Back to Journals » Journal of Inflammation Research » Volume 16
Systemic Inflammation Markers Associated with Bone Mineral Density in perimenopausal and Postmenopausal Women
Authors Chen Y ![]() , Yu J, Shi L, Han S, Chen J, Sheng Z, Deng M, Jin X, Zhang Z
, Yu J, Shi L, Han S, Chen J, Sheng Z, Deng M, Jin X, Zhang Z
Received 5 August 2022
Accepted for publication 24 December 2022
Published 22 January 2023 Volume 2023:16 Pages 297—309
DOI https://doi.org/10.2147/JIR.S385220
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monika Sharma
Yijie Chen,1,* Jingjing Yu,2,* Lan Shi,1 Shuyang Han,1 Jun Chen,1 Zhumei Sheng,3 Miao Deng,3 Xuejing Jin,1,3 Zhifen Zhang1,3
1The Fourth School of Clinical Medicine, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 2School of Public Health, Hangzhou Normal University, Hangzhou, People’s Republic of China; 3Department of the Reproductive Endocrinology Division, Hangzhou Women’s Hospital (Hangzhou Maternity and Child Health Care Hospital), Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhifen Zhang; Xuejing Jin, The Fourth School of Clinical Medicine, Zhejiang Chinese Medical University, 548 Binwen Road, Binjiang District, Hangzhou, Zhejiang, 310053, People’s Republic of China, Email [email protected]; [email protected]
Objective: The aim of this research was to determine whether systemic inflammatory indicators, including aggregate index of systemic inflammation (AISI), neutrophils lymphocyte to platelet ratio (NLPR), systemic immune-inflammation index (SII), and systemic inflammation response index (SIRI), are related to bone mineral density (BMD) in perimenopausal and postmenopausal women.
Methods: One hundred and eighty-one perimenopausal and 390 postmenopausal women were enrolled in this cross-sectional study. Continuous variables by analysis of variance and Kruskal Wallis test for comparing the clinical characteristics. Linear regression analysis was conducted to investigate the associations between inflammatory indicators with BMD. The comparison between the subgroups was performed using the nonparametric test and the T-test.
Results: AISI, NLPR, SII, and SIRI quartile values were inversely associated with BMD in menopausal women (P = 0.021; P = 0.047; P < 0.001; P < 0.001, respectively). After adjusting for confounding factors, four inflammatory indicators remained significantly associated with BMD (all P for trend < 0.001). Analysis according to menopausal status demonstrated that AISI, SII, and SIRI were significantly correlated with mean femoral neck BMD in postmenopausal women (P for trend = 0.015, 0.004, and 0.001), but not significantly associated with BMD in perimenopausal women (P for trend = 0.248, 0.054, and 0.352) after adjustment for covariates.
Conclusion: The quartile values of AISI, SII, and SIRI were inversely associated with BMD in postmenopausal women, following adjustment for individual variables, hormone profiles and glucolipid metabolism profiles. AISI, SII, and SIRI have potential to be important tools for screening and prevention of bone loss in menopausal women in future clinical practice.
Keywords: menopause, female, femur neck, cross-sectional studies, regression analysis, inflammation
Introduction
Postmenopausal osteoporosis (PMOP) is a primary disease characterized by increased bone turnover and decreased bone mass with concomitant skeletal fragility, leading to an increased risk of fractures.1 Among women in China ≥40 years, the prevalence of osteoporosis was 20.6% (95% confidence interval, 19.3%–22.0%) in 2021; however, despite the high prevalence of PMOP, only 1.4% of women with osteoporosis received treatment to prevent fractures.2 The prevalence of PMOP is increasing with the aging of the global population, causing a heavy economic and medical burdens.3 Accordingly, it is important to explore prevail biomarkers that can be applied for the early identification of bone loss in menopausal women.
Hip fracture is a very serious health problem for an individual, that often leads to a decline in mobility and may reduce life expectancy.4 Bone loss is closely related to inflammation and the immune system, and the skeletal system is exquisitely sensitive to persistent inflammatory burden.5 Various chronic inflammatory diseases are accompanied by osteoporosis, including osteoarthritis, gout, psoriasis, and rheumatoid arthritis, which can contribute to disability and increased mortality.6–8 Previous studies have indicated that the rapid decrease in estrogen during menopause increases inflammatory responses, which enhance bone resorption and bone remodeling.9–11 Further, the sudden decline of estrogen in older women has a direct negative effect on bone, while postmenopausal women also show gradual development of a chronic low-grade inflammatory state, and the indirect effect of this altered immune status may also contribute to sustained bone destruction.12
There have been extensively studies of blood indexes in patients with osteoporosis, including C reactive protein (CRP) levels, platelet to lymphocyte ratio (PLR), monocyte lymphocyte ratio (MLR) and neutrophil to lymphocyte ratio (NLR).13,14 The systemic immune-inflammation index (SII) is a new inflammation marker that is strongly predictive of tumor prognosis and immune response state.15,16 Clear associations between SII and inflammatory conditions have been observed.17,18 In our previous study, we found that quartile SII levels were negatively correlated with femoral neck bone mineral density (BMD) in postmenopausal women.19 The systemic inflammation response index (SIRI) is reported to be an effective predictor of survival of patients with breast cancer or aneurysmal subarachnoid hemorrhage.20,21 While very few studies have evaluated its relationship with PMOP. Neutrophil to lymphocyte*platelet ratio (NLPR) was reported as a promising predictor of acute kidney injury.22,23 Further, Zinellu et al found that the aggregate index of systemic inflammation (AISI) can predict idiopathic pulmonary fibrosis mortality and guide patient management.24
Data regarding SIRI, NLPR, SII, and AISI in patients with osteoporosis are limited. Here, we aimed to investigate the relationship between these combined systemic indicators of inflammation and BMD and evaluate whether they have potential as markers for early identification of decreased BMD in perimenopausal and postmenopausal women.
Methods
Study Population
This cross-sectional survey was included 571 women, 181 subjects undergoing menopausal transition and 390 subjects with postmenopausal status, determined according to the 2011 Stages of Reproductive Aging Workshop +10 recommendations.25 Menopausal transition is marked by irregular menstrual cycles, while postmenopausal women had experienced natural menopause (no menstrual bleeding for 1 year), accompanied by menopause symptoms. Patients (aged from 40 to 65 years old) were admitted to the clinic of Hangzhou Women’s Hospital from October 2016 to November 2021. The exclusion criteria were as follows: missing more than three laboratory results; taking medication that could affect bone density and bone metabolism; diseases history that could affect bone metabolism, such as hematological diseases, immune diseases, or malignant tumor. The research was approved by the institutional ethics committee of the Hangzhou Women’s Hospital (docket#2021-03-004). All subjects submitted a medical informed consent document and were informed the research purposes. Our manuscript complies with the Declaration of Helsinki.
