Back to Journals » Drug Design, Development and Therapy » Volume 19
Targeting CD20 in Primary Membranous Nephropathy Serologically and Histologically Negative for PLA2R: Is Obinutuzumab Superior to Rituximab?
Authors Cao H, Feng Y, Li X, Ke B ![]() , Gong L
, Gong L
Received 14 August 2025
Accepted for publication 25 October 2025
Published 7 November 2025 Volume 2025:19 Pages 9983—9992
DOI https://doi.org/10.2147/DDDT.S560746
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Solomon Tadesse Zeleke
Huiling Cao,1,* Yumei Feng,2,* Xueting Li,1 Ben Ke,1 Limin Gong3
1Department of Nephrology, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, 330006, People’s Republic of China; 2Department of Emergency, Pingxiang People’s Hospital, Pingxiang, Jiangxi, 337055, People’s Republic of China; 3Department of General Medicine, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, 330006, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ben Ke, Department of Nephrology, The Second Affiliated Hospital of Nanchang University, No. 1 Minde Road, Nanchang, Jiangxi, 330006, People’s Republic of China, Tel +8615270882765, Email [email protected] Limin Gong, Department of General Medicine, The Second Affiliated Hospital of Nanchang University, No. 1 Minde Road, Nanchang, Jiangxi, 330006, People’s Republic of China, Tel +8613907099310, Email [email protected]
Background: Anti-CD20 monoclonal antibody has become the first-line treatment option for primary membranous nephropathy (PMN), regardless of PLA2R status. Obinutuzumab (OBZ), a humanized anti-CD20 monoclonal antibody, has shown higher remission rates with an acceptable safety profile over rituximab (RTX), whether in the initial treatment or refractory PLA2R-associated membranous nephropathy. However, the efficacy evaluation of the OBZ and RTX in PLA2R-negative PMN has not been reported yet.
Methods: 39 patients with PMN who were negative for serum anti-PLA2R antibodies and showed negative PLA2R staining in renal biopsy were retrospectively included in this study, with 18 receiving OBZ and 21 receiving RTX. All patients received a 12-month follow-up. The primary outcome was the rate of patients achieving complete or partial remission (CR or PR) at 12 months. Secondary outcomes included changes in laboratory parameters, relapse, and adverse events.
Results: At 12 months, CR or PR was achieved in 17 of 18 (94.4%) patients in the OBZ group and 18 of 21 (85.7%) patients in the RTX group, with the difference between the two groups not being statistically significant (OR=2.83, 95% CI: 0.27– 29.96; p=0.61). Kaplan-Meier analyses showed that the cumulative CR or PR rates were not significantly different (Log-Rank p=0.68). Adverse events occurred in 4 cases (22.2%) in the OBZ group and 6 cases (28.6%) in the RTX group. During the 12-momth follow-up, no relapse was observed in the OBZ group, whereas post remission relapse occurred in 2 (9.5%) of 21 patients in the RTX group (p=0.49).
Conclusion: In patients with PLA2R-negative PMN, OBZ demonstrated similar efficacy to RTX, and both had a favorable safety profile.
Keywords: primary membranous nephropathy, rituximab, obinutuzumab, M-type phospholipase A2 receptor, anti-CD20 monoclonal antibody
Introduction
Primary membranous nephropathy (PMN) ranks as the second leading cause of nephrotic syndrome (NS) in adults, following diabetic nephropathy.1,2 Approximately 70% of patients with PMN have autoantibodies against the phospholipase A2 receptor (PLA2R) in their circulating.3 Over the past decade, researchers have also identified other target antigens present in the remaining patients.4 With the key pathogenic role of PLA2R in PMN gradually clarified, B-cell depletion therapy seems to be gradually replacing the traditional approaches due to its good safety profile.5 It is worth noting that, currently, B-cell depletion therapy, namely anti-CD20 monoclonal antibodies, is mainly used in PMN patients with PLA2R-positive,6–8 although the KIDGO guidelines recommend that anti-CD20 monoclonal antibodies can be used in PMN patients, regardless of PLA2R status.9 However, evidence regarding the efficacy of these therapies for PLA2R-negative PMN remains scarce. Therefore, the efficacy of anti-CD20 monoclonal antibodies in PMN patients with PLA2R-negative merits further investigation.
Anti-CD20 monoclonal antibodies mainly include murine-derived antibodies, such as rituximab (RTX), and human-derived antibody, such as obinutuzumab (OBZ). It’s known that RTX has been recommended as a first-line therapy option for PMN patients at intermediate to high risk.9 OBZ, a humanized type II anti-CD20 monoclonal antibody (mAb), exhibits stronger antibody-dependent cellular cytotoxicity (ADCC) but lower complement-dependent cytotoxicity (CDC) than RTX, resulting in more efficient B-cell clearance.10 In recent years, several studies have reported that OBZ induces higher remission rates and longer-lasting immunological responses in PMN patients with PLA2R-positive or negative, especially in patients with refractory PMN who had a poor response to RTX.11–14 However, it remains unknown whether the efficacy of OBZ is superior to that of RTX in PMN patients with PLA2R-negative.
Therefore, the aim of this study was to evaluate the therapeutic efficacy and safety of both drugs in this population.
