Back to Journals » Drug Design, Development and Therapy » Volume 16
Switching from a Non-Protease inhibitor-Based Regimen To the Fixed Dose Combination of Darunavir/Cobicistat/Emtricitabine/Tenofovir Alafenamide in Clinical Practice
Authors Ranzenigo M, Gianotti N ![]() , Galli L
, Galli L ![]() , Poli A, Mastrangelo A, Bruzzesi E, Chiurlo M
, Poli A, Mastrangelo A, Bruzzesi E, Chiurlo M ![]() , Nozza S, Bossolasco S, Spagnuolo V
, Nozza S, Bossolasco S, Spagnuolo V ![]() , Mancusi D
, Mancusi D ![]() , Termini R
, Termini R ![]() , Carini E, Lazzarin A, Castagna A
, Carini E, Lazzarin A, Castagna A
Received 18 January 2022
Accepted for publication 14 June 2022
Published 27 June 2022 Volume 2022:16 Pages 1975—1982
DOI https://doi.org/10.2147/DDDT.S358976
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Manfred Ogris
Martina Ranzenigo,1,2 Nicola Gianotti,2 Laura Galli,2 Andrea Poli,2 Andrea Mastrangelo,1,2 Elena Bruzzesi,1,2 Matteo Chiurlo,1,2 Silvia Nozza,2 Simona Bossolasco,2 Vincenzo Spagnuolo,2 Daniela Mancusi,3 Roberta Termini,3 Elisabetta Carini,2 Adriano Lazzarin,2 Antonella Castagna1,2
1Vita-Salute San Raffaele University, Milan, Italy; 2Infectious Diseases, IRCCS San Raffaele Scientific Institute, Milan, Italy; 3Medical Affairs Department, Infectious Disease and Vaccines & PAH, Janssen-Cilag SpA, Cologno Monzese, Italy
Correspondence: Daniela Mancusi, Medical Affairs Department, Infectious Disease and Vaccines & PAH, Janssen-Cilag SpA, Via Buonarroti 23, Cologno Monzese (MI), 20093, Italy, Tel +0039-345 9581944, Email [email protected]
Background: The primary objective of this study was to estimate the proportion of people living with HIV (PLWH) who switched from a non-protease inhibitor (PI)-based regimen [integrase strand transfer inhibitor (InSTI)-based or non-nucleoside reverse transcriptase inhibitor (NNRTI)-based regimen] to darunavir, cobicistat, emtricitabine, tenofovir alafenamide (D/C/F/TAF).
Methods: This was a retrospective study on PLWH treated with a non-PI regimen in January 2017, who switched to D/C/F/TAF or to another antiretroviral therapy (ART) within November 2019. Follow-up was from the start date of D/C/F/TAF until the last available visit or discontinuation for any reason of this regimen. Virological failure (VF) was defined as 2 consecutive HIV-RNA values > 50 copies/mL. Characteristics were reported as median (interquartile range) or frequency (%). A univariate Poisson regression model was used to measure the incidence rate of switch to D/C/F/TAF. Changes in laboratory parameters during D/C/F/TAF were assessed by univariate mixed linear models.
Results: Overall, 3076 PLWH were included; 83% were male, median age at ART switch was 50 (42– 56) years and median time on ART was 5.2 (0.3– 13.0) years. PLWH had a median follow-up of 4.76 (3.70– 6.38) years; during 17,099 person-years of follow-up (PYFU), 423/3076 (14%) participants discontinued the non-PI-based regimen and 106/423 (25%) switched to D/C/F/TAF, with an overall incidence rate of switch to D/C/F/TAF of 6.2 per 1000-PYFU (95% CI: 5.0– 7.4). Among PLWH who switched to D/C/F/TAF, the ongoing regimen was based on NNRTIs in 37 (35%) and on InSTIs in 69 (65%). Main reasons leading to switch to D/C/F/TAF included neuropsychiatric adverse events (37%), VF (26%) and Kaposi sarcoma progression (5%).
Conclusion: In the last years, a non-negligible proportion of patients on an NNRTI- or an InSTI-based regimen switched to D/C/F/TAF.
Keywords: treatment switching, anti-retroviral agents, HIV protease inhibitors, adverse drug events, sustained virologic response
Corrigendum for this paper has been published.
