Back to Journals » Journal of Inflammation Research » Volume 19
Tackling Neutrophilic Inflammation in Bronchiectasis: From Macrolides to Cathepsin C Inhibitors
Authors Gramegna A, Premuda C, Putti G ![]() , Piedepalumbo FV, Misuraca S, Ori M, Nigro M
, Piedepalumbo FV, Misuraca S, Ori M, Nigro M ![]() , Simonetta E, Aliberti S, Blasi F
, Simonetta E, Aliberti S, Blasi F ![]()
Received 12 January 2026
Accepted for publication 31 March 2026
Published 11 April 2026 Volume 2026:19 558745
DOI https://doi.org/10.2147/JIR.S558745
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Andrea Gramegna,1,2 Chiara Premuda,2 Gianmarco Putti,1,2 Federica Viola Piedepalumbo,2 Sofia Misuraca,2 Margherita Ori,2 Mattia Nigro,3,4 Edoardo Simonetta,4 Stefano Aliberti,3,4 Francesco Blasi1,2
1Department of Pathophysiology and Transplantation, University of Milan, Milan, Italy; 2Respiratory Unit and Cystic Fibrosis Adult Centre, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milan, Italy; 3Department of Biomedical Sciences, Humanitas University, Milan, 20072, Italy; 4IRCCS Humanitas Research Hospital, Respiratory Unit, Milan, 20089, Italy
Correspondence: Chiara Premuda, Respiratory Unit and Cystic Fibrosis Adult Centre, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Via Francesco Sforza, 35, Milano, Italy, Tel +39 0255032020, Email [email protected]
Abstract: Neutrophilic airway inflammation is a key pathogenic driver of bronchiectasis, sustaining a vicious cycle of infection, mucus obstruction, recurrent exacerbations and progressive airway damage. The growing knowledge on the neutrophilic bronchiectasis endotype has led to increasing interest in host-directed approaches targeting neutrophilic mediators. Long-term macrolide therapy currently represents the reference anti-inflammatory treatment for patients with bronchiectasis at high risk of exacerbations and is supported by randomized controlled trials and extensive clinical experience. However, its use is limited by antimicrobial resistance, drug–to-drug interactions, safety concerns in selected populations and uncertainty regarding optimal dosing and duration. More recently, inhibition of Cathepsin C (CatC), an upstream regulator of neutrophil serine protease activation, has emerged as a novel therapeutic strategy aimed at reducing protease-driven airway injury. This manuscript presents a focused review of the literature that critically examines and compares long-term macrolides and CatC inhibitors with respect to their mechanisms of action, clinical evidence, safety profiles and potential roles within future treatment algorithms. We summarize data from Phase II and III trials of CatC inhibitors, particularly brensocatib, highlighting their effects on exacerbation risk, lung function trajectories and biomarkers of neutrophilic inflammation. We also discuss the limitations of the current evidence base, including restricted trial populations, limited long-term data and the lack of validated biomarkers to guide treatment selection in clinical practice. Finally, we discuss future perspectives for integrating these therapies into individualized, biomarker-informed management of bronchiectasis. Together, these developments support a shift towards more mechanism-based and personalized anti-inflammatory treatment strategies in bronchiectasis, in which treatment selection is guided by underlying inflammatory pathways. This review aims to translate current clinical evidence into practical considerations for patient selection and future therapeutic positioning, thereby helping bridge the gap between research and clinical implementation.
Keywords: bronchiectasis, neutrophilic inflammation, cathepsin C, brensocatib, macrolides, DPP1 inhibitors, protease imbalance, host-directed therapy
Introduction
Neutrophilic airway inflammation represents a central pathogenic mechanism across several chronic respiratory diseases, including bronchiectasis, cystic fibrosis (CF), and chronic obstructive pulmonary disease (COPD).1,2 In bronchiectasis, persistent neutrophilic activation drives a self-perpetuating cycle in which infection, inflammation, and airway damage continuously reinforce one another.2
Despite the widespread use of inhaled antibiotics, airway clearance techniques, and existing anti-inflammatory interventions, many patients remain stuck in this vicious cycle and continue to experience high burden of symptoms, recurrent exacerbations and structural deterioration.
Over the past decade, growing evidence has shifted the therapeutic focus from a predominantly infection-centered perspective to a broader view in which inflammation, especially neutrophilic, emerges as a major contributor to disease progression.3 The intense and sustained neutrophilic inflammation characteristic of bronchiectasis leads to to excessive release of neutrophil serine proteases (NSPs), which exceed the capacity of endogenous antiprotease defenses and remain biologically active in the airway environment.2 As a consequence, protease activity contributes to structural lung injury, impaired mucociliary clearance, and increased susceptibility to persistent bacterial infection. Importantly, this neutrophil-driven inflammatory activity is not limited to acute exacerbations but persists over time, representing a stable and ongoing component of the disease process.2,4
This paradigm shift has led to increasing interest in pharmacological strategies that can modulate the inflammatory cascade. Two main therapeutic routes have gained prominence in this context. The first is long-term macrolide therapy, which has established anti-inflammatory and immunomodulatory properties in addition to its antimicrobial actions, and is now recommended for patients at high risk of exacerbations.5 More recently, a second approach has emerged: the inhibition of Cathepsin C (CatC - also known as dipeptidyl peptidase 1, DPP-1), an upstream regulator responsible for the activation of NSPs. By targeting this early step in neutrophil maturation, DPP-1 inhibitors offer a novel, host-directed strategy aimed at reducing the proteolytic burden that contributes to airway injury.
This review compares these two therapeutic approaches focusing on their mechanisms, clinical evidence, potential benefits, and limitations. Particular attention is given to the evolving concepts of patient selection, safety considerations, and practical incorporation into treatment pathways. Extending beyond current evidence, this review specifically addresses the anticipated post-approval positioning of brensocatib within bronchiectasis management and offers a structured comparison between CatC inhibition and chronic macrolide therapy, highlighting their potential roles within future treatment algorithms. This review seeks to clarify how targeted modulation of airway inflammation may translate into more individualized clinical decision-making and ultimately modify the therapeutic landscape of bronchiectasis in the coming years.
