Back to Journals » International Journal of Nanomedicine » Volume 21
The Application of Nanomaterials in Kidney Stone Disease: Emerging Strategies for Early Diagnosis, Targeted Therapy, and Prevention
Authors Zuo J, Zhang Z ![]() , Chen J
, Chen J ![]() , Gou K, Zhou J
, Gou K, Zhou J ![]() , Wen L, Wei H, Li X, Zhan P, Chen P
, Wen L, Wei H, Li X, Zhan P, Chen P ![]() , Li H
, Li H ![]() , Zhao J
, Zhao J ![]() , Wang H, Fu S, Chen J, Wang J
, Wang H, Fu S, Chen J, Wang J
Received 20 March 2026
Accepted for publication 5 May 2026
Published 16 June 2026 Volume 2026:21 610906
DOI https://doi.org/10.2147/IJN.S610906
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lijie Grace Zhang
Jieming Zuo,1,* Zhongsong Zhang,2,* Junhao Chen,1,* Keyi Gou,2,* Jingfeng Zhou,2,* Lingxiang Wen,3,* Hairong Wei,1 Xiangyun Li,1 Peiqin Zhan,1 Peng Chen,1 Haihao Li,1 Junxian Zhao,4 Haifeng Wang,1 Shi Fu,1 Jian Chen,1 Jiansong Wang1
1Department of Urology, The Second Affiliated Hospital of Kunming Medical University, Kunming, Yunnan Province, 650032, People’s Republic of China; 2School of Clinical Medicine, Chengdu Medical College, Chengdu, Sichuan Province, 610550, People’s Republic of China; 3School of Clinical Medicine, Kunming Medical University, Kunming, Yunnan Province, 650032, People’s Republic of China; 4Department of Urology, 920th Hospital of Joint Logistics Support Force of Chinese People’s Liberation Army, Kunming, Yunnan, 650032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian Chen; Jiansong Wang, Email [email protected]; [email protected]
Abstract: Kidney stone disease is one of the most common urologic disorders worldwide and imposes a growing clinical and socioeconomic burden because of its rising prevalence, high recurrence rate, and association with chronic kidney injury and systemic metabolic abnormalities. Calcium oxalate (CaOx) stones remain the predominant stone type, and their formation is now recognized as a multistep process involving urinary supersaturation, crystal nucleation and growth, tubular epithelial injury, oxidative stress, inflammation, and crystal retention. Although current management strategies, including dietary modification, pharmacologic prevention, and endourologic interventions, have substantially improved stone clearance, important limitations remain. These include inadequate early detection, suboptimal prevention of recurrence, insufficient targeting of the local renal microenvironment, and procedure-related complications. Recent advances in nanotechnology offer new opportunities to address these unmet needs. Owing to their large specific surface area, tunable physicochemical properties, versatile surface functionalization, and capacity for multimodal integration, nanomaterials have shown considerable promise in metabolic sensing, urinary biomarker detection, targeted drug delivery, modulation of crystal growth, biomimetic renal targeting, and photothermal or photoresponsive lithotripsy. In parallel, the convergence of nanotechnology with artificial intelligence, smart diagnostic devices, and personalized metabolic profiling is reshaping kidney stone management. This shift is moving the field from passive stone removal toward active risk prediction, dynamic monitoring, and precision prevention. In this review, we summarize recent advances in nanomaterial-based strategies for the diagnosis, treatment, and prevention of kidney stones, with particular emphasis on CaOx disease. We also discuss the major translational barriers, including biocompatibility, long-term safety, regulatory complexity, scalable manufacturing, and cost-effectiveness, and outline future directions for clinically integrated, intelligent, and individualized stone care.
Keywords: kidney stone, calcium oxalate, nanomaterials, nanomedicine, early diagnosis, targeted drug delivery, recurrence prevention, precision medicine
Introduction
Kidney stone disease is among the most common disorders affecting the kidney and urinary tract and represents a growing global health challenge.1,2 Recent epidemiologic analyses indicate that the burden of urolithiasis has increased substantially over the past decades across regions and demographic groups, with global prevalence estimates commonly ranging from approximately 5% to 15%, and a recent meta-analysis reporting an overall pooled prevalence of 10.85%.2–5 In the United States, kidney stone disease affects nearly 1 in 11 individuals, and relevant data have shown a marked increase in prevalence over time. Recurrence remains a defining feature of the disease: guideline-level evidence indicates that at least 50% of patients may experience another stone within 10 years of the first episode, while the European Association of Urology reports a recurrence rate of 26% within 5 years for first-time stone formers and notes that highly recurrent disease occurs in slightly more than 10% of patients.6–8 Kidney stones are also heterogeneous in composition. Calcium-containing stones, especially calcium oxalate and calcium phosphate, account for approximately 70%–80% of cases, whereas uric acid, struvite (infection-related), and cystine stones represent smaller but clinically important subtypes, each associated with distinct metabolic, infectious, or genetic mechanisms.9,10 Calcium oxalate stones are the most prevalent subtype and are typically driven by hypercalciuria, hyperoxaluria, hypocitraturia, and low urine volume, but their clinical behavior is not explained by urinary chemistry alone.11,12 Increasing evidence supports a multistep pathogenic model in which urinary supersaturation interacts with tubular epithelial injury, oxidative stress, inflammatory amplification, and crystal retention, thereby making kidney stone disease a complex metabolic and microenvironmental disorder rather than a simple precipitation event.13,14
Current management strategies remain effective yet incomplete. Dietary modification, high fluid intake, and selected pharmacologic interventions can reduce recurrence in appropriate patients, as reaffirmed by guideline statements and a recent systematic review of recurrent nephrolithiasis prevention.11,14,15 However, the real-world effectiveness of these strategies is often constrained by heterogeneous metabolic phenotypes, treatment burden, adverse effects, and suboptimal adherence; notably, one adherence study found that only about half of patients prescribed long-term chemopreventive therapy remained adherent. Surgical and endourologic advances have substantially improved stone clearance, but surgery does not eliminate the underlying propensity to recur.16,17 Moreover, residual fragments remain after an estimated 30% to 65% of procedures in some settings and may contribute to subsequent relapse, infection, stone regrowth, and ongoing patient morbidity.18,19 Accordingly, current care pathways are strong in acute stone removal but still limited in early risk detection, durable recurrence prevention, and direct modulation of the local renal microenvironment that promotes crystal retention and injury. These limitations underscore the need for new approaches that can enable earlier diagnosis, more precise local intervention, and individualized prevention.16,20
Nanomaterials offer a compelling framework to address these unmet needs. Their high specific surface area, tunable size and morphology, modifiable surface chemistry, and capacity for integrating sensing, targeting, imaging, and therapy make them highly suited to a disease characterized by multiscale interactions between urinary metabolites, crystals, renal epithelial cells, and inflammatory mediators.21–24 Recent studies suggest that nanomaterial-based platforms may support several clinically relevant functions in kidney stone disease, including urinary biochemical sensing, kidney-targeted drug delivery, antioxidant and anti-inflammatory mitigation of crystal-associated injury, biomimetic intervention, and photoresponsive stone fragmentation.25–27 Rather than serving as a purely conceptual innovation, nanotechnology is increasingly being explored as a translational platform that could bridge molecular detection, local therapy, and dynamic disease monitoring when aligned with pathophysiology and clinical workflow.21,28,29 At the same time, the future of kidney stone management is likely to be defined not by nanotechnology alone, but by its integration with artificial intelligence, smart diagnostics, and individualized metabolic profiling.30,31 A recent systematic review showed that AI is already being applied across stone detection, composition prediction, treatment planning, and recurrence forecasting, indicating that the field is moving toward a more predictive and personalized model of care.30 Against this background, nanotechnology may serve as the interfacial layer that links molecular detection, local treatment, and dynamic monitoring, thereby enabling a transition from passive stone removal to active and precision-based stone prevention.21,30,31
In this review, we summarize recent advances in nanomaterial-based strategies for the early diagnosis, targeted treatment, and recurrence prevention of kidney stone disease, with particular emphasis on calcium oxalate-related pathology. We also discuss the major barriers to clinical translation, including biocompatibility, long-term safety, regulatory complexity, manufacturing scalability, and cost-effectiveness, and highlight future trends involving intelligent diagnostics, AI-assisted risk stratification, and personalized therapeutic design. This review aims to provide a more evidence-grounded framework for the future treatment and prevention of nephrolithiasis.
Overview of Nanomaterials in the Mechanisms of Kidney Stone Formation
Nanomaterials and the Mechanisms of Stone Formation
Kidney stones, particularly calcium oxalate (CaOx) stones, are prevalent disorders of the urinary system.32 Their formation involves complex mechanisms and multiple contributing factors.32,33 Recent studies have gradually elucidated the role of nanomaterials in stone formation, particularly highlighting how nano-calcium and nano-hydroxyapatite influence stone nucleation, aggregation, and dissolution. The physicochemical properties of nanoparticles, including particle size, surface charge, and solubility, significantly affect kidney stone formation.27,34,35 Although these mechanisms are complex, understanding the application of nanomaterials in kidney stones is crucial.
Current evidence indicates that kidney stone formation is not merely a consequence of macroscopic crystal deposition. Instead, it represents a pathological biomineralization process involving nanoscale crystal nuclei, interfacial energy, surface charge, and cellular injury. Therefore, examining stone formation from a nanomaterial perspective not only clarifies the critical transition from Randall’s plaque to CaOx epitaxial growth but also informs the design of subsequent diagnostic, preventive, and interventional materials.36–38 In a nanoscale analysis of early human renal papillae affected by Randall’s plaque, Gay et al demonstrated that the plaque constitutes an interfacial structure composed of biologically deposited hydroxyapatite nanoparticles and an organic matrix. This finding suggests that nano-hydroxyapatite is not merely a passive component, but may also act as a precursor platform for subsequent CaOx heterogeneous nucleation.36 This interpretation is consistent with Khan’s summary of the pathological biomineralization of Randall’s plaque, which indicates that once subepithelial hydroxyapatite deposits are exposed to urine, they can adsorb urinary proteins, ions, and microcrystals through surface-active sites, thereby facilitating CaOx nucleation, aggregation, and anchored growth.39 In addition, direct material-science evidence arises from studies examining the size-dependent effects of nano-hydroxyapatite (nano-HAP). For instance, Han et al compared HAP crystals of 40 nm, 70 nm, 1 μm, and 2 μm in an HK-2 cell model. They reported that nano-HAP exhibits higher specific surface area, elevated surface energy, lower contact angle, and reduced zeta potential, facilitating adhesion to and internalization by renal tubular epithelial cells. These properties lead to upregulation of osteopontin and hyaluronic acid, disruption of lysosomal integrity, and induction of apoptosis or necrosis, ultimately conferring a stronger pro-lithogenic potential than micrometer-sized HAP.40 These findings indicate that particle size not only defines the physical dimensions of a particle, but also modulates the thermodynamic and kinetic behavior at the particle-cell interface. Smaller particles provide a larger reactive surface area per unit mass, contain more surface defects and uncoordinated ions, exhibit stronger adsorption of Ca2+, PO4 3−, oxalate, and urinary proteins, and more readily amplify epithelial damage through endocytosis and lysosomal stress. Adhesion molecules exposed on the damaged cell membrane subsequently serve as high-affinity sites for CaOx adhesion and retention, thereby establishing a positive feedback loop of nanocrystal-cell damage-crystal retention.40
Similar size-dependent effects have been observed for CaOx itself. Kumar et al reported a significant increase in CaOx nanocrystals in morning urine and post-dietary oxalate loading in human urine, suggesting that these nanocrystals are not in vitro artifacts but represent early structural units present in the preclinical stone microenvironment.37,38 Furthermore, Chen et al demonstrated that small COMs, ranging from 100 nm to 3 μm, are more readily internalized by HK-2 cells, inducing enhanced oxidative stress, NLRP3 inflammasome activation, and pyroptosis.41 Tong et al reported that COMs of varying sizes differentially affect macrophage pyroptosis and M1/M2 polarization, indicating that nano- and micron-scale CaOx crystals modulate the inflammatory microenvironment via either endocytosis-dominant or adhesion-dominant pathways, which is critical for understanding stone recurrence and local immune remodeling.42 Mechanistically, nanoparticle-mediated promotion or inhibition of stone formation depends on surface charge, particle size, surface functional groups, crystalline phase, and solubility. On one hand, nano-CaP/HAP particles with suitable negative charges or exposed Ca/P active sites can act as heterogeneous nucleation cores, lowering nucleation energy barriers and promoting preferential crystal growth through adsorption of Ca2⁺, oxalate ions, and urinary proteins.36,40,43 Conversely, if nanomaterials can competitively complex Ca2+ or oxalate ions, alter the step energy of the crystal surface, or enhance local solubility, stone-promoting materials may be converted into stone-resistant materials.44,45 The CIT-PAH supramolecular nanoparticles developed by Di Gianvincenzo et al exemplify this concept. The system simultaneously delivers citric acid and exploits the strong interaction between PAH and oxalate to disassemble CaOx nanocrystals. The dissolution of CaOx crystal structures is observed in both aqueous solution and artificial urine, demonstrating that nanomaterials can directly facilitate the breakdown of precursor nanocrystals via ion exchange and interfacial complexation.45 Biomimetic polyphosphate and phosphonic acid molecules recently proposed by Kim et al further demonstrate that mimicking the phosphorylation-related surface chemistry of natural anti-crystallization proteins can markedly inhibit CaOx nucleation and irreversibly block crystal growth, thereby providing a precise theoretical framework for designing anti-stone nanomaterials with tailored surface functionalities.44
At the same time, microbial and biological surfaces can function as specialized soft nano-interfaces. Noonin et al demonstrated that the urinary symbiont L. acidophilus inhibits CaOx crystallization, growth, aggregation, and cell adhesion, whereas E. coli promotes crystal growth and aggregation. This contrasting effect appears to arise primarily from surface S-layer proteins and flagellar components rather than from oxalate-degradation activity.46 Agudelo et al further showed in both mouse and human kidney tissues that the renal microbiota and its surface molecular environment, modulated by antibiotics, can influence the incorporation of CaOx crystallization inhibitors or promoters. This finding extends the concept of nano-micro interfacial regulation of stone formation to the level of the native renal niche in clinically relevant contexts.47
Effects of Nanomaterials on Renal Cells
The potential of nanomaterials in kidney stone research lies in monitoring and intervening in early crystal events. Their clinical translation depends less on inhibiting crystal growth and more on whether interactions with renal cells, particularly tubular epithelial cells, are controllable, reversible, and safe.40,48,49 During kidney stone formation, renal tubular epithelial cells serve not only as the initial biological interface for nanocrystals, but also as a pathological switch that governs crystal retention, inflammation amplification, and progression into stable stone cores. Therefore, assessing the adsorption, endocytosis, subcellular trafficking, and secondary cytotoxicity of nanomaterials in these cells is essential to define safe parameters for anti-stone nanomaterial strategies.48 Early studies indicate that crystal adhesion to renal epithelium is critical in stone formation. Damaged epithelial surfaces expose anionic groups and adhesion molecules that facilitate crystal binding, converting cells from a barrier into a stone-promoting substrate.27 Recent studies under this framework demonstrate that nanoscale crystals and engineered nanomaterials are not inert particles. They actively modulate the damage profile and crystalline phenotype of renal tubular epithelial cells, influenced by particle size, morphology, surface charge, and dispersion state.34,40,48,49
Using nano-hydroxyapatite (HAP) as an example, Sun et al compared particles of 40 nm, 70 nm, 1 μm, and 2 μm in HK-2 cells and found size-dependent cytotoxicity. HAP reduced cell viability, disrupted membrane integrity, increased ROS and intracellular Ca2+, decreased mitochondrial membrane potential, and induced cell cycle arrest and necrosis, with stronger effects observed for smaller particles. Flow cytometry further showed that particle uptake positively correlated with toxicity: 40 nm HAP was internalized most efficiently, whereas 2 μm particles showed minimal uptake, indicating that nanoscale size promotes cellular entry and enhances pro-lithogenic toxicity.48 For example, Han et al, using a pathology-relevant model, found that 40 nm and 70 nm nano-HAP adhered more readily to HK-2 cell surfaces than micro-sized HAP and were more efficiently internalized and concentrated in lysosomes.40 They also increased expression of osteopontin and hyaluronic acid, caused lysosomal damage, and promoted cell death, indicating that the high surface area and surface energy of nano-HAP amplify both surface adsorption and intracellular damage.40 From a materials science perspective, smaller particle sizes provide larger reaction interfaces per unit mass and more surface defects and uncoordinated ions, facilitating adsorption of Ca2⁺, oxalate, and urinary proteins. These particles also enter cells via clathrin-dependent or phagocytic pathways, subsequently inducing local ion imbalance and membrane instability in lysosomes, converting particle stimulation into organelle damage.40,48 Furthermore, Rao et al also reported that HAP particle morphology, aspect ratio, and aggregation state influence cell toxicity. Enhanced toxicity is typically associated with increased ROS, decreased mitochondrial membrane potential, lysosomal damage, and G0/G1 arrest, suggesting that cell entry, lysosomal retention, and oxidative stress are central mechanisms of nanocrystal-induced renal epithelial injury.34
