Back to Journals » Journal of Pain Research » Volume 19
The Concurrent and Temporal Associations Between Pain Self-Efficacy, Sleep Disturbance, and Pain Intensity in Individuals with Chronic Pain: A Cross-Lagged Analysis
Authors Atisook R ![]() , Euasobhon P
, Euasobhon P ![]() , Wangnamthip S
, Wangnamthip S ![]() , Watatham S
, Watatham S ![]() , Pooliam J, Li C
, Pooliam J, Li C ![]() , Jensen MP
, Jensen MP ![]()
Received 18 December 2025
Accepted for publication 4 June 2026
Published 3 July 2026 Volume 2026:19 588853
DOI https://doi.org/10.2147/JPR.S588853
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rune Häckert Christensen
Raviwon Atisook,1 Pramote Euasobhon,1 Suratsawadee Wangnamthip,1 Sarocha Watatham,2 Julaporn Pooliam,3 Caixia Li,4 Mark P Jensen,5
1Department of Anesthesiology, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, 10700, Thailand; 2Department of Anesthesiology, Faculty of Medicine, Prince of Songkla University, Songkhla, 90110, Thailand; 3Research Group and Research Network Division, Research Department, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, 10700, Thailand; 4Department of Anesthesiology, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, 200437, People’s Republic of China; 5Department of Rehabilitation Medicine, University of Washington, Seattle, WA, 98195, USA
Correspondence: Pramote Euasobhon, Department of Anesthesiology, Faculty of Medicine, Siriraj Hospital, Mahidol University, 2 Wanglang Road, Bangkoknoi, Bangkok, 10700, Thailand, Tel +66 2419 7995, Fax +66 2411 3256, Email [email protected]; Mark P Jensen, Department of Rehabilitation Medicine, University of Washington, Seattle, WA, 98195, USA, Tel +1-206 543-3185, Fax +1-206-897-4881, Email [email protected]
Purpose: The objective of this study was to replicate and extend prior evidence regarding the concurrent associations among pain self-efficacy, sleep disturbance, and pain intensity in adults with chronic pain, and to evaluate their temporal associations over time.
Patients and Methods: This prospective study enrolled 300 Thai chronic pain outpatients from Siriraj Hospital, of whom 50 were excluded due to loss to follow-up, yielding a final sample of 250 participants. Standard questionnaires were administered to assess pain severity, pain self-efficacy, and sleep disturbance at baseline (initial visit) and again at a follow-up assessment conducted about 6 weeks later (range 4– 8 weeks). Longitudinal associations were examined using cross-lagged panel models with covariate adjustment, and moderation analyses were conducted using multiple linear regression with interaction terms.
Results: Participants were primarily female with a mean age of 54 years; neuropathic pain was the most common condition. Due to the COVID-19, about half of the participants (52%) did not return to the hospital for follow-up. However, they did return completed follow-up questionnaires via email. The average time between two assessments was 6.25 ± 1.77 weeks. Concurrent associations among pain intensity, sleep disturbance, and pain-related self-efficacy were observed in expected directions (correlations ranging from r’s = 0.42 to 0.47). After controlling for age, birth sex, education level, and pain duration, each primary study variable was significantly correlated with its corresponding variable at follow-up (r’s = 0.42 to 0.56). The only significant cross-lagged association to emerge was between pain-related self-efficacy at the initial visit and pain intensity at follow-up (β = 0.17, p < 0.01). In unadjusted regression, T1 self-efficacy was negatively associated with T2 pain intensity (β = – 0.11, p = 0.08), but the direction reversed and became significant after adjustment (β = 0.18, p < 0.01), indicating a statistical suppression effect.
Conclusion: Medium to large concurrent associations were observed in expected directions between measures of pain severity, pain self-efficacy, and sleep disturbance; each of these measures were also stable over time. Only one significant cross-lagged effect emerged, which may reflect statistical suppression rather than a true adverse temporal effect. The temporal associations between these domains require further longitudinal evaluation.
Keywords: chronic pain, pain-related self-efficacy, sleep disturbance, cross-lag association
Introduction
Chronic pain is a common condition that affects millions of individuals worldwide, with prevalence rates ranging from 10% to 50%, depending on how chronic pain is defined.1,2 It significantly impacts physical functioning, emotional well-being, and quality of life.3–6 The severity and impact of pain are known to be influenced by many factors, including those that might be less modifiable (eg, biological factors such as degree of injury and nociception, birth sex) and those that are modifiable (eg, psychological and social factors such as pain-related thoughts, coping responses, and education level).7,8
Pain intensity and sleep disturbance are two of the many challenges faced by individuals with chronic pain, and have been shown to influence each other.7,9,10 The cyclical relationship between pain and poor sleep can exacerbate symptoms, leading to a decline in health and daily functioning. Moreover, because sleep quality, like pain, is influenced by the psychological factors,11–13 it may be possible to improve pain by improving sleep via interventions that target psychological factors that impact sleep. A better understanding of the role that psychological factors play in sleep and pain could therefore inform the development of, or adaptations to, pain treatments, ultimately helping to decrease the intensity and negative impact of chronic pain.12,14
Pain-related self-efficacy refers to an individual’s confidence in their ability to perform tasks or manage challenges, even in the presence of pain. It has been found to be associated with how individuals cope with and adapt to chronic pain.15 For example, higher levels of pain self-efficacy have been shown to be associated with greater resilience, reduced emotional distress, and improved physical functioning.15,16 Conversely, lower self-efficacy has been linked to heightened perceptions of pain, increased disability, and poorer overall health.15 Although the role of self-efficacy in chronic pain management is well-documented, its relationship with key pain-related outcomes, such as pain intensity and sleep disturbance, warrants further exploration. Self-efficacy may influence sleep through multiple pathways. Higher self-efficacy can promote engagement in adaptive coping strategies, such as appropriate activity pacing, thereby improving sleep outcomes. Consistent with the importance of domain specificity, Ghose et al demonstrated in a large sample (n = 3284) that sleep self-efficacy was more strongly associated with sleep health outcomes than general self-efficacy.17 Additionally, poor sleep quality has been linked to higher levels of depression and anxiety, as well as greater pain severity. Moreover, to our knowledge, no one has examined the potential moderators of the association between pain-related self-efficacy and other pain-related variables; such analyses are needed to help determine the subgroups of individuals for whom self-efficacy may be a particularly important treatment target. Finally, the majority of research examining associations between pain self-efficacy and other pain-related factors has relied on cross-sectional designs; longitudinal evidence regarding their temporal relationships remains limited. Research using longitudinal data is needed to help identify possible causal associations.