Long-Term Macrolides
Mechanistic Rationale
After the landmark paper by Kudoh et al in 1998, which first proposed the use of macrolides as anti-inflammatory agents for treating diffused panbronchiolitis, the molecular rationale of this treatment has been broadly explored6 Over the years, macrolides have proved to be effective in modulating inflammation by disrupting pro-inflammatory signaling pathways of airway epithelial cells, monocytes, macrophages, and dendritic cells. At the intracellular level, they inhibit key signaling cascades such as Nuclear Factor kappa B (NF-κB), Extracellular signal-Regulated Kinase (ERK1/2), and c-Jun N-terminal Kinase (JNK), thereby reducing transcription and release of pro-inflammatory cytokines such as interleukin-1 beta (IL-1β), interleukin-6 (IL-6), interleukin-8 (IL-8), and tumor necrosis factor-alpha (TNF-α).7,8 They can also impair pattern recognition receptor (PRR) signaling by reducing toll-like receptor (TLR) surface expression in dendritic cells and macrophages and they can hamper inflammasome activation by inhibiting endosome acidification.8,9 From an extracellular perspective, macrolides decrease neutrophil chemotaxis and infiltration by inhibiting the production of chemokines, adhesion molecules, and Granulocyte-Macrophage Colony-Stimulating Factor (GM-CSF).10 Timely apoptosis of neutrophils is induced, and macrophage differentiation is shifted toward an anti-inflammatory phenotype.7 Azithromycin and erythromycin also proved to interfere with the process of Gram-negative bacteria biofilm formation, such as in the case of Pseudomonas aeruginosa. At sub-inhibitory concentrations they suppress the transcription of key quorum sensing genes (lasI, rhlI) decreasing the production of Acyl-Homoserine Lactone (AHL), which determines population density and coordinates bacterial group behaviors including biofilm formation, production of virulence factors, and antibiotic resistance.11 Finally, by downregulating mucin gene expression (particularly MUC5AC) and reducing goblet cell hyperplasia, they also decrease mucus viscosity and stagnation.12
The effects of chronic macrolide therapy go therefore far beyond the simple antimicrobial action and target several pillars of the vicious cycle of bronchiectasis, resulting in a reduction in exacerbation frequency.13
Clinical Evidence
International guidelines from the British Thoracic Society (BTS) and the European Respiratory Society (ERS) recommend long-term macrolide therapy for patients with bronchiectasis who have a high exacerbation rate2,14 or are at high risk of exacerbations,3 regardless of their chronic airway infection state. While earlier guidelines primarily based macrolide use on exacerbation frequency,14,15 the 2025 update recognizes that exacerbation count alone is not the only predictor. A high burden of daily symptoms and additional clinical risk factors are now recognized as contributors to exacerbation risk.5,16
This indication is based on the evidence coming from three pivotal, small-sized double-blind randomized controlled trials (RCTs) and subsequent review and meta-analysis. The EMBRACE study, conducted in New Zealand in 2012 by Wong et al, was the first RCT evaluating the efficacy of azithromycin (AZM) 500 mg three times per week against placebo in reducing pulmonary exacerbations in six months in people with bronchiectasis. They demonstrated a 62% reduction in exacerbations compared to placebo and an improvement in the symptom component of the Saint-George Respiratory Questionnaire (SGRQ).17 In 2013, the BAT study was performed in the Netherlands by Altenburg et al, comparing the efficacy of AZM 250 mg daily against placebo in reducing exacerbations over the 12 months of study period18 Results showed a significant reduction in the number of infectious exacerbations in the subgroup treated with AZM (median 0; IQR 0–1) compared to the placebo group (median 2; IQR 1–3). In addition to clinical outcomes, C-reactive protein (CRP) and white blood cell count were evaluated as potential biomarkers of treatment response; however, no significant differences were observed between the AZM and placebo groups. Interestingly, sputum microbiology analyses showed a higher prevalence of macrolide-resistant organisms among patients exposed to AZM.18 The same year, Serisier and his group published data of the BLESS study conducted in Australia.19 They compared the annualized rate of pulmonary exacerbations in bronchiectasis patients treated with erythromycin 400 mg twice daily to the rate in the placebo group. Patients receiving the treatment experienced a significant reduction in pulmonary exacerbations with mean 1.29 [95% CI, 0.93–1.65] exacerbations per patient per year versus 1.97 [95% CI, 1.45–2.48] in the placebo group. A subgroup analysis conducted on P. aeruginosa infected patients demonstrated a mean of 1.32 (95% CI, 0.19–2.46) reduction in exacerbations/year. Daily sputum production also decreased, and the lung function decline was attenuated. In this study, CRP was also assessed as a secondary outcome, but similarly to BAT it did not differ significantly between treatment and placebo groups. Microbiological analyses showed no differences in the emergence of new pathogens in sputum cultures between groups; however, sputum samples from patients treated with erythromycin showed a greater tendency toward bacterial eradication, possibly reflecting the dual anti-inflammatory and antimicrobial role of macrolides.19 Interestingly, the proportion of macrolide resistant oropharyngeal streptococci was 25.5% higher in the treatment arm.19
A review and individual participant data (IPD) meta-analysis on the topic was published in 2019 by Chalmers et al,13 confirming that long-term macrolide therapy (6–12 months) significantly reduces the frequency of exacerbations (adjusted incidence rate ratio 0.49, 95% CI 0.36–0.66), prolongs time to first exacerbation, and improves quality of life measured with SGRQ. Regarding safety, the analyzed trials reported no major concerns, and antimicrobial resistance was not deemed a significant issue.5 Despite the increase in macrolide resistance reported by the BLESS study,19 subsequent meta-analysis and multicenter studies have shown that it has not translated into clinically significant adverse outcomes.13,20,21 Further research is however needed to address long-term safety profiles, define an optimal monitoring strategy, understand the optimal molecule and dosage and address the issue of safe discontinuation.
Limitations and Safety Concerns
Although macrolides have demonstrated clear efficacy and no major safety concerns were reported in the trials, their long-term use still warrants careful patient selection and regular monitoring. This is especially important given that many studies excluded patients with a higher baseline risk of macrolide-associated adverse events.5
One of the biggest concerns is the induction of antimicrobial resistance in the long term. Although not observed in trials of 6–12 months duration,5 macrolide resistance may potentially emerge, not only for respiratory pathogens, but also within the commensal oropharyngeal and gut microbiota.21 Concerning anti-microbial resistance, an important risk to consider is the interaction between long-term macrolide exposure and non-tuberculous mycobacteria (NTM). Since macrolides are key drugs for the treatment of many NTM species, prolonged macrolide monotherapy could drive the emergence of macrolide-resistant strains, compromising future therapeutic options.22 International guidelines advise systematic NTM screening before starting macrolide treatment and prompt discontinuation if NTM disease is identified.5,14 This is especially important to bear in mind given that bronchiectasis often provides a favorable environment for NTM infection and pulmonary disease.22
Adverse events may also represent important limitations. Gastrointestinal intolerance, including diarrhea, nausea, abdominal pain, and dysgeusia, occurs in approximately 15–40% of patients, although not always leading to treatment discontinuation.21,23 Cardiovascular safety is another critical concern. Macrolides can prolong the QT interval and predispose susceptible individuals to ventricular arrhythmias, particularly in the presence of structural cardiac disease, electrolyte abnormalities, or concurrent QT-prolonging drugs.21,23 Although more recent analyses provide reassurance regarding the absolute risk, they also emphasize the importance of baseline electrocardiogram (EKG) assessment and periodic monitoring in high-risk patients.5 Ototoxicity, typically reversible and presenting as sensorineural hearing loss or tinnitus, has also been reported with long-term macrolide use and appears more common in older adults or those with pre-existing auditory impairment.24
Drug–to-drug interactions represent an additional challenge. Macrolides may act as potent inhibitors of CYP3A4 and alter the pharmacokinetics of statins, anticoagulants, calcium-channel blockers, and antiarrhythmics, necessitating careful dose adjustment and clinical vigilance in polymedicated patients.25