Methods
Study Design and Participants
This retrospective cohort study enrolled consecutive patients diagnosed with membranous nephropathy at the Nephrology Department of the Second Affiliated Hospital of Nanchang University between September 2021 and March 2024. The inclusion criteria included: (i) age ≥18 years; (ii) newly diagnosed PMN confirmed by renal biopsy; (iii) a negative baseline serum anti-PLA2R antibody level and absence of PLA2R deposition in glomeruli by immunofluorescence; (iv) clinical manifestation of NS, defined as proteinuria >3.5 g/d, serum albumin <30 g/l and required an estimated glomerular filtration rate (eGFR) >30 mL/min/1.73m2; (v) receiving RTX or OBZ and completing at least 12 months of follow-up. Patients who had received corticosteroids or immunosuppressive therapy within 6 months prior to initiating RTX or OBZ, as well as those with secondary MN due to autoimmune diseases, malignancies, viral hepatitis, or HIV infection, were excluded from this study. The study protocol was approved by the Ethics Committee of the Second Affiliated Hospital of Nanchang University (approval no.: No. EFY20221011), and all included patients signed a written informed consent.
Clinical Data
Patient demographic and clinical information was obtained through the electronic medical record. Baseline data were defined as the assessed value of the patient’s first hospitalized for treatment with OBZ or RTX. Follow-up time was recorded from baseline for all patients, and proteinuria, serum creatinine, eGFR, serum albumin, and treatment-related adverse events were systematically recorded at 3, 6, and 12 months, respectively. eGFR was calculated according to the CKD-EPI formula.15 Serum anti-PLA2R antibody levels were measured by the EUROIMMUN ELISA, and results <14 RU/mL were considered negative.1,16 Glomerular PLA2R deposition was assessed by immunofluorescence as previously described.17,18 The staining intensity was semi-quantitatively scored as follows: 0, negative; 0.5, very weak; 1, weak; 2, moderate; 3, strong.
Treatment Protocols
Participants were treated with RTX or OBZ. The RTX regimen consisted of 375 mg/m2 intravenously weekly for 4 doses or 1 g intravenously every 2 weeks for 2 doses. RTX was reintroduced for those who did not achieve significant resolution of proteinuria (ie, proteinuria persisted at >3.5 g/d or decreased by less than 50% from baseline) within 6 months of the initial reintroduction of the drug, or who experienced a relapse. Thirty minutes prior to the RTX infusion, 5 mg of intravenous dexamethasone and 50 mg of intramuscular diphenhydramine were administered as premedication. The OBZ regimen was 1 g intravenously every 2 weeks for 2 doses. Thirty minutes prior to the infusion of OBZ, an intravenous administration of 80 mg of methylprednisolone, an oral dose of 10 mg of ebastine, and 600 mg of oral acetaminophen were administered as premedication. All patients received concomitant conventional supportive therapy, including renin-angiotensin-aldosterone system (RAAS) inhibitors, diuretics, and lipid-lowering medications, as determined by the treating physician on a clinical basis.
Study Outcomes and Definitions
The primary outcome was the proportion of patients achieving complete or partial remissions (CR or PR) at 12 months. Secondary outcomes included changes in laboratory parameters, relapse rate, and occurrence of treatment-related adverse events. CR was defined as proteinuria <0.3 g/d while maintaining stable renal function. PR was characterized by a reduction in proteinuria of at least 50% from baseline levels to a level between 0.3 and 3.5 g/d, accompanied by stable renal function. Relapse was defined as a renewed and sustained increase in proteinuria exceeding 3.5 g/d following the achievement of CR or PR. Primary refractoriness was defined as the failure to achieve at least a PR by the end of the 12-month observation period. A decline in renal function was indicated by a ≥50% decrease in eGFR from baseline or progression to ESRD, which is marked by persistently low eGFR (<15 mL/min/1.73 m2) or the initiation of long-term dialysis.
Statistical Analysis
For continuous variables following a normal distribution, data were presented as mean ± standard deviation (SD), with group comparisons performed using the independent samples t-test. Variables not conforming to normality were reported as median with interquartile range (IQR, 25th-75th percentiles) and analyzed via the Mann–Whitney U-test. Categorical variables were summarized as counts and percentages, with Fisher’s exact test employed for between-group analysis. Kaplan-Meier cures were applied to evaluate cumulative remission, and group differences were assessed using the Log rank test. In addition, multifactorial logistic regression models unadjusted as well as adjusted for age, serum albumin, and eGFR were constructed to assess independent associations between treatment regimens and remission outcomes.
All statistical analyses were done using SPSS software (version 26.0; IBM Corp., Armonk, NY, USA). Data visualization was carried out with GraphPad Prism (version 10.1.2) and R software (version 4.4.3). A two-sided p-value of <0.05 was regarded as indicative of statistical significance.
Results
Baseline Characteristics
This study enrolled 39 patients diagnosed with PMN based on renal biopsy, all of whom tested negative for serum anti-PLA2R antibody at baseline. Among them, 18 patients were treated with OBZ, while the remaining 21 received RTX (Figure 1). The overall cohort had a median (IQR) age of 52 years (44–63), and 31 individuals (79.5%) were male. The mean (SD) of serum albumin and eGFR of the overall cohort were 25.1±3.5 g/l and 90.8±24.8 mL/min/1.73m2, respectively. The median (IQR) of proteinuria and serum creatinine were 7.7 g/d (5.6–12.3) and 80.6 μmol/l (71.1–92.8), respectively. No significant differences were observed between the two groups regarding age, gender, and baseline clinical parameters, including serum creatinine, proteinuria, eGFR, serum albumin and blood pressure (P>0.05) (Table 1).
