Back to Journals » Infection and Drug Resistance » Volume 16
The CREPE Score: A Predictive Tool for Third-Generation Cephalosporin-Resistant Enterobacterales Pneumonia in Community Settings
Authors Khunkitti K, Sribenjalux W ![]() , Kuwatjanakul W
, Kuwatjanakul W ![]() , Arunsurat I, So-ngern A, Meesing A
, Arunsurat I, So-ngern A, Meesing A
Received 20 April 2023
Accepted for publication 21 June 2023
Published 27 June 2023 Volume 2023:16 Pages 4159—4169
DOI https://doi.org/10.2147/IDR.S417863
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Suresh Antony
Krisada Khunkitti,1,* Wantin Sribenjalux,2,3,* Waewta Kuwatjanakul,4 Itthiphat Arunsurat,5 Apichart So-ngern,6 Atibordee Meesing2,3
1Department of Internal Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 2Division of Infectious Diseases and Tropical Medicine, Department of Internal Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 3Research and Diagnostic Center for Emerging Infectious Diseases (RCEID), Khon Kaen University, Khon Kaen, Thailand; 4Microbiology Unit, Clinical Laboratory Section, Srinagarind Hospital Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 5Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 6Division of Sleep Medicine, Department of Internal Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
*These authors contributed equally to this work
Correspondence: Wantin Sribenjalux, Division of Infectious Diseases and Tropical Medicine, Department of Internal Medicine, Faculty of Medicine, 123 Moo 16 Mittraphap Road, Nai-Muang, Muang District, Khon Kaen, 40002, Thailand, Tel +66 4300 9700, Email [email protected]; [email protected]
Purpose: To evaluate risk factors and develop a prediction score for community-acquired pneumonia caused by third-generation cephalosporin-resistant Enterobacterales (3GCR EB-CAP).
Patients and Methods: A retrospective study was conducted by reviewing the medical records of patients hospitalized with community-acquired pneumonia caused by Enterobacterales (EB-CAP) between January 2015 and August 2021 at Srinagarind Hospital, Khon Kaen University, Thailand. Logistic regression was used to analyze clinical parameters associated with 3GCR EB-CAP. The coefficients of significant parameters were simplified to the nearest whole number for a prediction score, called the CREPE (third-generation Cephalosporin Resistant Enterobacterales community-acquired Pneumonia Evaluation).
Results: A total of 245 patients with microbiologically confirmed EB-CAP (100 in the 3GCR EB group) were analyzed. Independent risk factors for 3GCR EB-CAP included in the CREPE score were (1) recent hospitalization within the past month (1 point), (2) multidrug-resistant EB colonization (1 point), and (3) recent intravenous antibiotic use (2 points for within the past month or 1.5 points for between one and twelve months). The CREPE score had an area under the receiver operating characteristic curve (ROC) of 0.88 (95% CI 0.84– 0.93). Using a cut-off point of 1.75, the score had a sensitivity and specificity of 73.5% and 84.6%, respectively.
Conclusion: In areas with high prevalence of EB-CAP, the CREPE score can assist clinicians in selecting appropriate empirical therapy and reducing overuse of broad-spectrum antibiotics.
Keywords: community acquired pneumonia, Enterobacterales, third-generation cephalosporin-resistance, empirical antibiotics, CREPE score
Introduction
Community-acquired pneumonia (CAP) is recognized as a major cause of morbidity and mortality worldwide.1 Inadequate empirical antibiotic therapy has been linked to higher mortality rates in patients with sepsis due to pneumonia.2 On the other hand, the use of unnecessary broad-spectrum antibiotics has been associated with higher mortality rates in patients without shock due to antibiotic-resistant bacteria and Clostridioides difficile infection.3 In the past, the term “healthcare-associated pneumonia” (HCAP) was used to determine whether a patient should receive extended-spectrum antibiotics.4 However, recent studies have shown that using the HCAP category to determine initial therapy does not improve patient outcome, and can lead to unnecessary prescriptions of broad-spectrum antibiotics.5 As a result, the American Thoracic Society (ATS) and Infectious Diseases Society of America (IDSA) have recommended against using the HCAP category to determine empirical antibiotic treatment.6 A clinical practice guideline for the treatment of inpatient adults with CAP has been developed by the ATS and IDSA, including recommendations of empirical combination therapy using beta-lactam antibiotics in conjunction with macrolides or respiratory fluoroquinolones monotherapy to effectively target common pathogen.6 While this guideline addresses two important microorganisms, methicillin-resistant Staphylococcus aureus (MRSA) and Pseudomonas aeruginosa, which are resistant to standard first-line antibiotic therapy, it does not extensively discuss CAP caused by gram-negative bacteria in the order Enterobacterales (EB), which are typically more severe and have a higher mortality rate compared to other pathogens.7,8
The prevalence of EB among patients hospitalized with CAP in the US is low, at approximately 6%.7 However, Enterobacterales are one of the leading causes of CAP in Asia.9–12 For example, studies from a capital city in Thailand demonstrate prevalence rates of CAP caused by Enterobacterales (EB-CAP) up to 18%.10 In rural areas, Klebsiella pneumoniae accounted for more than one-third of the microbial etiology in hospitalized patients with CAP.13 According to the clinical practice guidelines from the ATS and IDSA, empiric standard regimen for nonsevere CAP in the inpatient setting, are adequate for covering common pathogens including Streptococcus pneumoniae, Haemophilus influenzae, Mycoplasma pneumoniae, methicillin-susceptible S. aureus, Legionella species, Chlamydia pneumoniae, and third generation cephalosporins susceptible EB.14 Considering the low prevalence of community-acquired MRSA pneumonia in Thailand15 and taking into account specific risks for P. aeruginosa,16 the decision for selecting empirical antibiotics for inpatients with CAP, whether following the guideline or a broader spectrum (eg, carbapenem or β-lactam/β-lactamase inhibitor), depends on the patient’s risk for multidrug resistant (MDR) EB.8,17 In the current study, the prevalence of CAP caused by MDR EB in certain regions was found to be as high as 19%17 with a higher mortality rate observed in patients who developed this condition compared to those infected with susceptible strains.18 Inappropriate empirical antibiotic treatment was one of the factors associated with mortality in this particular group.18 However, there have been few studies on risk factors for drug-resistant EB-CAP, and there is also no clear consensus on the appropriate empirical treatment for CAP in regions with a high prevalence of EB. This study aims to explore the risk factors associated with third-generation cephalosporin-resistant (3GCR) infections in patients with EB-CAP. Additionally, it seeks to propose a highly accurate clinical prediction score that can assist physicians in selecting appropriate empirical antibiotic regimens for patients presenting with CAP in areas with a high prevalence of EB.