Finally, another factor potentially limiting the widespread use of this treatment is the paucity of data on the optimal choice of macrolide agent, dosing and duration of treatment. Existing trials have used different molecules and dosing strategies with follow-up limited to 12 months.17–19 As a result, variability in clinical practice is to be expected and defining the most effective and safest regimens represents an important area for future research. Real-world evidence also suggests that long-term adherence may decline due to persistent low-grade adverse effects and the burden of chronic therapy. Enhancing adherence requires structured patient education, shared decision-making, and periodic clinical reassessment.5
Candidate Profile
In patients with bronchiectasis, determining the characteristics that support long-term macrolide therapy is a key clinical consideration. Previous ERS guidelines recommended macrolides mainly for patients without P. aeruginosa infection or for those who could not use inhaled antibiotics.15 The 2025 update now extend macrolide therapy to all patients at high risk of exacerbations despite standard treatment regardless of P. aeruginosa infection.5 This aligns with clinical experience in CF, where macrolides reduce exacerbations regardless of chronic P. aeruginosa infection.26,27 In addition, the previously cited IPD meta-analysis explored whether specific clinical subgroups experienced greater benefit from long-term macrolide therapy.13 The authors observed numerically larger reductions in exacerbation rates among several groups, including older adults, individuals with one or two exacerbations per year, patients at the extremes of body weight, those with elevated baseline CRP, and patients infected with P. aeruginosa. However, none of these subgroup differences reached statistical significance, indicating that the treatment effect of macrolides was not meaningfully modified by these characteristics. Taken together, these findings suggest that clear clinical or biological biomarkers identifying the patients most likely to benefit from long-term macrolide therapy are still lacking. Patients with more severe respiratory symptom scores (QoL-B-RSS) may also derive substantial benefit.16
Cathepsin C Inhibitors
Mechanistic Rationale
Growing interest in therapeutic strategies that modulate neutrophil activity has focused attention on CatC inhibition as a mean of suppressing upstream activation of NSPs.28–30 In bronchiectasis, excessive release of NSPs, particularly Neutrophil Elastase (NE), Proteinase 3 (PR3) and Cathepsin G (CatG), plays a central role in airway injury and disease progression.28,29,31 NE drives tissue damage through degradation of structural proteins such as elastin and collagen, increases mucus viscosity by upregulating MUC5AC and promotes goblet-cell hyperplasia.28,32 PR3 amplifies inflammation by activating pro-IL-1β, TNF-α and IL-8, thereby perpetuating neutrophil recruitment,31,33 while CatG contributes to extracellular matrix degradation and interleukin-36 (IL-36) activation, promoting airway remodelling.30,31 Consistently, elevated sputum NE activity correlates with disease severity, frequent exacerbations, and accelerated decline in forced expiratory volume in one second (FEV1)underscoring the pathogenic importance of NSPs.18,34
Under physiological conditions, NSPs are stored as inactive zymogens and are tightly regulated by endogenous inhibitors such as Alpha1-Antitrypsin (A1AT), Secretory Leukoprotease Inhibitor (SLPI) and Elafin. In bronchiectasis, however, NE and PR3 degrade these antiproteases, perpetuating a protease–antiprotease imbalance that sustains inflammation and tissue injury.31 Conventional anti-inflammatory therapies, including macrolides and corticosteroids, do not directly prevent NSPs activation. In contrast, CatC inhibition acts upstream by blocking the maturation of all three major NSPs within neutrophil precursors before their release into the circulation.35–37 CatC is highly expressed in bone-marrow myeloid cells, where it removes N-terminal dipeptides from NSP pro-enzymes during neutrophil maturation, generating their active forms. When CatC is absent or pharmacologically inhibited, neutrophils fail to develop mature NE, PR3, and CatG, resulting in a marked reduction in proteolytic activity.35–37 CatC-deficient mice are protected from inflammatory arthritis and glomerulonephritis with substantially reduced NSP activity and no evidence of severe immunodeficiency.38 Together, these data suggest that partial, reversible CatC inhibition can attenuate pathological protease activity while preserving host defense, reducing mucus burden, improving mucociliary clearance and limiting airway destruction.28,30,34
Several CatC inhibitors have been developed over recent years. The early irreversible inhibitor GSK2793660 provided proof-of-concept, but was associated with dose-limiting skin toxicity.39 This led to the development of reversible covalent inhibitors such as brensocatib (AZD7986) and BI 1291583, designed to achieve longer half-life and bone-marrow selectivity.40,41 More recently, the non-peptidyl, non-covalent inhibitor HSK31858 has demonstrated potent and well-tolerated suppression of NSP activity in early clinical studies.42 Collectively, these advances position CatC inhibition as a mechanistically targeted, next-generation strategy to address neutrophil-driven pathology in bronchiectasis, potentially complementing and surpassing the broad anti-inflammatory effects achieved with macrolide therapy.
Clinical Evidence
Brensocatib is a reversible, covalent nitrile CatC inhibitor originally developed as AZD7986 and subsequently licensed as INS1007.29,40 Preclinical studies demonstrated that brensocatib selectively inhibits its target with minimal activity against other cathepsins, resulting in dose-dependent reductions in bone-marrow NE, PR3, and CatG activity.29,40 The phase II WILLOW trial (NCT03218917) provided the first robust clinical evidence of efficacy in people with bronchiectasis.43 In this multicenter, randomized, double-blind, placebo-controlled study, 256 adults with bronchiectasis, chronic sputum production and ≥2 exacerbations in the previous year were randomized to placebo or brensocatib 10 mg or 25 mg once daily for 24 weeks. Both doses significantly prolonged time to first exacerbation compared with placebo, with hazard ratios of 0.58 (95% CI 0.35–0.95; p=0.03) for 10 mg and 0.62 (95% CI 0.38–0.99; p=0.046) for 25 mg.43 Post hoc analyses suggested that the benefit of brensocatib was consistent irrespective of macrolide concomitant therapy or eosinophilic disease status.44 Adverse events of special interest, including hyperkeratosis and dental/periodontal events, were more frequent in the brensocatib-treated arms, but they were predominantly mild and rarely led to treatment discontinuation. The Phase III ASPEN trial (NCT04594369) extended these findings to a larger and more heterogeneous population. This study enrolled more than 1600 participants with bronchiectasis, including a small adolescent cohort, all with ≥2 exacerbations in the preceding year. Participants were randomized to placebo, brensocatib 10 mg or brensocatib 25 mg once daily for 52 weeks.45 Both doses reduced the annualized exacerbation rate compared with placebo (21% reduction with 10 mg and 19% reduction with 25 mg) and prolonged time to first exacerbation. In addition, the 25 mg dose was associated with a slower decline in lung function over one year compared with placebo. The safety profile was consistent with that observed in the phase II study, with no increase in serious infections. Taken together, the WILLOW and ASPEN trials support brensocatib as a potential disease-modifying anti-inflammatory therapy in bronchiectasis and support CatC inhibition as a therapeutic strategy for neutrophil-mediated lung disease.28–30
BI 1291583 is a potent and selective CatC inhibitor that binds human CatC in a reversible covalent manner, leading to dose-dependent suppression of NE and PR3 activation, while preserving neutrophil viability without cytotoxicity.41 Its clinical efficacy was evaluated in the phase II AIRLEAF trial (NCT05238675), a randomized, double-blind, placebo-controlled, dose-finding study that enrolled 322 adults with bronchiectasis.46 Eligible participants had either a history of at least two exacerbations in the previous year or one exacerbation accompanied by a high symptom burden. Participants received placebo or BI 1291583 at doses of 1 mg, 2.5 mg or 5 mg once daily for 24–48 weeks. The study met its primary endpoint, demonstrating a significant, dose-dependent prolongation in time to first exacerbation. The greatest clinical benefit was observed in those treated with higher doses of the drug, also associated with improvements in lung function and quality-of-life compared with placebo. These findings indicate that CatC inhibitors may be effective also in those individuals with a high symptom burden. Importantly, BI 1291583 was generally well tolerated with a safety profile comparable to placebo and no evident increase in dermatologic or periodontal adverse events. A phase III randomized controlled trial is currently recruiting adults with bronchiectasis to further evaluate the efficacy and safety of BI 1291583 over a 76-week treatment period, with annualized rate of pulmonary exacerbations as the primary endpoint (NCT06872892).