Biochemical Measurements and Instruments
Venous blood samples (2–3 mL) were collected after overnight fasting for ≥8 h. A Mindray CAL 8000 cell analysis line was used to measure white blood cells (WBC), including neutrophils (N), platelets (PLT), monocytes (M), and lymphocytes (L). Four inflammatory indexes were also calculated to comprehensively reflect individual inflammation status, as follows: AISI = N × PLT × M/L; NLPR = N/(L × PLT); SII = N × PLT/L; and SIRI = N × M/L. Estradiol (E2), follicle stimulating hormone (FSH), luteinizing hormone (LH), total testosterone (T), thyroid-stimulating hormone (TSH) and fasting insulin levels were measured using a chemiluminescence methods (Beckman Coulter UniCel Dxl-800). For perimenopausal women, hormone assessments were performed in days 1–5 of the menstrual cycle. Fasting glucose, triglycerides, high-density lipoprotein (HDL), low-density lipoprotein (LDL), C-reactive protein (CRP), and homocysteine (HCY) levels were measured using a Beckman Coulter AU5821 chemistry analyzer. Biochemical parameters were evaluated using commercially available kits and standard automated laboratory methods, according to relevant protocols. The formula for calculation of homeostatic model assessment index of insulin resistance (HOMA-IR) was as follows: [fasting insulin (pmol/L) × fasting glucose (mmol/L)]/(22.5 × 6.965). A specialist nurse measured patient weight and height, and body mass index (BMI) was calculated as weight/height squared. Femoral neck BMD was measured by dual-energy X-ray absorptiometry (DPX Bravo, Ge Medical Systems China Ltd.). All BMD scans were performed by the same technician and the subjects were not carrying removable metal objects.
Statistical Analysis
BM-SPSS 22.0 statistics (IBM Inc., Armonk, NY, USA) was used for statistical analyses. Data are expressed as mean ± standard deviation. We analyzed continuous variables by analysis of variance (Conforming to homogeneity of variance) and Kruskal-Wallis test (heterogeneity of variance) for comparing the clinical characteristics across quartiles of AISI, NLPR, SII, and SIRI (Q1–Q4, AISI groups; Q5–Q8, NLPR groups; Q9–Q12, SII groups; Q13–Q16, SIRI groups). Multiple comparisons were made between the four groups with statistical significance. The multiple comparison method of parametric test was LSD, and the nonparametric was Nemenyi test, see STables 1–5. Associations between combined inflammatory indices and BMD were assessed using linear regression models. Four models were established to evaluate the possibility of confounding; Model 1 included adjustments for BMI and age; Model 2 was based on model 1, but included further adjustments for FSH, LH, E2, T, and