")
Back to Journals » Orthopedic Research and Reviews » Volume 14
Lower Back Pain Caused by the Impact of COVID-19 Quarantine on Physical Activity and Daily Sitting Among Adult Saudi Arabian Populations in Jeddah: A Cross-Sectional Study
Authors Abumunaser LA , Alfaraj KA, Kamal LK , Alzahrani RA, Alzahrani MM , AlAhmed AB
Received 20 August 2022
Accepted for publication 3 December 2022
Published 13 December 2022 Volume 2022:14 Pages 477—485
DOI https://doi.org/10.2147/ORR.S386995
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Clark Hung
Lutf Ahmed Abumunaser,1 Kawther Ali Alfaraj,2 Lujain Khalid Kamal,2 Renad Abdullah Alzahrani,2 Maram Misfer Alzahrani,2 Alzahraa Bader AlAhmed2
1Department of Orthopedic Surgery, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 2College of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Maram Misfer Alzahrani, Tel +966 537363683, Email [email protected]
Purpose: During the COVID-19 quarantine period, most outdoor activities and events were banned, resulting in a decrease in physical activity (PA) and prolonged sitting (PS) time, which are significant factors in the development of lower back pain (LBP). The aim of this study was to evaluate the association between physical inactivity and daily sitting time during quarantine with LBP among the Saudi Arabian population.
Patients and Methods: In this cross-sectional study conducted at King Abdulaziz University Hospital, 288 participants were recruited using an online, self-administered questionnaire in Arabic. It consisted of 21 questions assessing back pain, PA, and daily sitting time before and during quarantine. The main outcome measures included demographics, low back pain levels, daily sitting time, and PA level.
Results: The participants consisted of 236 women and 52 men aged 18– 65 years. During quarantine, 74% of participants sat most of the time and did not exercise or performed less exercise. Furthermore, almost half of the participants did not engage in PA both before and during the quarantine. There was an increase in the prevalence of LBP, with only 44.8% of participants presenting with LBP before quarantine and 59.4% having it during quarantine. A statistically significant association was found between daily sitting time and LBP (P=0.007) and PA and LBP (P=0.045) during quarantine. However, there was no significant association between age and painkiller use for LBP (P=0.251).
Conclusion: Our study highlights the relationship of physical inactivity and PS during quarantine with an increase in the prevalence and intensity of LBP. The limitations of the study include the use of self-reports, a small sample size, and unequal survey distribution. A well-distributed survey with a larger sample size is necessary to obtain an adequate representation of the entire Saudi population.
Keywords: painkiller, lockdown, exercise, pandemic, COVID-19
Introduction
The first outbreak of the coronavirus disease 2019 (COVID-19) was detected in a group of workers in the Wuhan animal market after they presented with respiratory symptoms and were initially diagnosed with pneumonia of an unknown origin.1 The outbreak was announced by the World Health Organization in January 2020, wherein they declared it to be a public health emergency of international concern.2 The Saudi Arabian Ministry of Health discovered the first cases of COVID-19 in March 2020 in Saudi Arabian citizens returning from Iran through Bahrain.3 Subsequently, lockdown and restrictions were imposed by public health institutions and governments owing to the outbreak,4 as well as quarantines and travel bans as an initial countermeasure against new infectious diseases.5 Owing to the lack of information about the treatment and prevention of COVID-19, in addition to its fast transmission rate, it was widely recommended for people to remain at home and maintain social distancing to limit the spread of the disease and reduce pressure on health systems worldwide.6 Moreover, most outdoor activities and social events were banned during the quarantine period, resulting in decreased physical activity (PA).7 This quarantine has inevitably influenced and heavily impacted the PA levels of individuals, particularly men and overweight individuals.8
PA is a form of skeletal muscle mobility that requires energy expenditure.9 Meanwhile, prolonged sitting (PS) is considered to be a provocative factor in the development of lower back pain (LBP).10 Furthermore, an international study revealed that daily sitting time increased from 5 to 8 h per day during quarantine.11 In fact, PS and lack of PA are often seen as risk factors for LBP.12 There has been a shortage of research regarding the pain intensity of LBP or the definition of sitting. Furthermore, most studies conducted were limited to professional workers, which may not be generalizable to the general population. Few studies were conducted to assess the impact of COVID-19 quarantine on back pain in the Saudi Arabian general population. Therefore, the aim of this study was to evaluate the association of physical inactivity and daily sitting time during the COVID-19 quarantine with LBP among Saudi Arabian population.
