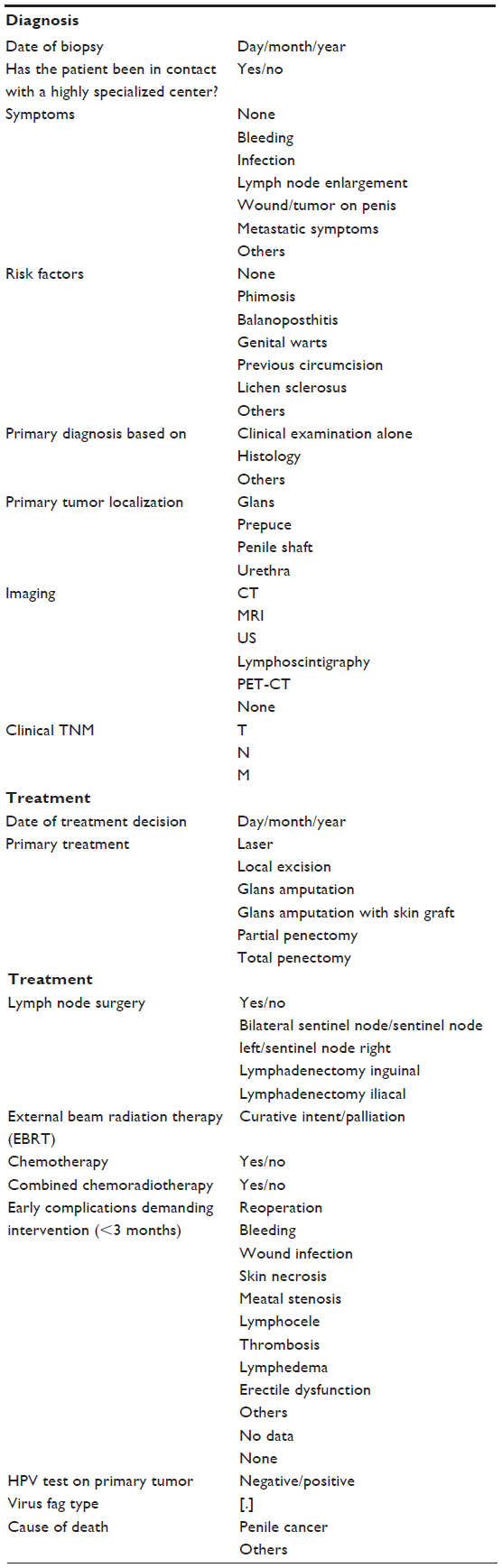 | Table 2 Overview of DaPeCa-data variables |
Follow-up
DaPeCa-data has promising potential to virtually complete the follow-up of its patient population. All penile cancer patients included in DaPeCa-data can be followed until death or emigration by means of data linkage to the Danish Civil Registration System.
An ongoing effort aims to facilitate automated follow-up prompts to appear at the relevant administrator in order to enter the follow-up data continuously. If this system fails to be implemented, the database will be updated in relation to specific studies with retrieval and addition of relevant data from records and registers via Danish Civil Registration System.
Examples of research
The group behind the DaPeCa-data is active within the research field and publishes regularly on the topic;2,8–12 however, no research paper as of yet has used data registered in the DaPeCa-data due to the rarity of the disease and the fact that the database was only established in June 2011. The first validation study is under preparation. Since its inception in 2011, DaPeCa-data has annually released a report with analyses of the clinical quality indicators (Table 3). However, results and data presented in the annual reports from the initial development years should be interpreted with reservation and caution. As reflected by the most recent annual reports, data validity and completeness has been improving over time, but validation and algorithm optimization is only progressing slowly at the current level of support and funding.
