Back to Journals » Clinical Epidemiology » Volume 8
The Danish Anaesthesia Database
Authors Antonsen K, Rosenstock CV, Lundstrøm LH
Received 16 January 2016
Accepted for publication 7 March 2016
Published 25 October 2016 Volume 2016:8 Pages 435—438
DOI https://doi.org/10.2147/CLEP.S99517
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Henrik Toft Sørensen
Kristian Antonsen,1 Charlotte Vallentin Rosenstock,2 Lars Hyldborg Lundstrøm2
1Board of Directors, Copenhagen University Hospital, Bispebjerg and Frederiksberg Hospital, Capital Region of Denmark, Denmark; 2Department of Anesthesiology, Copenhagen University Hospital, Nordsjællands Hospital-Hillerød, Capital Region of Denmark, Denmark
Aim of database: The aim of the Danish Anaesthesia Database (DAD) is the nationwide collection of data on all patients undergoing anesthesia. Collected data are used for quality assurance, quality development, and serve as a basis for research projects.
Study population: The DAD was founded in 2004 as a part of Danish Clinical Registries (Regionernes Kliniske Kvalitetsudviklings Program [RKKP]). Patients undergoing general anesthesia, regional anesthesia with or without combined general anesthesia as well as patients under sedation are registered. Data are retrieved from public and private anesthesia clinics, single-centers as well as multihospital corporations across Denmark. In 2014 a total of 278,679 unique entries representing a national coverage of ~70% were recorded, data completeness is steadily increasing.
Main variable: Records are aggregated for determining 13 defined quality indicators and eleven defined complications all covering the anesthetic process from the preoperative assessment through anesthesia and surgery until the end of the postoperative recovery period.
Descriptive data: Registered variables include patients' individual social security number (assigned to all Danes) and both direct patient-related lifestyle factors enabling a quantification of patients' comorbidity as well as variables that are strictly related to the type, duration, and safety of the anesthesia. Data and specific data combinations can be extracted within each department in order to monitor patient treatment. In addition, an annual DAD report is a benchmark for departments nationwide.
Conclusion: The DAD is covering the anesthetic process for the majority of patients undergoing anesthesia in Denmark. Data in the DAD are increasingly used for both quality and research projects.
Keywords: anesthesia, quality indicators, complication, registries, epidemiology, registry-based research
Aim of database
The principal aim of the Danish Anaesthesia Database (DAD) is the nationwide collection of data on all Danish patients undergoing anesthesia. Collected data are used for quality assurance, quality development, and serve as a basis for research projects.
Study population
The database was founded in 2004 and during the last decade the national coverage has been stable around 60%–70%. In this context anesthesia is defined as any anesthesia or sedation, general, local or combined provided by a specialist in anesthesiology (medical doctor [MD]), either directly or during direct supervision (ie, nurse anesthetist or MD during specialist training). Thus, in principle, the study population is the entire Danish population undergoing anesthesia annually, and the database can comprise up to an estimated total of 400,000 unique cases per year. Data are retrieved from both public and private anesthesia clinics, large and small practices, and both single-center and multihospital corporations across Denmark. The Danish health care system is however mostly publicly funded with tax-financed universal access. In 2014, a total of 278,679 unique entries were recorded in the DAD. As a part of the Danish Clinical Registries (Regionernes Kliniske Kvalitetsudviklings Program [RKKP]), reporting of data to the DAD is in principle mandatory. In reality however, it has not yet been possible to ensure complete data coverage, but data completeness is steadily increasing.