Material and Methods
This cross-sectional, descriptive, and analytical study was conducted at King Abdulaziz University Hospital. Ethical approval was obtained from the institutional review board of King Abdulaziz University Hospital, Jeddah, Saudi Arabia, in accordance with the Declaration of Helsinki. A total of 469 participants were recruited through online volunteer sampling using a self-administered questionnaire in Arabic for data collection. No sex restrictions were applied, and only Saudi Arabian residents in Jeddah aged 18–65 years were included in the study. Participants with any spinal deformities, malignancies, osteoporosis, back tumor or malignancies, multiple sclerosis, back fracture, back trauma, or a history of spine surgery were excluded from the study. The inclusion criteria were met by 288 participants who were immediately allowed to attempt the questionnaire. Data confidentiality was ensured, and consent was obtained at the beginning of the survey for participation and result publication. The study was conducted through social media from June 28 to July 10, 2021. The questionnaire was developed and modified based on a previous study performed in Riyadh.13 It consisted of 21 questions subdivided into three sections: (1) demographic characteristics, (2) assessment of PA and daily sitting before and during the quarantine, and (3) assessment of back pain before and during the quarantine. The variables included were: (a) sociodemographic and anthropometric data (age, sex, nationality, province, marital status, education level, occupation, total income, body mass index), (b) PA (frequency) and daily sitting and movement, and (c) back pain-related information (pain intensity, medical help-seeking, painkiller use). We hypothesize that there is significant relationship between daily sitting and low back pain, and also between physical activity and low back pain (alternate hypothesis). And we hypothesize that there is no significant relationship between age and seeking medical help or between age and using painkillers for low back pain (null hypothesis). All collected data were entered into Microsoft Excel and analyzed using IBM SPSS Statistics for Windows, version 24.0 (IBM Corp., Armonk, N.Y., USA). The analysis included univariate qualitative data, which were presented as frequency and percentage, and bivariate analysis using the chi-square test. Statistical significance was set at P<0.05.
Results
The study sample consisted of 288 participants divided according to sociodemographic characteristics, including age, sex, marital status, educational level, occupations, total income level, and body mass index (Table 1).
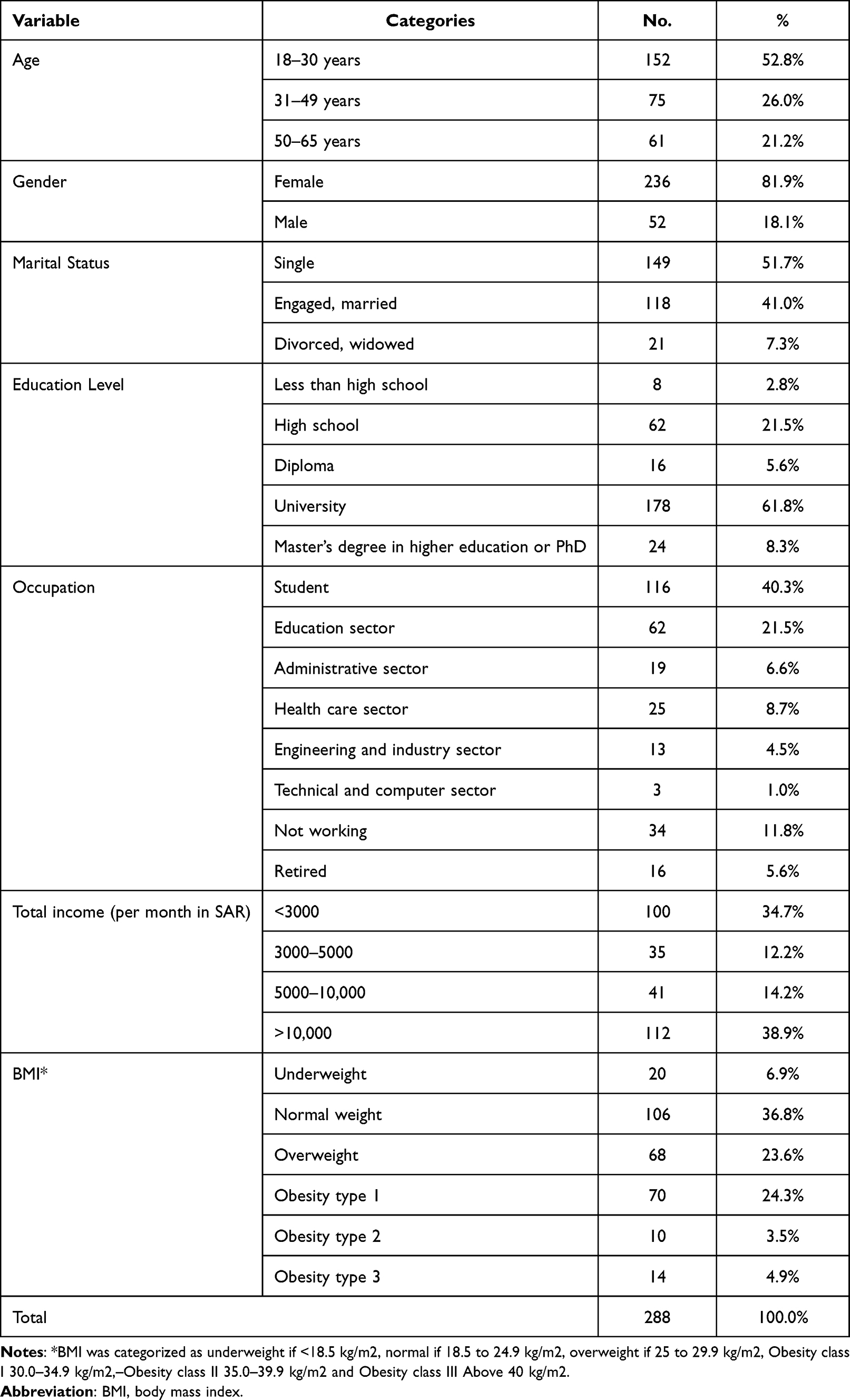 |
Table 1 Sociodemographic Characteristics of the Participants |
Furthermore, the proportion of participants who were always or most of the time sitting during the quarantine (74%) was higher than that before the quarantine (33%) (Figure 1).
