Back to Journals » Drug Design, Development and Therapy » Volume 20
Targeted Therapy–Induced Interstitial Lung Disease in NSCLC: Mechanisms, Clinical Signatures, and a Precision Medicine Roadmap
Authors Wang JF ![]() , Jiang LL, Wang MC, Li YL
, Jiang LL, Wang MC, Li YL
Received 1 February 2026
Accepted for publication 28 March 2026
Published 8 April 2026 Volume 2026:20 600434
DOI https://doi.org/10.2147/DDDT.S600434
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Jia-feng Wang,1,* Lei-lei Jiang,2,* Meng-chuan Wang,3 Yang-ling Li1
1Department of Clinical Pharmacy, Key Laboratory of Clinical Cancer Pharmacology and Toxicology Research of Zhejiang Province, Affiliated Hangzhou First People’s Hospital, School of Medicine, Westlake University, Hangzhou, Zhejiang, People’s Republic of China; 2The First Affiliated Hospital of Anhui University of Chinese Medicine, Hefei, Anhui, People’s Republic of China; 3Affiliated Cixi Hospital, Wenzhou Medical University, Ningbo, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yang-ling Li, Department of Clinical Pharmacy, Key Laboratory of Clinical Cancer Pharmacology and Toxicology Research of Zhejiang Province, Affiliated Hangzhou First People’s Hospital, School of Medicine, Westlake University, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected] Meng-chuan Wang, Affiliated Cixi Hospital, Wenzhou Medical University, Ningbo, Zhejiang, People’s Republic of China, Email [email protected]
Abstract: Molecularly targeted therapies have transformed the therapeutic landscape of non–small cell lung cancer (NSCLC), establishing precision oncology as the foundation of modern disease management. However, these advances are increasingly complicated by drug-induced interstitial lung disease (DILD), a potentially life-threatening adverse event that can disrupt treatment continuity and compromise clinical benefit. In this review, we provide a comprehensive evaluation of interstitial lung disease associated with targeted agents in NSCLC, including oncogene-directed tyrosine kinase inhibitors, antibody–drug conjugates (ADCs), and angiogenesis inhibitors. We summarize reported differences in ILD incidence, onset timing, clinical manifestations, and radiographic characteristics across targeted agents, with particular emphasis on high-risk populations and the elevated ILD incidence observed with deruxtecan-based ADCs. We further summarize current mechanistic evidence suggesting that DILD may arise from multiple overlapping processes, including immune-mediated inflammatory activation, direct epithelial cytotoxicity, off-target kinase inhibition, and payload-dependent bystander injury. Finally, we discuss current challenges and future directions for improving pulmonary safety, including real-world datasets, multi-omics approaches, and emerging AI-assisted tools for earlier detection and risk stratification. Importantly, the current evidence base remains limited by the predominance of retrospective studies, case reports, and incomplete mechanistic validation. These insights may help guide safer and more sustained implementation of targeted therapies in NSCLC.
Keywords: non-small cell lung cancer, targeted therapy, interstitial lung disease, precision oncology, antibody–drug conjugates
Introduction
Lung cancer remains a dominant global health burden, consistently ranking among the most frequently diagnosed malignancies and the leading cause of cancer-related mortality worldwide.1 Despite progress in screening strategies and therapeutic innovations, both its incidence and mortality rates remain disproportionately high. Non-small cell lung cancer (NSCLC), accounting for nearly 85% of all lung cancer cases, contributes to the vast majority of lung cancer–related deaths.2 NSCLC remains difficult to manage due to its marked biological heterogeneity, frequent late-stage diagnosis, and the compounding influence of genetic, environmental, and comorbid factors such as COPD, all of which complicate treatment tolerance and outcomes.3–5 These challenges underscore the need for more precise therapeutic strategies, setting the stage for the emergence of targeted therapies in modern NSCLC management.
Since the early 21st century, transformative advances in molecular diagnostics and targeted drug development have reshaped the therapeutic landscape of lung cancer. The identification of actionable oncogenic drivers, including EGFR, ALK, ROS1, BRAF, MET, RET and NTRK, has enabled precision medicine strategies that markedly improve disease control and overall quality of life in biomarker-defined populations.6 For example, osimertinib can extend the median progression-free survival (PFS) to 15.3 months in patients with EGFR-mutated non-small cell lung cancer, and selpercatinib has achieved a median progression-free survival of 22.0 months in individuals with RET fusion positive disease.7,8 These therapeutic advances firmly establish targeted agents as a central component of the management of advanced non-small cell lung cancer and have fundamentally altered its clinical trajectory.
However, the expanding clinical adoption of targeted therapies has heightened awareness of their associated adverse events. Among these toxicities, pulmonary complications have drawn particular concern because they may present abruptly, progress rapidly, and even result in fatal outcomes, thereby disrupting treatment continuity and compromising overall prognosis.9 Within the spectrum of drug-related pulmonary toxicities, interstitial lung disease (ILD) represents the most clinically significant entity. ILD encompasses a heterogeneous group of disorders characterized by varying degrees of inflammation and fibrosis of the lung parenchyma, typically manifesting as progressive dyspnea and, in severe cases, advancing to respiratory failure. Beyond drug-induced injury, the etiologies of ILD include environmental exposures, infections, and systemic diseases. Epidemiologically, idiopathic pulmonary fibrosis accounts for approximately 33% of cases, hypersensitivity pneumonitis for about 15%, and connective tissue disease–associated ILD for roughly 25%.10
Several targeted agents—particularly EGFR and ALK inhibitors—have been associated with the development of drug-induced ILD. The clinical identification of these toxicities is often challenging, as their manifestations can be easily confounded with infectious pneumonia, disease progression, or radiation-induced lung injury, thereby complicating timely recognition and accurate diagnosis.11,12
In the context of targeted therapy for NSCLC, drug-induced interstitial lung disease is typically diagnosed on the basis of a temporal relationship between drug exposure and new pulmonary symptoms and/or radiographic abnormalities, together with exclusion of alternative etiologies such as infection, tumor progression, radiation pneumonitis, immune-related pneumonitis, pulmonary edema, and autoimmune lung disease. In clinical practice, diagnosis usually relies on integrated assessment of treatment history, symptom onset, chest CT patterns, laboratory and microbiologic evaluation, and, when necessary, bronchoalveolar lavage or transbronchial lung biopsy. Because no single finding is pathognomonic, targeted therapy–associated ILD remains a diagnosis that depends on multidisciplinary clinical judgment.
To provide a focused and up-to-date overview, this review was informed by a targeted literature search of major biomedical databases, including PubMed, supplemented by manual screening of reference lists from relevant studies and cross-checking of regulatory information from publicly accessible FDA and NMPA sources where applicable. Priority was given to clinical trials, retrospective studies, pharmacovigilance reports, case series, case reports, and mechanistic investigations relevant to targeted therapy–associated ILD in NSCLC, with particular emphasis on recent evidence.
Importantly, susceptibility to targeted therapy–related ILD appears to vary across populations. Previous studies have suggested a higher incidence of EGFR-TKI–associated ILD in Asian patients than in Western cohorts, indicating potential ethnic and geographic variability in susceptibility. In addition, the incidence and spectrum of ILD reported in real-world studies may differ from those observed in clinical trials, likely owing to broader patient inclusion, greater comorbidity burden, pre-existing interstitial lung abnormalities, and differences in monitoring intensity. A more careful consideration of these population-level differences is therefore essential for accurate interpretation of safety data and individualized risk assessment.
Accordingly, this review provides a comprehensive synthesis of ILD associated with targeted agents in lung cancer, with emphasis on clinical presentation and classification, drug-specific risk profiles, proposed pathogenic mechanisms, clinical implications, and current management strategies. We further outline emerging research priorities and future directions, aiming to guide clinicians in risk stratification, therapeutic decision-making, and toxicity mitigation, thereby supporting the safe and sustained application of precision therapies in NSCLC.
Overview of Targeted Therapies in NSCLC
NSCLC accounts for approximately 85% of all lung cancer cases and exhibits substantial molecular complexity, encompassing a wide range of actionable oncogenic driver alterations. With the rapid advancement of second- and third-generation sequencing technologies, key genomic events such as EGFR mutations; ALK and ROS1 rearrangements; MET exon 14 skipping alterations or amplification; RET and NTRK fusions; HER2 and BRAF mutations, including BRAF V600E; and KRAS G12C mutations can now be routinely identified in clinical practice. These molecular alterations constitute the biological foundation of contemporary precision oncology and have become central therapeutic targets in NSCLC, as illustrated in Figure 1.
 |
Figure 1 Major oncogenic driver alterations in NSCLC. This schematic summarizes the principal molecular drivers in NSCLC and the corresponding categories of genetic alterations, including EGFR mutations; ALK and ROS1 rearrangements; MET exon 14 skipping or amplification; RET and NTRK fusions; HER2 and BRAF mutations (including BRAF V600E); KRAS G12C mutation; and dysregulated VEGF pathway activation. These alterations represent essential biomarkers for molecular stratification and serve as key therapeutic targets in precision oncology for NSCLC. |
Over the past decade, targeted therapies have profoundly reshaped the treatment landscape of NSCLC. Tyrosine kinase inhibitors (TKIs) directed against EGFR, ALK, ROS1, MET, RET, and NTRK, together with antibody–drug conjugates (ADCs) targeting HER2 or TROP2, are now recognized as standard-of-care options in multiple international guidelines. In EGFR-mutated NSCLC, therapeutic evolution from first-generation EGFR-TKIs to the third-generation inhibitor osimertinib has led to consistent improvements in progression-free survival (PFS), enhanced control of resistance mutations such as T790M, and superior central nervous system activity.13–15 A comparable trajectory has been observed in ALK-positive NSCLC, where treatment has progressed from crizotinib to second-generation inhibitors such as alectinib and brigatinib, and subsequently to the third-generation agent lorlatinib, yielding stepwise gains in systemic and intracranial disease control.16–18
Beyond EGFR and ALK, the development and regulatory approval of MET inhibitors (capmatinib and tepotinib), RET-selective TKIs (selpercatinib and pralsetinib), HER2-targeted agents, and KRAS G12C inhibitors have further expanded the therapeutic landscape of NSCLC. These therapies have demonstrated substantial clinical benefit in biomarker-defined populations and solidified the central role of molecular stratification in NSCLC management.19–23
Despite the remarkable clinical improvements achieved with targeted therapies, their toxicity profiles differ markedly from those of conventional cytotoxic chemotherapy and are strongly linked to their mechanisms of action. EGFR inhibitors frequently cause dermatologic toxicities and diarrhea; ALK inhibitors may induce visual disturbances or cardiovascular effects; and several TKIs as well as certain ADCs have been associated with ILD.24,25 Although relatively infrequent, drug-induced interstitial lung disease (DILD) can be clinically significant and may influence treatment planning, monitoring intensity, dose modification, and treatment continuity, particularly in patients with baseline lung vulnerability or prior pulmonary toxicity. As precision therapies become increasingly foundational in NSCLC care, proactive recognition and monitoring of these adverse events remain essential.
