Back to Journals » Infection and Drug Resistance » Volume 16
Targeted Antibiotics for Lower Respiratory Tract Infection with Corynebacterium striatum
Authors Zhang H ![]() , Tan X, Zhang Z, Yang X, Wang L
, Tan X, Zhang Z, Yang X, Wang L ![]() , Li M
, Li M ![]() , Shi D, Li Y, Li J, Li Z, Liao X
, Shi D, Li Y, Li J, Li Z, Liao X
Received 14 January 2023
Accepted for publication 29 March 2023
Published 4 April 2023 Volume 2023:16 Pages 2019—2028
DOI https://doi.org/10.2147/IDR.S404855
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Huan Zhang,1,2 Xiaojiao Tan,1 Zhen Zhang,1 Xuewei Yang,1 Lijie Wang,1 Meiqian Li,1 Dan Shi,1 Yao Li,1 Jianbo Li,1 Zhen Li,3 Xuelian Liao1,4
1Department of Critical Care Medicine, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 2Department of Critical Care Medicine, The Third People’s Hospital of Chengdu, Chengdu, People’s Republic of China; 3Clinical Research Unit, First Maternity and Infant Hospital of Shanghai, Shanghai, People’s Republic of China; 4Department of Critical Care Medicine, West China Tianfu Hospital of Sichuan University, Chengdu, People’s Republic of China
Correspondence: Xuelian Liao, Department of Critical Care Medicine, West China Hospital, Sichuan University, No. 37, Guoxue Lane, Wuhou district, Chengdu, People’s Republic of China, Tel +8613541023033, Email [email protected]
Purpose: To assess the impact of targeted antibiotic therapy on clinical outcomes of patients with lower respiratory tract (LRT) infection with Corynebacterium striatum (C. striatum).
Methods: A new propensity score-inverse probability of treatment weighting (IPTW) cohort study was conducted by using 10-year data. The study included LRT infection patients with respiratory secretions cultured positive for C. striatum simultaneously. The primary outcome was all-cause hospital mortality; the secondary outcomes included hospital stay, ICU stay and ventilation time. The safety outcomes were drug-related serum creatinine (Cr) increase and thrombocytopenia.
Results: A total of 339 patients were included in the cohort, and 84 (24.78%) initiated vancomycin or linezolid therapy. In the new IPTW cohort, targeted antibiotic therapy did not improve all-cause hospital mortality (P=0.632), and the OR (95% CI) was 0.879 (0.519– 1.488). Moreover, targeted antibiotic therapy was not associated with hospital stay (P=0.415), ICU stay (P=0.945) or ventilation time (P=0.885). The side effects of drug-related higher serum Cr (P=0.044) and thrombocytopenic levels (P=0.038) cannot be ignored.
Conclusion: Clinical benefits by vancomycin or linezolid targeted against LRT infection with C. striatum were limited and with drug-related side effects. A prospectively designed study is needed to further confirm the results.
Keywords: Corynebacterium striatum, lower respiratory tract infection, vancomycin, linezolid, all-cause mortality
Plain Language Summary
Corynebacterium striatum (C. striatum) is emerging as a possible cause for severe hospital-acquired pneumonia with high mortality rates, especially among immunocompromised patients. The information about targeted antibiotic therapy against C. striatum in lower respiratory tract infection is scarce.
In this study, a new propensity score-inverse probability of treatment weighting (IPTW) cohort study was conducted by using 10-year relatively large amount of data. Our results did not show any improvement in all-cause hospital mortality, hospital stay, ICU stay or ventilation time of targeted antibiotic therapy against C. striatum, but with drug-related side effects of serum creatinine increase and thrombocytopenia. Meanwhile, in subgroup analysis, targeted antibiotic therapy against C. striatum improved the all-cause hospital mortality when APACHE II score was higher than 15. That is to say, clinical benefits by vancomycin or linezolid targeted against C. striatum in LRT infection were limited, and with drug-related side effects. This study provides new insights into understanding the treatment of C. striatum in lower respiratory tract infection.
Introduction
Lower respiratory tract infection (LRT) is consistently among the leading causes of morbidity and mortality worldwide. As a normal resident of the human skin and mucous membranes, including the respiratory tract, Corynebacterium striatum (C. striatum) has historically been considered a contaminant, mainly due to the difficulty in distinguishing between colonization and infection.1 In the last few decades, an increasing number of cases and studies have reported that C. striatum is considered a pathogen in different types of infections,2 even as an emerging multidrug-resistant nosocomial pathogen.3,4
Giorgio Silva-Santana et al5 conducted a worldwide survey of C. striatum human invasive infections and nosocomial outbreaks over 44 years (1976–2020). They found that C. striatum has been increasingly reported as the etiologic agent of community-acquired and nosocomial diseases, especially for patients with chronic disease, long hospital stays, long ICU stays, and the use of continuous or prolonged medical devices or broad-spectrum antibiotics. A study of mNGS detection in patients in the ICU with pulmonary infection found that the predominant detected bacteria were C. striatum (11.76%, 51/434) and that C. striatum was always multidrug resistant, including resistance to MSLB, phenicol, fluoroquinolones and erythromycin. Despite multidrug resistance, C. striatum is sensitive to vancomycin and linezolid.6
A retrospective study was conducted in 51 advanced respiratory disease patients, mainly those with chronic obstructive pulmonary disease (COPD), for 38 months. Seventy-two C. striatum isolates were isolated that were all multidrug resistant to antibiotics, but all were sensitive to vancomycin. They contributed to a high mortality (41%) during the study period.7 Another study included 11 patients suffering from either COPD (n = 9) or pneumonia (n = 2). No other potential pathogens were isolated along with C. striatum. All patients made a complete recovery after antibiotic treatment.8
In reality, it is difficult to distinguish C. striatum as a pathogen causing infection and one causing colonization. Their degree of virulence also remains largely unknown. Vancomycin and linezolid are a mainstay of the target against C. striatum. However, there remains equivocal on their role for patients who have evidence of LRT infection, primarily because of a paucity of data. Emerging evidence for potential benefits or adverse effects in these patients remains limited, especially for relatively large clinical data. To address this, we used real-world data over the last 10 years from West China Hospital from patients with LRT infection and C. striatum detected in respiratory samples to explore the association of vancomycin and linezolid use with the incidence of all-cause hospital mortality, total hospital stays, ICU stays and ventilation time after the first cultivated C. striatum. We also analyzed the side effects of vancomycin and linezolid, including serum creatinine (Cr) increase and thrombocytopenia.