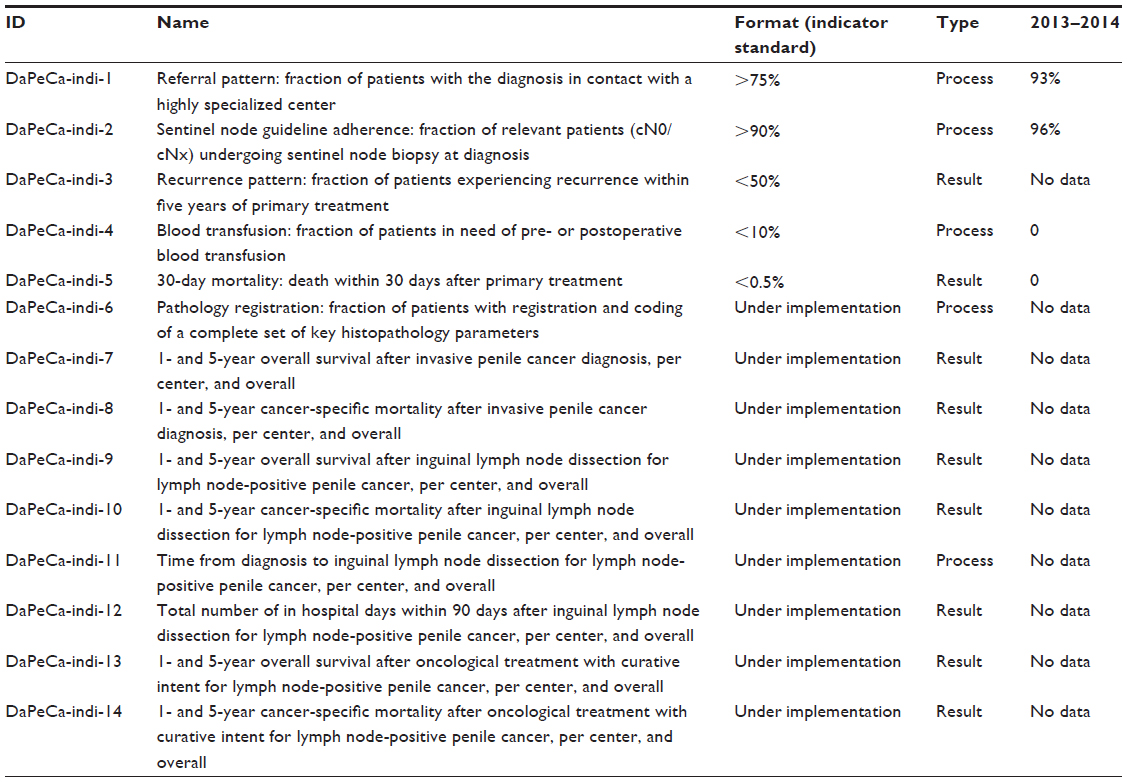 | Table 3 Overview of DaPeCa-data quality indicators |
Administrative issues and funding
The DaPeCa-data is administered in the two centers, such as Copenhagen University Hospital and Aarhus University Hospital, responsible for staging and treatment of the patients. Validation lists of all patients with the diagnosis within the uptake area of the specific center are presented to the database administrators every 3 months. Data are entered into an Internet-based online user interface with integrated range validation by treating clinicians. The completeness of registration is high, in some years approaching 100%. Data are linked to each patient’s unique ten-digit civil personal registration number. The database steering committee consists of clinicians and academic experts representing urology, oncology, and pathology and continuously updates and specifies the quality indicators and the contents of the data profile ensuring a clinically meaningful and realistic dataset. The database receives a limited amount of funding from public sources via the Danish Regions and is independent from private funding. DaPeCa-data is under the auspices of the Danish Multidisciplinary Cancer Groups (DMCG.dk), which is an umbrella organization comprising 24 national cancer groups and clinical databases in Denmark. The urological cancer groups and databases are further organized under the subgroup for Danish Urological Cancer Groups. The DaPeCa-data receives a limited administrative support from the Danish Clinical Quality Improvement Program (RKKP).13 Technical support and data management service are provided by the Competence Centre for Health Quality and Informatics (KCKS-Vest),14 and epidemiological and statistical support to the annual reports is provided by the Competence Centre for Clinical Epidemiology and Biostatistics, North (KCEB-Nord).15 Patient-reported outcome measure data are collected nationwide at both urological treatment centers as a part of an ongoing quality of life and sexuality study. On the basis of this pilot project, which is based on an adapted and validated version of the Scandinavian Prostate Cancer Group 4 items, a patient-reported outcome measure data collection is planned to commence with a validated set of sexuality and quality of life questionnaire items.