The effects of nanomaterials on kidney cells extend beyond direct toxicity; they can also modulate intracellular inflammatory signaling and intercellular communication networks. Li et al reported that extracellular vesicles (EVs) derived from human umbilical cord mesenchymal stem cells are primarily 30–100 nm in diameter. These EVs are internalized by HK-2 cells, reducing LDH, H2O2, MDA, and ROS in an oxidative-COM injury model while inhibiting TGF-β/Smad-mediated EMT changes. This suggests that specific natural nanovesicles do not worsen epithelial damage but can restore epithelial phenotype after oxidative injury by delivering regulatory factors.50 In contrast, Yuan et al found that CaOx exposure induces endoplasmic reticulum stress and lysosomal dysfunction in macrophages, resulting in the release of GRP94-enriched extracellular vesicles. These vesicles are internalized by renal tubular cells, promoting tubular injury and ultimately enhancing CaOx deposition in mouse kidneys.51 This implies that nanoscale extracellular vesicles can function both as protective carriers and as amplifiers of inflammation and crystal deposition within the stone microenvironment.51 This finding broadens nanomaterial safety assessment from single-particle toxicity to intercellular nanoinformation transmission, where even materials with limited direct toxicity may indirectly influence stone formation by modulating nanovesicle secretion from macrophages, epithelial cells, or fibroblasts.50,51 Tong et al further demonstrated that COM crystals of varying sizes differentially affect macrophage pyroptosis and polarization, indicating that nano- and micro-scale crystals can modulate the renal tubular injury environment via immune cell reprogramming. This provides key insights into the interplay among cytotoxicity, inflammation, and crystal retention.42
 |
Figure 1 Structural characterization and proposed renoprotective effect of CNPs. (A) Schematic diagram illustrating the ability of porous nanorod CNPs to inhibit renal calcium oxalate crystal deposition through mitigation of hyperoxaluria-associated oxidative stress. (B–D) TEM, high-resolution TEM, and SEM images of CNPs. (E) STEM-EDS elemental mapping images of CNPs. (F and G) XPS survey spectrum and high-resolution Ce 3d spectra of CNPs. (H) XRD pattern of CNPs compared with the standard CeO2 card. Adapted from,52 Copyright © 2022 by authors. |
Notably, nanomaterials are not inherently harmful to renal tubular cells. Increasing evidence indicates that appropriately designed nanomaterials can mitigate epithelial damage via antioxidant, anti-inflammatory, and targeted delivery mechanisms, thereby exerting indirect anti-stone effects. The CeO2 nanoenzyme developed by Deng et al exhibited strong ROS scavenging in a high-oxalate injury model, downregulated cell-surface adhesion proteins, alleviated renal tubular pathology, and significantly reduced renal CaOx deposition in an ethylene glycol-induced rat model, without notable systemic toxicity (Figure 1).52 Tian et al further reported that the MOF-818 nanozyme alleviates oxalate-induced oxidative stress, decreases IL-6, TNF-α, and adhesion molecule expression, and promotes macrophage polarization from M1 to M2. In animal models, it concurrently reduces crystal deposition and inflammatory damage, suggesting that antioxidant activity and immune remodeling are key dual mechanisms by which nanomaterials protect renal epithelium.53 Meanwhile, Biomimetic CeO2/TAK-242 nanoparticles developed by He et al further improve targeting to damaged kidney tissue. In a glyoxalate-induced mouse model, they inhibit the TLR4/NF-κB pathway, reduce oxidative stress and M1 polarization, and decrease crystal deposition, indicating that surface biomimicry not only enhances delivery efficiency but also improves safety by reducing nonspecific uptake and enhancing biocompatibility.54
In other words, nanomaterials exert a double-edged effect on renal tubular cells. Unregulated or highly reactive particles may aggravate injury through adsorption, endocytosis, and lysosomal accumulation, whereas surface-modified, morphology-optimized, and functionally loaded nanosystems can achieve protective delivery via the same entry routes.40,48,52,53 Clinically, this has two implications. First, nanomaterials for kidney stone therapy should not be judged solely by crystal suppression, but also by their effects on adhesion, endocytosis, subcellular localization, ROS production, mitochondrial injury, lysosomal stability, cytokine release, and crystal attachment in renal tubular cells; otherwise, materials that inhibit crystals in vitro may still promote stone formation in vivo.34,40,48 Second, safety evaluation should go beyond conventional viability assays to include disease-relevant indicators such as OPN/CD44/VCAM-1 expression, PS exposure, EMT markers, pyroptosis and ferroptosis pathways, macrophage polarization, and renal KIM-1, LCN-2, PAS/Von Kossa staining, as well as organ distribution in animal models, to determine whether a nanomaterial is both crystal-effective and kidney-compatible.50,52,55 Therefore, the key conclusion is that the renal cellular response to nanomaterials is central to their application in kidney stone prevention and treatment. Only materials that inhibit crystal formation while preventing or reversing oxidative stress, inflammatory activation, and renal tubular epithelial remodeling can be considered biocompatible and clinically translatable.53,54
Interaction Between Cells and Stones
From the perspective of pathological biomineralization, kidney stones are not inert byproducts that form passively after urinary supersaturation. Instead, they are selectively retained, amplified, and stabilized through dynamic interactions involving continuous contact, adhesion, endocytosis, and re-release between crystals and renal tubular epithelial cells. Therefore, nanoscale interactions at the cell–stone interface determine whether crystals are cleared or develop into stable stone cores.56–58
Classic studies have demonstrated that COM crystals rapidly bind to the microvilli of renal epithelial cells within minutes, are internalized, and subsequently transported to lysosomes for degradation. This indicates that adhesion and endocytosis are not incidental events but fundamental programs by which renal tubular cells process crystals.56,57 Recent research further shows that imbalance in this process—caused by oxidative stress, membrane damage, or altered material interface properties—shifts protective crystal clearance toward pro-lithogenic crystal retention.41,58 Petrović et al summarized CaOx–renal epithelial interactions, noting that cell-surface anionic sites, the glycosaminoglycan layer, phospholipid exposure, and adhesion molecules such as OPN, CD44, and hyaluronic acid collectively govern stable crystal adhesion. Cell damage and consequent rearrangement of these sites markedly enhance crystal retention, facilitating subsequent aggregation and epitaxial growth.58 Nanoscale properties further amplify these cell–stone interface effects. Chen et al reported that in COM models, small crystals (100 nm, 1 μm, 3 μm) are efficiently internalized by HK-2 cells, elevating intracellular ROS and activating NLRP3 inflammasomes and pyroptosis, whereas larger crystals (5–10 μm) predominantly remain extracellular.41 This suggests that particle size not only governs crystal internalization but also influences whether crystals induce mechanical adhesion and membrane damage or trigger stronger inflammatory cascades via lysosomal and mitochondrial stress.41
Consistently, Han et al demonstrated that nano-HAP exhibits stronger adhesion and internalization than micrometer-sized particles. Internalized particles primarily accumulate in lysosomes. The observed pattern of stronger adhesion, greater internalization, and higher toxicity indicates that nanocrystals with higher surface activity and larger specific surface area form more robust interactions at the cell interface.40 Collectively, these results support the view that interactions between stone particles and cells are not mere collisions but interface recognition processes regulated by particle size, surface charge, morphology, and cell damage status.40,41,58 Mechanistically, crystals must first establish an initial anchor on the cell surface before internalization or retention along enlarged branches. Lieske et al demonstrated that COM selectively binds to renal epithelial cells and that this binding is modulated by growth factors and cell activation status, indicating that cells actively regulate membrane transport and cytoskeletal remodeling rather than passively accepting crystal adhesion.56,57 Subsequent studies show that outward rotation of phosphatidylserine, brush edge disruption, and upregulation of adhesion proteins on damaged cell surfaces significantly enhance nanocOM adhesion. Conversely, repair of oxidative damage reduces surface retention while increasing internalization and lysosomal transport. Increased surface adhesion often indicates a higher risk of stone formation, whereas moderate internalization and clearance reflect a protective response.59–62 For instance, Li et al confirmed in a 100 nm COM model that damaged HK-2 cells have reduced endocytosis of nano-COM. Following tea polysaccharide treatment, crystal internalization increased and particles localized primarily to lysosomes, suggesting that restoring normal endocytic and lysosomal pathways is critical to inhibit crystal nucleation and aggregation.59 Zhao et al further demonstrated that moderately sized tea polysaccharides most effectively protect damaged cells and reduce nanocOM adhesion to cell surfaces. These findings indicate that the molecular weight and chain conformation of materials influence their capacity to repair membranes, mask adhesion sites, and modulate crystal–cell interfaces.60 Notably, subtle alterations in material structure can substantially change the nature of interactions between crystals and renal cells. Xiong et al reported that carboxymethylated polysaccharides significantly improved HK-2 cell viability following oxalate injury, decreasing adhesion to nano-COM and enhancing endocytosis. Internalized crystals primarily accumulate in lysosomes, suggesting that COOH groups enhance antioxidant and membrane-repair properties and may shift the adhesion–endocytosis balance by modulating cell surface charge and crystal interface hydration.61 Wang et al demonstrated in a Desmodium styracifolium polysaccharide model that carboxymethylation reduces CaOx stone risk by inhibiting crystal adhesion and promoting endocytosis. This effect is closely associated with the degree of substitution and functional group density, highlighting that structural optimization produces measurable functional differences at the crystal–cell interface.62 Similarly, Xu et al and He et al found that increasing sulfate group content in brown algae– or kelp-derived polysaccharides enhances both repair of damaged HK-2 cells and inhibition of nano-COM/COD adhesion.63,64 These findings suggest that increased negative charge density and hydrophilicity weaken direct crystal–cell membrane contact and reduce adhesion-promoting phenotypes by alleviating oxidative and ER stress.63,64 Moreover, Chen et al demonstrated that sulfated Undaria pinnatifida polysaccharides promote cellular endocytosis of nano-COD while mitigating mitochondrial and lysosomal damage. This indicates that structurally optimized biomaterials not only prevent crystals from contacting cells but also direct them toward intracellular pathways favoring degradation and clearance (Figure 2).65
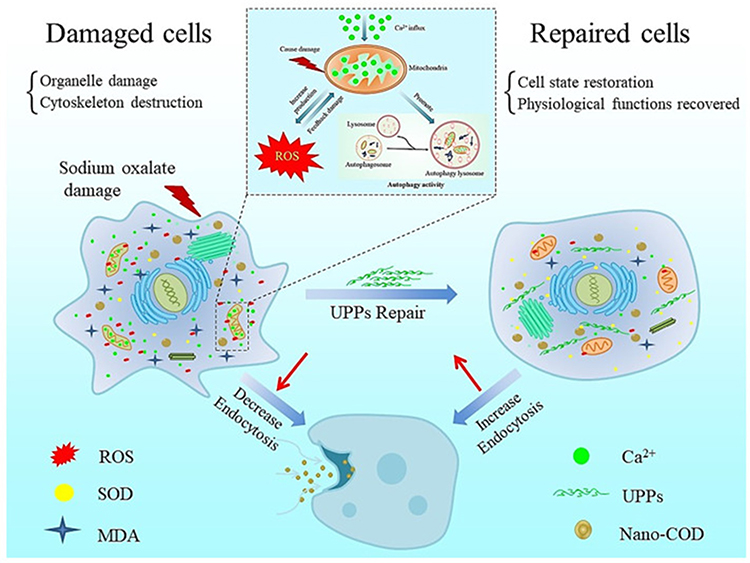 |
Figure 2 Proposed mechanism by which UPPs promote the endocytosis of nano-COD crystals after repair of oxalate-induced oxidative injury in HK-2 cells. Sodium oxalate-induced injury increases intracellular ROS generation, disrupts organelles and cytoskeletal structure, and impairs the normal physiological state of HK-2 cells, thereby decreasing endocytosis of nano-COD crystals. UPP treatment alleviates oxidative stress-related damage, restores mitochondrial and lysosomal function, promotes autophagy-related processing, and improves overall cellular status. As a result, damaged cells are repaired, crystal adhesion is reduced, and endocytosis of nano-COD is enhanced, facilitating intracellular trafficking and clearance. Red arrows indicate changes in cellular injury and repair, and blue arrows indicate the decrease or increase in crystal endocytosis before and after UPP treatment. Adapted from,65 Copyright © 2023 by authors. Abbreviations: ROS, reactive oxygen species; SOD, superoxide dismutase; MDA, malondialdehyde; UPPs, sulfated Undaria pinnatifida polysaccharides; nano-COD, nano-calcium oxalate dihydrate. |
Beyond chemical modification, crystal morphology itself also influences the strength of cell–crystal interactions. COD/COM crystals with larger faces, sharp edges, or elongated bipyramidal shapes induce greater membrane damage in HK-2 cells and increase effective contact area, thereby enhancing adhesion and toxicity.66,67 This suggests that regulating crystallization via nanomaterials to produce smoother, less aggregated crystals with lower surface activity may have greater therapeutic value than merely reducing crystal quantity.66,67 Liu et al showed that polysaccharide-regulated CaOx crystals exhibit improved antioxidant activity and cell compatibility, demonstrating that crystal engineering, through modulation of morphology, aggregation, and surface chemistry, reduces crystal affinity and cytotoxicity toward renal epithelium.68 Notably, external environmental nanoparticles may amplify crystal–cell interactions. Recent studies indicate that polystyrene nanoplastics promote CaOx nucleation, enhance crystal adhesion to renal tubular epithelium, and amplify inflammation and ferroptosis.69 This highlights that not all nanoparticles are therapeutically beneficial; some environmental nanoparticles may act as lithogenic cofactors by providing heterogeneous nucleation sites and disrupting membrane receptor signaling.69
Therefore, treatment design should optimize nanomaterial-cell-stone interactions according to three principles. First, material surfaces should avoid generating new adhesion-promoting cores and instead reduce direct crystal-membrane adhesion by increasing hydrophilicity, moderately enhancing negative charge density, introducing carboxyl, sulfate, or phosphonic acid groups, and competitively shielding Ca2+ or active crystal sites.61,62,64 Second, ideal materials should not only prevent crystal-cell contact but also repair damaged epithelium, thereby restoring normal endocytosis and lysosomal processing so that contacting nanocrystals are cleared rather than continuing to nucleate and aggregate on the cell surface61,62,64,65 Third, structural optimization must be evaluated together with biosafety. Effects on cell viability, ROS, mitochondrial membrane potential, lysosomal integrity, inflammatory markers, OPN/CD44 expression, crystal deposition, and renal pathology in animals should all be assessed, because anti-adhesion alone is insufficient to support translational potential.40,41,69 Ultimately, cell-stone interactions are central to the design of anti-stone nanomaterials. The full therapeutic potential of nanotechnology in kidney stone treatment can be realized only when materials shift the crystal-cell interface from a high-adhesion, low-clearance, pro-inflammatory state to a low-adhesion, endocytic, degradable, and low-damage protective state.68,69
The Application of Nanomaterials in the Treatment of Kidney Stones
Design and Application of Nanodrug Delivery System
Compared with therapies for tumors or infectious diseases, pharmacological treatment of kidney stones has long faced a less visible but critical bottleneck. Many bioactive molecules with antioxidant, anti-inflammatory, crystal-inhibitory, or crystal-clearing potential are limited by poor water solubility, short circulation time, insufficient renal exposure, brief retention at the lesion site, and systemic adverse effects. As a result, these agents often fail to maintain effective concentrations during the critical window of stone formation. This limitation provides the fundamental theoretical rationale for applying nanodrug delivery systems in kidney stone therapy. In kidney stone disease, nanodrug delivery may be achieved through systemic vascular transport, nephron-oriented renal access after glomerular filtration or peritubular capillary transport, or local urinary tract administration through catheter- or endoscopy-assisted approaches, with route selection depending on the intended site of action and therapeutic objective (Table 1 and Figure 3).27,70,71
 |
Figure 3 Overview of nanomaterial-based delivery systems relevant to kidney stone therapy. Schematic summary of the major delivery platforms discussed in this review, including lipid-based nanoparticles, natural and synthetic polymeric nanoparticles, dendrimers, protein-based nanoparticles, carbon nanotubes, metallic and silica nanoparticles, exosomes, hyaluronic acid-based systems, biomimetic nanoparticles, cell membrane-cloaked nanoparticles, and stimulus-responsive intelligent nanomaterials (IMNs). These platforms can be broadly interpreted according to key translational properties such as biodegradability/non-biodegradability and immunoactivity/immunoinactivity, which collectively influence their pharmacokinetics, biosafety, renal compatibility, and therapeutic applicability. In the context of kidney stone disease, such delivery systems provide diverse design options for improving drug solubility, prolonging circulation, enhancing kidney or lesion-specific accumulation, enabling stimulus-responsive release, and integrating microenvironment modulation with stone-directed intervention. As summarized in The Application of Nanomaterials in the Treatment of Kidney Stones, the therapeutic value of these systems lies not only in drug transport itself, but also in their potential to support renal targeting, oxidative stress reduction, anti-inflammatory treatment, crystal-growth interference, and multimodal intervention in stone-associated injury. Adapted from,72 Copyright © 2025 by authors. |
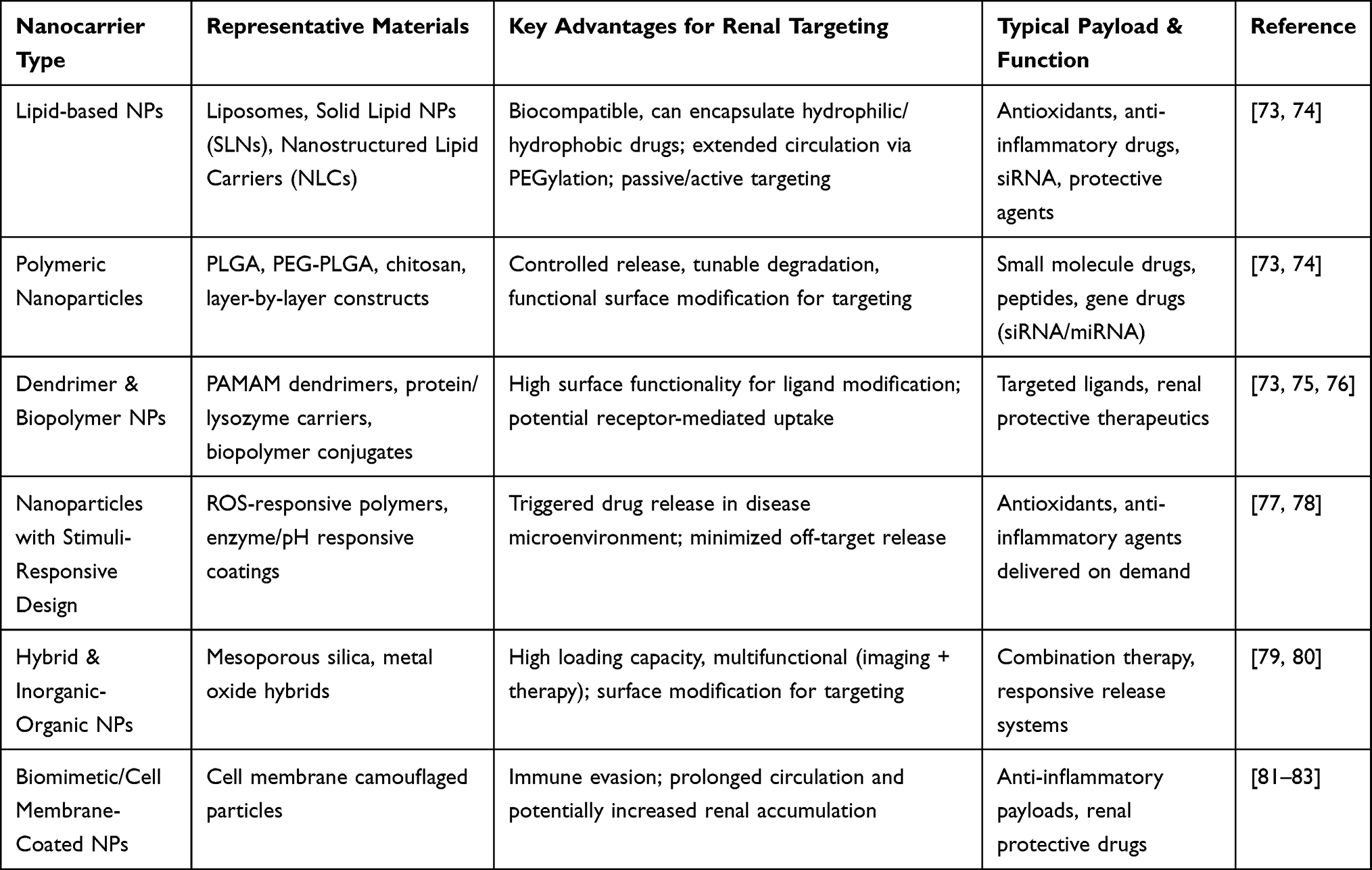 |
Table 1 Overview of Nanocarrier Platforms for Kidney Targeting and Drug Delivery |
Studies on nanodelivery systems for kidney diseases have shown that carriers such as liposomes, solid lipid nanoparticles, polymeric nanoparticles, dendrimers, mesoporous silica nanoparticles, biomimetic membrane-coated nanoparticles, and exosome-like vesicles can substantially improve therapeutic efficacy. These benefits arise from enhanced drug solubility, reduced premature clearance, prolonged half-life, protection of unstable drugs or nucleic acid cargoes, and improved local renal accumulation through passive or active targeting.70,71,73,74 Because the kidney is a highly specialized organ, the design of nanodelivery systems must account for physiological constraints, including the glomerular filtration barrier, proximal tubular reabsorption, and the distribution of renal interstitial blood flow. Accordingly, particle size, surface charge, hydrophilicity, elasticity, and surface ligands determine not only pharmacokinetics but also biodistribution. More specifically, these properties influence whether a carrier reaches the glomerulus or proximal tubules, or is preferentially cleared by the hepatic and splenic systems during circulation.74,84 Vasylaki et al concluded that there is no single optimal size for renal nanodelivery. Instead, carrier design should be defined in reverse according to the target site. Smaller particles are more likely to enter the nephron through filtration, whereas mesoscale polymeric nanoparticles measuring hundreds of nanometers may preferentially accumulate in the tubular epithelium through transcellular transport from the peritubular capillaries. This site-specific design strategy is particularly important for treating stone-related proximal tubular injury.84