Materials and Methods
Study Design and Data Source
This study was approved by the Ethical Committee of West China Hospital in 2021 (WCH2021-1548), and the requirement for obtaining patient informed consent was waived as this was a retrospective study. All patient data were retrieved from the medical record database. Prior to analysis, all patient data involved in the study were anonymized. After local ethics board approval, we performed a new user design and propensity score-inverse probability of treatment weighting (IPTW) cohort study of a major referral center in western China for patients with a variety of clinical conditions. The data sources were carried out from January 1, 2012, to December 31, 2021, in West China Hospital, Sichuan University, southwestern China. It is a 4300-bed tertiary-care hospital.
We included all adult inpatients having new or worse conditions of lower respiratory tract infection and their respiratory samples (including sputum, airway secretion or bronchoalveolar lavage fluid) cultured positive for C. Striatum at the same time. Day 1 was defined as the day when the respiratory sample was collected.
The LTR infections include pneumonia or bronchitis. Relevant clinical manifestations of LTR infection: (1) New onset of cough or expectoration or aggravation of existing symptoms of respiratory tract diseases, with or without purulent sputum, chest pain, dyspnea, or hemoptysis; (2) Fever; (3) Signs of pulmonary consolidation and/or moist rales; (4) Peripheral white blood cell count (WBC)> 10*10^9/L or < 4*10^9/L, with or without a left shift; (5) Chest radiograph (X-ray or CT scan) showing new patchy infiltrates, lobar or segmental consolidation, ground-glass opacities, or interstitial changes, with or without pleural effusion; (6) Physical findings (tachypnea, tachycardia, arterial hypotension, focal auscultatory abnormality). A clinical diagnosis can be established if a patient satisfies one of (1)~(4) and (5) or one of (1)~(4) and (6) when a chest radiograph is not feasible and all the manifestations have no other recognized cause.
We excluded patients with (1) incomplete information, including date of birth, sex, and discharged diagnosis; (2) extremely long hospital stay as they expected to stay at the hospital until their dying day; and (3) use of other antibiotic drugs against C. striatum (other than vancomycin or linezolid) according to its sensitivity test.
The patient information included age, sex, and diagnosis codes, which were used to identify comorbidities associated with therapy and clinical outcomes. These included heart failure, COPD, respiratory failure, liver dysfunction, renal failure, consciousness disorders, gastrointestinal bleeding, malignancy, hypertension, and diabetes. The severity of illness was evaluated by the Acute Physiology and Chronic Health Evaluation (APACHE) II score.9 The severity of sepsis was assessed by the Sequential Organ Failure Assessment (SOFA) score.10 The neutrophil: lymphocyte ratio (NLR) is an informative biomarker with infection reflecting underlying immune dysfunction.11 Related laboratory tests were collected from day 1 to day 7. All of the above indicators were considered the worst data point of 24 h of day 1 or day 7.
Cohort Identification
Patients meeting both of the following two conditions were divided into targeted antibiotic therapy group: (1) patients initiated vancomycin or linezolid within 3 days when the C. striatum samples were first collected; (2) the course of the treatment was sufficient. Otherwise, patients were divided into the nontargeted antibiotic therapy group including: (1) patients with any prior vancomycin or linezolid use but withdrawn before day 1; (2) the course of the treatment was not sufficient; (3) patients with vancomycin or linezolid targeted against other diseases for a long time before or after day 1; and (4) patients using other empirical therapies aimed at C. striatum.
Outcomes
The primary effectiveness outcomes were all-cause hospital mortality. Secondary effectiveness outcomes, including total hospital stay, ICU stay and ventilation time after day 1 when C. striatum were first cultivated, were collected. The primary safety outcomes were drug-related serum creatinine (Cr) increase and thrombocytopenia.
Statistical Analysis
We used means and standard deviations for continuous variables or frequencies and percentages for categorical variables to characterize the study cohort. Vancomycin or linezolid administration may be better tolerated by particular patients or more effective for patients who are more seriously ill. This results in a correlation—or confounding—between the patient characteristics that affect outcomes and the choice of therapy. Inverse probability of treatment weighting (IPTW) incorporating propensity scores12 was used to adjust for differences between groups to obtain valid estimates of the associations between the treatments being compared and the outcomes of interest. Multivariable statistical methods were used to estimate this association while adjusting for confounding. A standardized difference ≤0.1 for a baseline covariate reveals a negligible imbalance.
The following covariates related to the choice of therapy and the clinical outcomes were included in generating the propensity score13 based on the information from day 1: age, severe comorbidities (heart failure, respiratory failure, gastrointestinal bleeding, renal failure, malignant tumor), highest APACHE II score, highest SOFA score of Day 1, combined with other bacterial infections, administration of other empiric antibacterial therapy (including β-lactam antibiotics, quinolone antibiotics and so on), antifungal therapy, and neutrophil: lymphocyte ratio (NLR).
The patients in the targeted antibiotic therapy group were weighted by the inverse of the propensity score, and the patients in the nontargeted antibiotic therapy group were weighted by the inverse of 1 minus the propensity score. IPTW was chosen for confounder adjustment in this study because it allowed almost all eligible patients to be included in the analysis. It also has the favorable property of resulting in the exact balance of important covariates included in the logistic regression model used to derive the propensity scores.
The new weighted pseudocopopulation was created to ensure that at baseline, both groups were as similar as possible on the important variables that may affect the clinical outcomes and choice of therapy, except targeted antibiotic administration against C. striatum.
The baseline data were compared using Pearson’s chi-square test for categorical variables or the independent-samples t-test for continuous variables. In the IPTW weighting cohort, odds ratios and 95% confidence intervals for the primary outcome were estimated using weighted regression.