Patients and Methods
Participants and Study Design
In this retrospective study, we conducted a chart review of patients admitted to Srinagarind Hospital, a university hospital in Northeast Thailand, between January 2015 and August 2021. We selected the medical records of patients 18 years of age or older who were hospitalized with a principal diagnosis of pneumonia according to the International Classification of Diseases 10th Edition Clinical Modification (ICD-10 CM) and had a positive culture for EB from at least one clinical specimen (sputum, tracheal suction, or blood) collected within two calendar days of the admission date. Patients with incomplete medical records or who were initially misdiagnosed with pneumonia according to the ICD-10 CM code were excluded to avoid selection bias and misclassification of exposure or outcome. Due to the uncommon occurrence of MDR EB-CAP, conducting prospective studies would be time-consuming and impractical in our specific context.
Clinical data were collected from the medical charts, including demographic characteristics (age, sex, weight, and height), previous medical conditions, tobacco use, patient status (bedridden, nursing home resident, tracheostomy dependent, home oxygen use), and current medications (immunosuppressants, chemotherapy, corticosteroids, and gastric acid suppressants). We also collected laboratory findings, chest radiography results, and microbiological data for EB and antibiotic susceptibility from the electronic database. Isolates were identified using the VITEK card system (VITEK® 2 Compact, BioMerieux, France) until 2021, after which matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS) was used. Susceptibility profiles were determined using automated broth microdilution (Sensititre ARIS 2X, Thermo Scientific, Lenexa, KS). We combined data from the medical charts and electronic records to gather data on the history of pneumonia, hospitalization (including at Srinagarind Hospital and other hospitals), use of intravenous (IV) or oral antibiotics, and history of EB colonization. We defined 3GCR EB as gram-negative bacteria in the order Enterobacterales that are resistant to at least one third-generation cephalosporin according to the Clinical Laboratory section of Srinagarind Hospital. All clinical breakpoints were based on Clinical and Laboratory Standards Institute (CLSI) criteria from the relevant year. The hospital mortality of each admission was recorded to evaluate the mortality rate from EB-CAP and identify potential risk factors for mortality due to EB-CAP.
Sample Size Calculation
The sample size for this study was calculated based on its primary objective, which is to differentiate the characteristics of patients with CAP caused by 3GCR EB from those with susceptible ones. To identify possible factors, we conducted a literature review8 and found that prior IV antibiotic use resulted in the largest required sample size. Using a formula for a case-control study with a binary outcome and a 1:1 ratio, we determined that a sample size of 120 participants per group was required for a power of 80%. Furthermore, considering the elements to be analyzed in the multivariate logistic regression analysis, we performed a recalculation of the sample size. The revised estimation indicated a minimum sample size requirement of 157 participants. We selected the larger one for conducting the study.
Operational Definitions
- Third-generation cephalosporins are a class of antibiotics that belong to the cephalosporin family, a group of beta-lactam antibiotics. They have an aminothiazolyl substitution in the side chain positions, which extends their spectrum of activity to include gram-negative bacteria. Examples of third-generation cephalosporins include cefotaxime, ceftriaxone, ceftazidime, cefoperazone, and cefixime.19
- Severe CAP was defined as CAP that required mechanical ventilation (invasive or non-invasive) or was combined with septic shock within the first calendar day after admission.8
- Multidrug resistant EB (MDR EB) was defined as Enterobacterales, which is non-susceptible to at least one agent in three or more antimicrobial categories.20
- Appropriate empirical antibiotic treatment was defined as the first antibiotic administered at least 24 hours before the in vitro susceptibility result of the culprit pathogen was available and matching the subsequent result.21 The unnecessary use of broad-spectrum empiric therapy, such as prescribing piperacillin/tazobactam or carbapenems for third-generation cephalosporin-susceptible EB, was not considered appropriate.22
Statistical Analysis
The baseline characteristics of the third-generation cephalosporin resistance and susceptible groups were compared using Pearson’s chi-squared test. If this test was not suitable, Fisher’s exact test was used instead. Categorical variables were presented as the number and percentage, while continuous variables were reported as the mean with standard deviation (SD) or median with interquartile range (IQR) depending on whether they were normally distributed. Chronological data, including recent hospitalization and prior antibiotic use, were divided into duration categories of within the past month, between one and three months, and three to twelve months. Patients with a history of hospitalization or exposure to antibiotics for more than 12 months prior to admission were included in the non-exposed group and used as a reference. Associations were expressed as odds ratios (ORs) with 95% confidence intervals (95% CIs). Clinical parameters strongly associated with 3GCR EB-CAP (P-value <0.01) in the univariate analysis were selected for multivariate logistic regression. The risk score was derived from the logistic regression model, using the coefficients of individual factors to weigh the clinical parameters in the predictive model. The receiver-operating characteristics (ROC) curve was constructed to determine the area under the ROC curve and the optimal cut-off point. All statistical analyses were performed using SPSS for Windows, version 28.0. A P-value of less than 0.05 was considered statistically significant.
