Back to Journals » Psychology Research and Behavior Management » Volume 15
The COVID-19 Pandemic and Overall Wellbeing: Mediating Role of Virtual Reality Fitness for Physical-Psychological Health and Physical Activity
Authors Peng X, Menhas R ![]() , Dai J
, Dai J ![]() , Younas M
, Younas M ![]()
Received 5 April 2022
Accepted for publication 5 July 2022
Published 13 July 2022 Volume 2022:15 Pages 1741—1756
DOI https://doi.org/10.2147/PRBM.S369020
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Xiang Peng,1,2 Rashid Menhas,3 Jianhui Dai,2 Muhammad Younas4
1College of Physical Education, Hunan City University, Yiyang, People’s Republic of China; 2College of Physical Education and Sports, Soochow University, Suzhou, People’s Republic of China; 3Research Center of Sports Social Sciences, College of Physical Education and Sports, Soochow University, Suzhou, People’s Republic of China; 4School of Education, Soochow University, Suzhou, People’s Republic of China
Correspondence: Rashid Menhas, Research Center of Sports Social Sciences, College of Physical Education and Sports, Soochow University, Suzhou, People’s Republic of China, Email [email protected] Jianhui Dai, College of Physical Education and Sports, Soochow University, Suzhou, People’s Republic of China, Email [email protected]
Background: Virtual reality applications are made for various objectives such as business, entertainment, education, and healthcare. Anxiety, phobias, distress, disordered eating, drug addiction, panic disorder, post-traumatic stress disorder, schizophrenia, bipolar disorder, psychosis, depression, and autism spectrum disorders may benefit from virtual reality-based approaches. The 2019 coronavirus (COVID-19) pandemic has impacted the way we live, enjoy, study, sport, and socialize significantly. Virtual reality fitness technology gained much attention during the COVID-19 preventive measures time.
Objective: The present study explores the role of virtual reality fitness in improving overall wellbeing during the COVID-19 pandemic home isolation period in terms of physical-psychological health and physical activity.
Methods: A total of 2300 individuals were recruited using the snowball sampling technique to participate in the study. The primary data were collected using an anonymous web-based survey. SPSS-23 and Smart-PLS 3.2.9 software were used to analyze the data.
Results: The direct path coefficient analysis of the study constructs show that virtual reality fitness has (preventive measures -> virtual reality fitness -> overall wellbeing, preventive measures -> virtual reality fitness -> physical exercise, and preventive measures -> virtual reality fitness -> physical health) profound effects on the research participants’ mental and physical wellbeing of the study participants while indirect mediation analysis shows that virtual reality fitness has (preventive measures -> virtual reality fitness ->overall wellbeing, preventive measures -> virtual reality fitness -> physical exercise, preventive measures -> virtual reality fitness ->physical health) significant impacts.
Conclusion: Our study results concluded that house exercises through virtual reality fitness are a good substitute for public gyms and private group fitness programs during the first pandemic wave for physical-psychological and overall wellbeing. Virtual reality fitness technology can alleviate many of the challenges brought on by the epidemic, resulting in increased utilization.
Keywords: COVID-19, virtual reality fitness, lockdown, psychological and physical health, overall wellbeing
Introduction
The COVID-19 pandemic has significantly influenced how we work, play, study, exercise, and socialize. Virtual reality (VR) technology can alleviate many of the issues posed by the epidemic, prompting growing usage.1 Virtual reality training has recently been viewed as another technique to deal with enhanced physical activity and wellness practices, and it is increasingly being used in improving health.2 Scientists have shown that virtual reality exercise improves the mental benefits of physical activity and increases the likelihood of long-term workout persistence.3 VR is a novel technology that has the potential to be used in medicine. It is the interface of humans with computers in a practical and realistic environment. In a virtual world, it delivers perceptual and intellectual exercises. Virtual reality has been employed in various medical sectors, but rehabilitate science is the most recent user of this technology.4
VR can improve physiological, psychological, and rehabilitative outcomes in healthy and clinical populations. Physiological and emotional wellbeing are critical aspects of our life. Professionals in the medical field tirelessly enhance men’s wellness and quality of lifestyle. These tremendous technological advancements have favorably affected and improved medical and healthcare services.5 From a psychological and metabolic standpoint, maintaining a physically active lifestyle while taking care looks to be a straightforward hygiene approach.6 It’s crucial to comprehend the processes that underpin exercise’s beneficial benefits.7 VR-based fitness activities are also fun and encouraging. Still, they also give data that tells the user how well they are doing and establish goals appropriately. Diabetic, dementia, Psoriatic arthritis, cord injury, brain injury, multiple sclerosis, Down's syndrome, and aging have all been demonstrated to be useful in healing physical and mental symptoms induced by VR-based games.8
According to research, workout games enhance perceptual and cognitive capabilities, endurance, balancing synchronization, response speed, and exercise habits.9 Exercising enhances sensory and motor capabilities, strength, balance coordination, response speed, and exercise habits. It aids not only the physiological but also the psychological components. It improves learning and memory and helps those with chronic conditions fight depression. The bulk of its applications are for people with various physical and mental illnesses, but it may also promote good health. It can enhance the elderly’s standard of living and aid in the battle against aging.10 Virtual reality-based games have been utilized worldwide for health and therapeutic reasons over the past decade, with favorable results. Virtual reality is computer software that simulates sensory experiences such as visual, aural, tactile, and olfactory sensations while allowing users to control items within the simulated space.11 Perceptions and beliefs have been shown to impact health and wellbeing significantly and very well. Several studies have shown that having good health ideas and advantages regarding fitness improves one’s health.12 The findings of these and other studies have been so persuasive that assessing perception and belief, for example, must be evaluated and potentially controlled for in medical and psychiatric research methods by integrating placebo situations. With the awareness that perspective can positively impact health and wellbeing, researchers are looking at new ways to change perception to see whether it can improve health outcomes. Virtual reality, for example, is currently one of the most promising paths of investigation in this field. Virtual reality is technology’s solution to a different state of consciousness, and it has been shown to improve psychological health through modifying perception and the behaviors that follow.13
Virtual reality’s impacts have also been studied in the context of disabled people who cannot engage in numerous workouts due to limited mobility. For example, researchers employed augmented reality, a virtual reality method, to treat akinesia, or halting gait, in Parkinson’s disease.14 Virtual reality allows disabled people to participate in previously dangerous or impossible things to perform. Furthermore, virtual reality can provide corrective experiences that can change attitudes and concerns, resulting in fresh insights into pathogenic mechanisms and inventive solutions that may be used to re-enable impaired people.15 Virtual reality, particularly augmented reality (AR), has lately emerged as an important tool for suitable treatment in a variety of health-related areas, including (a) evaluation, (b) diagnostic, (c) treatment, and (d) fellow human. VR has been widely employed in rehabilitation to effectively manage neuro-developmental disorders (NDDs) such as attention deficit disorder (ADHD) and autistic spectrum diseases (ASD).16 COVID-19 has a negative influence on psychological aspects of health reported by Akter et al17 which further influences overall wellbeing.18,19
Mixing virtual reality with common exercise devices, such as the stationary exercise bike utilized in this study, may help to boost exercise’s psychological effects. Additional psychological benefits may increase the likelihood of long-term exercise programmed adherence, create a sense of pressure and controlled competitiveness, and conclude a more joyful exercise experience in general.20 Goal planning, monitoring, incentives, and social considerations are common strategies used in fitness technology.21 In the disciplines of public health and kinesiology, the progress of VR technology and its application during PA through its integration with standard exercise apparatus and restoration procedures have received a lot of interest. As a therapeutic tool, VR treatment allows users to intensify repetitious exercises and boost auditory and visual input, assembling it more engaging than old-style physical remedies while offering no major harm or physical limits.22 Previous studies looked at the properties of virtual reality exercise on psychological, rehabilitative, and physiological results. VR has been suggested to help stroke patients improve their lower limb function.23 VR exercise has been demonstrated to enhance balance in patients with Parkinson’s disease (PD), stroke, and children with cerebral palsy (CP).24 Virtual reality apps have been developed for various purposes, including pleasure, entertainment, commerce, and medicine. Virtual reality has benefitted users’ mental health in a variety of ways. Most aspects of our lives have been affected by the Covid-19 epidemic. The quarantine enforcement by the health experts impacted the quality of life in terms of socioeconomic, physical health, physical activity, psychological and overall wellbeing. A growing body of research suggests that customers’ mental and physical wellbeing can be profoundly influenced by their participation in computer-generated virtual reality activities. The present study explores the role of virtual reality fitness (VrF) in improving overall wellbeing during the COVID-19 pandemic home isolation period in terms of physical-psychological health and physical activity (see Figure 1). For detailed hypotheses of the study, see (Supplementary Hypotheses of the Study).
