")
Back to Journals » International Journal of General Medicine » Volume 16
Pharmacological Methods of Pain Management: Narrative Review of Medication Used
Authors Alorfi NM
Received 28 April 2023
Accepted for publication 2 July 2023
Published 31 July 2023 Volume 2023:16 Pages 3247—3256
DOI https://doi.org/10.2147/IJGM.S419239
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Luca Testarelli
Nasser M Alorfi
Department of Pharmacology and Toxicology, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Nasser M Alorfi, Email [email protected]
Background: Pain management is a critical aspect of healthcare, aimed at alleviating discomfort and improving the quality of life for individuals experiencing acute or chronic pain. Pharmacological methods constitute a primary approach to pain management, including a diverse array of drugs that work through different mechanisms.
Aim: Identifying medications commonly employed in pain management, focusing on their mechanism of actions, uses, efficacy and pharmacological applications.
Methods: The methodology involved a systematic search of scientific literature using various databases, including PubMed, Scopus, and Google Scholar. Relevant articles published between 2000 and 2023 were screened for inclusion. The selected studies encompassed original research, review articles, therapeutic guidelines and randomized controlled trials.
Results: The findings of this review suggest that a multimodal approach combining various analgesics can enhance pain relief while minimizing adverse effects. It emphasizes the importance of assessing pain intensity, determining the underlying etiology, and utilizing evidence-based guidelines to optimize pain management outcomes.
Conclusion: Pharmacological methods of pain management are an essential component of pain management strategies to achieve optimal pain relief while minimizing adverse effects. The article concludes with a discussion on emerging trends and future directions in pharmacological pain management, including novel drug targets and advances in drug delivery systems.
Keywords: pain, pharmacology, neuroscience, analgesia, hypersensitivity
Introduction
Pain is a subjective experience that involves physical, psychological, and social factors.1 It can arise from a variety of sources, including injury, disease, inflammation, and nerve damage.2,3 Pain can greatly influence an individual’s overall well-being, impairing their capacity to perform daily activities, fulfill work obligations, and participate in social interactions.4,5 Pain sensation is a complex process that involves the activation of sensory neurons, the transmission of electrical and chemical signals along neural pathways, and the interpretation of these signals by higher brain centers.6,7 The generation and modulation of pain sensation involve various mechanisms.6 One mechanism is the activation of nociceptors, specialized sensory neurons that respond to noxious stimuli.7 Nociceptors express ion channels, such as transient receptor potential vanilloid 1 (TRPV1) and acid-sensing ion channels (ASICs), which are activated by heat, acid, and other noxious stimuli.8,9 These ion channels depolarize the neuron, leading to the release of excitatory neurotransmitters, such as substance P and glutamate, which stimulate neighboring neurons and create a cascade of electrical and chemical signals that travel up to the spinal cord.10 Another mechanism involves the transmission of these signals along neural pathways, such as the spinothalamic tract.3 Within the spinal cord, these signals are transmitted to secondary neurons responsible for conveying the information to higher brain centers.11 The perception of pain is influenced by several factors, such as the intensity and duration of the stimulus, the emotional state of the individual, and the context in which the pain occurs.12,13 The modulation of pain sensation also involves several mechanisms, including the activation of descending pathways from higher brain centers to the spinal cord.6 These pathways release neurotransmitters, such as endorphins and enkephalins, that inhibit the release of neurotransmitters involved in pain transmission, thereby reducing the perception of pain.12,14 In addition, inflammation and tissue damage can lead to sensitization of nociceptors, resulting in hyperalgesia or allodynia.15,16 Overall, the mechanisms of pain sensation are complex and involve the activation and modulation of multiple neural pathways and signaling molecules. Understanding these mechanisms is crucial for the development of effective pain management. The prevalence and significance of pain as a healthcare issue cannot be underestimated. It affects a significant proportion of the population and has far-reaching consequences for individuals, healthcare systems, and society. Efforts to effectively manage pain and improve patient outcomes remain a crucial priority in healthcare. Effective pain management is an essential aspect of healthcare, and it involves a multi-disciplinary approach that includes pharmacological and non-pharmacological methods.17,18
Pain Management
Pharmacological methods of pain management include non-opioid and opioid analgesics, adjuvant analgesics, and corticosteroids. Non-opioid analgesics are commonly used for mild to moderate pain management. Opioid analgesics are potent pain relievers used for moderate to severe pain management. However, they are associated with a range of adverse effects, including sedation, respiratory depression, and constipation. Opioid analgesics also have a high risk of dependence and addiction. Adjuvant analgesics, such as antidepressants and anticonvulsants additionally to enhance pain relief.19 Corticosteroids are potent anti-inflammatory agents used for pain associated with inflammation. They are commonly used for pain associated with conditions such as rheumatoid arthritis and back pain.20 Emerging therapies like neuromodulation for pain offer innovative approaches to alleviate chronic pain by modulating the activity of the nervous system through techniques such as spinal cord stimulation, deep brain stimulation, and transcutaneous electrical nerve stimulation.21,22
Patient-specific factors play a significant role in determining the most suitable medication and dosage regimen for pain management. One important set of factors to consider is the patient’s pain intensity and type.23 The severity and nature of pain experienced by the patient influence the choice of medication. Another critical factor is the presence of underlying medical conditions.24 Patients with comorbidities, such as liver or kidney disease, cardiovascular disorders, or gastrointestinal issues, may require adjustments in medication selection or dosage to minimize potential adverse effects or drug interactions.25 Age-related physiological changes can also impact medication selection.26 Elderly patients may experience altered pharmacokinetics and pharmacodynamics, making them more susceptible to adverse effects.27 As a result, they may require lower doses or alternative medications that are better tolerated. Evaluation of the patient’s medication profile is essential to identify potential drug interactions.28 Some medications may interact with analgesics, altering their efficacy or increasing the risk of adverse effects. Considering concomitant medications is crucial in order to avoid unwanted interactions.29
Ensuring effective pain management is essential in enhancing the quality of life for individuals who are dealing with pain.29 Pharmacological methods of pain management are an essential component of pain management strategies and should be used judiciously to achieve optimal pain relief while minimizing adverse effects.30 This article provides an overview of the different pharmacological methods of pain management.