Clinical Features of ILD from Targeted Therapies
With the expanding use of targeted therapies in lung cancer, their associated ILD have come under increasing scrutiny. ILD represents a serious yet frequently underestimated adverse effect of TKIs, often characterized by insidious onset, rapid clinical deterioration, and a substantial risk of misdiagnosis. Among agents such as EGFR-TKIs and ALK inhibitors, ILD has been consistently linked to drug exposure across multiple studies and is now recognized as a major factor limiting long-term treatment and adversely influencing patient prognosis.26,27
The clinical manifestations of TKI-related ILD are highly heterogeneous and may present acutely, subacutely, or chronically.28 Patients typically experience nonspecific respiratory symptoms, including dry cough, dyspnea, chest tightness, low-grade fever, and fatigue. Severe cases may progress to hypoxemia, respiratory failure, or even acute respiratory distress syndrome (ARDS).28 In some instances, radiographic abnormalities precede or exceed clinical symptoms, further complicating early detection. The timing of onset varies across agents: events associated with osimertinib may occur early during therapy, whereas toxicities related to agents such as crizotinib may arise after months or prolonged treatment durations.28–30 Combination strategies, such as the administration of TKIs in combination with radiotherapy, chemotherapy, or immunotherapy, significantly amplify the risk of ILD. For example, the incidence of ILD increases to 4.8% when EGFR-TKIs are combined with stereotactic body radiotherapy,31 and co-administration of osimertinib with durvalumab has been shown to elevate ILD incidence.32
Beyond small-molecule TKIs, an expanding spectrum of non-TKI targeted agents has also been implicated in ILD development, with distinct clinical characteristics that differ substantially from those observed with kinase inhibitors. Antibody–drug conjugates (ADCs), particularly those incorporating potent cytotoxic payloads such as deruxtecan, are associated with a disproportionately higher incidence of ILD and represent one of the most clinically concerning categories of targeted therapy–related lung injury. ADC-associated ILD often presents insidiously, with a subacute onset over weeks to months, and may initially manifest with minimal respiratory symptoms despite extensive radiographic involvement.33 Ground-glass opacities and organizing pneumonia–like patterns are frequently observed, and progression can be rapid if not recognized early, underscoring the importance of proactive surveillance even in asymptomatic patients.34
Anti-angiogenic agents targeting the VEGF/VEGFR axis, including monoclonal antibodies and small-molecule inhibitors, have also been linked to ILD, although at a relatively lower incidence compared with TKIs and ADCs. ILD associated with these agents is often characterized by diffuse or patchy interstitial infiltrates and may coexist with other pulmonary complications such as hemorrhage or thromboembolic events, complicating clinical assessment.35 The onset is typically delayed and may overlap with cumulative vascular injury or prior thoracic radiotherapy, making causal attribution challenging in real-world settings.
Diagnosing ILD is inherently challenging and requires the careful exclusion of multiple alternative etiologies, including pulmonary infections, radiation pneumonitis, immune checkpoint inhibitor–associated pneumonitis, tumor progression or metastasis, and autoimmune lung diseases. For instance, pulmonary symptoms arising after the combined use of radiotherapy and targeted agents are frequently misinterpreted as radiation-induced pneumonitis. Similarly, patients with drug-induced ILD who fail to respond to standard antimicrobial therapy may be incorrectly diagnosed with antibiotic-resistant infections. Accordingly, obtaining a comprehensive medical history, establishing a precise timeline of drug exposure, evaluating dynamic radiologic changes, and, when indicated, performing bronchoalveolar lavage (BAL) or transbronchial lung biopsy are essential for achieving diagnostic certainty.
Beyond its immediate pulmonary toxicity, targeted therapy–associated ILD may also adversely affect survival in patients with NSCLC by interrupting effective anticancer treatment, limiting subsequent therapeutic options, and increasing the risk of severe respiratory complications. Available evidence suggests that severe ILD, particularly high-grade or fatal events, is associated with poor clinical outcomes; however, direct survival comparisons between treated and untreated ILD cases in this setting remain scarce. In many reports, outcome is further confounded by differences in ILD severity, baseline lung function, cancer burden, and the extent to which anticancer therapy can be resumed after recovery. These limitations underscore the need for more systematic evaluation of the prognostic impact of ILD and the extent to which timely recognition and appropriate management may improve survival outcomes.
In summary, ILD associated with targeted therapies is frequently insidious in onset and heterogeneous in both clinical manifestation and radiographic appearance, making early recognition particularly challenging. Its clinical significance extends beyond acute pulmonary toxicity, as severe events may interrupt effective anticancer treatment and adversely affect patient outcomes. At the same time, cross-study interpretation of ILD incidence and presentation should be approached cautiously, as available data are influenced by differences in diagnostic criteria, adverse event attribution, patient selection, and monitoring intensity across clinical trials and real-world settings. Accurate interpretation of imaging features, adherence to standardized grading frameworks, and continuous clinical monitoring are therefore essential to mitigating ILD-related complications while preserving the antitumor efficacy of targeted agents.
In summary, ILD associated with targeted therapies is frequently insidious in onset and heterogeneous in both clinical manifestation and radiographic appearance, making early recognition particularly challenging. Its severity is closely tied to patient outcomes, underscoring the need for heightened clinical vigilance and prompt intervention. At the same time, cross-study interpretation of ILD incidence and presentation should be approached cautiously, as available data are influenced by differences in diagnostic criteria, adverse event attribution, patient selection, and monitoring intensity across clinical trials and real-world settings. Accurate interpretation of imaging features, adherence to standardized grading frameworks, and continuous clinical monitoring are essential to mitigating ILD–related complications while preserving the antitumor efficacy of targeted agents.
ILD Profiles Across Targeted Therapy Classes in NSCLC
Targeted therapies differ markedly in their propensity to induce ILD, with substantial variability observed across drug classes in terms of incidence, timing of onset, clinical manifestations, and radiographic patterns. As illustrated in Figure 2, the therapeutic landscape of NSCLC has expanded rapidly over the past two decades, with successive approvals of molecularly directed agents that differ not only in their mechanisms of action but also in their safety profiles. Reflecting these distinctions, Table 1 provides a consolidated overview of the reported incidence, mortality, symptomatology, onset timing, imaging characteristics, and recommended management strategies for ILD associated with representative targeted agents used in NSCLC.
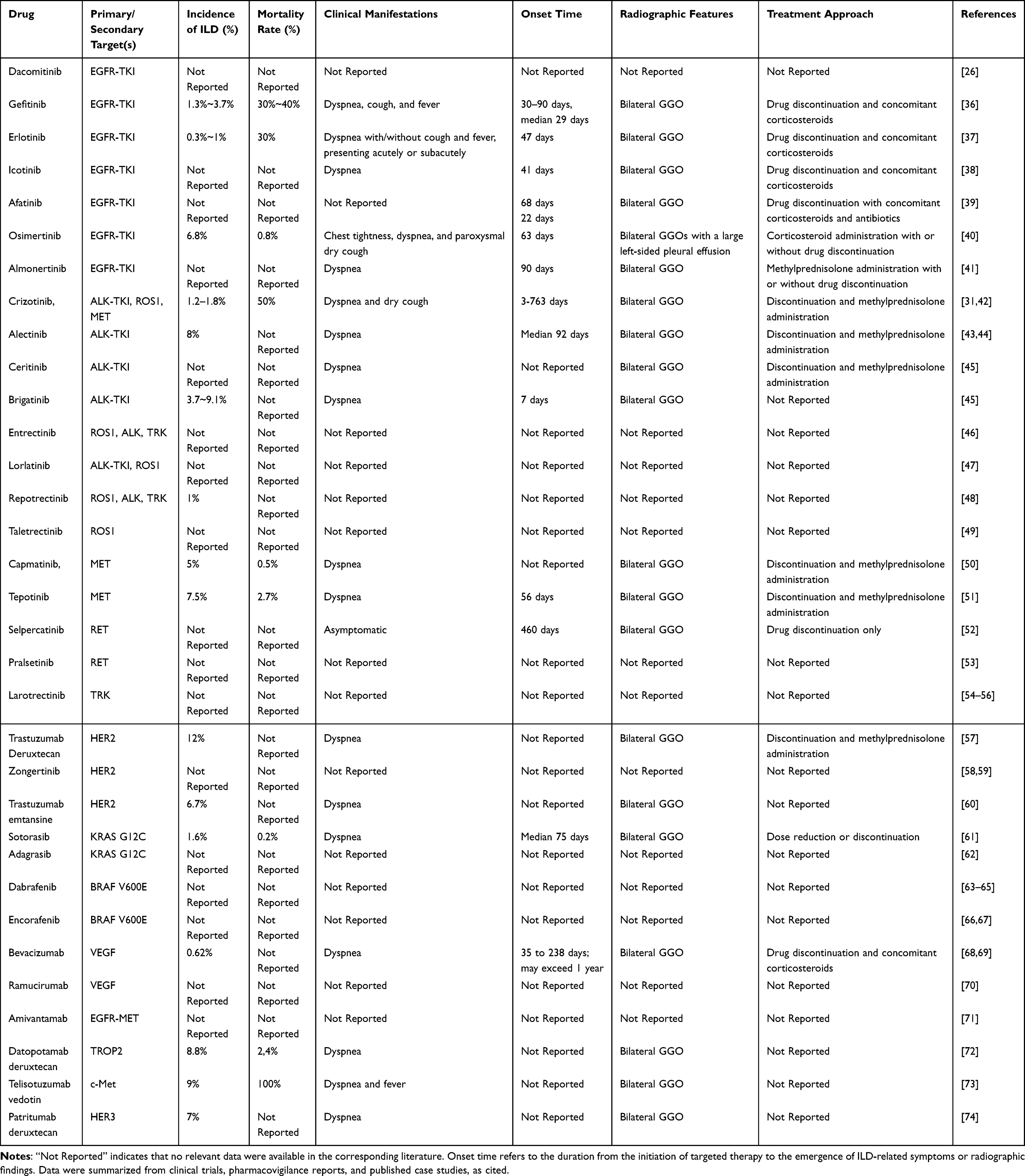 |
Table 1 Clinical Manifestations, Radiological Features, and Management of Targeted Therapy-Associated ILD in NSCLC Patients |
 |
Figure 2 Timeline of FDA approvals and recent regulatory advances for targeted therapies in NSCLC (2003–2025). The landscape of targeted therapy has evolved from early EGFR-TKIs and monoclonal antibodies to a diverse array of kinase inhibitors and novel antibody-drug conjugates (ADCs). Drugs are categorized by their primary mechanism of action: red, EGFR Tyrosine Kinase Inhibitors (TKIs); blue, Other Targeted Kinase Inhibitors (targeting ALK, ROS1, MET, RET, KRAS, BRAF, or HER2); green, Monoclonal Antibodies (mAbs); yellow, Antibody-Drug Conjugates (ADCs). Notes: Timeline represent the year of the first FDA approval for NSCLC, regardless of treatment line. Agents listed under 2025 include those recently approved or currently under regulatory review. |
A detailed understanding of these drug-specific risk signatures is essential for enhancing clinical vigilance, guiding individualized risk stratification, and informing rational therapeutic decision-making. In the following sections, we systematically compare the ILD profiles of major targeted therapy classes, highlighting both shared features and class-specific patterns that are clinically relevant for daily practice. Approval information for individual targeted agents, including initial authorization dates and regulatory designations, was retrieved from the U.S. FDA Drugs@FDA and NMPA public databases75,76 (see Supplementary Table S1 for detailed approval history and source links).
EGFR-TKIs
EGFR-TKIs represent one of the earliest classes of molecularly targeted therapies applied in the precision treatment of NSCLC. Several agents in this category have received regulatory approval for the first-line treatment of metastatic NSCLC harboring EGFR exon 19 deletions or exon 21 L858R substitution mutations, including the first-generation inhibitors gefitinib and erlotinib, the second-generation inhibitors afatinib and dacomitinib, and the third-generation inhibitor osimertinib. In addition, icotinib has been approved by the NMPA in China for EGFR-mutated NSCLC, while almonertinib has been approved in China for T790M-positive disease. Collectively, these agents have significantly improved PFS and OS in patients with EGFR-mutated tumors. Despite these clinical benefits, drug-induced ILD—though relatively uncommon—has drawn substantial attention due to its potential for severe and sometimes fatal outcomes. Notably, both the incidence and mortality of ILD appear to be higher in Asian populations compared with Western cohorts, highlighting important ethnic and geographic differences in susceptibility.35,77
According to previous systematic reviews, the incidence of ILD associated with the first-generation EGFR-TKI gefitinib ranges from 1.3% to 3.7%, with a reported mortality rate reaching 30%–40%.27 The median onset time is approximately 29 days. Clinically, patients often present with acute dyspnea (100%), cough (60%), and fever (13.3%), while radiologic manifestations commonly feature bilateral diffuse ground-glass opacities. Standard management typically consists of immediate drug discontinuation and initiation of high-dose corticosteroids, such as methylprednisolone.36 Erlotinib-induced ILD occurs less frequently, with an estimated incidence of 2% and a mortality rate of about 30%.27 The average onset time is roughly 36.5 days, and imaging features also predominantly demonstrate bilateral ground-glass changes.37
Although published data on the domestically developed EGFR-TKI icotinib remain limited, reports have described acute dyspnea and radiographic ground-glass opacities emerging approximately six weeks after treatment initiation.38
Among second-generation EGFR-TKIs, afatinib has been associated with a comparatively higher incidence of ILD, estimated at approximately 4%, whereas its mortality rate remains relatively low at around 1%.39 Reported cases indicate that ILD typically develops within 3 to 10 weeks of therapy and commonly presents with fever and exertional dyspnea. HRCT findings frequently reveal bilateral ground-glass opacities. Despite prompt drug discontinuation and corticosteroid administration, disease progression and fatal outcomes have still been documented in some patients. In contrast, no definitive cases of dacomitinib-induced ILD have been reported to date.