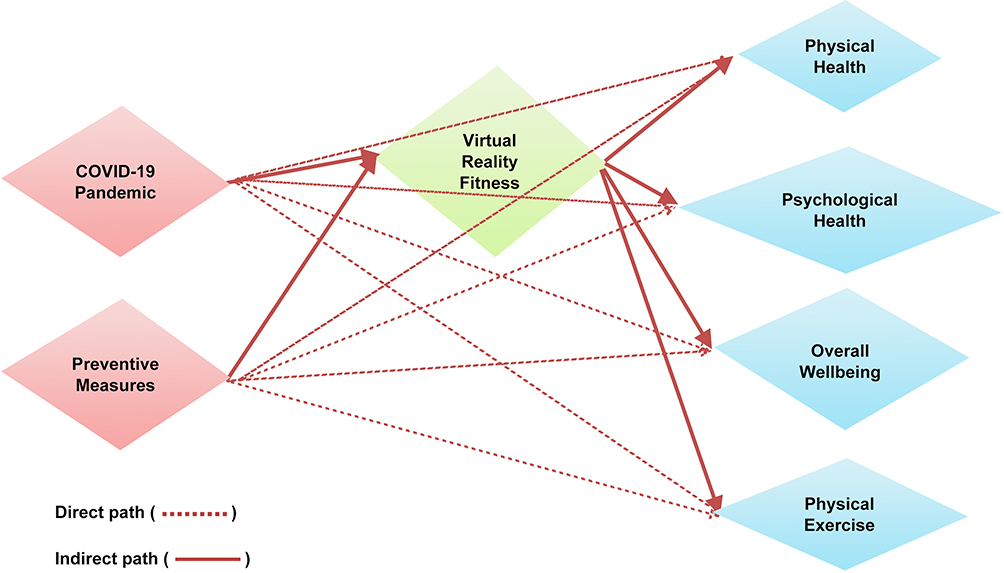 |
Figure 1 Proposed relationship of the study variables. |
Materials and Methods
The present study was conducted in the People’s Republic of China. The World Medical Helsinki Policy parameters were adopted in the research, and the study was approved by the ethics committee of Soochow University, Suzhou, Jiangsu, China. Informed consent was taken from the study participants before conducting the final survey.
Study Participants
The current study focused on people living in home isolation in Guangdong province during the pandemic. A snowball sampling strategy was adopted to obtain primary data for the study. The eligibility criteria to participate in the survey were +19 years old, must have high school level education, and using virtual reality fitness to improve the quality of life during the home quarantine. A total of 2300 individuals were recruited using the snowball sampling technique to participate in the study.
Data Collection Tool and Procedures
After reviewing the relevant literature and previously validated instruments,25,26 an initial questionnaire survey was developed in Chinese. The questionnaire survey was pre-tested with 40 people to ensure a valid response rate. After pre-testing, certain questions were altered to get the best and most accurate answer. The primary data were collected using an anonymous web-based survey. A web-based survey link was sent to the study participants using social media such as Wechat, QQ, Douyin, Weibo, Hellotalk, Kuaishou, Zhihu, and Bilibili. A total of 2300 individuals have received the web-based questionnaire survey link with the study purpose and instructions related to the completion and submission of the survey (15th January to 15th March 2020). Table 1 shows the survey questionnaire distribution statistics. A total of 100 respondents, about 4.35% of data were excluded because of wrong and incomplete data after performing the quality check by the study’s principal investigator. The data from 2200 respondents (95.65%) was used in the final analysis.
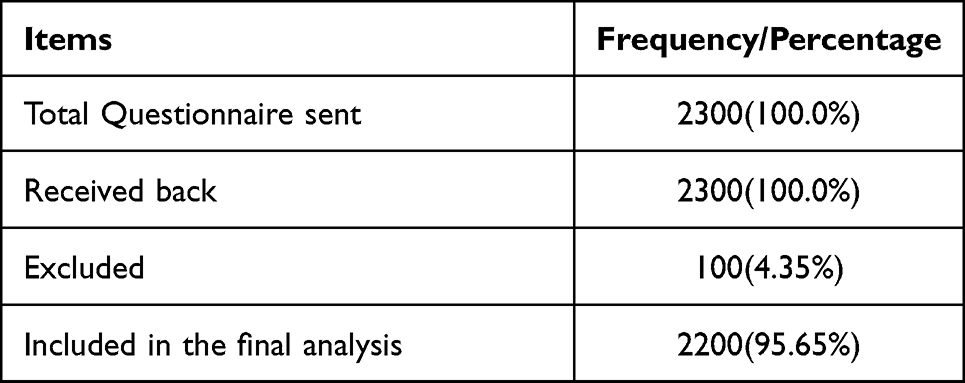 |
Table 1 Distribution Statistics of the Questionnaire |
Study Constructs Operationalization
Demographics
Background questions were based upon gender (male, female, others), age (19–20, 21–25, 26–30, 31–35, 36–40, 41+), education (high school, college graduate, and university graduate), occupation (government employee, self-employed, private companies employee, student, no occupation, retired), marital status (single; unmarried, cohabitant, married, divorced, widowed, separated), cohabitation at home (live alone, live with family, live with pets, others) and consciousness about COVID-19 (low, moderate, high).
COVID-19 Pandemic and Preventive Measures
Quarantine, self-isolation, or lockdown may make it difficult for certain persons to exercise. During quarantine, self-isolation, and lockdown, the population’s general physical mobility is stated to be considerably decreased, with serious negative health and wellbeing consequences.27 Because of COVID-19ʹs high infectivity and toxicity, maintaining social distance is crucial in preventing the virus’s transmission.28 On the other hand, the social distance technique is unfavorable for mental health since it reduces face-to-face and group physical activity.29 The psychological discomfort caused by the epidemic may be exacerbated by the constrained social connection brought on by social separation.30 The survey participants were given questions on the COVID-19 pandemic and preventative measures (lockdown, quarantine, social distance, wearing the mask, washing hands, using sanitizer, avoiding travel and crowded areas, vaccine) using a 5-point Likert scale.
Virtual Reality Fitness and Overall Wellbeing
Virtual reality fitness’s role in the improvement of overall wellbeing related to 5-points Likert scale questions (using virtual reality fitness is helpful to reduce depression anxiety, using virtual reality fitness is helpful to maintain an active living and physical activity, using virtual reality fitness is helpful to maintain physical health, using virtual reality fitness is helpful in psychological Wellbeing) were asked to the study participants. Physical and emotional wellbeing are critical aspects of our lives. Tremendous technological advancements have favorably affected and enhanced medical and healthcare services in the past several decades. Virtual reality has been employed in various medical sectors, but rehabilitation science is the most recent user of this technology. Fitness games based on virtual reality are entertaining and inspiring, but they also provide information that specifically states how they do and helps them set appropriate objectives. Virtual reality is an interactive technology that can be used in healthcare. It is the interaction of humans with computers in a practical and realistic environment. In a virtual world, it delivers sensorimotor and cognitive exercises. Diabetic, strokes, Psoriatic arthritis, spinal injury, brain injury, sclerosis, cerebral palsy, and aging have all been shown to benefit from virtual reality-based games in treating and curing physical and mental symptoms.31–33
Data Analysis
SPSS-23 and Smart-PLS 3.2.9 software were used to analyze the data.34 Univariate, bivariate, and multivariate statistical analyses were performed. The data were analyzed in two steps: first, a measuring model was established to evaluate construct validity, reliability, and convergent validity, and then a structural model was created to test the hypothesis.35,36
Results
Characteristics of the Study Participants
Table 2 statistics show that the majority of the study individuals (53.41%) were male, female (43.05%), and (3.54%) were others. Age distribution shows that major proportion belongs to (25.64%:21–25), (24.95%: 19–20), (20.45%: 26–30), (17.23%: 31–35), (5.5%: 36–40) and (6.23%: 41+). The educational paradigm shows that half of the participants were university graduates (50.0%), college graduates (31.5%), and high school graduates (18.5%). Occupation distributions show that the majority were students (34.14%), self-employed (25.77%), private companies employees (17.41%), no occupation and retired (13.5%), and government employees (8.32%). In the context of marital status, a major proportion (45.14%) belongs to the single (unmarried), married (42.04%), divorced (4.91%), cohabitant (3.41%), widowed (2.5%), and separated (2.0%). Cohabitation at the home statistics show that most study participants (33.14%) lived with their families, (26.32%) lived with their pets, (23.32%) lived alone, and (17.22%) others. The majority of the participants (77.2%) were highly conscious about COVID-19 and (21.77%) low.