Among currently available carrier types, liposomes and other lipid-based nanoparticles are the most clinically established systems because their composition resembles that of biological membranes and confers favorable biocompatibility, biodegradability, and scalable manufacturing potential. In addition, they exhibit strong encapsulation capacity for hydrophobic drugs, bioactive lipids, and nucleic acid payloads.71,74,85 Mechanistically, PEGylated liposomes or liposomes modified with surface ligands can prolong circulation by reducing plasma protein adsorption and reticuloendothelial clearance. In diseased tissues, these systems can further enhance local accumulation through increased inflammation-associated vascular permeability or ligand-receptor recognition.86,87 A representative example of this strategy has been reported in kidney disease. Wu et al developed VCAM-1-targeted celastrol phospholipid nanoparticles (PC-PLNs), which delivered the otherwise highly toxic and poorly soluble drug to injured glomerular endothelial cells and podocytes. This formulation reduced endothelial injury and inflammatory responses in chronic kidney disease models, while also markedly decreasing systemic toxicity.88 This study indicates that lipid nanocarriers in kidney disease serve not merely as passive loading vehicles, but as platforms that redefine the therapeutic window by reshaping tissue distribution.88 This concept is also transferable to kidney stone disease. Oxalate-induced tubular injury and crystal deposition are accompanied by oxidative stress, upregulation of inflammatory adhesion molecules, and disruption of local vascular and epithelial barriers. Therefore, encapsulating antioxidant or anti-inflammatory agents in liposomes and functionalizing them with ligands targeting tubular or injury-associated markers may substantially enhance effective drug exposure at sites of stone-related lesions.27,70,84,88 Broader clinical experience further supports the value of liposomes as a versatile platform. Gabizon et al noted that PEGylated liposomal doxorubicin (PLD) has become a landmark model in nanomedicine. Its key pharmacological contribution lies in demonstrating that prolonged circulation, sustained release, and redistribution across tissues can substantially improve the efficacy-toxicity balance of conventional drugs.89 Although this principle was first established in oncology, it is also relevant to kidney stone therapy.89 More recently, research on lipid nanoparticles has shown that these carriers have become one of the most successful platforms for nucleic acid delivery. The clinical success of mRNA vaccines demonstrates the practical feasibility of lipid nanoparticles for nucleic acid stabilization, membrane translocation, and large-scale manufacturing. This progress provides an important technical foundation for the future delivery of siRNA, miRNA, and anti-inflammatory nucleic acid therapeutics in kidney stone disease.90,91 Interestingly, a recent study by Khabbazian et al reported tetherless, urease-loaded soft magnetic robots for local dissolution of uric acid stones through ultrasound-guided magnetic navigation and sustained urinary basification. Although this mechanism is particularly suited to uric acid stones rather than calcium oxalate stones, the platform itself may still be adaptable to CaOx disease by replacing the urease-based chemolytic strategy with alternative payloads that inhibit crystal growth, destabilize CaOx crystals, or modulate the local renal microenvironment.92
Compared with liposomes, polymeric nanoparticles offer greater structural programmability and functional integration. These features make them particularly suitable for stone therapy, which requires a careful balance among renal localization, stimulus responsiveness, sustained release, and surface functionalization.71,74,84 Materials such as PLGA, chitosan, hyaluronic acid, PVP copolymers, and layer-by-layer self-assembled systems support diverse loading strategies, ranging from small-molecule drugs to siRNA and miRNA.74,93 This versatility arises from the ability to tune molecular weight, charge density, degradation rate, and surface ligands. The HA-KTP-modified layer-by-layer polymeric nanoparticles reported by Gu et al provide an informative example.86 In this system, PLGA serves as the core, whereas chitosan and hyaluronic acid are sequentially incorporated into the outer layers to improve siRNA loading and stability.86 A renal-targeting peptide is then introduced to enhance accumulation in the proximal tubules. This platform ultimately enabled efficient delivery of Arg-2 siRNA, preserved mitochondrial function, and improved renal function in a contrast agent-related acute kidney injury model. These findings suggest that the major strengths of polymeric nanoparticles lie in their hierarchical design and multifunctional integration. These properties are particularly important for the coordinated modulation of oxidative stress, inflammation, and crystal adhesion in stone therapy.93
In addition, polymeric systems are especially well suited for improving the bioavailability of natural products and polyphenolic compounds. A review of acute kidney injury research suggests that chitosan nanoparticles, PAMAM dendrimer-based carriers, and hyaluronic acid-modified nanosystems have been used to enhance the stability and renal distribution of active agents such as the mitochondria-targeted antioxidant peptide SS-31 and rosmarinic acid. Collectively, these studies indicate that polymeric nanoparticle-based delivery may substantially improve the druggability of anti-stone candidate molecules with poor oral bioavailability or insufficient plasma exposure.71,74 A more direct example in kidney stone research is provided by the CIT-PAH supramolecular nanoparticles developed by Di Gianvincenzo et al. This system simultaneously delivers citric acid and strengthens interactions with oxalate groups through a polycationic framework, thereby promoting the dissolution of CaOx nanocrystals in aqueous solution and artificial urine. This finding suggests that nanocarrier systems in kidney stone disease may serve not only to deliver drugs to the kidney, but also to actively regulate ion exchange and crystal stability within the urinary microenvironment.45 In addition to traditional liposomes and polymeric particles, biomimetic nanosystems and inorganic or hybrid nanodelivery platforms have attracted increasing attention in stone therapy in recent years. A major reason is that they can combine delivery capacity with the intrinsic therapeutic activity of the material itself.52,54 The porous rod-shaped CeO2 nanozyme developed by Deng et al functions not merely as a carrier in hyperoxaluria- and CaOx-related models. Rather, the material itself exerts enzyme-like ROS-scavenging activity through reversible Ce3+/Ce4+ conversion. As a result, it reduces HK-2 cell injury, downregulates cell-surface adhesion proteins, and decreases CaOx deposition in rat kidneys, thereby illustrating the nanotherapeutic concept of carrier as drug.52 Building on this concept, He et al further developed ROS-responsive CeO2/TAK-242 biomimetic nanoparticles coated with red blood cell membrane, designated RBCM@CeO2/TAK-242. This design conferred both prolonged circulation and preferential accumulation in injured kidney tissue through membrane biomimicry, while simultaneously enabling TLR4 inhibitor delivery and ROS scavenging. Ultimately, the system suppressed oxidative stress, M1 macrophage polarization, and crystal deposition in a mouse model.54 This design is particularly well suited to the complex pathological cascade of epithelial injury, inflammatory amplification, and crystal adhesion in stone lesions.54 It is also noteworthy that the MOF-818 nanozyme reported by Tian et al alleviates oxidative stress and inflammatory injury while reducing crystal deposition in animal models. This finding highlights the significance of inorganic and metal-organic framework-based nanoplatforms in stone therapy. Their value lies not only in increasing drug-loading capacity, but also in integrating delivery with local pathological microenvironment remodeling through tunable pores, surface coordination sites, and enzyme-like activity.53
From a design perspective, nanodrug delivery systems for kidney stones should satisfy at least four key requirements. First, they should improve bioavailability. For molecules such as citrate derivatives, natural products, antioxidants, and small nucleic acids that are easily degraded, poorly soluble, or rapidly cleared, nanoencapsulation can improve aqueous dispersibility, protect active components, and prolong in vivo exposure.71,84,91,94 Second, they should enhance targeting to both the kidney and the lesion site. Passive accumulation can be promoted by controlling particle size, surface charge, and the degree of PEGylation. Active localization can be further achieved by incorporating VCAM-1, KIM-1, proximal tubule-targeting peptides, or biomimetic cell membranes, thereby increasing drug concentration in injured renal tissue while reducing systemic toxicity.54,84,88,93 Third, they should enable stimulus-responsive and programmed release. Stone-forming sites are typically characterized by elevated ROS levels, inflammation, local pH changes, and high ionic strength. Accordingly, carriers responsive to ROS, pH, or ionic competition can promote preferential drug release within the lesion microenvironment rather than premature release during circulation.53,54 Finally, the intrinsic safety and non-lithogenic properties of the material must be carefully balanced. Because the kidney is both a therapeutic target and a clearance organ, any nanocarrier must avoid acting as a new heterogeneous nucleation interface or causing epithelial injury. This requirement means that surface chemistry, degradation products, long-term accumulation, and effects on the crystal-cell interface must all be systematically evaluated.52,71,84 From the perspective of clinical translation, the most realistic path for kidney stone therapy may not be the immediate development of entirely new specialized nanomedicines. Rather, a more practical strategy is to build on validated carrier platforms already established in kidney disease and other fields, and then adapt their delivery logic to the specific pathology of kidney stones. Liposomal platforms have already demonstrated industrial and regulatory feasibility in oncology and nucleic acid therapeutics.89–91 Polymeric nanoparticles provide directly transferable engineering templates for renal tubular targeting and siRNA delivery.93 In addition, biomimetic membrane-coated systems and nanozyme platforms may offer multimechanistic advantages over single small-molecule agents in the injury-inflammation-crystal deposition process of kidney stone disease.52,54 Therefore, the central argument is that the value of nanomedicine-based delivery systems in kidney stone therapy lies not only in delivering drugs more efficiently, for longer durations, and with greater precision. More importantly, through refined carrier design, these systems can transform conventional pharmacotherapy from an inefficient model of systemic administration with insufficient local exposure into a precise therapeutic paradigm characterized by renal targeting, lesion-responsive release, and multimodal intervention. This shift may represent a key step toward the substantive transformation of traditional kidney stone treatment through nanotechnology.52,54,88,94
Antioxidant Nanozymes in Prevention and Treatment of Kidney Stones
Oxidative stress is a key pathological driver of the formation and progression of calcium oxalate (CaOx) kidney stones. Excessive production of reactive oxygen species (ROS) contributes to renal tubular injury, upregulation of epithelial adhesion molecules, and subsequent crystal retention and aggregation in both cell-based and animal models. Therefore, strategies that efficiently scavenge ROS and restore redox homeostasis may offer therapeutic potential beyond conventional litholytic approaches.27,53,95 In this context, antioxidant nanozymes, including cerium oxide (CeO2) and Prussian blue derivatives, have emerged as promising therapeutic candidates. These nanomaterials possess enzyme-mimicking free radical-scavenging activity and are capable of mitigating oxidative stress, preserving renal epithelial integrity, and ultimately reducing stone burden in vitro and in vivo.
Among the earliest and most extensively studied nanozymes in this field are cerium oxide nanoparticles (CNPs). These nanoparticles exhibit catalase-like and superoxide dismutase-like activity through reversible surface valence cycling between Ce3⁺ and Ce4⁺. This redox mechanism enables the catalytic decomposition of superoxide anions and hydrogen peroxide into less reactive species without substantial degradation or loss of activity.52,96 Building on the success of CeO2 nanozymes, recent studies have expanded the range of antioxidant nanocatalysts to include Prussian blue nanozymes. These systems have been engineered to hitchhike on endogenous neutrophils for targeted delivery to sites of CaOx crystal-induced renal injury. These citrate-coated Prussian blue nanozymes, termed NM@CPBzyme, exert both antioxidant and anti-inflammatory effects by inhibiting pyroptosis and neutrophil extracellular trap (NET) formation. As a result, they alleviate CaOx-induced tubular injury and reduce crystal deposition in murine stone models. Preliminary data further show that NM@CPBzyme treatment significantly reduces oxidative damage markers and renal crystal burden, while concurrently improving histopathological injury scores. These findings underscore the feasibility of integrating targeted delivery with robust ROS scavenging in a single therapeutic platform (Figure 4).95 In addition to discrete nanozyme formulations, hybrid materials such as MOF-based catalysts have also shown strong antioxidant potential under CaOx challenge conditions. A recent example is the MOF-818 nanozyme, which significantly suppressed CaOx stone deposition in vivo by alleviating oxidative stress and inflammatory injury in renal tissues. Its activity derives from the combination of high surface area and tailored catalytic sites, which efficiently neutralize free radicals in situ and thereby reduce both cellular oxidative damage and downstream pro-stone pathways.53 Collectively, these studies highlight a recurring mechanistic theme. By continuously decomposing excess ROS, antioxidant nanozymes not only protect renal cells from oxidative injury, but also indirectly downregulate pro-adhesive and pro-inflammatory signaling pathways that would otherwise promote stone nucleation and retention.27,53,95 From the perspective of clinical translation, antioxidant nanozyme-based therapy offers several practical advantages. First, the intrinsic catalytic activity of nanomaterials such as CNPs and Prussian blue nanozymes reduces the need for repeated high-dose administration of small-molecule antioxidants, which often suffer from poor renal targeting and rapid systemic clearance. The catalytic turnover of nanozymes enables sustained ROS mitigation at lower effective doses and with reduced systemic exposure.52,97 Second, nanozyme platforms can be further functionalized with targeting ligands or delivered via endogenous cell carriers such as neutrophils. This strategy enhances delivery to injured renal microenvironments, where oxidative stress is most pronounced, thereby increasing local therapeutic efficacy while reducing off-target effects.95 Finally, favorable safety profiles in rodent models provide encouraging support for further preclinical development and eventual clinical trials. This conclusion is supported by unchanged serum biochemical markers and the absence of histological damage in major organs at therapeutic doses.95
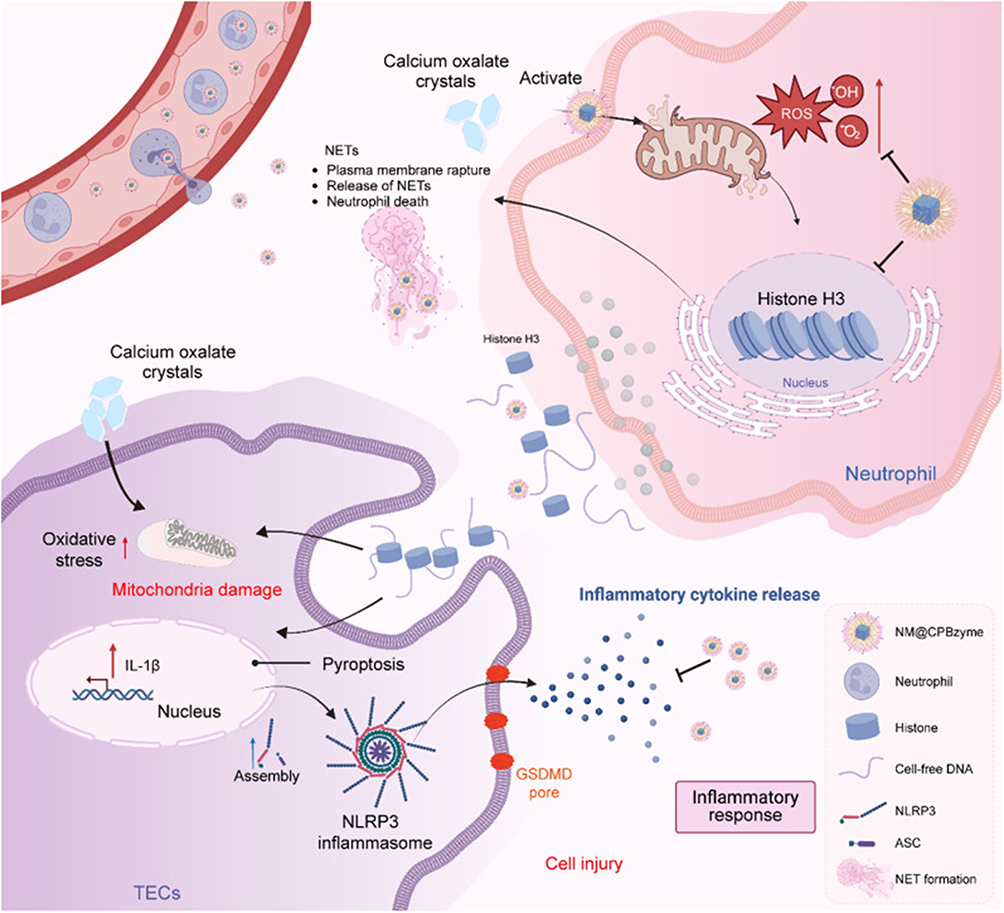 |
Figure 4 Schematic illustration of the mechanism by which NM@CPBzyme ameliorates CaOx crystal-induced kidney injury. Calcium oxalate (CaOx) crystals activate neutrophils and trigger the formation of neutrophil extracellular traps (NETs), accompanied by plasma membrane rupture, release of extracellular DNA and histones, and neutrophil death. In parallel, CaOx crystals induce oxidative stress and mitochondrial damage in tubular epithelial cells (TECs), thereby promoting NLRP3 inflammasome assembly, gasdermin D (GSDMD) pore formation, pyroptosis, and IL-1β release. These events further amplify inflammatory cytokine secretion and aggravate renal cell injury. NM@CPBzyme suppresses crystal-induced oxidative stress, inhibits NET formation and histone H3 release from neutrophils, attenuates mitochondrial injury and NLRP3 inflammasome activation in TECs, and consequently reduces pyroptosis and inflammatory amplification, ultimately alleviating CaOx crystal-induced kidney injury. Adapted from,95 Copyright © 2026 by authors. |
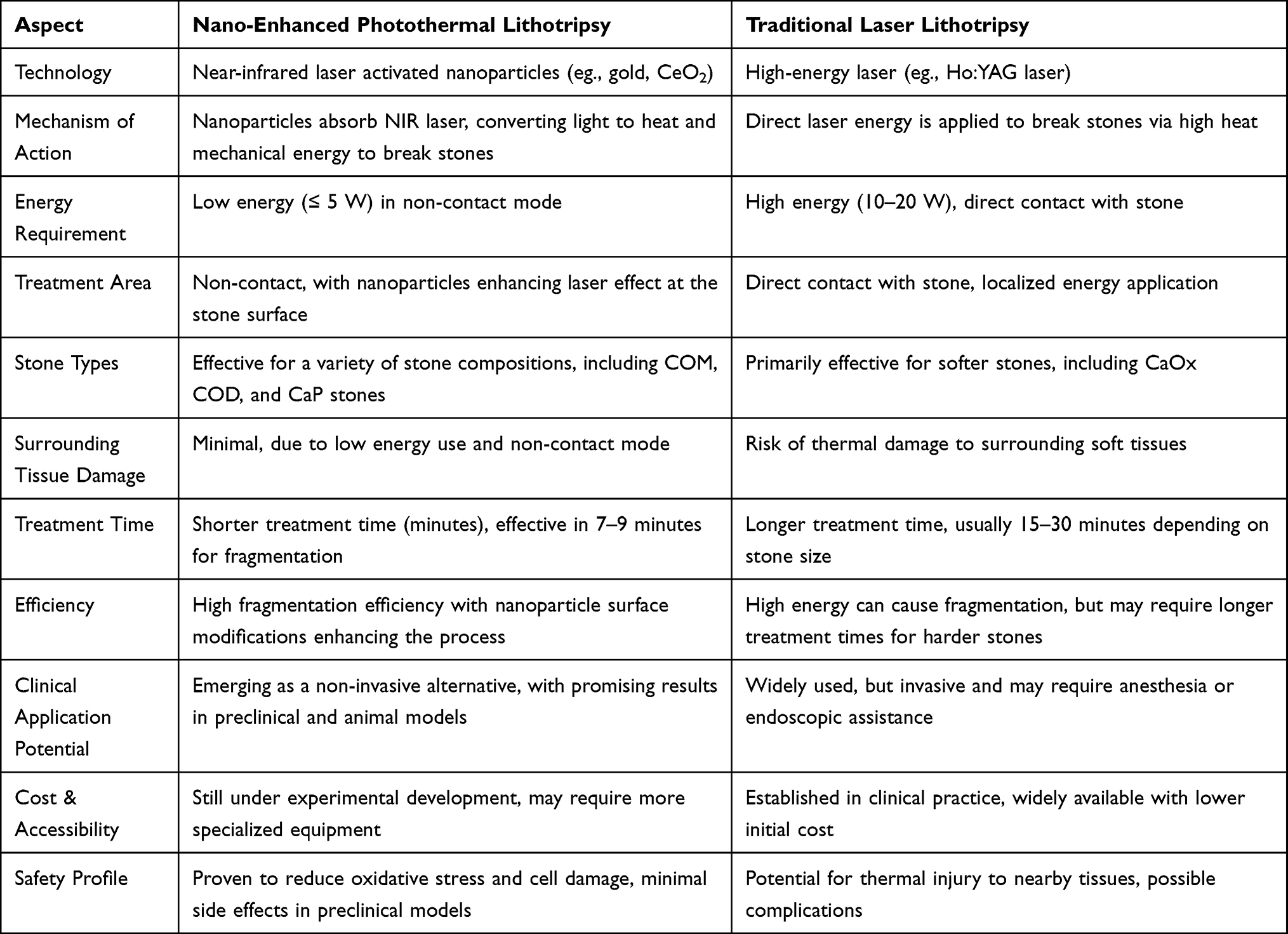 |
Table 2 Comparison Between Nano-Enhanced Photothermal Lithotripsy and Traditional Laser Lithotripsy |
Nanomaterials in Crystal Dissolution and Stone Fragmentation Technology
If conventional stone fragmentation technologies address the problem of how to break existing stones, the major appeal of nano-mediated photothermal and photodynamic strategies lies in their ability to reconstruct energy deposition from whole-tissue exposure to targeted release at the material interface (Table 2).25,98 In principle, this approach may preserve fragmentation efficiency while minimizing thermal injury to the surrounding urinary tract epithelium and renal parenchyma. This concept is particularly relevant in the current clinical era of laser lithotripsy dominated by thulium fiber laser (TFL) systems.99–101 Although these modern platforms have markedly improved lithotripsy efficiency, thermal accumulation, local temperature elevation, and potential urinary tract mucosal injury remain central concerns in the optimization of treatment parameters.100,102–104
At the material level, the rationale of nanothermal platforms is not simply to replace lasers with nanoparticles. Rather, it is to exploit the strong near-infrared absorption, surface plasmon or nonradiative transition behavior, and interfacial thermoacoustic coupling properties of carbon-based, gold-based, or Prussian blue-based nanomaterials. In this way, low-power and non-contact near-infrared irradiation can be converted into localized thermal stress and photoacoustic or mechanical stress at the stone surface. As a result, the fragmentation process shifts from conventional high-energy bulk destruction toward selective destabilization at the stone-particle interface.25,105,106 The most representative experimental evidence for this approach comes from the photonic lithotripsy study by Houlihan et al, published in Nano Letters. In that study, the authors used photonic nanomaterials, including fullerene, carbon nanotubes, graphene, gold nanoshells, and gold nanorods, to coat human kidney stones. Under non-contact excitation with a near-infrared laser operating at less than 5 W and positioned at least 10 mm from the stone surface, common stone types, including calcium oxalate monohydrate, calcium oxalate dihydrate, calcium phosphate, and uric acid stones, were effectively fragmented. These findings indicate that the size, morphology, and optical properties of the nanomaterials directly influence fragmentation efficiency. This low-power, non-contact mode is conceptually distinct from conventional high-power endoscopic laser systems (Figure 5).25