Ethics Statement
Ethical approval for this study was obtained from Center for Ethics in Human Research, Khon Kaen University in accordance with the Declaration of Helsinki (Number HE631130). The need for patient consent was waived due to the retrospective nature of the study. The data were anonymized or maintained with confidentiality.
Results
A retrospective study was conducted on hospital admissions diagnosed with CAP at Srinagarind Hospital in Thailand between January 2015 and August 2021. Of the 269 cases that were microbiologically confirmed as caused by EB-CAP, three were misdiagnosed as pneumonia, and 21 cases’ data were unavailable. Therefore, a total of 245 CAP admissions were analyzed, of which 100 were cases of 3GCR EB-CAP. However, since the calculated number of cases of 3GCR EB-CAP was not met, all 245 CAP admissions were analyzed (Figure 1). The study included individuals with a median age of 74.6 years, of whom 149 (60.8%) were male. The proportion of bedridden patients was higher in the 3GCR EB-CAP group compared to the non-3GCR EB-CAP group (48.0 vs 31.3%, P-value = 0.008). Almost half of the 3GCR EB-CAP group (46%) had neurological disease, while only 31% of the others did (P-value = 0.017). The proportions of severe CAP requiring mechanical ventilation or vasopressors were not significantly different between two groups (Table 1).
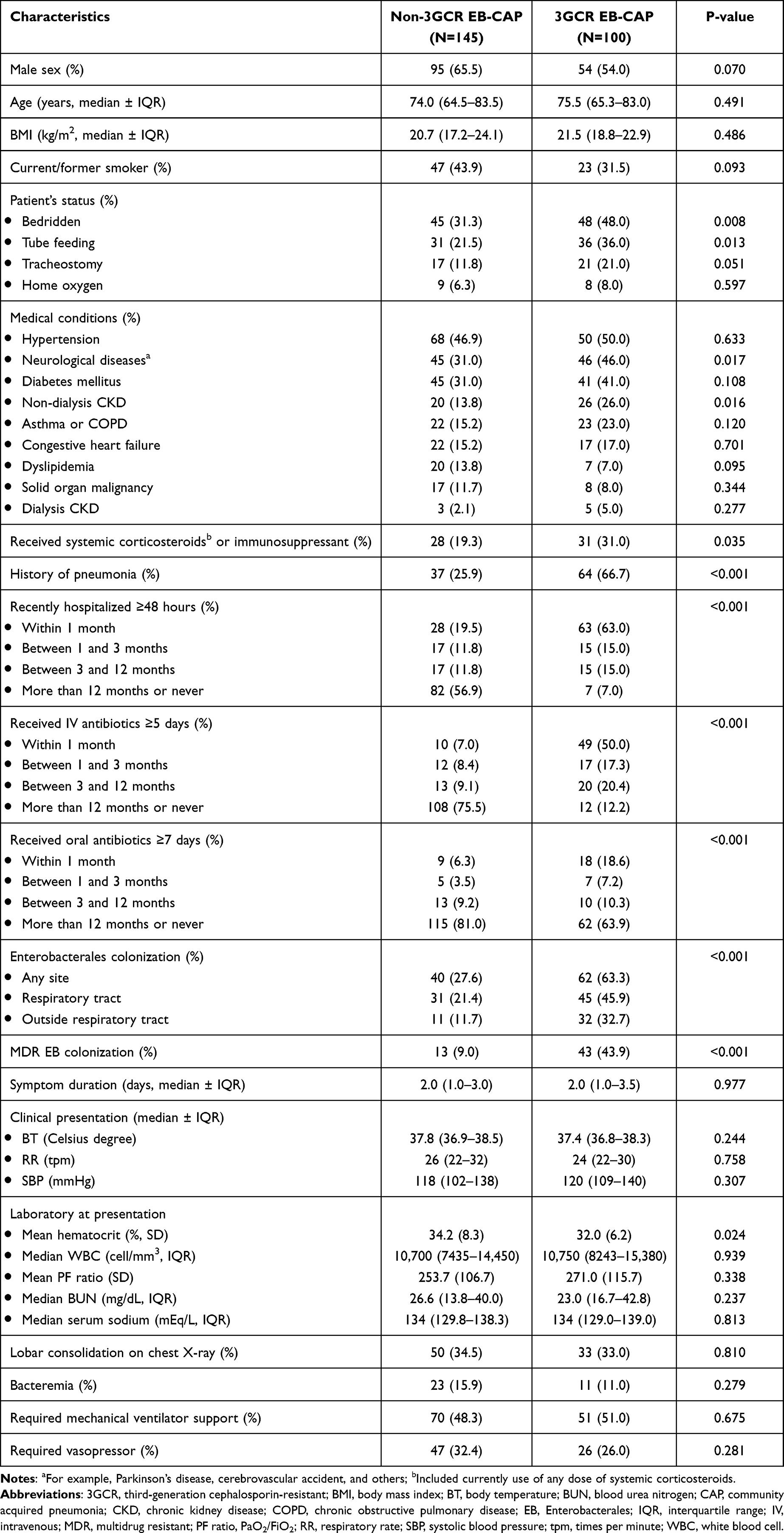 |
Table 1 Baseline Characteristics of All 245 Patients |
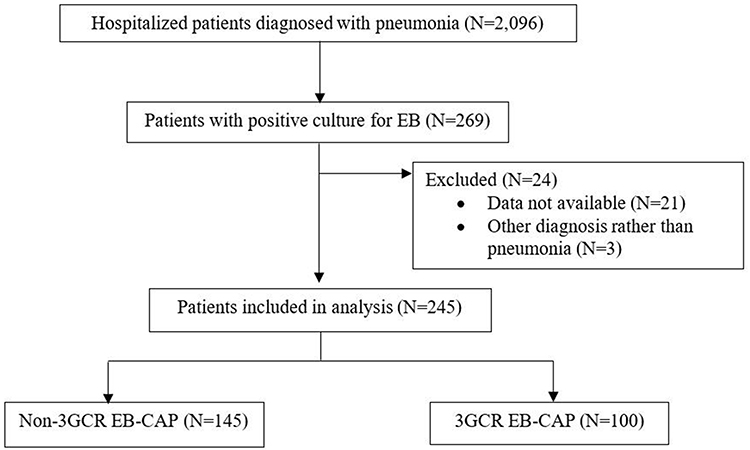 |
Figure 1 Trial profile for the study protocol. |
Univariate Analysis