TSH; Model 3 included the adjustments of model 2 plus HCY, CRP, HDL, LDL, and triglycerides; Model 4 included the adjustments in model 3 plus fasting glucose and fasting insulin. Linear trends of inflammatory index quartiles were evaluated by modeling the median values of all quartiles as continuous variables. Subgroup analysis was conducted based on menopause status, and comparisons between the two groups were performed using a nonparametric test (uneven square difference between the two groups) and the T-test. Tests were two-sided and P < 0.05 indicated statistical significance.
Results
Characteristics of Study Participants
Based on relevant data from the 571 participants, we calculated the inflammatory markers, AISI, NLPR, SII, and SIRI, and divided the results for each index into four groups based on quartile values.
Women with AISI values in the highest quartile had significantly higher serum levels of WBC, CRP, triglycerides, fasting glucose, fasting insulin, and HOMA-IR than those in the lower quartiles. In addition, women with AISI levels in higher quartiles had significantly lower BMD (groups Q1–Q4, P = 0.021, one-way ANOVA) (Table 1). Hence, our findings indicated that the higher AISI was significantly associated with lower BMD; however, there were no significant associations of BMD with age, BMI, or serum levels of FSH, LH, total T, TSH, HDL, LDL, or HCY. Regarding NLPR, BMI and LDL differed significantly among groups Q5–Q8, as did femoral neck BMD (P = 0.047) (Table 2); there was no significant difference in other variables. There were significant differences in serum WBC, CRP, fasting glucose, fasting insulin, and HOMA-IR levels among groups Q9–Q12 of SII. Further, there was significant difference in femoral neck BMD among groups Q9–Q12 (P < 0.001); as shown in Table 3, lower BMD was associated with higher SII (0.887, 0.862, 0.853, and 0.832 g/cm2, respectively). There were no significant differences in age, BMI, FSH, LH, E2, total T, TSH, triglycerides, HDL, LDL, or HCY among the four SII groups.
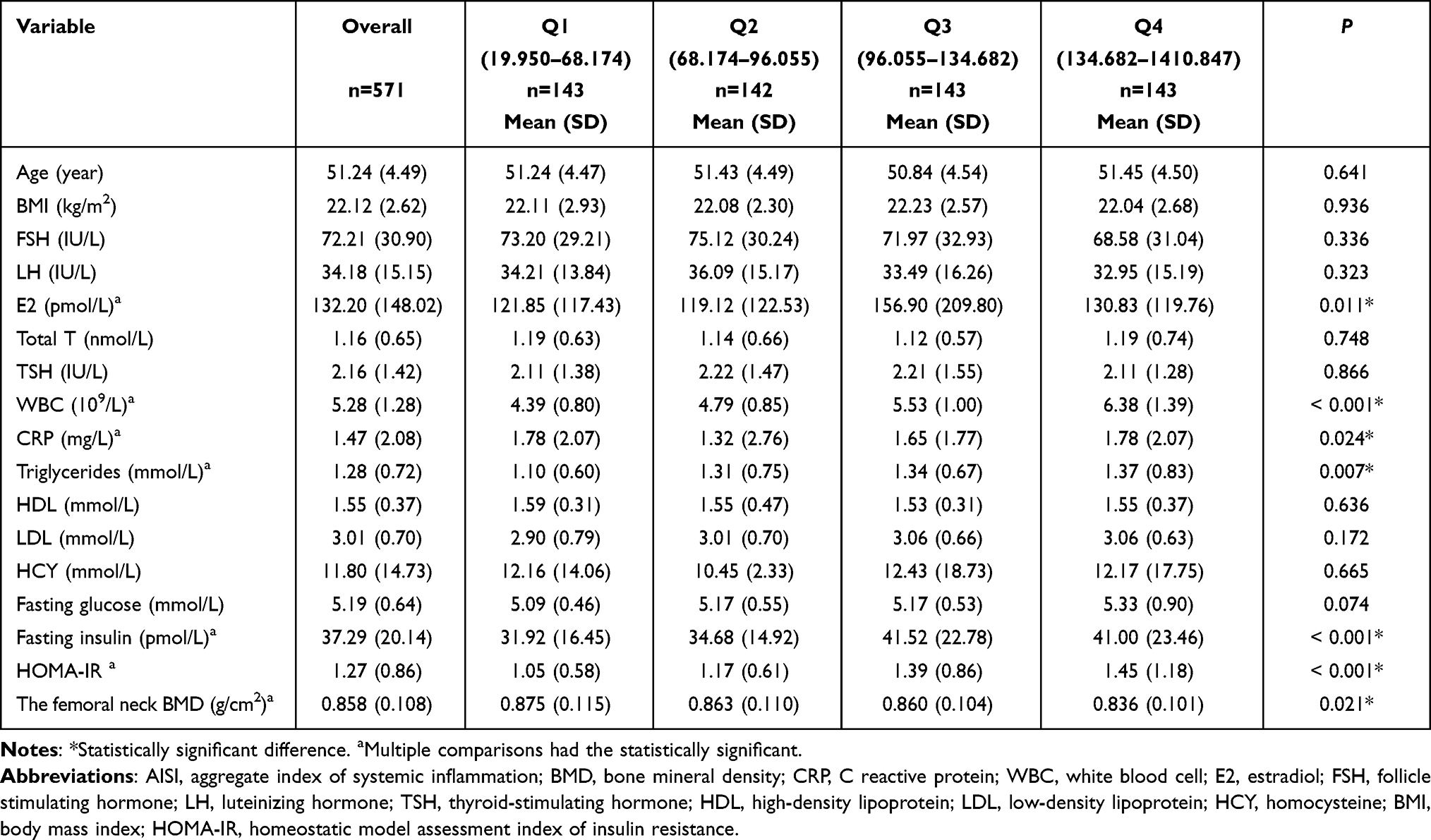 |
Table 1 Participant Characteristics Classified According to Quartile Values of AISI |
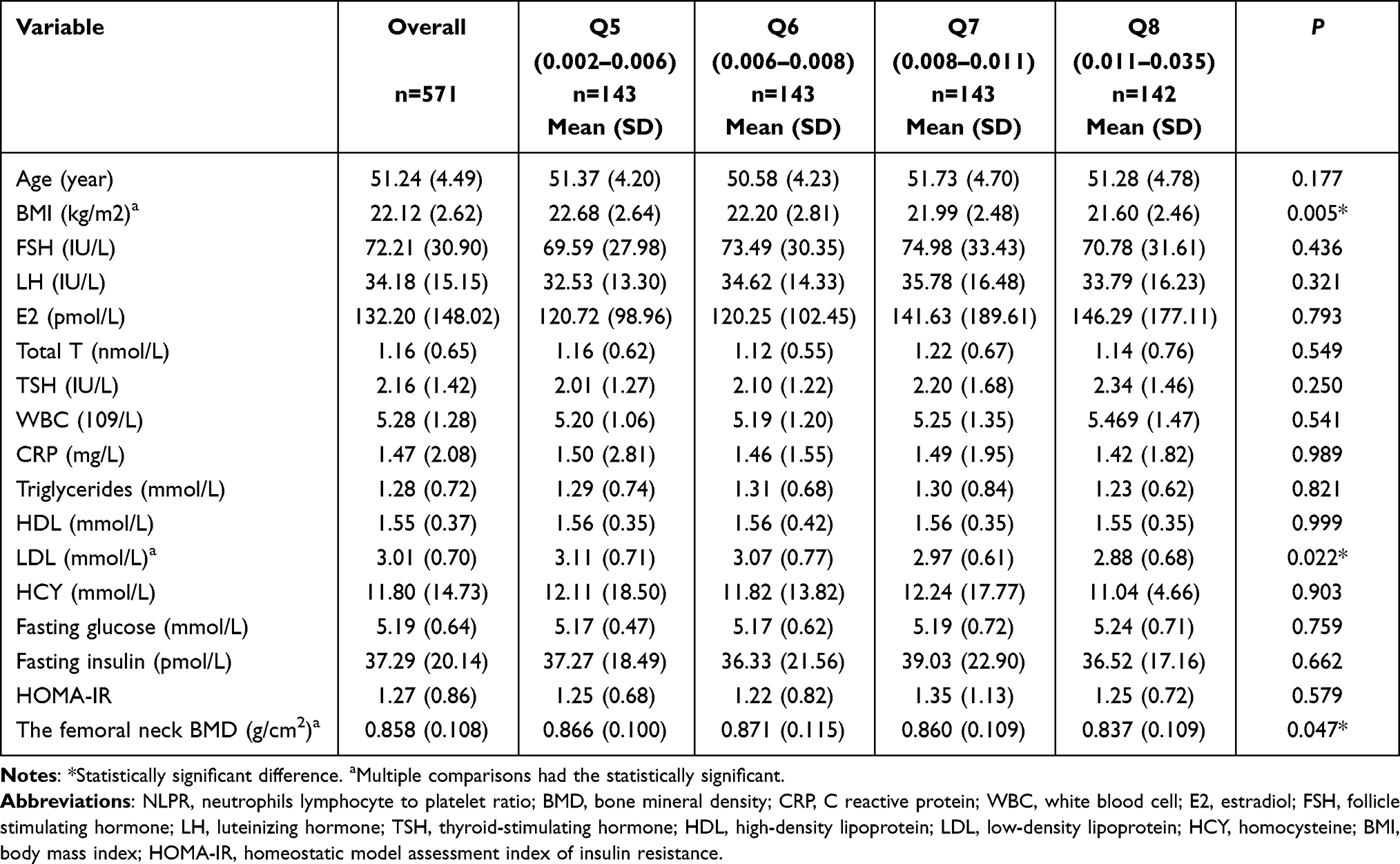 |
Table 2 Participant Characteristics Classified According to Quartile Values of NLPR |
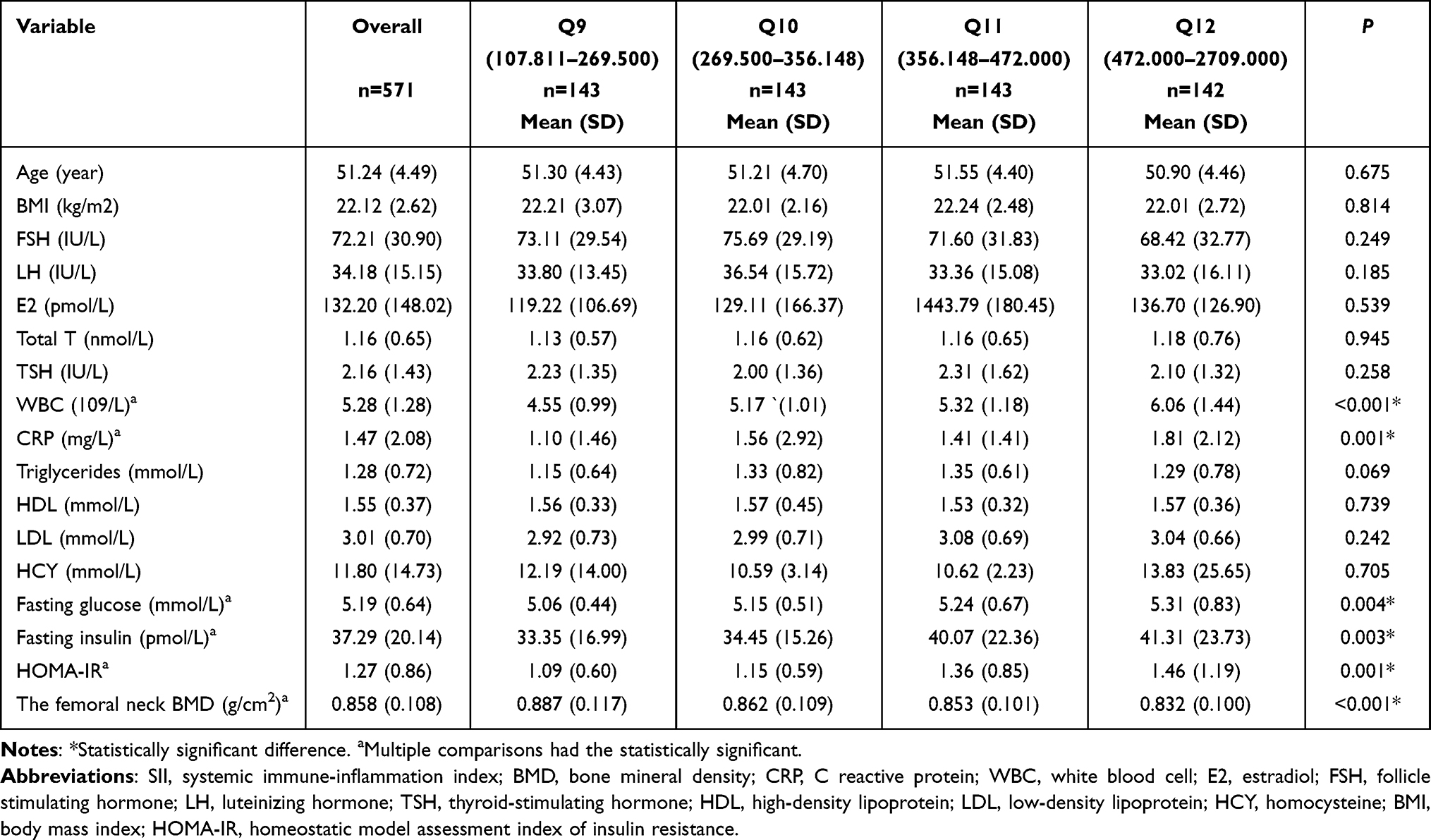 |
Table 3 Participant Characteristics Classified According to Quartile Values of SII |
There were significant differences in serum WBC, triglycerides, fasting glucose, and HOMA-IR among SIRI groups Q13–Q16. Further, higher quartile SIRI levels were significantly associated with lower BMD in groups Q13–Q16 (0.870, 0.859, 0.875, 0.827, P = 0.001, Table 4).