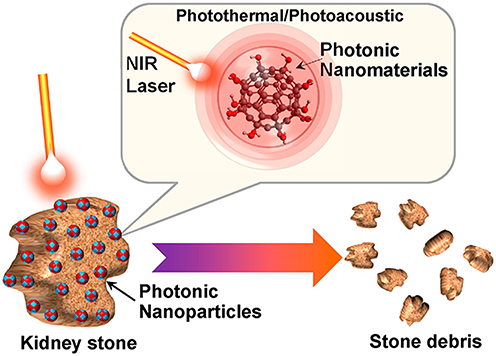 |
Figure 5 Schematic illustration of photonic nanomaterial-assisted lithotripsy for kidney stone fragmentation. Photonic nanoparticles accumulate within the kidney stone matrix and are activated by near-infrared (NIR) laser irradiation. Upon stimulation, these nanomaterials generate localized photothermal and photoacoustic effects, leading to efficient disruption of the stone structure and its fragmentation into smaller debris. This strategy highlights the potential of photonic nanomaterials as a minimally invasive platform for enhanced stone comminution. Adapted from,25 Copyright © 2023 by authors. |
More importantly, this study went beyond a purely phenomenological observation of stone cracking. By combining Fourier transform infrared spectroscopy, scanning electron microscopy, and micro-computed tomography, the authors documented surface reconstruction, crack propagation, and the conversion of calcium oxalate into calcium carbonate-like thermal degradation products after treatment.25,107 These findings indicate that the effects triggered by nanoparticle activation under near-infrared irradiation are not limited to simple heat release. Instead, they reflect a materials-level failure process involving both thermal and photoacoustic or thermomechanical effects. This mechanism shifts stone fragmentation from macroscopic cracking toward an interfacial energy-transfer process that can, in principle, be engineered and controlled.25,98 Subsequent proof-of-concept research in urolithiasis moved this strategy closer to translational application. In an in vitro human stone model, treatment with 785 nm or 1320 nm near-infrared irradiation in combination with different carbon-based or gold-based nanoparticles achieved fragmentation rates of at least 70% in most groups, with the exception of the gold nanoparticle plus 1320 nm combination. Under 785 nm irradiation, most stones fragmented within the first 3 minutes.98 In contrast, the control group did not undergo fragmentation when exposed to the same irradiation conditions without nanoparticles. This result directly demonstrates that the activated nanomaterials, rather than the laser alone, were primarily responsible for the fragmentation effect.98 The study also used micro-computed tomography to quantify the increase in stone surface area and the decrease in mean Hounsfield units after treatment. The authors further proposed that, because the selected wavelengths exhibit relatively low water absorption, a lower thermal burden may theoretically be achieved through surface activation within a limited tissue depth. These findings provide a conceptual and technical basis for the future development of minimally invasive, or even extracorporeal, strategies for targeted activation of stone fragmentation. However, substantial challenges remain, including efficient particle delivery, specific adhesion to the stone surface, and reliable in vivo imaging guidance.21,98 For instance, Ye et al advanced the concept of material-enabled lithotripsy to a new stage characterized by simultaneous modulation of the post-lithotripsy microenvironment. Specifically, the authors developed a hollow Prussian blue (HPB) nanozyme that used stable photothermal conversion under low-power 808 nm near-infrared irradiation to promote surface stone fragmentation, while its superoxide dismutase-, catalase-, and peroxidase-like activities enabled efficient ROS scavenging. In a calcium oxalate crystal-related renal injury model, this platform reduced oxidative stress in the renal tubular epithelium, downregulated crystal-adhesion and kidney injury-related proteins, and caused no significant renal tissue damage in animal experiments. These findings suggest that the next generation of lithotripsy nanomaterials should not focus solely on stone fragmentation, but should also reduce stone-related tissue injury and inhibit redeposition. These capabilities are particularly important because they directly address factors associated with recurrence risk (Figure 6).106
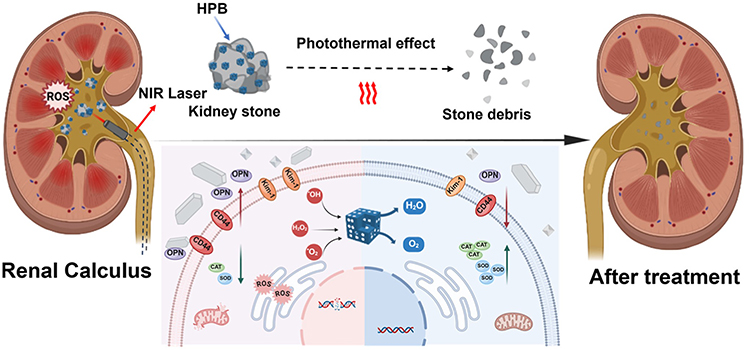 |
Figure 6 Schematic diagram illustrating the mechanism by which HPB relieves oxidative stress and mediates photonic lithotripsy. Following near-infrared (NIR) laser irradiation, HPB associated with renal calculi generates a photothermal effect that promotes stone fragmentation into smaller debris. Meanwhile, HPB exerts antioxidant activity by scavenging reactive oxygen species (ROS) and catalytically modulating redox-related species, thereby alleviating oxidative stress-induced cellular injury. This protective effect is accompanied by reduced expression of stone injury- and adhesion-related markers, including osteopontin (OPN), CD44, and kidney injury molecule-1 (Kim-1), as well as enhanced antioxidant enzyme activity, such as superoxide dismutase (SOD) and catalase (CAT). Through the combined effects of photonic lithotripsy and microenvironmental protection, HPB contributes to both stone clearance and attenuation of renal injury. Adapted from,106 Copyright © 2025 by authors. |
From this perspective, material selection is itself a major determinant of both efficacy and safety. Carbon-based nanomaterials offer strong near-infrared absorption together with high design flexibility, whereas gold-based nanomaterials achieve efficient energy conversion through tunable localized surface plasmon resonance. Prussian blue-based nanomaterials combine favorable biocompatibility, photothermal performance, and enzyme-mimetic antioxidant capacity. Accordingly, the key distinctions among lithotripsy platforms will increasingly depend on which material mediates heat generation, whether it exhibits affinity for the stone surface, and whether it provides antioxidant or anti-adhesion functions, rather than on laser power alone.25,105,106
Regarding photodynamic therapy (PDT), current evidence indicates that original research on its direct use for kidney stone fragmentation remains far more limited than that for photothermal approaches. At present, PDT remains largely at the stage of theoretical feasibility and cross-disciplinary extrapolation. Its basic mechanism involves the use of photosensitizers that generate reactive oxygen species under excitation at specific wavelengths, thereby inducing localized oxidative damage. Nanocarriers can improve the stability, local accumulation, and photoresponsiveness of photosensitizers. However, the highly mineralized structure of kidney stones, together with limited oxygen diffusion within their inorganic and organic composite core, creates major barriers to direct PDT-based fragmentation. In particular, the short effective radius of ROS, limited tissue penetration depth, and insufficiently efficient anchoring to the stone surface remain key constraints. Therefore, in the context of kidney stones, PDT is currently more likely to be used for inhibiting infectious biofilms, modulating post-fragmentation local inflammation, or enhancing interfacial damage in combination with photothermal therapy (PTT), rather than serving as a mature standalone technology for lithotripsy.21,105 This also means that its clinical translation pathway must be developed in conjunction with existing laser platforms rather than in isolation from current clinical practice. On the one hand, TFL has shown higher stone-free rates and lower intraoperative complication rates than Ho:YAG for some endpoints, although its thermal safety window remains highly dependent on power, frequency, irrigation, and intracavitary space. On the other hand, nano-mediated photothermal lithotripsy is valuable because it may enable selective interfacial destruction under lower total power and non-contact conditions, thereby reducing thermal accumulation and mechanical displacement. This material-based lowering of the energy threshold may prove more transformative than simply iterating laser hardware.100,103
However, it should be acknowledged that nano-mediated photothermal and photodynamic lithotripsy remains largely at the stage of in vitro human stone experiments and early animal studies. Before clinical application can be achieved, several major barriers must still be overcome, including in vivo delivery efficiency, biological clearance of particles, long-term safety, intraoperative visualization, regulatory consistency, and validation in large-animal and prospective clinical studies. Nevertheless, this field is particularly promising because it elevates stone fragmentation from a purely energetic problem to a coupled regulatory process involving material, light, stone, and tissue interactions. For this reason, it is expected to become one of the most promising frontiers for the future noninvasive or minimally invasive treatment of kidney stones.21,98,106
Targeted Biomimetic Cell Membrane Nanotechnology in Stone Treatment
Rather than attributing the bottleneck in kidney stone therapy simply to a lack of drugs, a more fundamental challenge is that therapeutic agents often fail to cross the complex renal hemodynamics, filtration barriers, and inflammatory microenvironment to reach the actual lesions requiring intervention, namely crystal deposits and the surrounding injured renal tubules. Therefore, biomimetic nanotechnology based on cell membrane engineering deserves separate discussion because it advances nanomaterial delivery from passive distribution to active homing through natural cellular recognition programs. This concept is consistent with the contemporary view that kidney stones are not merely a mechanical disorder, but a coupled pathological process involving crystals, epithelial injury, and immune responses (Table 3).104,108–110
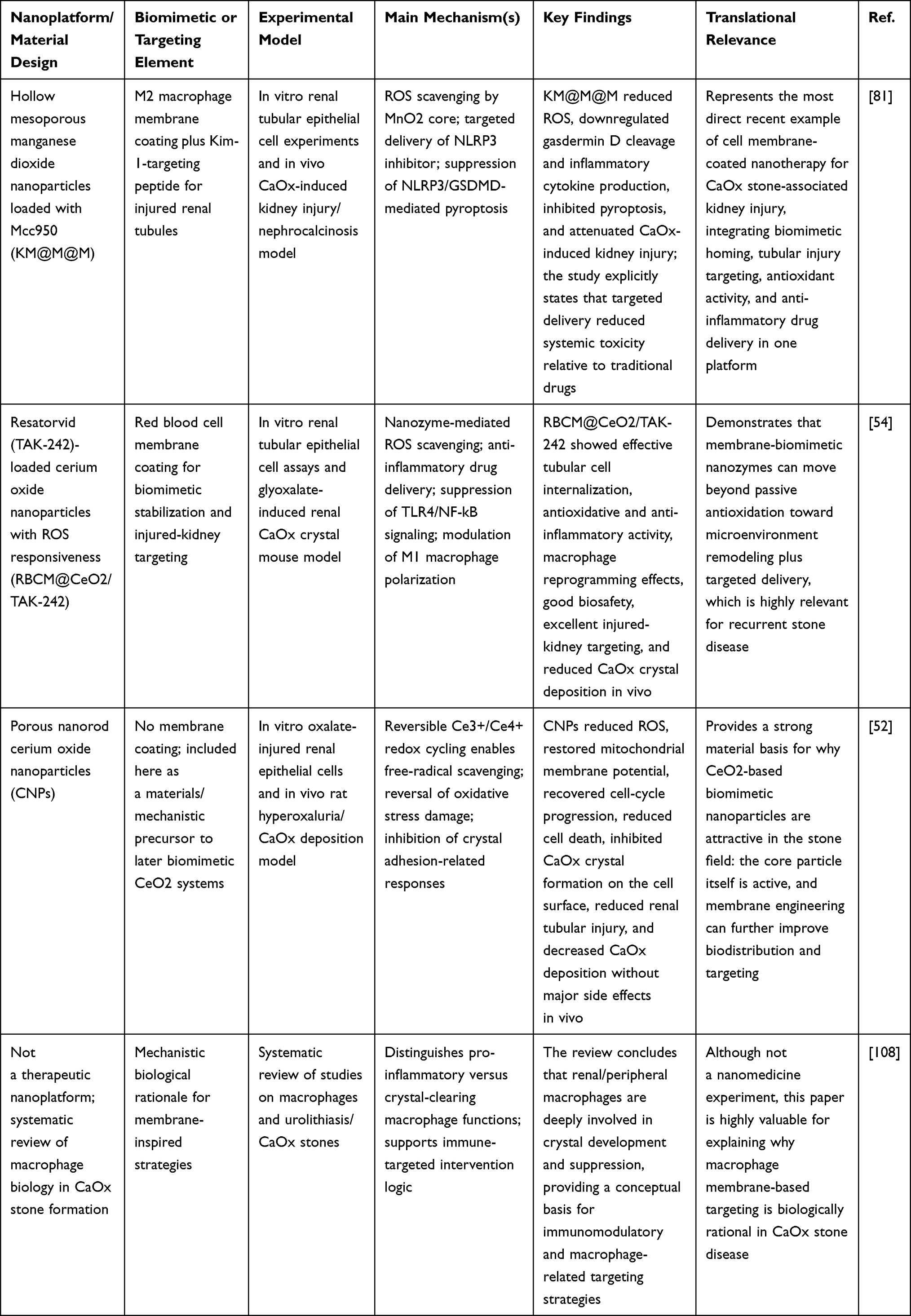 |
Table 3 Biomimetic/Cell Membrane-Inspired Nanotechnology for Calcium Oxalate Stone-Associated Kidney Injury and Targeted Intervention |
Cell membrane-coated nanoparticles (CMNPs) do not simply provide a shell for the nanocore. Instead, by retaining adhesion molecules, chemokine receptors, and immune regulatory proteins from the source cell membrane, they endow the material with immune evasion, inflammatory homing, prolonged circulation, and lesion-specific recognition. In urological diseases, such platforms have been systematically reviewed for applications in tumors, inflammation, and acute kidney injury. Their core value lies in using natural membrane proteins to shift traditional nanodrug delivery from simple renal accumulation toward precise localization within injured nephrons or inflammatory sites.109,110 In kidney stone research, original studies published over the past five years that directly address cell membrane-engineered targeted delivery for stone-related lesions remain limited. Nevertheless, the field has begun to progress from proof-of-concept investigations toward precise designs guided by pathological mechanisms. Moreover, Ba et al reported an engineered M2 macrophage membrane-coated hollow mesoporous manganese dioxide nanoparticle, designated KM@M@M. A KIM-1-targeting peptide was further introduced onto the membrane surface to enhance recognition of and accumulation in renal tubules injured by calcium oxalate (CaOx) crystals. The materials design of this platform is highly rational. The macrophage membrane provides inflammatory homing and biocompatibility, the KIM-1 peptide enables secondary targeting of injured renal tubules, the MnO2 core scavenges ROS, and the loaded NLRP3 inhibitor MCC950 directly interrupts pro-inflammatory and pyroptotic signaling after crystal injury. Together, these elements create a triple-synergistic strategy integrating membrane targeting, nanozyme-like antioxidant activity, and drug delivery.81
In vitro and in vivo experiments further demonstrated that this biomimetic material does more than reduce inflammatory markers. It inhibits NLRP3 inflammasome activation, decreases gasdermin D cleavage and inflammatory cytokine release in renal tubular epithelial cells, and ultimately suppresses pyroptosis while alleviating CaOx-related renal injury. Notably, the authors emphasized that kidney-targeted delivery reduced the toxicity risk associated with systemic exposure to conventional small molecules. This point is particularly important for future long-term prevention and repeated treatment of kidney stones, because the management of recurrent stones requires therapeutic platforms that balance safety, reproducibility, and efficacy.81 Consistent with this concept, He et al developed ROS-responsive red blood cell membrane-coated cerium oxide biomimetic nanoparticles, termed RBCM@CeO2/TAK-242. In this design, cerium oxide nanozyme served as the antioxidant core, TAK-242 was loaded as a TLR4 inhibitor, and the red blood cell membrane was used to improve circulatory stability and biosafety. The results showed that this platform was efficiently taken up by renal tubular epithelial cells and also exhibited effective targeting to injured kidneys in a glyoxylate-induced CaOx crystal mouse model. Moreover, it significantly suppressed oxidative stress and M1 macrophage polarization, downregulated the TLR4/NF-κB pathway, and ultimately reduced crystal deposition. These findings suggest that the true advantage of biomimetic nanodelivery in stone therapy lies not merely in transporting drugs to the lesion, but also in actively regulating the crystal-related immune microenvironment through the properties of the material itself.54
From a pathological perspective, this design strategy is not incidental. Systematic reviews have shown that M1 macrophages are associated with amplification of inflammation and crystal-induced injury during CaOx stone formation, whereas M2 macrophages are more favorable for crystal phagocytosis and clearance. Therefore, drawing inspiration from macrophage membranes, or directly using macrophage-related biomimetic shells, essentially represents a form of reverse engineering in which the intrinsic immune tendencies of stone lesions are converted into drug-delivery tools. This concept is also one of the most innovative aspects of this field.108
In other words, the value of biomembrane-targeted nanotechnology in kidney stone disease is no longer limited to passive delivery of antioxidant agents to the kidney. Instead, it has begun to enable multilevel integration of lesion localization, inflammatory recognition, drug release, and microenvironment remodeling. On the one hand, membrane-coating structures improve the stability and biodistribution of nanoparticles in vivo. On the other hand, the biological properties of the source membrane facilitate retention within CaOx-induced injured renal tubules and inflammatory regions, thereby increasing local drug concentration and reducing systemic adverse effects.54,81,109,110 However, it should also be acknowledged that current research directly applying biomimetic cell membranes to stone localization remains more limited than work focused on stone-related kidney injury targeting. This difference indicates that the field is still in a transitional stage, moving from targeting damaged nephrons toward direct targeting of crystal or stone surfaces and the Randall plaque microenvironment. Existing studies are better suited to addressing oxidative stress, inflammation, and cell death caused by crystal deposition, but still lack sufficient in vivo evidence regarding direct adhesion to the stone core, duration of drug retention, and differential recognition among distinct stone components.54,81 Nevertheless, from a translational perspective, this direction still offers substantial clinical potential, because kidney stone management does not rely exclusively on surgery or metabolic intervention. If cell membrane-biomimetic carriers can eventually be integrated with near-infrared imaging, photothermal lithotripsy, or local anti-infective strategies, it may be possible to establish a therapeutic platform that combines lesion localization, treatment delivery, and efficacy monitoring. Similar biomimetic membrane-coated nanosystems have already achieved active accumulation and therapy under imaging guidance, including photoacoustic and magnetic resonance modalities, in other diseases. This suggests that the methodological foundation for such systems is already established, although scenario-specific adaptation is still required for kidney stone applications.111
The most pressing challenges for clinical translation include the source and batch-to-batch stability of cell membranes, preservation of membrane protein fidelity, scalable manufacturing, long-term immunological safety, and optimization of particle size to balance renal filtration and retention in humans. It is also noteworthy that the SPAGOPIX-01 clinical trial, which evaluated the human pharmacokinetics of the functional nanoparticle SN132D, suggests that renal filtration behavior in humans has clear size-dependent characteristics. Although this finding is not specific to kidney stones, it provides an important clinical reference for identifying the optimal design window for future biomimetic nanoplatforms, namely between being small enough to facilitate renal access and large enough to avoid rapid clearance.112
Therefore, based on the available evidence, the true innovation of biomimetic membrane-targeted nanotechnology in stone therapy lies not only in increasing the likelihood that drugs reach the lesion, but also in converting the natural recognition functions of cell membranes into an engineered materials strategy. In this way, precise delivery to injured renal tubules and crystal-related microenvironments becomes an experimentally testable objective. Although considerable distance remains before clinical application, this direction has already shown practical potential for overcoming the limitations of traditional drug delivery while simultaneously addressing lesion localization and microenvironmental regulation.109–111
In the preceding subsections, we have discussed the major therapeutic nanoplatforms currently being explored for kidney stone disease, including nanodrug delivery systems, antioxidant nanozymes, nano-enabled stone fragmentation strategies, and biomimetic targeting approaches. Collectively, these studies show that current research is moving beyond single-function proof-of-concept designs toward more integrated platforms capable of combining targeting, microenvironment modulation, and stone-directed intervention. At the same time, the field remains highly heterogeneous, as different nanoplatforms vary substantially in their material composition, targeting strategy, mechanism of action, translational maturity, and current limitations. Therefore, for both the manuscript and the field itself, a structured cross-comparison is needed to clarify the overall technical landscape, identify the relative strengths and weaknesses of representative platforms, and better highlight the key opportunities and barriers for clinical translation. To address this need, we summarized the representative nanoplatforms discussed in Table 4, with comparison across material type, targeting strategy, primary mechanism, developmental stage, and major advantages and limitations. This table is intended to improve the logical integration of the section, increase information density, and provide readers with a more practical framework for understanding the current status and future direction of nanomaterial-based therapy in kidney stone disease.