HSK31858 represents a next-generation, non-peptidyl, non-covalent DPP-1 inhibitor.29 The phase II SAVE-BE trial (NCT05601778) is a single-country, multicenter, randomized, placebo-controlled study investigating HSK31858 in adults with bronchiectasis.47 This trial enrolled more than 200 patients in China with a history of ≥2 exacerbations in the previous year. Preliminary findings show that HSK31858 significantly reduced exacerbation frequency and prolonged time to first exacerbation compared with placebo. Treatment was also associated with marked reductions in NSPs activity in blood and sputum, along with decreases in daily sputum production, indicating potential effects on both neutrophilic inflammation and mucus burden. No concerning signals of hyperkeratosis or periodontal disease have been observed to date and overall tolerability appears excellent. However, the geographic and ethnic specificity of the study population should be considered, as treatment responses may differ in broader and more diverse patient cohorts.
Clinical Advantages of CatC Inhibition
CatC inhibition represents an emerging therapeutic strategy in bronchiectasis and offers a number of clinical advantages that may complement (or overcome) the established role of long-term macrolide therapy. Although the evidence supporting macrolides is solid, their use is limited by the previously recognized limitations. By contrast, CatC inhibitors are a more recent therapeutic class; while clinical evidence is currently limited to clinical trials, available data suggest a promising therapeutic profile.
A key advantage of CatC inhibitors lies in their mechanism of action, which targets the inflammatory cascade at an upstream level.28,30 Because CatC inhibitors do not rely on antimicrobial activity, they do not carry the same risk of promoting antimicrobial resistance associated with long-term macrolide use. This feature is particularly relevant in chronic airway diseases such as bronchiectasis, where prolonged antibiotic exposure is common and the emergence of multidrug-resistance represents an increasing clinical challenge. Another potential advantage is the possibility of monitoring CatC inhibition through the use of biomarkers. In clinical studies, the reduction in sputum NE activity has served as indicator of pharmacodynamic effect and may help identify patients who are more likely to benefit from treatment, as well as those who show limited response and might need a change in therapy.43
Across clinical trials, CatC inhibitors have been associated with mild adverse events that only rarely required discontinuation. Consequently, CatC inhibition may represent a suitable therapeutic option for patients who are unable to initiate macrolides or who discontinue them due to intolerance or contraindications. Importantly, post-hoc analysis of the WILLOW study showed that the clinical benefits of brensocatib were observed irrespective of background macrolide use, suggesting that CatC inhibitors may be considered as add-on option in patients who remain symptomatic or continue to experience exacerbations despite optimized treatment.45,48
Finally, a further potential advantage of CatC inhibitors is their limited impact on drug–drug interactions. Unlike macrolides, which are potent inhibitors of CYP3A4 and may interfere with commonly prescribed therapies, CatC inhibitors do not seem to significantly affect major metabolic pathways.25 This characteristic becomes relevant in older patients with multiple comorbidities, in whom polypharmacotherapy often constrains therapeutic choices.
Limitations and Open Questions
Despite the encouraging results reported in recent trials, important limitations should be considered when evaluating the role of CatC inhibitors in routine clinical practice.
First, the current evidence base derives exclusively from RCT conducted under controlled conditions and with restrictive inclusion and exclusion criteria. Patients with significant comorbidities, advanced organ dysfunction, or active NTM disease are typically excluded. As a result, trial populations may not fully represent the clinical heterogeneity of bronchiectasis seen in real-world settings, where patients are often older, have multiple comorbidities, and receive several concomitant therapies. It therefore remains uncertain to what extent the efficacy and safety signals observed in trials will translate to routine clinical practice.
Second, long-term data remain limited. Although the ASPEN trial provides one year of follow-up and substantially advances current knowledge, bronchiectasis is a chronic, lifelong condition.45 It is still unclear whether the benefits of CatC inhibition are sustained with prolonged treatment over multiple years, or whether treatment discontinuation or cycling strategies may be appropriate. The long-term safety profile has not yet been fully characterized. While adverse events appear generally mild in the short to medium term, their cumulative burden over time and potential for delayed toxicity require further investigation, especially with broader post-marketing use.
Third, the use of biomarkers as indicators of treatment response presents additional challenges. Although reductions in NE activity correlate with pharmacodynamic effect, this biomarker is not routinely available and assay methods across studies lack standardization across centers. Variability in sample collection, processing, analytical platforms and ranges limit comparisons across sites. Moreover, no data or validated measures are currently available to quantify drug impact on disease activity or to identify potential non-responders in clinical practice. Until these methodological gaps are addressed and clear thresholds established, biomarker-guided treatment decisions remain challenging outside research setting.
Candidate Patient Profile
Current guidelines identify patients with deteriorating disease or at increased risk of exacerbations as key candidates for long-term anti-inflammatory treatment with macrolides.5 As the available evidence was limited and regulatory approval was not received at the time these recommendations were developed, the guidelines did not address the use of CatC inhibitors.
Despite these constraints, the mechanism of action of CatC inhibitors, together with emerging clinical evidence, allows a preliminary profiling of the patient groups most likely to benefit from this therapeutic class. Patients with persistent neutrophilic inflammation, manifested by recurrent exacerbations, daily symptoms, or elevated NE activity where available, represent a plausible target population. CatC inhibitors may be particularly useful as an adjunct or an alternative in individuals who do not achieve sufficient disease control with long-term macrolides because of limited clinical response, intolerance or safety concerns. They also may provide a potential therapeutic option for patients with contraindications to macrolides, including those with NTM infection or other conditions that preclude the safe use of chronic antibiotic therapy. A comparative clinical overview of macrolides and CatC inhibitors is provided in Table 1.
