Back to Journals » Journal of Pain Research » Volume 18
The Analgesic Effect of Low-Dose S(+)-Ketamine in Knee Joint Replacement: A Randomized Controlled Trial
Authors Deng SY, Song X, Chen LN, Zhao F, Guo L
Received 10 June 2025
Accepted for publication 19 October 2025
Published 4 November 2025 Volume 2025:18 Pages 5815—5826
DOI https://doi.org/10.2147/JPR.S545997
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Shi-Yuan Deng, Xiao Song, Li-Na Chen, Fei Zhao, Liang Guo
Department of Anesthesiology and Perioperative Medicine, The First Affiliated Hospital of Shandong First Medical University (Shandong Provincial Qianfoshan Hospital), Jinan, Shandong, 250014, People’s Republic of China
Correspondence: Liang Guo, Department of Anesthesiology and Perioperative Medicine, The First Affiliated Hospital of Shandong First Medical University (Shandong Provincial Qianfoshan Hospital), No. 16766 Jingshi Road, Jinan, Shandong, 250014, People’s Republic of China, Email [email protected]
Background: Insufficient pain relief during knee joint replacement surgery can have adverse effects on the postoperative recovery of the patient. In this study, we evaluated the analgesic effect of intravenous infusion of low-dose S(+)-ketamine in patients following knee joint replacement surgery.
Methods: This study was a randomized, single-blind, placebo-controlled trial involving 144 patients who underwent knee joint replacement. Patients were randomly assigned to receive an intravenous infusion of S(+)-ketamine (0.3 mg/kg/h) or 0.9% sodium chloride solution. The primary efficacy endpoint was evaluated based on NRS scores at 2 h, 24 h, and 48 h after surgery. Additionally, the intraoperative doses of sufentanil, propofol, and remifentanil were investigated. The number of patients who required analgesic rescue and the number of patients who experienced adverse reactions within 48 h postoperatively were recorded.
Results: S(+)-ketamine reduced NRS scores for movement pain at 2 h [2.36 ± 0.66 vs 3.1 ± 0.65, P < 0.001], 24 h [2.15 ± 0.62 vs 2.79 ± 0.85, P < 0.001], and 48 h [1.81 ± 0.6 vs 2.29 ± 0.76, P < 0.001] postoperatively. Administering S(+)-ketamine reduced the dose of sufentanil [30 (30, 35) vs 40 (35, 40), P < 0.001] but not propofol [333.68 ± 75.02 vs 323.06 ± 79.94, P = 0.412] or remifentanil [1.8 (1.4, 2.2) vs 1.6 (1.325, 2), P = 0.131]. The use of intraoperative S(+)-ketamine significantly reduced the patient proportion of requiring additional analgesics postoperatively (4.2% vs 19.4%, P = 0.004). A lower incidence of dizziness (1.4% vs 12.5%, P = 0.009), nausea (11.1% vs 29.2%, P < 0.001), and vomiting (8.3% vs 29.2%, P = 0.001) was found in patients treated with S(+)-ketamine (P < 0.05).
Conclusion: Intravenous infusion of S(+)-ketamine during surgery of elderly patients undergoing knee joint replacement can alleviate postoperative acute pain, providing research support for the application of S(+)-ketamine in multimodal analgesia.
Trial Registration: NCT05289050.
Keywords: S(+)-ketamine, total knee arthroplasty surgery, elderly patients, analgesia, pain
Introduction
As the aging population and obesity rates keep increasing, the number of patients opting for total knee arthroplasty (TKA) is increasing worldwide.1–5 TKA is regarded as the safest and most effective method for treating patients with end-stage knee osteoarthritis.6 Analgesic strategies, including nonsteroidal anti-inflammatory drugs (NSAIDs), opioids, and nerve blocks, are commonly used to alleviate acute postoperative pain following knee joint replacement.7–9 However, about 50% of patients experience severe postoperative acute pain.10 Inadequate analgesia adversely affects postoperative recovery, and the extensive use of opioids can lead to side effects such as nausea and vomiting.11 Postoperative pain can prolong the patient’s hospitalization time, affect their recovery, and increase the burden of medical expenses. Therefore, exploring more effective pain management strategies is crucial for postoperative rehabilitation of patients underwent TKA.
S(+)-ketamine, an N-methyl-D-aspartate (NMDA) receptor antagonist rapidly alleviates depression and anxiety in patients.12,13 Additionally, as part of a multimodal analgesia approach, S(+)-ketamine is safe and reliable. It can stabilize hemodynamic fluctuations during the perioperative period, reduce inflammatory responses, and has neuroprotective effects.14 At present, S(+)-ketamine is widely utilized as an adjunct to general anesthesia for managing acute pain during the perioperative period.15–17 Hireno Guará Sobrinho et al found that the lowest dose of intra-articular S(+)-ketamine (0.25mg.kg) resulted in better pain scores and less rescue analgesia, with longer time to first request.18 However, Touil et al found that an anti-hyperalgesic dose of ketamine failed to prevent the development of rebound pain.19 While a study of Li et al found S(+)-ketamine effectively reduces the risk of rebound pain and early pain levels, improves patient satisfaction, and enhances recovery quality.20 The efficacy and safety of S(+)-ketamine in relieving pain and reducing analgesic consumption in surgical patients are still uncertain. Some studies have shown that low-dose S(+)-ketamine can reduce the incidence of side effects (such as induced hypotension) of high-dose opioids by stimulating the sympathetic nervous system, providing analgesia, and exerting an antagonistic effect on NMDA receptors.15 Although low-dose S(+)-ketamine has been shown to be beneficial in pain management after various surgeries, there is no consensus regarding the effectiveness of an S(+)-ketamine analgesic combined with opioids in older patients with knee arthroplasty. In addition, the appropriate administration duration and dose of S(+)-ketamine to achieve pain relief in older patients are unknown. A double-blind, randomized, placebo-controlled trial showed that continuous S(+)-ketamine infusion (0.3 mg/kg/h) during laparoscopic cholecystectomy under target-controlled intravenous anesthesia provided better postoperative pain control than placebo, reducing morphine requirement.21 Therefore, we conducted a randomized, single-blind, placebo-controlled trial to investigate the effects of intraoperative administration of S(+)-ketamine on early postoperative pain in elderly patients undergoing knee joint replacement.