Non-Opioid Analgesics
Non-opioid analgesics are drugs that are commonly used to relieve mild to moderate pain.31 Examples include aspirin, acetaminophen, and nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and naproxen.24 These drugs are widely available over the counter and have a low risk of addiction and dependence.
Types of Non-Opioid Analgesics
Non-opioid analgesics can be classified into three main categories: NSAIDs, acetaminophen, and topical agents. NSAIDs are the most commonly used non-opioid analgesics.32 They work by inhibiting the production of prostaglandins, which are responsible for pain and inflammation.33 NSAIDs can be further classified into two categories: selective and non-selective. Selective NSAIDs primarily target cyclooxygenase-2 (COX-2) enzymes, while non-selective NSAIDs target both COX-1 and COX-2 enzymes.34,35 Examples of non-selective NSAIDs include aspirin, ibuprofen, and naproxen, while examples of selective NSAIDs include celecoxib.31,36,37 Acetaminophen is another type of non-opioid analgesic commonly used for pain management.38 It works by inhibiting the production of prostaglandins in the central nervous system.39 Acetaminophen is not effective in reducing inflammation but is useful in managing mild to moderate pain.39 It has a low risk of adverse effects and is often used as an alternative to NSAIDs.40 Topical agents are a newer class of non-opioid analgesics that are applied directly to the skin. They work by blocking pain signals at the site of application. Examples of topical agents include capsaicin cream, and diclofenac gel.41,42
Pharmacological Effects and Mechanism of Action
Non-opioid analgesics work by inhibiting the production of prostaglandins, which are responsible for pain and inflammation.43 NSAIDs work by blocking the COX enzymes that produce prostaglandins.44 Acetaminophen works by inhibiting prostaglandin production in the central nervous system.40 Topical agents work by blocking pain signals at the site of application.45 NSAIDs have additional pharmacological effects, including anti-inflammatory, antipyretic, and antiplatelet activity.46 They reduce inflammation by inhibiting the production of inflammatory mediators, such as cytokines and chemokines.24,47 They also reduce fever by blocking the production of prostaglandins that regulate body temperature.48 Lastly, NSAIDs have antiplatelet activity.49
Adverse Effects
Non-opioid analgesics can cause adverse effects, which may limit their use in some patients.35 NSAIDs can cause gastrointestinal (GI) adverse effects, such as dyspepsia, nausea, vomiting, and peptic ulcer disease.48 They can also cause renal adverse effects, such as acute kidney injury and chronic kidney disease. NSAIDs should be used with caution in patients with renal impairment, heart failure, or a history of GI bleeding.37 Acetaminophen is generally well-tolerated, but it can cause hepatotoxicity in overdose.50 Topical agents can cause local adverse effects, such as skin irritation, itching, and burning. They can also cause systemic adverse effects if absorbed through the skin, such as GI upset, headache, and dizziness.51
Opioid Analgesics
Opioid analgesics are the most potent drugs in pain management.31 They produce a range of pharmacological effects, including analgesia, sedation, respiratory depression, and euphoria.52,53 Opioid analgesics can cause respiratory depression, gastrointestinal adverse effects, hormonal changes, tolerance, dependence, and addiction when used long-term.52,53 Careful monitoring of patients receiving opioid analgesics is essential to ensure safe and effective pain management.54 Examples of opioid analgesics include morphine, oxycodone, hydrocodone, fentanyl, and codeine.55–57 These medications are available by prescription only and have a high risk of addiction and dependence.4,55
Types of Opioid Analgesics
Opioid analgesics can be classified into three main categories: natural opioids, synthetic opioids, and semi-synthetic opioids.58 Natural opioids are derived from the opium poppy, while synthetic and semi-synthetic opioids are manufactured in a laboratory.58,59 Examples of natural opioids include morphine, codeine, and thebaine. Examples of synthetic opioids include fentanyl, methadone, and tramadol. Examples of semi-synthetic opioids include oxycodone, hydrocodone, and buprenorphine.58
Pharmacological Effects and Mechanism of Action
The mechanism of action of opioid analgesics is complex and involves multiple steps, including receptor binding, G protein activation, and neurotransmitter inhibition.60 By targeting opioid receptors in various parts of the body, these drugs can effectively reduce the perception of pain and provide relief to patients suffering from moderate to severe pain.61 There are three main types of opioid receptors: mu, delta, and kappa.62 Mu opioid receptors are responsible for producing analgesia, while delta and kappa opioid receptors have other effects, such as producing sedation and reducing anxiety.60,63 Opioids have antitussive, anti-diarrheal, and pupil-constricting effects.64
Adverse Effects
Opioid analgesics can cause a range of adverse effects, which can limit their use in some patients.65,66 The most common adverse effects are related to the central nervous system and include sedation, dizziness, confusion, addiction and respiratory depression.67,68 Respiratory depression can be life-threatening and requires close monitoring of patients receiving opioid analgesics.69 Opioid analgesics can also cause gastrointestinal adverse effects, such as nausea, vomiting, and constipation.52,70 They can cause urinary retention and may exacerbate symptoms in patients with benign prostatic hyperplasia.71 Opioid analgesics can also cause hormonal changes, including decreased testosterone levels and increased prolactin levels.72 Long-term use of opioid analgesics can lead to tolerance, dependence, and addiction.73 Patients who use opioid analgesics for an extended period may require higher doses to achieve the same level of pain relief.74 Sudden cessation of opioid analgesics can cause withdrawal symptoms, including anxiety, agitation, and flu-like symptoms.75,76
Adjuvant Analgesics
Adjuvant analgesics are a diverse group of medications that can be used in combination with other pain management drugs to enhance their analgesic effects or to manage specific types of pain.77 These medications work by modulating the activity of neurotransmitters and ion channels in the central and peripheral nervous systems. Examples of adjuvant analgesics include antidepressants, benzodiazepines, anticonvulsants, and corticosteroids.78,79
Categories of Adjuvant Analgesics