Given these considerations, the purpose of this study was to better understand the concurrent and longitudinal associations between pain self-efficacy, sleep disturbance, and pain intensity in a sample of adults with chronic pain. Given prior research findings, we hypothesized that self-efficacy would evidence negative concurrent associations with sleep disturbance and pain intensity, and the latter two variables would be positively associated with one another at two assessment points range 4–8 weeks, depending on the next available appointment). Also, given prior research, if significant temporal associations between pain intensity and sleep disturbance emerged, we anticipated that higher levels of pain intensity assessed at one point in time would predict higher levels of sleep disturbance at the next visit, and vice versa. Also, given self-efficacy theory proposing self-efficacy as an adaptive belief, as well as the preponderance of evidence supporting negative associations between self-efficacy and dysfunction, we hypothesized that higher levels of self-efficacy at an initial assessment would prospectively predict decreases in both pain intensity and sleep disturbance at the next visit. Prior research has shown that psychological factors such as pain catastrophizing may mediate treatment-related changes in pain outcomes over the course of several weeks.18,19 Therefore, a follow-up interval of approximately six weeks was selected to allow sufficient time for potential temporal associations among pain-related self-efficacy, sleep disturbance, and pain intensity to emerge. However, temporal effects are likely dependent on the length of the lag interval, and thus the six-week follow-up period used in this study should be considered a clinically pragmatic timeframe rather than a definitive temporal window for detecting directional effects. Finally, we did not have any a priori hypotheses regarding the potential moderation effects of demographic variables on the associations among the study variables, and therefore viewed tests of moderation effects as exploratory.
Materials and Methods
Participants
The participants for this study were patients receiving care at an outpatient chronic pain clinic, in Siriraj Hospital, Bangkok, Thailand. Study inclusion criteria were: (1) ≥ 18 years old; (2) chronic pain (ie, pain duration ≥ 3 months); (3) able to read and speak Thai; (4) able to complete the study measures; and (5) provide complete data at both assessment periods. The exclusion criteria were: (1) decline study participation; (2) pain due to cancer; (3) unable to complete study procedures due to lack of Thai language literacy. This study (COA si 273/2025) was a retrospective analysis of our previous prospective collecting data trial (COA si 607/2020) with calculated sample size with reference to a prior study by Wilson et al20 After the study was approved by the Siriraj Institutional Review Board of the Faculty of Medicine in Siriraj Hospital, Mahidol University, Bangkok, Thailand, a total of 250 consecutive outpatients provided data at both assessment points from August 2020 to June 2021. In the present study, 300 participants were enrolled; 50 were excluded due to loss to follow-up, yielding a final sample of 250. Follow-up was conducted during in-person visits to the outpatient department (n = 119) or via Email (n = 131). No missing data were observed for the variables included in the analyses irrespective of the mode of follow-up data collection. The study was conducted in accordance with the Declaration of Helsinki.
Procedures
After enrolling in the study and signing informed consent forms, participants completed a demographic and pain history questionnaire at the initial visit (T1). They were then administered hard copies of the study measures (described in the next section) by a research staff member who also provided verbal instructions and was available to answer questions about the scales. Depending on appointment availability, participants were scheduled for a follow-up visit (T2) about 4–8 weeks after the initial visit and were again asked to complete the study measures. Due to the COVID-19, about half of the participants (52%) did not return to the hospital for follow-up. However, they did return completed follow-up questionnaires via email. The average time between initial (T1) and follow-up (T2) assessments was 6.25 ± 1.77 weeks.
Measures
Demographic Data
The study participants were asked to complete a questionnaire that collected demographic data (ie, age, birth sex, and education level) and pain history information, including pain diagnosis, pain duration, and cause of pain For the planned moderation analyses, participants were classified into different age (≤ 60 years old vs. > 60 years old), education level (≤ 12 years or > 12 years of education) and pain period duration (categorized into three groups as ≤ 2 years, > 2-5 years, and > 5 years) groups.
Pain Intensity
Based on prior research showing that the 0 to 10 Numerical Rating Scale (NRS-11) has the most utility in Thai individuals with chronic pain,21,22 we administered this measure to assess 7-day recalled average pain intensity. With this measure, respondents are asked to choose a number from 0 to 10 that best represents their “Usual pain intensity in the past 7 days,” with 0 = “No pain at all” and 10 = “Pain as bad as it could be.”