All analyses were conducted in R.version 4.2.1. P< 0.05 (2-sided) was considered statistically significant. We use the Power Analysis and Sample Size 21.0 (PASS 21.0) to calculate statistical power of using vancomycin or linezolid against C. striatum in our study.
Results
Baseline Characteristics
In our study, during the last 10 years between 1 Jan 2012 and 31 Dec 2021, the non duplication of all adult patients at the hospital cultured positive for C. Striatum at any site of body fluid or tissue was 898. At the site of the respiratory tract, a total of 389 unique cases were detected. A total of 339 patients who were known to have LTR infection in the hospital with respiratory secretions that cultured positive for C. striatum met the eligibility criteria. The numbers of patients in the targeted antibiotic therapy group and nontargeted antibiotic therapy group were 84 and 255, respectively (Supplemental Figure 1 Flowchart of included patients).
The baseline characteristics of all eligible patients between the two groups are displayed in Table 1. Some notable baseline differences existed in the two cohorts. Compared with the nontargeted antibiotic therapy patients, the targeted antibiotic therapy patients were much younger (62.37±15.88 vs 67.53±16.82) but had a higher incidence of heart failure (57.1% vs 44.3%), respiratory failure (56.0% vs 42.4%), and gastrointestinal bleeding (41.7% vs 27.1%). Additionally, the targeted antibiotic therapy patients suffered more severe conditions, with higher APACHE II scores (16.11±6.14 vs 14.32±5.77) and SOFA scores (5.57±3.14 vs 4.58±3.23). The immunity of the targeted antibiotic therapy group was more dysfunctional, with a higher NLR than that of the nontargeted antibiotic therapy group (14.40±11.49 vs 11.54±9.79). In the new cohort derived using IPTW analysis, none of these differences persisted, and the two groups were similar on all covariates, which are displayed in Supplemental Table.
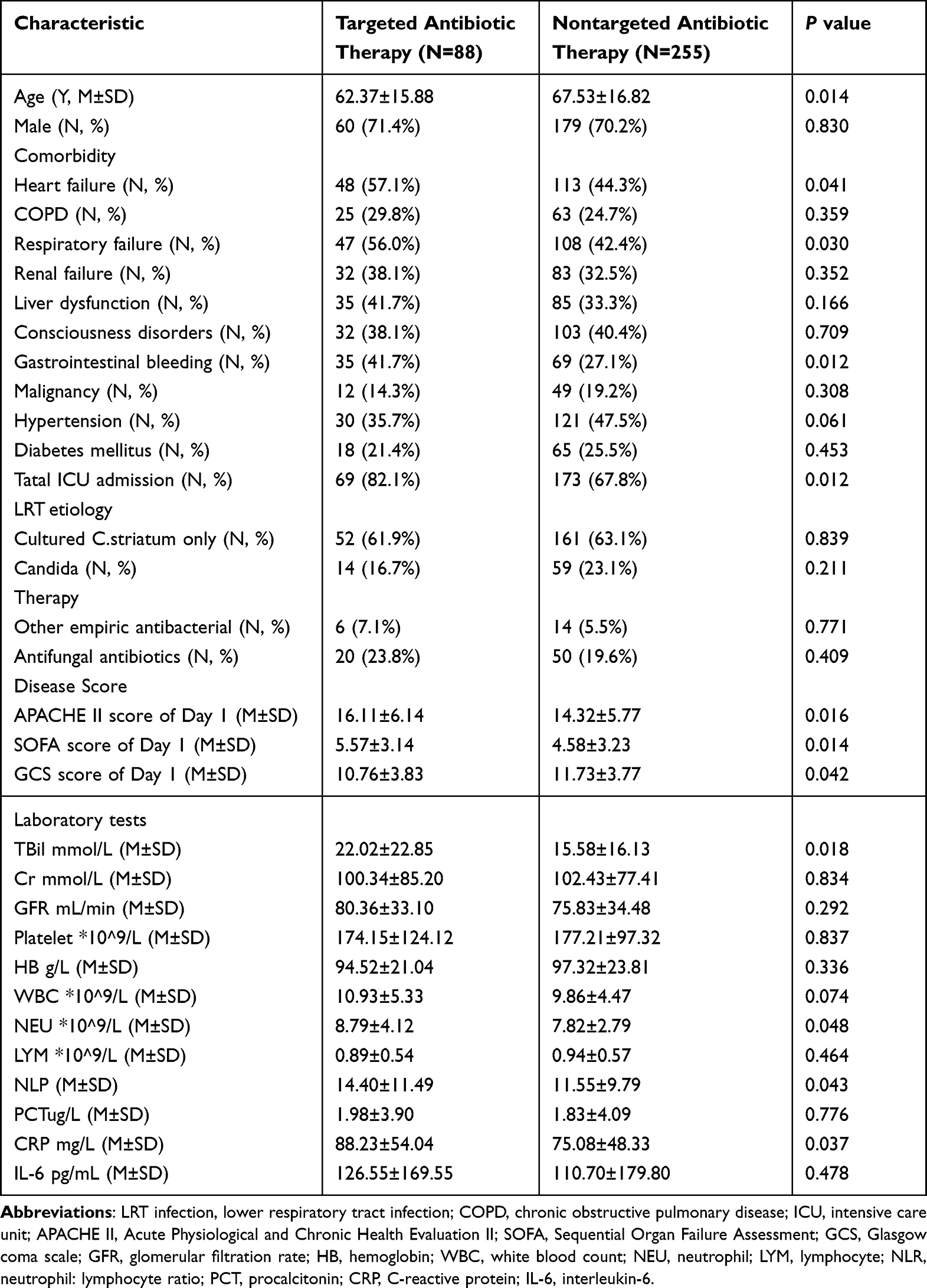 |
Table 1 Baseline Characteristics in the Cohort of 339 Eligible Patients |
Primary Outcomes
The total all-cause hospital mortality was 118. In the targeted antibiotic therapy group, 36 (42.9%) patients suffered, while in the nontargeted antibiotic therapy group, the all-cause hospital mortality was 82 (32.2%), P≥0.05. In the new IPTW cohort, to err on the side of conservative estimates, a doubly robust analysis accounting for all covariables originally included in the generation of propensity scores to derive an adjusted OR was used. In the adjusted regression analyses, administration of vancomycin or linezolid against C. Striatum did not improve the all-cause hospital mortality (P=0.632), and the OR (95% CI) was 0.879 (0.519–1.488).