The study found that several risk factors were associated with 3GCR EB-CAP in univariate analysis. These risk factors included a history of receiving IV antibiotics for at least five days within one year (OR 22.1, 95% CI 10.8–45.2), hospitalization within 1 year (OR 17.6, 95% CI 7.6–40.5), oral antibiotics use for at least seven days within one month (OR 3.71, 95% CI 1.57–8.75), EB colonization (OR 4.52, 95% CI 2.61–7.83), MDR EB colonization (OR 7.95, 95% CI 3.96–15.9), history of pneumonia (OR 5.73, 95% CI 3.25–10.1), chronic kidney disease (OR 2.20, 95% CI 1.15–4.21), tube feeding (OR 2.05, 95% CI 1.16–3.63), bedridden status (OR 2.03, 95% CI 1.20–3.44), neurological disease (OR 1.89, 95% CI 1.12–3.21), and current use of systemic corticosteroids or immunosuppressants (OR 1.88, 95% CI 1.04–3.39). The analysis also revealed that recent use of IV antibiotics and hospitalization within 1 month had a stronger correlation with 3GCR EB-CAP than the use of IV antibiotics and hospitalization in other intervals. The ORs for recent use of IV antibiotics and hospitalization within 1 month were 44.1 (95% CI 11.8–109.0) and 26.4 (95% CI 10.8–64.2), respectively (Table 2).
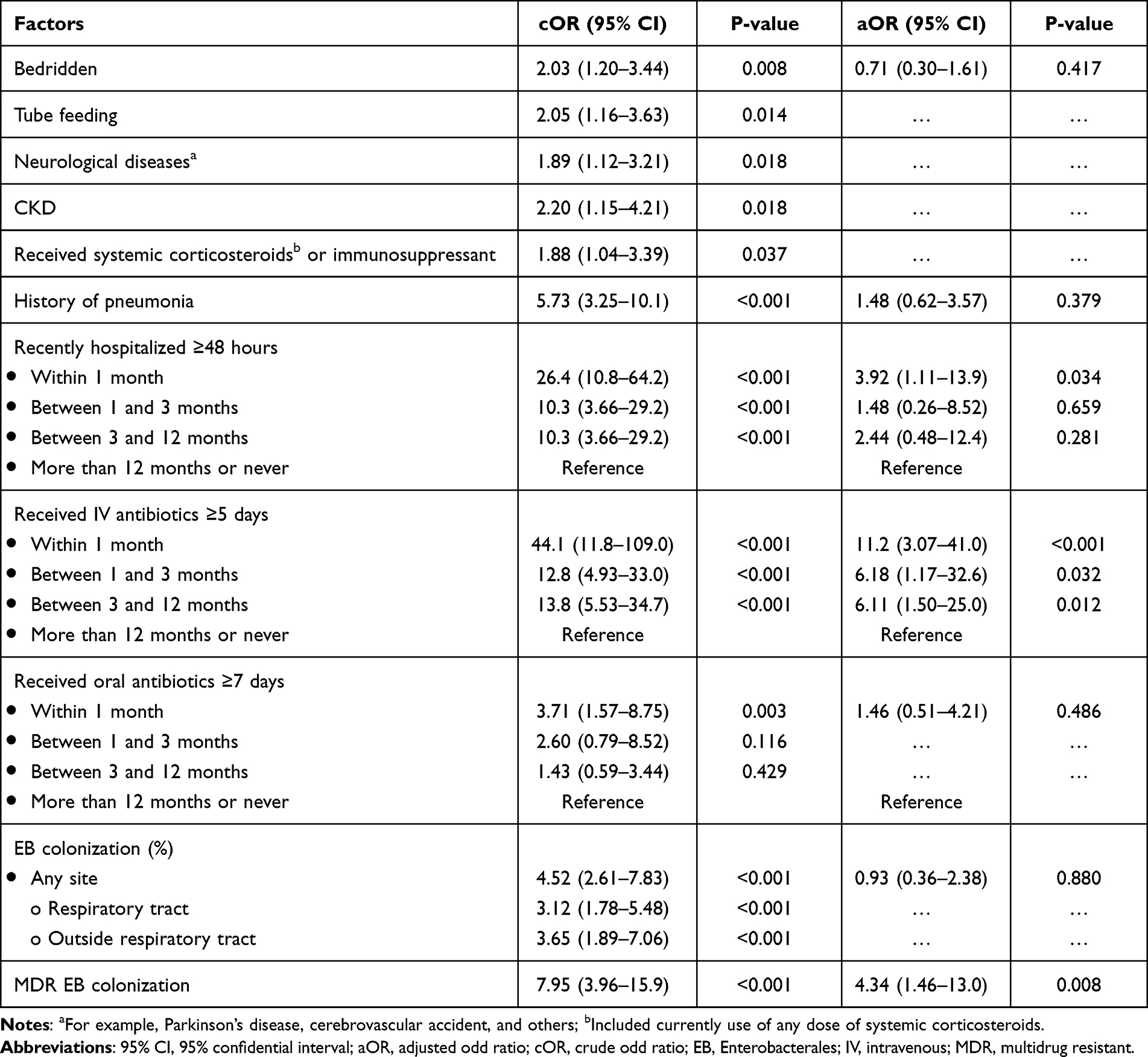 |
Table 2 Factors Associated with MDR EB-CAP, Univariate and Multivariate Analysis |
Multivariate Analysis
Highly related risk factors for 3GCR EB-CAP with a P-value <0.01, including being bedridden, a history of pneumonia, hospitalization within the past year, oral antibiotic use within the past month, EB colonization, and MDR EB colonization, were chosen for multiple logistic regression analysis. Recent IV antibiotic use within the past month was found to have a strong association with 3GCR EB-CAP, with an adjusted odds ratio (aOR) of 11.2 (95% CI 3.07–41.0). The association between IV antibiotics and 3GCR EB-CAP was found up to a