Material and Methods
Study Design
This study was a single-center, single-blind, randomized controlled trial.22 This clinical study was conducted at the First Affiliated Hospital of Shandong First Medical University. This study was approved by the Ethics Committee of The First Affiliated Hospital of Shandong First Medical University (YXLL-KY-2021(077)) and was registered at https://clinicaltrials.gov (NCT05289050). All patients signed an informed consent document before participating in the study. The study was conducted in accordance with the Declaration of Helsinki.23
Participants
The participants included elderly patients who underwent knee joint replacement surgery under general anesthesia at The First Affiliated Hospital of Shandong First Medical University from April 2022 to September 2022. The inclusion criteria were as follows: (1) Patients who underwent unilateral total knee joint replacement surgery under general anesthesia; (2) Elderly patients (aged ≥ 65 years), regardless of sex; (3) BMI between 18 kg/m2 and 30 kg/m2; (4) No psychiatric disorders, normal consciousness, or ability to communicate effectively; (5) American Society of Anesthesiologists (ASA) classification I–III; (6) All patients had the entire surface of the femur, tibia, and patella of the knee joint replaced, and the prosthesis was fixed to the bone with bone cement. The exclusion criteria were as follows: (1) Untreated or poorly controlled hypertension, hyperthyroidism, or neurological or psychiatric disorders; (2) Patients had severe respiratory diseases and abnormal liver or kidney function; (3) Patients had allergies to the study drugs, including S(+)-ketamine and propofol; (4) Patients had a history of opioid or S(+)-ketamine addiction; (5) Patients who withdraw midway or are unable to complete the entire trial process; (6) Patients with incomplete information.
Power Analysis
NRS scores at different postoperative time points as the primary outcome. Based on previous studies, the difference in postoperative pain scores between the experimental group and the control group was at least 1.5. Using Power Analysis and Sample Size (PASS; NCSS, LLC, USA) 15 software. The sample size was calculated by comparing the mean values between the two groups: assuming a sample ratio of 1:1, a bilateral test, α = 0.05, and β = 0.20; with a standard deviation of 3. Considering a 10% loss to follow-up, the required number of cases for each group was 72, ie, 144 cases in total.
Randomization and Allocation Concealment
Using SPSS software, this study generated a random allocation sequence based on a preset 1:1 allocation ratio. Each patient’s allocation result was encoded as a unique identification code, printed and sealed in an unmarked, opaque envelope to achieve strict allocation concealment. After the patients were confirmed that they meet the inclusion criteria, independent third-party assistants who did not participate in the trial design, intervention implementation, or outcome evaluation will open the corresponding numbered envelopes in the order of inclusion. Based on the allocation code inside the envelopes, patients will be randomly assigned to the treatment group or control group in a 1:1 ratio.
Blinding
The day before the surgery, an anesthesiologist who has received clinical trial training will conduct a preoperative visit. He will determine the patients as the experimental group or control group based on a random list and provide a detailed explanation that “the trial will adopt a single blind design”, meaning patients may be assigned to the experimental group or control group, but the specific grouping will not be known. At the same time, patients should be informed of the purpose, process, risks, and benefits of the trial. Patients can choose to refuse this experiment without any concealment. Data management: Researchers’ records, such as case report forms, are regularly checked by a monitoring officer (CRA) to ensure that there are no suggestive language or group information leaks. Blinding rule: Establish clear conditions for blinding, and if a subject experiences serious adverse reactions, they must be immediately informed of the grouping for further treatment. After unblinding, the reason should be recorded and the subject should be excluded from the main analysis (if unblinding affects the results).
Interference
In the S(+)-ketamine group, an adductor canal block was performed with 0.375% ropivacaine (20 mL) under ultrasound guidance before anesthesia induction, followed by standard anesthesia induction. During anesthesia maintenance, an intravenous infusion of S(+)-ketamine (0.3 mg/kg/h) was administered.24 In the control group, an adductor canal block was also performed with 0.375% ropivacaine (20 mL) under ultrasound guidance before anesthesia induction, followed by standard anesthesia induction. During anesthesia maintenance, an intravenous infusion of an equivalent dose of 0.9% sodium chloride was administered. The successful sign of nerve block is: under ultrasound, the saphenous nerve can be seen located on the outer or inner side of the femoral artery, forming a spindle shaped or elliptical high echo structure, and the surrounding muscles can be seen as sartorius muscle, medial thigh muscle, and adductor magnus muscle. The nerve stimulation needle breaks through the adductor muscle membrane, and after the breakthrough, the medication spreads in an elliptical shape around the artery.
Upon entering the operating room, routine monitoring of electrocardiogram, blood pressure, and anesthesia depth was conducted. The anesthesia method adopted was general anesthesia with a laryngeal mask. Induction involved administering dexamethasone (10 mg), midazolam (0.01–0.05 mg/kg), sufentanil (0.2–0.4 µg/kg), etomidate (0.15–0.3 mg/kg), and atracurium (0.3–0.6 mg/kg). After complete muscle relaxation occurred, a laryngeal mask was inserted (with different models selected based on body weight). General intravenous anesthesia maintenance was adopted. In the experimental group, 0.3 mg/kg/h S(+)-ketamine, propofol (4–12 mg/kg/h), and remifentanil (0.15–0.3 µg/kg/min) were administered using an intravenous pump. In the control group, an equivalent dose of 0.9% sodium chloride injection, propofol (4–12 mg/kg/h), and remifentanil (0.15–0.3 µg/kg/min) were also administered using an intravenous pump. Both groups received 8 mg of ondansetron hydrochloride intravenously during anesthesia induction to prevent postoperative nausea and vomiting. The pumping time of two groups started after anesthesia induction and stopped when the commencement of the final layer of skin closure. After the laryngeal mask was inserted, mechanical ventilation was adjusted, and respiratory parameters were set as follows: the tidal volume for the subject was 6–10 mL/kg, the respiratory rate was 10–14 breaths/min, and the PaCO2 was maintained at 30–35 mmHg. To ensure cerebral blood flow balance, the mean arterial pressure was maintained above 70 mmHg. If noninvasive blood pressure exceeded the baseline value of the participant by 10%, urapidil was administered for treatment. If the pressure was below 70 mmHg, norepinephrine was provided. All participants received a cocktail (1:1000 adrenaline 0.5 mg (0.5 mL) + 0.75% ropivacaine 10 mL + compounded betamethasone injection 7 mg (1 mL) + 0.9% sodium chloride 28.5 mL) for additional analgesia around the knee joint cavity after placement of the knee prosthesis. Drug infusion was stopped 15 min before the end of the surgery in both groups.