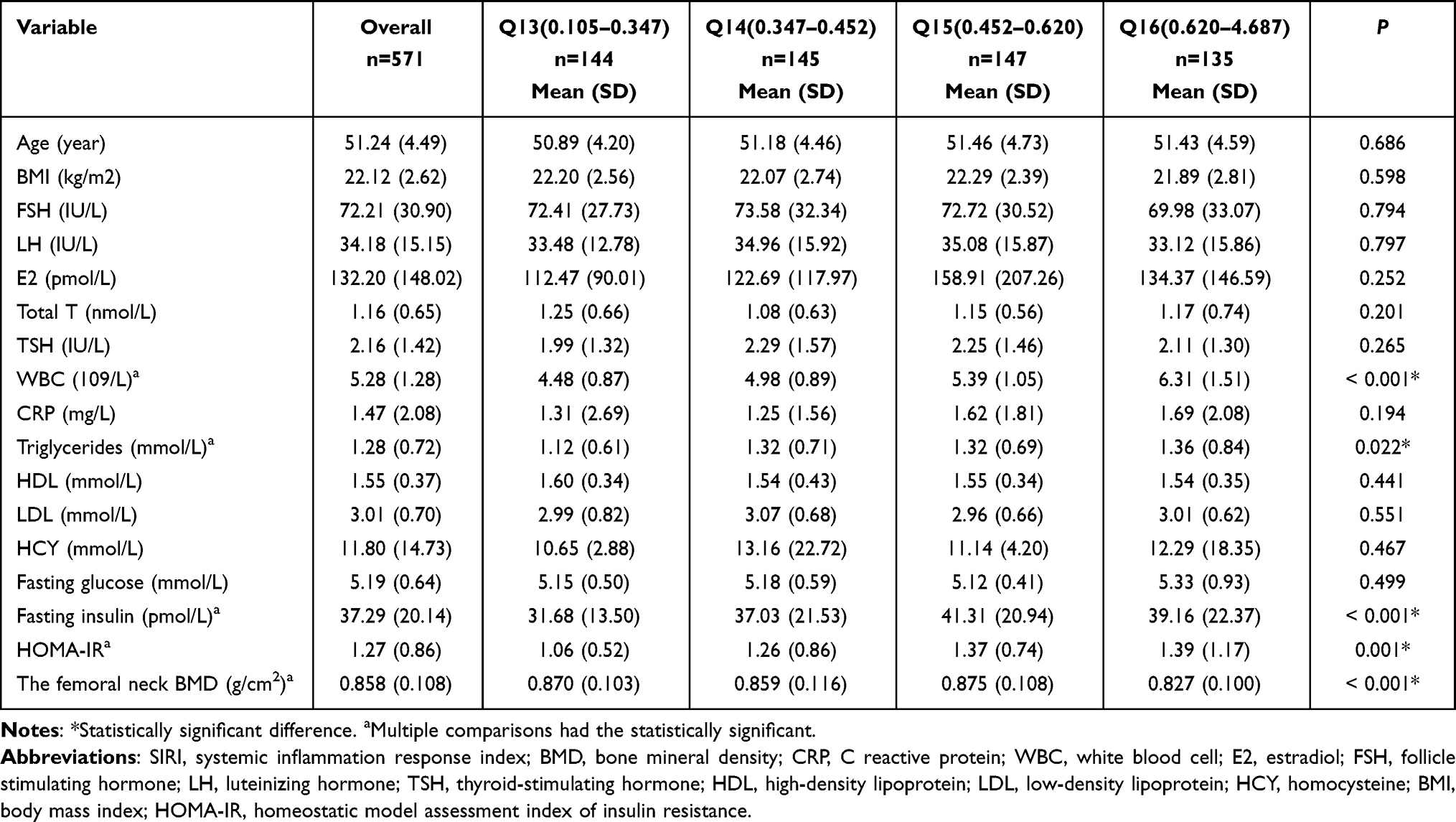 |
Table 4 Participant Characteristics Classified According to Quartile Values of SIRI |
Overall, although several other variables differed among patients with inflammatory index values across the four quartiles, associations between quartiles and femoral neck BMD were consistently significant, with a trend toward association of higher values for the four inflammatory indexes with lower BMD.
Model for Prediction of Femoral Neck BMD Based on Inflammatory Markers
To assess the potential for confounding, we established a series of models using multivariate linear regression analysis (Table 5). In the unadjusted model, mean femoral neck BMD decreased with increasing AISI levels. After adjustment for age and BMI (model 1), a significant inverse association remained between AISI levels and BMD across the quartiles (P for trend < 0.001). Additional adjustment for FSH, LH, E2, T, and TSH (model 2) only modestly attenuated the results and the association remained significant (P for trend < 0.001). Further adjustment for HCY, CRP, HDL, LDL (model 3), and fasting glucose and fasting insulin (model 4) had a minimal impact on the findings, with higher AISI level remaining significantly associated with lower BMD. In model 4, the regression coefficients for quartiles 1–3 of AISI versus quartile 4 were 0.037, 0.025, and 0.022, respectively (P for trend < 0.001).