Adjuvant analgesics can be classified into several categories based on their mechanism of action and therapeutic indications. These categories include:
Antidepressants
Antidepressants, particularly those that affect serotonin and noradrenaline signaling, have been used in pain management.80 These drugs modulate the descending pain pathways from the brainstem to the spinal cord, leading to a reduction in pain perception.19 Selective serotonin reuptake inhibitors (SSRIs) such as fluoxetine and paroxetine have been shown to be effective in the treatment of chronic pain conditions such as fibromyalgia, chronic lower back pain, and neuropathic pain.30 Tricyclic antidepressants (TCAs), such as amitriptyline and nortriptyline, are also commonly used in the treatment of chronic pain and have been shown to be effective in reducing pain severity and improving function in conditions such as diabetic neuropathy, postherpetic neuralgia, and chronic low back pain.81,82 However, these drugs can also cause side effects such as dry mouth, sedation, and cognitive impairment.83
Anticonvulsants
Anticonvulsants, such as gabapentin and pregabalin, have emerged as promising agents for the management of neuropathic pain.84 These medications work by modulating the activity of voltage-gated calcium channels in the central nervous system, which can help to reduce pain perception14 via reducing the release of excitatory neurotransmitters and dampening the hyperexcitability of neurons that contribute to the development and maintenance of chronic pain.10,14 Moreover, anticonvulsants have been shown to improve sleep quality, anxiety, and depression, all of which are common comorbidities in patients with chronic pain.85,86 Clinical studies have demonstrated the efficacy of anticonvulsants in various neuropathic pain conditions, such as diabetic neuropathy, postherpetic neuralgia, and spinal cord injury.87,88 However, despite their effectiveness, anticonvulsants are associated with adverse effects, such as sedation, dizziness, and cognitive impairment.88
Local Anesthetics
Local anesthetics, such as lidocaine and bupivacaine, can be used in the management of chronic pain.89 They work by blocking the transmission of nerve impulses in a specific area of the body, thus producing a temporary loss of sensation and pain relief.90 They are also used for the treatment of chronic pain conditions, such as neuropathic pain and postherpetic neuralgia.91 The primary mechanism of action of local anesthetics is the blockade of voltage-gated sodium channels in nerve fibers.92 This prevents the influx of sodium ions required for the generation and propagation of action potentials, effectively blocking the transmission of nerve impulses.93 The onset of action of local anesthetics depends on the type of medication used, the route of administration, and the characteristics of the tissue being anesthetized. Local anesthetics can be administered through various routes, such as infiltration, nerve block, epidural, and intrathecal.94 Epidural and intrathecal injections involve the injection of the anesthetic into the epidural space or cerebrospinal fluid, respectively.95 Local anesthetics have several advantages in the management of pain. They also have a rapid onset of action, and their effects can be reversed with the administration of specific antidotes, such as naloxone.96 However, local anesthetics can also have adverse effects, such as systemic toxicity, allergic reactions, and nerve damage. Systemic toxicity can occur due to the inadvertent injection of a high dose of the anesthetic or the use of a medication with a narrow therapeutic index.97 The symptoms of systemic toxicity include central nervous system depression, cardiovascular collapse, and respiratory arrest.98 Patients with comorbidities, such as liver or renal impairment, require special consideration in the choice and administration of local anesthetics.99 Collectively, local anesthetics are an essential component of pharmacological approaches for pain management in various medical procedures.
Corticosteroids
Corticosteroids have potent anti-inflammatory and analgesic effects, making them useful in the management of various types of pain. They reduce the production of pain-inducing substances and inflammatory mediators, such as prostaglandins, leukotrienes, and cytokines.20 Corticosteroids, such as prednisone and dexamethasone, can be used in the management of inflammatory pain. Corticosteroids also have immunosuppressive effects, which can be beneficial in the management of pain associated with autoimmune diseases, such as rheumatoid arthritis.100 They are used to manage pain associated with a variety of conditions, such as rheumatoid arthritis, osteoarthritis, and acute and chronic pain.101,102 Corticosteroids are associated with a range of adverse effects such as weight gain, fluid retention, hypertension, mood changes, and gastrointestinal disturbances, such as ulcers and bleeding.103–105 While long-term use of corticosteroids can also lead to osteoporosis, muscle weakness, and increased risk of infections.106 A summary of pharmacological options for pain management is tabulated in Table 1.
 |
Table 1 Pharmacological Options for Pain Management |
Emerging Therapies
Neuromodulation for pain is a therapeutic technique that involves using electrical or chemical stimulation to modulate the activity of the nervous system and alleviate pain.21 It targets chronic pain conditions that have not responded well to traditional treatments.22 One common method is Spinal Cord Stimulation (SCS), where a small device is implanted near the spinal cord to deliver electrical impulses that disrupt pain signals.107 Deep brain stimulation (DBS) involves implanting electrodes in specific brain areas to regulate abnormal neural activity associated with pain.108 Transcutaneous electrical nerve stimulation (TENS) uses a portable device to deliver low-voltage electrical impulses near the painful area, blocking or reducing pain signals.109 Intrathecal drug delivery (IDD) utilizes a pump to deliver pain-relieving medication directly into the spinal cord.110 Overall, neuromodulation for pain provides an alternative approach, offering relief and improved functionality for individuals living with chronic pain by directly influencing the neural pathways involved in pain perception.
Non-Pharmacological Interventions
Non-pharmacological options for pain management encompass a variety of interventions and techniques that do not rely on medications to alleviate pain. These approaches are aimed at addressing pain through alternative means, such as physical, psychological, or complementary therapies. A descriptive of each non-pharmacological options for pain management are provided in Table 2.