Sleep Disturbance
The four items assessing sleep disturbance subscale from Thai version of the Patient Reported Outcomes Measurement Information System (T-PROMIS-29) were used to measure sleep disturbance over the past 7 days.23,24 Each item is rated on a 1 (“Very good/Very much”) to 5 (“Very poor/not at all”) Likert scale. Higher scores indicate greater sleep disturbance. The responses are summed and transformed to a T-score (ie, mean of 50 and SD of 10 in the normative sample). The PROMIS Sleep Disturbance scale demonstrates high reliability and validity similarly to the EuroQol (EQ-5D-5L).25
Pain-Related Self-Efficacy
Pain-related self-efficacy refers to the confidence that individuals with chronic pain have in coping with their condition and managing the impact of pain on their lives. It is conceptually distinct from related constructs such as pain catastrophizing, depression/anxiety, coping style, and fear-avoidance, which reflect maladaptive cognitions, emotional distress, behavioral tendencies, and avoidance responses, respectively. The University of Washington Pain-Related Self-Efficacy Scale (T-UW-PRSE) was developed in 2018 from an expert panel of pain clinicians26 and translated into Thai version with good internal consistency (Cronbach α = 0.85) and moderate test-retest reliability (ICC(2,1) = 0.72).27 The measure has demonstrated good validity and moderate test-retest reliability for individuals with chronic pain,28 including individuals from Thailand with chronic low back pain.24
The 6-item Thai version of the University of Washington Pain-Related Self-Efficacy Scale (T-UW-PRSES)27 was used to assess pain-related self-efficacy. With the T-UW-PRSES, respondents were asked to rate their level of confidence in being able to engage in six activities despite their pain on a 1 (“Not at All”) to 5 (“Very much”) scale. A sample item is, “How confident are you that you can do most of your daily activities in spite of your pain?” The responses are summed into a total score and transformed into T-scores; a higher T-score represents a higher level of self-efficacy. The original measure has demonstrated good validity and reliability in individuals with low back pain,28 and the Thai version of this measure used in the current study has also demonstrated good validity and moderate test-retest reliability.27
Statistical Analyses
We first computed descriptive statistics for demographic variables to characterize the study sample. To evaluate the hypothesized concurrent associations between pain self-efficacy, sleep disturbance, and pain intensity, we computed Pearson correlation coefficients between these variables at both assessment points. Next, to estimate and test for the lagged associations between pain intensity, sleep disturbance, and pain-related self-efficacy, we employed longitudinal cross-lagged path models within a structural equation modeling framework. Age, birth sex, education level, and pain duration were included as control variables to better isolate the unique variance associated with the relationships between pain intensity, sleep disturbance, and pain-related self-efficacy. Although we intended for the final models to include these demographic covariates, we also evaluated the models without these covariates in sensitivity analyses to determine if the patterns of results were affected by their inclusion. We included measures of pain intensity, sleep disturbance, and pain-related self-efficacy at both time points in the model. To account for autocorrelations (the associations between the same variable at subsequent time points), we added auto-regressive paths between each measure of pain intensity, sleep disturbance, and pain-related self-efficacy and the same measure at the next consecutive time point. To account for synchronous correlations, we allowed the errors corresponding to the measures of pain intensity, sleep disturbance, and pain-related self-efficacy at the same time points to correlate. We included auto-regressive paths between pain intensity, sleep disturbance, and pain-related self-efficacy, as well as the opposite measure at the subsequent time point (eg, T1 pain intensity predicts T2 sleep disturbance, T1 pain intensity predicts T2 pain-related self-efficacy, and vice versa) to assess the cross-lagged associations between the study variables Cross-lagged path coefficients were evaluated using post-estimation analyses via the Structural Equation Modeling (SEM) command to determine whether differences in coefficients were statistically significant Model fit for the cross-lagged analyses was assessed using the root mean square error of approximation (RMSEA), χ2, the comparative fit index (CFI), and the Tucker–Lewis index (TLI). Adequate fit was indicated by RMSEA ≤ 0.06 and CFI and TLI ≥ 0.95 and SRMR ≤ 0.08.29
Finally, to address the aim to identify possible demographic and pain-related factors that might moderate the cross-lagged associations between the study variables, we conducted a series of multiple linear regressions, testing the interaction terms between each predictor assessed at the initial assessment and candidate moderator variables, as a predictor of the other variables assessed six weeks later We used a p value of 0.05 to identify significant associations for all tests of direct effects. However, we used a p value of 0.01 to identify potential moderators in the moderation analyses, to balance the need to control for both type 1 and type 2 errors, given the large number of moderation tests conducted. Longitudinal cross-lagged path analyses were performed using STATA version 17.0 (Stata Corp LP, Texas, USA), and descriptive statistics were computed using IBM SPSS Statistics version 29.0 (IBM Corp, Armonk, NY, USA).
Results
Descriptive Data
After the exclusion of 50 participants due to loss to follow-up, the final sample comprised 250 participants. The sample was predominantly female (60%), with a mean age of 54 years; neuropathic pain was the most common diagnosis. Pain duration on average was 6 years, with the minimum of 3 months and the maximum of 30 years. Descriptive data for the study sample are presented in Table 1.
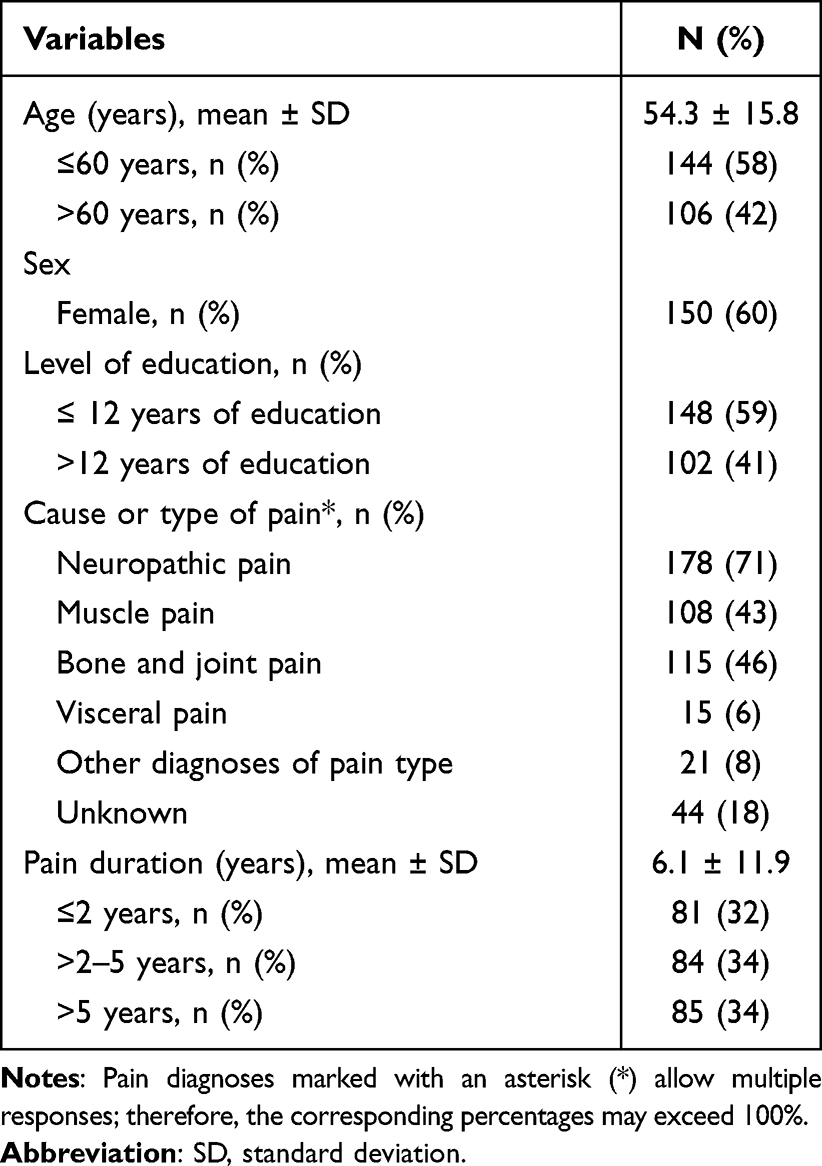 |
Table 1 Descriptive Data for the Study Sample |
Concurrent Associations Between Pain Intensity, Sleep Disturbance, and Self-Efficacy
The concurrent Pearson’s correlation coefficients between pain intensity, sleep disturbance, and pain-related self-efficacy at T1 and T2 are presented in Table 2. As can be seen, the magnitude of these associations were in the medium to large effect size range (ie absolute value range, 0.42 to 0.47), and the directions of the correlation were as expected; that is, there were moderate positive associations between pain intensity and sleep disturbance, and moderate negative correlations between self-efficacy and both pain intensity and sleep disturbance.