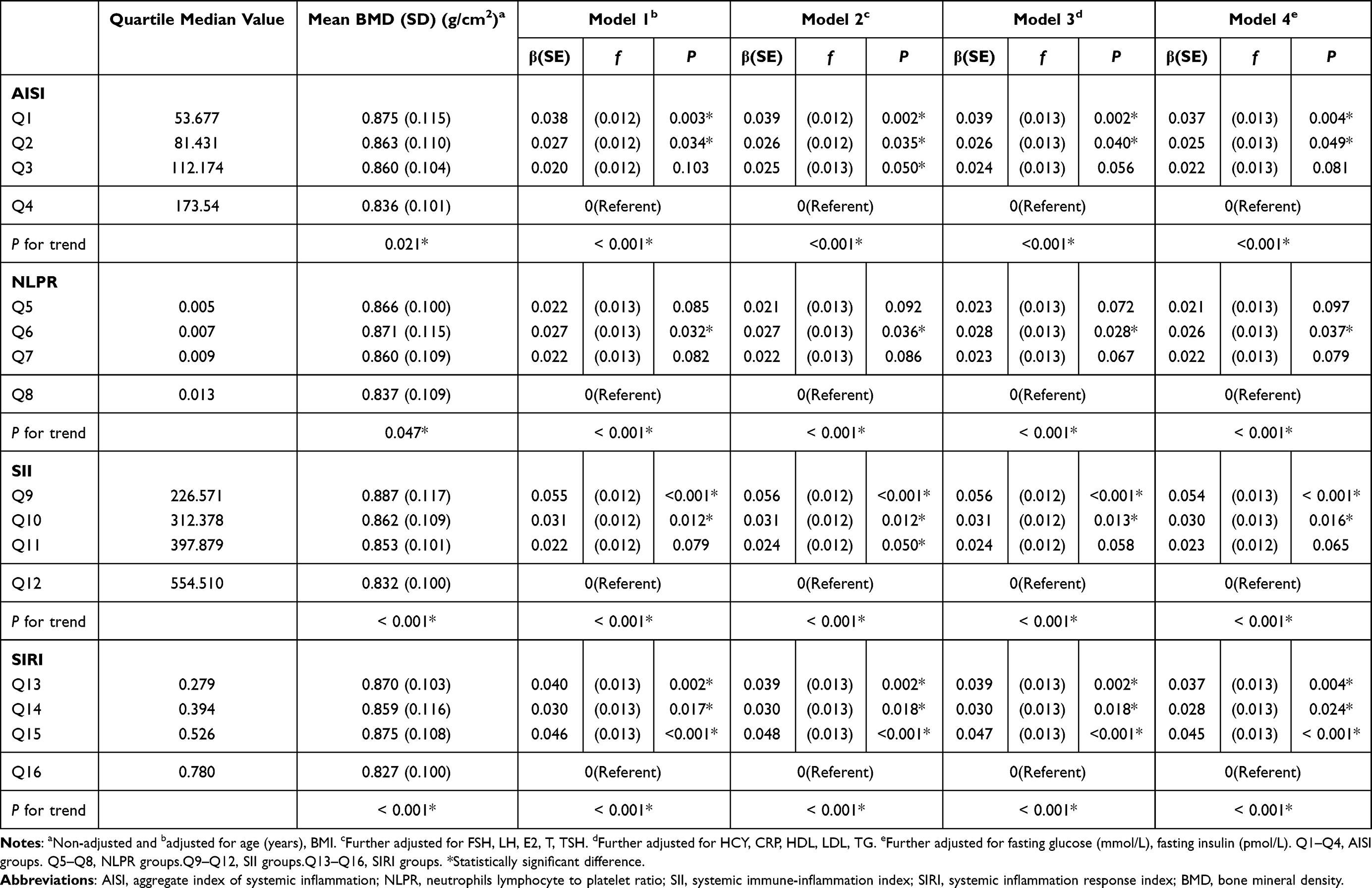 |
Table 5 Association of Systemic Inflammatory Blood Indexes and the Femoral Neck BMD Among Perimenopausal and Postmenopausal Women |
NLPR levels were linearly related to mean BMD. Unadjusted mean BMD values across groups Q5–Q8 were 0.866, 0.871, 0.860, and 0.837 g/cm2, respectively (P = 0.047). After adjustment for age and BMI (model 1) the association was significant (P for trend < 0.001). Further, following adjustment for individual variables, hormone profiles, and glucolipid metabolism profiles, higher NLPR level remained significantly associated with lower BMD (P for trend < 0.001).
Mean BMD values in SII groups Q9–Q12 were 0.887, 0.862, 0.853, and 0.832 g/cm2, respectively (P < 0.001). Application of the adjustments in models 1–4 modestly attenuated the association, but higher SII levels remained significantly associated with lower BMD (all P for trend < 0.001). The model 4 regression coefficients for Q9–Q11 versus Q12 were 0.054, 0.030, and 0.023, respectively.
We also detected a negative association between SIRI levels and BMD in perimenopausal and postmenopausal women. Model 1–4 adjustments had minimal effects on the results (P for trend = 0.001, < 0.001, < 0.001, and < 0.001, respectively). The model 4 regression coefficients for Q13–Q15 versus Q16 were 0.037, 0.028 and 0.045, respectively.
Subgroup Analysis Based on Menopausal Status
To facilitate comparisons according to menopausal status, we stratified the data into perimenopausal and postmenopausal groups (Table 6; Figures 1–4). Mean BMD levels were marginally lower in postmenopausal women than those in perimenopausal women (0.852 vs 0.871 g/cm2). Among postmenopausal women, higher AISI levels were related to lower mean BMD, with regression coefficients larger than those generated by analysis of the entire study group (P for trend = 0.015). In contrast, among perimenopausal women, AISI levels were not significantly linearly associated with BMD (P for trend = 0.248). The association between NLPR levels and mean BMD also varied according to menopausal status, with no significant association in either perimenopausal (P for trend = 0.276) or postmenopausal (P for trend = 0.190) women. Among postmenopausal women, those with the highest SII and SIRI levels had a lower mean BMD than those with the lowest levels (P for trend = 0.004 and = 0.001, respectively); however, in perimenopausal women, associations with SII and SIRI were not significant (P for trend = 0.054, P for trend = 0.352). In addition, comparisons of inflammatory indices between the premenopausal and the postmenopausal groups showed that AISI differed significantly (P = 0.021), while there were no significant differences in the other inflammatory indexes.
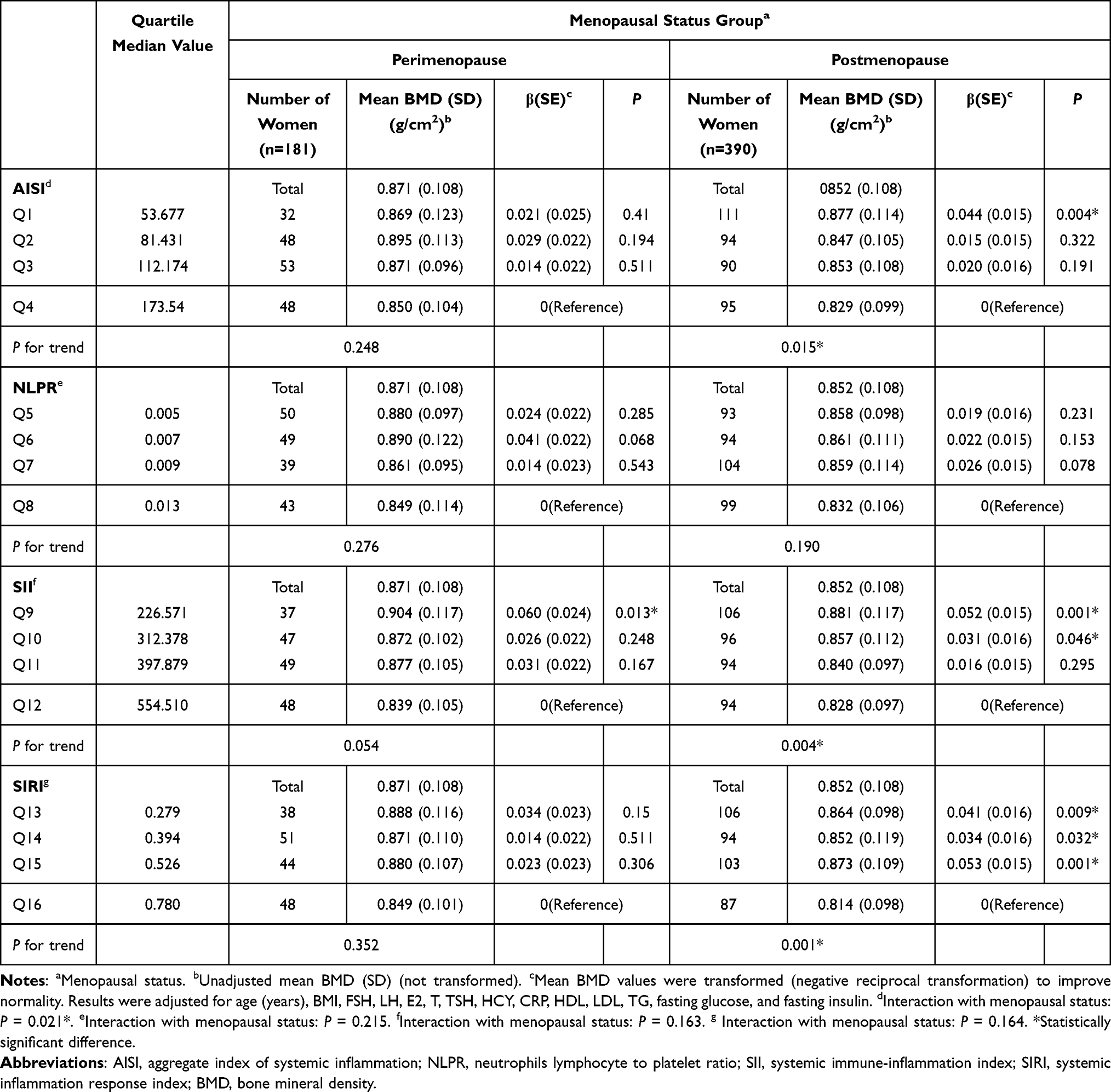 |
Table 6 Association of Systemic Inflammation Blood Indexes and the Femoral Neck BMD by Menopausal Status Group |
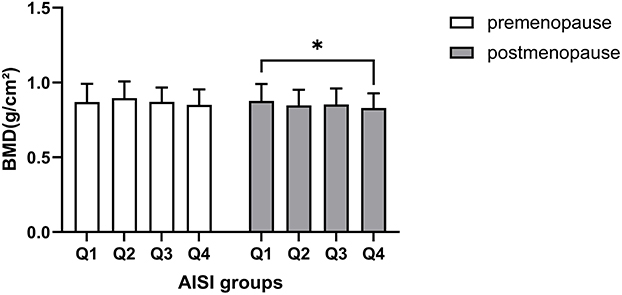 |
Figure 1 Femoral neck BMD across quartiles of AISI in perimenopausal and postmenopausal women. Abbreviations: AISI, aggregate index of systemic inflammation; BMD, bone mineral density. Note: *Statistically significant difference. |
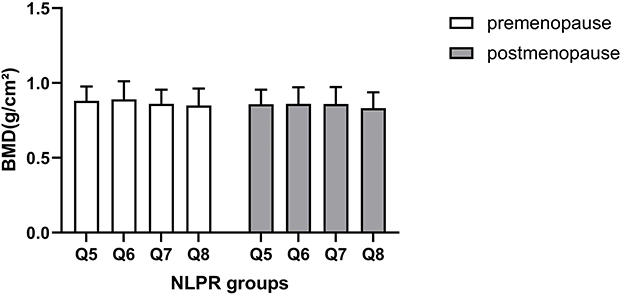 |
Figure 2 Femoral neck BMD across quartiles of NLPR in perimenopausal and postmenopausal women. Abbreviations: NLPR, neutrophils lymphocyte to platelet ratio; BMD, bone mineral density. Note: *Statistically significant difference. |
 |
Figure 3 Femoral neck BMD across quartiles of SII in perimenopausal and postmenopausal women. Abbreviations: SII, systemic immune-inflammation index; BMD, bone mineral density. Note: *Statistically significant difference. |
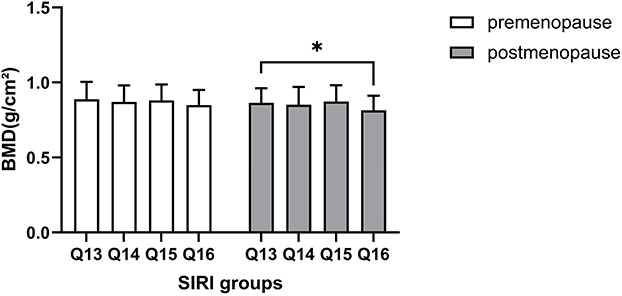 |
Figure 4 Femoral neck BMD across quartiles of SIRI in perimenopausal and postmenopausal women. Abbreviations: SIRI, systemic inflammation response index; BMD, bone mineral density. Note: *Statistically significant difference. |
Discussion
Here, we analyzed data obtained during 2016 to 2021, with the aim of assisting in the management of PMOP, to prevent fractures, depending on some easily accessible, simple inflammation indices; specifically, we investigated associations between systemic inflammatory indicators (AISI, NLPR, SII, and SIRI) and BMD in menopausal women. Associations between altered neutrophil, lymphocyte, monocyte, and bone homeostasis factors with osteoporosis have been reported previously.26,27 Therefore, we hypothesized that predictive tools, such as AISI, NLPR, SII, and SIRI, based on measurements of neutrophils, lymphocytes, monocytes, and platelets, might represent superior, easy-to-use indices, which better reflect inflammatory status in the context of specific disease states.