All patients underwent surgery under anesthesia by the same surgical anesthesia team. The general surgical procedure is as follows: (1) Disinfect and lay a cloth after anesthesia, make an incision along the front of the knee, separate soft tissue, and expose the knee joint capsule; (2) Cut open the cyst wall, dislocate the knee joint, remove the damaged meniscus, hypertrophic synovium, and osteophyte; (3) Accurately remove the diseased bone in the distal femur and proximal tibia according to the prosthesis model, and repair the joint surface; (4) Install femoral and tibial prostheses and pads, adjust force lines and tightness; (5) After rinsing, suture the incision layer by layer and cover it with dressing to complete the surgery. Starting from 24 hours after surgery, the patient will undergo functional training. (1) Ankle pump exercise: hook and extend the foot, repeat activities to promote blood circulation. (2) Raise straight legs: Lie flat, lift straight legs off the bed, hold for a few seconds, then lower them to strengthen the quadriceps. (3) Knee bending exercise: Sitting beside the bed, slowly bend the knee to a tolerable angle, then straighten and gradually increase the curvature. (4) Walking: Short distance slow walking in the early postoperative period, gradually increasing the duration and distance according to the recovery situation.
Observation Indicators
Primary Observation Indicators
At 2 h, 24 h, and 48 h postoperatively, the resting and movement numerical rating scale (NRS) scores were evaluated.25 Resting pain is defined as a rating of the patient’s supine position without exercise, while exercise pain refers to the pain state of full ankle extension, mild knee flexion exercise (sitting by the bed, with the lower leg naturally drooping and bending using gravity), and early use of walking aids to walk for 10 minutes in a single session. The NRS score quantifies the degree of pain based on self-reported numbers from patients, making it easier for healthcare professionals to accurately understand the pain conditions of patients. The NRS score divides pain levels into 0–10 points. A score of 0 points indicates no pain, and the patient does not feel any pain or discomfort. A score of 1–3 points indicates mild pain, the patient can tolerate it, and it has negligible effects on daily life and sleep. A score of 4–6 points indicates moderate pain, with a greater degree of pain. The patient may feel uncomfortable and may sleep, but it is usually tolerable. A score of 7–9 points indicates severe pain, characterized by the inability of the patient to tolerate it, serious effects on their daily life and sleep, and the need for emergency intervention. A score of 10 points indicates severe pain, with the patient experiencing extremely severe pain.
Secondary Observation Indicators
(1) Number of patients requiring analgesic rescue within 48 h postoperatively. According to the patient’s reported pain, the doctor provides corresponding treatment. Patients with moderate pain should be given 100 mg of tramadol hydrochloride sustained-release tablets orally or 40 mg of parecoxib sodium for intravenous injection. After relief, the administration time and dose should be recorded. If relief is not achieved, a single dose of 0.3 mg/kg of pethidine hydrochloride injection should be added and recorded. The total dose of tramadol hydrochloride sustained-release tablets within 24 hours should not exceed 400mg, the total dose of parecoxib sodium for injection within 24 hours should not exceed 80 mg, and the total dose of pethidine hydrochloride injection within 24 hours should not exceed 5 mg/kg. Patients who exceed the maximum dose of use are considered dropouts. Patients with severe pain should receive intravenous injection of 0.3 mg/kg pethidine hydrochloride, and the total dose should not exceed 5 mg/kg within 24 hours. Patients who exceed the maximum dosage will be considered as dropouts. If the patient experiences repeated pain, even worsening, and the use of the above drugs does not provide significant relief, we will promptly organize a consultation with anesthesiologists, associate chief orthopedic surgeons, and above to summarize and analyze, and provide the optimal analgesic plan. Simultaneously recorded as a dropped case. During our entire trial period, there were no patients who used the maximum dose of analgesics to relieve pain within 24 hours, or whose pain could not be relieved or even worsened after the maximum dose of medication.
(2) Incidence of adverse reactions (nausea, vomiting, nystagmus, dizziness, nightmares, hallucinations, and skin itching) within 48 h after the operation. Hallucination: defined as perceptual abnormalities (such as visual and auditory hallucinations); Nightmare: Abnormal dream content (such as terrifying scenes) accompanied by strong negative emotions; Nausea: discomfort in the upper abdomen; Vomiting: Forced expulsion of stomach contents. Once a serious adverse event occurs during the follow-up process, the researcher will take necessary treatment measures as soon as possible. If the type of medication needs to be specified for treatment, the emergency letter will be opened with the approval of the main researcher. After unblinding, the subject will be treated as a dropout case, and will be followed up until the Serious Adverse Event (SAE) is completely relieved, stabilized, or restored to baseline status.
Statistical Analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences 27.0 software (SPSS, Chicago, IL, USA) and R software (http://www.r-project.org/). For normally distributed quantitative data determined by the Kolmogorov–Smirnov test, statistical descriptions are presented as the mean ± standard deviation; differences between the two groups were determined by conducting the independent sample t-test. For non-normally distributed quantitative data, the median (interquartile range) was used for statistical description; differences between the two groups were determined by conducting the Mann–Whitney U-test. Categorical data were presented as frequencies and percentages, with differences determined by conducting the Chi-square test or Fisher’s exact probability method. The NRS scores at different time points between two groups were analyzed via Scheirer-Ray-Hare test. The changes of NRS scores at different time points were evaluated using Friedman test. Mann–Whitney U-test was performed to evaluate the difference of NRS scores at one point. The changes in continuous variables before and after surgery were assessed by paired rank-sum tests. Changes in categorical variables before and after surgery were evaluated by conducting paired Chi-square tests or Fisher’s exact probability tests. For all statistical analyses, bilateral tests were performed, with P < 0.05 considered to be statistically significant.
Results
Baseline Characteristics of the Patients
Between April 2022 and September 2022, 144 participants were recruited and analyzed for study outcomes. The flow chart of the recruitment of participants is presented in Figure 1. A total of 144 eligible participants were randomly divided into two groups: 72 patients in the S(+)-ketamine group and 72 patients in the control group. The baseline characteristics of these participants are shown in Table 1. The mean ages of the participants in the S(+)-ketamine and control groups were similar (68.22 ±3.003 for the S(+)-ketamine group vs 69.24 ± 3.282 for the control group). However, no significant differences were found in the average BMI (P > 0.05). Additionally, male-to-female ratios of 18:54 in the S(+)-ketamine group and 13:59 in the control group were found, but the differences were not significant (P > 0.05). No significant difference in height, time for anesthesia to dissipate, history of hypertension, history of diabetes, history of hyperthyroidism, and preoperative opioid was found between the S(+)-ketamine group and the control group (P > 0.05).