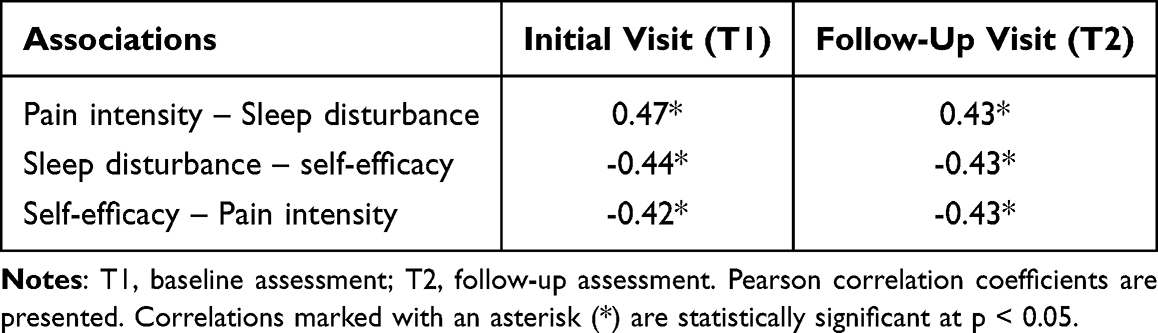 |
Table 2 Concurrent Pearson Correlations Among Pain Intensity, Sleep Disturbance, and Pain-Related Self-Efficacy at the Initial Visit (T1) and Follow-Up Visit (T2) |
Longitudinal Cross-Lagged Path Models
The structural equation model showed χ2(61) = 143.81, p < 0.001 RMSEA = 0.074 (90% CI = 0.058-0.089), CFI = 0.904, and SRMR = 0.031. Standardized path coefficients with 95% confidence intervals are presented in Table 3. As can be seen, each primary study variable at the initial visit (pain intensity, sleep disturbance, and pain-related self-efficacy) had a strong association with its corresponding variable at the second visit. The only significant cross-lagged association to emerge was between pain-related self-efficacy assessed at T1 and pain intensity assessed at T2. This association indicated that participants who endorsed higher levels of pain-related self-efficacy at T1 subsequently reported larger increases in pain intensity from T1 to T2 than those who reported lower levels of self-efficacy at T1. The cross-lagged coefficient for this effect (β = 0.17) indicates a large effect size (ie, > 0.12).29
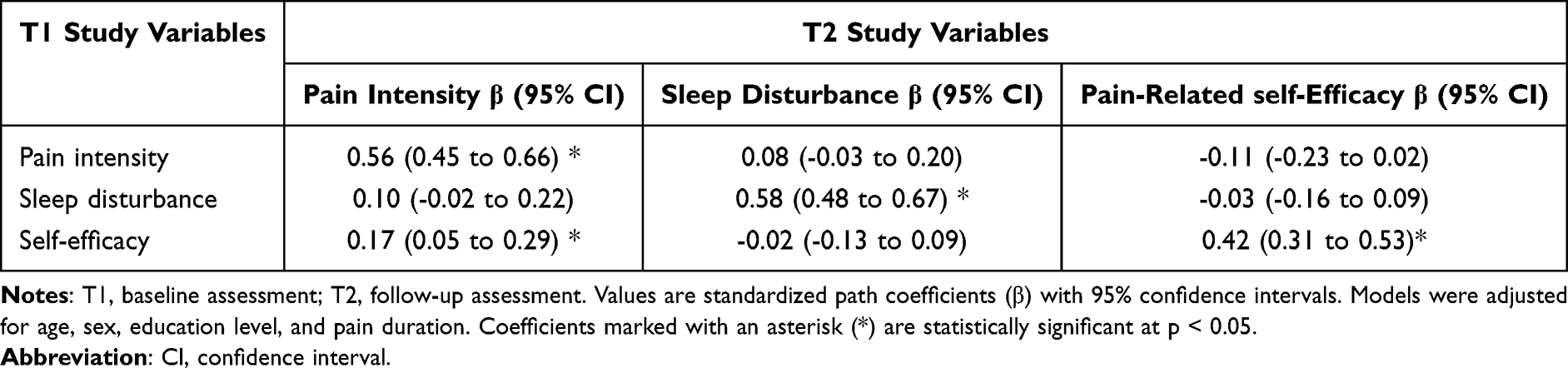 |
Table 3 Cross-Lagged Coefficients for the Study Variables From the Initial Visit (T1) to the Follow-Up Visit (T2) |
As this cross-lagged effect for self-efficacy was inconsistent with what we anticipated given both theory and prior evidence regarding the concurrent associations between pain self-efficacy and pain intensity as well as in the current study (see prior section and Table 2), we conducted a series of unadjusted and adjusted regression analyses to test whether the temporal association between T1 self-efficacy and a subsequent increase in pain intensity might reflect an instance of statistical suppression, due to the inclusion of one or more variables in the model. The results of these additional analyses are presented in Table 4. As can be seen, in the unadjusted model, T1 self-efficacy was negatively associated with T2 pain intensity, consistent with the study hypothesis and suggesting a potentially beneficial effect of self-efficacy, although this association did not reach statistical significance. With inclusion of covariates in an adjusted model, the direction of the relationship changed; that is, T1 self-efficacy became positively associated with T2 pain intensity, and this association was statistically significant. This shift in direction supports the presence of a suppression effect, wherein the inclusion of certain variables—most notably T1 pain intensity—changed the direction of the lagged associated between T1 self-efficacy and T2 pain intensity. The conclusion of longitudinal cross-lagged panel model is shown in Figure 1.