Main variables
The DAD is a national, clinical quality assurance database containing selected quantifiable indicators, covering the full anesthetic process (from preoperative assessment through anesthesia/surgery to the postoperative recovery period). Data are gathered online by clinical personnel in the individual departments and reported through data-collection systems either directly to Tieto Klinisk Måle System or by web-based solution (SAS, web services). In 2014, 36 out of a total of 44 public hospitals reported 269,967 anesthetic cases and nine out of 19 registered private clinics reported 8,712 cases. Variables registered in the DAD include patients’ individual social security number (assigned to all Danes) and both direct patient related-lifestyle factors enabling a quantification of patients’ comorbidity as well as variables that are strictly related to the type, duration, and safety of anesthesia. Data covering patients’ own experiences of quality are not collected. In 2014, the DAD underwent a major revision during which the scientific evidence behind previous quality indicators was scrutinized and newly defined. Recorded information is now aggregated for determining 13 defined quality indicators thereby providing a benchmark for clinical outcome. Quality fulfillments are compared with evidence-based predefined standards (see Table 1). Variables reflecting patient comorbidity include age, American Society of Anesthesiologists physical classification system I–V, sex, height, weight, smoking and drinking status. Table 2 shows registered complications in the DAD. Data and specific data combinations can be extracted within each department in order to monitor patient treatment. In addition, an annual DAD report is a benchmark for departments nationwide.
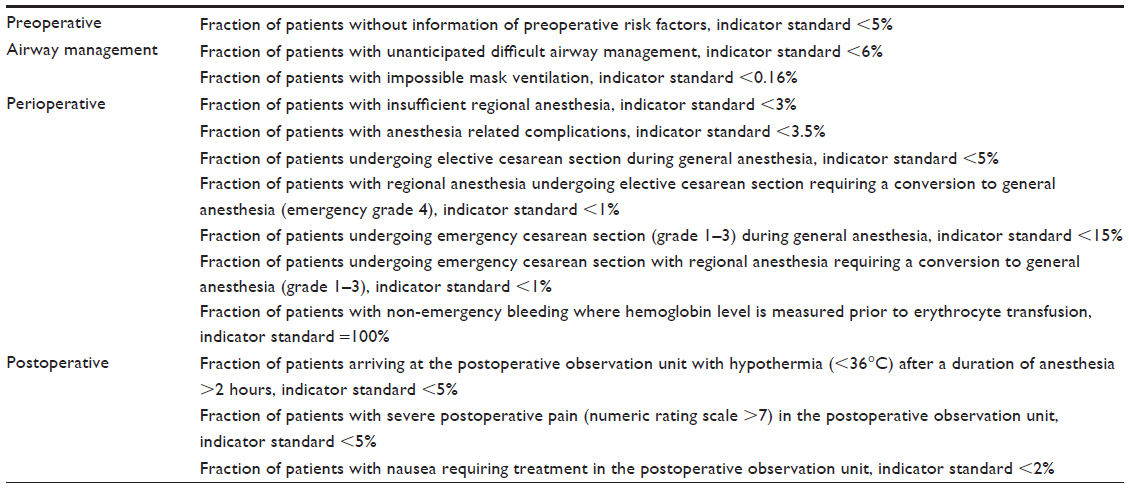 | Table 1 Danish Anaesthesia Database quality indicators |
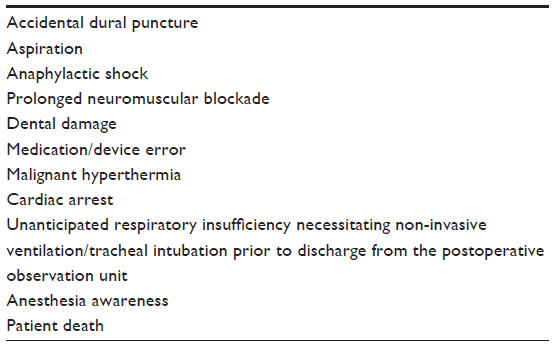 | Table 2 Danish Anaesthesia Database registered complications |
Data validity
Historically, a principal explanation for a relatively low degree of coverage has been data transfer challenges from local databases via a web interface to the DAD, often rendering it difficult to enforce the concept of mandatory registration, especially at the individual hospital/clinic level. Thus, the main reason for the low degree of national coverage may be explained by specific hospitals/clinics not reporting data at all. It is estimated that public hospitals not reporting at present comprise an estimated 70,000 cases per year. Unreported cases from private clinics are estimated to be ~50,000 to 60,000 cases per year, the majority being short duration cases involving patients undergoing ear, nose, and throat surgery. Thus, the total number of private clinics providing anesthetic services is presently unknown. The information technology infrastructure of the database is presently under reconstruction. When completed, it will finally allow data transfer at all levels, thus anticipating coverage above 90% and perhaps even approaching 100% from all public hospitals by 2017.