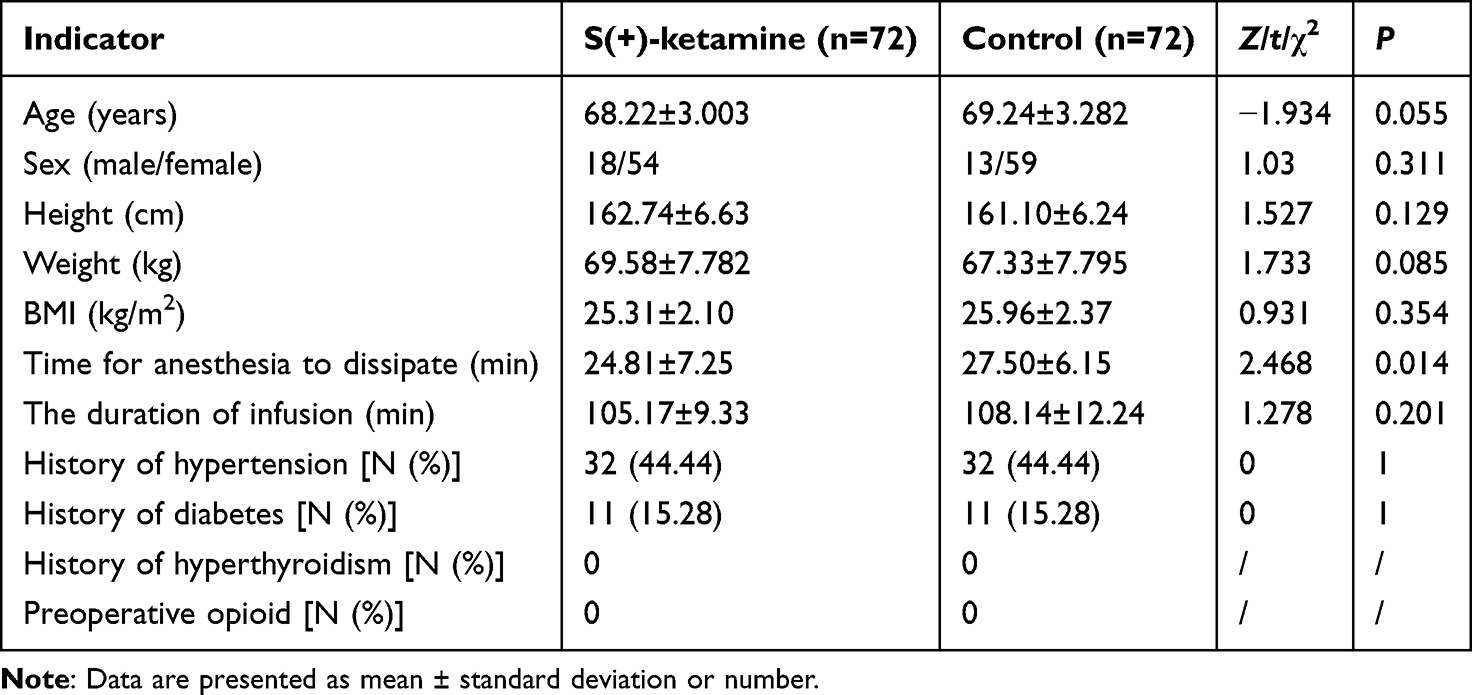 |
Table 1 Baseline Characteristics of the Patients |
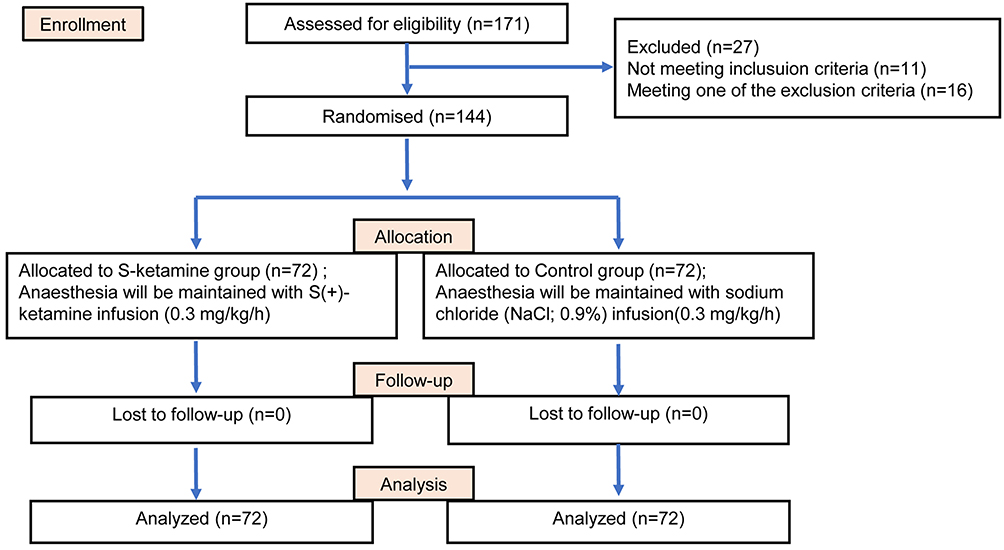 |
Figure 1 Flow diagram of the CONSORT trial. CONSORT, consolidated standards of reporting trials. |
Comparison of NRS Scores at Rest and During Movement at 2 h, 24 h, and 48 h Postoperatively
We investigated the changes in NRS scores at rest and during movement before the operation and at 2 hours, 24 hours and 48 hours after the operation. At baseline, the NRS scores for rest of the two groups of patients were similar (P > 0.05). After the operation, the NRS scores of the two groups of patients continued to decrease over time (P < 0.05). However, the trend of decreasing NRS scores for the two groups was similar (H = 1.331, P = 0.722). At 24 h and 48 h postoperatively, the NRS scores of the two groups of patients were similar, while the patients in the S(+)-ketamine group had significantly lower NRS scores at 2 h postoperatively than those in the control group (Table 2 and Figure 2A; P < 0.05).