Not surprisingly, the other variables independently associated with increased odds of all-cause hospital mortality included severity of condition: (1) SOFA score, OR (95% CI) was 1.204 (1.115–1.305); (2) comorbidity: heart failure, OR (95% CI) was 1.949 (1.271–3.003) and malignant tumor OR (95% CI) was 4.194 (2.539–7.002); and (3) poor immune status reflected by NLR, OR (95% CI) was 1.049 (1.031–1.068). Excluding targeted therapy against C. striatum, we found that other therapies aimed at LRT infection, including empirical antibacterials and antifungals, may reduce all-cause mortality, with ORs (95% CI) of 0.117 (0.046–0.279) and 1.959 (1.231–3.120), respectively. The primary outcomes are displayed in Table 2.
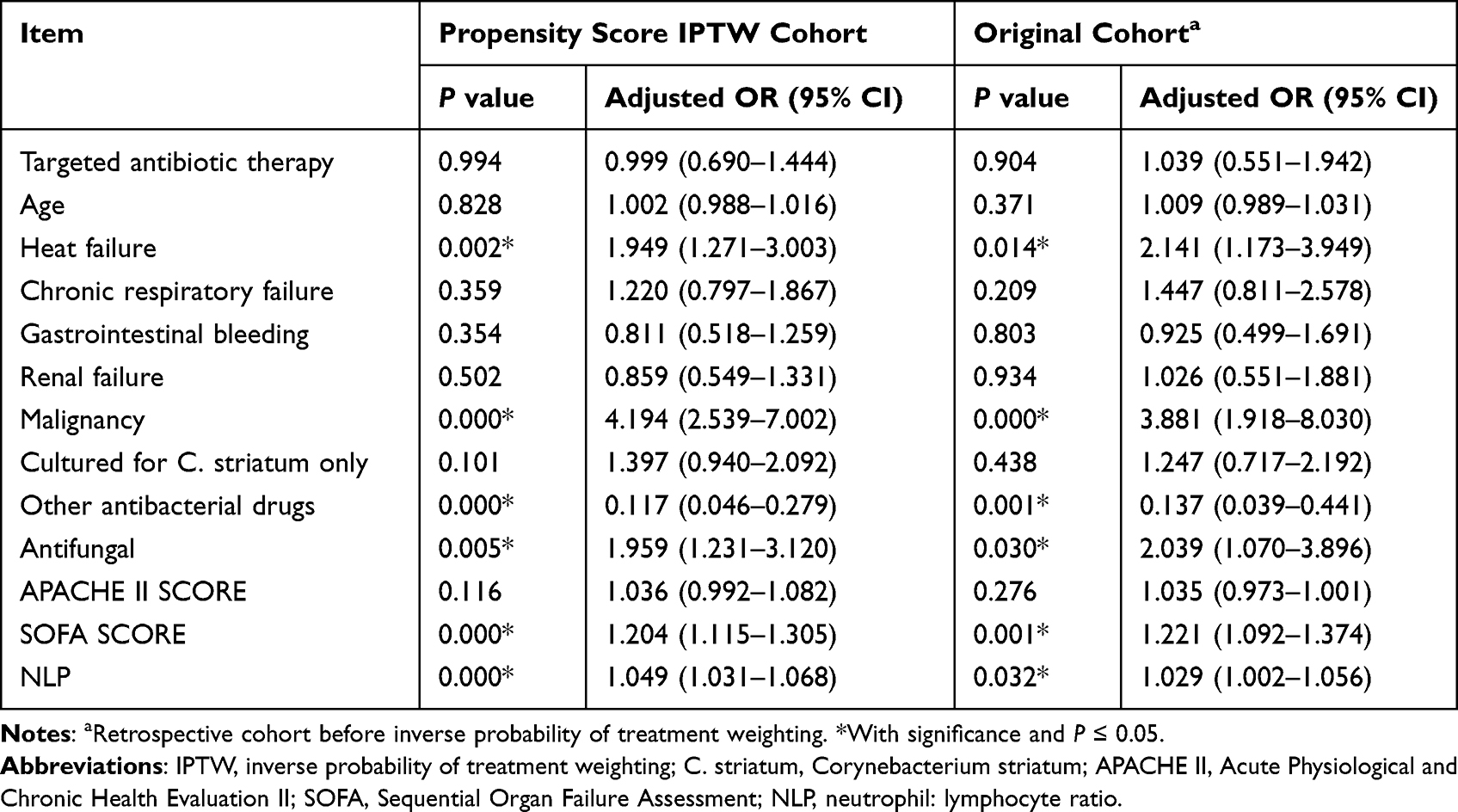 |
Table 2 Multivariable Analysis of All-Cause Mortality for 339 Patients with C. Striatum LRT Infection After Using an Inverse Probability of Treatment Weighted Cohort Based on Propensity Scores |
We conducted a subgroup analysis according to the APACHE II score. A total of 169 patients with APACHE II scores higher than 15 were divided into the severity condition subgroup. A total of 170 patients with APACHE II scores less than 15 were divided into the mild condition subgroup. In the severity condition subgroup, the all-cause hospital mortality was 76 (22.4%), which was significantly higher than that in the mild condition subgroup (42 (12.4%)), P≤0.05. In the severity condition subgroup, 53 (31.36%) patients received vancomycin or linezolid. After IPTW, we found that vancomycin or linezolid use may significantly decrease all-cause hospital mortality (P=0.028) (OR (95% CI) = 0.549 (0.319–0.932)), while in the mild condition subgroup, 31 (18.24%) patients initiated vancomycin or linezolid, which was not associated with all-cause hospital mortality (P=0.256), and the OR (95% CI) was 1.455 (0.769–2.819). The subgroup analysis outcomes are displayed in Table 3.