To our knowledge, the inverse association between AISI and BMD in menopausal women detected in this study has not been observed previously. As summarized in Tables 1 and 5, menopausal women with the highest AISI levels had higher WBC, fasting glucose, and HOMA-IR levels than those with lower AISI levels. Further, AISI was negatively correlated with BMD, even after adjustment for age, BMI, metabolic profile, individual variables, hormone profile, and glucolipid metabolic profile. AISI is reported to be valuable for predicting length of stay in patients undergoing elective open thoracic surgery, as well as prognosis of patients with COVID-19 and idiopathic pulmonary fibrosis.28–30 Few previous studies have assessed the relationship between AISI and BMD during the menopausal period, when participants are likely in a state of chronic inflammation.
Some studies have indicated that NLR, MLR, and PLR values are higher in patients with osteoporosis than in those with osteopenia or healthy controls, suggesting their potential as inflammation indicators in osteoporosis.31,32 There are few reports of analysis of NLPR, which is a relatively novel indicator with predictive value in patients with COVID-19,30 and the relationship between NLPR and osteoporosis has not previously been reported. We observed that there was significant association between femoral neck BMD and NLPR, even following comprehensive adjustment (Models 1–4). Nevertheless, analysis of data divided into perimenopausal and postmenopausal groups generated a P for trend > 0.05 for NLPR, suggesting that correlation of this index with BMD was weaker than those of the other three inflammatory indexes.
Menopausal women with the highest SII had lower femoral neck BMD. After adjustment for age, BMI, metabolic profile, individual variables, hormone profile, and glucolipid metabolic profile, P for trend remained < 0.001 in postmenopausal women. Yang et al previously proposed that higher systemic immune inflammatory index is associated with an increased risk of hemorrhagic conversion in patients with anterior circulation acute ischemic stroke due to aorta atherosclerosis.33 Further, high SII is a novel factor for predicting overall survival in patients with pancreatic ductal adenocarcinoma, superior to PLR and NLR.34 Moreover, a previous study indicated that quartile SII levels were negatively correlated with femoral neck BMD in postmenopausal women, consistent with our findings.19
T cells, B cells, and cytokines play key roles in regulating bone resorption.35,36 B cells appear be important in regulating osteoclast formation through the NF-κB ligand (RANKL)/osteoprotegerin signaling system. Activation of B cells by estrogen deficiency and pro-inflammatory conditions promotes bone resorption by secreting enhanced levels of granulocyte colony stimulating factor and RANKL during PMOP.37,38 T lymphocytes can regulate inflammatory factors, thereby influencing bone cells and immune system hematopoietic function.39,40 Neutrophils can affect bone homeostasis under estrogen deficiency, but their excessive activation increases osteoclast formation and promotes osteoblast apoptosis by releasing reactive oxygen species and stimulating RANKL signal transduction.41,42
High levels of SIRI and SII can predict adverse clinical outcomes in patients with aneurysmal subarachnoid hemorrhage.21 In addition, SIRI can be used to predict overall survival of patients with advanced soft tissue sarcoma and the efficacy of follow-up drugs.43 We found that fasting insulin and HOMA-IR are significantly related with AISI, SII and SIRI. There is few research about these systemic inflammation markers with insulin metabolism. Gasmi A et al describes the relationship between chronic low-grade inflammation and insulin.44 The relationship between SIRI and BMD in menopausal women is poorly investigated. We found that menopausal women with the highest SIRI values had higher levels of WBC, triglycerides, fasting insulin, and HOMA-IR than those with lower SIRI levels. Further, SIRI was negatively correlated with BMD (Tables 4 and 5).