 |
Table 2 Comparison of NRS Scores at Rest and During Movement at 2 h, 24 h, and 48 h Postoperatively |
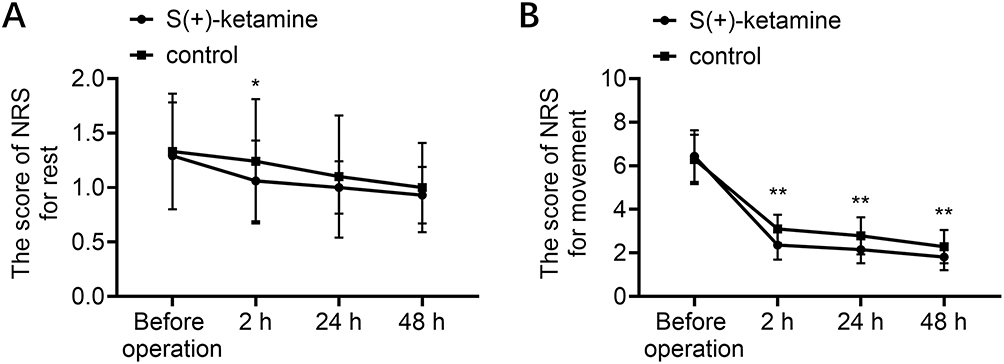 |
Figure 2 The NRS scores. The changes of NRS scores for rest (A) and movement (B) before the operation and at 2 hours, 24 hours and 48 hours after the operation. “*” indicates a significant difference when S(+)-ketamine group compared with the control group at the different time point. Statistical significance was set at *P < 0.05, **P < 0.001. |
At baseline, we found that the NRS scores for movement of the two groups of patients were similar (P > 0.05). The NRS score for movement pain in the two groups continued to decrease at 2 h, 24 h, and 48 h postoperatively (Table 2 and Figure 2B; P < 0.05). While S(+)-ketamine group showed a more significant decrease (H = 11.570, P = 0.009). The S(+)-ketamine group had significantly lower NRS scores for movement pain than the control group at 2 h postoperatively (Table 2 and Figure 2B; P < 0.05). Similar patterns were also found at 24 h and 48 h postoperatively (Table 2 and Figure 2B; P < 0.05).
Differences in Intraoperative Dosages of Sufentanil, Remifentanil, and Propofol Between the Two Groups
The quantitative results related to the intraoperative dosages of sufentanil, remifentanil, and propofol are presented in Table 3. The Mann–Whitney U-test revealed that patients in the S(+)-ketamine group required significantly lower doses of sufentanil (P < 0.001). However, no significant differences were found in the intraoperative dosages of remifentanil between the two groups (P > 0.05). Similar patterns were also found for propofol (P > 0.05).
 |
Table 3 Differences in Intraoperative Dosages of Sufentanil, Remifentanil, and Propofol Between the Two Groups |
Comparison of the Incidence of Postoperative Adverse Reactions Between the Two Groups
No chills, agitation, nystagmus, hallucinations, or skin itching were found in the recruited patients after surgery. In the S(+)-ketamine group, one patient experienced dizziness, with an incidence rate of 1.4%, 11.1% of patients (8/72) experienced nausea, and six patients (8.3%) experienced vomiting. In the control group, the incidence rates of dizziness, nausea, and vomiting were 12.5% (9/72), 29.2% (21/72), and 29.2% (21/72), respectively. The incidences of dizziness, nausea, and vomiting in the S(+)-ketamine group were significantly lower than those in the control group (P < 0.05). However, no significant difference in agitation, nystagmus, hallucinations, or skin itching was found between the S(+)-ketamine group and the control group (Table 4, P > 0.05).
 |
Table 4 Comparison of the Incidence of Postoperative Adverse Reactions Between the Two Groups |
The Number of Patients Requiring Additional Analgesics Postoperatively in the Two Groups
We compared the number of patients who required additional analgesics postoperatively between the two groups (Table 5). Compared to the control group (19.4%, 14/72), three patients (4.2%) in the study group needed additional analgesics postoperatively, and the difference was significant (P < 0.05).
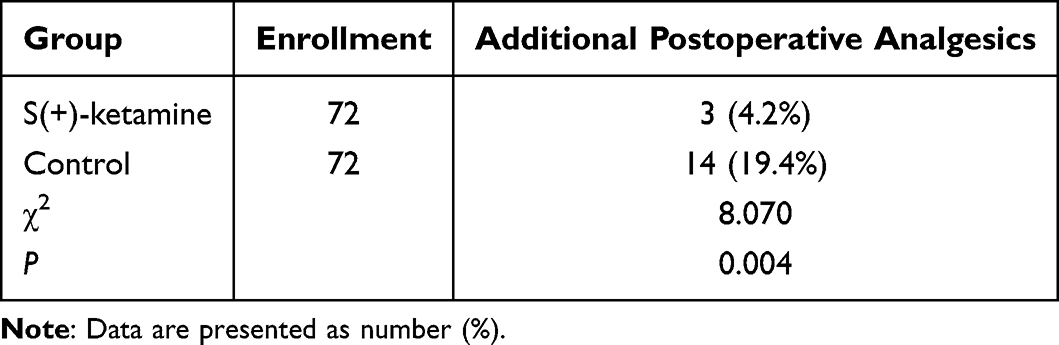 |
Table 5 The Number of Patients Requiring Additional Analgesics Postoperatively in the Two Groups |
Discussion
Owing to the release of many inflammatory substances, knee joint replacement surgery increases pain sensitivity in the central and peripheral nervous systems, with about 60% of patients experiencing severe postoperative pain and 30% experiencing moderate pain.26–28 Severe pain can hinder the willingness of patients to engage in early rehabilitation training, thereby affecting surgical outcomes. Inadequate management of postoperative pain may also lead to complications such as atelectasis, hypoxemia, and cardiovascular diseases.29,30 Although commonly used opioid analgesics can alleviate postoperative pain, using them in high doses may result in side effects such as nausea and vomiting, which can delay patient recovery.31 The multimodal analgesia approach developed under the ERAS concept provides new avenues for managing acute postoperative pain, playing an important role in reducing the dosage of opioids and their adverse effects on postoperative analgesia.32 We conducted a randomized, controlled, single-blind study to evaluate the effect of continuous infusion of low-dose S(+)-ketamine during surgery on postoperative pain in elderly patients who underwent knee joint replacement. This study demonstrated that continuous infusion of low-dose S(+)-ketamine during surgery contributed to a decrease in NRS scores for movement pain at 2 h, 24 h, and 48 h postoperatively. We also noted that the amount of sufentanil was reduced for patients who received S(+)-ketamine. The incidence of dizziness, nausea, and vomiting and the incidence of requiring additional analgesics postoperatively decreased significantly.
