")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Tenofovir versus Entecavir on Outcomes of Hepatitis B Virus-Related Hepatocellular Carcinoma After FOLFOX-Hepatic Arterial Infusion Chemotherapy
Authors Zheng Z , Wang J, Wu T , He M, Wang J, Pan Y , Chen J , Hu D, Xu L , Zhang Y , Chen M, Zhou Z
Received 18 August 2023
Accepted for publication 22 November 2023
Published 30 November 2023 Volume 2023:10 Pages 2117—2132
DOI https://doi.org/10.2147/JHC.S436062
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmed Kaseb
Zhikai Zheng,1,2,* Jiongliang Wang,1,2,* Tianqing Wu,1,2,* Minrui He,1,2,* Juncheng Wang,1,2 Yangxun Pan,1,2 Jinbin Chen,1,2 Dandan Hu,1,2 Li Xu,1,2 Yaojun Zhang,1,2 Minshan Chen,1,2 Zhongguo Zhou1,2
1Department of Liver Surgery, Sun Yat-sen University Cancer Center, Guangzhou, People’s Republic of China; 2Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhongguo Zhou; Minshan Chen, Department of Liver Surgery, Sun Yat-sen University Cancer Center, Dongfeng Road East 651, Guangzhou, Guangdong, 510060, People’s Republic of China, Tel +86-20-87343117, Email [email protected]; [email protected]
Purpose: The efficacy of entecavir (ETV) versus tenofovir (TDF) on the prognosis of hepatitis B virus (HBV)-related hepatocellular carcinoma (HCC) patients who underwent FOLFOX-hepatic arterial infusion chemotherapy (HAIC) remains unclear. In this study, we compared the outcomes between ETV and TDF in HBV-related advanced HCC patients who underwent FOLFOX-HAIC.
Methods: A total of 683 patients diagnosed with HBV-related HCC who underwent FOLFOX-HAIC and received TDF or ETV between January 2016 and December 2021 were included. Overall survival (OS), progression-free survival (PFS), HBV reactivation, and liver function of patients were compared between the ETV and TDF groups by propensity score matching (PSM).
Results: In the PSM cohort, for all patients and patients with ≥ 4 cycles of FOLFOX-HAIC, the median OS in the ETV group (15.2 months, 95% CI: 13.0– 17.4 months; 16.6 months, 95% CI: 14.8– 18.5 months; respectively) was shorter than that in the TDF group (23.0 months, 95% CI: 10.3– 35.6 months; 27.3 months, 95% CI: 16.5-NA months; p=0.024, p=0.028; respectively). The median PFS in the ETV group (8.7 months, 95% CI: 7.9– 9.5 months; 8.9 months, 95% CI: 8.0– 9.8 months; respectively) was also shorter than that in the TDF group (11.8 months, 95% CI: 8.0– 15.6 months; 12.7 months, 95% CI: 10.8– 14.6 months; p=0.036, p=0.025; respectively). The rate of HBV reactivation in the ETV group was higher than that in the TDF group (12.3% vs 6.3%, p=0.040; 16.5% vs 6.2%, p=0.037, respectively). For liver function, the rate of ALBI grade that remained stable or improved in the ETV group was lower than that in the TDF group (44.6% vs 57.6%, p=0.006; 37.2% vs 53.8%, p=0.019, respectively).
Conclusion: Compared with ETV, TDF was associated with a better prognosis, lower proportion of HBV reactivation, and better preservation of liver function in advanced HBV-HCC patients who underwent FOLFOX-HAIC, especially those who received ≥ 4 cycles.
Keywords: tenofovir, entecavir, hepatitis B virus, hepatocellular carcinoma, hepatic arterial infusion chemotherapy
Introduction
Hepatocellular carcinoma (HCC) is the sixth most common malignancy and the third reason of cancer-related mortality worldwide.1 Hepatitis B virus (HBV) infection is the major risk factor for HCC, especially in Asia, and can drive carcinogenesis in the human genome through integrations.2 Moreover, a high HBV virus load has been considered as an independent risk factor for the progression of HCC.3 Several studies have shown that antiviral treatment is associated with the improved prognosis of HBV-related HCC patients who underwent various antitumor treatments.3–9 Antiviral treatment is important for HBV-related HCC patients.
For advanced-stage HCC, hepatic artery infusion chemotherapy (HAIC) may be an optional treatment that can improve therapeutic efficacy. It has been reported that compared with sorafenib, HAIC using the FOLFOX regimen had better survival in advanced HCC, even with a high intrahepatic tumor burden.10 FOLFOX-HAIC also significantly improved overall survival in patients with unresectable hepatocellular carcinoma whose largest diameter was ≥7 cm compared with transarterial chemoembolization (TACE).11 When combined with immunotherapy or targeted therapy, FOLFOX-HAIC could also improve the prognosis of patients.12–14 For HBV-related HCC patients who underwent FOLFOX-HAIC, antiviral treatment was reported to be associated with less HBV reactivation and longer overall survival.15
At present, both entecavir (ETV) and tenofovir (TDF) are recommended as first-line antiviral drugs because of their similarly high efficacy and low rate of adverse events and resistance.16,17 Several studies have compared the effect of ETV and TDF on prognosis after hepatectomy and ablation, but the results were controversial.18–21 Similarly, the efficacy of ETV vs TDF therapy on the prognosis of HBV-related HCC patients who underwent FOLFOX-HAIC remains unclear.