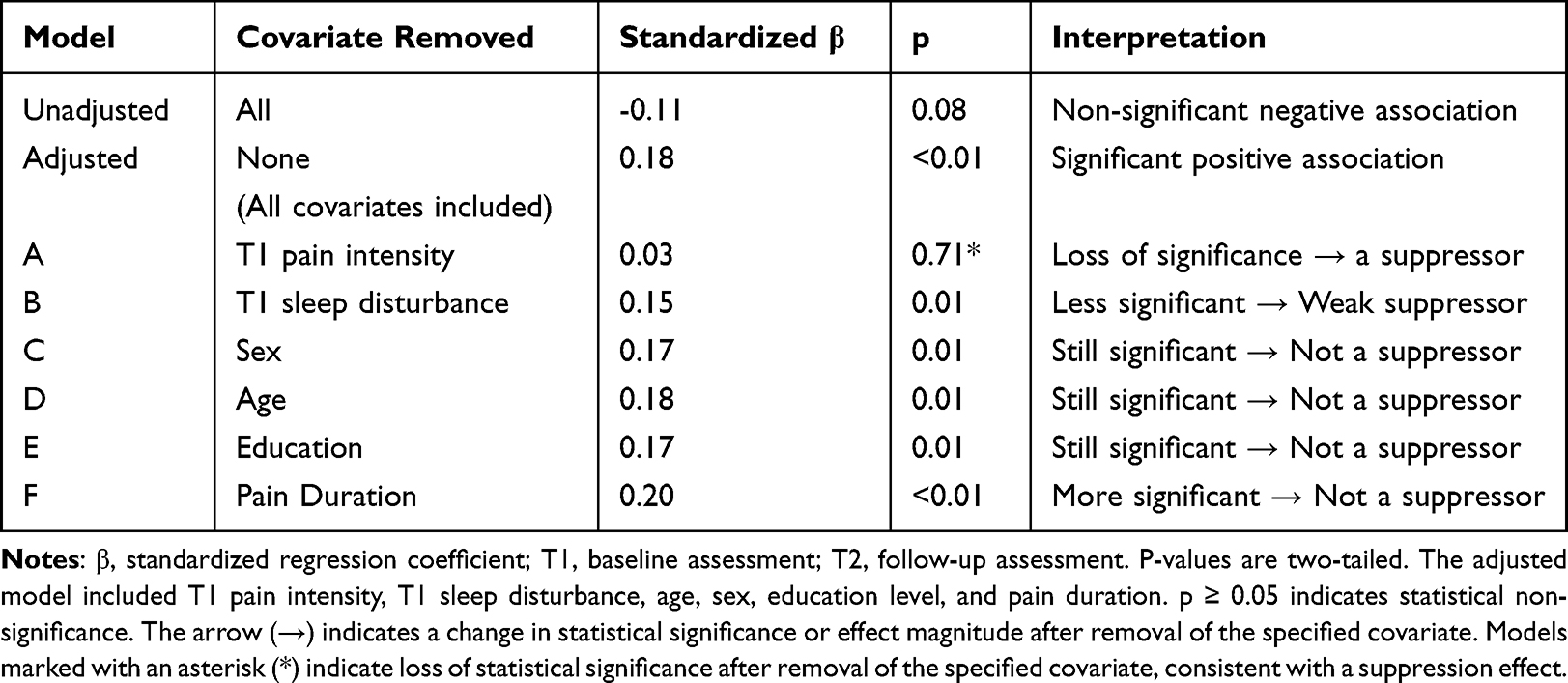 |
Table 4 Regression Analysis Evaluating the Suppression Effect of Individual Covariates From the Adjusted Model on the Association Between T1 Self-Efficacy and T2 Pain Intensity |
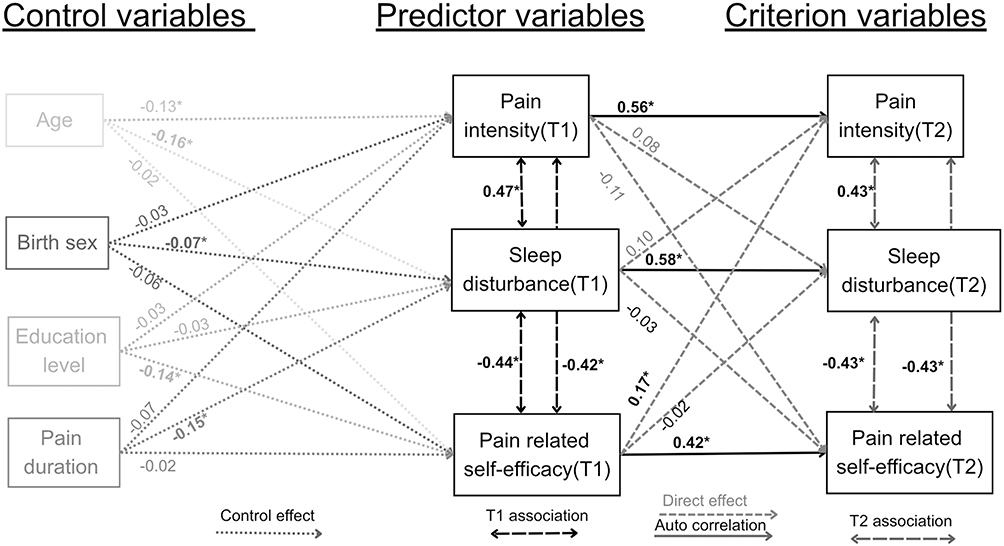 |
Figure 1 The longitudinal cross-lagged panel model. Notes: Statistically significant associations (p <0.05) are presented in bold and marked with an asterisk. |
Moderation Effects
Four of the candidate moderators of the associations between the study variables were non-significant (p > 0.01) in all of the moderation analyses: birth sex, education level, and two pain duration variables (ie, ≤ 2 years vs >2-5 years vs. > 5 years). However, two of the moderation tests emerged as significant: Age X T1 Self-Efficacy predicting T2 pain intensity (β for interaction term = -1.10, p < 0.01) and Age X T1 Self-Efficacy predicting T2 Self-efficacy (β for interaction term = -1.16, p < 0.01). To help interpret these moderation effects, we computed the associations between T1 self-efficacy and T2 pain intensity and between T1 self-efficacy and T2 self-efficacy for both younger (≤ 60 years) and older (> 60 years) participants. In both cases, the magnitudes of the associations were stronger for the younger participants (-0.25 and 0.60, respectively) than older participants (0.08 and 0.33, respectively).