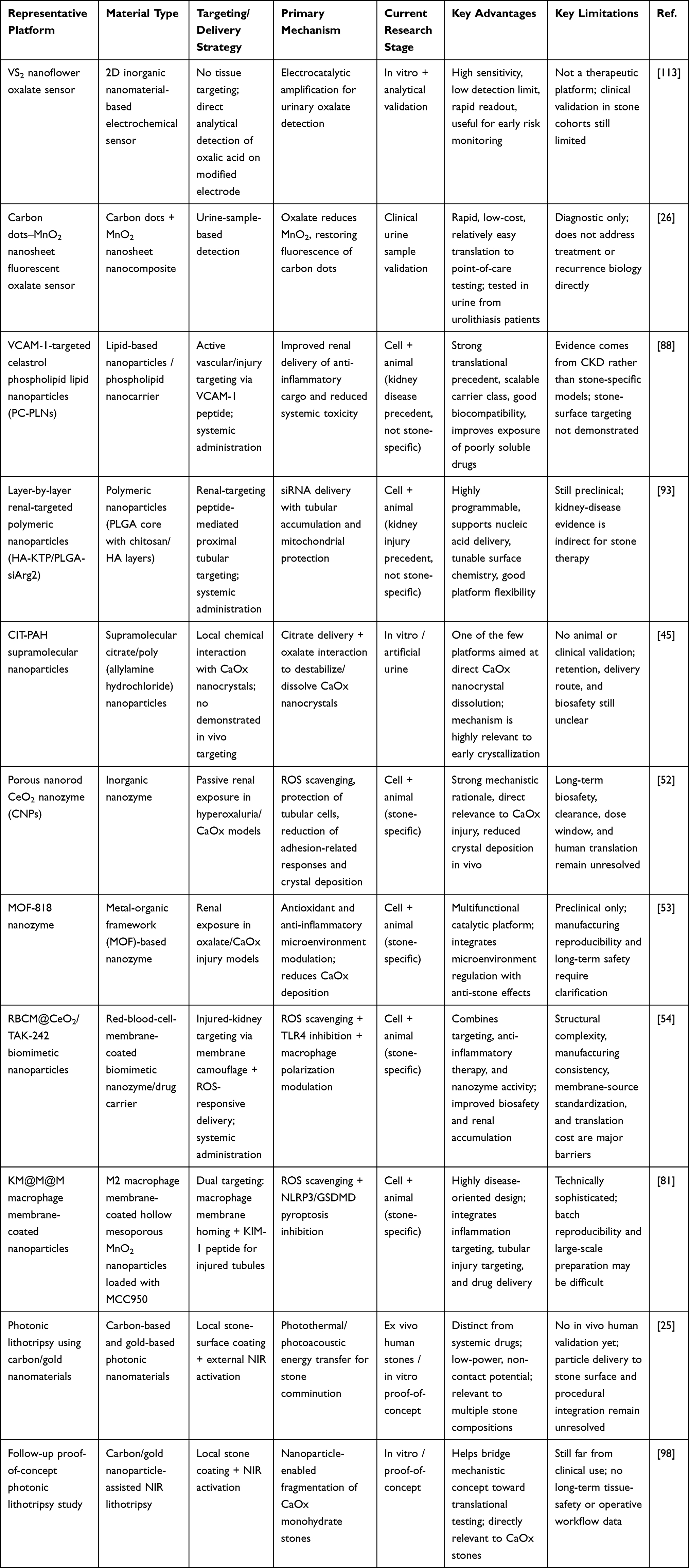 |
Table 4 Cross-Comparison of Representative Nanoplatforms for Kidney Stone Diagnosis and Treatment |
Innovative Application of Nanomaterials in the Prevention of Kidney Stones
Nanomaterials as Early Diagnostic Tools
In kidney stone prevention, clinical outcomes are often determined not by whether stones can be detected after they have formed, but by whether quantifiable risk signals such as oxalate, calcium ions, and uric acid can be identified in urine before crystals nucleate, aggregate, and adhere to the renal tubular epithelium. This is clinically important because calcium oxalate remains the predominant component of kidney stones, and hypercalciuria is one of the most important metabolic risk factors for recurrent calcium stone disease. Therefore, early screening for metabolic abnormalities represents a critical intervention point between primary and secondary prevention.114–116
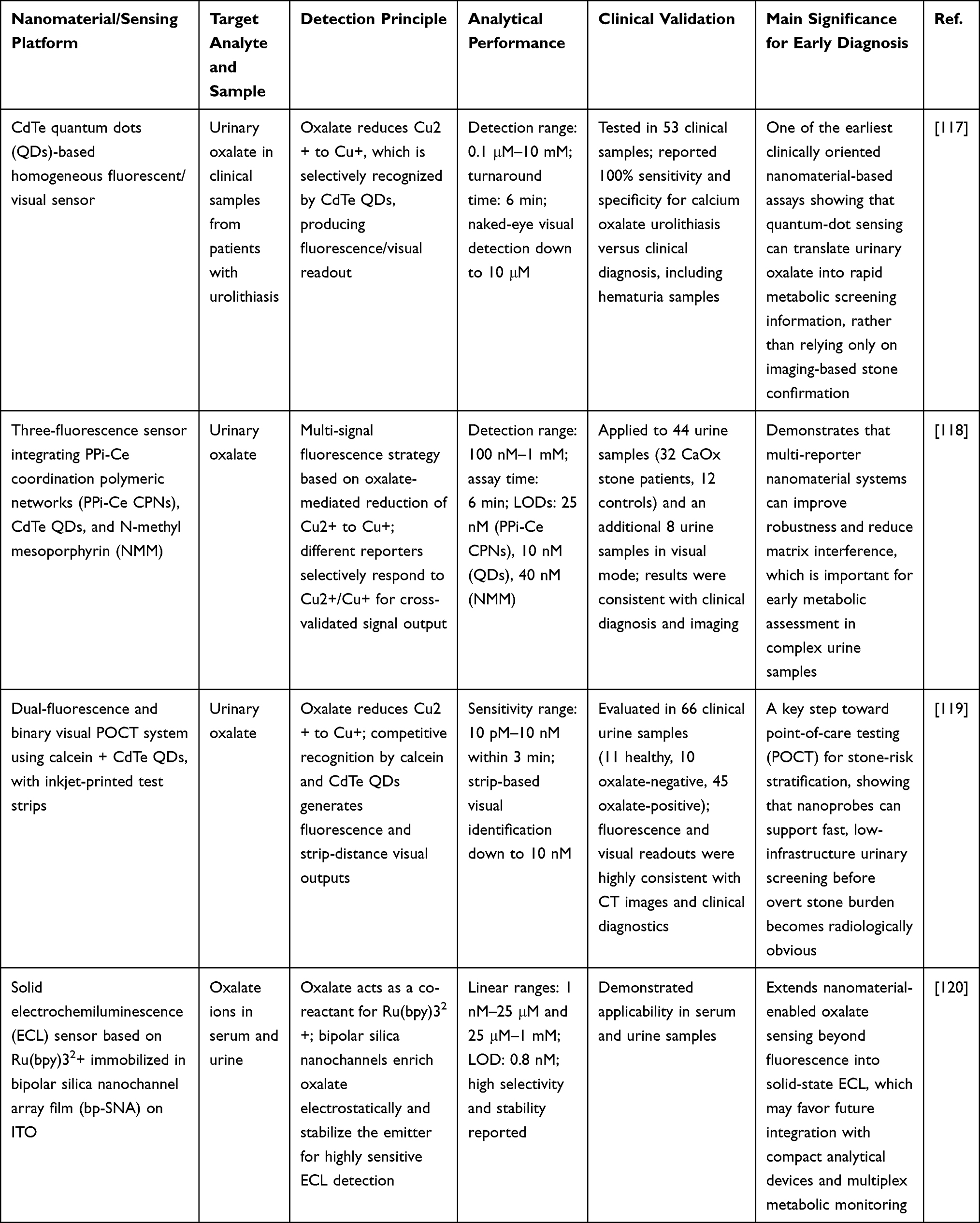 |
Table 5 Representative Nanomaterial-Based Early Diagnostic Tools for Kidney Stone-Related Oxalate Detection |
In this context, nanomaterials offer several unique advantages, including high specific surface area, tunable surface functional groups, efficient electronic and optical transduction, and the ability to construct multilevel signal-amplification interfaces. These properties make it possible to convert analytes such as oxalate, which are highly susceptible to matrix interference, large concentration fluctuations, and short detection windows in routine urinalysis, into faster, more sensitive, and potentially visualized readout signals (Table 5).114,121 A representative recent example is the urinary oxalate detection platform developed by Jiang et al, which was based on a three-fluorescence sensing system composed of pyrophosphate-cerium coordination polymer networks (PPI-Ce CPNs), CdTe quantum dots, and N-methyl mesoporphyrin. The underlying mechanism relies on oxalate-mediated reduction of Cu2⁺ to Cu⁺, followed by selective recognition of Cu2⁺ and Cu⁺ by different nano- and supramolecular fluorescence reporter units. This design enables multichannel, cross-validated signal output. This system provided a detection range of 100 nM to 1 mM, and the analysis could be completed within 6 minutes. The limits of detection for the three reporting channels were 25 nM, 10 nM, and 40 nM, respectively. The platform was further validated in 44 clinical urine samples and showed results consistent with clinical diagnosis and imaging findings. This multichannel mutual-verification strategy is particularly suitable for complex urine matrices, in which the risks of false-positive and false-negative results are relatively high.118 Building on this concept, Chen et al combined a competitive recognition strategy with distance-based test-strip readout to develop a dual-fluorescence, binary-visualization nanodetection system based on calcein and CdTe quantum dots. This method also relies on the selective chemical conversion of Cu2⁺ to Cu⁺ induced by oxalate, but places greater emphasis on translating laboratory-based instrumental analysis into point-of-care testing (POCT). It enabled high-sensitivity detection over a range of 10 pM to 10 nM within 3 minutes, and the inkjet-printed visual test strip could detect oxalate concentrations as low as 10 nM. In 66 clinical urine samples, including healthy controls as well as oxalate-negative and oxalate-positive individuals, this system showed significant improvement over conventional methods. Its high consistency with computed tomography findings and clinical diagnosis suggests that nanoprobes are no longer limited to achieving lower detection limits in analytical chemistry. Instead, they are approaching practical clinical applications in outpatient risk stratification, home-based monitoring, and recurrence warning.119
The clinical significance of this trend lies in the fact that, although conventional imaging remains the cornerstone of stone diagnosis, it is not well suited for identifying very early crystallization, metabolism-driven high-risk individuals, or pre-recurrence states. By contrast, nanomaterial-based electrochemical and fluorescence sensing platforms can shift the diagnostic focus from already formed macroscopic stones to ongoing urinary stone-related chemistry. This shift may provide an earlier basis for decisions regarding dietary intervention, fluid management, citrate therapy, thiazide treatment, and close follow-up of patients with primary hyperoxaluria or hypercalciuria.116,121 It is also important to note that the ideal targets of early diagnostic tools should not be limited to oxalate alone. Clinical studies have shown that elevated fasting urinary calcium-to-creatinine ratios and dynamic changes after calcium loading also have value for etiological stratification. This observation suggests a promising direction for next-generation nanodiagnostic platforms. Such systems may integrate oxalate, calcium ions, uric acid, citrate, and even crystal-related proteins into a multiplex detection chip, thereby generating a urinary nanofingerprint map that more closely reflects the actual pathological process of stone risk.116,121
At the same time, despite substantial progress in high-sensitivity detection, several key barriers must still be overcome before clinical translation can be achieved. These include protein contamination and sensor fouling in complex urine samples, batch-to-batch consistency in nanomaterial synthesis, long-term storage stability, inter-center comparability of results, and the transition from small case-control validation studies to prospective, multicenter clinical evidence focused on recurrence prediction endpoints. In other words, the greatest value of nanomaterials in early kidney stone screening lies not only in lowering detection limits, but also in their ability to reliably translate molecular events into clinically interpretable, reproducible, and actionable risk information.114,121 Therefore, based on current evidence, nanosensors and nanoprobes have shifted the diagnostic time window for kidney stone prevention from the stage of visible imaging to the stage of metabolic abnormality. This advance represents one of the most practical and precise innovations for reducing stone formation and recurrence.118,121,122
Prevention Strategies Combining Nanomedicine with Lifestyle
Accordingly, the latest EAU updates on recurrence prevention, together with related reviews, regard sufficient fluid intake, appropriate calcium intake, restriction of sodium and excessive animal protein, and personalized metabolic correction guided by 24-hour urine monitoring as the cornerstone of secondary stone prevention. These guidelines also emphasize that patients at high risk of recurrence require more systematic metabolic assessment and targeted intervention.3,123
For patients with recurrent kidney stones, the most clinically translatable preventive strategy does not rely solely on a stronger drug or a stricter diet. Instead, it combines lifestyle interventions that reduce urinary supersaturation with nanomedicine that mitigates crystal adhesion, oxidative stress, and epithelial injury. In this way, the prevention window can be shifted forward to multiple nodes along the continuous pathological cascade from urinary chemical abnormalities to crystal formation and crystal retention.3,123,124
Based on the available evidence, the most direct entry point for understanding nanomedicine-lifestyle synergy is the redesign of delivery systems around citrate, a core molecule in lifestyle-based stone prevention. Supramolecular CIT-PAH nanoparticles developed by Gianvincenzo et al can both load and release citrate and promote the dissolution of CaOx nanocrystals through the strong interaction between poly(allylamine) and oxalate. WAXS, DLS, TEM, NMR, and confocal Raman analyses showed that this system not only disrupted the crystal structure of calcium oxalate in the aqueous phase but also maintained crystal-dissolution activity in artificial urine. These findings suggest that the future priority should not be a general emphasis on citrate supplementation alone. Instead, greater value may lie in developing nanocarriers that enable local citrate enrichment and sustained release in real urinary environments, thereby enhancing the effective exposure achieved by citrus-rich diets or other natural citrate-based interventions.45 This approach is important because the clinical and translational bottlenecks are already clear. The PUSH randomized trial showed that even with multicomponent adherence interventions, including smart water bottles, behavioral incentives, and health coaching, improved drinking behavior did not significantly reduce symptomatic stone recurrence. This finding suggests that simply asking patients to do more may be insufficient to overcome interindividual differences in urinary chemistry and thresholds for renal tubular injury.125 In contrast, a multicenter randomized controlled trial by Dissayabutra et al showed that a lime-based regimen rich in citrate and flavonoids reduced the 2-year recurrence rate from 45% to 14%, accompanied by decreases in urinary IL-8 and 24-hour urinary protein.126 These results further suggest that lifestyle-related molecules can be effective, but their clinical benefits depend strongly on local concentration, exposure duration, and the stability of their anti-inflammatory effects, which are precisely the parameters that nanodelivery may improve.125,126 Therefore, the most evidence-based interpretation of how nanomaterials may synergize with lifestyle modification is that nanomedicine does not replace hydration or citrate-oriented diets. Rather, it may convert them from broad behavioral prescriptions into programmable local treatment platforms. For example, naturally derived citrate, flavonoids, polyphenols, or other anti-stone metabolites could be incorporated into nanosystems designed for renal accessibility, urinary release, and tunable surface chemistry, thereby reducing gastrointestinal degradation, increasing tubular exposure, and transforming fluctuating dietary signals into a more stable anti-crystallization microenvironment.22,45,84,126 Another strategy, more closely related to synergy with hydration, is not to use nanomaterials to replace water intake or directly dilute urine. Instead, nanozymes or biomimetic nanoparticles may reduce the likelihood that CaOx supersaturation will translate into epithelial injury and crystal adhesion in patients who have difficulty maintaining an ideal urine volume over the long term. Deng et al reported that a porous nanorod-shaped CeO2 nanozyme could scavenge excess free radicals through reversible Ce3+/Ce4+ cycling, thereby reducing oxidative damage in HK-2 cells and inhibiting renal CaOx deposition under hyperoxaluric conditions.52 He et al further developed ROS-responsive, RBC membrane-coated CeO2/TAK-242 biomimetic nanoparticles that simultaneously reduced oxidative stress and M1 macrophage polarization in a CaOx model, thereby decreasing crystal deposition.54 Collectively, these findings indicate that if nanozymes are integrated with hydration-based management, their true synergistic value may not lie in marginally reducing supersaturation itself. Instead, they may interrupt the biological amplification triggered by low urine volume or urinary fluctuations through antioxidant, anti-inflammatory, and anti-adhesive effects.52,54 It is also worth noting that the variable effectiveness of lifestyle interventions in real-world settings is not solely due to poor adherence, but also reflects interpatient differences in urinary chemistry and renal tubular surface biology.22,62,84 In this context, Wang et al provided insightful mechanistic evidence using carboxymethylated polysaccharides from Desmodium styracifolium. In HK-2 cells and a nanoCOD crystal model, moderate carboxymethylation reduced crystal-surface adhesion and promoted appropriate crystal endocytosis. These findings suggest that if natural polysaccharides or plant-derived bioactive compounds are developed into controllable nanoformulations, their value may extend beyond simple component supplementation to the fine modulation of crystal-cell interfacial interactions.62 From the general principles of renal nanomedicine delivery, the feasibility of such synergistic strategies is supported by recent evidence showing that nanoparticle size, charge, surface ligands, protein corona, and disease state jointly determine glomerular filtration, tubular uptake, intraluminal retention, and excretion behavior. Therefore, to rigorously verify nanomedicine-lifestyle synergy in future studies, experimental designs should not only record water or citrate intake but also quantify the causal links among urinary supersaturation, urinary citrate concentration, renal nanoparticle exposure, inflammatory markers, and imaging-defined recurrence.22,84 Based on the current evidence, there remains a lack of high-quality kidney stone studies that directly demonstrate a clinical synergistic effect between nanomaterials and standard lifestyle interventions.3,52,123,124,127
Therefore, this concept is better regarded as an emerging translational direction than as a mature interventional paradigm. The two most promising routes for further development are nanocarriers for the precise delivery of citrate or plant-derived bioactive compounds, and kidney-targeted nanozymes or biomimetic nanosystems that buffer oxidative stress and crystal adhesion in parallel with hydration management. Both strategies are supported by clear mechanistic foundations as well as in vitro, animal, and preliminary clinical evidence. The next step is to validate these approaches in prospective combined studies incorporating 24-hour urinary parameters and recurrence-based endpoints.3,54,123,128
Challenges and Future Research Directions
Challenges in Clinical Application
From basic research to clinical practice, the greatest challenge facing nanomaterials in kidney stone disease is often not whether they are effective, but whether their benefits can be achieved safely, predictably, reproducibly, and affordably in the human body.54,129 This issue is particularly important because cerium oxide nanozymes designed to inhibit calcium oxalate deposition, biomimetic membrane-coated nanoparticles developed for lesion-targeted delivery, and photothermal or photonic nanomaterials used for near-infrared lithotripsy have all shown encouraging antioxidant, anti-inflammatory, crystal-inhibitory, or lithotriptic effects in cell models, ex vivo stone systems, and animal studies. However, these advantages have not yet translated into clinical usability, indicating that a series of general nanomedicine barriers and kidney-specific challenges still separate established efficacy from clinical translatability.21,25,52,54,81
The first major challenge is the tension between biocompatibility and renal exposure. The kidney is not only a potential target organ for many nanoparticles, but also a major clearance organ. Therefore, any nanosystem intended to act on kidney stone lesions must address two questions simultaneously: whether it can reach the kidney efficiently and whether it may cause additional renal injury after arrival. This issue becomes even more complex in the setting of renal tubular injury, local inflammation, and an abnormal urinary environment in stone-forming patients. Under these conditions, the size, charge, surface modification, and protein corona formation of nanomaterials may alter filtration, reabsorption, luminal retention, and cellular uptake, thereby amplifying unpredictable differences in tissue exposure.22,129,130 The second core challenge is the uncertainty surrounding long-term toxicity and in vivo fate. Kidney stone disease differs from short-course conditions such as tumors because of its high recurrence rate. As a result, many preventive strategies require long-term, intermittent, or repeated administration. Accordingly, nanomaterials intended for stone prevention require more stringent long-term safety evaluation than therapies administered only once. However, current nanomaterial research in kidney stone disease still focuses mainly on observation windows ranging from a few days to a few weeks, with primary emphasis on serum creatinine, tissue staining, and short-term biochemical indices. Evidence remains markedly insufficient regarding chronic accumulation, immune remodeling, effects on the gut-kidney axis, reproductive toxicity, and risks associated with underlying metabolic abnormalities.21,22,25 The third obstacle is the mismatch between preclinical efficacy assessment systems and clinically meaningful endpoints. In most nanomaterial-based kidney stone studies, the primary endpoints remain CaOx deposition area, ROS levels, inflammatory cytokine expression, or in vitro fragmentation rates. Although these indicators are important for mechanistic elucidation, they remain far removed from clinically meaningful benefits such as lower recurrence rates, longer stone-free intervals, reduced need for surgical intervention, symptom relief, and preservation of renal function.21,25,98 The fourth challenge is that the regulatory pathway remains insufficiently clear, and nanomedicine cannot be readily accommodated within conventional drug-evaluation frameworks. The FDA has explicitly stated that drugs containing nanomaterials in their final dosage form may exhibit product properties that differ substantially from those of conventional formulations, and may therefore require special review with respect to CMC, quality control, safety, and efficacy. In other words, nanomedicines cannot be approved through conventional pathways simply by loading an active ingredient into a smaller carrier. Parameters such as particle size distribution, surface chemistry, aggregation behavior, drug release, impurity profile, and biological interactions may all become key regulatory variables.131 Recent industrial and renal nanomedicine reviews have repeatedly emphasized that the greatest regulatory difficulty lies not in the absence of regulations, but in the extreme heterogeneity of nanoproducts. Many properties that determine efficacy and risk are difficult to capture using traditional single quality attributes, which makes bioequivalence assessment, batch consistency, and bridging-study design considerably more complex.129,132 In kidney stone disease, this obstacle may be even more pronounced because there are currently no nanomedicines specifically developed and approved for stones, no established regulatory precedents, and no mature submission templates for recurrence prevention, local delivery, or drug-device-material combination products. Therefore, many future products may need to identify the most appropriate regulatory classification among drugs, devices, and combination products.129,131,132 In addition, nanoplatforms developed in academic research often rely on multistep synthesis, complex surface modification, and highly refined characterization, particularly in the case of biomimetic membrane-coating systems, functionalized gold nanomaterials, or multicomponent theranostic platforms. Feasibility at the laboratory scale does not necessarily translate into scalability under GMP conditions. Once industrial development begins, factors such as raw-material stability, membrane-source acquisition, sterility control, lyophilization, transport stability, and drift in particle size or zeta potential during long-term storage will directly determine whether a product is truly manufacturable.54,81,129,132