Therefore, in this study, we aimed to compare the outcomes between entecavir and tenofovir in HBV-related advanced-stage HCC patients who underwent FOLFOX-HAIC.
Materials and Methods
Patients
In this study, we retrospectively analyzed patients with a diagnosis of hepatitis B-related HCC who received FOLFOX-HAIC and were treated with either ETV or TDF for chronic hepatitis B (CHB). Patient data was obtained from a database of 2924 consecutive patients from January 2016 to December 2021 at Sun Yat-sen University Cancer Center (SYSUCC).
Patients were eligible for the study if they met the following inclusion criteria: (1) aged 18 years or older; (2) diagnosed with unresectable HBsAg-positive HCC; (3) Child‒Pugh grade A or B; (4) initially received FOLFOX-HAIC at SYSUCC; and (5) initially treated with either TDF or ETV for CHB. The diagnosis of HCC was based on pathology or noninvasive criteria according to the American Association for the Study of Liver Diseases (AASLD) guidelines.22 Unresectability was confirmed by hepatobiliary surgeons after multidisciplinary review and defined as the inability to achieve R0 resection due to multifocal liver disease, extensive vascular involvement, distant metastasis, insufficient functional liver remnant, or a combination of these factors.
Patients who met the following criteria were excluded: (1) treated with at least one other local antitumor treatment, including hepatectomy, ablation, liver transplantation, TACE, and radiotherapy before FOLFOX-HAIC; (2) less than 2 cycles of FOLFOX-HAIC; (3) negative test for HBsAg; (4) treated with neither TDF nor ETV, including lamivudine, telbivudine, clevudine and other antiviral drugs, or combined with other antiviral treatments; (5) initiation of ETV or TDF therapy within 1 week after FOLFOX-HAIC or within 1 month before FOLFOX-HAIC; (6) younger than 18; (7) coinfection with hepatitis C virus; (8) history of other malignancies or nonmalignant severe illness; and (9) Child‒Pugh grade C.
Finally, a total of 683 patients who were treated with either ETV (n=522) or TDF (n=161) were included in the analysis (Figure 1). This study was approved by the ethics committee of Sun Yat-sen University Cancer Center (Protocol code: B2022-238-01).
 |
Figure 1 Flowchart of enrolled patients. |
Antiviral Treatment
In the Entecavir group, patients received entecavir 0.5mg orally every day. On the contrary, patients in the Tenofovir group took tenofovir disoproxil fumarate 0.3g daily. All patients were suggested to continue treatment with ETV or TDF during antitumor treatment.
FOLFOX-HAIC Procedure
FOLFOX-HAIC was performed every 3 weeks and was administered as follows: a catheter/microcatheter was placed in the main feeding hepatic artery of the tumor. Then, FOLFOX-based chemotherapy was delivered into the liver in order via a HAIC pump through the catheter/microcatheter: oxaliplatin, 130 mg/m2, for 3 hours; leucovorin, 400 mg/m2, for 2 hours; fluorouracil, 400 mg/m2, bolus at hour 5; and 2400 mg/m2 over 46 hours.14,23 FOLFOX-HAIC was repeated until intolerable adverse events was observed, until the patients refused to accept the treatment, or until the patients could not benefit from it, which was confirmed by the MDT panel.
During the treatment of HAIC, patients may be combined with systemic treatment including the anti-PDL1/PD1 or tyrosine kinase inhibitor due to the needs of the treatment and patients’ option. The details were showed in the Supplementary Table 1.
Baseline Characteristics, Outcomes and Follow-Up
Baseline characteristics, including age, sex, diabetes, hypertension, platelet (PLT) count, alanine aminotransferase (ALT), aspartate aminotransferase (AST), albumin (ALB), total bilirubin (TBil), prothrombin time (PT), alpha fetoprotein (AFP), protein induced by vitamin K absence or antagonist-II (PIVKA-II), HBV-DNA, cirrhosis, tumor number, tumor size, macrovascular invasion (MVI), metastasis, Child‒Pugh class, albumin to bilirubin score (ALBI grade) before the first treatment, cycles of FOLFOX-HAIC, and antitumor regimen, were collected and analyzed. Cirrhosis was diagnosed based on ultrasound (US), computerized tomography (CT), or magnetic resonance imaging (MRI). The tumor size was defined as the maximum diameter of the tumor. Macrovascular invasion was defined as invasion of hepatic vein and its branches, the portal vein and its branches, or inferior vena cava.
The primary outcomes were overall survival (OS), which was defined as the time from first treatment to death regardless of any cause, and progression-free survival (PFS), which was defined as the time from the first treatment until progression or death from any cause. PFS was evaluated according to the Response Evaluation Criteria in Solid Tumors (RECIST). The secondary outcomes were the rate of HBV reactivation and liver function after FOLFOX-HAIC. HBV reactivation was defined as a more than 10-fold increase in the serum HBV-DNA level compared with the nadir (lowest value) level for patients with detectable viral load or a greater than 200 IU/mL HBV-DNA level for patients with undetectable viral load during follow-up.3,6,16 ALBI grade, which performed at least as well as the Child‒Pugh class and is known as a simple, evidence-based, objective, effective method of assessing liver function in HCC, was used to evaluate liver function in our study.24
All patients were suggested to continue treatment with ETV or TDF as before. Serum AFP levels, serum HBV-DNA levels, and liver function tests were inspected at the end of each cycle. Contrast-enhanced CT or MRI was performed 1 week after every 2 cycles to evaluate tumor response.