The third-generation EGFR-TKI osimertinib warrants particular attention due to its heightened ILD risk reported among Asian populations. A real-world Japanese study documented an ILD incidence of 6.8% and a mortality rate of 0.8%.40 According to the FDA label, osimertinib has also been associated with ILD/pneumonitis in approximately 2.1% of treated patients, along with pneumonia (2.9%) and pulmonary embolism (1.8%). These regulatory data, derived from pooled clinical trial populations, indicate a lower incidence compared with real-world findings in Asian cohorts, suggesting potential differences in population susceptibility, exposure patterns, or clinical management practices. Another domestically developed third-generation agent, almonertinib, is generally well tolerated; however, isolated case reports have described the onset of ILD approximately three months after treatment initiation. Interestingly, some patients exhibited symptomatic improvement with corticosteroids alone without discontinuing therapy, suggesting that the ILD spectrum and optimal management strategies for this agent require further elucidation.41
Although the precise mechanisms underlying EGFR-TKI–induced ILD remain incompletely defined, available evidence suggests that these agents may perturb coordinated processes of alveolar epithelial repair, immune homeostasis, and tissue remodeling; detailed mechanistic insights are discussed in Mechanisms of Drug-Induced ILD.78,79
Notably, the risk of ILD varies substantially across different generations and structural classes of EGFR-TKIs, suggesting that on-target and off-target effects may differentially influence susceptibility. These risks may also be amplified by host-specific factors, including genetic background, pre-existing lung abnormalities, and concurrent treatments such as radiotherapy or immunotherapy. However, these comparisons should be interpreted cautiously, as reported incidence is influenced by heterogeneity in study design, patient selection, ILD definitions, and methods of adverse event reporting.
ALK-TKIs
Anaplastic lymphoma kinase (ALK) inhibitors constitute a major therapeutic class in the management of ALK-positive NSCLC, achieving substantial improvements in PFS and OS. Several ALK tyrosine kinase inhibitors have received regulatory approval from the U.S. Food and Drug Administration for first-line treatment of ALK-positive non–small cell lung cancer. Crizotinib, the first-generation ALK inhibitor, was initially approved in 2011 for metastatic ALK-positive disease, with its indication subsequently expanded in 2016 to include ROS1-rearranged NSCLC. This was followed by the approval of second-generation agents, including alectinib, ceritinib, and brigatinib, all of which are currently indicated for first-line therapy in ALK-positive NSCLC. The third-generation TKI Lorlatinib is likewise approved as a first-line option for ALK-positive metastatic disease.
Crizotinib, the first-generation ALK inhibitor, is an oral small-molecule tyrosine kinase inhibitor that also inhibits ROS1 and MET kinases.80 The reported incidence of crizotinib-associated ILD ranges from 1.2% to 1.8%, with a mortality rate of up to 50%,29 making it one of the most clinically concerning pulmonary toxicities among ALK-TKIs. The time to onset is highly variable, ranging from as early as 3 days to more than 2 years after treatment initiation. Clinically, patients commonly develop acute dyspnea and dry cough, with radiologic patterns dominated by bilateral diffuse ground-glass opacities. Standard management includes immediate drug discontinuation, corticosteroid pulse therapy (eg, methylprednisolone), and empiric antibiotics when appropriate. Timely recognition and intervention may result in clinical improvement.42
Second-generation ALK inhibitors include alectinib, ceritinib, and brigatinib. Alectinib itself is associated with ILD. Analyses from the Japanese pharmacovigilance database report an ILD incidence of approximately 8%, with a median onset time of 92 days. Notably, no fatal cases have been documented, and most patients respond well to corticosteroid therapy.43,44 Ceritinib-related ILD is less frequently reported. One case involved dyspnea and bilateral ground-glass opacities after 11 months of treatment, which improved after drug discontinuation and methylprednisolone therapy.81
Brigatinib exhibits a characteristic “early-onset” ILD profile, with symptoms such as dyspnea, hypoxemia, and radiologic ground-glass opacities occurring within hours to 48 hours after treatment initiation. The incidence of ILD ranges from 3.7% to 9.1%.45 This unique temporal pattern underscores the need for close monitoring during early treatment and supports the use of cautious dose-escalation strategies.
Lorlatinib, a third-generation ALK inhibitor that also targets ROS1, has not been definitively linked to ILD. Case reports suggest that lorlatinib may be safely administered to patients who developed ILD from alectinib or brigatinib, implying a potential safety advantage in susceptible individuals.82 However, due to limited sample sizes and a lack of systematic real-world evidence, further studies are needed to validate these observations and to clarify the pulmonary safety profile of lorlatinib.
Although the pathogenesis of ALK-TKI–related ILD remains incompletely defined, current evidence suggests that it may reflect a convergence of multiple injury pathways, including alveolar epithelial damage, immune-mediated inflammation, oxidative stress, and aberrant fibrotic remodeling. The apparent heterogeneity in ILD across different ALK-TKI generations further supports a possible contribution of drug-specific factors, such as molecular structure, hydrophobicity, off-target kinase inhibition, and differential pulmonary tissue penetration, to toxicity risk. Host-related determinants, including baseline lung impairment, prior thoracic radiotherapy, and concurrent anticancer therapies, may additionally modulate individual susceptibility.
ROS1-TKIs
ROS1 gene rearrangements account for approximately 1–2% of NSCLC cases and represent an actionable oncogenic driver.83 Several ROS1-targeted TKIs have been developed, with multiple agents now approved for clinical use. The first-generation TKI crizotinib, initially approved by the U.S. FDA in 2011 for ALK-positive metastatic NSCLC and subsequently expanded in 2016 to include ROS1-positive disease, remains a foundational therapy in this setting. Entrectinib, a multi-target inhibitor of ROS1, ALK, and TRK, is FDA-approved for first-line treatment of ROS1-positive metastatic NSCLC as well as NTRK fusion–positive solid tumors.8,14 The third-generation ALK/ROS1 inhibitor lorlatinib, previously described in the ALK-TKI section, is likewise FDA-approved for ROS1-positive NSCLC in later-line settings. In 2023, the macrocyclic next-generation inhibitor repotrectinib received FDA approval as a first-line therapy for ROS1-positive metastatic NSCLC, offering potent activity against resistance mutations.15 Taletrectinib, a next-generation selective ROS1 inhibitor, was approved by the U.S. FDA in June 2025 for the treatment of adults with locally advanced or metastatic ROS1-positive NSCLC, making it an additional first-line therapeutic option within the ROS1-targeted therapy landscape.
The ILD profile of the first-generation ROS1 inhibitor crizotinib has been comprehensively addressed in the ALK-TKI section and will not be repeated here. To overcome acquired resistance and improve CNS activity, several next-generation ROS1 inhibitors have been developed with enhanced target affinity and broader activity against resistance mutations. Entrectinib, a multi-target inhibitor of ROS1, ALK, and TRK, has not been clearly associated with ILD; in clinical studies, dyspnea occurred in fewer than 1% of patients.46 Notably, a case report described an 85-year-old woman with ROS1-rearranged NSCLC who developed crizotinib-induced ILD after two months of therapy. Following drug discontinuation and prednisone treatment, her pulmonary symptoms improved, and she was successfully transitioned to entrectinib, achieving subsequent disease stability.84 This case highlights the potential role of entrectinib as a feasible alternative in patients unable to tolerate crizotinib due to ILD.
Lorlatinib, a third-generation ALK/ROS1 inhibitor, has not demonstrated a clear signal of increased ILD risk in ROS1-positive patients, consistent with the safety profile described in the ALK-TKI section.47 Repotrectinib (TPX-0005), a next-generation macrocyclic TKI targeting ROS1, TRKA–C, and ALK, reported an ILD incidence of approximately 1% in a clinical study of 426 patients, suggesting a generally manageable pulmonary safety profile.48 Taletrectinib, another emerging selective ROS1 inhibitor, has shown encouraging safety outcomes in the China-based TRUST-I trial, with no confirmed ILD cases reported to date, indicating a potentially favorable ILD profile.49
Compared with EGFR- and ALK-targeted therapies, ROS1 inhibitors generally exhibit a lower overall incidence of ILD, with severe or fatal cases being exceedingly rare. However, the true risk profile remains incompletely defined due to the inherently small ROS1-positive patient population, limited sample sizes, and relatively short follow-up durations in existing studies. Drug-specific structural features, kinase selectivity profiles, and differences in pulmonary tissue penetration may further contribute to heterogeneity in toxicity risk across ROS1 inhibitors. Future research should prioritize large-scale, multi-center real-world analyses and refine high-risk patient stratification. Integrating pharmacokinetic/pharmacodynamic modeling and multi-omics approaches may facilitate the development of predictive biomarkers and tailored monitoring strategies, ultimately enabling more precise assessment and individualized management of ROS1 inhibitor–associated ILD.
MET-TKIs
Mesenchymal–epithelial transition (MET) exon 14 skipping mutations (METex14) represent a clinically actionable oncogenic driver present in approximately 3% of NSCLC cases.50 Two selective MET inhibitors have been approved by the U.S. FDA for the first-line treatment of metastatic NSCLC harboring METex14 alterations: capmatinib, the first MET inhibitor to receive regulatory approval, and tepotinib, subsequently approved based on confirmatory efficacy data. The MET-inhibitory activity of crizotinib, although well recognized, lacks FDA approval for METex14-altered NSCLC and has been discussed previously in the ALK-TKI section.
Clinical studies have reported an ILD incidence of approximately 5% with capmatinib, with a mortality rate of around 0.5%. Affected patients typically present with dyspnea and radiologic findings characterized by bilateral ground-glass opacities. Discontinuation of the drug, combined with corticosteroid therapy, generally leads to clinical improvement.85 Moreover, case reports and small case series have suggested that transitioning to tepotinib after capmatinib-induced ILD may allow continued disease control without recurrence of ILD, indicating that tepotinib may exhibit a comparatively lower pulmonary risk profile.86
Tepotinib, a potent and highly selective MET inhibitor, also warrants close attention with regard to pulmonary safety. A real-world study from Japan reported an ILD incidence of 7.5% and a mortality rate of 2.7%, with a median onset of 56 days. The clinical and radiologic manifestations largely mirror those observed with capmatinib, including dyspnea and bilateral ground-glass opacities.51,87 While most patients experienced symptomatic improvement following drug discontinuation and corticosteroid therapy, several cases progressed to fatal outcomes, underscoring the need for vigilant monitoring during treatment.
The ILD profile of crizotinib, which also inhibits MET, has been comprehensively reviewed in the ALK-TKI section and will not be repeated here.
In summary, although ILD associated with MET-TKIs is relatively uncommon, it can lead to substantial pulmonary impairment when it occurs. Emerging evidence suggests that capmatinib and tepotinib may differ in their pulmonary risk profiles, potentially reflecting variations in molecular structure, kinase selectivity, and pulmonary tissue penetration. Current data are largely derived from clinical trials and limited real-world cohorts, with a lack of direct head-to-head comparisons or long-term follow-up. Future investigations should characterize toxicity risk across diverse patient populations—including older individuals and those with baseline lung disease—and incorporate pharmacokinetic, pharmacogenomic, and multi-omics approaches to develop predictive models. Such strategies will be essential for optimizing agent selection and enabling proactive mitigation of MET-TKI–associated ILD.
RET-TKIs
Rearranged during transfection (RET) gene fusions represent a rare but well-established oncogenic driver, occurring in approximately 1–2% of NSCLC cases.88 The development of selective RET inhibitors has markedly improved therapeutic options for patients with RET fusion–positive NSCLC. Selpercatinib and pralsetinib are two such agents that received approval from the U.S. Food and Drug Administration in 2020 for first-line treatment of metastatic disease, based on evidence demonstrating robust and durable clinical efficacy. These approvals have firmly established selective RET inhibition as a standard targeted therapeutic approach in RET fusion–positive NSCLC.
Selpercatinib, the first selective RET inhibitor approved for the treatment of unresectable or metastatic RET fusion–positive NSCLC, has been associated with only limited reports of ILD to date. In 2024, Hiroki et al described the first documented case of selpercatinib-induced DILD.52 Interestingly, the patient remained asymptomatic, yet imaging revealed bilateral ground-glass opacities indicative of subclinical pulmonary injury. These radiographic abnormalities gradually resolved following drug discontinuation, with no long-term sequelae. Although the true incidence of ILD associated with Selpercatinib remains unknown, this case underscores the importance of routine radiographic surveillance, even in the absence of overt respiratory symptoms.