Therefore, the real challenge in the clinical application of nanomaterials for kidney stones is not simply a single issue of toxicity or cost, but rather an interdisciplinary coupling problem. It requires understanding how the kidney, as a filtering organ, determines the fate of materials, how material function can be maintained in real urine and complex lesions, and how added value can be demonstrated through standardized manufacturing, appropriate regulatory pathways, and cost-effective clinical trials. In this sense, future research should focus not only on further improving crystal-inhibition or fragmentation efficiency in a given system, but also on establishing animal models that more closely resemble recurrent human stone disease, conducting long-term toxicological and pharmacokinetic studies, clarifying the relationship between quality attributes and clinical endpoints, and prioritizing nanoplatforms with relatively simple structures, clear mechanisms, and strong manufacturability. Only in this way can current promising laboratory achievements be translated into genuine clinical application.3,131,132
Future Research Directions and Trends
Therefore, in order to overcome the shortcomings of nanomaterials in current kidney stone diseases, we should not view it as an isolated next-generation technology catalog in the future, but rather as a problem-oriented transformation roadmap, where each research direction is clearly aimed at solving a clear clinical bottleneck. Because in this field, the scientific value will ultimately depend not on the elegance of the nanosystem in vitro, but on whether it can enter the kidneys in a controllable manner, remain safe under repeated use conditions, and bring important benefits to patients with stone formation in practical practice.84,133,134 First, to address the tension between renal targeting and biocompatibility, future studies should move from empirical particle optimization toward physiology-guided design, systematically integrating glomerular filtration constraints, tubular uptake pathways, protein corona evolution, and disease-state urinary chemistry into nanoparticle engineering; notably, renal nanomedicine studies have already shown that kidney accumulation is highly dependent on particle physicochemical features, while albumin-corona nanocomplexes can be deliberately exploited to enhance tubular delivery, suggesting that “kidney targeting” must be treated as a measurable transport problem rather than a qualitative label.84,135 Second, to overcome uncertainty in long-term toxicity and in vivo fate, the field should prioritize repeated-dose pharmacokinetic and toxicology studies with longer observation windows, ideally extending to metabolically relevant and, where feasible, large-animal models, because renal handling of nanomaterials can be counterintuitive and even particles larger than the classical filtration threshold may show atypical renal clearance, making short-term serum biochemistry alone clearly insufficient for translational decision-making.136,137 Third, mechanistically defined stone models should be used to link material function to disease biology more rigorously: for example, carboxymethylated Desmodium styracifolium polysaccharides were shown to reduce nano-calcium oxalate crystal adhesion and modulate crystal endocytosis in HK-2 cells, whereas ROS-responsive RBC membrane-coated cerium oxide nanoparticles loaded with TAK-242 suppressed oxidative stress, inhibited M1 macrophage polarization, and reduced crystal deposition in a glyoxylate-induced model, indicating that future work should compare whether anti-adhesion, antioxidant, inflammasome-suppressive, and macrophage-reprogramming strategies yield distinct advantages in different stone phenotypes instead of repeatedly reporting only smaller CaOx deposition areas.54,62 Fourth, to correct the current mismatch between preclinical readouts and clinical relevance, future translational studies should adopt endpoints closer to actual patient benefit, including recurrence-free interval, symptomatic recurrence, need for re-intervention, stone-free duration, imaging-based progression, and preservation of renal function, because the contemporary stone literature makes clear that recurrence surveillance is inherently longitudinal and cannot be captured adequately by single-time-point crystal burden alone.133,138 Fifth, to reduce regulatory uncertainty, nanomaterial programs for urolithiasis should establish chemistry, manufacturing, and controls (CMC) strategies at an early stage, with predefined critical quality attributes such as particle-size distribution, surface chemistry, membrane-source consistency, aggregation behavior, release kinetics, sterility, and storage stability, since both the FDA nanomaterial guidance and recent regulatory analyses emphasize that nanodrugs cannot simply be evaluated as smaller versions of conventional formulations.131,139 Sixth, manufacturability should become a selection criterion rather than an afterthought, meaning that platforms with simpler composition, modular assembly, scalable raw materials, and robust lyophilization or transport stability may deserve priority over overly sophisticated theranostic constructs, especially in a stone field where the comparator is not theoretical efficacy but practical competition with increasingly less invasive technologies; indeed, first-in-human break wave lithotripsy has already demonstrated that new stone interventions are more likely to gain traction when they show acceptable safety, low anesthesia burden, and realistic workflow advantages in multicenter settings.138,139 In this sense, the most credible future direction is not simply “smarter” nanotechnology, but a more selective translational strategy: choose platforms with clear mechanisms, verify them under recurrent-disease conditions, evaluate them against clinically meaningful longitudinal endpoints, and build regulatory-grade quality packages early, so that the field can finally move from promising anti-crystal laboratory observations to nanomedicines or nano-enabled interventions that are genuinely testable in clinical stone prevention and treatment.62,134
Meanwhile, the most important change in the field of kidney stones may not simply be the emergence of more nanomaterials, but the evolution of these materials from single tools for crystal inhibition or drug delivery into closed-loop management platforms integrated with artificial intelligence, digital monitoring, and precise phenotyping. In other words, stone management may shift from the simple detection of existing stones to a continuous medical pathway involving risk prediction, dynamic monitoring, intelligent intervention, and recurrence warning.3,21,129 A trend extending beyond intelligent detection is the use of AI for nanotherapy design and personalized treatment development.22,140,141 On the one hand, AI can be used to screen material parameters that are most suitable for different pathological scenarios. For example, nanozyme systems with ROS-scavenging and anti-inflammatory properties may be prioritized for patients with high urinary oxalate and pronounced oxidative stress, whereas biomimetic nanoplatforms with lesion imaging, local drug delivery, or antibiofilm capabilities may be more suitable for patients with residual fragments or infection-related stones.140,141 On the other hand, AI may also support the reverse design of nanomaterials by integrating variables such as particle size, surface charge, protein corona formation, renal filtration behavior, and lesion-adhesion capacity to predict which platforms are most likely to achieve effective renal delivery while maintaining biological safety. This algorithm-assisted optimization of materials has been recognized as an important trend in medical AI in general and as one of the key future directions highlighted in reviews of renal nanomedicine translation.22,140,141
From the perspective of disease heterogeneity in kidney stone disease, individualized treatment will increasingly rely on the integration of genetic information and electronic medical records. For example, several studies have suggested that future stone management will no longer be limited to selecting medication according to stone composition.129,142,143 Instead, it may integrate genetic background, metabolic profiles, radiomic features, and lifestyle data to generate precise prevention strategies with different intervention intensities, material platforms, and follow-up frequencies for different patients.144,145 However, it should also be acknowledged that direct evidence for the integration of AI and nanotechnology in kidney stone disease remains limited. Most studies are still in a stage of parallel development, with AI being used for risk stratification and nanomaterials being developed separately for detection or treatment, rather than forming a truly large-scale and prospective closed-loop system.3,22,141 Therefore, the most worthwhile directions for future research are not based on simply stacking concepts, but on solving several concrete problems. First, it is necessary to establish multimodal databases that can simultaneously incorporate imaging, 24-hour urine data, genetic information, lifestyle variables, and nanosensor outputs in order to support high-quality algorithm training.129,142,143 Second, intelligent nanodiagnostic devices compatible with clinical workflows should be developed so that detection results can be automatically returned and incorporated into recurrence prediction.114,119 Third, prospective studies of digital monitoring combined with metabolic intervention and nanotherapy should be conducted in high-risk recurrence subgroups to determine whether such platforms can truly reduce recurrence, lower the need for surgery, and improve long-term renal outcomes.146,147 Fourth, the co-translation of simplified, manufacturable, and regulatable nanoplatforms with algorithmic systems should be promoted to avoid a future in which technologies remain individually strong but collectively fragmented.3,124,129
Overall, the most likely future outcome in kidney stone management is not the appearance of a single revolutionary drug, but the establishment of a precise management system in which AI performs identification and prediction, intelligent nanodevices enable sensing and monitoring, and personalized strategies guide intervention and adjustment. In such a system, the significance of nanotechnology will shift from that of a new material platform to that of an interface layer for precision stone medicine, while artificial intelligence may become the central coordinator that truly connects molecular events, imaging information, and clinical decision-making.
Conclusion
In conclusion, kidney stone disease is a complex disorder involving metabolic disturbance, epithelial injury, oxidative stress, inflammation, and crystal retention rather than a simple process of crystal precipitation. Nanomaterials have emerged as promising tools for this field because they offer opportunities for early diagnosis, renal-targeted therapy, microenvironmental regulation, and recurrence prevention. The most clinically meaningful advances can be grouped into several core directions: nanoscale metabolic sensing for earlier risk identification, targeted delivery systems for renal and lesion-specific intervention, antioxidant and biomimetic platforms for protection of the crystal-injured microenvironment, and photoresponsive strategies that may complement stone-disruption technologies. At the same time, these emerging strategies should be interpreted in the context of the current state of the art in stone treatment, in which mechanical stone disruption remains the clinical cornerstone. Established approaches such as shock wave lithotripsy (SWL), together with endourologic fragmentation techniques, are highly effective for debulking or removing formed stones, while newer ultrasound-based technologies, including burst wave lithotripsy and ultrasonic propulsion, further highlight the potential of noninvasive or minimally invasive mechanical management, particularly for fragmentation and clearance of residual fragments. However, mechanical disruption and drug-based or nanomaterial-enabled treatment are not competing paradigms so much as complementary ones. Mechanical techniques are best suited to the immediate physical management of established stones and obstruction, whereas pharmacologic and nanotechnology-based approaches are more relevant to upstream disease modification, including suppression of crystal-cell adhesion, attenuation of oxidative and inflammatory injury, microenvironmental remodeling, and long-term recurrence prevention. In this sense, nanomedicine is unlikely to replace SWL or other stone-breaking technologies in the near term; rather, its greatest translational value may lie in improving what mechanical treatment alone cannot fully solve, namely early risk detection, lesion-specific renal protection, residual fragment management, and durable prevention of re-formation. This distinction also helps clarify the translational role of nanotechnology: its value lies less in replacing existing procedures than in bridging the gap between acute stone removal and long-term biologic control of recurrence. Despite this progress, important challenges remain, including long-term safety, renal biocompatibility, large-scale manufacturing, regulatory barriers, and limited clinical validation. Among these, safety evaluation deserves particular emphasis, because materials intended for kidney stone applications must not only demonstrate therapeutic efficacy but also avoid renal epithelial toxicity, off-target accumulation, immunologic risk, and unintended promotion of crystal nucleation or retention. Moreover, future studies should compare nanomaterial-based strategies more explicitly with existing mechanical and pharmacologic standards, so that their true added value can be judged in terms of efficacy, tissue protection, fragment clearance, recurrence reduction, and clinical practicality. Future progress in the field will likely depend not on choosing between stone disruption and drug treatment, but on integrating them more intelligently—for example, combining mechanical debulking with nano-enabled protection of the renal microenvironment, anti-redeposition strategies, or adjunctive technologies that facilitate fragment clearance while reducing tissue injury and recurrence risk. Overall, the integration of nanotechnology with intelligent diagnostics and individualized metabolic evaluation may provide a more precise and clinically relevant direction for the future prevention and treatment of kidney stones.
Data Sharing Statement
No new data has been generated, all references are cited in the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Natural Science Foundation Project of Yunnan Province (Grant No. 2024YNLCYXZX0506).
Disclosure
The authors declare that there are no competing interests associated with the manuscript.