Despite a low degree of national coverage, several surveys have demonstrated that the patients who are registered in the DAD are most likely also registered in the Danish National Health Register. In general, the DAD data coverage concerning public hospitals is considered high because entered data in addition to measuring quality is used for productivity measurement, thereby reinforcing follow-up registrations on missing patients. Thus, for specific surgical or anesthetic procedures registered in the DAD, there is a 98% to 99% correspondence to records also found in the Danish National Health Register.1–3 Quality of data entry is controlled during the process of registration in the DAD, as most variables are predefined, mandatory for registration and are linked to user manuals that are an integrated part of the DAD interface for each variable. Further, the designs of the categories of the registered parameters in the DAD are mostly exclusive and exhaustive. However, in previous versions of the database the ability to register complications was not intuitively easy, in addition to some systems having “no complications” as a default answer. Both issues have been altered in the present version of the database in order to improve data quality. Because multiple numbers of clinical evaluators register many parameters concerning anesthetic patients in an everyday clinical set up, we cannot ensure controlled and uniform evaluation and registration of all parameters for all patients. However, the registration platform comprises several validation and completion rules, securing data completeness and preventing obscure data registration. The number of missing values (variable categorized as “unknown”) range between 0% and 11% for specific variables. Generally, the completeness of variables is high with missing values less than 2% for the large majority of the variables due to the fact that the final DAD record for each patient cannot be delivered to the central server without the obligatory fields filled in.
Follow-up
All data entered are transferred to an analytic portal every 24 hours allowing for day to day reporting and follow-up at the departmental level. All data are aggregated annually and contributing departments and clinics are measured through the clinical indicators.
Examples of research
Scientific papers from the DAD have been published in several major international peer-reviewed journals and include traditional epidemiologic studies focusing on interventions, organizational- and patient-related risk factors of importance for the perioperative treatment of patients. As each patient is entered into the database with a unique identifying social security number from the centralized civil register it is possible to link information from the DAD to other research databases or population-based registries. Thus, some publications are studies based upon a merger of more data sources than the DAD,1,3–6 and others are based upon data retrieved solely from the DAD.7–11 In the different studies the various covariates describing comorbidity have either been retrieved directly from the DAD, or if needed parameters have been retrieved from other data sources such as the Danish National Registry of Patients. Some of the publications are primarily dealing with specific anesthetic procedures, while other studies are focusing on specific types of surgery (eg, abdominal and hip fracture surgery).
The examples of studies previously represent traditionally epidemiological cohort studies. In addition, the DAD has served as a platform for a large intervention study, the DIFFICAIR trial, which was a stratified, parallel group, cluster (cluster = department) randomized, multicenter trial involving 28 departments of anesthesiology in Denmark. Patients were randomized to two different strategies of preoperative airway evaluation before tracheal intubation in association with general anesthesia. The database was programmed so that the registration of the specific airway evaluation was mandatory for the intervention group, but invisible to control departments. Data collection is finished and the results have been accepted for publication.12,13
Administrative issues and funding
The DAD is a part of the RKKP which constitutes the infrastructure of National Clinical Quality Databases as well as the funding. RKKP’s primary objective is to ensure a continued improvement in the utilization of the Danish clinical registries in a clinical as well as managerial, and research oriented sense. The RKKP supports centers of epidemiology and biostatistics affiliated to specialized university departments, with the responsibility for analytical methods including defining relevant register population, indicator algorithms, risk adjustment, and relevant interpretation of results in the yearly reports. Funding is revised and granted annually and the DAD has to pass appraisal in the National Health Authority every third year, with assessment of fulfillment of national criteria on functionality, data safety, and methodology. The DAD is also approved by the Danish Data Protection Agency (file number 2012-58-0023) and Statens Serum Institut (file number 14/15955). The database is led by a steering committee with representatives (clinicians) from all five national regions in Denmark, including a member and a chairman appointed by the Danish Society for Anesthesia and Intensive Care Medicine, thus representing the main clinical stakeholders.