The limitations of this study include its cross-sectional design, which made it impossible to evaluate causal effects. Further, the computational complexity of the related indicators mean that they may be difficult to implement in clinical practice. Further, there is no clear consensus on standard threshold values for AISI, NLPR, SII, and SIRI, unlike other biomarkers. In addition, our research did not include some factors that may influence BMD, such as markers of bone turnover, ethnicity, and smoking status, among others. Moreover, we did not stratify subjects based on bone loss or osteoporosis compared with healthy groups for further follow-up. The number of perimenopausal women in this study was also relatively small, relative to that of postmenopausal women. Further multi-center studies with larger sample numbers are warranted to validate and confirm our results.
We found that, of the four indicators tested, all except NLPR were negatively correlated with mean femoral neck BMD in postmenopausal women (Table 6). Notably, the difference between quartiles was reflected in mean femoral neck BMD value in postmenopausal women, while in premenopausal women the difference was not significant, suggesting that inflammatory markers are more likely to be useful as predictors of BMD in postmenopausal women.
Conclusion
Our results suggested that elevated levels of systemic inflammatory markers, determined using the AISI, SII, and SIRI indexes, are associated with lower femoral neck BMD in menopausal women. Further, AISI, SII, and SIRI can be used as independent predictors of BMD in postmenopausal women, and their utility is superior in postmenopausal women than in perimenopausal women. In summary, AISI, SII, and SIRI are an economical, effective and independent predictor of bone loss in the older adult women.
Abbreviations
AISI, aggregate index of systemic inflammation; ANOVA, analysis of variance; BMD, bone mineral density; BMI, body mass index; CRP, C reactive protein; E2, estradiol; FSH, follicle stimulating hormone; HCY, homocysteine; HDL, high-density lipoprotein; HOMA-IR, homeostatic model assessment index of insulin resistance; L, lymphocytes; LDL, low-density lipoprotein; LH, luteinizing hormone; M, monocytes; MLR, monocyte lymphocyte ratio; N, neutrophils; NLR, neutrophil to lymphocyte ratio; NLPR, neutrophils lymphocyte to platelet ratio; PLT, platelets; PLR, platelet to lymphocyte ratio; PMOP, postmenopausal osteoporosis; SII, systemic immune-inflammation index; SIRI, systemic inflammation response index; T, testosterone; TSH, thyroid-stimulating hormone; WBC, white blood cell.
Acknowledgments
This research was supported by the Training Program for Young and Middle-aged Doctors in Bethune Women‘s Health Research Project (X-J-2019-024); Zhejiang Province Major Science and Technology Program of Medicine and Health (WKJ-ZJ-2010); Hangzhou Agriculture and Social Development Research Project (202004A12, 202204B21); Special Project of Traditional Chinese Medicine Modernization of Zhejiang Province (2021ZX013); Medical and Health Science and Technology Project of Zhejiang Province (2022KY275). Yijie Chen and Jingjing Yu are co-first authors for this study. Zhifen Zhang and Xuejing Jin are co-correspondence authors for this study.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Arceo-Mendoza RM, Camacho PM. Postmenopausal osteoporosis: latest guidelines. Endocrinol Metab Clin North Am. 2021;50:167–178. doi:10.1016/j.ecl.2021.03.009
2. Wang L, Yu W, Yin X, et al. Prevalence of osteoporosis and fracture in China: the China Osteoporosis Prevalence Study. JAMA Netw Open. 2021;4:e2121106. doi:10.1001/jamanetworkopen.2021.21106
3. Williams SA, Daigle SG, Weiss R, Wang Y, Arora T, Curtis JR. Economic burden of osteoporosis-related fractures in the US Medicare population. Ann Pharmacother. 2021;55:821–829. doi:10.1177/1060028020970518
4. Hagino H, Osaki M, Okuda R, Enokida S, Nagashima H. Recent trends in the incidence of Hip fracture in Tottori Prefecture, Japan: changes over 32 years. Arch Osteoporos. 2020;15:152. doi:10.1007/s11657-020-00823-3
5. Wu D, Cline-Smith A, Shashkova E, Perla A, Katyal A, Aurora R. T-cell mediated inflammation in postmenopausal osteoporosis. Front Immunol. 2021;12:687551. doi:10.3389/fimmu.2021.687551
6. Clayton ES, Hochberg MC. Osteoporosis and osteoarthritis, rheumatoid arthritis and spondylarthropathies. Curr Osteoporos Rep. 2013;11:257–262. doi:10.1007/s11914-013-0172-1
7. Gulati AM, Michelsen B, Diamantopoulos A, et al. Osteoporosis in psoriatic arthritis: a cross-sectional study of an outpatient clinic population. RMD Open. 2018;4:e000631. doi:10.1136/rmdopen-2017-000631
8. Schett G, Gravallese E. Bone erosion in rheumatoid arthritis: mechanisms, diagnosis and treatment. Nat Rev Rheumatol. 2012;8:656–664. doi:10.1038/nrrheum.2012.153
9. Azizieh F, Raghupathy R, Shehab D, Al-Jarallah K, Gupta R. Cytokine profiles in osteoporosis suggest a proresorptive bias. Menopause. 2017;24:1057–1064. doi:10.1097/GME.0000000000000885
10. McClung MR, O’Donoghue ML, Papapoulos SE, et al. Odanacatib for the treatment of postmenopausal osteoporosis: results of the LOFT multicentre, randomised, double-blind, placebo-controlled trial and LOFT Extension study. Lancet Diabetes Endocrinol. 2019;7:899–911. doi:10.1016/S2213-8587(19)30346-8
11. Muñoz J, Akhavan NS, Mullins AP, Arjmandi BH. Macrophage polarization and osteoporosis: a review. Nutrients. 2020;12:2999. doi:10.3390/nu12102999
12. Börjesson AE, Lagerquist MK, Windahl SH, et al. The role of estrogen receptor α in the regulation of bone and growth plate cartilage. Cell Mol Life Sci. 2013;70(21):4023–4037. doi:10.1007/s00018-013-1317-1
13. Hirofumi B, Takeshi A, Daiki H, et al. Association of postoperative neutrophil lymphocyte ratio (NLR) and monocyte lymphocyte ratio (MLR) with the presence of osteoporosis in Japanese patients after Hip fracture surgery: a retrospective cohort study. J Osteoporos. 2021;2021:5524069. doi:10.1155/2021/5524069
14. Mehmet D, Ali K, Sedat A, et al. Evaluation of bone mineral density (BMD) and indicators of bone turnover in patients with hemophilia. Bosn J Basic Med Sci. 2018;18:206–210. doi:10.17305/bjbms.2018.2335
15. Shui Y, Li M, Su J, et al. Prognostic and clinicopathological significance of systemic immune-inflammation index in pancreatic cancer: a meta-analysis of 2365 patients. Aging. 2021;13(16):20585–20597. doi:10.18632/aging.203449
16. Ji Y, Wang H. Prognostic prediction of systemic immune-inflammation index for patients with gynecological and breast cancers: a meta-analysis. World J Surg Oncol. 2020;7(18):197. doi:10.1186/s12957-020-01974-w
17. Hamad DA, Aly MM, Abdelhameid MA, et al. Combined blood indexes of systemic inflammation as a mirror to admission to intensive care unit in COVID-19 patients: a multicentric study. J Epidemiol Glob Health. 2021;13:1–10.