Introduction
In the mid-1990s, the introduction of protease inhibitors (PIs) revolutionized HIV treatment, leading to greater virological suppression rates, better immune reconstitution, and a significant decline in AIDS-related deaths.1 Moreover, second-generation PIs, such as darunavir, are well tolerated, although gastrointestinal side effects and metabolic complications are not infrequent.2
Currently, a larger number of therapeutic options are available; in particular, integrase strand transfer inhibitors (InSTI) are one of the latest antiretroviral drug classes approved and now widely recommended in international guidelines for ART-naïve and -experienced people living with HIV (PLWH) due to their high efficacy and safety.3,4
However, discontinuations of non-nucleoside reverse transcriptase inhibitors (NNRTI) and InSTI-based regimens have been observed in clinical practice, mainly secondary to drug-related adverse events and virological failure.5,6 Switching to a single tablet regimen (STR) once per day containing darunavir combined with cobicistat as booster, which is generally not associated with gastrointestinal symptoms and has a better drug-drug interaction profile, emtricitabine and tenofovir alafenamide may enhance patient adherence, ensure virological outcomes, and also prevent the emergence of drug-resistant mutations because of its high genetic barrier.
It has already been demonstrated that switching from boosted protease inhibitors plus emtricitabine and tenofovir disoproxil fumarate regimens to a STR including darunavir/cobicistat/emtricitabine/tenofovir alafenamide (D/C/F/TAF) is safe and effective;7 nonetheless, no data are reported in literature on PLWH switching from non PI-based regimens to D/C/F/TAF.
The primary objective of the study was to estimate the proportion of patients who switched from a non PI-based regimen (InSTI- or NNRTI-based regimen) to D/C/F/TAF.
Methods
Study Population
This was a retrospective study conducted on adult PLWH who were receiving a non PI-based regimen (InSTI- or NNRTI-based regimen) in January 2017 and switched to D/C/F/TAF or another ART regimen within November 2019. Patients with decompensated cirrhosis, cancers requiring chemotherapy and/or radiotherapy or known for using concomitant medications not allowed with D/C/F/TAF according to the summary of product characteristics were excluded from the analysis. Drug changes within the NNRTI or InSTI class were ignored.
Follow-up accrued from the starting date of D/C/F/TAF until the last available visit or discontinuation of this regimen. Virological failure was defined as two consecutive HIV RNA values >50 copies/mL.
Anonymized data from the Infectious Diseases Department database (CSLHIV Cohort) of IRCCS San Raffaele Scientific Institute (Milan, Italy) were analyzed.
The study was approved by the ethics committee of the IRCCS San Raffaele Scientific Institute; all participants provided written informed consent.
Statistical Analysis
Results were reported as median (IQR, interquartile range) or frequency (%).
At baseline, defined as the starting date of the non PI-based regimen (InSTI- or NNRTI-based regimen), demographic, clinical and immune-virological factors were compared between people who switched to D/C/F/TAF and who did not, using Chi-square for categorical variables and Kruskal–Wallis or Mann–Whitney test for continuous variables.
Secondary objectives were to evaluate factors associated with switching to D/C/F/TAF, to assess the proportion of PLWH with virological failure with the corresponding 95% confidence interval (95% CI, Wald method), to describe mean changes of laboratory parameters during D/C/F/TAF, and to investigate reasons for switching to D/C/F/TAF.
A univariate Poisson regression model was used to measure the incidence rate of switch to D/C/F/TAF; the rate was reported as the number of switches per 1000 person-years of follow-up (PYFU) with the corresponding 95% CI.
Univariate and multivariate Cox proportional hazard regression models were performed to identify factors associated with switching from a non-PI regimen to D/C/F/TAF. The multivariate model was performed in a stepwise manner with entry and removal criteria at 0.05 alpha level and included statistically significant variables (p<0.05) in univariate analysis or other potential predictors of switch. Potential predictor variables were assessed for multicollinearity before being included in the multivariate model.
For the calculation of: i) incidence rate of switch and the ii) Cox proportional hazard models, baseline was defined as the date of start of the non-PI regimen (InSTI-based or NNRTI-based regimen) and follow-up was censored at the date of the switch to D/C/F/TAF or to another antiretroviral class or last available visit.
Mean changes in laboratory parameters during D/C/F/TAF were assessed by univariate mixed linear models; models were calculated on raw data with random intercept and random slope (uniform variance-covariance matrix). For these analyses, baseline was defined as the date of start of D/C/F/TAF and follow-up was censored at the last available visit or discontinuation of this regimen.
The analyses were conducted using two-sided test at 0.05 alpha level of significance and SAS 9.4 (Cary, NC).
Results
Overall, 3076 people with HIV infection were included: 2555 were male (83.1%) and median age at baseline was 50.1 (41.9–56.3) years. Median time from HIV diagnosis was 9.0 (2.9–17.0) years, while median exposure to ART was 5.2 (0.3–13.0) years. Other patients’ characteristics are reported in Table 1.