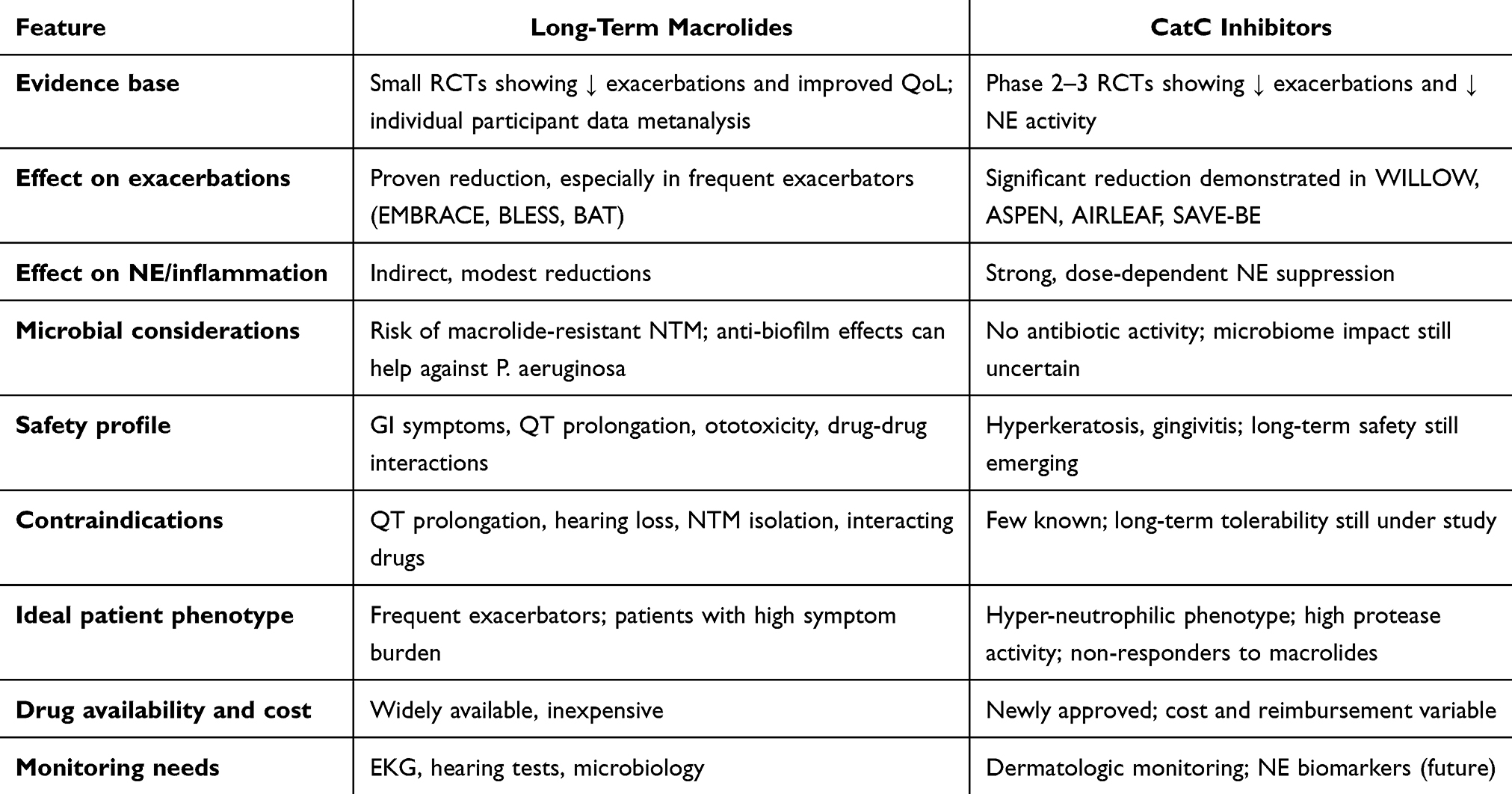 |
Table 1 Comparative Appraisal: Macrolides versus CatC Inhibitors |
In addition, data emerging from the ASPEN trial suggest a broader potential role for CatC inhibition. The observed dose-dependent reduction in MUC5AC expression and the slower FEV1 decline suggest the drug may also influence mucus biology and long-term lung function trajectories, although these findings require confirmation. These findings could support earlier intervention in the disease course, particularly in patients with prominent mucus hypersecretion or evidence of accelerated functional deterioration.16,45 Although these findings require confirmation, they point toward a wider therapeutic window for CatC inhibition than previously assumed.
Future Perspectives and Clinical Implications
The recent approval of brensocatib by both the FDA and the EMA marks an important milestone forward in the treatment of bronchiectasis, introducing the first anti-inflammatory agent with the potential to modify disease progression through a mechanism distinct from antimicrobial therapy. However, the practical clinical implications are not yet fully defined. The extent to which CatC inhibitors will be adopted in routine clinical practice is likely to vary across countries, influenced by national regulatory frameworks, reimbursement policies and drug costs.48 In the absence of updated guidelines, clinical use is expected to remain heterogeneous, informed by patient-specific disease characteristics and shared decision-making between clinicians and patients. At present, no standardized algorithms exist and it remains uncertain whether brensocatib will ultimately replace long-term macrolides in selected phenotypes, be used in complement, or be reserved for specific patient subgroups.
In the short term, an individualized treatment approach is likely to predominate while awaiting more robust real-world evidence and the development of validated biomarkers to guide therapeutic selection. Several potential strategies may emerge. Long-term macrolides may continue to represent first-line therapy for patients at high risk of exacerbations, particularly in settings where regulatory approval or reimbursement pathways for CatC inhibitors are prolonged or uncertain. Another option is that CatC inhibitors could be considered as first-line agents in individuals with evidence of neutrophilic inflammation. A third, more exploratory, approach may involve the combined use of macrolides and CatC inhibitors in selected patients with more severe disease or in those with an incomplete response to monotherapy, yet this option will require further validation. Finally, CatC inhibitors may represent an alternative strategy to control inflammation and reduce exacerbations in patients with contraindications to macrolides, including patient with NTM infection. However, macrolides may still be preferred in individuals with concurrent bacterial airway infection, given their combined anti-inflammatory and antimicrobial effects.
In routine practice, clinicians are likely to rely on therapies that are most accessible and familiar, progressively moving toward more personalized approaches as clinical experience grows. Mechanisms of action of macrolides and CatC inhibitors are illustrated in Figure 1.
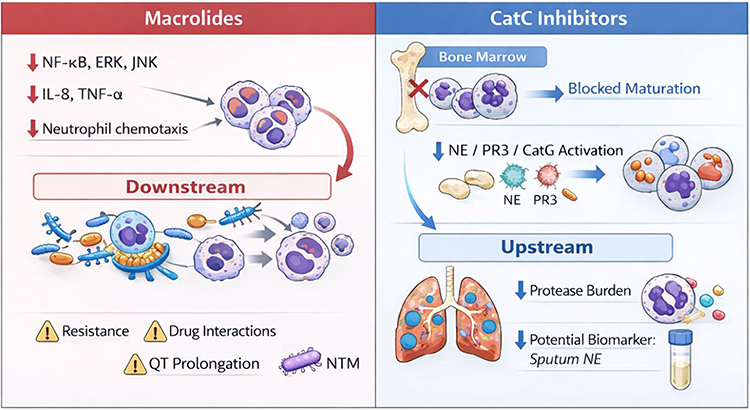 |
Figure 1 Mechanisms of action of macrolides and Cathepsin C inhibitors. Macrolides act downstream in the inflammatory cascade and they have multiple anti-inflammatory and antimicrobial effects. CatC inhibitors act upstream by blocking neutrophil maturation, thus inhibiting the activation of neutrophil serine proteases such as NE, PR3 and CatG. Abbreviations: CatC, Cathepsin C; CatG, Cathepsin G; ERK, Extracellular-signal Regulated Kinase; IL−8, interleukin−8; JNK, c-Jun N-terminal Kinase; NE, neutrophil elastase; NF-κB, Nuclear Factor kappa B; NTM, Non-Tuberculous Mycobacteria; PR3, Proteinase 3; TNF-α, tumor necrosis factor-alpha. |
Exploring Emerging Anti-Neutrophilic Approaches
The encouraging results of clinical trials evaluating CatC inhibitors in bronchiectasis have generated growing interest in extending this therapeutic approach to other diseases characterized by neutrophil-driven inflammation.