18. Lei H, Xu S, Mao X, et al. Systemic immune-inflammatory index as a predictor of lymph node metastasis in endometrial cancer. J Inflamm Res. 2021;14:7131–7142. doi:10.2147/JIR.S345790
19. Du YN, Chen YJ, Zhang HY, Wang X, Zhang ZF. Inverse association between systemic immune-inflammation index and bone mineral density in postmenopausal women. Gynecol Endocrinol. 2021;37:650–654. doi:10.1080/09513590.2021.1885642
20. Chen L, Kong X, Wang Z, Wang X, Fang Y, Wang J. Pretreatment systemic inflammation response index in patients with breast cancer treated with neoadjuvant chemotherapy as a useful prognostic indicator. Cancer Manag Res. 2020;3:1543–1567. doi:10.2147/CMAR.S235519
21. Yun S, Yi HJ, Lee DH, et al. Systemic inflammation response index and systemic immune-inflammation index for predicting the prognosis of patients with aneurysmal subarachnoid hemorrhage. J Stroke Cerebrovasc Dis. 2021;30:105861. doi:10.1016/j.jstrokecerebrovasdis.2021.105861
22. Li Y, Zou Z, Zhang Y, et al. Dynamics in perioperative neutrophil-to-lymphocyte*platelet ratio as a predictor of early acute kidney injury following cardiovascular surgery. Ren Fail. 2021;43:1012–1019. doi:10.1080/0886022X.2021.1937220
23. de Hond TAP, Ocak G, Groeneweg L, et al. Hematological ratios are associated with acute kidney injury and mortality in patients that present with suspected infection at the emergency department. J Clin Med. 2022;11(22):1–7. doi:10.3390/jcm11041017
24. Zinellu A, Collu C, Nasser M, et al. The aggregate index of systemic inflammation (AISI): a novel prognostic biomarker in idiopathic pulmonary fibrosis. J Clin Med. 2021;10:4134. doi:10.3390/jcm10184134
25. Harlow SD, Gass M, Hall JE, et al. Executive summary of the Stages of Reproductive Aging Workshop + 10: addressing the unfinished agenda of staging reproductive aging. J Clin Endocrinol Metab. 2012;97:1159–1168. doi:10.1210/jc.2011-3362
26. Zhang W, Dang K, Huai Y, Qian A. Osteoimmunology: the regulatory roles of T lymphocytes in osteoporosis. Front Endocrinol. 2020;11:465. doi:10.3389/fendo.2020.00465
27. Fischer V, Haffner-Luntzer M. Interaction between bone and immune cells: implications for postmenopausal osteoporosis. Semin Cell Dev Biol. 2022;123:14–21. doi:10.1016/j.semcdb.2021.05.014
28. Paliogiannis P, Ginesu GC, Tanda C, et al. Inflammatory cell indexes as preoperative predictors of hospital stay in open elective thoracic surgery. ANZ J Surg. 2018;88:616–620. doi:10.1111/ans.14557
29. Zinellu A, Paliogiannis P, Sotgiu E, et al. Blood cell count derived inflammation indexes in patients with idiopathic pulmonary fibrosis. Lung. 2020;198:821–827. doi:10.1007/s00408-020-00386-7
30. Fois AG, Paliogiannis P, Scano V, et al. The systemic inflammation index on admission predicts in-hospital mortality in COVID-19 patients. Molecules. 2020;25:5725. doi:10.3390/molecules25235725
31. Gao K, Zhu W, Liu W, et al. The predictive role of monocyte-to-lymphocyte ratio in osteoporosis patient. Medicine. 2019;98:e16793. doi:10.1097/MD.0000000000016793
32. Yilmaz H, Uyfun M, Yilmaz TS, et al. Neutrophil-lymphocyte ratio may be superior to C-reactive protein for predicting the occurrence of postmenopausal osteoporosis. Endocr Regul. 2014;48:25–33. doi:10.4149/endo_2014_01_25
33. Yang Y, Han Y, Sun W, et al. Increased systemic immune-inflammation index predicts hemorrhagic transformation in anterior circulation acute ischemic stroke due to large-artery atherosclerotic. Int J Neurosci;2021. 1–7. doi:10.1080/00207454.2021.1953021
34. Jomrich G, Gruber ES, Winkler D, et al. Systemic immune-inflammation index (SII) predicts poor survival in pancreatic cancer patients undergoing resection. J Gastrointest Surg. 2020;24:610–618. doi:10.1007/s11605-019-04187-z
35. Srivastava RK, Dar HY, Mishra PK. Immunoporosis: immunology of osteoporosis-role of T cells. Front Immunol. 2018;9:657. doi:10.3389/fimmu.2018.00657
36. Kalyan S. It may seem inflammatory, but some T cells are innately healing to the bone. J Bone Miner Res. 2016;31:1997–2000. doi:10.1002/jbmr.2875
37. Nordqvist J, Bernardi A, Islander U, Carlsten H. Effects of a tissue-selective estrogen complex on B lymphopoiesis and B cell function. Immunobiology. 2017;222:918–923. doi:10.1016/j.imbio.2017.05.013
38. Ponte F, Kim HN, Iyer S, Han L, Almeida M, Manolagas SC. Cxcl12 deletion in mesenchymal cells increases bone turnover and attenuates the loss of cortical bone caused by estrogen deficiency in mice. J Bone Miner Res. 2020;35:1441–1451. doi:10.1002/jbmr.4002
39. Ginaldi L, De Martinis M. Osteoimmunology and beyond. Curr Med Chem. 2016;23:3754–3774. doi:10.2174/0929867323666160907162546
40. Li JY, Tawfeek H, Bedi B, et al. Ovariectomy disregulates osteoblast and osteoclast formation through the T-cell receptor CD40 ligand. Proc Natl Acad Sci USA. 2011;108:768–773. doi:10.1073/pnas.1013492108
41. Hu X, Sun Y, Xu W, Lin T, Zeng H. Expression of RANKL by peripheral neutrophils and its association with bone mineral density in COPD. Respirology. 2017;22:126–132. doi:10.1111/resp.12878
42. Gaida MM, Mayer B, Stegmaier S, Schirmacher P, Wagner C, Hansch GM. Polymorphonuclear neutrophils in osteomyelitis: link to osteoclast generation and bone resorption. Eur J Inflamm. 2012;10:413–426. doi:10.1177/1721727X1201000317
43. Kobayashi H, Okuma T, Okajima K, et al. Systemic inflammation response index (SIRI) as a predictive factor for overall survival in advanced soft tissue sarcoma treated with eribulin. J Orthop Sci. 2022;27:222–228. doi:10.1016/j.jos.2020.11.006
44. Amin G, Sadaf N, Alain M, et al. Obesity and Insulin Resistance: associations with Chronic Inflammation, Genetic and Epigenetic Factors. Curr Med Chem. 2021;28:800–826. doi:10.2174/0929867327666200824112056
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Associations Between Inflammatory Mediators and Bone Outcomes in Postmenopausal Women: A Cross-Sectional Analysis of Baseline Data from the Prune Study
Damani JJ, De Souza MJ, Strock NCA, Koltun KJ, Williams NI, Weaver C, Rogers CJ
Journal of Inflammation Research 2023, 16:639-663
Published Date: 15 February 2023
The Monocyte-to-High-Density Lipoprotein Cholesterol Ratio as a Novel Predictor of the Prevalence of Senile Osteoporosis
Lin N, Li D, Lin S, Ke Y, Lu J, Wu Y, Huang T, Hong H
Clinical Interventions in Aging 2024, 19:1773-1788
Published Date: 1 November 2024