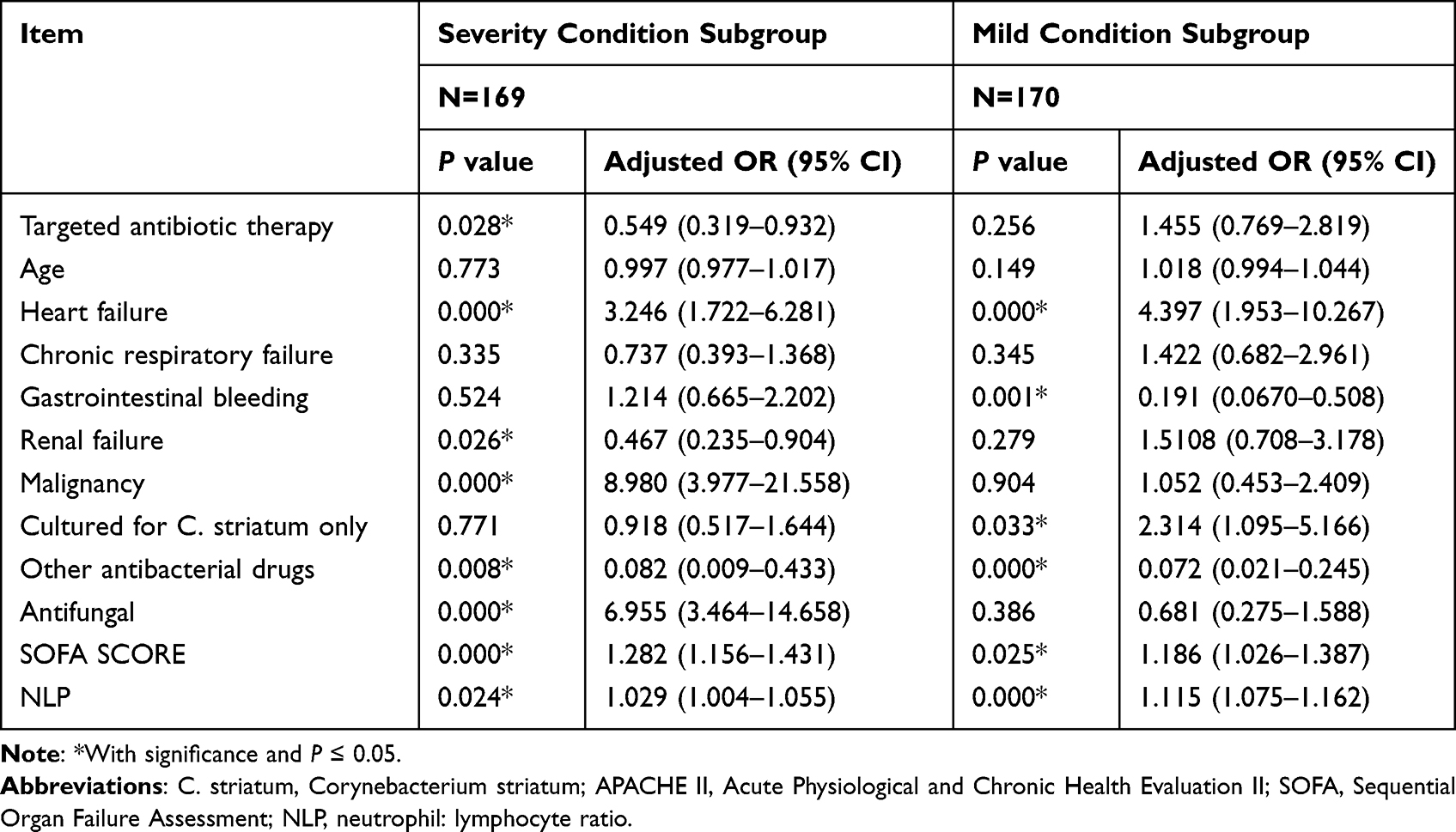 |
Table 3 Multivariable Analysis of All-Cause Mortality for Subgroup Analysis According to APACHE II Score After Using an Inverse Probability of Treatment Weighted Cohort Based on Propensity Scores |
Secondary Outcomes
After day 1, the mean time for ICU stay was 15.12±11.13 days, the mean time for hospital stay was 17.88±15.78 days and the mean ventilation time was 231.97±225.90 hours. In the new IPTW cohort, vancomycin or linezolid therapy was not associated with ICU stay (P=0.945), hospital stay (P=0.415) or ventilation time (P=0.885) according to the multiple linear regression model. In the model, gastrointestinal bleeding (P=0.008) and LTR samples only detecting C. striatum (P=0.006) were independently related to the ICU stay. Gastrointestinal bleeding (P=0.009), malignant tumors (P=0.008) or a higher SOFA score (P=0.006) reflected a serious inflammatory response effect on hospital stay. While the patients whose respiratory sample only cultivated C. striatum, more ventilation time may suffer (P=0.019). The secondary outcomes are displayed in Table 4.