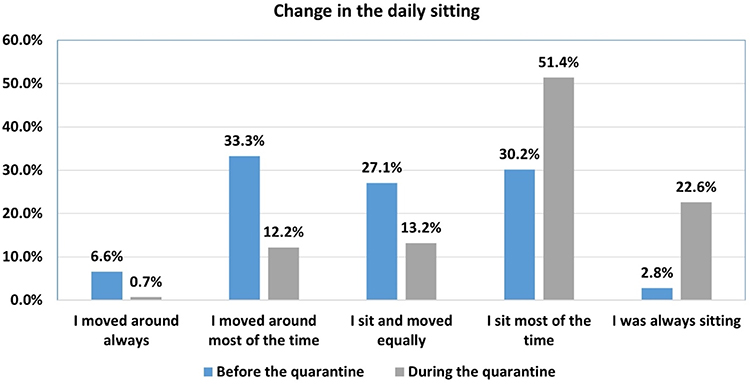 |
Figure 1 Changes in daily sitting before and during the quarantine. |
Regarding the change in PA before and during quarantine, the number of participants who either had no PA or only performed exercise once a week was noted to be similar both before and during quarantine (69.4%) (Figure 2).
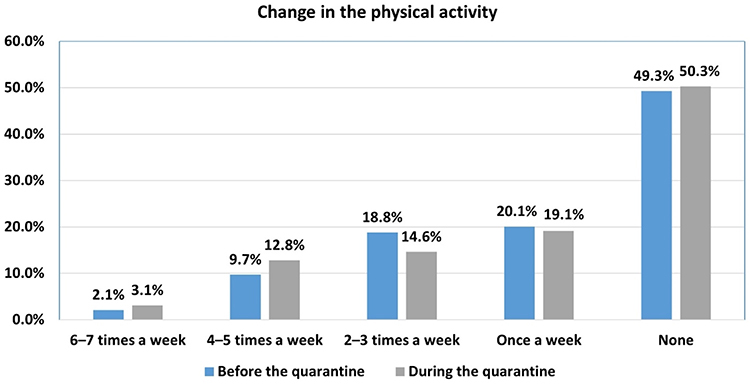 |
Figure 2 Changes in physical activities before and during the quarantine. |
With regard to the change in LBP before and during quarantine, 59.4% of the participants had LBP during quarantine compared to only 44.8% before the quarantine. Similar numbers of participants had mild LBP before and during quarantine (31.9%). Among the participants, 21.9% had moderate LBP during quarantine compared with 10.4% before the quarantine. Furthermore, only 2.4% of the participants had severe LBP before quarantine compared to 5.6% during quarantine. Thus, only 12.8% of the participants presented with moderate-to-severe back pain before quarantine, while there were 27.5% with it during quarantine (Figure 3).
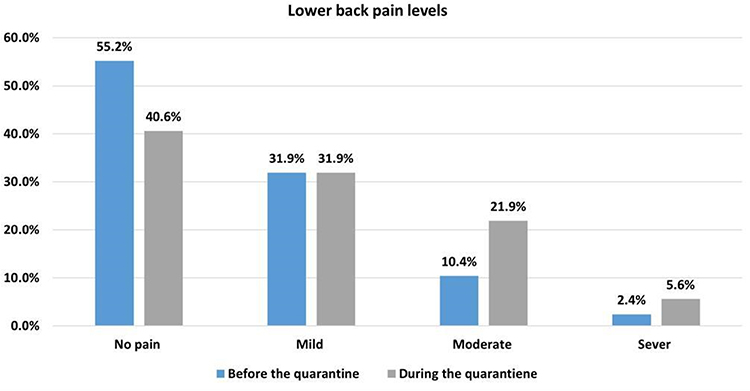 |
Figure 3 Lower back pain (LBP) levels before and during the quarantine. |
The results of the cross-tabulation and chi-square tests for independence for the relationship between daily sitting and LBP during quarantine showed that the test value was (27.7), and the P-value was 0.007, which is less than the significance level (0.05). Therefore, there was no evidence to reject the alternative hypothesis that there is a statistically significant association at level 0.05 between daily sitting and LBP during quarantine (Table 2).