 |
Table 2 Study Participant’s Background Information |
Multivariate Analysis
Assessment of the Model Measurement
Internal consistency reliability, convergent validity, and discriminant validity were analyzed to investigate the model fit (see Table 3). The internal consistency of the measures was assessed using composite reliability (CR) and Cronbach’s alpha (CA). It varied from (0.823 to 0.966) and (0.876 to 0.975), above the 0.70 cut off in both cases.37 The average variance extracted (AVE) and the factor loadings (FA) of all the items were used to determine convergent validity. Because all of the items loaded greater than 0.6 and the AVE for all of the constructs exceeded the 0.5 limits, convergent validity was proven.37 Table 3 and Figure 2 show all of the statistics mentioned above.
 |
Table 3 Construct Validity and Reliability |
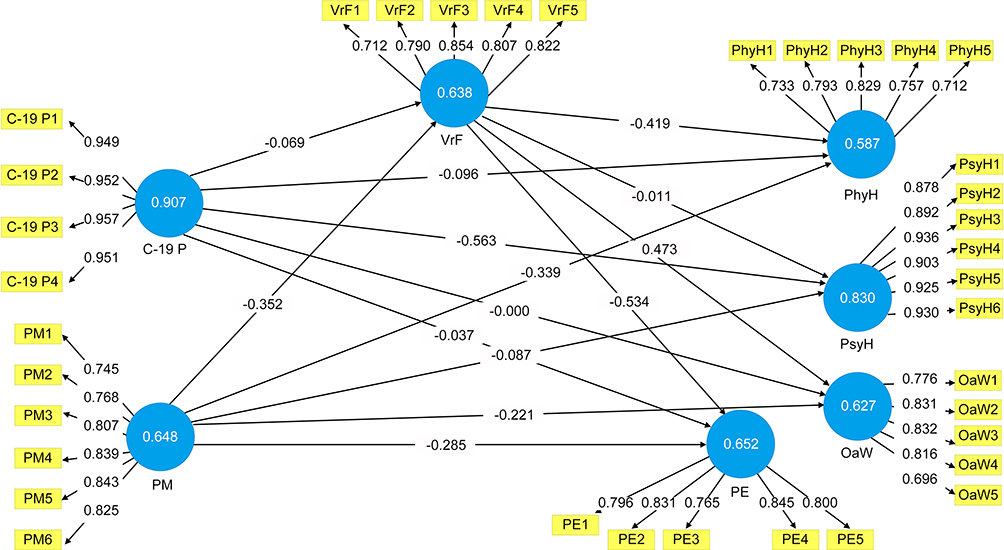 |
Figure 2 Factor loadings, path coefficient, and R-square result (PLS-Algorithm). |
Discriminant Validity
Discriminant validity is established using the Fornell Larcker and Hetro Trait-Mono Trait (HTMT) procedures. Fornell Larcker is the first requirement for discriminant validity to be verified. According to this strategy, the square root of the AVE of one construct must be bigger than the inter-correlations between constructs. A construct must show greater variability between its constituents than the other research constructs. As seen in Table 4, the square roots of all structures’ AVEs are bigger than their corresponding inter-correlations values. Henseler et al38 presented the Heterotrait-Monotrait Ratio (HTMT) approach to confirm discriminant validity between each pair of variables in terms of discriminant validity. The HTMT values are below the 0.90 criterion, as shown in Table 5.
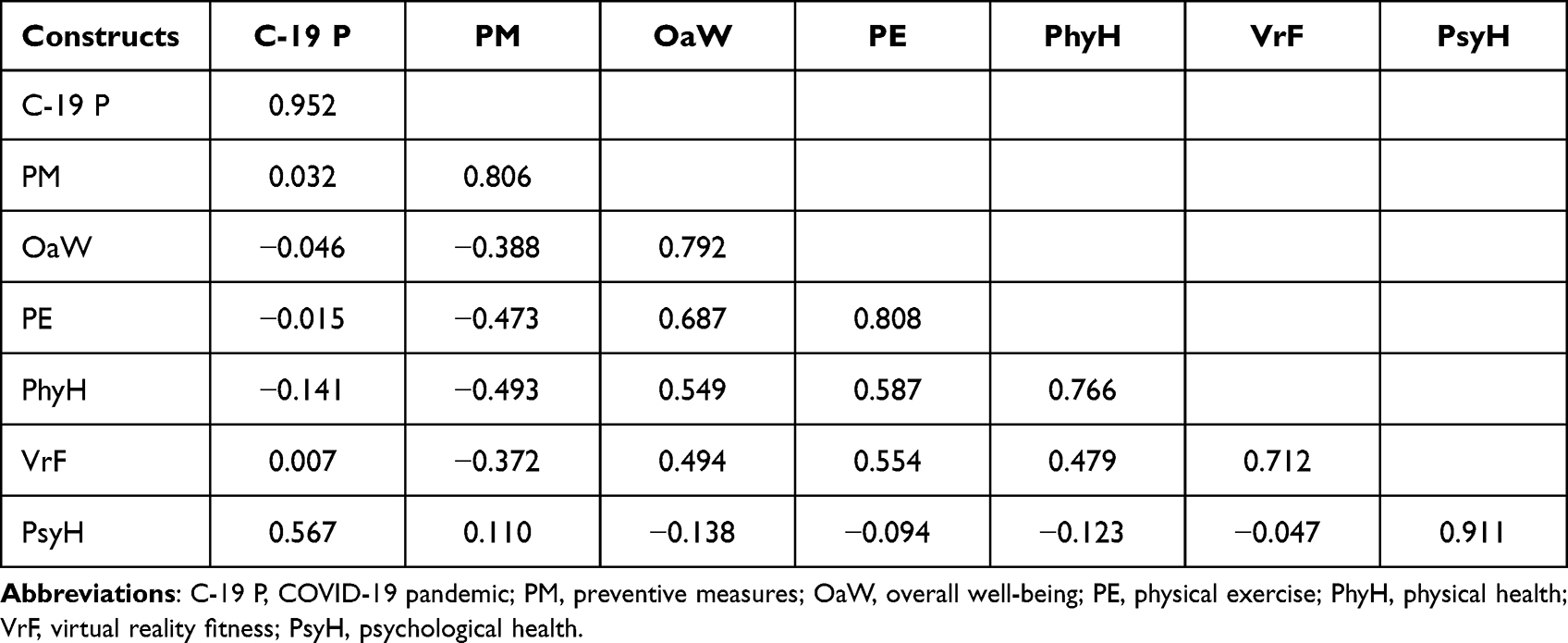 |
Table 4 Discriminant Validity: Fornell Larcker |
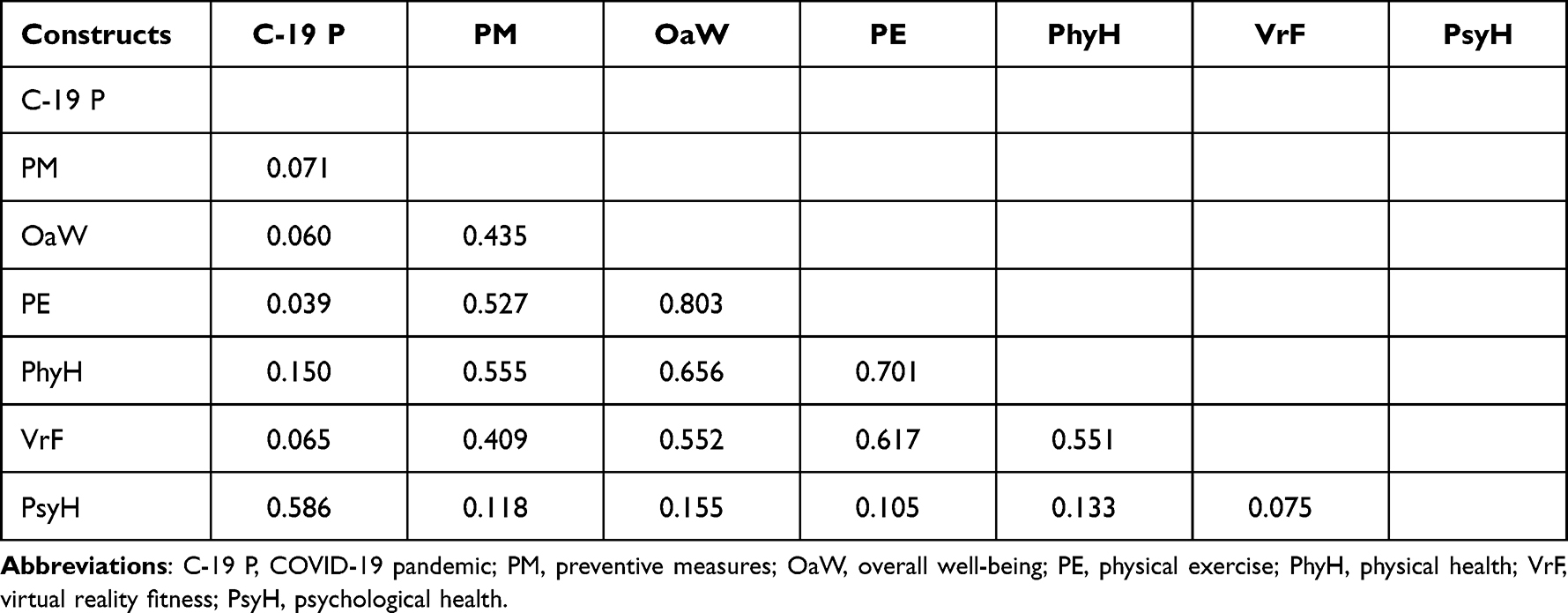 |
Table 5 Discriminant Validity (HTMT) |
Structural Model Assessment
The structural model is a theoretical model that evaluates the inner path model using a set of structural equations.39 The structural model was evaluated using the following criteria: endogenous variable coefficient of determination (R2), path coefficient (β), prediction relevance (q2), multicollinearity (inner VIF), and effect magnitude (f2).40,41 Table 6 of the structural model below shows each benchmark’s threshold value and description. All of the direct hypotheses were supported, except the path C-19 P->PE, which was not supported since the p-value was larger (0.623) than 0.05 (see Table 7). Significant associations like C-19 P -> OaW, C-19 P -> PhyH, PM -> OaW, PM -> PE, and PM -> PhyH have a negative direction, whereas C-19 P -> PsyH and PM -> PsyH have a positive direction. Table 7 and Figure 2 show the entire set of correlations. Furthermore, with t-values larger than 1.96 and p-values less than 0.05, the mediating role of VrF was revealed to be statistically significant in the mediating routes of PM -> VrF -> OaW, PM -> VrF -> PE, and PM -> VrF -> PhyH. The lower and higher ranges of the confidence intervals for those relationships have negative values (ie, “0” is not in between), indicating that the moderating effect is present. Furthermore, any significant mediating roles are only partial since their direct links are critical. Additional five mediating routes, such as C-19 P -> VrF -> OaW, C-19 P -> VrF -> PE, C-19 P -> VrF -> PhyH, C-19 P -> VrF -> PsyH, and PM -> VrF -> PsyH, found no significant mediating since their p-values were greater than 0.05 and there was a “0” between the lowest and the highest. Table 8 and Figure 3 show the statistics mentioned above.
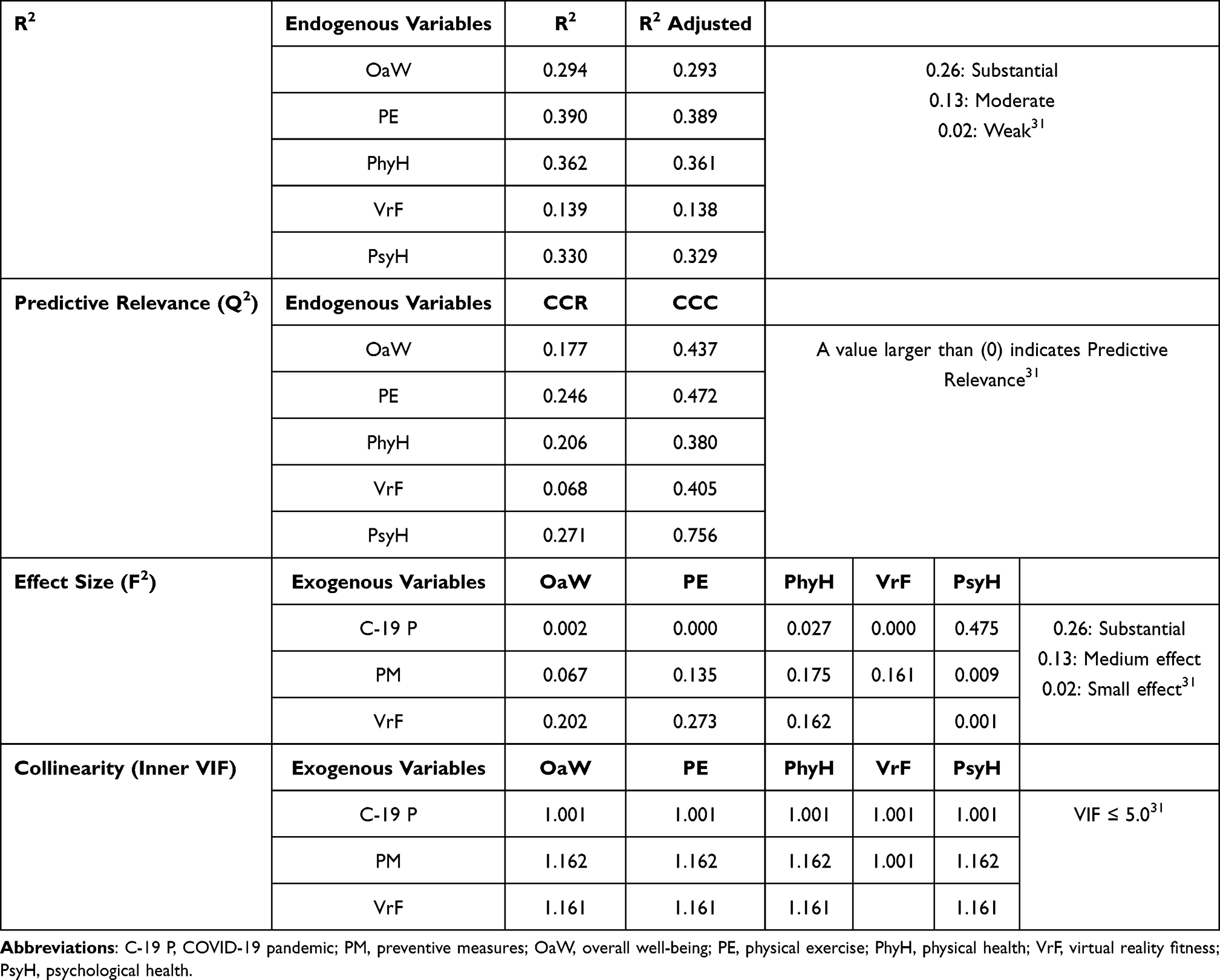 |
Table 6 Assessment of Structural Model |
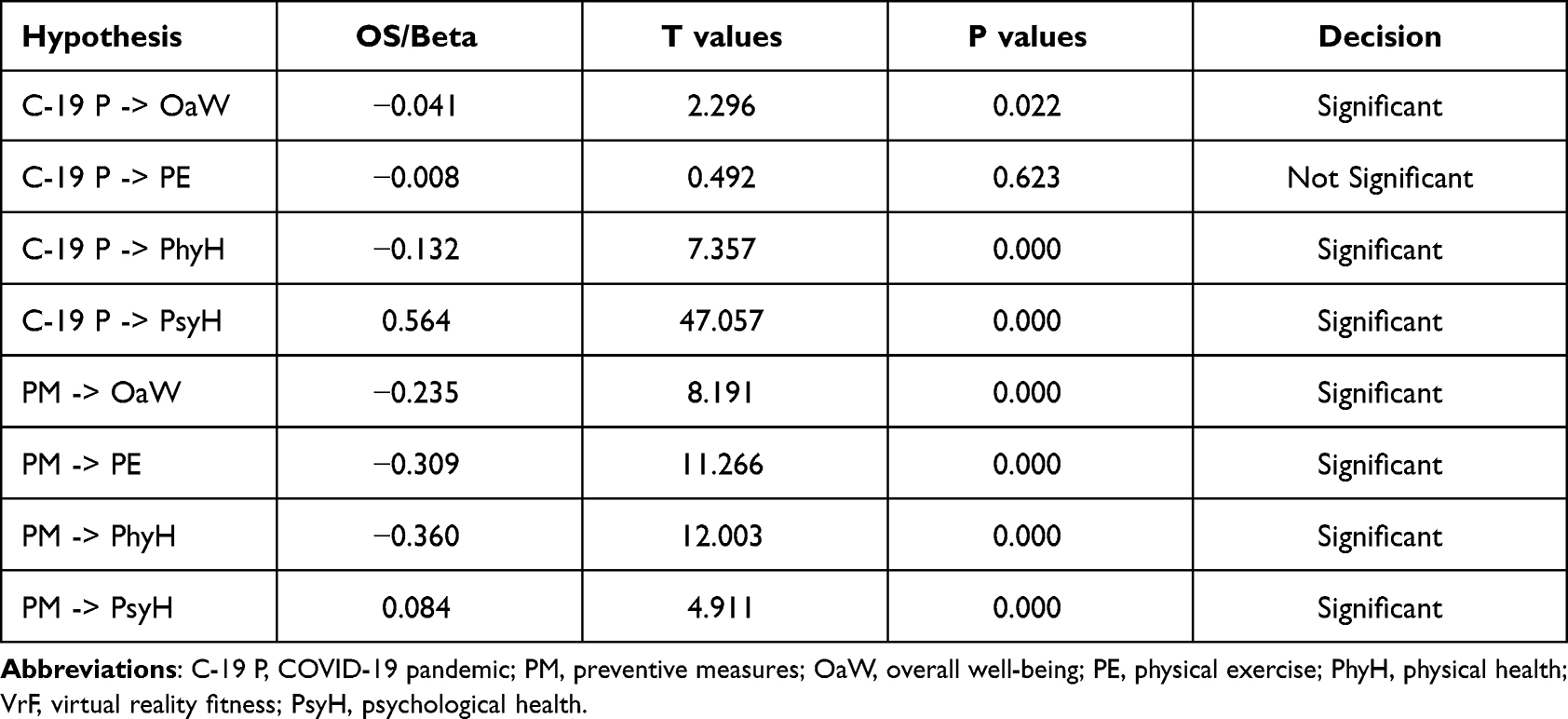 |
Table 7 Path Coefficient (Direct Effect) Result |