duration of 12 months, with a lower association than one month with an aOR of 6.18 (95% CI 1.17–32.6) in one to three months and an aOR of 6.11 (95% CI 1.50–25.0) in patients exposed to IV antibiotics between 3 and 12 months. Other factors that were found to be associated with 3GCR EB-CAP included MDR EB colonization at any site (aOR 4.34, 95% CI 1.46–13.0) and a history of hospitalization within the past month (aOR 3.92, 95% CI 1.11–13.9). However, non-ambulatory status (aOR 0.71, 95% CI 0.30–1.61), having a history of pneumonia (aOR 1.48, 95% CI 0.62–3.57), having a history of oral antibiotic use within the past month (aOR 1.46, 95% CI 0.51–4.21), and having EB colonization (aOR 0.93, 95% CI 0.36–2.38) were not found to be significantly associated with 3GCR EB-CAP in the multivariate analysis (Table 2). The model displayed a robust relationship, as evidenced by the goodness-of-fit statistics. It achieved a Nagelkerke R Square of 0.552, along with a significant omnibus test (P-value <0.001).
Prediction Score
The logistic regression coefficients of significant risk factors are shown in Table 3. These coefficients were then simplified to the nearest number for a prediction score, called the CREPE (third-generation Cephalosporin Resistant Enterobacterales community acquired Pneumonia Evaluation) score, which is also shown in Table 3. The area under the receiver operating characteristic curve (ROC) of the score was 0.88 (95% CI 0.84–0.93) (Figure 2). The optimal cut-off point, as determined by the ROC curve, was 1.75, resulting in a sensitivity of 73.5% and specificity of 84.6%. When using a lower cut-off point of 1.25, the sensitivity increases to 87.8%, but the specificity decreases to 74.1%.