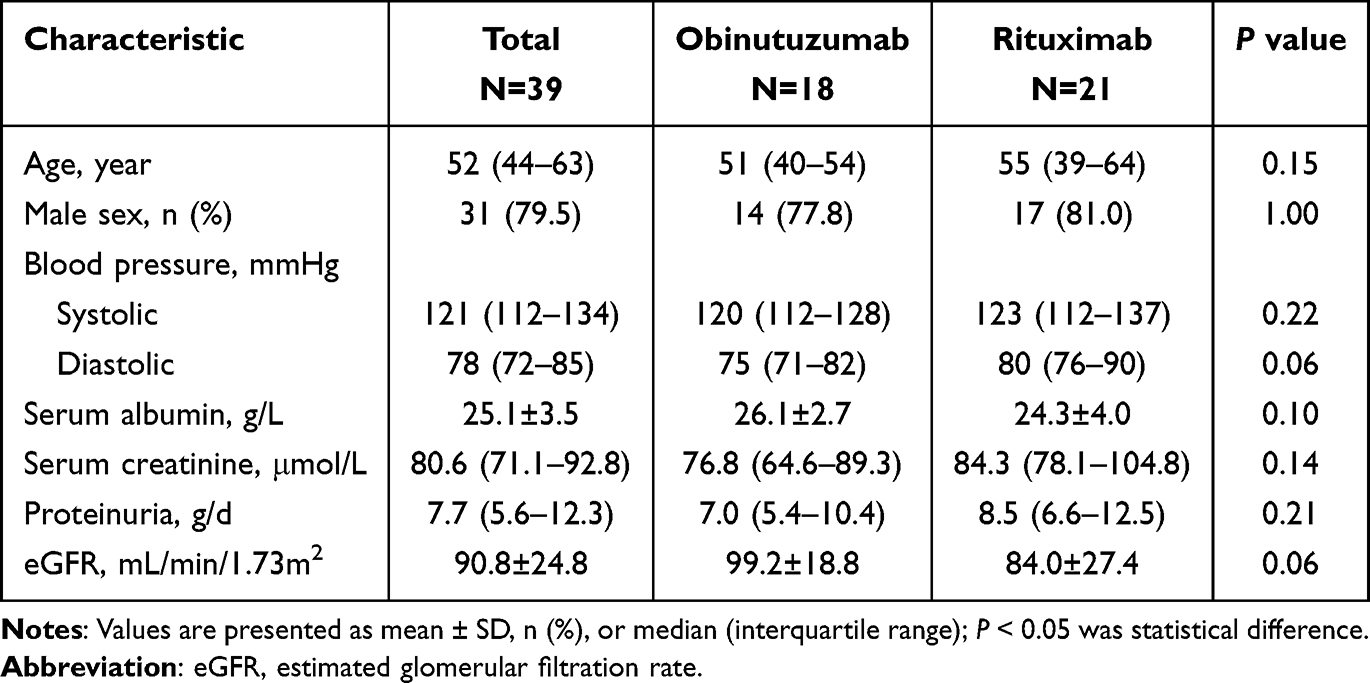 |
Table 1 Baseline Characteristics of Patients in the Obinutuzumab and Rituximab Groups |
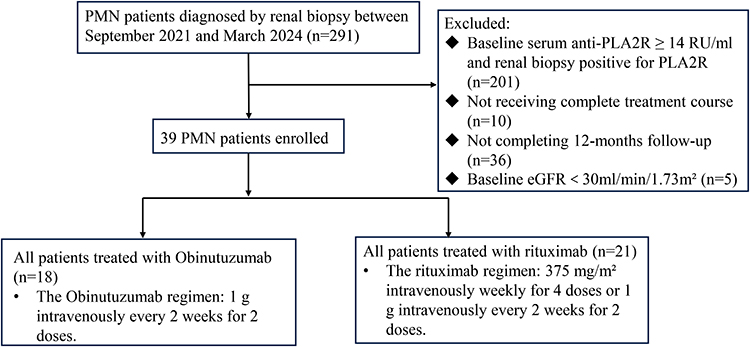 |
Figure 1 Patient selection flowchart. Abbreviations: PMN, primary membranous nephropathy; Anti-PLA2R, anti-M-type phospholipase A2 receptor; eGFR, estimated glomerular filtration rate. |
Primary Outcome
At 12 months, 17 out of 18 patients (94.4%) in the OBZ group and 18 out of 21 patients (85.7%) in the RTX group achieved CR or PR (OR=2.83, 95% CI: 0.27–29.96; p=0.61) (Table 2). Kaplan-Meier analysis showed that the cumulative CR or PR rate was higher in the OBZ group than in the RTX group from month 6 post-treatment. However, the Log rank test showed no significant difference between groups (p=0.68) (Figure 2A).