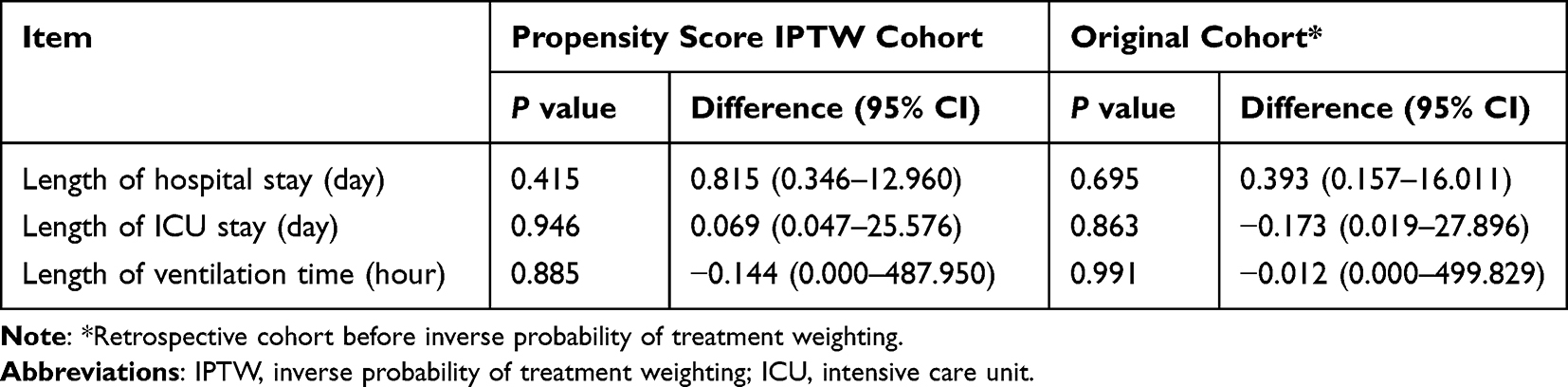 |
Table 4 Multivariable Analysis of Secondary Outcomes in the Two Groups |
Safety Outcomes
After 7 days, the SOFA score and NLR were significantly decreased in both groups (P≤0.05). Although the mean serum Cr was higher in the targeted antibiotic group without significance, the serum Cr was significantly decreased in the nontargeted antibiotic group (P≤0.05). The blood platelets were significantly increased in the bother group after 7 days (P≤0.05) (Supplemental Figure 2 Comparison of day 1 and day 7 of laboratory testing in 339 patients). The decreased degree of serum Cr in the nontargeted antibiotic group was significantly higher than that in the targeted antibiotic group, and the increased degree of blood PLT in the nontargeted antibiotic group was also significantly higher than that in the targeted antibiotic against C. striatum (Supplemental Figure 3 Degree of change in laboratory testing (day 7 vs day 1) between the two groups).
Discussion
Our research provides new insights into understanding the treatment of C. striatum in lower respiratory tract infection by conducting a new IPTW cohort study. This study contained 10-year relatively large amount of data. The results showed that targeted antibiotic therapy against C. striatum in lower respiratory tract infection did not improve all-cause hospital mortality, hospital stay, ICU stay or ventilation time, but with drug-related side effect of serum creatinine increase and thrombocytopenia. Meanwhile, in subgroup analysis, targeted antibiotic therapy against C. striatum improved all-cause hospital mortality when APACHE II score was higher than 15.
Due to being common components of the skin microbiota, C. striatum is usually thought of as a colonizer or contaminant. In recent years, the clinically related C. striatum has been recognized, particularly as a cause of respiratory tract infection.14 Before undertaking this work, we defined the use of vancomycin or linezolid administration as a targeted antibiotic therapy group for the following reasons: (1) The prevalence of C. striatum isolated from the respiratory tract always exhibited multiple drug-resistance (MDR) profiles, but all were susceptible to vancomycin or linezolid in previous studies.15 (2) In China, a total of 260 isolates were collected from respiratory infection patients from three hospitals in three regions. Almost all isolates (96.2%, 250/260) showed multidrug resistance, but all were susceptible to vancomycin or linezolid,16 which was similar to the findings from other countries.17–19
Antimicrobial resistance of C. striatum has evolved rapidly. To date, studies of antibiotic therapy against C. striatum in LRT infection were limited. For this reason, we developed a retrospective cohort study with 339 C. striatum-related LRT infection patients during last 10 years. Most of them were in the context of underlying diseases. A total of 118 (34.81%) patients suffered all-cause hospital mortality. The result was close to another systematic review including 42 studies and 85 invasive infections caused by C. striatum. The review reported that 62.30% of the patients experienced a complete recovery after antibiotic treatment, and the mortality rates were 34.00% among those with bacteremia caused by C. striatum.2
The high mortality rates observed in our study can be partly attributed to the severity of disease, and also to the infectious exacerbation of disease by C. striatum. To eliminate the differences in the baseline characteristics between the two groups. We created a similar severity of the clinical condition in both groups by IPTW. We found that the use of vancomycin or linezolid against C. striatum, as opposed to nontargeted antibiotic therapy, did not reduce the odds of all-cause hospital mortality, and the targeted therapy could not reduce the hospital stay, ICU stay or ventilation time.
Similar findings were shown in Jin Woong Suh’s study.20 Sixty-seven C. striatum isolates from nonduplicated patients were characterized in his study. All strains were susceptible to vancomycin and linezolid. Additionally, this study showed no difference regarding in-hospital mortalities between the treatment and observation groups. However, in his study, no strains were isolated from LRT. Another 9 isolates from bronchoalveolar lavage samples were indicated by clinicians to be clinically relevant in immunocompetent adult patients. All of these patients were empirically treated with vancomycin for healthcare-associated pneumonia. No clinical failures in vancomycin therapy were documented.21 The clinical results of this study may be affected by the immunocompetence of patients. Meanwhile, F. Renom observed 72 C. striatum isolates from 51 advanced respiratory disease patients, mainly chronic obstructive pulmonary disease, over 38 months. Twenty-five of the 51 patients (49%) died during follow-up, but his study did not describe how the antibiotics were used.7
C. striatum is an opportunistic pathogen, and patients always suffer immunosuppression and serious conditions. Therefore, in our subgroup analysis, patients encountered severe conditions with the APACHE II score higher than 15. In the subgroup analysis, use of vancomycin or linezolid may result in lower all-cause hospital mortality. However, in the group with mild conditions, exposure to vancomycin or linezolid was not associated with all-cause hospital mortality.
Other comprehensive therapies (such as sputum drainage and nutritional support) may contribute to the improvement of whole condition of LRT infection patients with C. striatum. In our study, the SOFA score was used to evaluate the inflammatory reaction. On day 7, both groups had significantly lower SOFA scores than that on day 1, and the degree of decrease was similar in both groups. As a systematic review and meta-analysis of Clark D. Russell reported that a higher NLR of bacteremic patients was associated with mortality.22 In our study, compared to day 1, the NLR of both groups was significantly decreased on day 7, and the degree of change in both groups was similar. That is, after systematic therapy, the condition of immunity in both groups was improved, which may improve the clinical condition.