Discussion
The primary study aim was to better understand the concurrent and longitudinal associations between pain self-efficacy, sleep disturbance, and pain intensity. Concurrent associations were as expected, with medium to large effect size associations between the three primary study variables at each assessment point. We identified one significant temporal association between the study variables; higher pain self-efficacy assessed at one point in time predicted subsequent increases in pain intensity over the course of the next six weeks, although the direction of this association was opposite of what was hypothesized. Finally, age (but not birth sex, education level, or pain duration) was found to moderate the associations between self-efficacy measured at the initial assessment and subsequent pain intensity and self-efficacy assessed 6 weeks later, with these associations being stronger for younger participants than older participants. The study findings have important implications for understanding the potential mutual influences between pain intensity, sleep disturbance, and self-efficacy.
Overall, the fit indices indicated an acceptable model fit. Although the CFI and SRMR satisfied the predefined criteria for adequate fit, the RMSEA and TLI values fell marginally outside the recommended thresholds (RMSEA ≤ 0.06; TLI ≥ 0.95). Nevertheless, because the CFI and SRMR are generally less sensitive to model complexity than the RMSEA and TLI, the overall pattern of fit indices suggests that the hypothesized model provided a reasonable representation of the observed data.29
Concurrent associations
The medium to strong concurrent associations between pain intensity, sleep disturbance, and self-efficacy were all in expected directions, and consistent with prior research. For example, Adegbola and colleagues found that pain related self-efficacy was positively associated with sleep quality and negatively associated with pain intensity in 90 sickle cell disease patients with chronic sickle cell disease pain.30 Similarly, a meta-analysis of 83 studies on self-efficacy and chronic pain outcomes by Jackson et al found that the overall associations between self-efficacy impairment and chronic pain severity were highly significant and remarkably consistent across studies (r = -0.39, 95% CI, -0.47 to -0.39, p < 0.001).15
Cross-Lagged Associations
Prior research has been inconsistent with respect to the temporal associations between pain intensity and sleep disturbance, with some studies identifying significant associations (sometimes bi-directional/mutual9,10,15,30–32 and sometimes not bi-directional33) and other studies not showing significant associations.31 However, when significant, the associations found tend to be in the expected directions, with more pain intensity predicting more subsequent sleep disturbance and vice versa.31 The findings from the analyses conducted here fall within the range of findings from prior research, with weak and non-significant associations that were still in the expected directions. In addition, as noted, the sample size and high autoregressive stability (which reduced the variance available for prediction) may not have allowed sufficient power to detect anything other than large effects. Therefore, the absence of statistically significant cross-lagged associations should not be interpreted as evidence of no temporal relationship. The current sample size may have been underpowered to detect small cross-lagged effects. Additional studies with larger sample sizes and additional assessment waves are needed to help identify cross-lagged paths that may exist but could not be detected in the current study.
Taken as a whole, the findings suggest that there is a generally consistent but weak impact of pain on sleep and of sleep on pain, on average. What is not known is whether the associations are generally weak for everyone with chronic pain, or if there are individuals for whom the associations are strong and individuals for whom the associations are minimal; that is, whether there are moderators that might influence the strength of the temporal associations between pain intensity, self-efficacy, and sleep disturbance. Research to understand this latter issue is needed in order to determine if there are individuals with chronic pain who might benefit more or less from treatments that are known to be effective for improving sleep quality (see the discussion of moderation effects later in this Discussion).
To our knowledge, this study is the first that examined the temporal associations between pain self-efficacy and both pain intensity and sleep disturbance. Inconsistent with the study hypothesis, as well as with findings from the concurrent association analyses and moderation analyses, we found that higher levels of pain self-efficacy measured at the initial assessment predicted increases in subsequent pain intensity. If this finding is reliable, it could have a number of explanations. Because activity levels and pacing behaviors were not directly measured, this unexpected finding should be interpreted cautiously and may reflect statistical suppression or residualized associations among correlated baseline variables rather than a true adverse effect of self-efficacy. It is also possible that low pain levels might both (1) influence an individual’s beliefs about an individual’s ability to control pain and its effects and (2) be associated with a greater likelihood of experiencing more subsequent pain due to regression to the mean. Finally, the reversal in direction between unadjusted and adjusted analyses supports the possibility of statistical suppression. Overall, the findings both support the potential importance of self-efficacy as playing a role in pain intensity, while also underscoring the complexity of pain and the factors that can impact pain.
Moderation Effects
As noted previously, one possible explanation for inconsistency in findings regarding the association among variables is that such associations vary as a function of the specific characteristics of the population. Identifying the characteristics that may moderate the concurrent or temporal associations between pain-related variables is important for helping to understand the reasons for inconsistent findings, as well as for identifying populations for whom targeting specific factors in treatment might be most helpful. Here, we found that birth sex, pain duration, and education level did not moderate the temporal associations among the study variables, suggesting that treatments that target these variables would have similar effects across these groups. However, two significant age effects emerged. These findings should be interpreted cautiously as exploratory and hypothesis-generating rather than as evidence supporting specific clinical recommendations; additional research is needed to determine the reliability of these age-moderating effects.
Discrepancy Between the Concurrent and Cross-Lagged Findings
The contrast between the concurrent associations and the much weaker—and mostly non-significant—temporal associations warrants comment. Such differences are unlikely to be due to shared method variance, as all data were obtained via self-report; if anything, shared method variance would be expected to result in consistent associations between the concurrent and temporal analyses. Nevertheless, some conceptual overlap exists between pain intensity and sleep disturbance because both partly reflect shared symptom burden. Therefore, some observed associations may reflect overlapping constructs rather than directional effects alone.