Statistical Analysis
Continuous variables are presented as the mean ± standard deviation (SD) or median ± interquartile range according to normal or nonnormal distribution and were compared by Student’s t-tests or rank sum tests as appropriate. Categorical variables are presented as frequencies and percentages, which were compared by chi-squared tests or Fisher’s exact tests. To minimize the effect of selection bias and potential confounding between the two groups, we performed 1-to-3 propensity score matching (PSM) considering variables including age, sex, diabetes, hypertension, PLT, ALT, AST, ALB, TBil, PT, AFP, PIVKA-II, log10HBV-DNA, cirrhosis, tumor number, tumor size, MVI, metastasis, Child‒Pugh class, ALBI grade before the first treatment, cycles of FOLFOX-HAIC, and the antitumor regimen. One patient treated with TDF could match up to three patients treated with ETV.25,26 PSM was conducted by the R package “MatchIt”, and the caliper width was 0.2. Kaplan‒Meier curves were generated to estimate OS and PFS, and differences between curves were evaluated using a log rank test. Univariable and multivariable Cox proportional hazards models with a forward conditional stepwise procedure were used to assess the risk factors for OS and PFS in the full cohort. Variables that were statistically significant in the univariable analysis (p<0.05) were selected for multivariable analysis. All statistical analyses above were completed by SPSS version 26.0 and R statistical software version 4.1.2. A p value <0.05 was considered statistically significant.
Results
Baseline Characteristics of the Patients
There were 683 patients with a diagnosis of HBsAg-positive HCC who received FOLFOX-HAIC initially included in the study, of which 522 patients received ETV and 161 patients received TDF. Among them, 609 (89.2%) patients were male, and the median age was 51 years (range, 18–78 years). A total of 419 (61.3%) patients were diagnosed with cirrhosis. The median tumor diameter was 103 mm (range, 19–231 mm), and the number of patients with metastasis was 133 (19.5%), while the majority of patients had multiple tumors (n=458, 67.1%) and MVI (n=388, 56.8%). The median serum log10HBV-DNA was 3.72 IU/mL (range, 0–8.34 IU/mL). The number of patients with Child‒Pugh class A was 647 (94.7%), and the number of patients with Child‒Pugh class B was 36 (5.3%). The number of patients with ALBI grade 1 was 380 (55.6%), while the number of patients with grade 2 was 302 (44.2%), and the number of patients with grade 3 was 1 (0.1%). The median number of FOLFOX-HAIC cycles received was 3 (range, 2–8). For the antitumor regimen, 243 (35.6%) patients received FOLFOX-HAIC alone, 280 (41.0%) patients received FOLFOX-HAIC plus systemic treatment, including targeted therapy or immunotherapy, 70 (10.2%) patients received conversion surgery after FOLFOX-HAIC, and 90 (13.2%) patients received conversion surgery after the combination of FOLFOX-HAIC and systemic treatment.
In the full cohort, there was no significant difference in age, sex, diabetes, hypertension, PLT, PT, ALT, AST, ALB, TBil, AFP, serum log10HBV-DNA, cirrhosis, tumor number, MVI, metastasis, ALBI grade, or cycles of FOLFOX-HAIC between the two groups. However, the levels of PIVKA-II in the ETV group were higher than those in the TDF group (p=0.022), and more patients had larger tumor size and liver function with Child‒Pugh class A in the ETV group than in the TDF group (p=0.047; p=0.009). Additionally, more patients were treated with FOLFOX-HAIC alone in the ETV group, while more patients were treated with the combination of FOLFOX-HAIC and systemic treatment in the TDF group (p=0.039). The baseline characteristics of the two groups are shown in Table 1.
 |
Table 1 Baseline Characteristics of Patients Before PSM (n=683) and After PSM (n=566) |
To minimize the difference between the two groups, 1-to-3 PSM was performed. In the matched cohort, 566 patients were included, of whom 408 patients were treated with ETV and 158 patients were treated with TDF. Baseline characteristics after PSM between the two groups are shown in Table 1. After matching, there was no significant difference between the two groups.
The TDF Group Had Better Overall Survival and Progression-Free Survival Than the ETV Group
In the whole cohort, the 1-year and 2-year OS rates for the ETV group and the TDF group were 59.1% and 34.4% and 69.3% and 49.2%, respectively. The median OS in the ETV group (15.0 months, 95% CI: 13.2–16.9 months) was shorter than that in the TDF group (23.0 months, 95% CI: 10.3–35.6 months, p=0.0077, Figure 2). The 1-year and 2-year PFS rates for the ETV group and the TDF group were 33.6% and 16.9% and 48.9% and 27.4%, respectively. The median PFS was 8.4 (95% CI: 7.7–9.0) months and 10.8 (95% CI: 7.2–14.4) months in the ETV and TDF groups, respectively. The PFS in the ETV group was also shorter than that in the TDF group (p=0.0097, Figure 3).