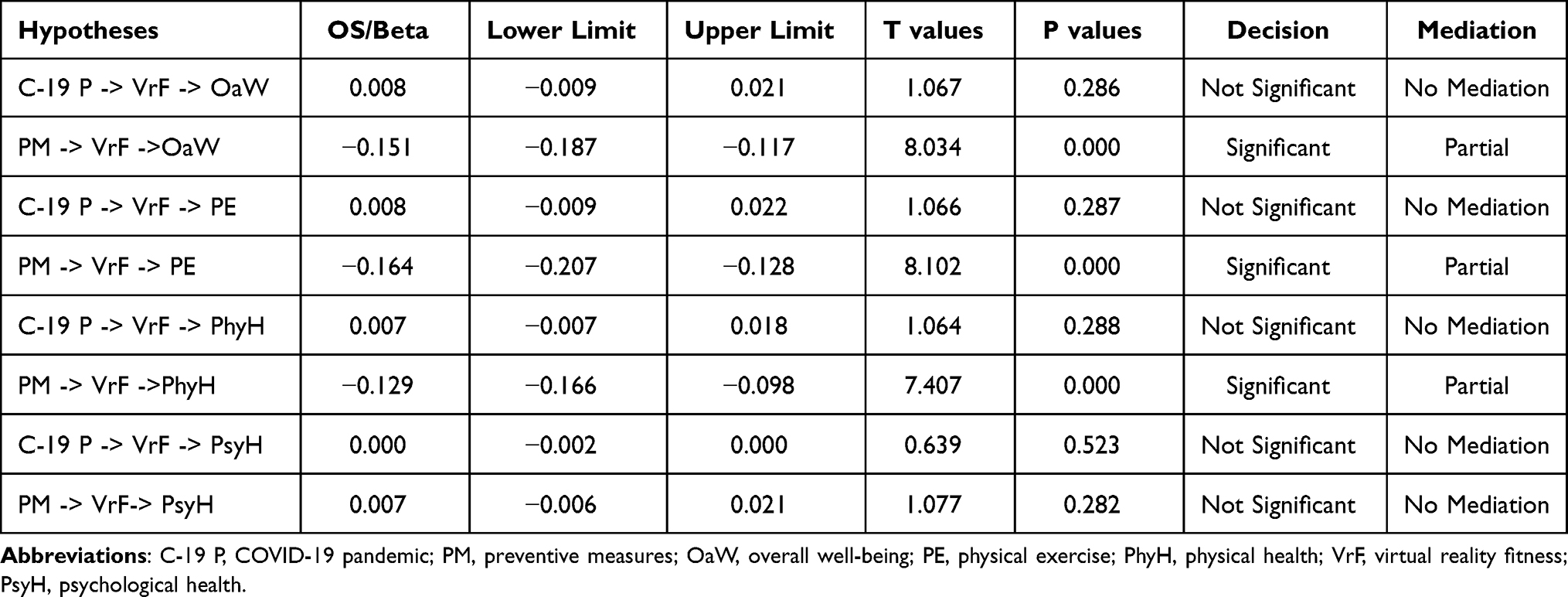 |
Table 8 Mediation (Indirect Effect) Result |
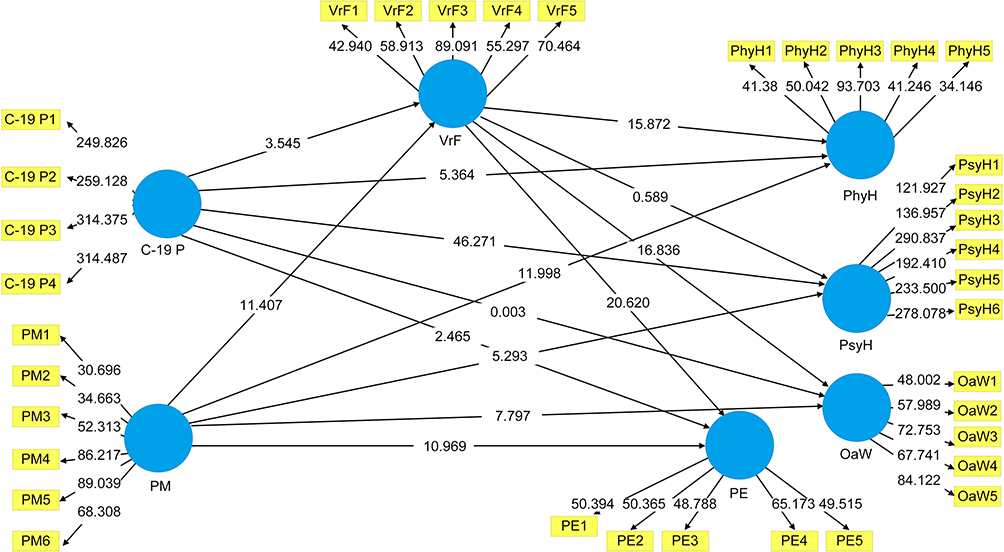 |
Figure 3 Bootstrapping results with inner model t-values. |
Discussion
Virtual reality has been utilized in combination with treatment and cognitive-behavioral psychotherapy to cure disorders. Virtual reality is utilized to simulate a situation in which addictive behavior is very likely to happen, allowing the therapist to see the client’s actions and reactions.42
The direct path coefficient analysis of the study shows that VrF has (PM -> VrF -> OaW, PM -> VrF -> PE, and PM -> VrF -> PhyH) profound effects on the research participants’ mental and physical wellbeing while indirect mediation analysis shows that VrF has (PM -> VrF ->OaW, PM -> VrF -> PE, PM -> VrF ->PhyH) significant impacts. Post-traumatic stress disorder (PTSD) might be treated using virtual reality. The patient is exposed to the source of their illness, such as war, using VR technology. The therapy approach is founded on the premise that by exposing the patient to the cause of their problem and teaching them relaxation skills, the patient will adapt to the stress. Furthermore, as individuals get more exposed to it, the threat level diminishes, reducing their dread. The patient’s anxiety caused by their ailment is expected to lessen over time.43 The psychological toll of the epidemic has been said to be rather substantial.44 Anglophobia, chronic anxiety, claustrophobia, trypanophobia, oneirophobia, and driving phobia have all been proven to benefit from it. Virtual reality has also aided cognitive recovery. It’s most often utilized to assist toddlers and adults in developing autonomous learning skills such as crossing the street and identifying distinct facial expressions in psychotic patients (this same incorporation of VR into delusional systems is a possibility),45 picking up visual cues, and paying attention to another person while they speak.46
In the therapy of schizophrenia individuals, symptom assessment, creating symptomatic connections, identifying predictor variables, creating causal factors, identifying distinct predictors, and determining environment predictors have all been employed. According to scientists, it could lead to rapid advances in our knowledge of paranoia.47 Preventive measures related constructs of the study (C-19 P -> OaW, C-19 P -> PhyH, PM -> OaW, and PM -> PE) shows significant associations. These results were further confirmed by various studies conducted on the same aspects. Isolation at home has negative socio-psychological consequences for physical and mental health. Isolation generates unpleasant emotions, cognitive deterioration, and uneasiness.48 Travel and outdoor leisure restrictions would gradually affect the everyday routines and lives of Chinese citizens. Individuals have become less active, sedentary, and depressed, all of which may put their health in danger.49
According to research, exercise enhances sensory and motor capabilities, strength, balance coordination, response speed, and activity levels. It aids not only the physiological but also the mental components. It improves learning and memory and helps those with chronic conditions overcome depression. Most of its applications are for people with various physical and mental illnesses, but it may also promote good health. It can improve the life quality and aid in the battle against aging. Virtual reality-based games have been utilized for fitness and therapeutic reasons worldwide over the past decade, with favorable results.50 Workout gaming enhances sensory and motor capabilities, strength, balance coordination, response speed, and activity levels.51 The mediation analysis of the study constructs related to virtual reality fitness for overall Well-being (PM -> VrF ->OaW) shows the significant positive impacts during