References
1. Khan SR, Pearle MS, Robertson WG, et al. Kidney stones. Nat Rev Dis Primers. 2016;2(1):16008. doi:10.1038/nrdp.2016.8
2. Ferraro PM, Bargagli M, Trinchieri A, Gambaro G. Risk of Kidney Stones: influence of Dietary Factors, Dietary Patterns, and Vegetarian–Vegan Diets. Nutrients. 2020;12(3):779. doi:10.3390/nu12030779
3. Skolarikos A, Straub M, Knoll T, et al. Metabolic Evaluation and Recurrence Prevention for Urinary Stone Patients: EAU Guidelines. Europ urol. 2015;67(4):750–35. doi:10.1016/j.eururo.2014.10.029
4. Li Y, Di X, Liu M, Wei J, Li T, Liao B. Association between daily sitting time and kidney stones based on the National Health and Nutrition Examination Survey (NHANES) 2007–2016: a cross-sectional study. Int J Surg. 2024;110(8):4624–4632. doi:10.1097/JS9.0000000000001560
5. Yuan S, Larsson SC. Coffee and Caffeine Consumption and Risk of Kidney Stones: a Mendelian Randomization Study. Am J Kidney Dis. 2022;79(1):9–14.e1. doi:10.1053/j.ajkd.2021.04.018
6. Pearle MS, Goldfarb DS, Assimos DG, et al. Medical Management of Kidney Stones: AUA Guideline. J Urol. 2014;192(2):316–324. doi:10.1016/j.juro.2014.05.006
7. Vera-Ponce VJ, Sanchez-Tamay NM, Ballena-Caicedo J, Zuzunaga-Montoya FE, De Carrillo CIG, Poemape Mestanza RL. Global prevalence of urolithiasis: a meta-analysis accounting for methodological heterogeneity. Front Urol. 2025;5:1705953. doi:10.3389/fruro.2025.1705953
8. Collaborators G. The global, regional, and national burden of urolithiasis in 204 countries and territories, 2000–2021: a systematic analysis for the Global Burden of Disease Study 2021. 2021. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11618031/.
9. Robertson WG. Potential role of fluctuations in the composition of renal tubular fluid through the nephron in the initiation of Randall’s plugs and calcium oxalate crystalluria in a computer model of renal function. Urolithiasis. 2015;43(1):93–107. doi:10.1007/s00240-014-0737-1
10. Kok DJ, Boellaard W, Ridwan Y, Levchenko VA. Timelines of the “free-particle” and “fixed-particle” models of stone-formation: theoretical and experimental investigations. Urolithiasis. 2017;45(1):33–41. doi:10.1007/s00240-016-0946-x
11. Peerapen P, Thongboonkerd V. Kidney Stone Prevention. Adv Nutr. 2023;14(3):555–569. doi:10.1016/j.advnut.2023.03.002
12. Fontenelle LF, Sarti TD. Kidney Stones: treatment and Prevention. Am Fam Physician. 2019;99(8):490–496.
13. Zhu Z, Ruan S, Jiang Y, et al. α-Klotho released from HK-2 cells inhibits osteogenic differentiation of renal interstitial fibroblasts by inactivating the Wnt–β-catenin pathway. Cell Mol Life Sci. 2021;78(23):7831–7849. doi:10.1007/s00018-021-03972-x
14. Kaur M, Varanasi R, Nayak D, Tandon S, Agrawal V, Tandon C. Molecular insights into cell signaling pathways in kidney stone formation. Urolithiasis. 2025;53(1):30. doi:10.1007/s00240-025-01702-7
15. Dauw CA, Yi Y, Bierlein MJ, et al. Factors Associated With Preventive Pharmacological Therapy Adherence Among Patients With Kidney Stones. Urology. 2016;93:45–49. doi:10.1016/j.urology.2016.03.030
16. Ito K, Takahashi T, Somiya S, et al. Predictors of Repeat Surgery and Stone-related Events After Flexible Ureteroscopy for Renal Stones. Available from: https://www.goldjournal.net/article/S0090-4295(21)00216-8/abstract.
17. Zeng G, Traxer O, Zhong W, et al. International Alliance of Urolithiasis guideline on retrograde intrarenal surgery. BJU Int. 2023;131(2):153–164. doi:10.1111/bju.15836
18. Sorensen MD, Harper JD, Borofsky MS, et al. Removal of Small, Asymptomatic Kidney Stones and Incidence of Relapse. N Engl J Med. 2022;387(6):506–513. doi:10.1056/NEJMoa2204253
19. Pozdzik A, Grillo V, Sakhaee K. Gaps in kidney stone disease management: from clinical theory to patient reality. Urolithiasis. 2024;52(1):61. doi:10.1007/s00240-024-01563-6
20. Senel S, Ceviz K, Ozden C, Gultekin H, Gokkaya CS, Koudonas A. The fate of clinically insignificant residual fragments following retrograde intrarenal surgery and factors affecting spontaneous passage. Urolithiasis. 2024;52(1):39. doi:10.1007/s00240-024-01544-9
21. Prachi, Kaur M, Varanasi R, et al. Nanotechnology in Urolithiasis: transformative Approaches for Kidney Stone Theranostics. BioNanoScience. 2025;15(1):106. doi:10.1007/s12668-024-01760-y
22. Huang Y, Ning X, Ahrari S, et al. Physiological principles underlying the kidney targeting of renal nanomedicines. Nat Rev Nephrol. 2024;20(6):354–370. doi:10.1038/s41581-024-00819-z
23. Yuan ZX, Shang Z, Gu J, He L. Renal targeting delivery systems. Future Med Chem. 2019;11(17):2237–2240. doi:10.4155/fmc-2019-0152
24. Chade AR, Bidwell GL. Novel Drug Delivery Technologies and Targets for Renal Disease. Hypertension. 2022;79(9):1937–1948. doi:10.1161/HYPERTENSIONAHA.122.17944
25. Houlihan I, Kang B, De S, Krishna V. Photonic Lithotripsy: near-Infrared Laser Activated Nanomaterials for Kidney Stone Comminution. Nano Lett. 2023;23(13):5981–5988. doi:10.1021/acs.nanolett.3c01166
26. Hu K, Chen X, Song X, Wu Y, Huang K, Chen P. Carbon dots and MnO2 nanosheet nanocomposites sensing platform for sensitive detection of oxalate in urine samples of urolithiasis patients. Talanta. 2024;266:124976. doi:10.1016/j.talanta.2023.124976
27. Wang Y, Yang J, Amier Y, Yuan D, Xun Y, Yu X. Advancements in Nanomedicine for the Diagnosis and Treatment of Kidney Stones. Int J Nanomed. 2025;20:1401–1423. doi:10.2147/IJN.S504318
28. Pallares RM, Barmin RA, Wang A, Kiessling F, Lammers T. Clinical cancer nanomedicines. J Control Release. 2025;385:113991. doi:10.1016/j.jconrel.2025.113991
29. Shi J, Kantoff PW, Wooster R, Farokhzad OC. Cancer nanomedicine: progress, challenges and opportunities. Nat Rev Cancer. 2017;17(1):20–37. doi:10.1038/nrc.2016.108
30. Altunhan A, Soyturk S, Guldibi F, et al. Artificial intelligence in urolithiasis: a systematic review of utilization and effectiveness. World J Urol. 2024;42(1):579. doi:10.1007/s00345-024-05268-8
31. Lim EJ, Castellani D, So WZ, et al. Radiomics in Urolithiasis: systematic Review of Current Applications, Limitations, and Future Directions. J Clin Med. 2022;11(17):5151. doi:10.3390/jcm11175151
32. Abou-Elela A. Epidemiology, pathophysiology, and management of uric acid urolithiasis: a narrative review. J Adv Res. 2017;8(5):513–527. doi:10.1016/j.jare.2017.04.005
33. Bargagli M, Scoglio M, Howles SA, Fuster DG. Kidney stone disease: risk factors, pathophysiology and management. Nat Rev Nephrol. 2025;21(11):794–808. doi:10.1038/s41581-025-00990-x
34. Rao CY, Sun XY, Ouyang JM. Effects of physical properties of nano-sized hydroxyapatite crystals on cellular toxicity in renal epithelial cells. Mater Sci Eng C. 2019;103:109807. doi:10.1016/j.msec.2019.109807
35. Huang Y, Wang J, Jiang K, Chung EJ. Improving Kidney Targeting: the Influence of Nanoparticle Physicochemical Properties on Kidney Interactions. J Control Release. 2021;334:127–137. doi:10.1016/j.jconrel.2021.04.016
36. Gay C, Letavernier E, Verpont MC, et al. Nanoscale Analysis of Randall’s Plaques by Electron Energy Loss Spectromicroscopy: insight in Early Biomineral Formation in Human Kidney. ACS Nano. 2020;14(2):1823–1836. doi:10.1021/acsnano.9b07664
37. Kumar P, Patel M, Thomas V, Knight J, Holmes RP, Mitchell T. Dietary Oxalate Induces Urinary Nanocrystals in Humans. Kidney Int Rep. 2020;5(7):1040–1051. doi:10.1016/j.ekir.2020.04.029
38. Kumar P, Bell A, Mitchell T. Estimation of urinary nanocrystals in humans using calcium fluorophore labeling and Nanoparticle Tracking Analysis. J Vis Exp. 2021;10(168):62192. doi:10.3791/62192
39. Khan SR. Inflammation and injury: what role do they play in the development of Randall’s plaques and formation of calcium oxalate kidney stones? 2021. Available from: https://comptes-rendus.academie-sciences.fr/chimie/articles/10.5802/crchim.93/.
40. Han J, Tong XY, Rao CY, Ouyang JM, Gui BS. Size-Dependent Cytotoxicity, Adhesion, and Endocytosis of Micro-/Nano-hydroxyapatite Crystals in HK-2 Cells. ACS Omega. 2023;8(50):48432–48443. doi:10.1021/acsomega.3c08180
41. Chen XW, Tong XY, Tan RM, Ouyang JM. Size-dependent pyroptosis induction by calcium oxalate monohydrate crystals in HK-2 cells. iScience. 2025;29(1):114459. doi:10.1016/j.isci.2025.114459
42. Tong XY, Nong WJ, Tan RM, Ouyang JM. Differences in macrophage pyroptosis and polarization induced by nano-/micro-calcium oxalate crystals. J Nanobiotechnology. 2025;23(1):499. doi:10.1186/s12951-025-03549-x
43. Khan SR. Inflammation and injury: what role do they play in the development of Randall’s plaques and formation of calcium oxalate kidney stones? CR Chim. 2022;25(S1):355–372. doi:10.5802/crchim.93
44. Kim D, Chauhan VP, Alamani BG, et al. Bio-inspired multifunctional disruptors of calcium oxalate crystallization. Nat Commun. 2025;16(1):5229. doi:10.1038/s41467-025-60320-4
45. Gianvincenzo PD, Leyes MF, Boonkam K, et al. Supramolecular citrate poly allylamine hydrochloride nanoparticles for citrate delivery and calcium oxalate nanocrystal dissolution. J Colloid Interface Sci. 2024;669:667–678. doi:10.1016/j.jcis.2024.04.185
46. Noonin C, Putpim A, Thongboonkerd V. The direct inhibitory effects of Lactobacillus acidophilus, a commensal urinary bacterium, on calcium oxalate stone development. Microbiome. 2024;12(1):175. doi:10.1186/s40168-024-01877-y
47. Agudelo J, Chen X, Mukherjee SD, Nguyen JK, Bruggeman LA, Miller AW. Cefazolin shifts the kidney microbiota to promote a lithogenic environment. Nat Commun. 2024;15(1):10509. doi:10.1038/s41467-024-54432-6
48. Sun XY, Chen JY, Rao CY, Ouyang JM. Size-Dependent Cytotoxicity of Hydroxyapatite Crystals on Renal Epithelial Cells. Int J Nanomed. 2020;15:5043–5060. doi:10.2147/IJN.S232926
49. Lieske JC, Norris R, Toback FG. Adhesion of hydroxyapatite crystals to anionic sites on the surface of renal epithelial cells. Am J Physiol Renal Physiol. 1997;273(2):F224–F233. doi:10.1152/ajprenal.1997.273.2.F224
50. Li D, Zhang D, Tang B, et al. Exosomes from Human Umbilical Cord Mesenchymal Stem Cells Reduce Damage from Oxidative Stress and the Epithelial-Mesenchymal Transition in Renal Epithelial Cells Exposed to Oxalate and Calcium Oxalate Monohydrate. Stem Cells Int. 2019;2019:6935806. doi:10.1155/2019/6935806
51. Yuan Y, Ma Y, Dai L, Jin X, Qi S, Yin Z. ER stress induced extracellular vesicles secretion from macrophages promotes calcium oxalate crystals formation in kidney. Mol Biomed. 2025;6(1):110. doi:10.1186/s43556-025-00351-x
52. Deng J, Yu B, Chang Z, et al. Cerium oxide-based nanozyme suppresses kidney calcium oxalate crystal depositions via reversing hyperoxaluria-induced oxidative stress damage. J Nanobiotechnology. 2022;20(1):516. doi:10.1186/s12951-022-01726-w
53. Tian Y, Ye Z, Wang X, et al. MOF-818 Nanozyme Suppresses Calcium Oxalate Kidney Stones by Alleviating Oxidative Stress and Inflammatory Injury. Adv Healthcare Mater. 2025;14(8):2401574. doi:10.1002/adhm.202401574
54. He Y, Peng E, Ba X, et al. ROS Responsive Cerium Oxide Biomimetic Nanoparticles Alleviates Calcium Oxalate Crystals Induced Kidney Injury via Suppressing Oxidative Stress and M1 Macrophage Polarization. Small. 2025;21(3):2405417. doi:10.1002/smll.202405417
55. Peng QL, Li CY, Zhao YW, Sun XY, Liu H, Ouyang JM. Protective Effect of Degraded Porphyra yezoensis Polysaccharides on the Oxidative Damage of Renal Epithelial Cells and on the Adhesion and Endocytosis of Nanocalcium Oxalate Crystals. Oxid Med Cell Longev. 2021;2021:6463281. doi:10.1155/2021/6463281
56. Lieske JC, Swift H, Martin T, Patterson B, Toback FG. Renal epithelial cells rapidly bind and internalize calcium oxalate monohydrate crystals. Proc Natl Acad Sci U S A. 1994;91(15):6987–6991. doi:10.1073/pnas.91.15.6987
57. Lieske JC, Norris R, Swift H, Toback FG. Adhesion, internalization and metabolism of calcium oxalate monohydrate crystals by renal epithelial cells. Kidney Int. 1997;52(5):1291–1301. doi:10.1038/ki.1997.454
58. Petrović A, Kizivat T, Ćurčić IB, Smolić R, Smolić M. In Vitro Cell Culture Models of Hyperoxaluric States: calcium Oxalate and Renal Epithelial Cell Interactions. Crystals. 2021;11(7):735. doi:10.3390/cryst11070735
59. Li CY, Liu L, Zhao YW, et al. Repair of Tea Polysaccharide Promotes the Endocytosis of Nanocalcium Oxalate Monohydrate by Damaged HK-2 Cells. Oxid Med Cell Longev. 2020;2020:2198976. doi:10.1155/2020/2198976
60. Zhao YW, Liu L, Li CY, Zhang H, Sun XY, Ouyang JM. Preprotection of Tea Polysaccharides with Different Molecular Weights Can Reduce the Adhesion between Renal Epithelial Cells and Nano-Calcium Oxalate Crystals. Oxid Med Cell Longev. 2020;2020:1817635. doi:10.1155/2020/1817635
61. Xiong P, Cheng XY, Sun XY, Chen XW, Ouyang JM. Interaction between nanometer calcium oxalate and renal epithelial cells repaired with carboxymethylated polysaccharides. Biomater Adv. 2022;137:212854. doi:10.1016/j.bioadv.2022.212854
62. Wang Z, Liu L, Zhao YW, Tong XY, Tang GH, Ouyang JM. Carboxymethylated Desmodium styracifolium polysaccharide reduces the risk of calcium oxalate kidney stone formation by inhibiting crystal adhesion and promoting crystal endocytosis. J Cell Physiol. 2024;239(6):e31272. doi:10.1002/jcp.31272
63. He TQ, Wang Z, Li CY, et al. Sulfated Laminarin Polysaccharides Reduce the Adhesion of Nano-COM Crystals to Renal Epithelial Cells by Inhibiting Oxidative and Endoplasmic Reticulum Stress. Pharmaceuticals. 2024;17(6):805. doi:10.3390/ph17060805
64. Xu QS, Wu ZJ, Sun JM, Liu JH, Huang WB, Ouyang JM. Different Degrees of Sulfated Laminaria Polysaccharides Recovered Damaged HK-2 Cells and Inhibited Adhesion of Nano-COM and Nano-COD Crystals. Bioinorg Chem Appl. 2024;2024:8843214. doi:10.1155/2024/8843214
65. Chen XW, Zheng YY, Ouyang JM. Sulfated Undaria pinnatifida Polysaccharide Promotes Endocytosis of Nano-Calcium Oxalate Dihydrate by Repairing Subcellular Organelles in HK-2 Cells. Antioxidants. 2023;12(5):1015. doi:10.3390/antiox12051015
66. Sun XY, Ouyang JM, Yu K. Shape-dependent cellular toxicity on renal epithelial cells and stone risk of calcium oxalate dihydrate crystals. Sci Rep. 2017;7:7250. doi:10.1038/s41598-017-07598-7
67. Sun XY, Xu M, Ouyang JM. Effect of Crystal Shape and Aggregation of Calcium Oxalate Monohydrate on Cellular Toxicity in Renal Epithelial Cells. ACS Omega. 2017;2(9):6039–6052. doi:10.1021/acsomega.7b00510
68. Liu JH, Zheng YY, Ouyang JM. Antioxidant Activities and Cytotoxicity of the Regulated Calcium Oxalate Crystals on HK-2 Cells of Polysaccharides from Gracilaria lemaneiformis with Different Molecular Weights. Foods. 2023;12(5). doi:10.3390/foods12051031
69. Su X, Yang Y, Xiang H, et al. Supplemental exposure to polystyrene nanoplastics synergistically amplifies calcium oxalate crystal–induced injury to renal tubular epithelium, accelerating the formation of calcium oxalate kidney stones. Part Fibre Toxicol. 2026;23(1):8. doi:10.1186/s12989-026-00661-0
70. Sabiu G, Kasinath V, Jung S, Li X, Tsokos GC, Abdi R. Targeted nanotherapy for kidney diseases: a comprehensive review. Nephrol Dial Transplant. 2022;38(6):1385–1396. doi:10.1093/ndt/gfac233
71. Qin W, Huang J, Zhang M, et al. Nanotechnology-Based Drug Delivery Systems for Treating Acute Kidney Injury. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11480945/.
72. Zhang C, Xiang Z, Yang P, Zhang L, Deng J, Liao X. Advances in Nano-Immunomodulatory Systems for the Treatment of Acute Kidney Injury. Adv Sci. 2025;12(17):2409190. doi:10.1002/advs.202409190
73. Shang S, Li X, Wang H, et al. Targeted therapy of kidney disease with nanoparticle drug delivery materials. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10979125/.