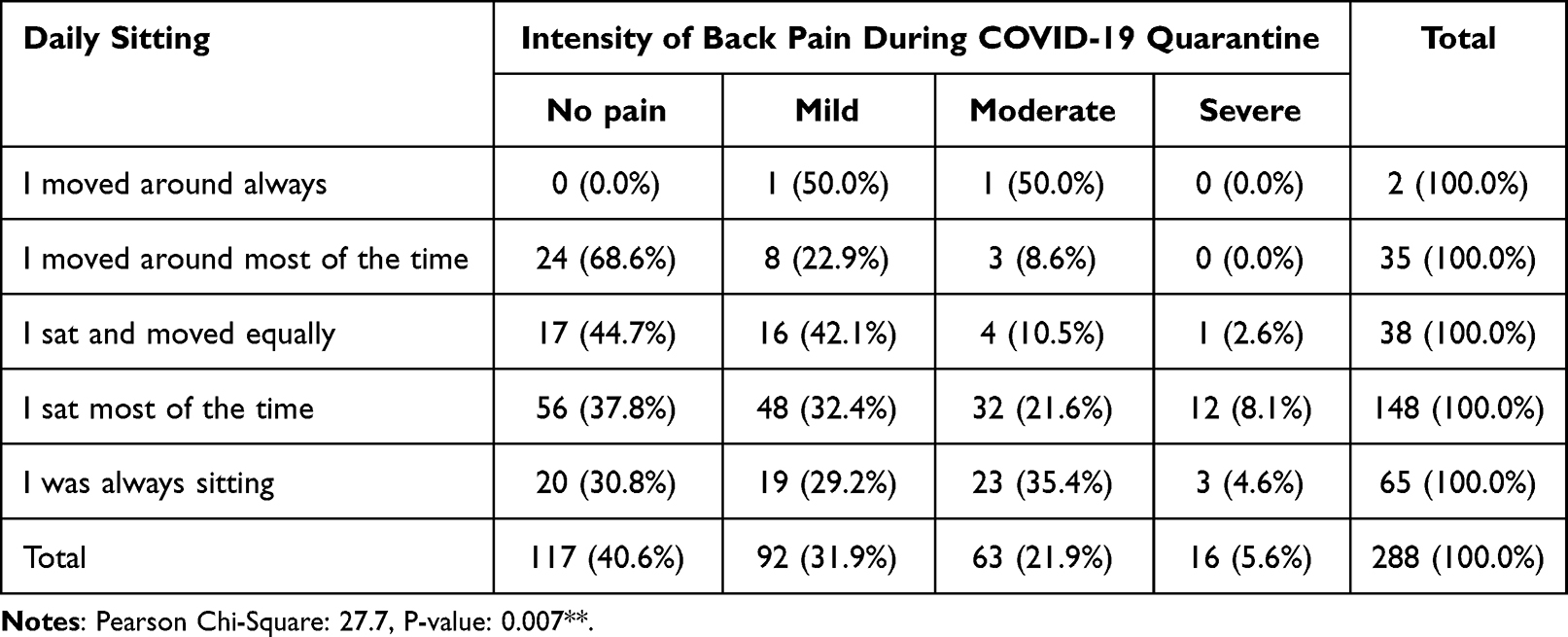 |
Table 2 Relationship Between Daily Sitting and LBP During the Quarantine |
In addition, the results of the cross-tabulation and chi-square tests for independence for the relationship between PA and LBP during quarantine showed that the test value was 21.4, and the P-value was 0.045, which is less than the significance level (0.05). Therefore, there was no evidence to reject the alternative hypothesis that there is a statistically significant association at level 0.05 between PA and LBP during quarantine (Table 3).