the preventive measures of the pandemic. Fitness games based on virtual reality are entertaining and inspiring, but they also provide information that specifically states how they do and help them set appropriate objectives. Diabetic, strokes, Psoriatic arthritis, spinal injury, brain injury, sclerosis, cerebral palsy, and aging have all been shown to benefit from VR-based games in treating and curing physical and mental symptoms.52 Physical and emotional wellbeing is a critical aspect of our life. Healthcare professionals work relentlessly to improve the health and quality of life of their patients. Virtual reality is a technological evolution with the capability to be applied in healthcare. It is the interaction of humans with computers in a practical and realistic environment. In a virtual world, it delivers sensorimotor and cognitive exercises. Virtual reality has been employed in various medical sectors, but rehabilitation science is the most recent user of this technology.53 VrF exercise has recently been discovered as a unique tool for boosting physical exercise and healthy habits.54 In population health, it is now used more frequently. Interactive virtual exercise has been demonstrated to improve the psychological impacts of fitness while also increasing the likelihood of protracted exercise compliance.55,56 Mental health issues are a significant concern for society, healthcare practitioners, and healthcare systems, and the current COVID-19 epidemic has only exacerbated these pre-existing difficulties.57
Chinese individuals’ lack of physical activity and sedentary sitting time rose during home confinement. Sitting for long periods has also been shown to negatively influence one’s wellbeing and quality of life.58 The benefits of physical exercise on personal health are well reported in different years.59–61 Technology has been ingrained in our society, and it has a positive and negative impact on our lives. Indeed, advancements in technology have impacted every scientific field, including physical exercise and health. These technological advances have made their way into people’s homes, workplaces, communities, and other settings, where they have proven to be immensely popular.62,63 Mediation analysis of the study constructs (PM -> VrF -> PE) shows that VrF has a positive impact on physical exercise and fitness during the preventive measures of the pandemic. Patients undergoing physical rehabilitation can improve physical fitness, muscle strength, balance, limb function, and overall quality of life using virtual reality-based interventions.64,65 As a result of the COVID-19 epidemic, people’s attention has been called to the need for physical activity. The mainstream media has emphasized the benefits of regular physical activity on general fitness and individuals with moderate coronavirus infection throughout the outbreak. Frequent and extended physical activity increases immunological surveillance, works as an anti-inflammatory agent, lowers the chance of acquiring various chronic diseases, and supports general fitness and sickness protection and reaction.66 Mobile phones, for instance, enable us to track our health and physical activity habits using a range of health-related applications and communicate with others via telephone texts and call messaging.67,68 Physical exercise frequency has a variable impact on cognitive health. During the pandemic, people who participated in more physical exercise activities reported greater mental health and Well-being.69 There are three options from a cognitive context; first, exercise can reduce anxiety sensitivity and promote mental health by improving receptivity to anxiety-related stimuli.70 Second, exercise may help you build confidence in yourself, enhance your self-image, and lift your mood, both of which can help you feel more in control of challenging situations. Third, exercise efficiently reduces anxiety by providing a diversion from stresses that allow you to enjoy regular exercise time.71