Brensocatib (INS1007) has been investigated across a range of inflammatory conditions associated with excessive or dysregulated neutrophilic activity, including COVID-19 (NCT04817332), cystic fibrosis (NCT05090904),49 chronic rhinosinusitis without nasal polyps (NCT06013241) and hidradenitis suppurativa (NCT06685835). Similarly, the safety and tolerability of BI 1291583 have been evaluated in individuals with cystic fibrosis–related bronchiectasis in a phase II study (NCT05865886),50 further supporting the rationale for targeting neutrophilic inflammation in bronchiectasis irrespective of the underlying etiology. In parallel, HSK31858 has been assessed in bronchial asthma (NCT06637254) and in chronic lung diseases characterized by mucus hypersecretion (NCT06820749), suggesting potential applicability in conditions where neutrophilic inflammation and impaired mucociliary clearance coexist. Along this lines, XH-S004, a novel CatC inhibitor, is currently being evaluated in both bronchiectasis (NCT06981091) and COPD (NCT07035652). Although most of these studies remain in early phases of development, their development reflects increasing interest in CatC inhibition as a potential disease-modifying strategy across related inflammatory airway disorders.
In the field of bronchiectasis, therapeutic research is expanding beyond CatC inhibition to target neutrophilic inflammation through multiple complementary strategies. These include trials on direct inhibition of NE using both oral and inhaled agents (NCT06166056),51,52 as well as approaches aimed at limiting neutrophil recruitment via CXCR2 antagonism.53 Although the results of these early-phase studies are heterogeneous and often inconclusive, they collectively reflect a shift toward host-directed anti-inflammatory therapies in bronchiectasis. Nevertheless, the available evidence remains preliminary and exploratory, and further large-scale randomized studies will be required before these strategies can be translated into clinical practice.
Conclusions and Key Messages
Long-term macrolides currently remain the reference anti-inflammatory therapy for bronchiectasis patients at high risk of exacerbations, supported by a limited number of randomized controlled trials and extensive clinical experience. In parallel, CatC inhibitors represent an emerging class of host-directed therapies that act upstream of the neutrophil cascade, offering a mechanistically distinct option for individuals with prominent neutrophilic inflammation or intolerance to macrolides, although limited by the absence of real-life studies.
Key research priorities in the near future include the identification of reliable biomarkers to predict treatment response and pharmacological studies evaluating potential combination strategies. This will include comparative trials directly assessing macrolides versus CatC inhibitors, as well as studies exploring their complementary use.3
Looking ahead, treatment algorithms in bronchiectasis are likely to evolve toward biomarker-informed approaches that integrate measures of sputum protease activity, exacerbation patterns, and infection phenotype to better individualize therapy. The feasibility of widespread implementation will depend on economic considerations, the accumulation of long-term safety data and insights derived from real-world use following regulatory approval. Taken together, these developments point toward a shift to more precise, mechanism-based care in bronchiectasis.
Declaration of Artificial Intelligence (AI) Use
The authors declare using AI (ChatGPT version 4.1) to rephrase some sentences in order to avoid unnecessary repetitions.
Data Sharing Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Individual contributions are stated below:
Andrea Gramegna, Chiara Premuda: conceptualization, investigation, writing (original draft)
Gianmarco Putti, Federica Viola Piedepalumbo, Sofia Misuraca: investigation, writing (original draft)
Margherita Ori, Mattia Nigro, Edoardo Simonetta, Stefano Aliberti: investigation, writing (review and editing)
Francesco Blasi: conceptualization, supervision, writing (review and editing).
Funding
The authors did not receive fundings related to this review.
Disclosure
AG declares payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Chiesi, Insmed and Vertex, support for attending meetings and/or travel from Chiesi, participation on a Data Safety Monitoring Board or Advisory Board from Insmed and Vertex and leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid as ECFS Director SOC working group. CP declares leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid as ERS Early Career Member Representative – Assembly 10 (Respiratory Infections) and Chair of the Early Career Member Committee in ERS. GP, FVP, MO and ES declare no conflicts of interest. SM declares payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Zambon and support for attending meetings and/or travel from Menarini. MN declares Participation on a Data Safety Monitoring Board or Advisory Board for Insmed, Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid in EMBARC, in the ERS task force on the management of bronchiectasis and in the ERS task force on chronic pulmonary aspergillosis. SA declares grants GSK, consulting fees from Insmed Incorporated, Insmed Netherlands and GSK, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Insmed Netherlands, Insmed Germany, Physioassist, Boehringer Ingelheim Italia, Boehringer Ingelheim International, Thermo Fisher Scientific, Zambon, Sanofi, Providens Doo, Pfizer, Limare, GSK, Chiesi and Vertex, participation on data safety monitoring board or advisory board for GSK, Boehringer Ingelheim Italia, Moderna Italy, Zambon, Chiesi, Insmed Incorporated, Insmed Netherlands, AN2 therapeutics, ModernaTx and Boehringer Ingelheim International.
FB declares grants from Astrazeneca, Chiesi and Insmed, consulting fees from Menarini, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Astrazeneca, Chiesi, Boehringer Ingelheim, GSK, Grifols, Insmed, Menarini, MSD, OM Pharma, Pfizer, Sanofi, Vertex and Zambon.
The authors declare no other conflicts of interest in this study.
References
1. Long MB, Chalmers JD. Treating neutrophilic inflammation in airways diseases. Arch Bronconeumol. 2022;58(6):463–13. doi:10.1016/j.arbres.2021.11.003
2. Chalmers JD, Metersky M, Aliberti S, et al. Neutrophilic inflammation in bronchiectasis. Eur Respir Rev. 2025;34(176):240179. PMID: 40174958; PMCID: PMC11962982. doi:10.1183/16000617.0179-2024
3. Long MB, Chotirmall SH, Shteinberg M, Chalmers JD. Rethinking bronchiectasis as an inflammatory disease. Lancet Respir Med. 2024;12(11):901–914. PMID: 38971168. doi:10.1016/S2213-2600(24)00176-0
4. Chalmers JD, Mall MA, Nielsen KG, et al. Neutrophil-derived biomarkers in bronchiectasis: identifying a common therapeutic target. Eur Respir J. 2025;66(3):2500081. PMID: 40639876; PMCID: PMC12441583. doi:10.1183/13993003.00081-2025
5. Chalmers JD, Haworth CS, Flume P, et al. European respiratory society clinical practice guideline for the management of adult bronchiectasis. Eur Respir J. 2025;66(6):2501126. PMID: 41016738. doi:10.1183/13993003.01126-2025
6. Kudoh S, Azuma A, Yamamoto M, Izumi T, Ando M. Improvement of survival in patients with diffuse panbronchiolitis treated with low-dose erythromycin. Am J Respir Crit Care Med. 1998;157(6 Pt 1):1829–1832. PMID: 9620913. doi:10.1164/ajrccm.157.6.9710075
7. Reijnders TDY, Saris A, Schultz MJ, van der Poll T. Immunomodulation by macrolides: therapeutic potential for critical care. Lancet Respir Med. 2020;8(6):619–630. PMID: 32526189. doi:10.1016/S2213-2600(20)30080-1
8. Zimmermann P, Ziesenitz VC, Curtis N, Ritz N. The immunomodulatory effects of macrolides-a systematic review of the underlying mechanisms. Front Immunol. 2018;9:302. PMID: 29593707; PMCID: PMC5859047. doi:10.3389/fimmu.2018.00302
9. Kanoh S, Rubin BK. Mechanisms of action and clinical application of macrolides as immunomodulatory medications. Clin Microbiol Rev. 2010;23(3):590–615. PMID: 20610825; PMCID: PMC2901655. doi:10.1128/CMR.00078-09
10. Bosnar M, Bosnjak B, Cuzic S, et al. Azithromycin and clarithromycin inhibit lipopolysaccharide-induced murine pulmonary neutrophilia mainly through effects on macrophage-derived granulocyte-macrophage colony-stimulating factor and interleukin-1beta. J Pharmacol Exp Ther. 2009;331(1):104–113. PMID: 19633061. doi:10.1124/jpet.109.155838
11. Kumar L, Patel SKS, Kharga K, et al. Molecular mechanisms and applications of N-Acyl homoserine lactone-mediated quorum sensing in bacteria. Molecules. 2022;27(21):7584. PMID: 36364411; PMCID: PMC9654057. doi:10.3390/molecules27217584
12. Wang J, Xu L, Lv Y, Sun L. Azithromycin inhibits the production of MUC5AC in the airway mucosa of patients with bronchiectasis induced by Pseudomonas aeruginosa. Pak J Pharm Sci. 2021;34(3(Special):1179–1185. PMID: 34602387.