DaPeCa-data collects nationwide health care data in accordance with Danish data protection laws. Laws and procedures for data access to DaPeCa-data are governed by the Data Protection Agency (Datatilsynet) and the Danish Ministry of Health (Sundhedstyrelsen). Applications for data access to DaPeCa-data are reviewed by the Chair and Steering Committee upon application to RKKP.13
Conclusion
DaPeCa-data has been in existence since 2011. More than 200 patients are registered. Validation of the register data sources is ongoing, and the first validation study based on data from the DaPeCa-data is under preparation. With an increased level of support and funding, the important validation iterations could be optimized faster. The DaPeCa-group has already published studies based on medical records. Updated information on DaPeCa-data is available at the DaPeCa-group Internet homepage: http://ducg.dk/dapeca-peniscancer/.
Acknowledgments
Mary Nguyen Nielsen, MD, PhD student, generously provided the textual framework. This article was funded by the Program for Clinical Research Infrastructure established by the Lundbeck Foundation and the Novo Nordisk Foundation and administered by the Danish Regions. This study was conducted on behalf of the DaPeCa group.
Disclosure
The authors report no conflicts of interest in this work.
References
DUCG [webpage on the Internet]. DaPeCa Clinical Guidelines (in Danish); 2013. Available from: http://ducg.dk/dapeca-peniscancer/kliniske-retningslinjer/. Accessed August 25, 2015. | |
Jakobsen JK, Krarup KP, Kirrander P, et al; Scandinavian Penile Cancer Group (SCAPECA). Penile cancer in Scandinavia: current practice and future perspectives. Scand J Urol. 2014;2:1–3. | |
Hakenberg OW, Comperat E, Minhas S, Necchi A, Protzel C, Watkin N [webpage on the Internet]. EAU Guidelines on Penile Cancer; 2014. Available from: uroweb.org/guideline/penile-cancer/. Accessed September 09, 2014. | |
Ulff-Moller CJ, Simonsen J, Frisch M. Marriage, cohabitation and incidence trends of invasive penile squamous cell carcinoma in Denmark 1978–2010. Int J Cancer. 2013;133(5):1173–1179. | |
NOPHO [webpage on the Internet]. SIOP Europe, the European Society for Paediatric Onclogy. Available from: http://www.nopho.org/organization/history/NOPHO%20history%20SIOPE%20news%202014-02.pdf. Accessed February 19, 2016. | |
Patobank [homepage on the Internet]. The Danish Pathology Registry. Available from: http://www.patobank.dk/. Accessed 25 August, 2015. | |
Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health. 2011;39(7 suppl):30–33. | |
Jakobsen JK. A urologist’s contemporary guide to penile cancer. Scand J Urol. Epub 2015 Aug 14. | |
Jakobsen JK, Alslev L, Ipsen P, et al. DaPeCa-3: promising results of sentinel node biopsy combined with F-fluorodeoxyglucose positron emission tomography/computed tomography in clinically lymph node-negative patients with penile cancer – a national study from Denmark. BJU Int. Epub 2015 Jul 28. | |
Jakobsen JK, Jensen JB. DaPeCa-2: Implementation of fast-track clinical pathways for penile cancer shortens waiting time and accelerates the diagnostic process – a comparative before-and-after study in a tertiary referral centre in Denmark. Scand J Urol. 2016;50(1):80–87. | |
Jakobsen JK, Krarup KP, Sommer P, et al. DaPeCa-1: diagnostic accuracy of sentinel lymph node biopsy in 222 patients with penile cancer at four tertiary referral centres – a national study from Denmark. BJU Int. 2016;117(2):235–243. | |
Mortensen GL, Jakobsen JK. Patient perspectives on quality of life after penile cancer. Dan Med J. 2013;60(7):A4655. | |
Danish Quality Improvement Program (RKKP) [homepage on the Internet]. Internet Homepage. Available from: http://rkkp.dk/. Accessed 27 August, 2015. | |
KCKS [webpage on the Internet]. Competence Centre for Health Quality and Informatics (KCKS-Vest). Available from: http://www.kcks-vest.dk/kliniske-kvalitetsdatabaser. Accessed 27 August, 2015. | |
KEA [webpage on the Internet]. Competence Centre for Clinical Epidemiology and Biostatistics, North (KCEB-Nord). Available from: http://www.kea.au.dk/en/ClinicalQuality/CentreClinEpiBiostatNorth.html. Accessed 27 August, 2015. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.