Conclusion
Many individuals use virtual reality exercising at home as a coping method to enhance psychological wellbeing during the pandemic since outside activity time has been considerably curtailed and outdoor activity space has been limited. Virtual swims, sailing, bicycling, jogging, and hiking are examples of technologically assisted human contact exercises that may help maintain and enhance overall health throughout the pandemic. The COVID-19 outbreak has significantly influenced Chinese people’s life quality, physical exercise, and mental stress levels. Our study results concluded that house exercises through virtual reality fitness are a good substitute for public gyms and private group fitness programs during the first pandemic wave for physical-psychological and overall wellbeing. Older people’s stress, attitude, interpersonal, and psychological wellbeing have improved. Exergames, or video game-based exercises, are popular among the younger population for home-based activities. Physical exercise through virtual reality fitness is well-known for improving and maintaining overall health and improving the overall quality of life.
Study Implications
The Chinese government has established a program called “Internet plus Exercise” to encourage people to live a more active lifestyle and improve their overall health. The application of virtual reality fitness for physical, psychological, and physical exercise focuses on our research. It provides insight into the Chinese masses’ technology usage trend for overall physical health and wellbeing. Furthermore, three cognitive components may be engaged in an activity from a psychological standpoint: (I) ideas about the exercise, (ii) motivation for the activity, and (iii) the sense of pleasure gained from the activity. More intriguing research in the future could focus on the impact of the Chinese government’s “Internet plus Exercise” policy on the use of digital platforms for physical activity, as well as the relationship between digital platforms and the three cognitive factors mentioned above that are linked to physical activity under the psychological framework.
Limitations of the Study
The results of the current study, which used the snowball sampling technique, cannot be applied to the entire population. The primary data was collected through a web-based survey during the first wave of the pandemic lockdown. The mediating role of VRF was assessed with physical exercise, physical health, psychological health, and overall wellbeing. The age group of 41+ means active elderly population who used VRF for overall wellbeing.
Acknowledgment
We thank the participants for participating in this research and making this study possible. Rashid Menhas is the principal investigator.
Funding
Hunan Province Educational Science Planning Project (XJK22ZDJD52)
Disclosure
The authors report no conflicts of interest in this work.
References
1. IDC. Worldwide spending on augmented and virtual reality forecast to deliver strong growth through 2024, According to a new IDC spending guide. Available from: https://www.idc.com/getdoc.jsp?containerId=prUS47012020.
2. Ahn SJ, Fox J. Immersive virtual environments, avatars, and agents for health. Oxford Res Encycl Commun. 2017. doi:10.1093/acrefore/9780190228613.013.325
3. Mestre DR, Dagonneau V, Mercier C-S. Does virtual reality enhance exercise performance, enjoyment, and dissociation? An exploratory study on a stationary bike apparatus. Presence: Teleoperators Virtual Environ. 2011;20(1):1–14. doi:10.1162/pres_a_00031
4. Karasu AU, Batur EB, Karataş GK. Effectiveness of Wii-based rehabilitation in stroke: A randomized controlled study. J Rehabil Med. 2018;50(5):406-412. doi:10.2340/16501977-2331.