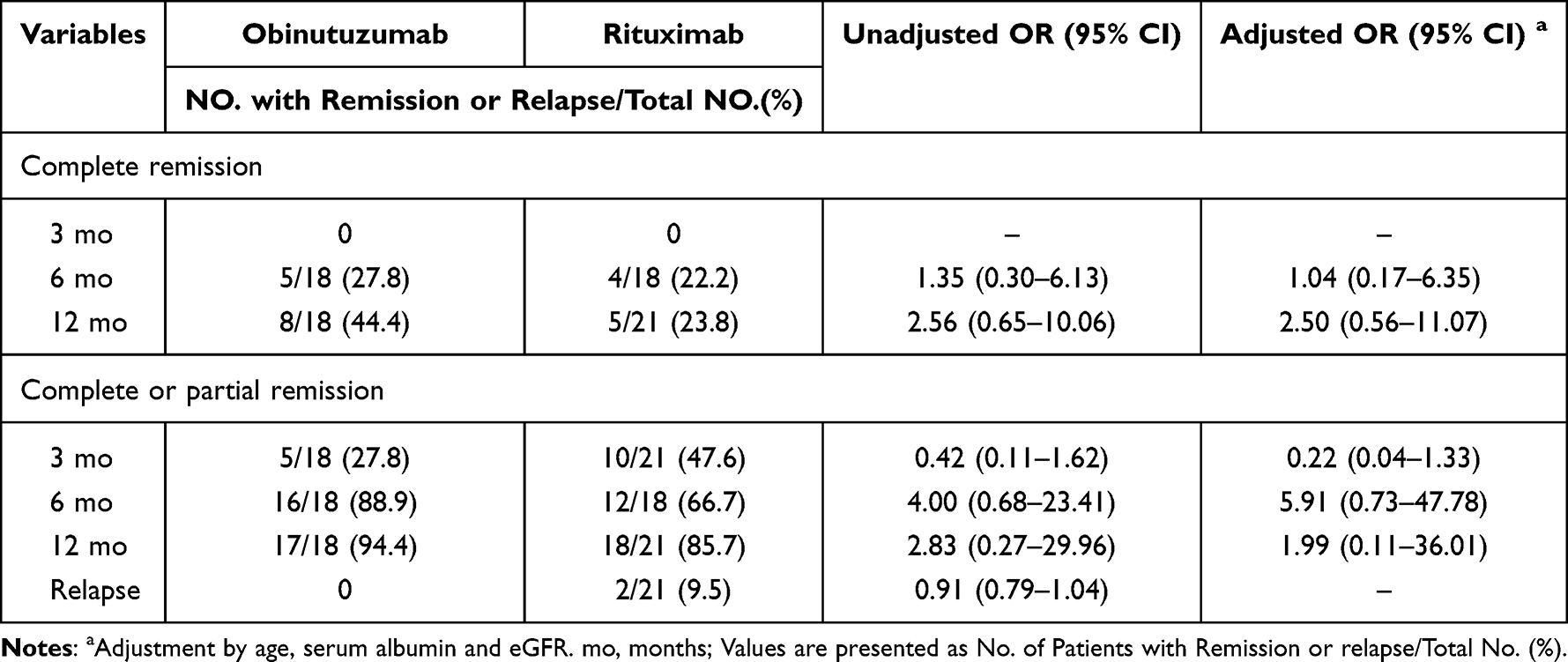 |
Table 2 Complete Remission, Composite Remission and Relapse at 3–12 months in Patients in the Obinutuzumab and Rituximab Groups |
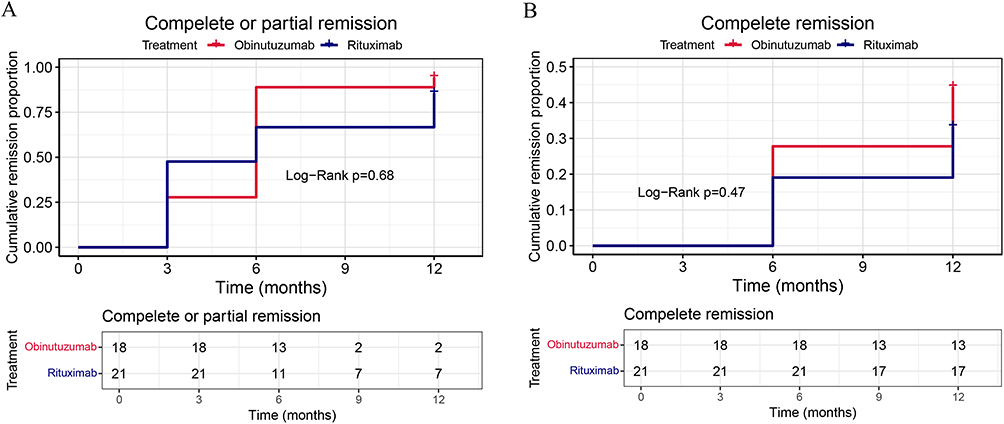 |
Figure 2 (A) Kaplan-Meier analysis of complete or partial remission in the rituximab and obinutuzumab groups. (B) Kaplan-Meier analysis of complete remission in the rituximab and obinutuzumab groups. |
The CR rates at 12 months were 44.4% and 23.8% in the OBZ and RTX groups, respectively (OR=2.56, 95% CI: 0.65–10.06; p=0.20) (Table 2). Kaplan–Meier analysis further indicated no significant difference in the cumulative CR rate between the groups (log-rank p = 0.47) (Figure 2B).
Given the known effects of age, serum albumin, and eGFR on PMN disease severity and treatment outcomes, as well as their tendency to show relatively strong associations in univariate logistic analyses (Figure S1), the study incorporated these three variables into a multifactorial logistic regression model to further control for possible confounders. Multifactorial logistic regression adjusting for the aforementioned variables showed no significant difference at the 12-month follow-up CR or PR rates between the OBZ and RTX groups (adjusted OR = 1.99, 95% CI: 0.11–36.01) (Table 2).