Pralsetinib, another highly selective RET inhibitor approved for RET-rearranged NSCLC and several other solid tumors,89 has not been clearly associated with ILD in the NSCLC population to date. However, in patients with RET-mutated thyroid cancer, clinical studies have reported a pneumonia incidence of up to 10.7%.53 Although these observations arise from a different tumor context, they highlight the need for caution, particularly when treating individuals with underlying pulmonary comorbidities or those who may have increased susceptibility due to concurrent therapies. However, the current evidence base for RET inhibitor–associated ILD remains limited, particularly in NSCLC, and is largely derived from isolated case reports or indirect observations rather than dedicated pulmonary safety analyses. Accordingly, any comparison of ILD risk across RET inhibitors should be interpreted in the context of sparse data and the absence of robust head-to-head or long-term real-world evidence.
NTRK-TKIs
Neurotrophic tyrosine receptor kinase (NTRK) gene fusions represent a rare but well-established oncogenic driver event across diverse solid tumors, with a prevalence of less than 1% in NSCLC.90 Despite their rarity, the tumor-agnostic nature of NTRK fusions has led to the development of histology-independent targeted therapies. Three TRK inhibitors have received regulatory approval for NTRK fusion–positive malignancies: Larotrectinib, approved by the U.S. FDA in 2018 as the first tumor-agnostic targeted therapy; entrectinib, subsequently approved for metastatic NTRK fusion–positive solid tumors; and repotrectinib, a next-generation macrocyclic TKI with potent activity against TRK, ROS1, and ALK. As entrectinib and repotrectinib have been discussed extensively in the ROS1-TKI section, the current subsection will primarily focus on pulmonary safety data for Larotrectinib.
Larotrectinib, the first TRK-targeted agent approved for the treatment of NTRK fusion–positive tumors irrespective of tissue origin, has demonstrated favorable efficacy and tolerability across a broad range of cancer types.54 Clinical trials indicate a generally manageable safety profile, with approximately 8% of patients requiring dose reductions due to adverse events and only 2% discontinuing therapy permanently.55 To date, no definitive association has been reported between larotrectinib and ILD.56 However, given the rarity of NTRK fusion–positive NSCLC and the limited pulmonary safety data available from NSCLC-specific cohorts, the true ILD risk remains insufficiently characterized. Entrectinib and repotrectinib, both multi-targeted TKIs with activity against ROS1 and TRK fusions, have been discussed extensively in the ROS1-TKI section and will not be reiterated here.
Her2-Tki
Human epidermal growth factor receptor 2 (HER2) alterations, although relatively uncommon in non–small cell lung cancer (NSCLC), constitute a clinically actionable molecular subset and have stimulated the development of targeted therapeutic strategies. In contrast to antibody–drug conjugates, small-molecule HER2-targeted tyrosine kinase inhibitors (TKIs) represent a distinct treatment modality with a generally more favorable pulmonary safety profile.
Zongertinib is a highly selective, orally administered HER2-TKI developed for the treatment of HER2 tyrosine kinase domain (TKD)–mutant non-squamous NSCLC.91 The agent received accelerated approval from the U.S. Food and Drug Administration in August 2025 and has subsequently entered clinical practice, reflecting its demonstrated antitumor activity in this molecularly defined population.92
To date, no cases of interstitial lung disease (ILD) have been reported in publicly available clinical studies of zongertinib.58,59 Although the currently available data may suggest a low incidence of clinically apparent ILD, the evidence remains preliminary, and experience with other oncogene-directed TKIs indicates that drug-induced ILD may emerge with broader real-world exposure and longer follow-up. Continued post-marketing surveillance and longitudinal safety assessment will therefore be important for more fully characterizing the pulmonary risk profile of zongertinib as its clinical use expands.
KRAS G12C Inhibitors
KRAS G12C is the most prevalent KRAS alteration in NSCLC, occurring in approximately 13% of lung adenocarcinomas.93 The longstanding view of KRAS as an “undruggable” target has been overturned by the development of two selective KRAS G12C inhibitors that have now received regulatory approval. Sotorasib became the first KRAS G12C inhibitor approved by the U.S. FDA in 2021 for adults with KRAS G12C–mutated locally advanced or metastatic NSCLC who have received prior systemic therapy (2L+), followed by adagrasib, which received FDA approval in 2022 for the same previously treated KRAS G12C–mutated NSCLC population (2L+).94,95 These approvals represent a major milestone in the clinical targeting of KRAS-driven lung cancer and have broadened the therapeutic landscape for this historically difficult-to-treat molecular subset.
In a pooled safety analysis of 549 patients treated with sotorasib, the incidence of ILD or pneumonitis was 1.6%, including 0.2% of patients who experienced fatal ILD-related complications. The median time to onset was approximately 74 days after treatment initiation, and management strategies primarily involved dose reduction or permanent discontinuation of therapy.61
Adagrasib, another selective KRAS G12C inhibitor, has also received regulatory approval; however, available data regarding its ILD remain limited. In a cohort of 116 patients, 35.3% reported dyspnea, although none of these events were clinically confirmed as ILD. The most frequently observed adverse events included gastrointestinal symptoms and elevations in liver enzymes.62
In summary, KRAS G12C inhibitors appear to exhibit a pulmonary safety profile that differs in some respects from that of other targeted therapies. Sotorasib has been associated with a low but clinically meaningful incidence of ILD, including rare fatal cases, typically emerging weeks after treatment initiation, whereas adagrasib has not yet shown confirmed ILD despite a notable frequency of dyspnea. However, these observations should be interpreted in the context of differences in available study size, follow-up duration, and adverse event characterization across agents. The apparent divergence may reflect agent-specific pharmacologic properties rather than a uniform class-wide toxicity profile, although the current evidence remains insufficient for definitive comparison. Future efforts should focus on clarifying drug-specific patterns of lung injury and determining whether dyspnea observed with adagrasib reflects an early pulmonary signal or a non-pulmonary adverse event. Such insights may help refine expectations for each agent and support more tailored clinical decision-making in KRAS G12C–mutant NSCLC.
BRAF V600E-Targeted Therapies
BRAF is a serine/threonine kinase within the RAS–RAF–MEK–ERK signaling cascade, and the V600E substitution represents the most common activating BRAF mutation in NSCLC.96 Two BRAF/MEK inhibitor combinations are now FDA-approved for BRAF V600E–mutated metastatic NSCLC: dabrafenib plus trametinib (approved in 2017) and encorafenib plus binimetinib (approved in 2023). Both regimens are used as fixed combinations rather than monotherapies, as single-agent BRAF inhibition can trigger compensatory reactivation of MEK or upstream signaling, leading to rapid therapeutic resistance. The addition of a MEK inhibitor effectively suppresses downstream ERK activation and enhances antitumor efficacy.97
Dabrafenib plus trametinib represents the established therapeutic backbone for BRAF V600E–mutated NSCLC. Across multiple clinical trials, the combination has demonstrated a favorable safety profile, with no definitive association with ILD.63–65 Encorafenib plus binimetinib, approved for BRAF V600E–mutated solid tumors, is now being explored in NSCLC. To date, no ILD signals have been reported in published studies.66,67
Overall, current evidence indicates that BRAF/MEK inhibitor combinations confer a low incidence of ILD in BRAF V600E–mutated NSCLC. However, given the central role of the RAF–MEK–ERK axis in inflammatory regulation and stress signaling, rare or delayed-onset pulmonary events cannot be excluded. As combination strategies involving immunotherapy or radiotherapy become more common, understanding regimen-specific pulmonary interactions will be essential to ensuring safe clinical implementation.
VEGF Pathway Inhibitors
Angiogenesis is essential for tumor growth and progression, making the VEGF/VEGFR signaling axis an important therapeutic target in NSCLC. Two anti-angiogenic monoclonal antibodies, bevacizumab and ramucirumab, have received approval from the U.S. Food and Drug Administration. Bevacizumab is a monoclonal antibody targeting VEGF-A and was the first angiogenesis inhibitor approved for the treatment of non-squamous NSCLC. It is routinely administered in combination with carboplatin and paclitaxel as part of first-line therapy. Ramucirumab, which targets VEGFR-2, was approved in combination with docetaxel as second-line therapy in 2014 and later in combination with erlotinib in 2020 for first-line treatment of EGFR-mutated metastatic NSCLC. Both agents act through indirect antitumor mechanisms by inhibiting VEGF-mediated vascularization, and their therapeutic benefit relies largely on combination regimens rather than monotherapy.
With respect to ILD, bevacizumab has been associated with a low incidence of ILD. A meta-analysis of 7021 patients reported an overall ILD rate of 0.62%, with onset occurring from several weeks to more than one year after treatment initiation, highlighting the need for long-term monitoring.68 Typical presentations include dyspnea and diffuse ground-glass opacities; management consists of prompt drug withdrawal and corticosteroid therapy.69 Ramucirumab has not been definitively linked to ILD when used as monotherapy; however, in patients with a pre-existing history of ILD, the ramucirumab–docetaxel combination has been associated with recurrence rates of up to 25%,68 underscoring the importance of evaluating baseline lung status and exercising caution in high-risk individuals.
These findings suggest that perturbation of vascular signaling, particularly in the context of combination regimens and underlying lung vulnerability, may contribute to distinct patterns of lung injury. Accordingly, baseline pulmonary assessment and careful consideration of treatment context may be important when selecting anti-angiogenic therapies. Further studies are needed to clarify the vascular and inflammatory mechanisms involved and to improve risk stratification for patients receiving these agents.
ADCs
Antibody–drug conjugates (ADCs) represent a rapidly expanding class of targeted therapies for NSCLC. Structurally, ADCs consist of a monoclonal antibody linked to a highly potent cytotoxic payload through a cleavable linker, enabling antigen-specific delivery of chemotherapy to tumor cells while minimizing systemic exposure.98 Upon binding to tumor-associated antigens, ADCs undergo internalization and intracellular linker cleavage, releasing their cytotoxic payload and inducing targeted cell death.99
Several ADCs have recently entered clinical practice in NSCLC based on pivotal regulatory approvals.
Trastuzumab deruxtecan (T-DXd) received accelerated approval from the U.S. Food and Drug Administration in 2022 and conditional approval from the National Medical Products Administration for previously treated HER2-mutant NSCLC. In pivotal clinical studies, T-DXd was associated with an ILD incidence of up to 12%, markedly higher than that observed with most tyrosine kinase inhibitors. Clinically, dyspnea represents the most frequent presenting symptom, while radiologic findings typically include bilateral ground-glass opacities. Management generally requires immediate treatment discontinuation and prompt initiation of systemic corticosteroids.57 This disproportionately elevated risk highlights a likely ADC-specific mechanism of lung injury, emphasizing the importance of careful patient selection, early symptom recognition, and close radiographic surveillance.
Trastuzumab emtansine (T-DM1), another HER2-directed ADC widely used in HER2-positive breast cancer, remains approved only for that indication, with its application in NSCLC limited to exploratory studies. In a small cohort of 49 patients with NSCLC, ILD occurred in 6.7% of cases, with no fatal events reported,60 suggesting a comparatively more manageable pulmonary safety profile than that observed with T-DXd.
Amivantamab, a bispecific antibody targeting EGFR and MET with additional antibody-dependent cellular cytotoxicity (ADCC) activity, received FDA approval in 2024 in combination with carboplatin and pemetrexed as first-line therapy for locally advanced or metastatic NSCLC harboring EGFR exon 20 insertion mutations.71 Although its immune-modulating mechanism theoretically raises concern for inflammatory lung injury, no definitive cases of ADC-related ILD have been reported to date.
In contrast, Datopotamab deruxtecan (Dato-DXd), a TROP2-directed ADC bearing a deruxtecan topoisomerase-I inhibitor payload, was granted FDA accelerated approval in 2025 for patients with EGFR-mutated NSCLC previously treated with both EGFR-directed targeted therapy and platinum-based chemotherapy. Notably, clinical trial data show an ILD incidence of 8.8%, including 2.4% fatal cases,72 underscoring the critical need for stringent pulmonary monitoring.