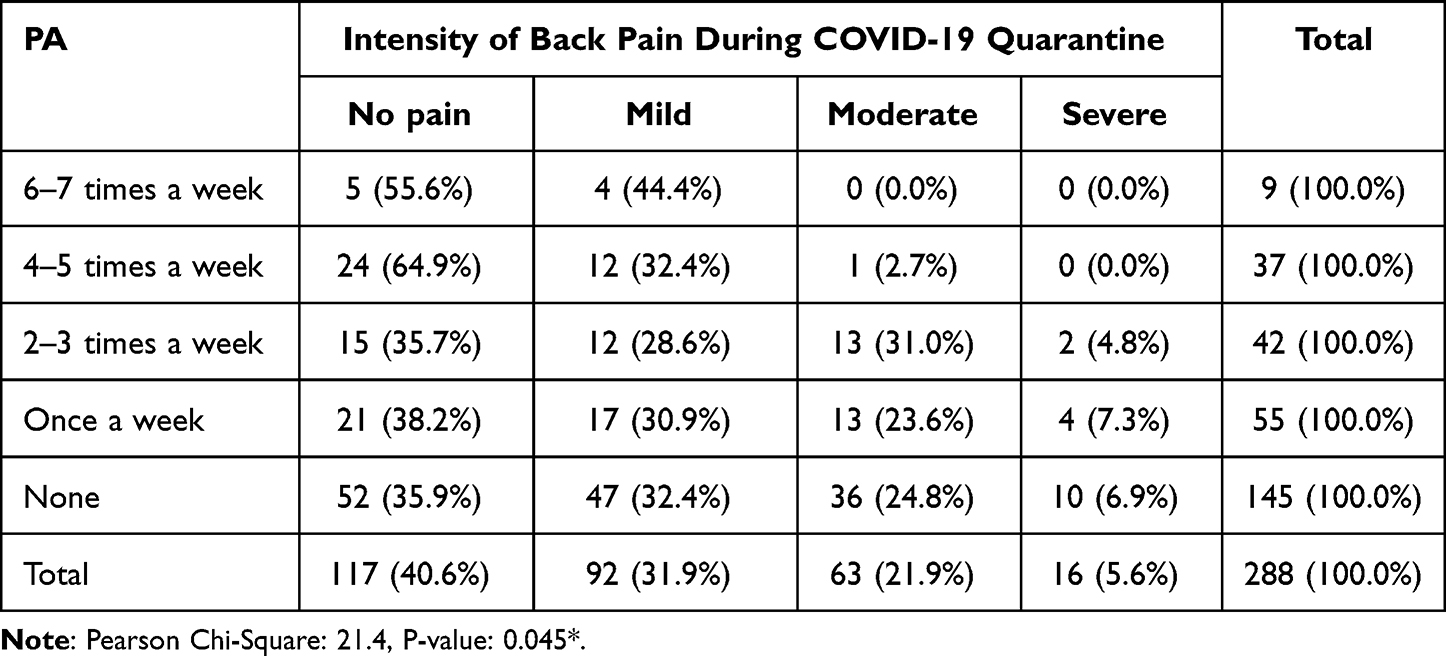 |
Table 3 Relationship Between PA and LBP During the Quarantine |
Table 4 demonstrates the results of the cross-tabulation and chi-square tests for independence for the relationship between age and medical help-seeking. The test value is 5.03, and the P-value is 0.081, which is greater than the significance level (0.05). Therefore, there is no evidence to reject the null hypothesis: there is no statistically significant association between age and medical help-seeking.
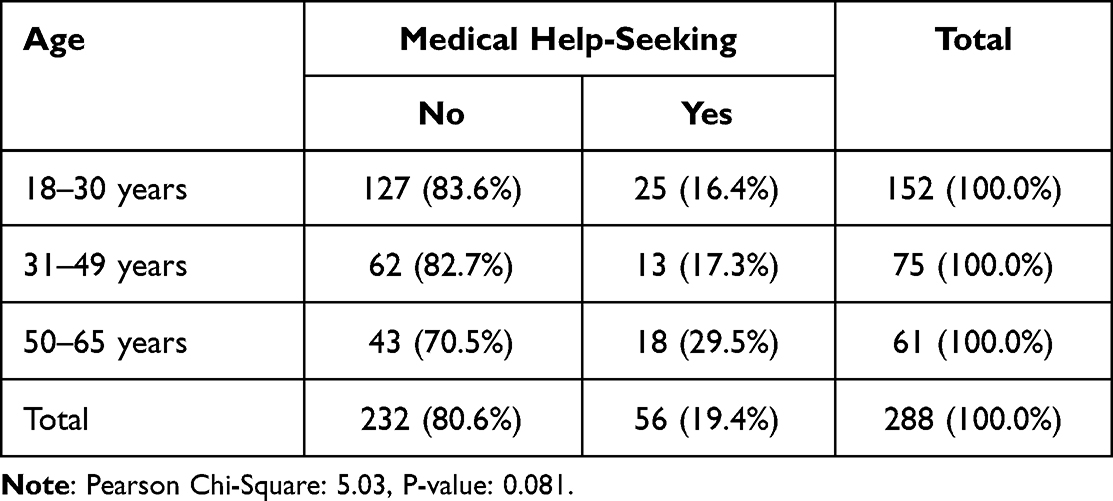 |
Table 4 Relationship Between Age and Medical Help-Seeking |
Table 5 highlights the results of the chi-squared test for independence to test the relationship between age and painkiller use for back pain. The test value is 2.77, and the P-value is 0.251, which was greater than the significance level (0.05). Therefore, there is no evidence to reject the null hypothesis: there is no statistically significant association between age and painkiller use for LBP.