Secondary Outcome
Proteinuria levels decreased from 7.0 g/d (5.4–10.4) at baseline to 0.3 g/d (0.3–0.7) at 12 months in the OBZ group, and from 8.5 g/d (6.6–12.5) at baseline to 0.6 g/d (0.2–2.3) at 12 months in the RTX group (p = 0.23) (Figure 3A) (Table S1). Although serum albumin levels increased in both groups at 12-month follow-up, the difference between the two groups did not reach statistical significance (p = 0.22) (Figure 3B) (Table S1). Furthermore, not significant differences were observed between the two groups regarding the changes in eGFR and serum creatinine (p = 0.27 and p = 1.00, respectively) (Figure 3C and D) (Table S1).
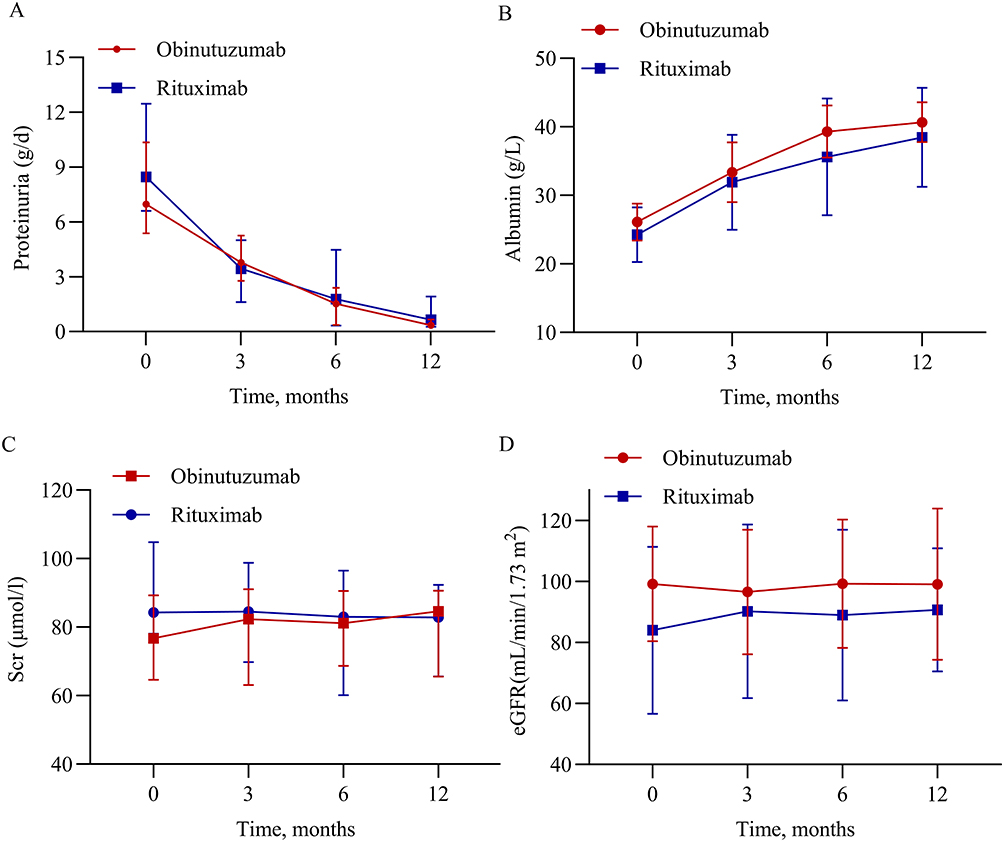 |
Figure 3 Changes in clinical indicators during follow-up in patients in the rituximab and obinutuzumab groups. (A) Proteinuria, expressed as median (interquartile range). (B) Serum albumin, expressed as mean ± SD. (C) Scr, expressed as median (interquartile range). (D) eGFR, expressed as mean ± SD. Abbreviations: Scr, serum creatinine; eGFR, estimated glomerular filtration rate; SD, standard deviation. |
Throughout the follow-up period, no patients in either group experienced progressive decline in renal function or progression to ESRD. No relapse occurred in the OBZ group, whereas 2 patients (9.5%) in the RTX group experienced relapse after achieving remission (OR = 0.91, 95% CI: 0.79–1.04; p = 0.49) (Table 2). Both patients regained remission after re-treatment with RTX.
Adverse Events
Adverse events were reported in 6 (29%) patients in the RTX group and 4 (22%) patients in the OBZ group (p=0.73) (Table 3). Infections occurred in 4 (19%) patients receiving RTX and 3 (17%) patients treated with OBZ, all of which were mild to moderate pulmonary or urinary tract infections. All cases improved following standard outpatient antimicrobial therapy. Drug infusion reactions occurred in 1 case (5.6%) in the OBZ and 2 cases (9.5%) in the RTX group, and were resolved by slowing the infusion rate and treatment with dexamethasone. In addition, 1 patient in the RTX group developed mild liver enzyme elevations, which were considered to be related to the combined use of atorvastatin, and liver function returned to normal after discontinuation of the drug. No malignant neoplasms, serious cardiovascular events, or deaths were observed in any of the patients throughout the follow-up period.