 |
Table 3 Multivariate Analysis of Factors Associated with MDR EB-CAP, Coefficients, and the CREPE Score for Predicting 3GCR EB-CAP |
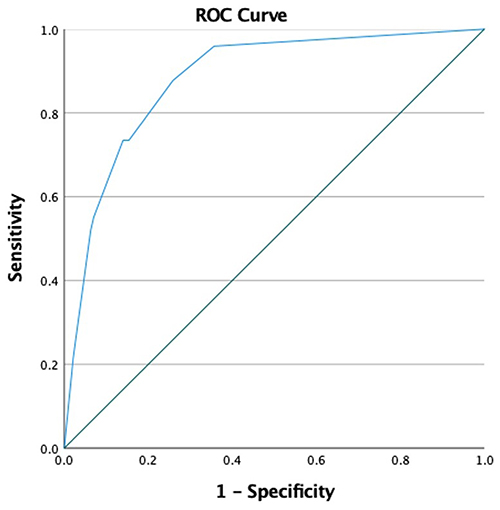 |
Figure 2 Receiver operating characteristic (ROC) curve of CREPE score for predicting 3GCR EB-CAP. |
Mortality Analysis
In this study, the prevalence of 3GCR EB-CAP among all EB-CAP cases was 40%. All-cause mortality among patients with EB-CAP during hospitalization was 20.8%. Characteristics of the patients classified by survival and risk factors potentially associated with in-hospital mortality are presented in the Supplementary Material. (Supplementary Table 1) Severe CAP, high initial blood urea nitrogen (more than 30 mg/dL), and history of EB colonization were significantly associated with case fatality in the multivariate analysis, with odds ratios of 2.70 (95% CI 1.27–5.73), 3.03 (95% CI 1.50–6.15), and 2.46 (95% CI 1.24–4.87), respectively (Supplementary Table 2). Appropriate empirical antibiotic treatment tends to associate with reduction in mortality but not met statistically significant (OR 0.53, 95% CI 0.28–1.00). CAP caused by MDR EB was not shown statistically significant association with in-hospital mortality in this study. The model exhibited a moderate relationship, supported by the goodness-of-fit statistics. It achieved a Nagelkerke R Square value of 0.205, and the omnibus test indicated a significant relationship (P-value <0.001).
Microbiological results
Microbiological results are presented in the Supplementary Material (Supplementary Table 3). K. pneumoniae was the most common cause of EB-CAP in the study with the prevalence of 64.1%, followed by Escherichia coli (22.4%), and Enterobacter spp. (6.8%), respectively. Out of the total 281 isolates, 100 were identified as 3-GCR (35.5%). Among the antibiotics tested, amikacin and meropenem exhibited the highest coverage against these pathogens, with susceptibility rates of 94% and 82%, respectively. Piperacillin/tazobactam showed good activity against MDR E. coli, with 80.6% susceptibility, but had higher resistance rates for MDR K. pneumoniae (30.9%) and Enterobacter spp. (25.0%).
Discussion
This study aimed to identify factors associated with 3GCR EB-CAP and develop a prediction score. Three independent factors were identified: recent hospitalization within the past month, MDR EB colonization, and recent IV antibiotic use within the past 12 months. The prediction score, known as the CREPE score, was derived from these factors and ranges from 0 to 4 points. With a cut-off point of 1.75, the CREPE score demonstrated good sensitivity (73.5%) and high specificity (84.6%). While most EB-CAP can be treated with a third-generation cephalosporin, as recommended by the ATS and IDSA guidelines,6 extended-spectrum antibiotics may be necessary in patients with risk factors for antibiotic-resistant pathogens.23 Hence, the CREPE score can aid in choosing the right empirical antibiotics for patients with CAP who reside in areas with a high prevalence of EB or with specific risk factors for EB-CAP. For stable, non-critically ill patients, using a cut-off score of 1.75 to prescribe broad-spectrum antibiotics can reduce unnecessary usage and improve specificity up to 84.6%. However, for critically ill patients, a lower cut-off point of 1.25 may be more suitable, as it offers high sensitivity at 87.8%. When the score is higher than the cut-off, it is crucial to consider the hospital’s microbiological profile and previous colonizing organisms, and to at least cover extended spectrum β-lactamase (ESBL) producing organisms due to the risk of third-generation cephalosporin resistance. This approach can help decrease the usage of unnecessary broad-spectrum antibiotics, which can contribute to drug-resistant organisms,24 and prevent high mortality rates associated with ineffective empirical antibiotics in severe cases.2
In this retrospective study, the use of IV antibiotics was found to have the strongest association with 3GCR EB-CAP, particularly recent use within the past month. This may be related to the mechanism of resistance from β-lactamase chromosome expression after exposure to β-lactam drugs.24 Many studies have demonstrated an association between the use of IV antibiotics and drug-resistant organisms causing CAP, with the last exposure to antibiotics being within three months.25,26 However, some studies, including this one, have found an association even with exposure to IV antibiotics for a duration up to one year.8,18 Recent hospitalization within the past month, even without the use of antibiotics, has been found to have an individual association with 3GCR EB-CAP in logistic regression, in line with findings in other studies.26 The potential mechanisms could be patient-to-patient transmission or exposure to MDR organisms in health-care facilities.27 Previous colonization with multidrug-resistant organisms (MDROs) has been identified as one of the risk factors for MDR CAP. Evidence supports a strong association with MRSA and P. aeruginosa.5,26 In addition, the association was also found in MDR EB.1,26 However, the duration between the last positive culture for MDROs and the onset of MDR EB-CAP has not been definitively demonstrated. Thus, in this study, we considered all patients with a history of MDR EB colonization at any time as the exposure group. With these significant risk factors, primary physicians should be concerned about their patients having a higher chance of infection by MDR pathogens. It is crucial to make appropriate antibiotic choices in response.