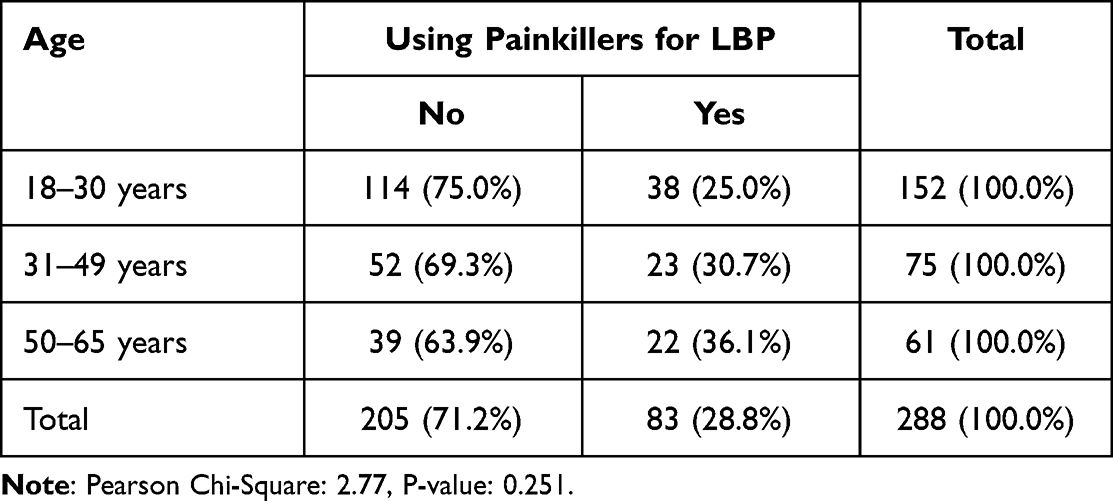 |
Table 5 Relationship Between Age and Painkiller Use for Back Pain |
Discussion
LBP is characterized by pain in the posterior part of the body from the lower margin of the twelfth rib to the lower gluteal folds lasting for at least one day. It is considered a significant public health concern and was one of the leading causes of disability globally in 2015.14 The results of this study indicated that the Saudi Arabian population had a decreased amount of movement and an increased daily sitting time during the COVID-19 quarantine period. Although the respondents were mainly younger individuals and students, most participants did not exercise or performed less exercise during the quarantine. Furthermore, the prevalence of moderate and severe back pain increased during quarantine compared with that before the quarantine.
In 2016, 27.5% of adults worldwide and approximately 58.5% of adults in Saudi Arabia were physically inactive.15 In 2013, 90% of the Saudi Arabian population sat consecutively for more than 2 h per day.16 The findings of this study confirm the results of international and local studies declaring that PA levels decreased during quarantine.13,17,18 Moreover, a cross sectional study was showed that PA and exercise characteristics for both before and after the COVID-19 pandemic, that The PA self-perception in the Brazilian and Italian samples was considerably influenced by the COVID-19 lockdown by significant decrease in PA.19 Recent studies demonstrating a decrease in all physical activity levels during house confinement in Brazil and other nations are consistent with this.20
COVID-19 home confinement dramatically impacted lifestyle activities worldwide, including participation in sports and engagement in PA.21,22 Notably, a similar number of participants (69.4%) reported no PA or PA only once a week before and during the quarantine. Meanwhile, only 3.1% of the participants performed PA 6–7 times a week during the quarantine. Furthermore, a study in Riyadh conducted by Sagat et al13 investigated the frequency of PA and found a significant increase in participants who did not perform PA and only practiced it once a week during quarantine.