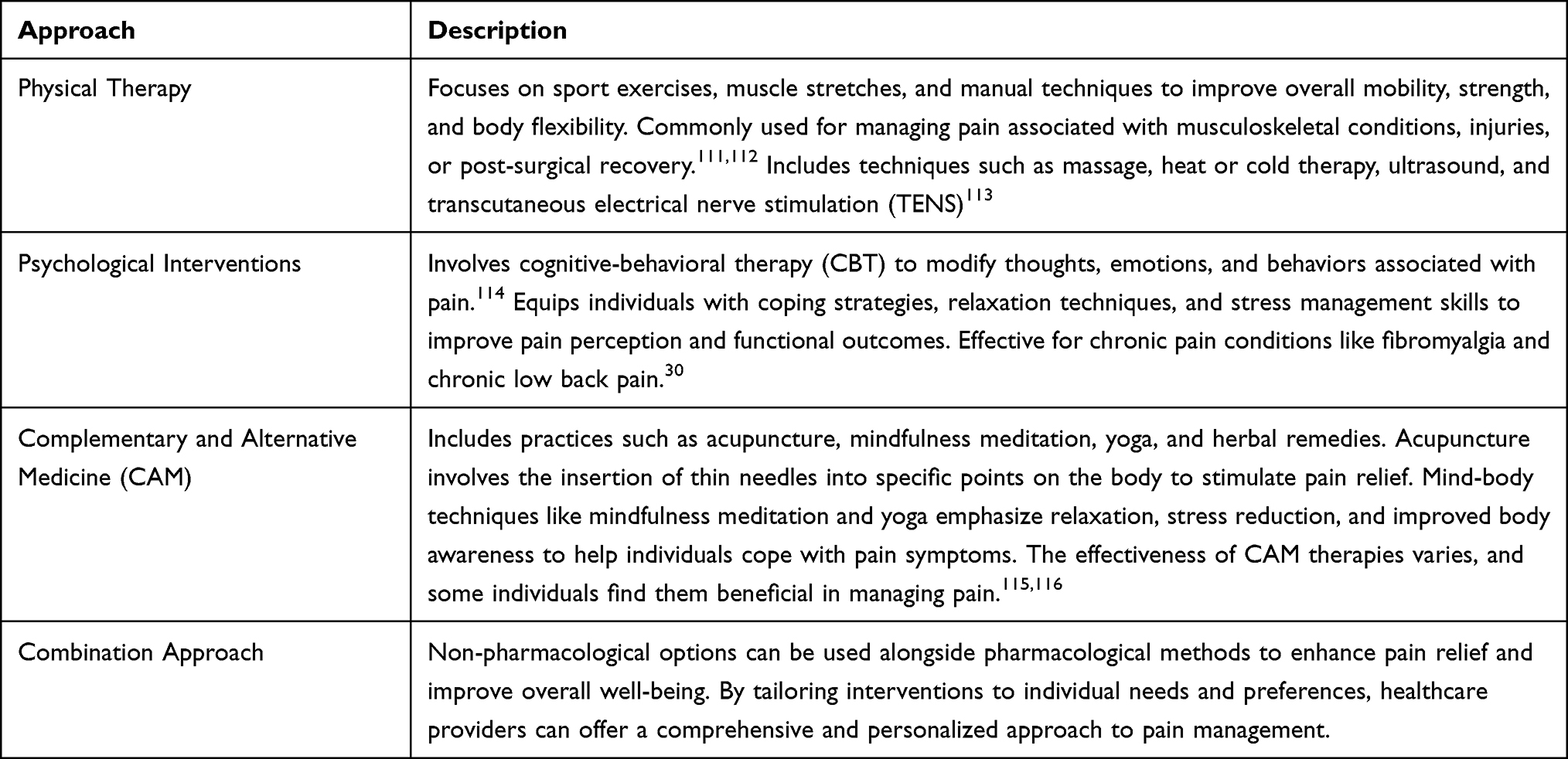 |
Table 2 Non-Pharmacological Options for Pain Management |
Conclusion
In conclusion, opioids, nonsteroidal anti-inflammatory drugs (NSAIDs), anticonvulsants, and antidepressants are commonly used drugs for pain management. Opioids are effective for acute pain, but their long-term use is associated with tolerance, dependence, and addiction. NSAIDs are effective in the management of inflammatory pain, but their use is limited by the risk of adverse effects such as gastrointestinal bleeding and renal dysfunction. Anticonvulsants and antidepressants are increasingly used for the treatment of neuropathic pain, and they have demonstrated efficacy in reducing pain severity and improving function. However, these drugs can also cause side effects, and careful patient selection and dosing are necessary to balance the benefits and risks of treatment. Emerging trends and future directions in pharmacological pain management encompass novel drug targets and advancements in drug delivery systems, paving the way for more effective and personalized pain relief.117 In recent years, there has been an increasing focus on identifying and developing novel drug targets to enhance pain management. This includes targeting specific receptors, ion channels, or signaling pathways involved in pain transmission and modulation.118,119 Overall, pharmacological methods of pain management should be used judiciously and tailored to individual patient needs to achieve optimal pain relief and improve quality of life.