Compared to the racemic mixture of ketamine, the dextrorotatory isomer of ketamine (S(+)-ketamine) has about twice the affinity for N-methyl-D-aspartate receptors. Many recent studies have used S(+)-ketamine for treating acute and chronic pain. For example, Nielsen et al found that the intraoperative use of S(+)-ketamine can reduce analgesic consumption and postoperative pain.33 However, large-scale, prospective, randomized controlled trials are needed to verify the effect of S(+)-ketamine on postoperative pain after knee joint replacement. Therefore, we evaluated the efficacy of S(+)-ketamine in alleviating postoperative pain after knee joint replacement. The intravenous infusion of S(+)-ketamine during knee joint replacement surgery significantly alleviated acute movement pain in elderly patients for 2 h postoperatively while also reducing movement pain at 24 h and 48 h postoperatively, enabling patients to engage in knee joint functional exercises earlier; these findings are similar to those of another study.34 These findings highlight the potential of S(+)-ketamine as a valuable adjunct within a multimodal analgesia regimen, offering effective management of postoperative pain and facilitating improved clinical outcomes in TKA procedures. However, the effect of S(+)-ketamine on postoperative acute resting pain in elderly patients is not significant. This differs from Wang’s research findings.35 This suggests that in the future, it is still necessary to expand the sample for in-depth research. Early ambulation in postoperative patients is a critical indicator of enhanced recovery after surgery (ERAS), and S(+)-ketamine is metabolized in the body to produce the pharmacologically active metabolite norketamine via hepatic microsomal enzymes. Norketamine has an anesthetic potency equivalent to one-fifth to one-third of the potency of S(+)-ketamine, but its elimination half-life is longer. Consequently, S(+)-ketamine provides a certain degree of analgesic effect after the patient awakens.36,37 Among the patients who received S(+)-ketamine during surgery, fewer patients required additional pain relief within 48 h postoperatively. Xu et al showed that compared to placebo, intravenous ketamine was effective for pain relief during 0–8 h but not during 8–24 h after the operation.38 Based on our research findings and literature reports, we speculate that the analgesic effect of S(+)-ketamine lasted longer than that of ketamine, which is better than the analgesic effect of ketamine. This prospective study provided evidence supporting the usefulness of S(+)-ketamine in patients who undergo knee joint replacement surgery.
Tan et al showed that intraoperative ketamine in TKA does not decrease narcotic consumption.39 However, the effect of S(+)-ketamine on intraoperative anesthesia consumption in patients undergoing knee joint replacement surgery is uncertain. This study revealed a possible opioid-sparing effect of S(+)-ketamine. In this study, the intraoperative infusion of subanaesthetic doses of S(+)-ketamine significantly reduced the use of intraoperative sufentanil, but not propofol or remifentanil. These findings are similar to the meta-analysis results reported by Wang et al.35 The analgesic mechanism of S(+)-ketamine is quite complex. The antagonistic effect on NMDA receptors is the basis for S(+)-ketamine’s various pharmacological properties, such as dissociative anesthesia and analgesia. S(+)-ketamine also interacts with other receptors or channels to exert various pharmacological properties. S(+)-ketamine primarily acts on the GluN2B subunit as part of the analgesic process. To produce analgesic effects, S(+)-ketamine can also activate opioid receptors. S(+)-ketamine also excites sympathetic nerves and causes the release of norepinephrine (NA) by blocking sodium channels, inhibiting nitric oxide (NO) release, and inhibiting muscarinic acetylcholine receptors. This, in turn, promotes the release of endogenous opioids and activates opioid receptors, which produce further analgesic effects upon binding to receptors. Additionally, the increase in NA and serotonin also enhances the analgesic effect by activating the descending analgesic pathway. Inhibiting excessive Ca2+ permeability reduces thalamocortical signaling, leading to loss of consciousness and analgesic effectsS(+)-ketamineS(+)-ketamine.40 Therefore, patients who are administered S(+)-ketamine during surgery require lower doses of sufentanil.
Although S(+)-ketamine plays a significant role in clinical anesthesia, its use may trigger a wide range of adverse effects, including dizziness, nausea, vomiting, greater airway secretions, and an increase in heart rate and blood pressure. In this study, we found that the incidence of dizziness, nausea, and vomiting in patients who received continuous infusions of low-dose S(+)-ketamine during knee joint replacement surgery was lower. Consistent with these findings, intravenous ketamine administered during the perioperative period not only alleviated acute postoperative pain but also reduced the incidence of postoperative nausea and vomiting.41 This may be attributed to the lower intraoperative use of sufentanil and the lower usage of additional analgesics after surgery. These findings provide evidence for the clinical use of S(+)-ketamine.
This study had certain limitations. First, this was a single-center study with a relatively small sample size, and it included only elderly patients who underwent TKA, which limited the generalizability of our findings. Second, our follow-up concluded at 48 h postoperatively. Longer follow-up periods are necessary to establish the long-term effects and safety of S(+)-ketamine. This study also lacked comprehensive data to demonstrate the effect of S(+)-ketamine on patient rehabilitation, which may be investigated in future studies.
Conclusions
To summarize, intravenous administration of low-dose S(+)-ketamine during knee joint replacement surgery can effectively alleviate acute pain following surgery in elderly patients, reduce the need for rescue analgesics, and decrease the side effects associated with opioids, including dizziness, nausea, and vomiting. Therefore, our study provides a reference for the application of S(+)-ketamine in multimodal short-term analgesia during the perioperative period.
Abbreviations
NRS, Numerical Rating Scale; NSAID, Nonsteroidal Anti-inflammatory Drugs; TKA, Total Knee Arthroplasty; NMDA, N-methyl-D-aspartate; ERAS, Enhanced Recovery After Surgery; SAE, Serious Adverse Event.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of The First Affiliated Hospital of Shandong First Medical University (YXLL-KY-2021(077)). All patients signed an informed consent document before participating in the study.