Telisotuzumab vedotin, a c-MET–targeting ADC, received FDA accelerated approval in 2025 for second-line or later treatment of NSCLC with high c-MET protein overexpression. Among 49 treated patients, ILD occurred in 9%, including fatal events,73 suggesting a clinically relevant ILD signal despite molecular selectivity.
Patritumab deruxtecan (HER3-DXd), a HER3-directed ADC, had shown promising activity across HER3-expressing and EGFR-mutated NSCLC populations. However, following the failure of the Phase III trial to meet its OS endpoint, Merck voluntarily withdrew the BLA for HER3-DXd in May 2025, leaving the drug investigational with no current regulatory approval. Reported ILD incidence is approximately 7%, though no treatment-related deaths have been documented.74
In summary, ADCs have emerged as an important therapeutic class in NSCLC, extending targeted treatment beyond traditional kinase inhibition. However, their payload-dependent mechanisms appear to introduce a distinct and clinically significant risk of ILD, particularly with topoisomerase-I–based platforms such as deruxtecan. Compared with kinase inhibitors, ADC-associated ILD may in some cases present with more abrupt onset, more rapid deterioration, and a greater risk of fatal outcomes; however, these comparisons are influenced by heterogeneity in study design, patient populations, and ILD ascertainment across datasets. Agents including Dato-DXd, telisotuzumab vedotin, and HER3-DXd have shown variable but clinically relevant ILD signals, underscoring the importance of careful baseline assessment, close radiologic monitoring, and early intervention. Moving forward, further delineation of payload-specific toxicity mechanisms, refinement of risk prediction models, and integration of pharmacokinetic and immunogenomic profiling may help support the safer implementation of ADCs as their role continues to expand within precision oncology for NSCLC.
Mechanisms of Drug-Induced ILD
With the increasing use of targeted therapies in NSCLC, drug-induced interstitial lung disease (DILD) has emerged as a clinically significant toxicity that can limit treatment continuity and compromise patient outcomes. Although the pathogenic basis of DILD remains multifactorial and incompletely defined, accumulating evidence suggests that lung injury results from the convergence of three major mechanistic processes: inflammatory and immune-mediated responses, direct epithelial cytotoxicity including off-target effects, and host-related susceptibility factors.17,80,100–105 These mechanisms are not mutually exclusive and often interact to shape the overall risk and phenotype of lung injury. Table 2 summarizes the primary mechanistic pathways supported by current evidence, and Figure 3 provides a schematic representation of these molecular events across different drug classes.
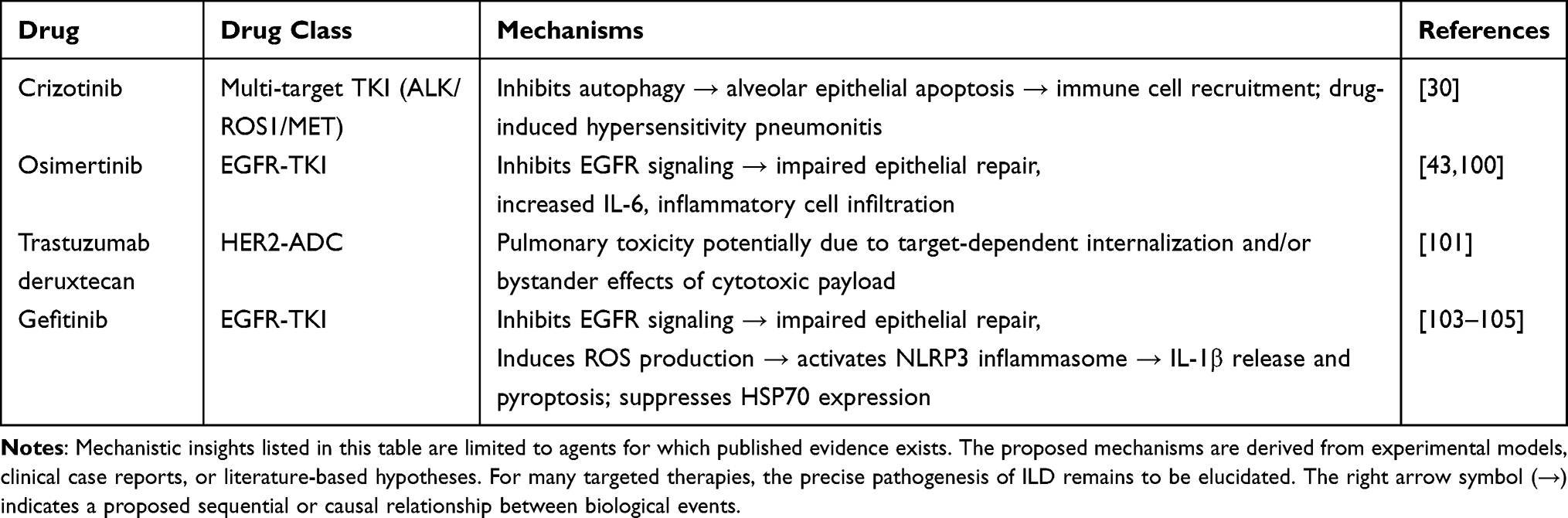 |
Table 2 Proposed Mechanisms of ILD Reported for Selected Targeted Agents in NSCLC |
 |
Figure 3 Schematic illustration of proposed molecular mechanisms underlying DILD in NSCLC. (A) Gefitinib-induced toxicity involves mitochondrial dysfunction and ROS accumulation, leading to DNA damage, PARP1 activation, and assembly of the NLRP3 inflammasome, which subsequently triggers IL-1β release and downstream inflammatory cascades. (B) Osimertinib inhibits EGFR phosphorylation, thereby disrupting epithelial homeostasis and enhancing IL-6/JAK/STAT3 signaling loops that sustain pro-inflammatory responses. (C) ADCs, exemplified by T-DXd, induce lung injury through a bystander effect. Following linker cleavage, DXd is released and taken up by adjacent normal alveolar cells, leading to DNA damage and apoptosis independent of target antigen expression. (D) Crizotinib blocks autophagy in alveolar cells, resulting in the accumulation of ROS and apoptotic bodies. This process stimulates CCL2 secretion, promotes macrophage recruitment and M1 polarization, and ultimately amplifies pulmonary tissue injury. Abbreviations: ROS, reactive oxygen species; NLRP3, NOD-like receptor protein 3; HMGB1, high-mobility group box 1; PARP1, poly (ADP-ribose) polymerase 1; JAK/STAT, Janus kinase/signal transducer and activator of transcription. |
Inflammatory and Immune-Mediated Injury
Several targeted agents appear to disrupt signaling pathways involved in maintaining alveolar epithelial integrity and immunologic homeostasis, thereby contributing to aberrant inflammatory activation. EGFR plays a central role in epithelial repair, barrier maintenance, and suppression of pro-inflammatory signaling. EGFR-TKIs such as gefitinib and osimertinib may impair these physiological functions, leading to epithelial vulnerability and excessive immune activation. Available evidence suggests that these agents can upregulate IL-6 and IL-1β, activate the NLRP3 inflammasome, and induce pyroptosis in alveolar macrophages, thereby contributing to diffuse inflammation and fibrotic remodeling (Figure 3A).100,103,104 Osimertinib may further suppress EGFR phosphorylation in damaged epithelium, potentially amplifying JAK/STAT3-mediated cytokine cascades and delaying epithelial regeneration (Figure 3B).41
Beyond EGFR-TKIs, inflammatory amplification plays a role in the toxicity of other agents. Crizotinib, through autophagy blockade, triggers apoptotic signaling that promotes chemokine release (eg, CCL2), macrophage recruitment, and M1-polarized inflammation (Figure 3D), contributing to a self-propagating cycle of epithelial injury.30 Collectively, these observations support a contributory role for dysregulated inflammatory signaling in DILD pathogenesis across multiple molecular classes, although the mechanistic evidence remains more mature for some agents than for others and is derived largely from preclinical models.
Direct Cytotoxicity and Off-Target Injury
A second major pathway may involve direct cellular injury that is not solely explained by the intended on-target effects of these agents. TKIs such as crizotinib have been reported to induce apoptosis in alveolar epithelial cells through disruption of autophagy, while gefitinib may reduce pulmonary HSP70 expression, impair oxidative stress defense, and facilitate mitochondrial ROS accumulation.103–105 These cytotoxic events are proposed to contribute to DNA damage, PARP1 activation, HMGB1 release, and subsequent tissue remodeling.
Antibody–drug conjugates (ADCs) may exhibit distinct ILD mechanisms because of the high potency of their cytotoxic payloads. Agents such as T-DXd have been proposed to induce lung injury through a bystander effect, whereby the payload is released extracellularly or taken up by non-tumor alveolar cells following linker cleavage (Figure 3C).74 This process may contribute to diffuse alveolar injury independent of HER2 or TROP2 expression and may partly explain the relatively high ILD incidence observed with deruxtecan-based ADCs.102
Collectively, these observations support a contributory role for direct cytotoxicity—including ROS accumulation, DNA damage, apoptosis, and payload diffusion—in DILD pathogenesis. However, the relative importance of these pathways likely differs across agents, and much of the current mechanistic evidence remains based on preclinical or translational studies rather than direct clinical validation.
Host-Related Susceptibility and Treatment Context
DILD does not arise solely from drug properties; host-related factors may substantially influence susceptibility. Structural lung abnormalities, pre-existing ILD, and reduced pulmonary reserve may prime the lung for exaggerated inflammatory or cytotoxic responses. Hypoalbuminemia (≤3.0 g/dL) has been proposed as a risk marker for gefitinib-induced ILD, possibly reflecting impaired drug distribution or systemic inflammation.41
Treatment history may also shape DILD susceptibility. Patients previously exposed to thoracic radiotherapy or immune checkpoint inhibitors may harbor latent lung inflammation or subclinical pneumonitis, which could increase vulnerability to subsequent injury from targeted agents. Rechallenge with TKIs after prior ILD episodes has been associated with an increased risk of recurrence, underscoring the importance of individualized risk assessment.24
In contrast, the mechanisms underlying MET inhibitor–associated ILD remain poorly defined. Although the HGF/MET axis is implicated in epithelial–mesenchymal transition and fibrotic regulation, current evidence does not convincingly link MET inhibition to ILD pathogenesis, suggesting that toxicity may be influenced more strongly by host- or treatment-related factors than by on-target effects.87
Collectively, current evidence suggests that DILD reflects the interaction of inflammatory dysregulation, direct cytotoxic injury, and host-specific vulnerabilities. EGFR-TKIs appear to impair epithelial repair and amplify inflammatory signaling; ADCs may induce payload-related cytotoxicity with bystander effects; and several agents have been linked to apoptosis or oxidative stress through off-target actions. However, the relative contribution of these pathways is unlikely to be uniform across drug classes, and much of the mechanistic evidence remains derived from preclinical studies or indirect clinical observations. A more refined understanding of these mechanisms may support the development of predictive models, improved risk stratification, and earlier intervention strategies in clinical practice. As the therapeutic landscape of NSCLC continues to evolve, deeper mechanistic insight into DILD may help improve the balance between antitumor efficacy and pulmonary safety.
Conclusion and Future Perspectives
The paradigm of NSCLC treatment has been revolutionized by targeted therapies, yet this progress is increasingly tempered by the emergence of drug-induced interstitial lung disease (DILD). As a clinically significant toxicity, DILD may interrupt treatment continuity, limit subsequent therapeutic options, and adversely affect patient outcomes, including survival in severe cases. However, direct comparative prognostic data in this setting remain limited. By comprehensively reviewing the pulmonary safety profiles across major drug classes—ranging from classical EGFR/ALK/ROS1 inhibitors to emerging ADCs and KRAS G12C inhibitors—this article highlights the heterogeneous patterns and mechanistic underpinnings of lung injury. These insights provide a critical foundation for refining risk stratification and optimizing individualized management.
At the same time, the available evidence remains heterogeneous across drug classes and study settings. Reported incidence, severity, and radiographic patterns are influenced by differences in study design, patient selection, ILD definitions, and adverse event ascertainment, while mechanistic understanding remains substantially more mature for some agents than for others. Accordingly, cross-class comparisons should be interpreted as a clinically informative framework rather than as direct head-to-head evidence.
Despite these advances, the pathogenesis of DILD remains a complex puzzle involving epithelial barrier disruption, immune dysregulation, and host susceptibility. The lack of validated biomarkers and standardized management algorithms continues to hinder early recognition and effective intervention.