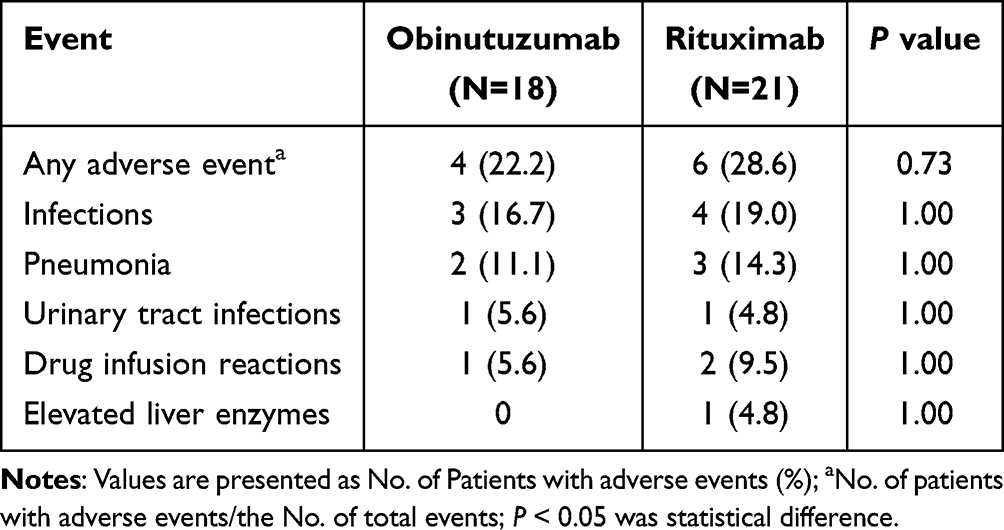 |
Table 3 Adverse Events Occurring in the Obinutuzumab and Rituximab Groups |
Discussion
B cells are considered to be key immune mediators in the pathogenesis of PMN.19 Anti-CD20 mAbs targeting B cells have become an important therapeutic option for PMN, and related therapeutic strategies are being optimized. It has been shown that OBZ is superior to RTX in inducing longer-lasting and more complete B-cell depletion in PMN patients with PLA2R-positive or negative.20 This study focused on PLA2R-negative PMN patients and represents the first systematic comparison of the efficacy and safety of OBZ and RTX in this population. The results showed that the two treatment regimens were comparable in terms of efficacy in inducing CR or PR within 12 months (OBZ vs RTX: 94.4% vs 85.7%, OR=2.83, 95% CI: 0.27–29.96, p=0.61), with both treatments demonstrating good tolerability, suggesting that for PMN patients with PLA2R-negative who do not respond well to RTX treatment, it might not be necessary to switch to OBZ.
RTX, a chimeric murine/human anti-CD20 mAb, contains murine sequences in its variable region, which is prone to induce the production of anti-drug antibodies (ADAs) and subsequently reduce its clinical efficacy.21 Studies have shown that approximately 23–43% of patients develop ADAs after receiving RTX, of which about 80% possess neutralizing activity.22–24 This significantly impairs RTX-mediated CDC and ADCC, leading to rapid B-cell reconstitution, increased disease relapse rates and diminished therapeutic responses. In contrast, OBZ is a humanized type II anti-CD20 mAb with enhanced affinity for the FcγRIIIa receptor after glycosylation of the Fc region, resulting in increased ADCC activity and lower immunogenicity, leading to longer-lasting B-cell clearance and a lower risk of ADAs.10,25
Hu et al11 conducted a retrospective study in an overall PMN population and found that OBZ resulted in a significantly higher clinical remission rate than RTX at 12 months, achieved a higher rate of immune remission in the PLA2R-positive subgroup, and sustained CD19+ B-cell depletion for a longer duration. Consistently, Xue et al also found that OBZ is effective as an initial treatment for PLA2R-associated PMN.14 Furthermore, OBZ showed good salvage therapy potential in patients with refractory PMN who were unresponsive to or relapsed after RTX treatment.12,26 Thus, OBZ may represent an attractive alternative therapy in RTX-refractory patients or in initial treatment of PMN. However, our study did not observe superior clinical efficacy of OBZ in PLA2R-negative PMN patients. We speculate that this discrepancy may be related to the inherent differences in the B-cell clearance mechanisms of the two drugs, as well as the different immune backgrounds of the study populations.
PLA2R and thrombospondin domain-containing 7A (THSD7A) are the most common PMN target antigens known, present in 70% and 1–5% of patients, respectively.3,27 In recent years, several novel target antigens have been discovered in PLA2R-negative PMN, including neural epidermal growth factor-like 1 protein (NELL-1),28 semaphorin 3B (Sema3B),29 and exotosin 1 and 2 (EXT1/2).30 These novel antigen-associated antibodies are mostly IgG1-based and are more likely to activate the classical complement pathway than PLA2R-associated IgG4.31 Moreover, PMN may not be limited to localized glomerular lesions, and the newly proposed immune-inflammatory-MGN triplets hypothesis suggests a broader systemic immune activation involving chemokines, the JAK-STAT pathway, and both T-cell and B-cell signaling networks.32 These findings indicate that PLA2R-negative PMN may be driven by distinct immunopathogenic mechanisms compared to PLA2R-positive disease. Within such an immune context, even the pharmacodynamically superior agent like OBZ, with its intensive B-cell depletion strategy, may not necessarily provide additional clinical benefits. However, this hypothesis still requires further validation through larger cohort studies and mechanistic investigations.