 |
Figure 2 Kaplan‒Meier curves of overall survival after HAIC between the two groups in the full cohort (A) and in the matched cohort (B), after HAIC with < 4 cycles between the two groups in the full cohort (C) and in the matched cohort (D), and after HAIC with ≥ 4 cycles between the two groups in the full cohort (E) and in the matched cohort (F). |
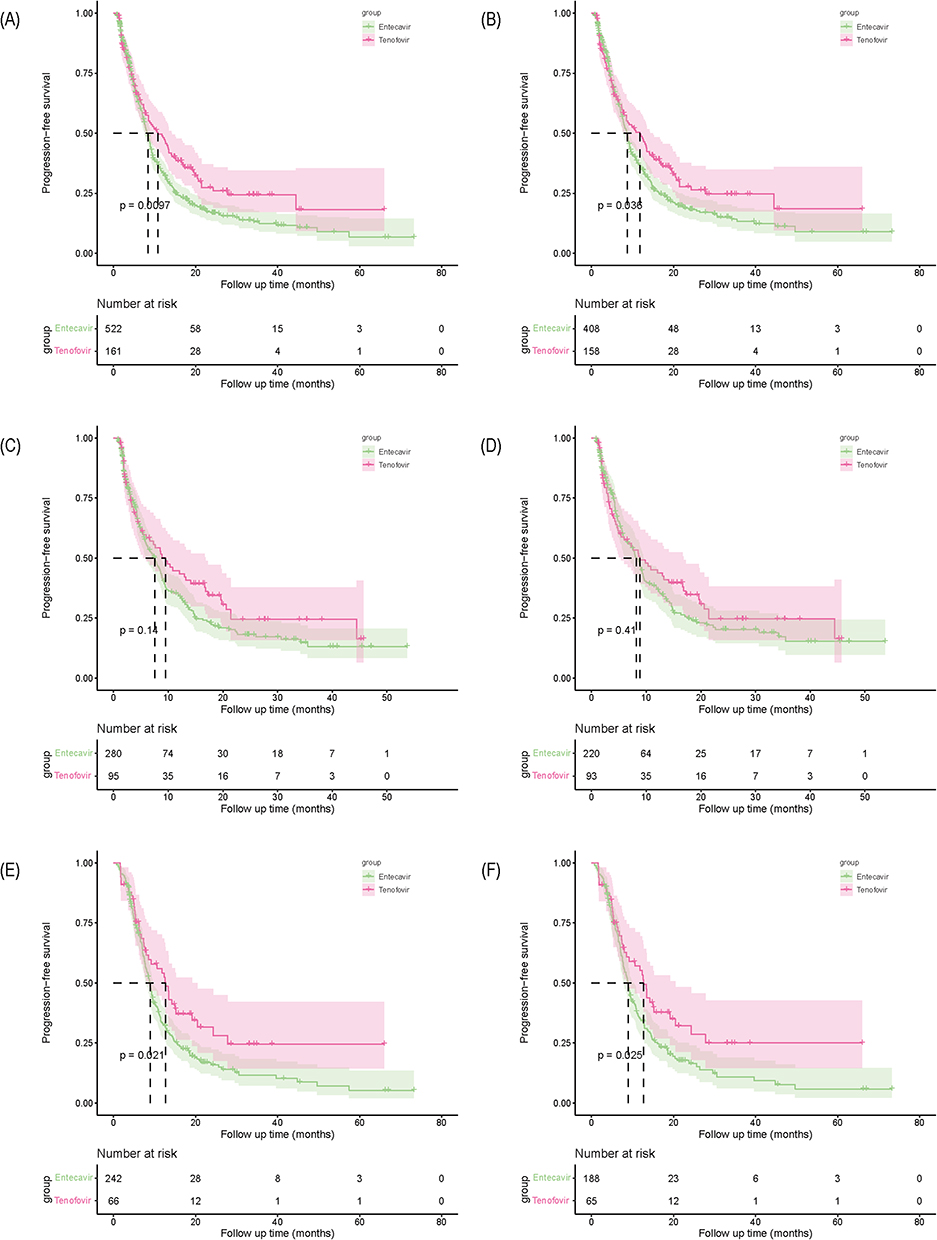 |
Figure 3 Kaplan‒Meier curves of progression-free survival after HAIC between the two groups in the full cohort (A) and in the matched cohort (B), after HAIC with < 4 cycles between the two groups in the full cohort (C) and in the matched cohort (D), and after HAIC with ≥ 4 cycles between the two groups in the full cohort (E) and in the matched cohort (F). |
Univariable and multivariable analyses revealed that patients with MVI (HR=1.339, 95% CI: 1.075–1.667, p=0.009), a higher level of serum AST (HR=1.002, 95% CI: 1.001–1.004, p=0.005), antitumor treatment with FOLFOX-HAIC alone (HR=0.424, 95% CI: 0.370–0.486, p<0.001), and fewer cycles of FOLFOX-HAIC (HR=0.656, 95% CI: 0.532–0.809, p<0.001) were significantly associated with unfavorable OS, while antitumor treatment with FOLFOX-HAIC alone (HR=0.699, 95% CI: 0.628–0.778, p<0.001) and antiviral treatment with ETV (HR=0.785, 95% CI: 0.628–0.982, p=0.034) were significantly associated with unfavorable PFS (Table 2).