74. Huang LF, Ye QR, Chen XC, et al. Research Progress of Drug Delivery Systems Targeting the Kidneys. Pharmaceuticals. 2024;17(5):625. doi:10.3390/ph17050625
75. Chen D, Xu J, Lv S, et al. Enzyme-activatable kidney-targeted dendrimer-drug conjugate for efficient childhood nephrotic syndrome therapy. Theranostics. 2024;14(18):6991–7006. doi:10.7150/thno.101606
76. Yuan F, Lerman LO. Targeted therapeutic strategies for the kidney. Expert Opin Ther Targets. 2024;28(11):979–989. doi:10.1080/14728222.2024.2421756
77. Wang S, Zeng N, Wang Y, Yang Y. Engineering Kidney-Targeted Drug Delivery Systems: principles, Materials, and Emerging Strategies. Int J Nanomed. 2026;21:582804. doi:10.2147/IJN.S582804
78. Deng Y, Liu Z, Zhu X, Wang Y, Feng X, Yang J. Kidney-targeted nanoplatforms: strategies and applications. Theranostics. 2026;16(6):3011–3031. doi:10.7150/thno.126217
79. Li H, Dai W, Xiao L, Sun L, He L. Biopolymer-Based Nanosystems: potential Novel Carriers for Kidney Drug Delivery. Pharmaceutics. 2023;15(8):2150. doi:10.3390/pharmaceutics15082150
80. Chen Z, Peng H, Zhang C. Advances in kidney-targeted drug delivery systems. Int J Pharm. 2020;587:119679. doi:10.1016/j.ijpharm.2020.119679
81. Ba X, Ye T, He Y, et al. Engineered macrophage membrane-coated nanoparticles attenuate calcium oxalate nephrocalcinosis-induced kidney injury by reducing oxidative stress and pyroptosis. Acta Biomater. 2025;195:479–495. doi:10.1016/j.actbio.2025.02.021
82. Sun D, Zhao J, Ma Y, et al. Stem Cell Membrane Biomimetic Nano-Formulation Achieves the Delivery of MKP5 to Ameliorate Diabetic Kidney Disease via the P38 and ERK Pathway. THE FASEB Journal. 2025;39(18). doi:10.1096/fj.202501936R
83. Thongboonkerd V. Roles for Exosome in Various Kidney Diseases and Disorders. Front Pharmacol. 2020;10:1655. doi:10.3389/fphar.2019.01655
84. Vasylaki A, Ghosh P, Jaimes EA, Williams RM. Targeting the Kidneys at the Nanoscale: nanotechnology in Nephrology. Kidney360. 2024;5(4):618–630. doi:10.34067/KID.0000000000000400
85. Azimizonuzi H, Ghayourvahdat A, Ahmed MH, et al. A state-of-the-art review of the recent advances of theranostic liposome hybrid nanoparticles in cancer treatment and diagnosis. Cancer Cell Int. 2025;25(1):26. doi:10.1186/s12935-024-03610-z
86. Allen TM, Cullis PR. Liposomal drug delivery systems: from concept to clinical applications. Adv Drug Delivery Rev. 2013;65(1):36–48. doi:10.1016/j.addr.2012.09.037
87. Gatto MS, Johnson MP, Najahi-Missaoui W. Targeted Liposomal Drug Delivery: overview of the Current Applications and Challenges. Life. 2024;14(6):672. doi:10.3390/life14060672
88. Wu Q, Wang J, Wang Y, et al. Targeted delivery of celastrol to glomerular endothelium and podocytes for chronic kidney disease treatment. Nano Res. 2022;15(4):3556–3568. doi:10.1007/s12274-021-3894-x
89. Gabizon AA, Gabizon-Peretz S, Modaresahmadi S, et al. Thirty years from FDA approval of pegylated liposomal doxorubicin (Doxil/Caelyx): an updated analysis and future perspective. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11751825/.
90. Rachamala HK. Translational Advances in Lipid Nanoparticle Drug Delivery Systems for Cancer Therapy: current Status and Future Horizons. Pharmaceutics. 2025;17(10):1315. doi:10.3390/pharmaceutics17101315
91. Song S, Baek J, Seo S. A Comprehensive Dataset of Lipid Nanoparticle Compositions and Properties for Nucleic Acid Delivery. Scientific Data. 2025;13(1):139. doi:10.1038/s41597-025-06456-w
92. Khabbazian A, Kwong L, Lewis A, et al. Kidney Stone Dissolution By Tetherless, Enzyme-Loaded, Soft Magnetic Miniature Robots. Adv Healthc Mater. 2025;14(23):2403423. doi:10.1002/adhm.202403423
93. Gu X, Tai Y, Liu Z, et al. Layer-by-Layer Assembly of Renal-Targeted Polymeric Nanoparticles for Robust Arginase-2 Knockdown and Contrast-Induced Acute Kidney Injury Prevention. Adv Healthcare Mater. 2024;13(20):2304675. doi:10.1002/adhm.202304675
94. Alallam B, Choukaife H, Seyam S, Lim V, Alfatama M. Advanced Drug Delivery Systems for Renal Disorders. Gels. 2023;9(2):115. doi:10.3390/gels9020115
95. Ba X, Yang X, He Y, et al. Citrate-coated Prussian blue nanozyme hitchhikes neutrophils to ameliorate calcium oxalate crystal-induced kidney injury via inhibiting pyroptosis and NETosis. J Nanobiotechnology. 2026;24(1):223. doi:10.1186/s12951-026-04087-w
96. Ma Y, Pan J, Ju C, et al. Antioxidant nanozymes: current status and future perspectives in spinal cord injury treatments. Theranostics. 2025;15(13):6146–6183. doi:10.7150/thno.114836
97. Huang H-S, Ma M-C, Seguro AC. High Sodium-Induced Oxidative Stress and Poor Anticrystallization Defense Aggravate Calcium Oxalate Crystal Formation in Rat Hyperoxaluric Kidneys. PLoS One. 2015;10(8):e0134764. doi:10.1371/journal.pone.0134764
98. Houlihan I, Kang B, Krishna V, De S. Proof-of-concept for a novel nanotechnology-based treatment for urolithiasis. Urolithiasis. 2024;52(1):60. doi:10.1007/s00240-024-01564-5
99. Belle JD, Chen R, Srikureja N, Amasyali AS, Keheila M, Baldwin DD. Does the Novel Thulium Fiber Laser Have a Higher Risk of Urothelial Thermal Injury than the Conventional Holmium Laser in an In Vitro Study? J Endourol. 2022;36(9):1249–1254. doi:10.1089/end.2021.0842
100. Chen R, Song Y, Liu Y, Li J, Qin C, Xu T. Efficacy and safety of thulium fiber laser versus holmium: yttrium-aluminum-garnet laser in lithotripsy for urolithiasis: a systematic review and meta-analysis. Urolithiasis. 2025;53(1):33. doi:10.1007/s00240-025-01709-0
101. Peng Y, Liu M, Ming S, et al. Safety of a Novel Thulium Fiber Laser for Lithotripsy: an In Vitro Study on the Thermal Effect and Its Impact Factor. J Endourol. 2020;34(1):88–92. doi:10.1089/end.2019.0426
102. Uleri A, Farré A, Izquierdo P, et al. Thulium Fiber Laser Versus Holmium:Yttrium Aluminum Garnet for Lithotripsy: a Systematic Review and Meta-analysis. Eur Urol. 2024;85(6):529–540. doi:10.1016/j.eururo.2024.01.011
103. Mishra A, Margolin EJ, Stewart AW, et al. Optimizing Fragmentation while Minimizing Thermal Injury Risk with the Thulium Fiber Laser in Ureteral Stone Lithotripsy: an In Vitro Study. J Endourol. 2025;39(7):698–707. doi:10.1089/end.2024.0637
104. Shastri S, Patel J, Sambandam KK, Lederer ED. Kidney Stone Pathophysiology, Evaluation and Management: core Curriculum 2023. Am J Kidney Dis. 2023;82(5):617–634. doi:10.1053/j.ajkd.2023.03.017
105. Shabnum SS, Siranjeevi R, Raj CK, et al. Advancements in nanotechnology-driven photodynamic and photothermal therapies: mechanistic insights and synergistic approaches for cancer treatment. RSC Adv. 2024;14(52):38952–38995. doi:10.1039/d4ra07114j
106. Ye Z, Tian Y, Guan H, et al. Harnessing hollow Prussian blue nanozymes for efficient photothermal lithotripsy while protecting the kidneys from oxidative stress injury. Mater Today Bio. 2025;35:102467. doi:10.1016/j.mtbio.2025.102467
107. Kf C, Tj P, Jm T, et al. A perspective on laser lithotripsy: the fragmentation processes. Available from: https://pubmed.ncbi.nlm.nih.gov/11339391/.
108. Taguchi K, Okada A, Unno R, Hamamoto S, Yasui T. Macrophage Function in Calcium Oxalate Kidney Stone Formation: a Systematic Review of Literature. Front Immunol. 2021;12:673690. doi:10.3389/fimmu.2021.673690
109. Yao C, Zhang D, Wang H, Zhang P. Recent Advances in Cell Membrane Coated-Nanoparticles as Drug Delivery Systems for Tackling Urological Diseases. Pharmaceutics. 2023;15(7):1899. doi:10.3390/pharmaceutics15071899
110. Liu H, Su YY, Jiang XC, Gao JQ. Cell membrane-coated nanoparticles: a novel multifunctional biomimetic drug delivery system. Drug Deliv Transl Res. 2023;13(3):716–737. doi:10.1007/s13346-022-01252-0
111. Chen Q, Zhang L, Li L, et al. Cancer cell membrane-coated nanoparticles for bimodal imaging-guided photothermal therapy and docetaxel-enhanced immunotherapy against cancer. J Nanobiotechnology. 2021;19(1):449. doi:10.1186/s12951-021-01202-x
112. Axelsson O, Yousefpour N, Björnberg O, Ekengard E, Lekmeechai S. Size-dependent renal filtration model explains human pharmacokinetics of a functional nanoparticle: the SPAGOPIX-01 clinical trial. Nanomed Nanotechnol Biol Med. 2024;62:102774. doi:10.1016/j.nano.2024.102774
113. Wu M, Sun Z, Shi P, et al. Enhanced Electrochemical Sensing of Oxalic Acid Based on VS2 Nanoflower-Decorated Glassy Carbon Electrode Prepared by Hydrothermal Method. Biosensors. 2024;14(8):387. doi:10.3390/bios14080387
114. Sun K, Zhao N, Shi P, et al. Early Detection and Monitoring of Nephrolithiasis: the Potential of Electrochemical Sensors. Sensors. 2025;25(8):2547. doi:10.3390/s25082547
115. Jung HD, Seo IY, Lee JY. Large database study of urinary stone composition in South Korea: korean Society of Endourology and Robotics (KSER) research series. Investig Clin Urol. 2021;62(4):462–469. doi:10.4111/icu.20210039
116. Tostivint IN, Castiglione V, Alkouri R, et al. How useful is an oral calcium load test for diagnosing recurrent calcium stone formers? Urolithiasis. 2022;50(5):577–587. doi:10.1007/s00240-022-01355-w
117. Chen P, Bai Y, Tang Y, et al. Rapid and highly sensitive visual detection of oxalate for metabolic assessment of urolithiasis via selective recognition reaction of CdTe quantum dots. Journal of Materials Chemistry B. 2020;8(34):7677–7684. doi:10.1039/D0TB01108H
118. Jiang X, Bai Y, Liu Q, et al. Three-fluorescence sensor for minute-time scale low-cost analysis of urinary oxalate in urolithiasis metabolic assessment. Anal Chim Acta. 2023;1237:340586. doi:10.1016/j.aca.2022.340586
119. Chen P, Cen L, Wang Y, Bai Y, Shi T, Chen X. Rapid binary visual detection of oxalate in urine samples of urolithiasis patients via competitive recognition and distance reading test strips. Journal of Materials Chemistry B. 2023;11(11):2530–2537. doi:10.1039/D2TB02666J
120. Yu R, Zhao Y, Liu J. Solid Electrochemiluminescence Sensor by Immobilization of Emitter Ruthenium(II)tris(bipyridine) in Bipolar Silica Nanochannel Film for Sensitive Detection of Oxalate in Serum and Urine. Nanomaterials. 2024;14(5):390. doi:10.3390/nano14050390
121. Crapnell RD, Adarakatti PS, Banks CE. Electroanalytical Overview: the Electroanalytical Detection of Oxalate. Sensors Actuators Rep. 2023;6:100176. doi:10.1016/j.snr.2023.100176
122. Estève E, Buob D, Jamme F, et al. Detection and localization of calcium oxalate in kidney using synchrotron deep ultraviolet fluorescence microscopy. J Synchrotron Radiat. 2022;29(Pt 1):214–223. doi:10.1107/S1600577521011371
123. Courbebaisse M, Travers S, Bouderlique E, et al. Hydration for Adult Patients with Nephrolithiasis: specificities and Current Recommendations. Nutrients. 2023;15(23):4885. doi:10.3390/nu15234885
124. Ferraro PM, Taylor EN, Curhan GC. 24-Hour Urinary Chemistries and Kidney Stone Risk. Available from: https://www.ajkd.org/article/S0272-6386(24)00693-0/fulltext.
125. Desai AC, Maalouf NM, Harper JD, et al. Prevention of Urinary Stones with Hydration: a Randomised Clinical Trial of an Adherence Intervention. Lancet. 2026;407(10534):1171–1181. doi:10.1016/S0140-6736(25)02637-6
126. Dissayabutra T, Anegkamol W, Ratchanon S, et al. Lime-based supplement reduces calcium oxalate stone recurrence: a multicenter randomized controlled trial. PLoS One. 2025;20(12):e0336892. doi:10.1371/journal.pone.0336892
127. Liu JH, Ouyang JM. Synergistic inhibition of calcium oxalate crystal formation and synergistic protection of HK-2 cells from crystal damage by sulfated Laminarin polysaccharide and potassium citrate. Biomater Sci. 2023;11(10):3524–3546. doi:10.1039/D3BM00087G
128. Zomorodian A, Moe OW. Citrate and calcium kidney stones. Clin Kidney J. 2025;18(9):sfaf244. doi:10.1093/ckj/sfaf244
129. Schoales Z, Ghosh P, Vasylaki A, et al. Pathways to translation for nanomedicine in nephrology. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12461149/.
130. Zhang M, Xie F, Zhou F. The impact of intestinal microbiota-derived metabolites on cancer and their potential application in tumor immunotherapy. MedComm – Future Medicine. 2024;3(3):e92. doi:10.1002/mef2.92
131. de Vlieger JSB, Crommelin DJA, Tyner K, et al. Report of the AAPS Guidance Forum on the FDA Draft Guidance for Industry: “Drug Products, Including Biological Products, that Contain Nanomaterials. AAPS J. 2019;21(4):56. doi:10.1208/s12248-019-0329-7
132. Clogston JD, Foss W, Harris D, et al. Current state of Nanomedicine Drug Products: an Industry Perspective. J Pharm Sci. 2024;113(12):3395–3405. doi:10.1016/j.xphs.2024.09.005
133. Tzelves L, Berdempes M, Mourmouris P, Mitsogiannis I, Skolarikos A. Optimal Delivery of Follow-Up Care for the Prevention of Stone Recurrence in Urolithiasis Patients: improving Outcomes. Res Rep Urol. 2022;14:141–148. doi:10.2147/RRU.S277498
134. Wang J, Zhao W, Zhang Z, et al. A Journey of Challenges and Victories: a Bibliometric Worldview of Nanomedicine since the 21st Century. Adv Mater. 2024;36(15):e2308915. doi:10.1002/adma.202308915
135. Qin S, Wu B, Gong T, Zhang ZR, Fu Y. Targeted delivery via albumin Corona nanocomplex to renal tubules to alleviate acute kidney injury. J Control Release. 2022;349:401–412. doi:10.1016/j.jconrel.2022.07.013
136. Adhipandito CF, Cheung SH, Lin YH, Wu SH. Atypical Renal Clearance of Nanoparticles Larger Than the Kidney Filtration Threshold. Int J Mol Sci. 2021;22(20):11182. doi:10.3390/ijms222011182
137. Calé A, Elblová P, Andělová H, Lunova M, Lunov O. Analyzing Molecular Determinants of Nanodrugs’ Cytotoxic Effects. Int J Mol Sci. 2025;26(14):6687. doi:10.3390/ijms26146687
138. Chew BH, Harper JD, Sur RL, et al. Break Wave Lithotripsy for Urolithiasis: results of the First-in-Human International Multi-Institutional Clinical Trial. J Urol. 2024;212(4):580–589. doi:10.1097/JU.0000000000004091
139. Musazzi UM, Franzè S, Condorelli F, Minghetti P, Caliceti P. Feeding Next-Generation Nanomedicines to Europe: regulatory and Quality Challenges. Adv Healthc Mater. 2023;12(30):2301956. doi:10.1002/adhm.202301956
140. Huang G, Chen X, Liao C. AI-Driven Wearable Bioelectronics in Digital Healthcare. Biosensors. 2025;15(7):410. doi:10.3390/bios15070410
141. Mazumdar H, Khondakar KR, Das S, Halder A, Kaushik A. Artificial intelligence for personalized nanomedicine; from material selection to patient outcomes. Expert Opin Drug Delivery. 2025;22(1):85–108. doi:10.1080/17425247.2024.2440618
142. Hill F, Sayer JA. Precision medicine in renal stone-formers. Urolithiasis. 2019;47(1):99–105. doi:10.1007/s00240-018-1091-5
143. Payne NG, Boddu SP, Wymer KM, et al. The Use of Genetic Testing in Nephrolithiasis Evaluation: a Retrospective Review From a Multidisciplinary Kidney Stone Clinic. Available from: https://www.goldjournal.net/article/S0090-4295(24)00595-8/abstract.
144. Geraghty R, Lovegrove C, Howles S, Sayer JA. Role of Genetic Testing in Kidney Stone Disease: a Narrative Review. Curr Urol Rep. 2024;25(12):311–323. doi:10.1007/s11934-024-01225-5
145. Hsi RS, Zhang S, Triozzi JL, Hung AM, Xu Y, Bejan CA. Evaluation of Genetic Associations with Clinical Phenotypes of Kidney Stone Disease. Eur Urol Open Sci. 2024;67:38–44. doi:10.1016/j.euros.2024.07.109
146. Sameh A, Rostami M, Oussalah M, Korpelainen R, Farrahi V. Digital phenotypes and digital biomarkers for health and diseases: a systematic review of machine learning approaches utilizing passive non-invasive signals collected via wearable devices and smartphones. Artif Intell Rev. 2024;58(2):66. doi:10.1007/s10462-024-11009-5
147. Li P, Li Y, Yang B, Zhang X, Li J. Machine learning algorithms in predicting the recurrence of renal stones using clinical data. Urolithiasis. 2023;52(1):12. doi:10.1007/s00240-023-01516-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Awareness and Predictors of the Use of Bioinformatics in Genome Research in Saudi Arabia
Alomair L, Abolfotouh MA
International Journal of General Medicine 2023, 16:3413-3425
Published Date: 11 August 2023
Current Dietary and Medical Prevention of Renal Calcium Oxalate Stones
Wang X, Wang Q
International Journal of General Medicine 2024, 17:1635-1649
Published Date: 29 April 2024
Nanomaterial-Enhanced Immunotherapy: Advancing T-Cell-Based Treatments for Bladder Cancer
Chen J, Fu Y, Zhang Z, Zhao J, Zuo J, Ye X, Xiong Q, Nie Z, Dong H, Shi H, Tan Z, Wang C, Chen B, Wang Z, Li X, Chen P, Wang H, Fu S
International Journal of Nanomedicine 2025, 20:15235-15275
Published Date: 18 December 2025
How Effective are Nanotechnology-Based Therapeutics to Treat Autoimmune Diseases
Barakat M, Abu Ershaid JM, Alzaghari LF, Abdulrazzaq SB, Raad D, Hasen E, Al-Qudah RA, Chellappan DK, Athamneh T, Al-Najjar MAA, Ashames A
International Journal of Nanomedicine 2026, 21:562959
Published Date: 20 January 2026
Peptide-Based Nanocarriers for Targeted Drug Delivery: Recent Advances, Strategies, and Therapeutic Frontiers
Adnan SB, Lim F, Ahmad H, Maarof M, Fauzi MB, Md Fadilah NI
International Journal of Nanomedicine 2026, 21:588558
Published Date: 27 March 2026