Acknowledgments
The language of this study was professionally edited by ExEditing.com.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Shandong Provincial Medical and Health Science and Technology Development Program Project (Grant No.: 2019WS504). The funder had no role in the conceptualization, design, data collection, analysis, decision to publish, or preparation of the paper.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Singh JA, Vessely MB, Harmsen WS, et al. A population-based study of trends in the use of total hip and total knee arthroplasty, 1969-2008. Mayo Clin Proc. 2010;85(10):898–904. doi:10.4065/mcp.2010.0115
2. Koh IJ, Kim TK, Chang CB, Cho HJ, In Y. Trends in use of total knee arthroplasty in Korea from 2001 to 2010. Clin Orthop Relat Res. 2013;471(5):1441–1450. doi:10.1007/s11999-012-2622-y
3. Singh JA, Yu S, Chen L, Cleveland JD. Rates of total joint replacement in the United States: future projections to 2020-2040 using the national inpatient sample. J Rheumatol. 2019;46(9):1134–1140. doi:10.3899/jrheum.170990
4. Rupp M, Lau E, Kurtz SM, Alt V. Projections of primary TKA and THA in Germany from 2016 through 2040. Clin Orthop Relat Res. 2020;478(7):1622–1633. doi:10.1097/corr.0000000000001214
5. Kim TW, Kang SB, Chang CB, Moon SY, Lee YK, Koo KH. Current trends and projected burden of primary and revision total knee arthroplasty in Korea between 2010 and 2030. J Arthroplasty. 2021;36(1):93–101. doi:10.1016/j.arth.2020.06.064
6. Callahan CM, Drake BG, Heck DA, Dittus RS. Patient outcomes following tricompartmental total knee replacement. A meta-analysis. JAMA. 1994;271(17):1349–1357. doi:10.1001/jama.1994.03510410061034
7. Davies AF, Segar EP, Murdoch J, Wright DE, Wilson IH. Epidural infusion or combined femoral and sciatic nerve blocks as perioperative analgesia for knee arthroplasty. Br J Anaesth. 2004;93(3):368–374. doi:10.1093/bja/aeh224
8. Sigirci A. Pain management in total knee arthroplasty by intraoperative local anesthetic application and one-shot femoral block. Indian J Orthop. 2017;51(3):280–285. doi:10.4103/0019-5413.205688
9. Society KK. Guidelines for the management of postoperative pain after total knee arthroplasty. Knee Surg Relat Res. 2012;24(4):201–207. doi:10.5792/ksrr.2012.24.4.201
10. Li JW, Ma YS, Xiao LK. Postoperative pain management in total knee arthroplasty. Orthop Surg. 2019;11(5):755–761. doi:10.1111/os.12535
11. Bohnert AS, Valenstein M, Bair MJ, et al. Association between opioid prescribing patterns and opioid overdose-related deaths. JAMA. 2011;305(13):1315–1321. doi:10.1001/jama.2011.370
12. Liu P, Li P, Li Q, et al. Effect of pretreatment of S-ketamine on postoperative depression for breast cancer patients. J Invest Sur. 2021;34(8):883–888. doi:10.1080/08941939.2019.1710626
13. Falk E, Schlieper D, van Caster P, et al. A rapid positive influence of S-ketamine on the anxiety of patients in palliative care: a retrospective pilot study. BMC Palliative Care. 2020;19(1):1. doi:10.1186/s12904-019-0499-1
14. Tu W, Yuan H, Zhang S, et al. Influence of anesthetic induction of propofol combined with esketamine on perioperative stress and inflammatory responses and postoperative cognition of elderly surgical patients. Am J Trans Res. 2021;13(3):1701–1709.
15. Eberl S, Koers L, van Hooft J, et al. The effectiveness of a low-dose esketamine versus an alfentanil adjunct to propofol sedation during endoscopic retrograde cholangiopancreatography: a randomised controlled multicentre trial. Eur J Anaesthesiol. 2020;37(5):394–401. doi:10.1097/eja.0000000000001134
16. Aronsohn J, Orner G, Palleschi G, Gerasimov M. Opioid-free total intravenous anesthesia with ketamine as part of an enhanced recovery protocol for bariatric surgery patients with sleep disordered breathing. J Clin Anesth. 2019;52:65–66. doi:10.1016/j.jclinane.2018.09.014
17. Li J, Wang Z, Wang A, Wang Z. Clinical effects of low-dose esketamine for anaesthesia induction in the elderly: a randomized controlled trial. J Clin Pharm Ther. 2022;47(6):759–766. doi:10.1111/jcpt.13604
18. Guará Sobrinho H, Garcia JB, Vasconcelos JW, Sousa JC, Ferro LS. Analgesic efficacy of the intra-articular administration of S(+)- ketamine in patients undergoing total knee arthroplasty. Rev Bras Anestesiol. 2012;62(5):665–675. doi:10.1016/s0034-7094(12)70165-4
19. Touil N, Pavlopoulou A, Barbier O, Libouton X, Lavand’homme P. Evaluation of intraoperative ketamine on the prevention of severe rebound pain upon cessation of peripheral nerve block: a prospective randomised, double-blind, placebo-controlled study. Br J Anaesth. 2022;128(4):734–741. doi:10.1016/j.bja.2021.11.043
20. Li Q, Tian S, Zhang L, et al. S-ketamine reduces the risk of rebound pain in patients following total knee arthroplasty: a randomized controlled trial. Drug Des Devel Ther. 2025;19:2315–2327. doi:10.2147/dddt.S515741
21. Miziara LE, Simoni RF, Esteves LO, Cangiani LH, Grillo-Filho GFR, Paula AG. Efficacy of continuous S(+)-ketamine infusion for postoperative pain control: a randomized placebo-controlled trial. Anesthesiol Res Pract. 2016;2016(1):6918327. doi:10.1155/2016/6918327
22. Deng S, Chen L, Song X, et al. Analgesic effect of intraoperative intravenous S(+)-ketamine during total knee arthroplasty surgery: study protocol for a randomized controlled clinical trial. JMIR Res Protoc. 2023;12:e53063. doi:10.2196/53063
23. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
24. Qiu D, Wang XM, Yang JJ, et al. Effect of intraoperative esketamine infusion on postoperative sleep disturbance after gynecological laparoscopy: a randomized clinical trial. JAMA Network Open. 2022;5(12):e2244514. doi:10.1001/jamanetworkopen.2022.44514
25. Castarlenas E, Jensen MP, von Baeyer CL, Miró J. Psychometric properties of the numerical rating scale to assess self-reported pain intensity in children and adolescents: a systematic review. Clin J Pain. 2017;33(4):376–383. doi:10.1097/ajp.0000000000000406
26. Wang Y, Zhu YZ, Liu G. Effects of preemptive analgesia with dexmedetomidine combined with tramadolon postoperative analgesia and anesthetic drug usage in orthopedic surgery. Hebei Med. 2016;22(3):415–418.