Vancomycin is a glycopeptide antibiotic that is active against Gram-positive bacteria. Nephrotoxicity, although usually reversible, is the most serious common adverse effect of vancomycin.23 Vancomycin-associated nephrotoxicity has been generally defined as changes in the serum Cr from baseline. In our study, we found that after 7 days, all the patients had a lower concentration of serum Cr, but the patients in the nontargeted group had significantly lower serum Cr levels than those on day 1. Additionally, the degree of change was significantly lower in the nontargeted antibiotic therapy group. Another side effect of vancomycin is induced immune thrombocytopenia.24 After 7 days of therapy, the concentration of blood platelets in the nontargeted antibiotic therapy group was also higher than that in the targeted antibiotic therapy group.
Strengths of the Study
There is some significance and impact of the study. First, we conducted a retrospective study over the last 10 years and obtained a relatively large amount of data. Second, we created a new IPTW cohort to imitate the randomized controlled trial, which had a similar baseline of the two groups. Moreover, unlike other studies without a definition of therapy, our study defined targeted therapy by using vancomycin or linezolid. We explored the effectiveness of clinical outcomes and the side effects of targeted therapy. Finally, as C. striatum is an opportunistic pathogen, patients always suffer immunosuppression and other serious conditions. We also conducted a subgroup analysis according to the severity of the clinical condition.
Our results did not show any improvement in all-cause hospital mortality or hospital stay by using vancomycin or linezolid in LRT-infected patients colonized or infected with C. striatum. We use the Power Analysis and Sample Size 21.0 (PASS 21.0) to calculate statistical power of using vancomycin or linezolid against C. striatum in our study. A logistic regression of a binary response variable on a binary independent variable with a sample size of 339 cases (of which 24.77% are in the targeted antibiotic group) at a 0.859 confidence level produces a two-sided confidence interval with a width of 0.754. The baseline response rate is assumed to be 49%,7 and the sample odds ratio is assumed to be 0.999. A Wald statistic is used to construct the confidence interval.
The targeted antibiotic may contribute to nephrotoxicity and thrombocytopenia. If patients encounter critical conditions, we should take systematic therapy to improve the clinical condition. Target antibiotic therapy may play a part in the improvement of the whole clinical condition, and further research is needed to support this idea.
Limitations of the Study
Our study has the following limitations. First, in this retrospective cohort study, the use of IPTW incorporating propensity scores to ensure the two comparable groups was very similar with regard to the demographic data, existing medical conditions, severity of the clinical condition at the onset of day 1, and use of other antibiotics. However, we did not consider additional factors that could impact the association between the initiation of target antibiotics and mortality as covariates, eg, chronic obstructive pulmonary disease, consciousness disorder and diabetes mellitus. These factors may have less of a coeffect on clinical outcomes. We selected all-cause mortality as the primary outcome since the initial choice of antibiotic therapy is more likely to be attributable to this endpoint, while other factors could also have impacted mortality (eg, poor fluid management, lack of source control). However, it may impede us from learning useful knowledge of targeted antibiotic use from the current study. Second, we did not perform other clinical outcomes, such as readmission after discharge or the survival data that analyzed the association of 28-day or 90-day mortality with target antibiotic use. The above items were seriously biased because this was a retrospective study. Finally, we did not conduct the study to compare the different effects between vancomycin and linezolid, as the sample size was reasonably small. Further research, including from randomized clinical trials, is needed to more definitively determine the role of vancomycin or linezolid therapy in different types of infection.
Conclusions
Our results showed that the clinical benefits by vancomycin or linezolid targeted against LRT infection with C. striatum were limited, but with side effect of serum creatinine increase and thrombocytopenia. Our data provide new insights into understanding the therapy when respiratory samples from LRT infected patients were positive for C. striatum. A prospectively designed study is needed to further confirm the results.
Abbreviations
LRT, lower respiratory tract; C. striatum, Corynebacterium striatum; IPTW, inverse probability of treatment weighting; SMD, standardized mean difference; COPD, chronic obstructive pulmonary disease; APACHE II score, Acute Physiology and Chronic Health Evaluation II score; SOFA score, Sequential Organ Failure Assessment score; NLR, neutrophil: lymphocyte ratio; GCS, Glasgow coma scale; WBC, white blood count; PCT, procalcitonin; CRP, C-reactive protein; IL-6, interleukin-6; TB, total bilirubin; Cr, creatinine; GFR, glomerular filtration rate; HB, hemoglobin; PLT, platelet.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are not publicly available due to all data from the electronic medical record system in the hospital which are not public, but are available from the corresponding author on reasonable request.
Ethics Approval
Ethics: This study protocol was in accordance with the Helsinki Declaration and was approved by the Ethical Committee of West China Hospital (Approval No. WCH2021-1548). As all the patients had signed informed consent to use the clinical data anonymously for future scientific research purposes upon admission, additional informed consent for this study was waived. All patient data were retrieved from the medical record database. Prior to the analysis, all data involved in the study were anonymized by information department.
Acknowledgments
The authors would like to thank West China Hospital, Sichuan University for data supply that made the study possible. We extend our gratitude to all data collectors for their cooperation and efforts during the data collection.
Author Contributions
All authors made a significant contribution to the work reported which not only including study design, execution, acquisition of data, analysis and interpretation, or in all these areas but also including drafting, revising or critically reviewing the article; All authors gave final approval of the version to be published and have agreed on the journal to which the article has been submitted. Also, all authors agree to be accountable for all aspects of the work.
Funding
This work was supported by program from Ministry of Science and Technology of China (2022YFC2009804).
Disclosure
All authors declare no potential conflicts of interest relevant to this article.