Deciphering drug class–specific mechanisms of toxicity remains a central priority for advancing the understanding of DILD. Although pulmonary injury induced by TKIs has been relatively better characterized, the distinct toxicity profile associated with antibody–drug conjugates requires further investigation. Emerging multi-omics platforms, including lung organoids, single-cell RNA sequencing, and spatial transcriptomics, offer promising tools to dissect the interplay between payload-driven cytotoxicity, bystander effects, and immune microenvironment modulation.106–108
Parallel efforts should focus on the development of precision biomarkers and predictive models capable of identifying early lung injury. Integrative strategies combining circulating biomarkers, such as proteomic signatures, radiomic features derived from imaging, and AI-driven clinical–imaging algorithms may help detect subclinical pulmonary damage before irreversible injury occurs.109,110
Equally important is the implementation of patient-centered risk stratification frameworks. Future models should extend beyond conventional risk factors by incorporating genetic susceptibility, prior exposure to immunotherapy, and relevant comorbidities into dynamic, individualized risk assessment, thereby informing preventive strategies and more tailored treatment decisions.
Finally, robust real-world evidence is essential to validate mechanistic insights and predictive tools. Large-scale, multicenter longitudinal registries will be critical for defining the true incidence and clinical spectrum of DILD in unselected populations, beyond the restrictive eligibility criteria of clinical trials.
Collectively, these strategic directions outline a roadmap for transforming the clinical management of DILD. A stepwise conceptual framework summarizing existing challenges, priority research objectives, enabling technologies, and translational goals is presented in Figure 4, providing a structured foundation for future investigations. From a clinical perspective, careful baseline assessment, vigilant monitoring during treatment, and prompt evaluation of new respiratory symptoms or radiographic abnormalities remain central to minimizing severe outcomes and preserving treatment continuity. As precision oncology continues to advance, the integration of mechanistic insight with early detection and standardized intervention will be indispensable for balancing therapeutic efficacy with pulmonary safety and safeguarding long-term patient outcomes.
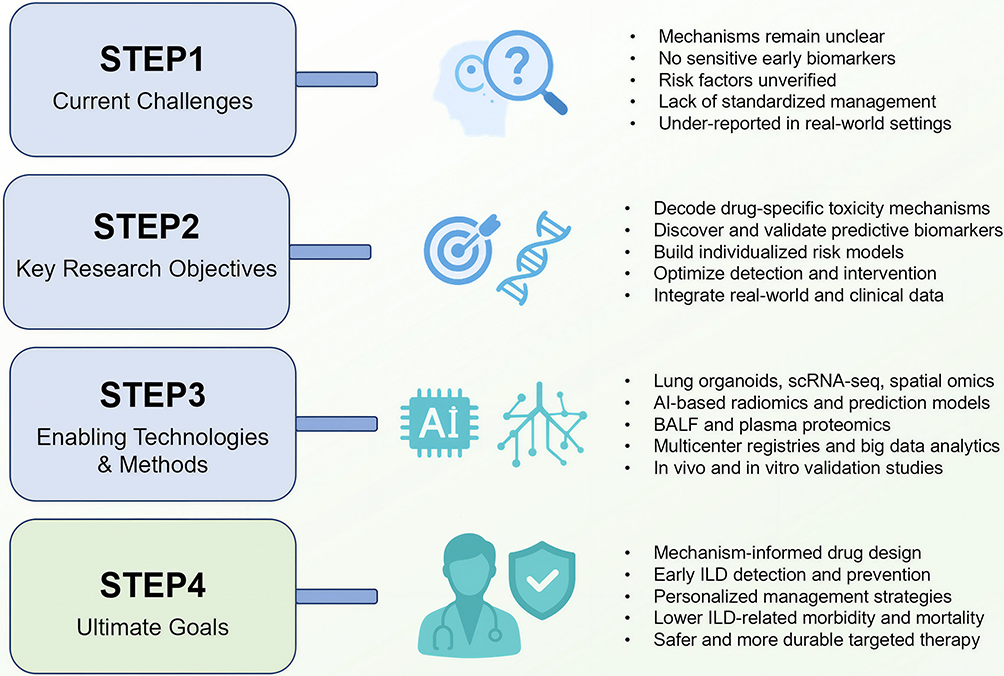 |
Figure 4 Strategic roadmap for advancing research and precision management of targeted therapy–DILD. This stepwise framework illustrates the progression from current clinical and mechanistic gaps (Step 1) to long-term translational goals in precision pulmonary safety (Step 4). Key research priorities (Step 2) include defining drug-specific injury pathways, identifying predictive biomarkers, and establishing risk-stratification strategies. These efforts are supported by enabling technologies (Step 3) such as patient-derived organoids, single-cell and spatial multi-omics, radiomics, and AI-driven predictive modeling. Together, these interconnected steps provide a structured pathway toward balancing therapeutic efficacy with optimized lung safety in the era of precision oncology. Bold step labels denote the four sequential conceptual stages in the proposed roadmap. |
Data Sharing Statement
No data and materials are available in the research described in the article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was financially supported by The Construction Fund of Key Medical Disciplines of Hangzhou (2025HZZD02) and the Key Laboratory of Clinical Cancer Pharmacology and Toxicology Research of Zhejiang Province (2020E10021).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca A Cancer J Clin. 2021;71(3):209–22. doi:10.3322/caac.21660
2. Guo L, Zhu C, Cai L, et al. Global burden of lung cancer in 2022 and projected burden in 2050. Chin Med J. 2024;137(21):2577–2582. doi:10.1097/CM9.0000000000003268
3. Hendriks LEL, Remon J, Faivre-Finn C, et al. Non-small-cell lung cancer. Nat Rev Dis Primers. 2024;10(1):71. doi:10.1038/s41572-024-00551-9
4. Obeng-Nyarkoh PI, Valentin-Figueroa ME, Cadham CJ, et al. Lung cancer risk in US adults with COPD: a systematic review and meta-analysis. Int J Chronic Obstr. 2025;20:3399–3421. doi:10.2147/COPD.S531972
5. Ettinger DS, Wood DE, Aisner DL, et al. Non-small cell lung cancer, version 3.2022, NCCN clinical practice guidelines in oncology. J Nat Comprehensive Cancer Network. 2022;20(5):497–530. doi:10.6004/jnccn.2022.0025
6. Jeon H, Wang S, Song J, Gill H, Cheng H. Update 2025: management of non‑small cell lung cancer. Lung. 2025;203(1):53. doi:10.1007/s00408-025-00801-x
7. Planchard D, Jänne PA, Cheng Y, et al; FLAURA2 Investigators. Osimertinib with or without chemotherapy in EGFR-mutated advanced NSCLC. New Engl J Med. 2023;389(21):1935–1948. doi:10.1056/NEJMoa2306434
8. Gautschi O, Park K, Solomon BJ, et al. Selpercatinib in RET fusion-positive non-small cell lung cancer: final safety and efficacy, including overall survival, from the LIBRETTO-001 phase I/II trial. J Clin Oncol. 2025;43(15):1758–1764. doi:10.1200/JCO-24-02076
9. Velimirovic M, Brignola M, Chheng E, Smith M, Hassan KA. Management of pulmonary toxicities associated with systemic therapy in non small cell lung cancer. Current Treatment Options Oncol. 2024;25(10):1297–1311. doi:10.1007/s11864-024-01257-6
10. M MT. Interstitial lung disease: a review. JAMA. 2024;331(19):1655–1665. doi:10.1001/jama.2024.3669
11. Ohmori T, Yamaoka T, Ando K, et al. Molecular and clinical features of EGFR-TKI-associated lung injury. Int J Mol Sci. 2021;22(2):792. doi:10.3390/ijms22020792
12. Dong J, Li L, Deng T, Song H, Zhang S, Zhong M. Interstitial lung disease associated with ALK inhibitors and risk factors: an updated comparative pharmacovigilance analysis. Front Pharmacol. 2024;15:1361443. doi:10.3389/fphar.2024.1361443
13. Katakami N, Yokoyama T, Morita S, et al. Overall survival analysis of patients enrolled in a randomized phase III trial comparing gefitinib and erlotinib for previously treated advanced lung adenocarcinoma (WJOG5108LFS). Int J Clin Oncol. 2023;28(1):79–88. doi:10.1007/s10147-022-02266-x
14. Soria JC, Ohe Y, Vansteenkiste J, et al; FLAURA Investigators. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. New Engl J Med. 2018;378(2):113–125. doi:10.1056/NEJMoa1713137
15. Ramalingam SS, Vansteenkiste J, Planchard D, et al; FLAURA Investigators. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. New Engl J Med. 2020;382(1):41–50. doi:10.1056/NEJMoa1913662
16. Mok T, Camidge DR, Gadgeel SM, et al. Updated overall survival and final progression-free survival data for patients with treatment-naive advanced ALK-positive non-small-cell lung cancer in the ALEX study. Annals Oncol. 2020;31(8):1056–1064. doi:10.1016/j.annonc.2020.04.478
17. Camidge DR, Kim HR, Ahn MJ, et al. Brigatinib versus crizotinib in ALK-positive non-small-cell lung cancer. New Engl J Med. 2018;379(21):2027–2039. doi:10.1056/NEJMoa1810171
18. Solomon BJ, Liu G, Felip E, et al. Lorlatinib versus crizotinib in patients with advanced ALK-positive non-small cell lung cancer: 5-year outcomes from the phase III CROWN study. J Clin Oncol. 2024;42(29):3400–3409. doi:10.1200/JCO.24.00581
19. Wolf J, Seto T, Han JY, et al; GEOMETRY mono-1 Investigators. Capmatinib in MET exon 14-mutated or MET-amplified non-small-cell lung cancer. New Engl J Med. 2020;383(10):944–957. doi:10.1056/NEJMoa2002787
20. Paik PK, Felip E, Veillon R, et al. Tepotinib in non-small-cell lung cancer with MET Exon 14 skipping mutations. New Engl J Med. 2020;383(10):931–943. doi:10.1056/NEJMoa2004407
21. Drilon A, Subbiah V, Gautschi O, et al. Selpercatinib in patients with RET fusion-positive non-small-cell lung cancer: updated safety and efficacy from the registrational LIBRETTO-001 phase I/II trial. J Clin Oncol. 2023;41(2):385–394. doi:10.1200/JCO.22.00393
22. Griesinger F, Curigliano G, Thomas M, et al. Safety and efficacy of pralsetinib in RET fusion-positive non-small-cell lung cancer including as first-line therapy: update from the ARROW trial. Annals Oncol. 2022;33(11):1168–1178. doi:10.1016/j.annonc.2022.08.002
23. de Langen AJ, Johnson ML, Mazieres J, et al; CodeBreaK 200 Investigators. Sotorasib versus docetaxel for previously treated non-small-cell lung cancer with KRASG12C mutation: a randomised, open-label, Phase 3 trial. Lancet. 2023;401(10378):733–746. doi:10.1016/S0140-6736(23)00221-0
24. Pruis MA, Veerman GDM, Hassing HC, et al. Cardiac toxicity of alectinib in patients with ALK+ lung cancer: outcomes of cardio-oncology follow-up. JACC Cardio Oncol. 2023;5(1):102–113. doi:10.1016/j.jaccao.2022.09.006
25. Kashizaki F, Chen H, Miyasaka A, et al. Safety of readministration of EGFR-TKI after onset of interstitial lung disease in advanced EGFR-mutated NSCLC: a systematic review and meta-analysis. Clin Lung Cancer. 2024;25(1):e52–e57e2. doi:10.1016/j.cllc.2023.09.009
26. Kanaji N, Ichihara E, Tanaka T, et al. Efficacy and safety of re-administration of epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKI) after EGFR-TKI-induced interstitial lung disease (CS-Lung-005). Lung. 2024;202(1):63–72. doi:10.1007/s00408-023-00669-9
27. Gemma A, Kusumoto M, Kurihara Y, et al. Interstitial lung disease onset and its risk factors in japanese patients with ALK-positive NSCLC after treatment with crizotinib. J Thoracic Oncol. 2019;14(4):672–682. doi:10.1016/j.jtho.2018.11.022
28. Zhou C, Deng H, Yang Y, et al. Cancer therapy-related interstitial lung disease. Chin Med J. 2025;138(3):264–277. doi:10.1097/CM9.0000000000003149
29. Wei FF, Zhang J, Jia Z, Yao ZC, Chen CQ. Furmonertinib re-challenge for epidermal growth factor receptor-mutant lung adenocarcinoma after osimertinib-induced interstitial lung disease: a case report. World J Clin Oncol. 2025;16(3):101766. doi:10.5306/wjco.v16.i3.101766
30. Zhang Y, Gao Z, Pan Z, et al. Crizotinib induces ILD by blocking autophagy flux in alveolar epithelial cells. Biochem Pharmacol. 2023;215:115636. doi:10.1016/j.bcp.2023.115636
31. Zhao M, Liu S, Xie R, Zhang J, Li J. Interstitial lung disease risk of anaplastic lymphoma kinase tyrosine kinase inhibitor treatment of non-small cell lung cancer: a real-world pharmacovigilance study. Expert Opin Drug Saf. 2023;22(12):1309–1316. doi:10.1080/14740338.2023.2245324
32. Ahn MJ, Cho BC, Ou X, et al. Osimertinib plus durvalumab in patients with EGFR-mutated, advanced NSCLC: a Phase 1b, open-label, multicenter trial. J Thoracic Oncol. 2022;17(5):718–723.