Considering all these factors, there was a general decline in PA, most likely due to social isolation, travel restrictions, and gym closure.17 The majority of the population suffers from LBP at least once in their lives.23 A systematic review conducted by Mai et al24 between 1995 and 2018 showed that the prevalence of LBP among professional workers in Saudi Arabia was between 63.8% and 89%. A large percentage of participants (27.5%) had either moderate or severe back pain during quarantine, whereas 12.8% had before the quarantine. Additionally, more than half of the participants (55.4%) had LBP during the quarantine period, whereas 44.8% had before the quarantine. Similarly, a study in Brazil found that more than half of the participants (65%) did not report previous back pain, but 44% started to experience back pain during the pandemic.11 Moreover, in parallel with the results of previous studies, our data found a significant relationship between PA and LBP during quarantine.13,17,18
Older individuals may perceive back pain as a reason for not exercising instead of seeking treatment for symptomatic management.25 In our study, however, most of the participants were young (<30 years old). Furthermore, most participants (74%) sat always or most of the time during the quarantine. Meanwhile, the number of participants who always moved or moved around most of the time had decreased (33.3% of participants who moved around most of the time before quarantine decreased to 12.2% during quarantine, and 6.6% of participants who always moved around before quarantine decreased to only 0.7% during quarantine). In this sense, our findings indicate that there was an increase in daily sitting time and a decrease in movement during the quarantine compared with that before. Furthermore, a significant relationship was found between daily sitting and LBP during quarantine, corroborating the previous findings from Riyadh.13 Regarding medical help-seeking and painkiller use, a statistically significant association with age was not found. In contrast, a previous study from the US demonstrated that elderly patients with back pain tend to use painkillers more often than younger patients.26 The majority of participants in this study did not seek medical help (80.6%) and did not use painkillers (71.2%) despite the severity of their back pain. Our findings are also in agreement with a multicenter study’s results that nearly 60% of participants who have back pain do not visit a doctor.17 This can be attributed to the fact that pain is a subjective experience and is multifactorial; hence, taking pain killers and seeking medical help are influenced by factors other than just the age of the population (eg, people’s fear of visiting hospitals during the pandemic, accessibility of painkillers, type of back pain, and age-related beliefs).
The main limitations of this study were the inadequate sample size and unequal distribution of the online survey across the participants. Furthermore, self-administered questionnaires to measure PA and daily sitting were more likely to result in a recall bias and overestimation. Moreover, few studies have been conducted worldwide on the impact of COVID-19 on back pain and PA. Despite these limitations, we believe that this study provides useful insights into the community. Future studies should consider a nationwide, well-distributed survey, as well as a suitable non-cross-sectional study design to determine causality. This study highlights the urgent need to conduct more studies on the impact of COVID-19 on back pain to determine a more recent percentage occurrence and increase the awareness of the need for PA during quarantine, thereby reducing the burden of back pain and its repercussions.
Conclusion
Our study highlights the significant relationship of physical inactivity and prolonged daily sitting during the COVID-19 quarantine with an increase in the prevalence and intensity of LBP. There is an urgent need to conduct further studies to determine the impact of COVID-19 on the Saudi Arabian population.
Abbreviations
COVID-19, coronavirus disease 2019; LBP, lower back pain; PA, physical activity; PS, prolonged sitting.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author on request.
Ethics Approval and Informed Consent
Ethical approval was obtained from the institutional review board of King Abdulaziz University Hospital, Jeddah, Saudi Arabia the reference number 353-21, in accordance with the Declaration of Helsinki. Consent was obtained at the beginning of the survey for the participation in the study.
Consent for Publication
Consent was obtained for the publication of results.
Acknowledgments
We would like to thank Editage website for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020;109:102433. doi:10.1016/j.jaut.2020.102433
2. World Health Organization (WHO) Web Site. Timeline – COVID-19; 2020. Available from: https://www.who.int/news-room/detail/27-04-2020-who-timeline---covid-19.
3. Alyami AH, Alyami AA, AlMaeen BN. Impact of COVID-19 on orthopedic surgery: experience from Saudi Arabia. Ann Med Surg. 2020;56:61–63. doi:10.1016/j.amsu.2020.05.048
4. Hossain MM, Sultana A, Purohit N. Mental health outcomes of quarantine and isolation for infection prevention: a systematic umbrella review of the global evidence. Epidemiol Health. 2020;42:e2020038. doi:10.4178/epih.e2020038
5. Parmet WE, Sinha MS. Covid-19 - The law and limits of quarantine. N Engl J Med. 2020;382(15):e28. doi:10.1056/NEJMp2004211
6. Peçanha T, Goessler KF, Roschel H, Gualano B. Social isolation during the COVID-19 pandemic can increase physical inactivity and the global burden of cardiovascular disease. Am J Physiol Heart Circ Physiol. 2020;318(6):H1441–H1446. doi:10.1152/ajpheart.00268.2020
7. Mattioli AV, Sciomer S, Cocchi C, Maffei S, Gallina S. Quarantine during COVID-19 outbreak: changes in diet and physical activity increase the risk of cardiovascular disease. Nutr Metab Cardiovasc Dis. 2020;30(9):1409–1417. doi:10.1016/j.numecd.2020.05.020
8. Giustino V, Parroco AM, Gennaro A, Musumeci G, Palma A, Battaglia G. Physical activity levels and related energy expenditure during COVID-19 quarantine among the Sicilian active population: a cross-sectional online survey study. Sustainability. 2020;12(11):4356. doi:10.3390/su12114356
9. World Health Organization (WHO) Web Site. Physical activity; 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/physical-activity.