Importantly, the two-wave cross-lagged design used here cannot distinguish stable between-person differences from within-person changes over time, which limits interpretation of the observed temporal associations. One possible explanation is that there exists an unmeasured variable (eg, depression, anxiety, neuroticism, catastrophizing) that influences all three of the primary study variables but does not substantially change over time In this case, if the unidentified variable is the key causal factor and the three primary study variables do not influence one another, then treatments that change any of these variables would likely yield benefits only for the directly targeted outcome. Another possibility is that the lag time studied here (6 weeks) was not the optimal timeframe for causal effects to emerge. For example, if the beneficial effects of self-efficacy on pain and sleep disturbance occur within one week or less, then it would be necessary to assess these variables over shorter intervals rather than six weeks. Determining which of these explanations is accurate would require both (1) assessing additional candidate causal variables and (2) assessing the variables multiple times (eg, weekly over the course of several weeks, to be able to evaluate 1-week and >1-week lag effects) period. Such research would be important to conduct because identifying causal factors is of critical importance for the design of effective interventions.
Limitations
This study had several limitations. First, all the participants were from a single tertiary care hospital in Bangkok, Thailand. According to data from Thailand’s Office of Education,34 our participants had a higher proportion of higher-education attainment than the general Thai population. Second, we examined temporal associations only over a 6-week period. It is possible that any causal effects among the study variables may have their largest impact over shorter or different timeframes. Third, although a 6-week interval may capture symptom variability, it may be insufficient to detect robust changes in self-efficacy. Future research employing both shorter and longer lag intervals is warranted. Fourth, due to COVID-19, follow-up data were collected either in person or via email, which may have introduced bias. However, sensitivity analyses adjusting for follow-up mode yielded similar findings. Fifth, treatments (including medication use) were not monitored and may have influenced pain and sleep outcomes, potentially attenuating associations with self-efficacy. Future studies should assess and adjust for these factors when possible. Sixth, all variables were assessed using self-report measures, and some overlap between pain intensity and sleep disturbance may have influenced the observed associations. Finally, although the analyses were hypothesis-driven, a large number of analyses were conducted. Replication of the findings in additional samples is needed to determine which of the study findings are reliable.
Summary and Conclusions
This study examined the concurrent and longitudinal associations between measures of pain-related self-efficacy, sleep disturbance, and pain intensity in adults with chronic pain. Medium to large effect-size concurrent associations were observed in expected directions (eg, higher self-efficacy was associated with lower pain intensity and less sleep disturbance). In contrast, short-term temporal relationships among these variables remain uncertain. Only one significant cross-lagged effect emerged: higher baseline self-efficacy predicted greater subsequent pain intensity; however, post hoc analyses suggested that this unexpected finding was likely due to statistical suppression rather than true adverse effects of self-efficacy on future pain intensity.
Overall, the findings highlight the complex interplay among psychological and physical factors in chronic pain and underscore the need for future longitudinal research and additional psychosocial variables. Future research using more comprehensive longitudinal designs, incorporating additional psychosocial variables, and employing varied follow-up intervals is needed to better clarify the mechanisms and temporal dynamics linking self-efficacy, sleep, and pain in individuals with chronic pain.
Acknowledgments
We are sincerely grateful to all participants who generously contributed their time to this study. We also thank Ms. Natsupa Wiriyakulsit for her support with coordination and document preparation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Siriraj Research Fund, Faculty of Medicine, Siriraj Hospital, Mahidol University (Grant No. R016331070), and by the Chalermprakiat Foundation, Faculty of Medicine, Siriraj Hospital, Mahidol University.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Zimmer Z, Fraser K, Grol-Prokopczyk H, Zajacova A. A global study of pain prevalence across 52 countries: examining the role of country-level contextual factors. Pain. 2022;163(9):1740–11. doi:10.1097/j.pain.0000000000002557
2. Rometsch C, Martin A, Junne F, Cosci F. Chronic pain in European adult populations: a systematic review of prevalence and associated clinical features. Pain. 2025;166(4):719–731. doi:10.1097/j.pain.0000000000003406
3. Duenas M, Ojeda B, Salazar A, Mico JA, Failde I. A review of chronic pain impact on patients, their social environment and the health care system. J Pain Res. 2016;9:457–467. doi:10.2147/JPR.S105892
4. Miaskowski C, Blyth F, Nicosia F, et al. A Biopsychosocial Model of Chronic Pain for Older Adults. Pain Med. 2020;21(9):1793–1805. doi:10.1093/pm/pnz329
5. Hadi MA, McHugh GA, Closs SJ. Impact of Chronic Pain on Patients’ Quality of Life: a Comparative Mixed-Methods Study. J Patient Exp. 2019;6(2):133–141. doi:10.1177/2374373518786013
6. Kawai K, Kawai AT, Wollan P, Yawn BP. Adverse impacts of chronic pain on health-related quality of life, work productivity, depression and anxiety in a community-based study. Fam Pract. 2017;34(6):656–661. doi:10.1093/fampra/cmx034
7. Yi D, Yang M, Luo Q, Li H, Kong L, Cheng Q. Bidirectional relationship between pain and sleep disturbance in middle-aged and older adults: evidence from the China health and retirement longitudinal study. Front Psychiatry. 2024;15:1485822. doi:10.3389/fpsyt.2024.1485822