13. Chalmers JD, Boersma W, Lonergan M, et al. Long-term macrolide antibiotics for the treatment of bronchiectasis in adults: an individual participant data meta-analysis. Lancet Respir Med. 2019;7(10):845–854. PMID: 31405828. doi:10.1016/S2213-2600(19)30191-2
14. Smith D, Du Rand I, Addy CL, et al. British thoracic society guideline for the use of long-term macrolides in adults with respiratory disease. Thorax. 2020;75(5):370–404. PMID: 32303621. doi:10.1136/thoraxjnl-2019-213929
15. Polverino E, Goeminne PC, McDonnell MJ, et al. European respiratory society guidelines for the management of adult bronchiectasis. Eur Respir J. 2017;50(3):1700629. PMID: 28889110. doi:10.1183/13993003.00629-2017
16. Sibila O, Stobo J, Perea L, et al. Symptoms, risk of future exacerbations, and response to long-term macrolide treatment in bronchiectasis: an observational study. Lancet Respir Med. 2025;13(10):911–920. PMID: 40885209. doi:10.1016/S2213-2600(25)00160-2
17. Wong C, Jayaram L, Karalus N, et al. Azithromycin for prevention of exacerbations in non-cystic fibrosis bronchiectasis (EMBRACE): a randomised, double-blind, placebo-controlled trial. Lancet. 2012;380(9842):660–667. PMID: 22901887. doi:10.1016/S0140-6736(12)60953-2
18. Altenburg J, de Graaff CS, Stienstra Y, et al. Effect of azithromycin maintenance treatment on infectious exacerbations among patients with non-cystic fibrosis bronchiectasis: the BAT randomized controlled trial. JAMA. 2013;309(12):1251–1259. PMID: 23532241. doi:10.1001/jama.2013.1937
19. Serisier DJ, Martin ML, McGuckin MA, et al. Effect of long-term, low-dose erythromycin on pulmonary exacerbations among patients with non-cystic fibrosis bronchiectasis: the BLESS randomized controlled trial. JAMA. 2013;309(12):1260–1267. PMID: 23532242. doi:10.1001/jama.2013.2290
20. Kelly C, Chalmers JD, Crossingham I, et al. Macrolide antibiotics for bronchiectasis. Cochrane Database Syst Rev. 2018;3(3):CD012406. PMID: 29543980; PMCID: PMC6494352. doi:10.1002/14651858.CD012406.pub2
21. Nakagawa N, Ito M, Asakura T, Horita N, Obase Y, Mukae H. Efficacy and safety of long-term macrolide therapy for non-cystic fibrosis bronchiectasis: a systematic review and meta-analysis. Respir Investig. 2024;62(6):1079–1087. Erratum in: Respir Investig. 2025 Mar;63(2):224-225. doi: 10.1016/j.resinv.2025.01.002. PMID: 39326270. doi:10.1016/j.resinv.2024.09.004
22. Griffith DE, Aksamit T, Brown-Elliott BA, et al. ATS mycobacterial diseases subcommittee; American thoracic society; infectious disease society of America. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367–416. Erratum in: Am J Respir Crit Care Med. 2007 Apr 1;175(7):744-5. Dosage error in article text. PMID: 17277290. doi:10.1164/rccm.200604-571ST
23. Haworth CS, Bilton D, Elborn JS. Long-term macrolide maintenance therapy in non-CF bronchiectasis: evidence and questions. Respir Med. 2014;108(10):1397–1408. PMID: 25301290. doi:10.1016/j.rmed.2014.09.005
24. Vanoverschelde A, Oosterloo BC, Ly NF, et al. Macrolide-associated ototoxicity: a cross-sectional and longitudinal study to assess the association of macrolide use with tinnitus and hearing loss. J Antimicrob Chemother. 2021;76(10):2708–2716. PMID: 34312676; PMCID: PMC8446930. doi:10.1093/jac/dkab232
25. Abu Mellal A, Hussain N, Said AS. The clinical significance of statins-macrolides interaction: comprehensive review of in vivo studies, case reports, and population studies. Ther Clin Risk Manag. 2019;15:921–936. PMID: 31413581; PMCID: PMC6661989. doi:10.2147/TCRM.S214938
26. Saiman L, Marshall BC, Mayer-Hamblett N, et al; Macrolide Study Group. Azithromycin in patients with cystic fibrosis chronically infected with Pseudomonas aeruginosa: a randomized controlled trial. JAMA. 2003;290(13):1749–1756. PMID: 14519709. doi:10.1001/jama.290.13.1749
27. Saiman L, Anstead M, Mayer-Hamblett N, et al; AZ0004 Azithromycin Study Group. Effect of azithromycin on pulmonary function in patients with cystic fibrosis uninfected with Pseudomonas aeruginosa: a randomized controlled trial. JAMA. 2010;303(17):1707–1715. PMID: 20442386. doi:10.1001/jama.2010.563
28. Chalmers JD, Mall MA, Chotirmall SH, et al. Targeting neutrophil serine proteases in bronchiectasis. Eur Respir J. 2025;65(1):2401050. PMID: 39467608; PMCID: PMC11694565. doi:10.1183/13993003.01050-2024
29. Tang RD, Yue JQ, Chalmers JD, Guan WJ. Dipeptidyl peptidase 1 inhibitors and neutrophilic inflammation in bronchiectasis: a narrative review. J Thorac Dis. 2025;17(7):5347–5360. PMID: 40809229; PMCID: PMC12340295.30. doi:10.21037/jtd-2025-289
30. Johnson E, Gilmour A, Chalmers JD. Dipeptidyl peptidase-1 inhibitors in bronchiectasis. Eur Respir Rev. 2025;34(176):240257. PMID: 40533102; PMCID: PMC12175074. doi:10.1183/16000617.0257-2024
31. Oriano M, Amati F, Gramegna A, et al. Protease-antiprotease imbalance in bronchiectasis. Int J Mol Sci. 2021;22(11):5996. PMID: 34206113; PMCID: PMC8199509. doi:10.3390/ijms22115996
32. Polverino E, Rosales-Mayor E, Dale GE, Dembowsky K, Torres A. The role of neutrophil elastase inhibitors in lung diseases. Chest. 2017;152(2):249–262. PMID: 28442313. doi:10.1016/j.chest.2017.03.056
33. Keir HR, Chalmers JD. Neutrophil extracellular traps in chronic lung disease: implications for pathogenesis and therapy. Eur Respir Rev. 2022;31(163):210241. PMID: 35197267; PMCID: PMC9488971. doi:10.1183/16000617.0241-2021