5. Khushnood K, Sultan N, Awan MMA. Virtual reality: a source to improve physical and mental wellbeing. J Coll Physicians Surg Pak. 2020;30(9):999. doi:10.29271/jcpsp.2020.09.999
6. Chirico A, Lucidi F, Galli F, et al. COVID-19 outbreak and physical activity in the Italian population: a cross-sectional analysis of the underlying psychosocial mechanisms. Front Psychol. 2020;11:2100. doi:10.3389/fpsyg.2020.02100
7. Codella R, Chirico A, Lucidi F, et al. The immune-modulatory effects of exercise should be favorably harnessed against COVID-19. J Endocrinol Invest. 2021;44:1119–1122. doi:10.1007/s40618-020-01403-5
8. Fleming TM, Bavin L, Stasiak K, et al. Serious games and gamification for mental health: current status and promising directions. Front Psy. 2017;7. doi:10.3389/fpsyt.2016.00215
9. Thornton M, Marshall S, McComas J, Finestone H, McCormick A, Sveistrup H. Benefits of activity and virtual reality based balance exercise programmes for adults with traumatic brain injury: perceptions of participants and their caregivers. Brain Injury. 2005;19(12):989–1000. doi:10.1080/02699050500109944
10. Gao Z, Zeng N, Pope ZC, Wang R, Yu F. Effects of exergaming on motor skill competence, perceived competence, and physical activity in preschool children. J Sport Health Sci. 2019;8(2):106–113. doi:10.1016/j.jshs.2018.12.001
11. Pasco D. The potential of using virtual reality technology in physical activity settings. Quest. 2013;65(4):429–441. doi:10.1080/00336297.2013.795906
12. Shephard RJ, Bouchard C. Population evaluations of health related fitness from perceptions of physical activity and fitness. Canad J Appl Physiol. 1994;19(2):151–173. doi:10.1139/h94-012
13. Blascovich J. Immersive virtual environment technology as a tool in psychological science. PsycEXTRA Dataset. 2001. doi:10.1037/e324232004-012
14. Riener R, Harders M. Introduction to virtual reality in medicine. Virtual Reality Med. 2012;1–12. doi:10.1007/978-1-4471-4011-5_1
15. Kirner C, Shneider C, Goncalves T. Using augmented reality cognitive artifacts in education and virtual rehabilitation. Virtual Reality Psychol, Med Pedagog Appl. 2012. doi:10.5772/46416
16. Altan Akin NT, Gokturk M. Comparison of the theory of mind tests on the paper, 2D touch screen and augmented reality environments on the students with neurodevelopmental disorders. IEEE Access. 2019;7:52390–52404. doi:10.1109/access.2019.2902836
17. Akter T, Zeba Z, Hosen I, et al. Impact of the COVID-19 pandemic on BMI: its changes in relation to socio-demographic and physical activity patterns based on a short period. PLoS One. 2022;17(3):e0266024. doi:10.1371/journal.pone.0266024
18. Hosen I, Al-Mamun F, Mamun MA. Prevalence and risk factors of the symptoms of depression, anxiety, and stress during the COVID-19 pandemic in Bangladesh: a systematic review and meta-analysis. Glob Ment Health. 2021;8:e47. doi:10.1017/gmh.2021.49
19. Al Mamun F, Gozal D, Hosen I, et al. Predictive factors of insomnia during the COVID-19 pandemic in Bangladesh: a GIS-based nationwide distribution. Sleep Med. 2022;91:219–225. doi:10.1016/j.sleep.2021.04.025
20. Erkkmen G, Asci FH. Relationships among perceived body appearance, social physique anxiety, physical self-concept, and dispositional flow state of exercise participants. Turkish J Sport Exercise. 2016;18(1):38. doi:10.15314/tjse.77952
21. Sullivan AN, Lachman ME. Behavior change with fitness technology in sedentary adults: a review of the evidence for increasing physical activity. Front Public Health. 2017;4. doi:10.3389/fpubh.2016.00289
22. Vieira GD, Araujo DF, Leite MA, Orsini M, Correa CL. Realidade virtual na reabilitação física de pacientes com doença de parkinson. J Human Growth Develop. 2014;24(1):31. doi:10.7322/jhgd.72046
23. Imam B, Jarus T. Virtual reality rehabilitation from social cognitive and motor learning theoretical perspectives in stroke population. Rehabil Res Pract. 2014;2014:1–11. doi:10.1155/2014/594540
24. Juras G, Brachman A, Michalska J, et al. Standards of virtual reality application in balance training programs in clinical practice: a systematic review. Games Health J. 2019;8(2):101–111. doi:10.1089/g4h.2018.0034
25. Qi M, Li P, Moyle W, Weeks B, Jones C. Physical activity, health-related quality of life, and stress among the Chinese adult population during the COVID-19 pandemic. Int J Environ Res Public Health. 2020;17(18):6494. doi:10.3390/ijerph17186494
26. Rubin GJ, Potts HWW, Michie S. The impact of communications about swine flu (Influenza a h1n1v) on public responses to the outbreak: results from 36 national telephone surveys in the UK. Health Technol Assess. 2010;14(34). doi:10.3310/hta14340-03
27. Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395(10227):912–920. doi:10.1016/s0140-6736(20)30460-8
28. Salari N, Hosseinian-Far A, Jalali R, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Global Health. 2020;16(1). doi:10.1186/s12992-020-00589-w
29. Moreira-Neto A, Martins B, Miliatto A, Nucci MP, Silva-Batista C. Can remotely supervised exercise positively affect self-reported depressive symptoms and physical activity levels during social distancing? Psychiatry Res. 2021;301:113969. doi:10.1016/j.psychres.2021.113969
30. Carvalho Aguiar Melo M, de Sousa Soares D. Impact of social distancing on mental health during the COVID-19 pandemic: an urgent discussion. Int J Soc Psy. 2020;66(6):625–626. doi:10.1177/0020764020927047
31. Reese G, Stahlberg J, Menzel C. Digital Shinrin-Yoku: do nature experiences in virtual reality reduce stress and increase wellbeing as strongly as similar experiences in a physical forest? Virtual Real. 2022. doi:10.1007/s10055-022-00631-9
32. Tariq H. Effect of balance exercises for person with multiple sclerosis using Wii®Game: a systematic review of randomized and non-randomized control trials. Acta Medica Int. 2016;3(1):196. doi:10.5530/ami.2016.1.39
33. Cheek C, Fleming T, Lucassen MFG, et al. Integrating health behavior theory and design elements in serious games. JMIR Mental Health. 2020. doi:10.26686/wgtn.12331295
34. Ringle CM, Da Silva D, Bido DD. Modelagem de Equações Estruturais com utilização do Smartpls. Rev Bras Gest Neg. 2014;13(2):56–73. doi:10.5585/remark.v13i2.2717
35. Anderson J, Gerbing D. Assumptions and comparative strengths of the two-step approach. Sociol Methods Res. 1992;20(3):321–333. doi:10.1177/0049124192020003002
36. Hair JF, Hult GT, Ringle CM, Sarstedt M, Thiele KO. Mirror, mirror on the wall: a comparative evaluation of composite-based structural equation modeling methods. J Acad Marketing Sci. 2017;45(5):616–632. doi:10.1007/s11747-017-0517-x
37. Henseler J, Hubona G, Ray PA. Partial least squares path modeling: updated guidelines. Partial Least Squares Path Modeling. 2017;19–39. doi:10.1007/978-3-319-64069-3_2
38. Chin WW. Bootstrap cross-validation indices for PLS path model assessment. Handbook of Partial Least Squares. 2009;83–97. doi:10.1007/978-3-540-32827-8_4
39. Tenenhaus M, Vinzi VE, Chatelin Y-M, Lauro C. PLS path modeling. Comput Stat Data Anal. 2005;48(1):159–205. doi:10.1016/j.csda.2004.03.005
40. Götz O, Liehr-Gobbers K, Krafft M. Evaluation of structural equation models using the partial least squares (PLS) approach. Handbook of Partial Least Squares. 2009;691–711. doi:10.1007/978-3-540-32827-8_30
41. Kock N. Common method bias in PLS-SEM: a full collinearity assessment approach. Int J e-Collab. 2015;11(4):1. doi:10.4018/ijec.2015100101
42. Riva G. Applications of virtual environments in medicine. Methods Inf Med. 2003;42(05):524–534. doi:10.1055/s-0038-1634379
43. Aldhous P. Schizophrenia explored with virtual reality. New Scientist. 2008;197(2640):30. doi:10.1016/s0262-4079(08)60230-4