Conclusion
The DAD is covering the anesthetic process for the majority of patients undergoing anesthesia in Denmark. The national coverage has until now been ~70%. However, the degree of completeness and data quality will improve steadily with the latest revision of indicators and improved data entry in the following year.
Acknowledgments
We want to thank the Danish Anesthesia Database and the participating departments. This paper was funded by the Program for Clinical Research Infrastructure (PROCRIN) established by the Lundbeck Foundation and the Novo Nordisk Foundation, and administered by the Danish Regions.
Disclosure
All authors are members of the steering committee of DAD. The authors have no other conflicts of interest to disclose in this work.
References
Vester-Andersen M, Lundstrom LH, Moller MH, et al. Mortality and postoperative care pathways after emergency gastrointestinal surgery in 2904 patients: a population-based cohort study. Br J Anaesth. 2014;112(5):860–870. | |
Lundstrom LH. Detection of risk factors for difficult tracheal intubation. Dan Med J. 2012;59(4):B4431. | |
Lund CA, Moller AM, Wetterslev J, Lundstrom LH. Organizational factors and long-term mortality after hip fracture surgery. A cohort study of 6143 consecutive patients undergoing hip fracture surgery. PLoS One. 2014;9(6):e99308. | |
Jorgensen ME, Torp-Pedersen C, Gislason GH, et al. Time elapsed after ischemic stroke and risk of adverse cardiovascular events and mortality following elective noncardiac surgery. JAMA. 2014;312(3):269–277. | |
Lohse N, Lundstrom LH, Vestergaard TR, et al. Anaesthesia care with and without tracheal intubation during emergency endoscopy for peptic ulcer bleeding: a population-based cohort study. Br J Anaesth. 2015;114(6):901–908. | |
Vester-Andersen M, Lundstrom LH, Buck DL, Moller MH. Association between surgical delay and survival in high-risk emergency abdominal surgery. A population-based Danish cohort study. Scand J Gastroenterol. 2016;51(1):121–128. | |
Lundstrom LH, Moller AM, Rosenstock C, et al. A documented previous difficult tracheal intubation as a prognostic test for a subsequent difficult tracheal intubation in adults. Anaesthesia. 2009;64(10):1081–1088. | |
Lundstrom LH, Moller AM, Rosenstock C, et al. Avoidance of neuromuscular blocking agents may increase the risk of difficult tracheal intubation: a cohort study of 103,812 consecutive adult patients recorded in the Danish Anaesthesia Database. Br J Anaesth. 2009;103(2):283–290. | |
Lundstrom LH, Moller AM, Rosenstock C, Astrup G, Wetterslev J. High body mass index is a weak predictor for difficult and failed tracheal intubation: a cohort study of 91,332 consecutive patients scheduled for direct laryngoscopy registered in the Danish Anesthesia Database. Anesthesiology. 2009;110(2):266–274. | |
Norskov AK, Rosenstock CV, Wetterslev J, Astrup G, Afshari A, Lundstrom LH. Diagnostic accuracy of anaesthesiologists’ prediction of difficult airway management in daily clinical practice: a cohort study of 188 064 patients registered in the Danish Anaesthesia Database. Anaesthesia. 2015;70(3):272–281. | |
Stendell L, Lundstrom LH, Wetterslev J, Itenov TS, Rosenstock CV. Risk Factors for and Prediction of a Difficult Neuraxial Block: A Cohort Study of 73,579 Patients from the Danish Anaesthesia Database. Reg Anesth Pain Med. 2015;40(5):545–552. | |
Norskov AK, Rosenstock CV, Wetterslev J, Lundstrom LH. Incidence of unanticipated difficult airway using an objective airway score versus a standard clinical airway assessment: the DIFFICAIR trial–trial protocol for a cluster randomized clinical trial. Trials. 2013;14:347. | |
Norskov AK, Lundstrom LH, Rosenstock CV, Wetterslev J. Detailed statistical analysis plan for the difficult airway management (DIFFICAIR) trial. Trials. 2014;15:173. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.