33. Shi J, Liu X, Wu L, Jiang Y, Zhang Y, Wang Y. Interstitial lung disease with antibody-drug conjugates: a real-world pharmacovigilance study based on the FAERS database during the period 2014-2023. Therapeut Adv Resp Dis. 2024;18:17534666241299935. doi:10.1177/17534666241299935
34. Sousa FE, Campainha M, Marques S, et al. Diagnosis and management of drug-induced interstitial lung disease in the context of anti-cancer therapy: a multidisciplinary viewpoint by portuguese experts. Clin Drug Invest. 2024;44(11):801–810. doi:10.1007/s40261-024-01400-z
35. Fujiwara Y, Shimomura K, Yamaguchi T, et al. The incidence of drug-induced interstitial lung disease caused by epidermal growth factor receptor tyrosine kinase inhibitors or immune checkpoint inhibitors in patients with non-small cell lung cancer in presence and absence of vascular endothelial growth factor inhibitors: a systematic review. Front Oncol. 2024;14:1419256. doi:10.3389/fonc.2024.1419256
36. Beom SH, Kim DW, Sim SH, et al. Gefitinib-induced interstitial lung disease in korean lung cancer patients. Cancer Res Treat. 2016;48(1):88–97. doi:10.4143/crt.2014.201
37. Miao X, Liu Y, Li X, Zhao R. Risk of interstitial lung disease in non-small cell lung cancer treated with EGFR-TKI: a real-world pharmacovigilance study. Front Pharmacol. 2025;16:1652750. doi:10.3389/fphar.2025.1652750
38. Li N, Ou W, Cheng C, et al. Adjuvant icotinib for resected EGFR-mutated stage II-IIIA non-small-cell lung cancer (ICTAN, GASTO1002): a randomized comparison study. Signal Transduction Targeted Ther. 2025;10(1):273. doi:10.1038/s41392-025-02358-w
39. Tamura K, Nukiwa T, Gemma A, et al. Real-world treatment of over 1600 Japanese patients with EGFR mutation-positive non-small cell lung cancer with daily Afatinib. Int J Clin Oncol. 2019;24(8):917–926. doi:10.1007/s10147-019-01439-5
40. Gemma A, Kusumoto M, Sakai F, et al. Real-world evaluation of factors for interstitial lung disease incidence and radiologic characteristics in patients with EGFR T790M-positive NSCLC treated with osimertinib in Japan. J Thoracic Oncol. 2020;15(12):1893–1906. doi:10.1016/j.jtho.2020.08.025
41. Zhou Q, Hu Z, Li X, Tang X. Almonertinib-induced interstitial lung disease in a lung adenocarcinoma patient complicated with interstitial lung abnormality. BMC Pulm Med. 2023;23(1):79. doi:10.1186/s12890-023-02367-x
42. Ryu WK, Cha H, Park MH, et al. Efficacy of crizotinib retreatment after crizotinib-related interstitial lung disease in a patient with ROS1-rearranged advanced lung adenocarcinoma: a case report and potential crizotinib retreatment strategy. Front Oncol. 2022;12:900966. doi:10.3389/fonc.2022.900966
43. Sato J, Uchida M, Wakabayashi H, Shimizu T. Evaluation of lung toxicity related to the treatment with alectinib using a pharmacovigilance database. Anticancer Res. 2022;42(6):3109–3116. doi:10.21873/anticanres.15799
44. Hida T, Nokihara H, Kondo M, et al. Alectinib versus crizotinib in patients with ALK-positive non-small-cell lung cancer (J-ALEX): an open-label, randomised phase 3 trial. Lancet. 2017;390(10089):29–39. doi:10.1016/S0140-6736(17)30565-2
45. Gettinger SN, Bazhenova LA, Langer CJ, et al. Activity and safety of brigatinib in ALK-rearranged non-small-cell lung cancer and other malignancies: a single-arm, open-label, phase 1/2 trial. Lancet Oncol. 2016;17(12):1683–1696. doi:10.1016/S1470-2045(16)30392-8
46. Drilon A, Siena S, Dziadziuszko R, et al; trial investigators. Entrectinib in ROS1 fusion-positive non-small-cell lung cancer: integrated analysis of three phase 1-2 trials. Lancet Oncol. 2020;21(2):261–270. doi:10.1016/S1470-2045(19)30690-4
47. Ou SI, Solomon BJ, Besse B, et al. Final overall survival and long-term safety of lorlatinib in patients with ALK-positive NSCLC from the pivotal Phase 2 study: a brief report. J Thoracic Oncol. 2025;20(4):513–520. doi:10.1016/j.jtho.2024.11.021
48. Desilets A, Repetto M, Drilon A. Repotrectinib: redefining the therapeutic landscape for patients with ROS1 fusion-driven non-small cell lung cancer. Clin Transl Med. 2024;14(10):e70017. doi:10.1002/ctm2.70017
49. Li W, Xiong A, Yang N, et al. Efficacy and safety of taletrectinib in Chinese patients with ROS1+ non-small cell lung cancer: The Phase II TRUST-I study. J Clin Oncol. 2024;42(22):2660–2670. doi:10.1200/JCO.24.00731
50. Riedel R, Fassunke J, Scheel AH, et al. MET fusions in NSCLC: clinicopathologic features and response to MET inhibition. J Thoracic Oncol. 2024;19(1):160–165. doi:10.1016/j.jtho.2023.06.020
51. Kato T, Ogura T, Sato M, et al. Safety and effectiveness of tepotinib in patients with unresectable, advanced or recurrent non-small cell lung cancer with METex14 skipping alterations: post-marketing surveillance in Japan. Japan J Clin Oncol. 2025;hyaf099. doi:10.1093/jjco/hyaf099
52. Zhang J, Qiu T, Zhou Y, Wu S, Chen E. Tyrosine kinase inhibitors-associated interstitial lung disease used in non-small cell lung cancer: a pharmacovigilance analysis based on the FDA adverse event reporting system database. Expert Opin Drug Saf. 2023;22(9):849–856. doi:10.1080/14740338.2023.2193392
53. Zheng X, Fang M, Fan Y, et al. Efficacy and safety of pralsetinib in Chinese advanced RET-mutant medullary thyroid cancer patients. Endocrine-Related Cancer. 2024;31(4):e230134. doi:10.1530/ERC-23-0134
54. Drilon A, Tan DSW, Lassen UN, et al. Efficacy and safety of larotrectinib in patients with tropomyosin receptor kinase fusion-positive lung cancers. JCO Precis Oncol. 2022;6:e2100418.
55. Hong DS, DuBois SG, Kummar S, et al. Larotrectinib in patients with TRK fusion-positive solid tumours: a pooled analysis of three phase 1/2 clinical trials. Lancet Oncol. 2020;21(4):531–540. doi:10.1016/S1470-2045(19)30856-3
56. Liguori V, Gaio M, Zinzi A, et al. The safety profiles of two first-generation NTRK inhibitors: analysis of individual case safety reports from the FDA adverse event reporting system (FAERS) database. Biomedicines. 2023;11(9):2538. doi:10.3390/biomedicines11092538
57. Smit EF, Felip E, Uprety D, et al. Trastuzumab deruxtecan in patients with metastatic non-small-cell lung cancer (DESTINY-Lung01): primary results of the HER2-overexpressing cohorts from a single-arm, phase 2 trial. Lancet Oncol. 2024;25(4):439–454. doi:10.1016/S1470-2045(24)00064-0
58. Heymach JV, Opdam F, Barve M, et al. HER2-selective tyrosine kinase inhibitor, zongertinib (BI 1810631), in patients with advanced/metastatic solid tumors with HER2 alterations: a phase ia dose-escalation study. J Clin Oncol. 2025;43(11):1337–1347. doi:10.1200/JCO-24-01727
59. Illini O, Lang-Stöberl AS, Fabikan H, Weinlinger C, Valipour A, Hochmair MJ. Very first real-world data on zongertinib use in non-small cell lung cancer patients with HER2 mutations: a brief report. Cancer Treatment Res Commun. 2024;42:100875. doi:10.1016/j.ctarc.2025.100875
60. Peters S, Stahel R, Bubendorf L, et al. Trastuzumab Emtansine (T-DM1) in patients with previously treated HER2-overexpressing metastatic non-small cell lung cancer: efficacy, safety, and biomarkers. Clin Cancer Res. 2019;25(1):64–72. doi:10.1158/1078-0432.CCR-18-1590
61. Skoulidis F, Li BT, Hochmair M, et al. Pooled safety analysis and management of sotorasib-related adverse events in KRAS G12C-mutated advanced non-small cell lung cancer. Oncologist. 2025;30(1):oyae356. doi:10.1093/oncolo/oyae356
62. Jänne PA, Riely GJ, Gadgeel SM, et al. Adagrasib in non-small-cell lung cancer harboring a KRASG12C mutation. New Engl J Med. 2022;387(2):120–131. doi:10.1056/NEJMoa2204619
63. Weng CD, Liu KJ, Jin S, et al. Triple-targeted therapy of dabrafenib, trametinib, and osimertinib for the treatment of the acquired BRAF V600E mutation after progression on EGFR-tyrosine kinase inhibitors in advanced EGFR-mutated non-small cell lung cancer patients. Transl Lung Cancer Res. 2024;13(10):2538–2548. doi:10.21037/tlcr-24-358
64. Fan Y, Zhou J, Zhao Y, et al. Efficacy, safety, and quality of life of dabrafenib plus trametinib treatment in Chinese patients with BRAFV600E mutation-positive metastatic non-small cell lung cancer. Transl Lung Cancer Res. 2024;13(12):3382–3391. doi:10.21037/tlcr-24-494
65. Yang W, Feng X, Ni J, et al. EGFR inhibitors plus dabrafenib and trametinib in patients with EGFR-mutant lung cancer and resistance mediated by BRAFV600E mutation: a multi-center real-world experience in China. Transl Lung Cancer Res. 2024;13(12):3500–3512. doi:10.21037/tlcr-24-803
66. Baik C, Cheng ML, Dietrich M, Gray JE, Karim NA. A practical review of encorafenib and binimetinib therapy management in patients with BRAF V600E-mutant metastatic non-small cell lung cancer. Adv ther. 2024;41(7):2586–2605. doi:10.1007/s12325-024-02839-4
67. Riely GJ, Ahn MJ, Clarke JM, et al. Updated efficacy and safety from the phase 2 PHAROS study of encorafenib Plus Binimetinib in patients with BRAF V600E-mutant metastatic NSCLC-A brief report. J Thoracic Oncol. 2025;S1556-0864(25):753. doi:10.1016/j.jtho.2025.05.023.
68. Nozawa K, Takatsuka D, Endo Y, et al. Association between bevacizumab with cancer drug therapies and drug-induced interstitial lung disease in patients with solid tumor: a systematic review and meta-analysis of randomized clinical trials. Crit Rev Oncol/Hematol. 2022;174:103703. doi:10.1016/j.critrevonc.2022.103703
69. Kanbayashi Y, Uchida M, Kashiwagi M, Akiba H, Shimizu T. Evaluation of lung toxicity with bevacizumab using the spontaneous reporting database. Sci Rep. 2022;12(1):15619. doi:10.1038/s41598-022-19887-x
70. Ebi N, Inoue H, Fujimoto Y, et al. Impact of docetaxel plus ramucirumab therapy on interstitial lung disease in recurrent advanced non-small cell lung cancer patients. Transl Lung Cancer Res. 2024;13(10):2573–2584. doi:10.21037/tlcr-24-460
71. Krebs MG, Cho BC, Hiret S, et al. Amivantamab in participants with advanced NSCLC and MET exon 14 skipping mutations: final results from the CHRYSALIS study. J Thoracic Oncol. 2025;S1556-0864(25):720–728. doi:10.1016/j.jtho.2025.05.012 Advance online publication.