 |
Table 2 Univariate and Multivariate Analyses of Prognostic Factors for Overall Survival and Progression-Free Survival |
After matching, the median OS in the ETV group was 15.2 (95% CI: 13.0–17.4) months, and that in the TDF group was 23.0 (95% CI: 10.3–35.6) months. The median OS in the ETV group was shorter than that in the TDF group (p=0.024, Figure 2). The median PFS in the ETV group (8.7 months, 95% CI: 7.9–9.5 months) was also shorter than that in the TDF group (11.8 months, 95% CI: 8.0–15.6 months, p=0.036, Figure 3). In the subgroup analysis by the number of FOLFOX-HAIC cycles, for patients with ≥ 4 FOLFOX-HAIC cycles, the median OS in the ETV group (16.6 months, 95% CI: 14.8–18.5 months) was shorter than that in the TDF group (27.3 months, 95% CI: 16.5-NA months, p=0.028, Figure 2). Similarly, the median PFS in the ETV group (8.9 months, 95% CI: 8.0–9.8 months) was shorter than that in the TDF group (12.7 months, 95% CI: 10.8–14.6 months, p=0.025, Figure 3). However, there was no significant difference in OS and PFS between the two groups for patients with < 4 cycles of FOLFOX-HAIC (p=0.28 and p=0.41, respectively, Figures 2 and 3).
HBV Reactivation and Liver Function
In the entire cohort, HBV reactivation presented in 66 (9.7%) patients, 56 (10.7%) patients in the ETV group and 10 (6.2%) patients in the TDF group. The rate in the ETV group was higher than that in the TDF group, although there was no significant difference (p=0.090, Supplementary Table 2). For liver function, compared with the ALBI grade before FOLFOX-HAIC, the rate of ALBI grade that remained stable or improved in the ETV group was lower than that in the TDF group (43.3% vs 57.8%, p=0.001, Supplementary Table 2 and Supplementary Figure 1).
In the PSM cohort, the rates of HBV reactivation in the ETV group of all patients and patients with ≥ 4 cycles FOLFOX-HAIC were higher than those in the TDF group (12.3% vs 6.3%, p=0.040; 16.5% vs 6.2%, p=0.037, respectively). In contrast, the rates of ALBI grade that remained stable or improved in the ETV group of all patients and patients with ≥ 4 cycles FOLFOX-HAIC were lower than those in the TDF group (44.6% vs 57.6%, p=0.006; 37.2% vs 53.8%, p=0.019; respectively, Table 3 and Figure 4). However, there were no significant differences in the rates of HBV reactivation and ALBI grade change between the two groups of patients with < 4 cycles FOLFOX-HAIC (p=0.515, p=0.131, respectively, Table 3 and Figure 4).
 |
Table 3 HBV Reactivation During HAIC and the ALBI Grade Remained Stable or Improved After HAIC in the Two Groups in the Matched Cohort |
 |
Figure 4 Sankey diagram of ALBI grade change after HAIC in the matched cohort of all patients (A), of patients with < 4 cycles of HAIC (B), and of patients with ≥ 4 cycles of HAIC (C). |
Discussion
In the present study, we analyzed 683 patients with a diagnosis of HBsAg-positive HCC treated with FOLFOX-HAIC who received ETV (n=522) or TDF (n=161) antiviral treatment. We found that TDF treatment was associated with better overall survival, better progression-free survival, a lower proportion of HBV reactivation and better preservation of liver function in the matched cohort of HBsAg-positive HCC patients treated with FOLFOX-HAIC, especially those treated with ≥ 4 cycles FOLFOX-HAIC, compared to ETV therapy.
For advanced-stage HCC, great progression has been made in the treatment. There are various recent advances in the treatment, such as TACE, HAIC, radiotherapy, immunotherapy, target therapy, and the combination of these treatments like FOLFOX-HAIC combined with immunotherapy or targeted therapy, external radiotherapy combined with sorafenib, PD-1 Inhibitors combined with antiangiogenic therapy and TACE.12–14,27,28
There is a consensus that antiviral treatment following antitumor therapy is recommended for patients with HBV-related HCC.29,30 Antiviral treatment can improve the prognosis of HBV-related HCC patients undergoing various antitumor treatments. Huang et al5 Huang et al4 and Sohn et al31 all reported that the recurrence-free survival (RFS) and overall survival for patients with antiviral treatment were significantly better than those without antiviral treatment after curative therapy, including operation or radiofrequency ablation (RFA). For patients with TACE or targeted therapy, the OS in the antiviral group was better than that in the nonantiviral group as well.3,7,9,32 As an alternative treatment for advanced HCC, HAIC can directly and continuously deliver chemotherapeutic drugs into the tumor-feeding artery, which can increase the local drug concentrations, enhance the antitumor effect and decrease the systemic toxicity.10,14 Similarly, antiviral treatment could improve the OS in HBV-related HCC treated with FOLFOX-HAIC compared with nonantiviral treatment.15 Due to ETV and TDF’s similarly higher antiviral efficacy and higher barrier to resistance than other antiviral drugs, they are equally chosen as first-line antiviral treatment for CHB in guidelines.16,17,29,33,34
HBV reactivation is a common complication in patients who undergo antitumor treatment, which may lead to antitumor treatment delays or discontinuation.35–38 Among CHB patients with solid tumors without receiving antiviral treatment, the risk of HBV reactivation due to antitumor therapy was 25%.35 Antiviral treatment can significantly reduce the occurrence of HBV reactivation after the treatment of the malignancy.8 In the present study, the rate of HBV reactivation in patients with HAIC was 9.7%. The potential mechanism of HBV reactivation due to HAIC is unclear. Unlike systemic chemotherapy, which may directly cause immunosuppression, or surgery, which may induce metabolic and endocrine responses and result in an immunosuppressive status, HAIC theoretically has little systemic effect on the host immune system because of its high local drug concentration.29 However, similar to TACE, HAIC may suppress the host immune system through an arteriovenous shunt or peritumoral microcirculation, which results in HBV reactivation.15,36,39 Several previous studies showed that patients in the TDF group had a higher virologic response rate and shorter serum HBV DNA clearance time after surgery and RFA.19,20 In our study, we found that patients, especially those treated with ≥ 4 cycles of FOLFOX-HAIC, in the TDF group had a lower HBV reactivation rate than those in the ETV group, which suggested that TDF might have a better antiviral effect.