Future Research and Upcoming Considerations
Emerging trends in pharmacological pain management focus on novel drug targets and innovative drug delivery systems. By expanding our understanding of pain mechanisms and utilizing advanced technologies, researchers and pharmaceutical companies are striving to develop more efficient, targeted, and personalized medications for pain relief.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Raja SN, Carr DB, Cohen M, et al. The revised IASP definition of pain: concepts, challenges, and compromises. Pain. 2020;161:1976. doi:10.1097/J.PAIN.0000000000001939
2. Pinho-Ribeiro FA, Verri WA, Chiu IM. Nociceptor sensory neuron–immune interactions in pain and inflammation. Trends Immunol. 2017;38:5–19. doi:10.1016/J.IT.2016.10.001
3. Steeds CE. The anatomy and physiology of pain. Surg. 2009;27:507–511. doi:10.1016/J.MPSUR.2009.10.013
4. Katz N. The impact of pain management on quality of life. J Pain Symptom Manage. 2002;24:S38–S47. doi:10.1016/S0885-3924(02)00411-6
5. Deshpande MA, Holden RR, Gilron I. The impact of therapy on quality of life and mood in neuropathic pain: what is the effect of pain reduction? Anesth Analg. 2006;102:1473–1479. doi:10.1213/01.ANE.0000204295.90178.77
6. Yam MF, Loh YC, Tan CS, Adam SK, Manan NA, Basir R. General pathways of pain sensation and the major neurotransmitters involved in pain regulation. Int J Mol Sci. 2018;19:2164. doi:10.3390/IJMS19082164
7. Dubin AE, Patapoutian A. Nociceptors: the sensors of the pain pathway. J Clin Invest. 2010;120:3760–3772. doi:10.1172/JCI42843
8. Ohashi N, Kohno T. Analgesic effect of acetaminophen: a review of known and novel mechanisms of action. Front Pharmacol. 2020;11:1916. doi:10.3389/FPHAR.2020.580289/BIBTEX
9. Chen R, Coppes OJM, Urman RD. Receptor and molecular targets for the development of novel opioid and non-opioid analgesic therapies. Pain Physician. 2021;24:153–163. doi:10.36076/ppj.2021.24.153-163
10. Zieglgänsberger W. Substance P and pain chronicity. Cell Tissue Res. 2018;375:227–241. doi:10.1007/S00441-018-2922-Y
11. Ahmad AH, Abdul Aziz CB. The brain in pain. Malays J Med Sci. 2014;21:46. doi:10.1097/01.bonej.0000265758.09846.32
12. Hill RG. Molecular basis for the perception of pain. Neuroscientist. 2001;7:282–292. doi:10.1177/107385840100700405
13. Ma RS, Kayani K, Whyte-Oshodi D, et al. Voltage gated sodium channels as therapeutic targets for chronic pain. J Pain Res. 2019;12:2709. doi:10.2147/JPR.S207610
14. Park JF, Luo ZD. Calcium channel functions in pain processing. Channels. 2010;4:510. doi:10.4161/CHAN.4.6.12869
15. Schaible HG, Richter F. Pathophysiology of pain. Langenbeck’s Arch Surg. 2004;389:237–243. doi:10.1007/S00423-004-0468-9/METRICS
16. Scherrmann J-M, Wolff K, Franco CA, et al. Allodynia. Encycl Psychopharmacol. 2022:65. doi:10.1007/978-3-540-68706-1_1043
17. Andronis L, Kinghorn P, Qiao S, Whitehurst DGT, Durrell S, McLeod H. Cost-effectiveness of non-invasive and non-pharmacological interventions for low back pain: a systematic literature review. Appl Health Econ Health Policy. 2017;15:173–201. doi:10.1007/S40258-016-0268-8/TABLES/3
18. Moisset X, Bouhassira D, Avez Couturier J, et al. Pharmacological and non-pharmacological treatments for neuropathic pain: systematic review and French recommendations. Rev Neurol. 2020;176:325–352. doi:10.1016/J.NEUROL.2020.01.361
19. Dharmshaktu P, Tayal V, Kalra BS. Efficacy of antidepressants as analgesics: a review. J Clin Pharmacol. 2012;52:6–17. doi:10.1177/0091270010394852
20. Vyvey M. Steroids as pain relief adjuvants. Can Fam Physician. 2010;56:1295.
21. Yu K, Niu X, He B, Yu K, Niu X, He B. Neuromodulation management of chronic neuropathic pain in the central nervous system. Adv Funct Mater. 2020;30:1908999. doi:10.1002/ADFM.201908999
22. Knotkova H, Hamani C, Sivanesan E, et al. Neuromodulation for chronic pain. Lancet. 2021;397:2111–2124. doi:10.1016/S0140-6736(21)00794-7
23. Fink R. Pain assessment: the cornerstone to optimal pain management. Proc. 2000;13:236. doi:10.1080/08998280.2000.11927681
24. Alorfi NM. Prescribing patterns and pharmacological knowledge of analgesics among community pharmacists in Jeddah, Saudi Arabia. Bull Pharm Sci Assiut. 2023;46:647–657. doi:10.21608/BFSA.2023.301293
25. Kim KH, Seo HJ, Abdi S, Huh B. All about pain pharmacology: what pain physicians should know. Korean J Pain. 2020;33:108. doi:10.3344/KJP.2020.33.2.108
26. Mullins S, Hosseini F, Gibson W, Thake M. Physiological changes from ageing regarding pain perception and its impact on pain management for older adults. Clin Med. 2022;22:307. doi:10.7861/CLINMED.22.4.PHYS
27. Yong RJ, Mullins PM, Bhattacharyya N. Prevalence of chronic pain among adults in the United States. Pain. 2022;163:E328–E332. doi:10.1097/J.PAIN.0000000000002291
28. Alorfi NM, Alqurashi RS, Algarni AS. Assessment of community pharmacists’ knowledge about drug-drug interactions in Jeddah, Saudi Arabia. Front Pharmacol. 2023;14. doi:10.3389/FPHAR.2023.1209318
29. Alorfi NM, Ashour AM, Algarni AS, Alsolami FA, Alansari AM, Tobaiqy M. Assessment of the community pharmacists’ knowledge and attitudes toward pain and pain management in Saudi Arabia. Int J Gen Med. 2022;15:8527–8537. doi:10.2147/IJGM.S387066
30. Alorfi NM. Pharmacological treatments of fibromyalgia in adults; overview of Phase IV clinical trials. Front Pharmacol. 2022;13. doi:10.3389/FPHAR.2022.1017129
31. Schug SA, Robert Garrett W, Gillespie G. Opioid and non-opioid analgesics. Best Pract Res Clin Anaesthesiol. 2003;17:91–110. doi:10.1053/BEAN.2003.0267
32. Ghlichloo I, Gerriets V. Nonsteroidal Anti-inflammatory Drugs (NSAIDs). In: Treatment of Chronic Pain Conditions: A Comprehensive Handbook. springer; 2023:77–79. doi:10.1007/978-1-4939-6976-0_21
33. Pountos I, Georgouli T, Bird H, Giannoudis PV. Nonsteroidal anti-inflammatory drugs: prostaglandins, indications, and side effects. Int J Interf Cytokine Mediat Res. 2011;3:19–27. doi:10.2147/IJICMR.S10200
34. Green GA. Understanding NSAIDs: from aspirin to COX-2. Clin Cornerstone. 2001;3:50–59. doi:10.1016/S1098-3597(01)90069-9
35. Labianca R, Sarzi-Puttini P, Zuccaro SM, Cherubino P, Vellucci R, Fornasari D. Adverse effects associated with non-opioid and opioid treatment in patients with chronic pain. Clin Drug Investig. 2012;32:53–63. doi:10.2165/11630080-000000000-00000/METRICS
36. Vane JR, Botting RM. The mechanism of action of aspirin. Thromb Res. 2003;110:255–258. doi:10.1016/S0049-3848(03)00379-7