In terms of safety, no serious adverse events were observed in this study. The incidence of adverse events was lower in the OBZ group than in the RTX group, but the difference was not statistically significant. The most common adverse events in both groups were infusion reactions and infections, both of which resolved with symptomatic treatment. This is consistent with the observations in the study by Hu et al11 as well as with results from other studies involving patients with refractory PMN.12,13,26 It is noteworthy that no relapses occurred in the OBZ group during follow-up, whereas 2 patients in the RTX group experienced relapse following remission. Although this difference did not reach statistical significance, it raises the possibility that OBZ may provide more sustained disease control compared with RTX, which warrants further investigation in larger studies. Overall, both treatment regimens demonstrated a good safety profile.
Limitations
This study has several limitations. First, as a retrospective study, there may have been selection bias and potential confounders. Second, the relatively limited sample size may have restricted the statistical power, and the absence of patients who switched from RTX to OBZ prevents any analysis of this treatment approach. However, given that PLA2R-positive PMN accounts for approximately 70% of cases and PLA2R-negative PMN is a relatively rare clinical subtype, the acquisition of relevant samples remains challenging.3 Therefore, future multicenter, large-sample, prospective studies are needed to further validate the findings of this study.
Conclusion
In conclusion, this study focused for the first time on PLA2R-negative PMN patients and found that OBZ and RTX had similar efficacy in such patients in terms of inducing clinical remission and safety. Further prospective randomized controlled trials are still needed to validate the results of this study and to comprehensively assess the efficacy and safety of OBZ in different PMN patient populations and clinical contexts.
Data Sharing Statement
The datasets generated and analysed during the current study are available from the corresponding author (Ben Ke) on reasonable request.
Ethics Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Bioethics Committee of The Second Affiliated Hospital to Nanchang University (approval no.: No. EFY20221011). All patients were unrelated. All patients signed an informed consent for participation prior to their inclusion in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the Natural Science Foundation of China (82360145 and 82560145).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ronco P, Beck L, Debiec H, et al. Membranous nephropathy. Nat Rev Dis Primers. 2021;7(1):69. doi:10.1038/s41572-021-00303-z
2. Ruggenenti P, Fervenza FC, Remuzzi G. Treatment of membranous nephropathy: time for a paradigm shift. Nat Rev Nephrol. 2017;13(9):563–579. doi:10.1038/nrneph.2017.92
3. Beck LH, Bonegio RGB, Lambeau G, et al. M-type phospholipase A2 receptor as target antigen in idiopathic membranous nephropathy. N Engl J Med. 2009;361(1):11–21.
4. Hoxha E, Reinhard L, Stahl RAK. Membranous nephropathy: new pathogenic mechanisms and their clinical implications. Nat Rev Nephrol. 2022;18(7):466–478. doi:10.1038/s41581-022-00564-1
5. Ahmad SB, Jefferson JA. Targeting B cells and plasma cells in glomerular disease. J Am Soc Nephrol. 2025;36(9):1844–1857. doi:10.1681/ASN.0000000772
6. Seitz-Polski B, Dahan K, Debiec H, et al. High-dose rituximab and early remission in PLA2R1-related membranous nephropathy. Clin J Am Soc Nephrol. 2019;14(8):1173–1182. doi:10.2215/CJN.11791018
7. Li H, Jin L, Xie X, et al. Additive obinutuzumab achieves high remission rates in rituximab-refractory membranous nephropathy. Am J Nephrol. 2025;1–9.
8. Vink CH, Wetzels JFM, Logt AV. Combination therapy with rituximab and low-dose cyclophosphamide and prednisone in membranous nephropathy. Kidney Int Rep. 2024;9(12):3439–3445. doi:10.1016/j.ekir.2024.08.033
9. Kidney Disease: improving Global Outcomes Glomerular Diseases Work G. KDIGO 2021 clinical practice guideline for the management of glomerular diseases. Kidney Int. 2021;100(4S):S1–S276. doi:10.1016/j.kint.2021.05.021
10. Mössner E, Brünker P, Moser S, et al. Increasing the efficacy of CD20 antibody therapy through the engineering of a new type II anti-CD20 antibody with enhanced direct and immune effector cell-mediated B-cell cytotoxicity. Blood. 2010;115(22):4393–4402. doi:10.1182/blood-2009-06-225979
11. Hu X, Zhang M, Xu J, et al. Comparison of obinutuzumab and rituximab for treating primary membranous nephropathy. Clin J Am Soc Nephrol. 2024;19(12):1594–1602. doi:10.2215/CJN.0000000000000555
12. Xu M, Wang Y, Wu M, et al. Obinutuzumab versus rituximab for the treatment of refractory primary membranous nephropathy. Nephrol Dial Transplant. 2025;40(5):978–986. doi:10.1093/ndt/gfae230