Non-ambulatory status and enteral tube feeding were independent risk factors for MDR EB-CAP in some studies8,26 and non-ambulatory status, tube feeding, and neurological disease were also found to be associated with 3GCR EB-CAP in univariate analysis of this study. However, as these factors share similar characteristics, such as patients with non-ambulatory status or tube feeding may also have underlying neurological disease, they were analyzed as a group in a multicollinearity analysis using non-ambulatory status as a representative factor. Non-ambulatory status in multivariate analysis did not show a significant association with 3GCR EB-CAP in this study. This suggests that being bedridden or receiving tube feeding may not be direct risk factors for MDROs, but non-ambulatory status may be associated with exposure to other strong risk factors such as previous infection, exposure to antibiotics, and hospitalization. In this study, current use of immunosuppressive drugs was not found to be associated with 3GCR EB-CAP in multivariate analysis, although some studies have shown an association.26 The inadequate number and wide range of stages of immunosuppression in the study may have contributed to the non-statistically significant result. Although immunocompromise has been shown to be associated with EB-CAP through the mechanism of EB translocation from the gastrointestinal tract,1 recent consensus recommends using broad-spectrum antibiotics to cover drug-resistant gram-negative bacilli in CAP treatment only when immunocompromised patients have other risk factors for MDROs,28 Therefore, it may be reasonable not to include immunocompromise status in the CREPE score.
Following the recommendation to avoid using the term HCAP,6 several prediction scores have been proposed for predicting drug-resistant pathogens in CAP, including the DRIP, Shorr, and PES scores.29–31 While the parameters included in the scores differ, they share some well-established risk factors, such as colonization of drug-resistant pathogens, history of hospitalization, and antibiotic use. However, the specific drug-resistant organisms focused on by these scores were different. For example, the DRIP and Shorr scores focused on MRSA and P. aeruginosa,29,30 while the PES score also included ESBL producing EB.31 After validation, the sensitivity and specificity of each score may vary depending on the local epidemiology.29,32,33 Since the CREPE score is designed to predict 3GCR EB-CAP, it may be suitable for areas with a high prevalence of EB-CAP, such as in Asia.10
This study has some limitations. Firstly, being a retrospective study, there is a possibility of missing information regarding the patients’ medical history, such as their history of taking antibiotics from a drug store or colonization with MDR EB from other hospitals, as this information may not have been communicated to the physician or recorded in the medical records. Additionally, the data extracted from medical records relied on the history-taking of primary physicians. Therefore, there is a potential for recall bias, as the accuracy of information recorded at the time of the patient’s visit may be affected, leading to potential bias in the data sources. Secondly, although we included all patients with EB-CAP from the institute, the number of patients in the 3GCR EB group were still less than the requirement from calculation, and might lead to under-detected some risk factors. However, upon reviewing our sample size, we found that we still achieved 79.8% power for the study, and the calculated area under the ROC curve demonstrated good performance of the CREPE score. Strong risk factors made less-associated risk factors are unlikely to significantly impact the probability of 3GCR EB-CAP. Moreover, parameters in the score are consistent with common factors from other scores, and controversial risk factors from other scores were excluded.29–31 Finally, resulting from inclusion of all EB-CAP patients, there are no available data for score validation. Further studies, particularly utilizing randomized control designs, should be conducted to validate the score and evaluate its impact on reducing the overuse of unnecessary broad-spectrum antibiotics.
Conclusion
It is crucial to assess the risk of MDR pathogens in empirical antibiotics for CAP. The CREPE score, which includes risk factors such as previous hospitalization, colonization of MDR EB, and prior IV antibiotics use, can be a helpful tool to consider along with local epidemiology and resistance patterns to select suitable empirical antibiotics.
Acknowledgments
We would like to express our gratitude to Associate Professor Siriluck Anunnatsiri for her role as a consultant in our reviewer’s responses.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Assefa M. Multi-drug resistant gram-negative bacterial pneumonia: etiology, risk factors, and drug resistance patterns. Pneumonia. 2022;14:4.
2. Kuti EL, Patel AA, Coleman CI. Impact of inappropriate antibiotic therapy on mortality in patients with ventilator-associated pneumonia and blood stream infection: a meta-analysis. J Crit Care. 2008;23(1):91–100.
3. Rhee C, Kadri SS, Dekker JP, et al. Prevalence of antibiotic-resistant pathogens in culture-proven sepsis and outcomes associated with inadequate and broad-spectrum empiric antibiotic use. JAMA Netw Open. 2020;3(4):e202899.
4. Niederman MS. Hospital-acquired pneumonia, health care-associated pneumonia, ventilator-associated pneumonia, and ventilator-associated tracheobronchitis: definitions and challenges in trial design. Clin Infect Dis. 2010;51(Suppl 1):S12–7.
5. Ewig S, Kolditz M, Pletz MW, et al. Healthcare-associated pneumonia: is there any reason to continue to utilize this label in 2019? Clin Microbiol Infect. 2019;25(10):1173–1179.
6. Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia: an official clinical practice guideline of the American thoracic society and infectious diseases society of America. Am J Respir Crit Care Med. 2019;200(7):e45–67.
7. von Baum H, Welte T, Marre R, et al. Community-acquired pneumonia through Enterobacteriaceae and Pseudomonas aeruginosa: diagnosis, incidence and predictors. Eur Respir J. 2010;35(3):598–605.
8. Villafuerte D, Aliberti S, Soni NJ, et al. Prevalence and risk factors for Enterobacteriaceae in patients hospitalized with community-acquired pneumonia. Respirol Carlton Vic. 2020;25(5):543–551.