34. Korkmaz B, Horwitz MS, Jenne DE, Gauthier F. Neutrophil elastase, proteinase 3, and cathepsin G as therapeutic targets in human diseases. Pharmacol Rev. 2010;62(4):726–759. PMID: 21079042; PMCID: PMC2993259. doi:10.1124/pr.110.002733
35. Adkison AM, Raptis SZ, Kelley DG, Pham CT. Dipeptidyl peptidase I activates neutrophil-derived serine proteases and regulates the development of acute experimental arthritis. J Clin Invest. 2002;109(3):363–371. PMID: 11827996; PMCID: PMC150852. doi:10.1172/JCI13462
36. Chalmers JD, Kettritz R, Korkmaz B. Dipeptidyl peptidase 1 inhibition as a potential therapeutic approach in neutrophil-mediated inflammatory disease. Front Immunol. 2023;14:1239151. PMID: 38162644; PMCID: PMC10755895. doi:10.3389/fimmu.2023.1239151
37. Korkmaz B, Lamort AS, Domain R, et al. Cathepsin C inhibition as a potential treatment strategy in cancer. Biochem Pharmacol. 2021;194:114803. PMID: 34678221. doi:10.1016/j.bcp.2021.114803
38. Aghdassi AA, Pham C, Zierke L, Mariaule V, Korkmaz B, Rhimi M. Cathepsin C role in inflammatory gastroenterological, renal, rheumatic, and pulmonary disorders. Biochimie. 2024;216:175–180. PMID: 37758158. doi:10.1016/j.biochi.2023.09.018
39. Miller BE, Mayer RJ, Goyal N, et al. Epithelial desquamation observed in a Phase I study of an oral cathepsin C inhibitor (GSK2793660). Br J Clin Pharmacol. 2017;83(12):2813–2820. PMID: 28800383; PMCID: PMC5698569. doi:10.1111/bcp.13398
40. Palmér R, Mäenpää J, Jauhiainen A, et al. Dipeptidyl peptidase 1 inhibitor AZD7986 induces a sustained, exposure-dependent reduction in neutrophil elastase activity in healthy subjects. Clin Pharmacol Ther. 2018;104(6):1155–1164. PMID: 29484635; PMCID: PMC6282495. doi:10.1002/cpt.1053
41. Kreideweiss S, Schänzle G, Schnapp G, Vintonyak V, Grundl MA. BI 1291583: a novel selective inhibitor of cathepsin C with superior in vivo profile for the treatment of bronchiectasis. Inflamm Res. 2023;72(8):1709–1717. PMID: 37542002; PMCID: PMC10499737. doi:10.1007/s00011-023-01774-4
42. Wang Y, Yu C, Hu M, et al. Safety, tolerability, pharmacokinetics and pharmacodynamics of HSK31858, a novel oral dipeptidyl peptidase-1 inhibitor, in healthy volunteers: an integrated Phase 1, randomized, double-blind, placebo-controlled, single- and multiple-ascending dose study. Br J Clin Pharmacol. 2025;91(8):2262–2272. PMID: 40170587; PMCID: PMC12304798. doi:10.1002/bcp.70027
43. Chalmers JD, Haworth CS, Metersky ML, et al; WILLOW Investigators. Phase 2 Trial of the DPP-1 inhibitor brensocatib in bronchiectasis. N Engl J Med. 2020;383(22):2127–2137. PMID: 32897034. doi:10.1056/NEJMoa2021713
44. Chalmers JD, Loebinger MR, Teper A, et al. Brensocatib in patients with bronchiectasis: subgroup analyses from the WILLOW trial. ERJ Open Res. 2025;11(1):00505–2024. doi:10.1183/23120541.00505-2024
45. Chalmers JD, Burgel PR, Daley CL, et al; ASPEN Investigators. Phase 3 trial of the DPP-1 inhibitor brensocatib in bronchiectasis. N Engl J Med. 2025;392(16):1569–1581. PMID: 40267423. doi:10.1056/NEJMoa2411664
46. Chalmers JD, Gupta A, Chotirmall SH, et al. A Phase 2 randomised study to establish efficacy, safety and dosing of a novel oral cathepsin C inhibitor, BI 1291583, in adults with bronchiectasis: airleaf. ERJ Open Res. 2023;9(3):00633–2022. PMID: 37465817; PMCID: PMC10351677. doi:10.1183/23120541.00633-2022
47. Zhong NS, Qiu R, Cao J, et al; SAVE-BE trial investigators. Effects of the DPP-1 inhibitor HSK31858 in adults with bronchiectasis in China (SAVE-BE): a phase 2, multicentre, double-blind, randomised, placebo-controlled trial. Lancet Respir Med. 2025;13(5):414–424. PMID: 40154523. doi:10.1016/S2213-2600(25)00019-0
48. Nigro M, Aliberti S. Positioning dipeptidyl peptidase-1 inhibitors in bronchiectasis: no drug is an island. Am J Respir Crit Care Med. 2025. PMID: 41052432. doi:10.1164/rccm.202508-2056VP
49. Konstan MW, Tolle JJ, DiMango E, et al. A phase IIa, single-blind, placebo-controlled, parallel-group study to assess safety, tolerability, and pharmacokinetics/pharmacodynamics of brensocatib in adults with cystic fibrosis. Clin Pharmacokinet. 2025;64(10):1561–1574. PMID: 40753522; PMCID: PMC12479633. doi:10.1007/s40262-025-01550-z
50. Badorrek P, Diefenbach C, Kögler H, Eleftheraki A, Seitz F, Hohlfeld JM. Novel cathepsin C inhibitor, BI 1291583, intended for treatment of bronchiectasis: phase I characterization in healthy volunteers. Clin Transl Sci. 2024;17(8):e13891. PMID: 39175217; PMCID: PMC11341832. doi:10.1111/cts.13891
51. Stockley R, De Soyza A, Gunawardena K, et al. Phase II study of a neutrophil elastase inhibitor (AZD9668) in patients with bronchiectasis. Respir Med. 2013;107(4):524–533. PMID: 23433769. doi:10.1016/j.rmed.2012.12.009
52. Watz H, Nagelschmitz J, Kirsten A, et al. Safety and efficacy of the human neutrophil elastase inhibitor BAY 85-8501 for the treatment of non-cystic fibrosis bronchiectasis: a randomized controlled trial. Pulm Pharmacol Ther. 2019;56:86–93. PMID: 30917927. doi:10.1016/j.pupt.2019.03.009
53. De Soyza A, Pavord I, Elborn JS, et al. A randomised, placebo-controlled study of the CXCR2 antagonist AZD5069 in bronchiectasis. Eur Respir J. 2015;46(4):1021–1032. PMID: 26341987. doi:10.1183/13993003.00148-2015
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
LILRB1 Modulates Neutrophil Migration, NETosis, and Inflammation in Drug-Resistant Pseudomonas aeruginosa-Associated Bronchiectasis
Zheng S, Yang S, Huang Y, Hong K, Tang J, Wu X, Qing C, Jiang Y, Lu W, Bao C, Luo J, Kong J
Infection and Drug Resistance 2026, 19:581113
Published Date: 23 February 2026