37. Risser A, Donovan D, Heintzman J, Page T. NSAID prescribing precautions. Am Fam Physician. 2009;80:1371–1378.
38. Blough ER, Wu M. Acetaminophen: beyond pain and fever-relieving. Front Pharmacol. 2011;2:72. doi:10.3389/FPHAR.2011.00072/BIBTEX
39. Botting RM. Mechanism of action of acetaminophen: is there a cyclooxygenase 3? Clin Infect Dis. 2000;31:S202–S210. doi:10.1086/317520
40. Serda M, Becker FG, Cleary M, et al. Acetaminophen (paracetamol): properties, clinical uses, and adverse effects. Uniw Slaski. 2012;7:1–24.
41. Sawynok J. Topical analgesics in neuropathic pain. Curr Pharm Des. 2005;11:2995–3004. doi:10.2174/1381612054865019
42. Stanos SP, Galluzzi KE. Topical therapies in the management of chronic pain. Postgrad Med. 2013;125(sup1):25–33. doi:10.1080/00325481.2013.1110567111
43. Hamza M, Dionne RA. Mechanisms of non-opioid analgesics beyond cyclooxygenase enzyme inhibition. Curr Mol Pharmacol. 2009;2:1. doi:10.2174/1874467210902010001
44. Langford RM. Pain management today—what have we learned? Clin Rheumatol. 2006;25:2–8. doi:10.1007/S10067-006-0311-5
45. Argoff CE. Topical analgesics in the management of acute and chronic pain. Mayo Clin Proc. 2013;88:195–205. doi:10.1016/J.MAYOCP.2012.11.015
46. Díaz-González F, Sánchez-Madrid F. NSAIDs: learning new tricks from old drugs. Eur J Immunol. 2015;45:679. doi:10.1002/EJI.201445222
47. Ziccardi P, Nappo F, Giugliano G, et al. Reduction of inflammatory cytokine concentrations and improvement of endothelial functions in obese women after weight loss over one year. Circulation. 2002;105:804–809. doi:10.1161/hc0702.104279
48. Bacchi S, Palumbo P, Sponta A, Coppolino MF. Clinical pharmacology of non-steroidal anti-inflammatory drugs: a review. Antiinflamm Antiallergy Agents Med Chem. 2012;11:52–64. doi:10.2174/187152312803476255
49. Marsico F, Paolillo S, Filardi PP. NSAIDs and cardiovascular risk. J Cardiovasc Med. 2017;18:e40–e43. doi:10.2459/JCM.0000000000000443
50. Ramachandran A, Jaeschke H. Acetaminophen hepatotoxicity. Semin Liver Dis. 2019;39:221–234. doi:10.1055/S-0039-1679919/ID/JR1800073-44
51. Hengge UR, Ruzicka T, Schwartz RA, Cork MJ. Adverse effects of topical glucocorticosteroids. J Am Acad Dermatol. 2006;54:1–15. doi:10.1016/J.JAAD.2005.01.010
52. Paul AK, Smith CM, Rahmatullah M, et al. Opioid analgesia and opioid-induced adverse effects: a review. Pharm. 2021;14:1091. doi:10.3390/PH14111091
53. Kotlińska-Lemieszek A, Żylicz Z. Less well-known consequences of the long-term use of opioid analgesics: a comprehensive literature review. Drug Des Devel Ther. 2022;16:251–264. doi:10.2147/DDDT.S342409
54. Wood E, Solomon ED, Hadland SE. Universal precautions for people at risk of opioid overdose in North America. JAMA Intern Med. 2023;183(5):401. doi:10.1055/s-0039-1679919
55. Inoue K, Nomura M. The neuropathology of drug addictions and substance misuse: assays for fentanyl. In: Neuropathology of Drug Addictions and Substance Misuse. Vol. 3. Academic Press; 2016:619–630. doi:10.1016/B978-0-12-800634-4.00063-9
56. Trescot AM, Datta S, Lee M, Hans H. Opioid pharmacology. Pain Physician. 2008;11(3;2s):S133–S153. doi:10.36076/ppj.2008/11/s133
57. Alshehri FS, Alghamdi BS, Hakami AY, Alshehri AA, Althobaiti YS. Melatonin attenuates morphine-induced conditioned place preference in Wistar rats. Brain Behav. 2021;11(12):e2397. doi:10.1002/BRB3.2397
58. Kerrigan S, Goldberger BA. Opioids. In: Princ Forensic Toxicol.
59. Skolnick P. Treatment of overdose in the synthetic opioid era. Pharmacol Ther. 2022;233:108019. doi:10.1016/J.PHARMTHERA.2021.108019
60. Valentino RJ, Volkow ND. Untangling the complexity of opioid receptor function. Neuropsychopharmacol. 2018;43(13):2514–2520. doi:10.1038/s41386-018-0225-3
61. Parsells Kelly J, Cook SF, Kaufman DW, Anderson T, Rosenberg L, Mitchell AA. Prevalence and characteristics of opioid use in the US adult population. Pain. 2008;138(3):507–513. doi:10.1016/J.PAIN.2008.01.027
62. Sobanski P, Krajnik M, Shaqura M, Bloch-Boguslawska E, Schäfer M, Mousa SA. The presence of mu-, delta-, and kappa-opioid receptors in human heart tissue. Heart Vessels. 2014;29:855–863. doi:10.1007/S00380-013-0456-5/FIGURES/5
63. Vanderah TW. Delta and kappa opioid receptors as suitable drug targets for pain. Clin J Pain. 2010;26(Supplement 10):S10–S15. doi:10.1097/AJP.0B013E3181C49E3A
64. Leibovici BL. Medical prescription in the context of drug prohibition: the example of opiates. In: Living with Drugs. Elsevier; 2020:295–303. doi:10.1016/B978-1-78548-317-2.50021-0
65. Smith H, Bruckenthal P. Implications of opioid analgesia for medically complicated patients. Drugs Aging. 2012;27:417–433. doi:10.2165/11536540-000000000-00000
66. Stephan BC, Parsa FD. Avoiding opioids and their harmful side effects in the postoperative patient: exogenous opioids, endogenous endorphins, wellness, mood, and their relation to postoperative pain. Hawaii J Med Public Health. 2016;75:63.