44. Al Mamun F, Hosen I, Misti JM, Kaggwa MM, Mamun MA. Mental disorders of Bangladeshi students during the COVID-19 pandemic: a systematic review. Psychol Res Behav Manag. 2021;14:645–654. doi:10.2147/PRBM.S315961
45. Rubio-Tamayo J, Gertrudix Barrio M, García F. Immersive environments and virtual reality: systematic review and advances in communication, interaction and simulation. Multimodal Technol Interact. 2017;1(4):21. doi:10.3390/mti1040021
46. Slater M, Sanchez-Vives MV. Is consciousness first in virtual reality? Front Psychol. 2022;13. doi:10.3389/fpsyg.2022.787523
47. Freeman D, Antley A, Ehlers A, et al. The use of immersive virtual reality (VR) to predict the occurrence 6 months later of paranoid thinking and posttraumatic stress symptoms assessed by self-report and interviewer methods: a study of individuals who have been physically assaulted. Psychol Assess. 2014;26(3):841–847. doi:10.1037/a0036240
48. Hawkley LC, Capitanio JP. Perceived social isolation, evolutionary fitness and health outcomes: a lifespan approach. Philos Trans R Soc Lond, B, Biol Sci. 2015;370(1669):20140114. doi:10.1098/rstb.2014.0114
49. Chen P, Mao L, Nassis GP, Harmer P, Ainsworth BE, Li F. Coronavirus disease (covid-19): the need to maintain regular physical activity while taking precautions. J Sport Health Sci. 2020;9(2):103–104. doi:10.1016/j.jshs.2020.02.001
50. Lau HM, Smit JH, Fleming TM, Riper H. Serious games for mental health: are they accessible, feasible, and effective? A systematic review and meta-analysis. Front Psy. 2017;7. doi:10.3389/fpsyt.2016.00209
51. O’Neil J, Egan M, Marshall S, Bilodeau M, Pelletier L, Sveistrup H. Remotely supervised home-based intensive exercise intervention to improve balance, functional mobility, and physical activity in survivors of moderate or severe traumatic brain injury: protocol for a mixed methods study. JMIR Res Protoc. 2019;8(10). doi:10.2196/14867
52. Lynch C, Bird S, Lythgo N, Selva-Raj I. Changing the physical activity behavior of adults with fitness trackers: a systematic review and meta-analysis. Am J Health Prom. 2019;34(4):418–430. doi:10.1177/0890117119895204
53. McClure C, Schofield D. Running virtual: the effect of virtual reality on exercise. J Human Sport Exercise. 2019;15(4). doi:10.14198/jhse.2020.154.13
54. Ndayizigamiye P, Kante M, Shingwenyana S. An adoption model of mHealth applications that promote physical activity. Cogent Psychol. 2020;7(1):1764703. doi:10.1080/23311908.2020.1764703
55. Qian J, McDonough DJ, Gao Z. The effectiveness of virtual reality exercise on individual’s physiological, psychological and rehabilitative outcomes: a systematic review. Int J Environ Res Public Health. 2020;17(11):4133. doi:10.3390/ijerph17114133
56. McAnally K, Wallis G. Visual–haptic integration, action and embodiment in virtual reality. Psychol Res. 2021. doi:10.1007/s00426-021-01613-3
57. Thomas L. Covid-19 pandemic has worsened pre-existing mental health conditions. News; 2020. Available from: https://www.news-medical.net/news/20200601/COVID-19-pandemic-has-worsened-pre-existing-mental-health-conditions.aspx.
58. Zhang Y, Ma ZF. Impact of the COVID-19 pandemic on Mental health and quality of life among local residents in Liaoning Province, China: a cross-sectional study. Int J Environ Res Public Health. 2020;17(7):2381. doi:10.3390/ijerph17072381
59. Plante TG, Aldridge A, Bogden R, Hanelin C. Might virtual reality promote the mood benefits of exercise? Comput Human Behav. 2003;19(4):495–509. doi:10.1016/s0747-5632(02)00074-2
60. Chou C-H, Hwang C-L, Wu Y-T. Effect of exercise on physical function, daily living activities, and quality of life in the frail older adults: a meta-analysis. Arch Phys Med Rehabil. 2012;93(2):237–244. doi:10.1016/j.apmr.2011.08.042
61. Byrne A, Byrne DG. The effect of exercise on depression, anxiety and other mood states: a review. J Psychosom Res. 1993;37(6):565–574. doi:10.1016/0022-3999(93)90050-P
62. Dong X, Yi X, Gao D, et al. The effects of the combined exercise intervention based on internet and Social Media Software (CEIBISMS) on quality of life, Muscle Strength and cardiorespiratory capacity in Chinese postoperative breast cancer patients: a randomized controlled trial. Health Qual Life Outcomes. 2019;17(1). doi:10.1186/s12955-019-1183-0
63. Pope Z, Barr-Anderson D, Lewis B, Pereira M, Gao Z. Use of wearable technology and social media to improve physical activity and dietary behaviors among college students: a 12-week randomized pilot study. Int J Environ Res Public Health. 2019;16(19):3579. doi:10.3390/ijerph16193579
64. Sañudo B, Abdi E, Bernardo-Filho M, Taiar R. Aerobic exercise with superimposed virtual reality improves cognitive flexibility and selective attention in young males. Appl Sci. 2020;10(22):8029. doi:10.3390/app10228029
65. Weber H, Barr C, Gough C, van den Berg M. How commercially available virtual reality–based interventions are delivered and reported in gait, posture, and balance rehabilitation: a systematic review. Phys Ther. 2020;100(10):1805–1815. doi:10.1093/ptj/pzaa123
66. Shephard RJ. Aging, physical activity and health. Int Encycl Public Health. 2008;61–69. doi:10.1016/b978-012373960-5.00627-4
67. Bort-Roig J, Gilson ND, Puig-Ribera A, Contreras RS, Trost SG. Measuring and influencing physical activity with smartphone technology: a systematic review. Sports Med. 2014;44(5):671–686. doi:10.1007/s40279-014-0142-5
68. Gao G, Lee L. Emerging technology in promoting physical activity and Health: challenges and opportunities. J Clin Med. 2019;8(11):1830. doi:10.3390/jcm8111830
69. Faulkner G, Rhodes RE, Vanderloo LM, et al. Physical activity as a coping strategy for mental health due to the COVID-19 virus: a potential disconnect among Canadian adults? Front Commun. 2020;5. doi:10.3389/fcomm.2020.571833
70. Ai X, Yang J, Lin Z, Wan X. Mental health and the role of physical activity during the COVID-19 pandemic. Front Psychol. 2021;12:759987. doi:10.3389/fpsyg.2021.759987
71. Hale BS, Raglin JS. State anxiety responses to acute resistance training and step aerobic exercise across eight weeks of training. J Sports Med Phys Fitness. 2002;42(1):108–112.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Behavioural Response To Self-Medication Practice Before and During Covid-19 Pandemic in Western Uganda
Dare SS, Eze ED, Echoru I, Usman IM, Ssempijja F, Bukenya EE, Ssebuufu R
Patient Preference and Adherence 2022, 16:2247-2257
Published Date: 20 August 2022
Resilience and Depressive Symptoms Mediated Pathways from Social Support to Suicidal Ideation Among Undergraduates During the COVID-19 Campus Lockdown in China
Zhang X, Liu X, Mi Y, Wang W, Xu H
Psychology Research and Behavior Management 2022, 15:2291-2301
Published Date: 23 August 2022
Lower Back Pain Caused by the Impact of COVID-19 Quarantine on Physical Activity and Daily Sitting Among Adult Saudi Arabian Populations in Jeddah: A Cross-Sectional Study
Abumunaser LA, Alfaraj KA, Kamal LK, Alzahrani RA, Alzahrani MM, AlAhmed AB
Orthopedic Research and Reviews 2022, 14:477-485
Published Date: 13 December 2022
How Interpersonal Sensitivity Affects Depression Under the COVID-19 Lockdown Among College Students in South China: A Moderated Mediation Model
Zhang Y, Sun Q
Psychology Research and Behavior Management 2023, 16:1271-1282
Published Date: 18 April 2023
Prevalence of Obesity and Lifestyle Risk Factors Following Two Years’ COVID-19 Related Service Closure at Wellness Center, Primary Health Care
Musa S, Al-Dahshan A, Singh R
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3851-3868
Published Date: 29 November 2023