10. Corlett EN. Background to sitting at work: research-based requirements for the design of work seats. Ergonomics. 2006;49(14):1538–1546. doi:10.1080/00140130600766261
11. Ammar A, Brach M, Trabelsi K, et al. Effects of COVID-19 home confinement on eating behaviour and physical activity: results of the ECLB-COVID19 international online survey. Nutrients. 2020;12(6):1583. doi:10.3390/nu12061583
12. Hoogendoorn WE, van Poppel MN, Bongers PM, Koes BW, Bouter LM. Physical load during work and leisure time as risk factors for back pain. Scand J Work Environ Health. 1999;25(5):387–403. doi:10.5271/sjweh.451
13. Šagát P, Bartík P, Prieto González P, Tohănean DI, Knjaz D. Impact of COVID-19 Quarantine on low back pain intensity, prevalence, and associated risk factors among adult citizens residing in Riyadh (Saudi Arabia): a Cross-Sectional Study. Int J Environ Res Public Health. 2020;17(19):7302. doi:10.3390/ijerph17197302
14. Hurwitz EL, Randhawa K, Torres P, et al. The Global Spine Care Initiative: a systematic review of individual and community-based burden of spinal disorders in rural populations in low- and middle-income communities. Eur Spine J. 2018;27(Suppl 6):802–815. doi:10.1007/s00586-017-5393-z
15. Awaji MA. Epidemiology of low back pain in Saudi Arabia. J Adv Med Pharm Sci. 2016;6(4):1–9. doi:10.9734/jamps/2016/24173
16. Ministry of Health Saudi Arabia Web Site. Health information survey in Kingdom of Saudi Arabia Ministry of Health Statistics and Indicators; 2013. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/Pages/healthinformatics.aspx.
17. Bailly F, Genevay S, Foltz V, et al. Effects of COVID-19 lockdown on low back pain intensity in chronic low back pain patients: results of the multicenter CONFI-LOMB study. Eur Spine J. 2022;31(1):159–166. doi:10.1007/s00586-021-07007-8
18. Silva DR, Werneck AO, Malta DC, et al. Changes in movement behaviors and back pain during the first wave of the COVID-19 pandemic in Brazil. Braz J Phys Ther. 2021;25(6):819–825. doi:10.1016/j.bjpt.2021.07.006
19. Sonza A, da Cunha de Sá-caputo D, Sartorio A, et al. COVID-19 lockdown and the behavior change on physical exercise, pain and psychological well-being: an international multicentric study. Int J Environ Res Public Health. 2021;18(7):3810. doi:10.3390/ijerph18073810
20. Fiok K, Karwowski W, Gutierrez E, et al. A Study of the Effects of the COVID-19 pandemic on the experience of back pain reported on Twitter® in the United States: a Natural language processing approach. Int J Environ Res Public Health. 2021;18(9):4543. doi:10.3390/ijerph18094543
21. Ammar A, Chtourou H, Boukhris O, et al. COVID-19 home confinement negatively impacts social participation and life satisfaction: a worldwide multicenter study. Int J Environ Res Public Health. 2020;17(17):6237. doi:10.3390/ijerph17176237
22. De Oliveira Neto L, Elsangedy HM, Tavares VD, Teixeira CV, Behm DG, Da silva-grigoletto ME. training in home - home-based training during COVID-19 (SARS-COV2) pandemic: physical exercise and behavior-based approach. Revista Brasileira de Fisiologia Do Exercício. 2020;19(2):9. doi:10.33233/rbfe.v19i2.4006
23. Ehrlich GE. Low back pain. Bull World Health Organ. 2003;81(9):671–676.
24. Aldera MA, Alexander CM, McGregor AH. Prevalence and incidence of low back pain in the Kingdom of Saudi Arabia: a systematic review. J Epidemiol Glob Health. 2020;10(4):269–275. doi:10.2991/jegh.k.200417.001
25. Macfarlane GJ, Beasley M, Jones EA, et al. The prevalence and management of low back pain across adulthood: results from a population-based cross-sectional study (the MUSICIAN study). Pain. 2012;153(1):27–32. doi:10.1016/j.pain.2011.08.005
26. Federman AD, Litke A, Morrison RS. Association of age with analgesic use for back and joint disorders in outpatient settings. Am J Geriatr Pharmacother. 2006;4(4):306–315. doi:10.1016/j.amjopharm.2006.12.009
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.