HBV reactivation is notably relevant to an increased risk of deterioration of liver function, the manifestations of which range from an asymptomatic elevation in transaminase levels to severe hepatitis, liver failure or even liver-related death.8,40 Patients with advanced HCC need to be treated with HAIC multiple times. Wang et al41 reported that liver function changes in patients were positively correlated with the number of FOLFOX-HAIC cycles. Moreover, our study found that the cycles of FOLFOX-HAIC were an independent risk factor for OS for patients treated with HAIC, so it was more important to protect liver function during HAIC. Antiviral treatment can inhibit HBV replication, improve liver function, and contribute to patients more tolerant of treatments for HCC.29 In previous studies, liver function in the TDF group was better than that in the ETV group after surgery and RFA.19,20 In our study, we used ALBI grade, which is known as a simple, effective method of assessing liver function and predicting the survival in HCC, to evaluate liver function.24,42 Similarly, in our study, the rates of ALBI grade that remained stable or improved in the TDF group of all patients and patients with ≥ 4 cycles of FOLFOX-HAIC were both higher than those in the ETV group. TDF could lead to better liver function preservation. More biomarkers such as alkaline phosphatase (ALP) and AST-Lym-R (ALR) score were also showed good performance in assessing liver function and prognosis of patients.43,44 Further research is needed to perform.
For the long-term effect, whether ETV or TDF has a better prognosis remains controversial. Choi et al18 and Shen et al45 reported that the TDF group had significantly better OS and RFS than the ETV group after surgery, while Hu et al20 and Lee et al21 failed to find a difference between the two groups. In our study, the OS and PFS in the TDF group were better than those in the ETV group of patients treated with FOLFOX-HAIC, especially with ≥ 4 cycles of FOLFOX-HAIC. Considering that sustained HBV replication would impair tumor immune surveillance, exert adverse effects on the liver microenvironment, and result in carcinogenesis in the liver, all of which may enhance tumor progression, superior virologic outcomes would lead to better prognosis.4,5,7 Moreover, improvement in liver function can enhance the tolerance of patients to receive further antitumor treatment.3,4 The lower HBV reactivation rate and better liver function preservation in the TDF group of patients with FOLFOX-HAIC, especially with ≥ 4 cycles of FOLFOX-HAIC, both contributed to the better prognosis.
Our study has some limitations. First, our study was a single-center retrospective study, which carries a risk of selection bias even after PSM. A randomized controlled trial is needed to provide more convincing conclusions. Second, our study included patients receiving targeted therapy or immunotherapy, which may result in HBV reactivation and liver function deterioration and influence the prognosis. To minimize this limitation, PSM was performed. Last, because of the late approval of TDF in China, the follow-up periods between the two groups were different. Further studies are needed.
Conclusion
In conclusion, TDF was associated with better overall survival, better progression-free survival, a lower proportion of HBV reactivation, and better preservation of liver function in advanced HBV-HCC patients treated with FOLFOX-HAIC, especially with ≥ 4 cycles FOLFOX-HAIC, compared to ETV.
Data Sharing Statement
All data generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was conducted according to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the ethics committee of Sun Yat-sen University Cancer Center (Protocol code: B2022-238-01). The study used retrospective data that were obtained after each patient agreed to treatment and all patients provided informed consent to review their medical data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; drafted, revised or critically reviewed the article; agreed on the journal to which the article will be submitted; gave final approval of the version to be published; agreed to take responsibility and be accountable for the contents of the article.