References
1. Zasada A, Mosiej A. Contemporary microbiology and identification of Corynebacteria Corynebacteria spp. causing infections in human. Lett Appl Microbiol. 2018;66(6):472–483. doi:10.1111/lam.12883
2. Milosavljevic MN, Milosavljevic JZ, Kocovic AG, et al. Antimicrobial treatment of Corynebacterium striatum invasive infections: a systematic review. Rev Inst Med Trop Sao Paulo. 2021;18(63):e49. doi:10.1590/s1678-9946202163049
3. Alibi S, Ferjani A, Boukadida J, et al. Occurrence of Corynebacterium striatum as an emerging antibiotic-resistant nosocomial pathogen in a Tunisian hospital. Sci Rep. 2017;7(1):9704. doi:10.1038/s41598-017-10081-y
4. Wang X, Zhou H, Chen D, et al. Whole-genome sequencing reveals a prolonged and persistent intrahospital transmission of Corynebacterium striatum, an emerging multidrug-resistant pathogen. J Clin Microbiol. 2019;57(9):e00683–19. doi:10.1128/JCM.00683-19
5. Silva-Santana G, Silva CMF, Olivella JGB, et al. Worldwide survey of Corynebacterium striatum increasingly associated with human invasive infections, nosocomial outbreak, and antimicrobial multidrug-resistance, 1976–2020. Arch Microbiol. 2021;203(5):1863–1880. doi:10.1007/s00203-021-02246-1
6. Chen H, Bai X, Gao Y, Liu W, Yao X, Wang J. Profile of bacteria with ARGs among real-world samples from ICU admission patients with pulmonary infection revealed by metagenomic NGS. Infect Drug Resist. 2021;27(14):4993–5004. doi:10.2147/IDR.S335864
7. Renom F, Gomila M, Garau M, et al. Respiratory infection by Corynebacterium striatum: epidemiological and clinical determinants. New Microbes New Infect. 2014;2(4):106–114. doi:10.1002/nmi2.48
8. Shariff M, Aditi A, Beri K. Corynebacterium striatum: an emerging respiratory pathogen. J Infect Dev Ctries. 2018;12(7):581–586. doi:10.3855/jidc.10406
9. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829. doi:10.1097/00003246-198510000-00009
10. Brown KA, Brain SD, Pearson JD, Edgeworth JD, Lewis SM, Treacher DF. Neutrophils in development of multiple organ failure in sepsis. Lancet. 2006;368(9530):157–169. doi:10.1016/S0140-6736(06)69005-3
11. Raith EP, Udy AA, Bailey M, et al. Prognostic accuracy of the SOFA score, SIRS criteria, and qSOFA score for in-hospital mortality among adults with suspected infection admitted to the intensive care unit. JAMA. 2017;317(3):290–300. doi:10.1001/jama.2016.20328
12. Reifeis SA, Hudgens MG. On variance of the treatment effect in the treated when estimated by inverse probability weighting. Am J Epidemiol. 2022;191(6):1092–1097. doi:10.1093/aje/kwac014
13. Brookhart MA, Schneeweiss S, Rothman KJ, Glynn RJ, Avorn J, Stürmer T. Variable selection for propensity score models. Am J Epidemiol. 2006;163(12):1149–1156. doi:10.1093/aje/kwj149
14. Kazuhiro Y, Hiroshi M. Corynebacterium species as one of the major causative pathogens of bacterial pneumonia. Respir Investig. 2020;58(3):131–133. doi:10.1016/j.resinv.2020.01.008
15. Chapartegui-González I, Fernández-Martínez M, Rodríguez-Fernández A, et al. Antimicrobial susceptibility and characterization of resistance mechanisms of Corynebacterium urealyticum clinical isolates. Antibiotics. 2020;9(7):404. doi:10.3390/antibiotics9070404
16. Xw A, Hz A, Pd B, et al. Genomic epidemiology of Corynebacterium striatum from three regions of China: an emerging national nosocomial epidemic. J Hosp Infect. 2021;110:67–75. doi:10.1016/j.jhin.2020.10.005
17. Campanile F, Carretto E, Barbarini D, et al. Clonal multidrug-resistant Corynebacterium striatum strains, Italy. Emerg Infect Dis. 2009;15(1):75–78. doi:10.3201/eid1501.080804
18. Verroken A, Bauraing C, Deplano A, et al. Epidemiological investigation of a nosocomial outbreak of multidrug‐resistant Corynebacterium striatum at one Belgian university hospital. Clin Microbiol Infect. 2014;20(1):44–50. doi:10.1111/1469-0691.12197
19. Asgin N, Otlu B. Antimicrobial resistance and molecular epidemiology of Corynebacterium striatum isolated in a Tertiary Hospital in Turkey. Pathogens. 2020;9(2):136. doi:10.3390/pathogens9020136
20. Suh JW, Yongguk J, Lee CK, Sohn JW, Kim MJ, Yoon YK. Molecular epidemiology and clinical significance of Corynebacterium striatum isolated from clinical specimens. Infect Drug Resist. 2019;12:161–171. doi:10.2147/IDR.S184518
21. Hahn WO, Werth BJ, Butler-Wu SM, Rakita RM. Multidrug-resistant Corynebacterium striatum associated with increased use of parenteral antimicrobial drugs. Emerg Infect Dis. 2016;22(11):1908–1914. doi:10.3201/eid2211.160141
22. Russell CD, Parajuli A, Gale HJ, et al. The utility of peripheral blood leucocyte ratios as biomarkers in infectious diseases: a systematic review and meta-analysis. J Infect. 2019;78(5):339–348. doi:10.1016/j.jinf.2019.02.006
23. Jeffres MN. The whole price of vancomycin: toxicities, troughs, and time. Drugs. 2017;77(11):1143–1154. doi:10.1007/s40265-017-0764-7
24. Von Drygalski A, Curtis BR, Bougie DW, et al. Vancomycin-Induced Immune Thrombocytopenia. N Engl J Med. 2007;356(9):904–910. doi:10.1056/NEJMoa065066
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Adult Empyema Caused by Refractory Methicillin-Resistant Staphylococcus aureus Treated Using Linezolid as Salvage Therapeutic Option: A Report of Two Cases
Seki M, Nagai T, Ozawa K
Infection and Drug Resistance 2026, 19:625227
Published Date: 10 July 2026