67. Machelska H, Celik M. Advances in achieving opioid analgesia without side effects. Front Pharmacol. 2018;9:1388. doi:10.3389/FPHAR.2018.01388/BIBTEX
68. Alshehri FS. Tapentadol: a review of experimental pharmacology studies, clinical trials, and recent findings. Drug Des Devel Ther. 2023;17:851–861. doi:10.2147/DDDT.S402362
69. Pattinson KTS. Opioids and the control of respiration. Br J Anaesth. 2008;100:747–758. doi:10.1093/BJA/AEN094
70. Camilleri M, Lembo A, Katzka DA. Opioids in gastroenterology: treating adverse effects and creating therapeutic benefits. Clin Gastroenterol Hepatol. 2017;15:1338. doi:10.1016/J.CGH.2017.05.014
71. Verhamme KMC, Sturkenboom MCJM, Stricker BHC, Bosch R. Drug-induced urinary retention: incidence, management and prevention. Drug Saf. 2008;31:373–388. doi:10.2165/00002018-200831050-00002
72. Seyfried O, Hester J. Opioids and endocrine dysfunction. Br J Pain. 2012;6:17. doi:10.1177/2049463712438299
73. Morgan MM, Christie MJ. Analysis of opioid efficacy, tolerance, addiction and dependence from cell culture to human. Br J Pharmacol. 2011;164:1322. doi:10.1111/J.1476-5381.2011.01335.X
74. Alford DP, Compton P, Samet JH. Acute pain management for patients receiving maintenance methadone or buprenorphine therapy. Ann Intern Med. 2006;144:127. doi:10.7326/0003-4819-144-2-200601170-00010
75. Wallace MS, Papp A. Opioid Withdrawal. In: Challenging Cases and Complication Management in Pain Medicine. Springer; 2023:15–20. doi:10.1007/978-3-319-60072-7_3
76. Pergolizzi JV, Raffa RB, Rosenblatt MH. Opioid withdrawal symptoms, a consequence of chronic opioid use and opioid use disorder: current understanding and approaches to management. J Clin Pharm Ther. 2020;45:892–903. doi:10.1111/JCPT.13114
77. Khan MIA, Walsh D, Brito-Dellan N. Opioid and adjuvant analgesics: compared and contrasted. Am J Hosp Palliat Care. 2011;28:378–383. doi:10.1177/1049909111410298
78. Knotkova H, Pappagallo M. Adjuvant analgesics. Anesthesiol Clin. 2007;25:775–786. doi:10.1016/J.ANCLIN.2007.07.006
79. Mitra R, Jones S. Adjuvant analgesics in cancer pain: a review. Am J Hosp Palliat Care. 2012;29(1):70–79. doi:10.1177/1049909111413256
80. Micó JA, Ardid D, Berrocoso E, Eschalier A. Antidepressants and pain. Trends Pharmacol Sci. 2006;27:348–354. doi:10.1016/J.TIPS.2006.05.004
81. Moore RA, Derry S, Aldington D, Cole P, Wiffen PJ. Amitriptyline for neuropathic pain and fibromyalgia in adults. Cochrane Database Syst Rev. 2012. doi:10.1002/14651858.CD008242.PUB2/INFORMATION/EN
82. Patetsos E, Horjales-Araujo E. Treating chronic pain with SSRIs: what do we know? Pain Res Manag. 2016;2016:1–17. doi:10.1155/2016/2020915
83. Raouf M, Glogowski AJ, Bettinger JJ, Fudin J. Serotonin-norepinephrine reuptake inhibitors and the influence of binding affinity (Ki) on analgesia. J Clin Pharm Ther. 2017;42:513–517. doi:10.1111/JCPT.12534
84. Durkin B, Page C, Glass P. Pregabalin for the treatment of postsurgical pain. Expert Opin Pharmacother. 2010;11(16):2751–2758. doi:10.1517/14656566.2010.526106
85. Argoff CE. The coexistence of neuropathic pain, sleep, and psychiatric disorders: a novel treatment approach. Clin J Pain. 2007;23(1):15–22. doi:10.1097/01.AJP.0000210945.27052.B3
86. Mula M, Pini S, Cassano GB. The role of anticonvulsant drugs in anxiety disorders: a critical review of the evidence. J Clin Psychopharmacol. 2007;27(3):263–272. doi:10.1097/JCP.0B013E318059361A
87. Jensen TS. Anticonvulsants in neuropathic pain: rationale and clinical evidence. Eur J Pain. 2002;6(SA):61–68. doi:10.1053/EUJP.2001.0324
88. Backonja -M-M. Use of anticonvulsants for treatment of neuropathic pain. Neurology. 2002;59(Issue 5, Supplement 2):S14–S17. doi:10.1212/WNL.59.5_SUPPL_2.S14
89. Deer TR, Serafini M, Buchser E, Ferrante FM, Hassenbusch SJ. Intrathecal bupivacaine for chronic pain: a review of current knowledge. Neuromodulation. 2002;5:196–207. doi:10.1046/J.1525-1403.2002.02030.X
90. Yanagidate F, Strichartz GR. Local anesthetics. Handb Exp Pharmacol. 2007;177:95–127. doi:10.1007/978-3-540-33823-9_4
91. Casale R, Symeonidou Z, Bartolo M. Topical treatments for localized neuropathic pain. Curr Pain Headache Rep. 2017;21:1–9. doi:10.1007/S11916-017-0615-Y/TABLES/1
92. Scholz A. Mechanisms of (local) anaesthetics on voltage-gated sodium and other ion channels. Br J Anaesth. 2002;89(1):52–61. doi:10.1093/bja/aef163
93. Taylor A, McLeod G. Basic pharmacology of local anaesthetics. Br J Anaesth Educ. 2020;20(2):34. doi:10.1016/J.BJAE.2019.10.002
94. Mazoit JX, Dalens BJ. Pharmacokinetics of local anaesthetics in infants and children. Clin Pharmacokinet. 2004;43:17–32. doi:10.2165/00003088-200443010-00002/FIGURES/5