Funding
This work was supported by the Sun Yat-sen University Cancer Center physician scientist funding (No. 16zxqk04), Wu Jieping Medical Foundation-special fund for tumor immunity (320.6705.2021-02-76), Bethune Fund-Advanced solid tumor project (STLKY2-041), Guangdong Basic and Applied Basic Research Foundation (2022A1515110961), Guangzhou Science and Technology Plan Project (2023A04J2125), and National Natural Science Foundation of China (82303893).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Péneau C, Imbeaud S, La Bella T, et al. Hepatitis B virus integrations promote local and distant oncogenic driver alterations in hepatocellular carcinoma. Gut. 2022;71(3):616–626. doi:10.1136/gutjnl-2020-323153
3. Xu L, Gao H, Huang J, et al. Antiviral therapy in the improvement of survival of patients with hepatitis B virus-related hepatocellular carcinoma treated with sorafenib. J Gastroenterol Hepatol. 2015;30(6):1032–1039. doi:10.1111/jgh.12910
4. Huang G, Lau WY, Wang ZG, et al. Antiviral therapy improves postoperative survival in patients with hepatocellular carcinoma: a randomized controlled trial. Ann Surg. 2015;261(1):56–66. doi:10.1097/SLA.0000000000000858
5. Huang G, Li PP, Lau WY, et al. Antiviral therapy reduces hepatocellular carcinoma recurrence in patients with low HBV-DNA levels: a randomized controlled trial. Ann Surg. 2018;268(6):943–954. doi:10.1097/SLA.0000000000002727
6. Huang S, Xia Y, Lei Z, et al. Antiviral therapy inhibits viral reactivation and improves survival after repeat hepatectomy for hepatitis b virus-related recurrent hepatocellular carcinoma. J Am Coll Surg. 2017;224(3):283–293 e4. doi:10.1016/j.jamcollsurg.2016.11.009
7. Jang JW, Yoo SH, Nam HC, et al. Association of prophylactic anti-hepatitis B virus therapy with improved long-term survival in patients with hepatocellular carcinoma undergoing transarterial therapy. Clin Infect Dis. 2020;71(3):546–555. doi:10.1093/cid/ciz860
8. Lao XM, Luo G, Ye LT, et al. Effects of antiviral therapy on hepatitis B virus reactivation and liver function after resection or chemoembolization for hepatocellular carcinoma. Liver Int Apr. 2013;33(4):595–604. doi:10.1111/liv.12112
9. Lee IC, Lee PC, Chao Y, et al. Application and impact of antiviral therapy for patients with HBV-related hepatocellular carcinoma receiving sorafenib and lenvatinib treatment. Viruses. 2022;14(11):2355. doi:10.3390/v14112355
10. Lyu N, Wang X, Li JB, et al. Arterial chemotherapy of oxaliplatin plus fluorouracil versus sorafenib in advanced hepatocellular carcinoma: a biomolecular exploratory, randomized, phase III Trial (FOHAIC-1). J Clin Oncol. 2022;40(5):468–480. doi:10.1200/JCO.21.01963
11. Li QJ, He MK, Chen HW, et al. Hepatic arterial infusion of oxaliplatin, fluorouracil, and leucovorin versus transarterial chemoembolization for large hepatocellular carcinoma: a randomized phase III trial. J Clin Oncol. 2022;40(2):150–160. doi:10.1200/JCO.21.00608
12. He M, Li Q, Zou R, et al. sorafenib plus hepatic arterial infusion of oxaliplatin, fluorouracil, and leucovorin vs sorafenib alone for hepatocellular carcinoma with portal vein invasion: a randomized clinical trial. JAMA Oncol. 2019;5(7):953–960. doi:10.1001/jamaoncol.2019.0250
13. Mei J, Tang YH, Wei W, et al. Hepatic arterial infusion chemotherapy combined With PD-1 Inhibitors plus lenvatinib versus PD-1 inhibitors plus lenvatinib for advanced hepatocellular carcinoma. Front Oncol. 2021;11:618206. doi:10.3389/fonc.2021.618206
14. Lyu N, Kong Y, Mu L, et al. Hepatic arterial infusion of oxaliplatin plus fluorouracil/leucovorin vs. sorafenib for advanced hepatocellular carcinoma. J Hepatol. 2018;69(1):60–69. doi:10.1016/j.jhep.2018.02.008
15. Liu S, Lai J, Lyu N, et al. Effects of antiviral therapy on HBV reactivation and survival in hepatocellular carcinoma patients undergoing hepatic artery infusion chemotherapy. Front Oncol. 2021;2021:10.
16. Lampertico P, Agarwal K, Berg T; European Association for the Study of the Liver. Electronic address eee, European association for the study of the L. EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67(2):370–398. doi:10.1016/j.jhep.2017.03.021
17. Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology Apr. 2018;67(4):1560–1599. doi:10.1002/hep.29800
18. Choi J, Jo C, Lim YS. Tenofovir versus entecavir on recurrence of hepatitis B virus-related hepatocellular carcinoma after surgical resection. Hepatology. 2021;73(2):661–673. doi:10.1002/hep.31289
19. Wang XH, Hu ZL, Fu YZ, et al. Tenofovir vs. entecavir on prognosis of hepatitis B virus-related hepatocellular carcinoma after curative resection. J Gastroenterol. 2022;57(3):185–198. doi:10.1007/s00535-022-01855-x
20. Hu Z, Zeng H, Hou J, et al. Tenofovir vs. entecavir on outcomes of hepatitis B virus-related hepatocellular carcinoma after radiofrequency ablation. Viruses. 2022;14(4):656. doi:10.3390/v14040656
21. Lee JH, Kim BK, Park SY, et al. The efficacies of entecavir and tenofovir in terms of enhancing prognosis after curative treatment of hepatitis B virus-related hepatocellular carcinoma. Eur J Intern Med. 2021;89:48–55. doi:10.1016/j.ejim.2021.02.019
22. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
23. Lyu N, Lin Y, Kong Y, et al. FOXAI: a phase II trial evaluating the efficacy and safety of hepatic arterial infusion of oxaliplatin plus fluorouracil/leucovorin for advanced hepatocellular carcinoma. Gut. 2018;67(2):395–396. doi:10.1136/gutjnl-2017-314138
24. Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-The ALBI grade. J Clin Oncol. 2015;33(6):550–558. doi:10.1200/JCO.2014.57.9151
25. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399–424. doi:10.1080/00273171.2011.568786
26. Rassen JA, Shelat AA, Myers J, et al. One-to-many propensity score matching in cohort studies. Pharmacoepidemiol Drug Saf. 2012;21(S2):69–80. doi:10.1002/pds.3263
27. Li H, Wu Z, Chen J, et al. External radiotherapy combined with sorafenib has better efficacy in unresectable hepatocellular carcinoma: a systematic review and meta-analysis. Clin Exp Med. 2022;23(5):1537–1549. doi:10.1007/s10238-022-00972-4
28. Li H, Su K, Guo L, et al. PD-1 inhibitors combined with antiangiogenic therapy with or without transarterial chemoembolization in the treatment of hepatocellular carcinoma: a propensity matching analysis. J Hepatocell Carcinoma. 2023;10:1257–1266. doi:10.2147/JHC.S415843
29. Zhang YQ. Antiviral therapies for hepatitis B virus-related hepatocellular carcinoma. World J Gastroenterol Apr. 2015;21(13):3860–3866. doi:10.3748/wjg.v21.i13.3860
30. Hwang JP, Feld JJ, Hammond SP, et al. Hepatitis B virus screening and management for patients with cancer prior to therapy: ASCO provisional clinical opinion update. J Clin Oncol. 2020;38(31):3698–3715. doi:10.1200/JCO.20.01757
31. Sohn W, Kang TW, Choi S-K, et al. Effect of oral antiviral treatment on long-term outcomes of radiofrequency ablation therapy for hepatitis B virus-related hepatocellular carcinoma. Oncotarget. 2016;7(30):47794–47807. doi:10.18632/oncotarget.10026
32. Zhou ZG, Zheng XR, Zhou Q, et al. Impact of oral anti-hepatitis B therapy on the survival of patients with hepatocellular carcinoma initially treated with chemoembolization. Chin J Cancer. 2015;34(5):205–216. doi:10.1186/s40880-015-0017-7
33. Cho H, Ahn H, Lee DH, et al. Entecavir and tenofovir reduce hepatitis B virus-related hepatocellular carcinoma recurrence more effectively than other antivirals. J Viral Hepat. 2018;25(6):707–717. doi:10.1111/jvh.12855
34. Reddy KR, Beavers KL, Hammond SP, Lim JK, Falck-Ytter YT. American Gastroenterological Association Institute guideline on the prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy. Gastroenterology. 2015;148(1):215–219. doi:10.1053/j.gastro.2014.10.039
35. Mustafayev K, Torres H. Hepatitis B virus and hepatitis C virus reactivation in cancer patients receiving novel anticancer therapies. Clin Microbiol Infect. 2022;28(10):1321–1327. doi:10.1016/j.cmi.2022.02.042
36. Jang JW. Hepatitis B virus reactivation in patients with hepatocellular carcinoma undergoing anti-cancer therapy. World J Gastroenterol. 2014;20(24):7675. doi:10.3748/wjg.v20.i24.7675
37. Voican CS, Mir O, Loulergue P, et al. Hepatitis B virus reactivation in patients with solid tumors receiving systemic anticancer treatment. Ann Oncol. 2016;27(12):2172–2184. doi:10.1093/annonc/mdw414
38. Kim HY, Yoo JJ, Oh S, et al. Scoring system for risk stratification of viral reactivation during prophylactic antiviral treatment in Korean patients with hepatitis B undergoing anticancer chemotherapy: a multicenter study. J Med Virol. 2018;90(10):1593–1603. doi:10.1002/jmv.25241
39. Papatheodoridi M, Tampaki M, Lok AS, Papatheodoridis GV. Risk of HBV reactivation during therapies for HCC: a systematic review. Hepatology. 2022;75(5):1257–1274. doi:10.1002/hep.32241
40. Shi Y, Zheng M. Hepatitis B virus persistence and reactivation. BMJ. 2020;370:m2200.
41. Wang J, Zheng Z, Wu T, et al. Hepatic arterial infusion chemotherapy as a timing strategy for conversion surgery to treat hepatocellular carcinoma: a single-center real-world study. J Hepatocell Carcinoma. 2022;9:999–1010. doi:10.2147/JHC.S379326
42. Su K, Shen Q, Tong J, et al. Construction and validation of a nomogram for HBV-related hepatocellular carcinoma: a large, multicenter study. Ann. Hepatol. 2023;28(4):101–109. doi:10.1016/j.aohep.2023
43. Su K, Huang W, Li X, et al. Evaluation of lactate dehydrogenase and alkaline phosphatase as predictive biomarkers in the prognosis of hepatocellular carcinoma and development of a new nomogram. J Hepatocell Carcinoma. 2023;10:69–79. doi:10.2147/JHC.S398632
44. Li H, Guo L, Su K, et al. Construction and validation of TACE therapeutic efficacy by ALR score and nomogram: a large, multicenter study. J Hepatocell Carcinoma. 2023;10:1009–1017. doi:10.2147/JHC.S414926
45. Shen J, Qi W, Dai J, et al. Tenofovir vs. entecavir on recurrence of hepatitis B virus-related hepatocellular carcinoma beyond Milan criteria after hepatectomy. Chin Med J. 2021;135(3):301–308. doi:10.1097/CM9.0000000000001864
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.