72. Ahn MJ, Tanaka K, Paz-Ares L, et al; TROPION-Lung01 Trial Investigators. Datopotamab deruxtecan versus docetaxel for previously treated advanced or metastatic non-small cell lung cancer: the randomized, open-label Phase III TROPION-Lung01 study. J Clin Oncol. 2025;43(3):260–272. doi:10.1200/JCO-24-01544
73. Waqar SN, Redman MW, Arnold SM, et al. A Phase II study of telisotuzumab vedotin in patients with c-MET-positive Stage IV or recurrent squamous cell lung cancer (LUNG-MAP Sub-study S1400K, NCT03574753). Clin Lung Cancer. 2021;22(3):170–177. doi:10.1016/j.cllc.2020.09.013
74. Yu HA, Yang JC, Hayashi H, et al. HERTHENA-Lung01: a phase II study of patritumab deruxtecan (HER3-DXd) in previously treated metastatic EGFR-mutated NSCLC. Future Oncol. 2023;19(19):1319–1329. doi:10.2217/fon-2022-1250
75. U.S. Food and Drug Administration. Drugs@FDA: FDA Approved Drug Products. Available from: https://www.accessdata.fda.gov/scripts/cder/daf/.
76. National Medical Products Administration (NMPA). Drug Approval Database. Available from: https://www.nmpa.gov.cn/datasearch/.
77. Sato J, Sadachi R, Koyama T, Katsuya Y, Okada M, Yamamoto N. Regional diversity in drug-induced lung diseases among the USA, European Union, and Japan. Front Med. 2024;11:1390083. doi:10.3389/fmed.2024.1390083
78. Enomoto N. Pathological roles of pulmonary cells in acute lung injury: lessons from clinical practice. Int J Mol Sci. 2022;23(23):15027. doi:10.3390/ijms232315027
79. Kodama H, Wakuda K, Yabe M, et al. Retrospective analysis of osimertinib re-challenge after osimertinib-induced interstitial lung disease in patients with EGFR-mutant non-small cell lung carcinoma. Invest New Drugs. 2021;39(2):571–577. doi:10.1007/s10637-020-01005-1
80. Vaz VR, Gandhi MM, Ricciuti B, et al. Response to crizotinib after entrectinib resistance in ROS1-rearranged, MET-amplified lung adenocarcinoma. JCO Precis Oncol. 2024;8:e2400394. doi:10.1200/PO-24-00394
81. Hotta T, Okimoto T, Hamaguchi M, Tsubata Y, Isobe T. Acute interstitial lung disease induced by rechallenge with ceritinib. Internal Med. 2020;59(2):253–256. doi:10.2169/internalmedicine.2597-18
82. Fletcher JA, Mullally WJ, Ladwa R, O’Byrne KJ. Lorlatinib after alectinib-induced pneumonitis: a case report. JTO Clin Res Rep. 2023;5(2):100591. doi:10.1016/j.jtocrr.2023.100591
83. Drilon A, Jenkins C, Iyer S, Schoenfeld A, Keddy C, Davare MA. ROS1-dependent cancers - biology, diagnostics and therapeutics. Nat Rev Clin Oncol. 2021;18(1):35–55. doi:10.1038/s41571-020-0408-9
84. Tanimura M, Kataoka N, Kunimatsu Y, et al. Entrectinib for ROS1-rearranged non-small cell lung cancer after crizotinib-induced interstitial lung disease: a case report. Respirol Case Rep. 2021;9(11):e0857. doi:10.1002/rcr2.857
85. Wolf J, Hochmair M, Han JY, et al. Capmatinib in MET exon 14-mutated non-small-cell lung cancer: final results from the open-label, phase 2 GEOMETRY mono-1 trial. Lancet Oncol. 2024;25(10):1357–1370. doi:10.1016/S1470-2045(24)00441-8
86. Tseng LW, Chang JW, Wu CE. Safety of tepotinib challenge after capmatinib-induced pneumonitis in a patient with non-small cell lung cancer harboring MET Exon 14 skipping mutation: a case report. Int J Mol Sci. 2022;23(19):11809. doi:10.3390/ijms231911809
87. Hashiguchi MH, Sato T, Yamamoto H, et al. Successful tepotinib challenge after capmatinib-induced interstitial lung disease in a patient with lung adenocarcinoma harboring MET exon 14 skipping mutation: case report. JTO Clin Res Rep. 2021;3(2):100271. doi:10.1016/j.jtocrr.2021.100271
88. Drilon A, Hu ZI, Lai GGY, Tan DSW. Targeting RET-driven cancers: lessons from evolving preclinical and clinical landscapes. Nat Rev Clin Oncol. 2018;15(3):151–167. doi:10.1038/nrclinonc.2017.175
89. Liao D, Long M, Zhang J, et al. Efficacy and safety of pralsetinib in patients with RET fusion positive non-small cell lung cancer: an observational real world study. Lung Cancer. 2024;196:107936. doi:10.1016/j.lungcan.2024.107936
90. Liu F, Wei Y, Zhang H, Jiang J, Zhang P, Chu Q. NTRK fusion in non-small cell lung cancer: diagnosis, therapy, and TRK inhibitor resistance. Front Oncol. 2022;12:864666. doi:10.3389/fonc.2022.864666
91. Hoe HJ, Solomon BJ. optimizing dosing of trastuzumab deruxtecan in HER2-mutant non-small-cell lung cancer: a reminder that more is not always better. J Clin Oncol. 2023;41(31):4849–4851. doi:10.1200/JCO.23.01768
92. Brazel D, Park CJ, Nagasaka M. The development of Zongertinib for HER2-mutant NSCLC. Crit Rev Oncol/Hematol. 2025;104896. Advance online publication. doi:10.1016/j.critrevonc.2025.104896
93. Isermann T, Sers C, Der CJ, Papke B. KRAS inhibitors: resistance drivers and combinatorial strategies. Trends Cancer. 2025;11(2):91–116. doi:10.1016/j.trecan.2024.11.009
94. Nakajima EC, Drezner N, Li X, et al. FDA approval summary: sotorasib for KRAS G12C-mutated metastatic NSCLC. Clin Cancer Res. 2022;28(8):1482–1486. doi:10.1158/1078-0432.CCR-21-3074
95. Barlesi F, Yao W, Duruisseaux M, et al; KRYSTAL-12 Investigators. Adagrasib versus docetaxel in KRASG12C-mutated non-small-cell lung cancer (KRYSTAL-12): a randomised, open-label, phase 3 trial. Lancet. 2025;406(10503):615–626. doi:10.1016/S0140-6736(25)00866-9
96. Chmielecki J, Mok T, Wu YL, et al. Analysis of acquired resistance mechanisms to osimertinib in patients with EGFR-mutated advanced non-small cell lung cancer from the AURA3 trial. Nat Commun. 2023;14(1):1071. doi:10.1038/s41467-023-35962-x
97. Subbiah V, Baik C, Kirkwood JM. Clinical development of BRAF plus MEK inhibitor combinations. Trends Cancer. 2020;6(9):797–810. doi:10.1016/j.trecan.2020.05.009
98. Zhao C, Zhang R, Yang H, Gao Y, Zou Y, Zhang X. Antibody-drug conjugates for non-small cell lung cancer: advantages and challenges in clinical translation. Biochem Pharmacol. 2024;226:116378. doi:10.1016/j.bcp.2024.116378
99. Filis P, Zerdes I, Soumala T, Matikas A, Foukakis T. The ever-expanding landscape of antibody-drug conjugates (ADCs) in solid tumors: a systematic review. Crit Rev Oncol/Hematol. 2023;192:104189. doi:10.1016/j.critrevonc.2023.104189
100. Li Y, Chen Y, Meng Y, Shen M, Yang F, Ren X. Osimertinib exacerbates immune checkpoint inhibitor-related severe adverse events by activating the IL-6/JAK/STAT3 pathway in macrophages. Cancer Biol Med. 2024;21(12):1156–1170. doi:10.20892/j.issn.2095-3941.2024.0269
101. Kumagai K, Aida T, Tsuchiya Y, Kishino Y, Kai K, Mori K. Interstitial pneumonitis related to trastuzumab deruxtecan, a human epidermal growth factor receptor 2-targeting Ab-drug conjugate, in monkeys. Cancer Sci. 2020;111(12):4636–4645. doi:10.1111/cas.14686
102. Swain SM, Nishino M, Lancaster LH, et al. Multidisciplinary clinical guidance on trastuzumab deruxtecan (T-DXd)-related interstitial lung disease/pneumonitis-Focus on proactive monitoring, diagnosis, and management. Cancer Treat Rev. 2022;106:102378. doi:10.1016/j.ctrv.2022.102378
103. Noguchi T, Sekiguchi Y, Kudoh Y, et al. Gefitinib initiates sterile inflammation by promoting IL-1β and HMGB1 release via two distinct mechanisms. Cell Death Dis. 2021;12(1):49. doi:10.1038/s41419-020-03335-7
104. Kagi T, Noguchi T, Matsuzawa A. Mechanisms of gefitinib-induced interstitial pneumonitis: why and how the TKI perturbs innate immune systems? Oncotarget. 2021;12(13):1321–1322. doi:10.18632/oncotarget.27958
105. Colunga Biancatelli RML, Solopov PA, Day T, et al. HSP70 is a critical regulator of HSP90 inhibitor’s effectiveness in preventing HCL-induced chronic lung injury and pulmonary fibrosis. Int J Mol Sci. 2024;25(3):1920. doi:10.3390/ijms25031920
106. Ma J, Li S, Zhang X, et al. Lung cancer organoids in translational research: bridging basic science, drug development, and clinical therapeutics. Crit Rev Oncol/Hematol. 2025;214:104840. doi:10.1016/j.critrevonc.2025.104840 Advance online publication.
107. Kim GD, Shin SI, Sun P, et al. Single-cell RNA sequencing of baseline PBMCs predicts ICI efficacy and irAE severity in patients with NSCLC. J ImmunoTher Cancer. 2025;13(5):e011636. doi:10.1136/jitc-2025-011636
108. Cao K, Wei S, Ma T, et al. Integrating bulk, single-cell, and spatial transcriptomics to identify and functionally validate novel targets to enhance immunotherapy in NSCLC. NPJ Precision Oncol. 2025;9(1):112. doi:10.1038/s41698-025-00893-x
109. Grinshpun A, Zick A, Perri T, et al. Detection of antibody-drug conjugate-induced interstitial lung disease using circulating cell-free DNA. ESMO Open. 2024;9(10):103715. doi:10.1016/j.esmoop.2024.103715
110. Mei X, Liu Z, Singh A, et al. Interstitial lung disease diagnosis and prognosis using an AI system integrating longitudinal data. Nat Commun. 2023;14(1):2272. doi:10.1038/s41467-023-37720-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Long Overdue Targeted Treatment for KRAS Mutations in NSCLC: Spotlight on Adagrasib
Brazel D, Arter Z, Nagasaka M
Lung Cancer: Targets and Therapy 2022, 13:75-80
Published Date: 10 November 2022
The Path to Personalized Treatment in KRAS-Mutant Non-Small Cell Lung Cancer: A Review of Targeted Therapies and Immunotherapy
Shu CL, Liu YL
Cancer Management and Research 2022, 14:3485-3492
Published Date: 16 December 2022
Comparative Cost Analysis for Direct Medical Costs of Protocol Administration of Non-Small Cell Lung Cancer Treatment Regimens in Curative Intent: A Micro-Costing Study in Jordan
Madae’en SS, Salem AA, Ararawi NS, Ramzi EJ, Aloueedat RF, Saabenh AM, Allouzi DA, Abuoudeh RH, Hnaif OE, Musa LM, Alshdaifat SH, Al-Tanashat AJ, Almasa’afeh HY, Abuallaban SM
ClinicoEconomics and Outcomes Research 2025, 17:455-471
Published Date: 12 July 2025