13. Sethi S, Kumar S, Lim K, Jordan SC. Obinutuzumab is effective for the treatment of refractory membranous nephropathy. Kidney Int Rep. 2020;5(9):1515–1518. doi:10.1016/j.ekir.2020.06.030
14. Li XQ, Liu Y, Cai ZY, Lv TG, Hao J. Obinutuzumab is effective as an initial treatment for PLA2R-associated primary membranous nephropathy: a retrospective, single-center trial. Drug Des Devel Ther. 2025;19:5961–5972. doi:10.2147/DDDT.S527661
15. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
16. Dähnrich C, Komorowski L, Probst C, et al. Development of a standardized ELISA for the determination of autoantibodies against human M-type phospholipase A2 receptor in primary membranous nephropathy. Clin Chim Acta. 2013;421:213–218. doi:10.1016/j.cca.2013.03.015
17. Zand L, Russo I, Vargas-Brochero MJ, et al. Phospholipase A2 receptor-positive membranous nephropathy detected by laser microdissection and mass spectrometry in patients negative by immunofluorescence for phospholipase A2 receptor on kidney biopsy. Kidney Int. 2025;108(3):481–484. doi:10.1016/j.kint.2025.04.032
18. Sun Y, Lan P, Feng J, et al. Analysis of glomerular PLA2R efficacy in evaluating the prognosis of idiopathic membranous nephropathy in the background of different serum anti-PLA2R levels. Ren Fail. 2022;44(1):731–740. doi:10.1080/0886022X.2022.2068442
19. Duan X, Lv X, Wang X, et al. Impact of immune cell metabolism on membranous nephropathy and prospective therapy. Commun Biol. 2025;8(1):405. doi:10.1038/s42003-025-07816-3
20. Marinov AD, Wang H, Bastacky SI, et al. The type II anti-CD20 antibody obinutuzumab (GA101) is more effective than rituximab at depleting B cells and treating disease in a murine lupus model. Arthritis Rheumatol. 2021;73(5):826–836. doi:10.1002/art.41608
21. Allinovi M, Teisseyre M, Accinno M, et al. Anti-rituximab antibodies occurrence and clinical outcomes in patients with primary membranous nephropathy. Kidney Int Rep. 2025;10(8):2621–2629. doi:10.1016/j.ekir.2025.04.059
22. Teisseyre M, Brglez V, Cremoni M, et al. Risk factors associated with the occurrence of anti-rituximab antibodies in membranous nephropathy. Clin J Am Soc Nephrol. 2023;18(6):785–787. doi:10.2215/CJN.0000000000000152
23. Boyer-Suavet S, Andreani M, Lateb M, et al. Neutralizing anti-rituximab antibodies and relapse in membranous nephropathy treated with rituximab. Front Immunol. 2019;10:3069. doi:10.3389/fimmu.2019.03069
24. Teisseyre M, Cremoni M, Boyer-Suavet S, et al. Advances in the management of primary membranous nephropathy and rituximab-refractory membranous nephropathy. Front Immunol. 2022;13:859419. doi:10.3389/fimmu.2022.859419
25. Golay J, Da Roit F, Bologna L, et al. Glycoengineered CD20 antibody obinutuzumab activates neutrophils and mediates phagocytosis through CD16B more efficiently than rituximab. Blood. 2013;122(20):3482–3491. doi:10.1182/blood-2013-05-504043
26. Teisseyre M, Allinovi M, Audard V, et al. Obinutuzumab and ofatumumab are more effective than rituximab in the treatment of membranous nephropathy patients with anti-rituximab antibodies. Kidney Int Rep. 2025;10(3):753–761. doi:10.1016/j.ekir.2024.12.012
27. Tomas NM, Beck LH, Meyer-Schwesinger C, et al. Thrombospondin type-1 domain-containing 7A in idiopathic membranous nephropathy. N Engl J Med. 2014;371(24):2277–2287. doi:10.1056/NEJMoa1409354
28. Sethi S, Debiec H, Madden B, et al. Neural epidermal growth factor-like 1 protein (NELL-1) associated membranous nephropathy. Kidney Int. 2020;97(1):163–174. doi:10.1016/j.kint.2019.09.014
29. Sethi S, Debiec H, Madden B, et al. Semaphorin 3B-associated membranous nephropathy is a distinct type of disease predominantly present in pediatric patients. Kidney Int. 2020;98(5):1253–1264. doi:10.1016/j.kint.2020.05.030
30. Sethi S, Madden BJ, Debiec H, et al. Exostosin 1/exostosin 2-associated membranous nephropathy. J Am Soc Nephrol. 2019;30(6):1123–1136. doi:10.1681/ASN.2018080852
31. Gu Y, Xu H, Tang D. Mechanisms of primary membranous nephropathy. Biomolecules. 2021;11(4):513. doi:10.3390/biom11040513
32. Zhang C, Leng L, Li Z, Zhao Y, Jiao J. Identification of biomarkers and drug repurposing candidates based on an immune-, inflammation- and membranous glomerulonephritis-associated triplets network for membranous glomerulonephritis. BMC Med Genomics. 2020;13(1):5. doi:10.1186/s12920-019-0655-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sequential Treatment by Antiviral Drugs Followed by Immunosuppressive Agents for COVID-19 Patients with Hematological Malignancy
Seki M, Hashimoto K, Kondo N, Ohya Y, Kotajima F, Mitsutake K
Infection and Drug Resistance 2022, 15:7117-7124
Published Date: 5 December 2022
Obinutuzumab as a Rescue and Maintenance Strategy in Children with Difficult-to-Treat Nephrotic Syndrome After Rituximab-Based Treatment Failure or Intolerance: A Preliminary Single-Center Real-World Retrospective Study
Sun H, Guo L, Shao P, Liang W, Ma X, He Y, Qiu L
Drug Design, Development and Therapy 2026, 20:619807
Published Date: 15 July 2026