95. Bucklin BA, Chestnut DH, Hawkins JL. Intrathecal opioids versus epidural local anesthetics for labor analgesia: a meta-analysis. Reg Anesth Pain Med. 2002;27:23–30. doi:10.1053/RAPM.2002.29111
96. Bagshaw KR, Hanenbaum CL, Carbone EJ, et al. Pain management via local anesthetics and responsive hydrogels. Ther Deliv. 2015;6:165. doi:10.4155/TDE.14.95
97. El-Boghdadly K, Pawa A, Chin KJ. Local anesthetic systemic toxicity: current perspectives. Local Reg Anesth. 2018;11:35–44. doi:10.2147/LRA.S154512
98. Dillane D, Finucane BT. Local anesthetic systemic toxicity. Can J Anaesth. 2010;57:368–380. doi:10.1007/S12630-010-9275-7
99. Gitman M, Barrington MJ. Local anesthetic systemic toxicity: a review of recent case reports and registries. Reg Anesth Pain Med. 2018;43:124–130. doi:10.1097/AAP.0000000000000721
100. Coutinho AE, Chapman KE. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistic insights. Mol Cell Endocrinol. 2011;335:2. doi:10.1016/J.MCE.2010.04.005
101. Arroll B, Goodyear-Smith F. Corticosteroid injections for osteoarthritis of the knee: meta-analysis. Br Med J. 2004;328(7444):869. doi:10.1136/BMJ.38039.573970.7C
102. van der Goes MC, Jacobs JW, Bijlsma JW. The value of glucocorticoid co-therapy in different rheumatic diseases - positive and adverse effects. Arthritis Res Ther. 2014;16(Suppl 2):1–13. doi:10.1186/AR4686/FIGURES/3
103. Wharton S, Raiber L, Serodio KJ, Lee J, Christensen RAG. Medications that cause weight gain and alternatives in Canada: a narrative review. Diabetes Metab Syndr Obes. 2018;11:427–438. doi:10.2147/DMSO.S171365
104. Savas M, Wester VL, Staufenbiel SM, et al. Systematic evaluation of corticosteroid use in obese and non-obese individuals: a Multi-cohort Study. Int J Med Sci. 2017;14:615. doi:10.7150/IJMS.19213
105. Brown ES, Chandler PA. Mood and cognitive changes during systemic corticosteroid therapy. Prim Care Companion J Clin Psychiatry. 2001;3:17. doi:10.4088/PCC.V03N0104
106. Oray M, Abu Samra K, Ebrahimiadib N, Meese H, Foster CS. Long-term side effects of glucocorticoids. Expert Opin Drug Saf. 2016;15:457–465. doi:10.1517/14740338.2016.1140743
107. Galafassi GZ, Simm Pires de Aguiar PH, Simm RF, et al. Neuromodulation for medically refractory neuropathic pain: spinal cord stimulation, deep brain stimulation, motor cortex stimulation, and posterior insula stimulation. World Neurosurg. 2021;146:246–260. doi:10.1016/J.WNEU.2020.11.048
108. Alamri A, Pereira EAC. Deep brain stimulation for chronic pain. Neurosurg Clin N Am. 2022;33:311–321. doi:10.1016/J.NEC.2022.02.013
109. Johnson MI, Paley CA, Jones G, Mulvey MR, Wittkopf PG. Efficacy and safety of transcutaneous electrical nerve stimulation (TENS) for acute and chronic pain in adults: a systematic review and meta-analysis of 381 studies (the meta-TENS study). BMJ Open. 2022;12. doi:10.1136/BMJOPEN-2021-051073
110. Capozza MA, Triarico S, Mastrangelo S, Attinà G, Maurizi P, Ruggiero A. Narrative review of intrathecal drug delivery (IDD): indications, devices and potential complications. Ann Transl Med. 2021;9:186. doi:10.21037/ATM-20-3814
111. George SZ, Goode AP. Physical therapy and opioid use for musculoskeletal pain management: competitors or companions? Pain Rep. 2020;5:E827. doi:10.1097/PR9.0000000000000827
112. Chimenti RL, Frey-Law LA, Sluka KA, Chimenti RL, Frey-Law LA, Sluka KA. A mechanism-based approach to physical therapist management of pain. Phys Ther. 2018;98:302–314. doi:10.1093/PTJ/PZY030
113. Rakel B, Barr JO. Physical modalities in chronic pain management. Nurs Clin North Am. 2003;38:477–494. doi:10.1016/S0029-6465(02)00097-X
114. Bao S, Qiao M, Lu Y, Jiang Y. Neuroimaging mechanism of cognitive behavioral therapy in pain management. Pain Res Manag. 2022;2022. doi:10.1155/2022/6266619
115. Tournaire M, Theau-Yonneau A. Complementary and alternative approaches to pain relief during labor. Evid Based Complement Alternat Med. 2007;4:409–417. doi:10.1093/ECAM/NEM012
116. Singh P, Chaturvedi A. Complementary and alternative medicine in cancer pain management: a systematic review. Indian J Palliat Care. 2015;21:105. doi:10.4103/0973-1075.150202
117. Hua S, Cabot PJ. PAIN - novel targets and new technologies. Front Pharmacol. 2014;5:111026. doi:10.3389/FPHAR.2014.00211/BIBTEX
118. Hone AJ, McIntosh JM. Nicotinic acetylcholine receptors: therapeutic targets for novel ligands to treat pain and inflammation. Pharmacol Res. 2023;190:106715. doi:10.1016/J.PHRS.2023.106715
119. Sharma A, Behl T, Sharma L, et al. Exploring the molecular pathways and therapeutic implications of angiogenesis in neuropathic pain. Biomed Pharmacother. 2023;162:114693. doi:10.1016/J.BIOPHA.2023.114693
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.