9. Luan Y, Sun Y, Duan S, et al. Pathogenic bacterial profile and drug resistance analysis of community-acquired pneumonia in older outpatients with fever. J Int Med Res. 2018;46(11):4596–4604.
10. Peto L, Nadjm B, Horby P, et al. The bacterial aetiology of adult community-acquired pneumonia in Asia: a systematic review. Trans R Soc Trop Med Hyg. 2014;108(6):326–337.
11. Tran HD, Bach Nguyen YT, Thanh Tran T, et al. Community-acquired pneumonia-causing bacteria and antibiotic resistance rate among Vietnamese patients: a cross-sectional study. Medicine. 2022;101(36):e30458.
12. Qu J, Zhang J, Chen Y, et al. Aetiology of severe community acquired pneumonia in adults identified by combined detection methods: a multi-centre prospective study in China. Emerg Microbes Infect. 2022;11(1):556–566.
13. Olsen SJ, Laosiritaworn Y, Siasiriwattana S, et al. The incidence of pneumonia in rural Thailand. Int J Infect Dis. 2006;10(6):439–445.
14. Bjarnason A, Westin J, Lindh M, et al. Incidence, etiology, and outcomes of community-acquired pneumonia: a population-based study. Open Forum Infect Dis. 2018;5(2):ofy010.
15. Mekviwattanawong S, Srifuengfung S, Chokepaibulkit K, et al. Epidemiology of Staphylococcus aureus infections and the prevalence of infection caused by community-acquired methicillin-resistant Staphylococcus aureus in hospitalized patients at Siriraj Hospital. J Med Assoc Thai. 2006;89(Suppl 5):S106–117.
16. Restrepo MI, Babu BL, Reyes LF, et al. Burden and risk factors for Pseudomonas aeruginosa community-acquired pneumonia: a multinational point prevalence study of hospitalised patients. Eur Respir J. 2018;52:1701190.
17. Aston SJ, Wootton DG. Community-acquired pneumonia due to drug-resistant Enterobacteriaceae: a global perspective. Respirology. 2020;25(5):468–469.
18. Maruyama T, Fujisawa T, Ishida T, et al. A therapeutic strategy for all pneumonia patients: a 3-year prospective multicenter cohort study using risk factors for multidrug-resistant pathogens to select initial empiric therapy. Clin Infect Dis. 2019;68(7):1080–1088.
19. Klein NC, Cunha BA. Third-generation cephalosporins. Med Clin North Am. 1995;79(4):705–719.
20. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281.
21. Fraser A, Paul M, Almanasreh N, et al. Benefit of appropriate empirical antibiotic treatment: thirty-day mortality and duration of hospital stay. Am J Med. 2006;119(11):970–976.
22. Mettler J, Simcock M, Sendi P, et al. Empirical use of antibiotics and adjustment of empirical antibiotic therapies in a university hospital: a prospective observational study. BMC Infect Dis. 2007;7:21.
23. Cillóniz C, Dominedò C, Torres A. Multidrug resistant gram-negative bacteria in community-acquired pneumonia. Crit Care. 2019;23:79.
24. Dever LA, Dermody TS. Mechanisms of bacterial resistance to antibiotics. Arch Intern Med. 1991;151(5):886–895.
25. Madaras-Kelly KJ, Remington RE, Fan VS, et al. Predicting antibiotic resistance to community-acquired pneumonia antibiotics in culture-positive patients with healthcare-associated pneumonia. J Hosp Med. 2012;7(3):195–202.
26. Shindo Y, Ito R, Kobayashi D, et al. Risk factors for drug-resistant pathogens in community-acquired and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2013;188(8):985–995.
27. Baljin B, Gurjav U, Tulgaa K, et al. High acquisition rate of gram-negative multi-drug resistant organism colonization during hospitalization: a perspective from a high endemic setting. Infect Drug Resist. 2021;14:3919–3927.
28. Ramirez JA, Musher DM, Evans SE, et al. Treatment of community-acquired pneumonia in immunocompromised adults. Chest. 2020;158(5):1896–1911.
29. Fadrian F, Chen K, Kumalawati J, et al. The validation of drug resistance in pneumonia (DRIP) score in predicting infections due to drug-resistant pathogens in community-acquired pneumonia at Cipto Mangunkusumo Hospital, Jakarta, Indonesia. Acta Medica Indones. 2021;53(4):416–422.
30. Shorr AF, Myers DE, Huang DB, et al. A risk score for identifying methicillin-resistant Staphylococcus aureus in patients presenting to the hospital with pneumonia. BMC Infect Dis. 2013;13:268.
31. Prina E, Ranzani OT, Polverino E, et al. Risk factors associated with potentially antibiotic-resistant pathogens in community-acquired pneumonia. Ann Am Thorac Soc. 2015;12(2):153–160.
32. Ceccato A, Mendez R, Ewig S, et al. Validation of a Prediction Score for Drug-Resistant Microorganisms in Community-acquired Pneumonia. Ann Am Thorac Soc. 2021;18(2):257–265.
33. Oliver MB, Fong K, Certain L, et al. Validation of a community-acquired pneumonia score to improve empiric antibiotic selection at an academic medical center. Antimicrob Agents Chemother. 2021;65(2):e01482–20.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.