8. Meints SM, Edwards RR. Evaluating psychosocial contributions to chronic pain outcomes. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87(Pt B):168–182. doi:10.1016/j.pnpbp.2018.01.017
9. Burgess HJ, Burns JW, Buvanendran A, et al. Associations Between Sleep Disturbance and Chronic Pain Intensity and Function: a Test of Direct and Indirect Pathways. Clin J Pain. 2019;35(7):569–576. doi:10.1097/AJP.0000000000000711
10. Amtmann D, Bamer AM, Askew R, Jensen MP. Cross-lagged longitudinal analysis of pain intensity and sleep disturbance. Disabil Health J. 2020;13(3):100908. doi:10.1016/j.dhjo.2020.100908
11. Zaidel C, Musich S, Karl J, Kraemer S, Yeh CS. Psychosocial Factors Associated with Sleep Quality and Duration Among Older Adults with Chronic Pain. Popul Health Manag. 2021;24(1):101–109. doi:10.1089/pop.2019.0165
12. Zambelli Z, Halstead EJ, Fidalgo AR, Dimitriou D. Good Sleep Quality Improves the Relationship Between Pain and Depression Among Individuals With Chronic Pain. Front Psychol. 2021;12:668930. doi:10.3389/fpsyg.2021.668930
13. Chen YM, Wang JH, Liang CS, Lin YK, Yang FC. Clinical and psychological predictors of sleep quality in chronic migraine: a preliminary retrospective analysis study. BMC Neurol. 2025;25(1):156. doi:10.1186/s12883-025-04165-w
14. Keilani M, Crevenna R, Dorner TE. Sleep quality in subjects suffering from chronic pain. Wien Klin Wochenschr. 2018;130(1–2):31–36. doi:10.1007/s00508-017-1256-1
15. Jackson T, Wang Y, Wang Y, Fan H. Self-efficacy and chronic pain outcomes: a meta-analytic review. J Pain. 2014;15(8):800–814. doi:10.1016/j.jpain.2014.05.002
16. Van Liew C, Brown KC, Cronan TA, Bigatti SM, Kothari DJ. Predictors of pain and functioning over time in fibromyalgia syndrome: an autoregressive path analysis. Arthritis Care Res. 2013;65(2):251–256. doi:10.1002/acr.21792
17. Ghose SM, Dzierzewski JM, Dautovich ND. Sleep and self-efficacy: the role of domain specificity in predicting sleep health. Sleep Health. 2023;9(2):190–195. doi:10.1016/j.sleh.2022.09.008
18. Gilliam WP, Craner JR, Schumann ME, Gascho K. The Mediating Effect of Pain Catastrophizing on PTSD Symptoms and Pain Outcome. Clin J Pain. 2019;35(7):583–588. doi:10.1097/AJP.0000000000000713
19. Smeets RJ, Vlaeyen JW, Kester AD, Knottnerus JA. Reduction of pain catastrophizing mediates the outcome of both physical and cognitive-behavioral treatment in chronic low back pain. J Pain. 2006;7(4):261–271. doi:10.1016/j.jpain.2005.10.011
20. Wilson M, Skeiky L, Muck RA, et al. Pain Catastrophizing Mediates the Relationship Between Pain Intensity and Sleep Disturbances in U.S. Veterans With Chronic Pain. Mil Med. 2023;188(7–8):e2639–45. doi:10.1093/milmed/usac065
21. Euasobhon P, Atisook R, Bumrungchatudom K, Zinboonyahgoon N, Saisavoey N, Jensen MP. Reliability and responsivity of pain intensity scales in individuals with chronic pain. Pain. 2022;163(12):e1184–e1191. doi:10.1097/j.pain.0000000000002692
22. Atisook R, Euasobhon P, Saengsanon A, Jensen MP. Validity and Utility of Four Pain Intensity Measures for Use in International Research. J Pain Res. 2021;14:1129–1139. doi:10.2147/JPR.S303305
23. Rawang P, Janwantanakul P, Correia H, Jensen MP, Kanlayanaphotporn R. Cross-cultural adaptation, reliability, and construct validity of the Thai version of the Patient-Reported Outcomes Measurement Information System-29 in individuals with chronic low back pain. Qual Life Res. 2020;29(3):793–803. doi:10.1007/s11136-019-02363-x
24. Khutok K, Janwantanakul P, Jensen MP, Kanlayanaphotporn R. Responsiveness of the PROMIS-29 Scales in Individuals With Chronic Low Back Pain. Spine. 2021;46(2):107–113. doi:10.1097/BRS.0000000000003724
25. Mulhern BJ, Pan T, Norman R, et al. Understanding the measurement relationship between EQ-5D-5L, PROMIS-29 and PROPr. Qual Life Res. 2023;32(11):3147–3160. doi:10.1007/s11136-023-03462-6
26. Amtmann D, Liljenquist K, Bamer A, et al. Measuring Pain Catastrophizing and Pain-Related Self-Efficacy: expert Panels, Focus Groups, and Cognitive Interviews. Patient. 2018;11(1):107–117. doi:10.1007/s40271-017-0269-1
27. Khampanthip A, Kanlayanaphotporn R, Jensen MP, Janwantanakul P. Cross-cultural adaptation, test-retest reliability, and construct validity of the Thai version of the University of Washington Pain-Related Self-Efficacy Scale. Pain Rep. 2019;4(6):e787. doi:10.1097/PR9.0000000000000787
28. Fritz JM, Alodaibi F, Bamer AM, Amtmann D. Psychometric examination of short forms from the University of Washington pain-related self-efficacy and concerns about pain item banks in patients with low back pain. Qual Life Res. 2022;31(2):621–631. doi:10.1007/s11136-021-02923-0
29. Orth U, Meier LL, Buhler JL, et al. Effect size guidelines for cross-lagged effects. Psychol Methods. 2024;29(2):421–433. doi:10.1037/met0000499
30. Adegbola M. Sleep Quality, Pain and Self-Efficacy among Community-Dwelling Adults with Sickle Cell Disease. J Natl Black Nurses Assoc. 2015;26(1):15–21.
31. Lapane KL, Shridharmurthy D, Harkey MS, Driban JB, Dube CE, Liu SH. The relationship between restless sleep and symptoms of the knee: data from the Osteoarthritis Initiative. Clin Rheumatol. 2021;40(6):2167–2175. doi:10.1007/s10067-020-05531-4
32. Alsaadi SM, McAuley JH, Hush JM, et al. The bidirectional relationship between pain intensity and sleep disturbance/quality in patients with low back pain. Clin J Pain. 2014;30(9):755–765. doi:10.1097/AJP.0000000000000055
33. Vaegter HB, Hoybye MT, Bergen FH, Parsons CE. Sleep disturbance in patients attending specialized chronic pain clinics in Denmark: a longitudinal study examining the relationship between sleep and pain outcomes. Scand J Pain. 2021;21(3):539–547. doi:10.1515/sjpain-2020-0155
34. Office of the Education Coucil. Average years of schooling in Thailand. 2024. https://www.onec.go.th/th.php/book/BookView/2135.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Factors Associated with Depression, Anxiety, and Sleep Disturbance Among Patients with Moderate-to-Severe Chronic Pain: A Multicenter Cross-Sectional Study
Guo SQ, Wang LQ, Tu JF, Yang JW, Shi GX, Yan SY, Li T, Fu Y, Zhou ZY, Ji CC, Hu H, Han LF, Liu M, Xu SF, Li M, Liu LY, Chen F, Liu CZ
Journal of Pain Research 2025, 18:6791-6805
Published Date: 16 December 2025