27. Malviya A, Martin K, Harper I, et al. Enhanced recovery program for hip and knee replacement reduces death rate. Acta orthopaedica. 2011;82(5):577–581. doi:10.3109/17453674.2011.618911
28. McCartney CJ, Nelligan K. Postoperative pain management after total knee arthroplasty in elderly patients: treatment options. Drugs Aging. 2014;31(2):83–91. doi:10.1007/s40266-013-0148-y
29. Su Y, Zhang XY, Lan L, Wang R. Clinical observation of multimodal analgesic nursing intervention applied to patients after hip replacement surgery. Yunnan J Tradit Chin Med Materia Medica. 2013;34(3):77–80.
30. Castorina S, Luca T, Privitera G, El-Bernawi H. An evidence-based approach for laparoscopic inguinal hernia repair: lessons learned from over 1000 repairs. Clin Anat. 2012;25(6):687–696. doi:10.1002/ca.22022
31. Wheeler M, Oderda GM, Ashburn MA, Lipman AG. Adverse events associated with postoperative opioid analgesia: a systematic review. J Pain. 2002;3(3):159–180. doi:10.1054/jpai.2002.123652
32. Gan TJ, Joshi GP, Zhao SZ, Hanna DB, Cheung RY, Chen C. Presurgical intravenous parecoxib sodium and follow-up oral valdecoxib for pain management after laparoscopic cholecystectomy surgery reduces opioid requirements and opioid-related adverse effects. Acta anaesthesiologica Scandinavica. 2004;48(9):1194–1207. doi:10.1111/j.1399-6576.2004.00495.x
33. Nielsen RV, Fomsgaard JS, Nikolajsen L, Dahl JB, Mathiesen O. Intraoperative S-ketamine for the reduction of opioid consumption and pain one year after spine surgery: a randomized clinical trial of opioid-dependent patients. Eur J Pain. 2019;23(3):455–460. doi:10.1002/ejp.1317
34. Xie M, Liang Y, Deng Y, Li T. Effect of S-ketamine on postoperative pain in adults post-abdominal surgery: a systematic review and meta-analysis. Pain Physician. 2023;26(4):327–335. doi:10.36076/ppj.2023.26.327
35. Wang X, Lin C, Lan L, Liu J. Perioperative intravenous S-ketamine for acute postoperative pain in adults: a systematic review and meta-analysis. J Clin Anesth. 2021;68:110071. doi:10.1016/j.jclinane.2020.110071
36. Lim JA, Oh CS, Yoon TG, et al. The effect of propofol and sevoflurane on cancer cell, natural killer cell, and cytotoxic T lymphocyte function in patients undergoing breast cancer surgery: an in vitro analysis. BMC Cancer. 2018;18(1):159. doi:10.1186/s12885-018-4064-8
37. Ye L, Xiao X, Zhu L. The comparison of etomidate and propofol anesthesia in patients undergoing gastrointestinal endoscopy: a systematic review and meta-analysis. Surg Laparosc Endosc Percutan Tech. 2017;27(1):1–7. doi:10.1097/sle.0000000000000373
38. Xu B, Wang Y, Zeng C, et al. Analgesic efficacy and safety of ketamine after total knee or hip arthroplasty: a meta-analysis of randomised placebo-controlled studies. BMJ Open. 2019;9(9):e028337. doi:10.1136/bmjopen-2018-028337
39. Tan TL, Longenecker AS, Rhee JH, et al. Intraoperative ketamine in total knee arthroplasty does not decrease pain and narcotic consumption: a prospective randomized controlled trial. J Arthroplasty. 2019;34(8):1640–1645. doi:10.1016/j.arth.2019.04.017
40. Zhou J, Peng G, Liang W, et al. Recent advances in the study of anesthesia-and analgesia-related mechanisms of S-ketamine. Front Pharmacol. 2023;14:1228895. doi:10.3389/fphar.2023.1228895
41. Brinck EC, Tiippana E, Heesen M, et al. Perioperative intravenous ketamine for acute postoperative pain in adults. Cochrane Database Syst Rev. 2018;12(12):Cd012033. doi:10.1002/14651858.CD012033.pub4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pharmacological Methods of Pain Management: Narrative Review of Medication Used
Alorfi NM
International Journal of General Medicine 2023, 16:3247-3256
Published Date: 31 July 2023
Exploration of Key Brain Regions Involved in Acupuncture and Moxibustion Analgesia: An Imaging-Based Study
He L, Zhou R, Hou S, Huang D, Zhao X, Wang M, Huang M, Yin T, Yin H, Yu S
Journal of Pain Research 2025, 18:2051-2067
Published Date: 15 April 2025
Effects of Intrathecal Sufentanil at Different Doses on Postoperative Pain Relief and Opioid Consumption in Elderly Patients Undergoing Lower Limb Orthopedic Surgery: A Randomized Controlled Trial
Li Y, Gu Y, Liu W, Liu X, Wang F, Tian B, Zhou W, Ye Q
Journal of Pain Research 2025, 18:2439-2451
Published Date: 15 May 2025
Effect of Thoracic Paravertebral Block on Postoperative Pulmonary Complications After Video-Assisted Thoracoscopic Surgery: A Dual-Center Randomized Clinical Trial
Zhu J, Wei B, Wu L, Li H, Zhang Y, Lu J, Su S, Xi C, Liu W, Wang G
Therapeutics and Clinical Risk Management 2025, 21:691-703
Published Date: 15 May 2025
Circadian Variation in Ropivacaine Requirement for Initiation of Epidural Labour Analgesia: A Random-Allocation Graded Dose-Response Study
Huang XD, Xiao F, Hu B, Dong XY, Chen XZ
Drug Design, Development and Therapy 2026, 20:573078
Published Date: 10 March 2026