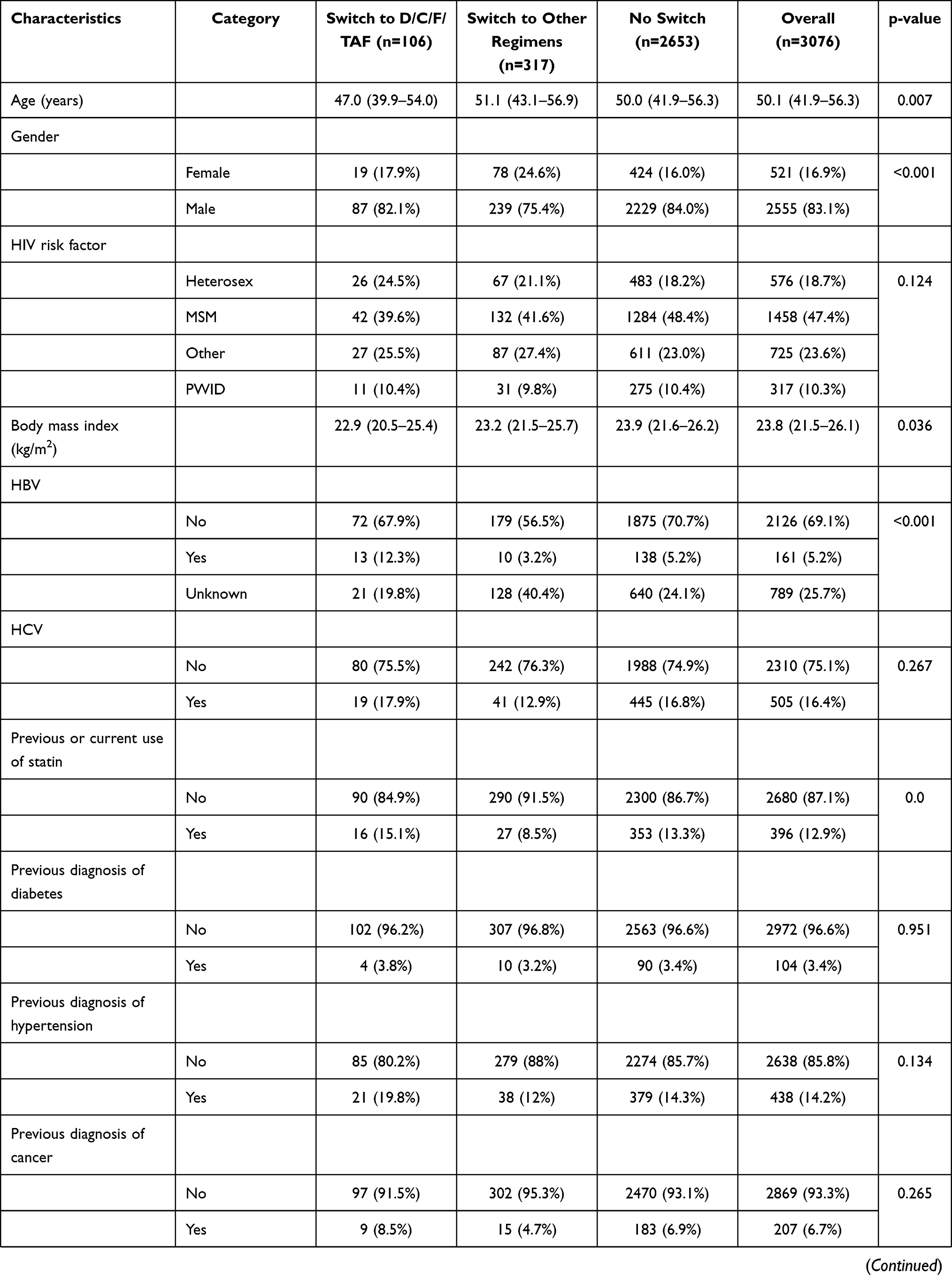 |  | 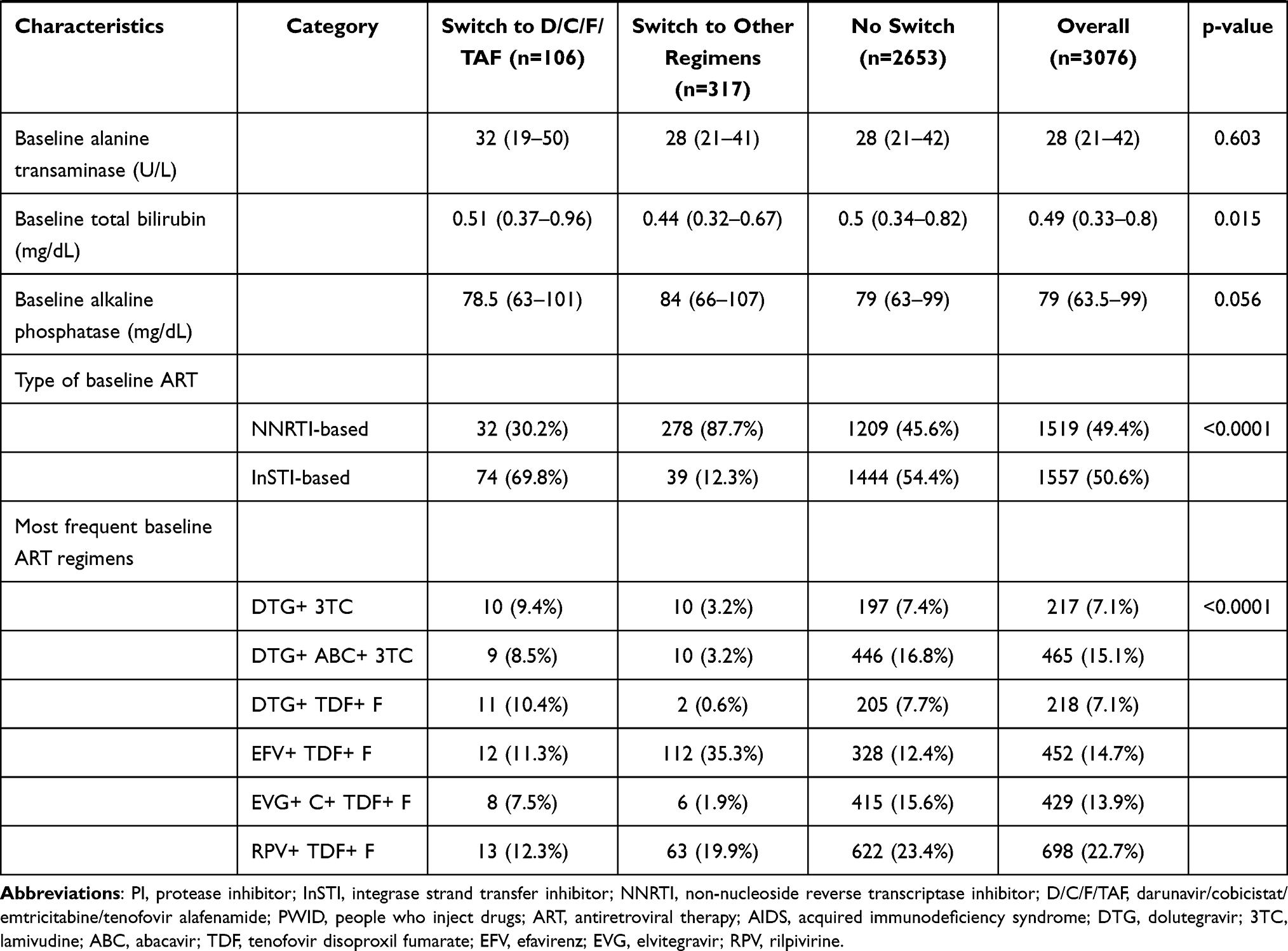 |
Table 1 Patients’ Characteristics at the Start of the Non-PI Regimen (InSTI-Based or NNRTI-Based Regimen) |
During 17,099 PYFU, median follow-up was 4.8 (3.7–6.4) years; 423/3076 (14.0%) PLWH discontinued the non PI-based regimen: 106/423 (25.1%) switched to D/C/F/TAF for an overall incidence rate of switch to D/C/F/TAF of 6.2 per 1000-PYFU (95% CI: 5.02–7.38), while 317/423 (74.9%) switched to other classes.
Median time to switch was 4.1 (2.0–7.7) years: 1.1 (0.4–2.8) year for people who switched to D/C/F/TAF and 5.3 (3.2–8.4) years for people who switched to other antiretroviral classes (p<0.001). The ongoing regimen used by individuals who switched to D/C/F/TAF was based on NNRTIs in 32/106 (30.2%) and on InSTIs in 74/106 (69.8%).
Overall, 423 PLWH discontinued their current regimen and toxicity was the main reason leading to switch for 122 (28.8%) patients: 43/106 (40.6%) among people who switched to D/C/F/TAF and 79/317 (24.9%) among people who switched to other antiretroviral classes; the following causes were simplification in 114 (27.0%) [1/106 (0.9%) vs 113/317 (35.6%)], immune virological failure in 61 (14.4%) [34/106 (32.1%) vs 27/317 (8.5%)] drug interaction in 18 (4.3%) [1/106 (0.9%) vs 17/317 (5.4%)], and other reasons in 108 [(25.5%) 27/106 (25.5%) vs 81/317 (25.6%)] (p<0.001).
Among toxicities responsible for switching to D/C/F/TAF, neuropsychiatric adverse events were reported in 39/106 patients (36.8%), mainly related to depressed mood (16/39, 41.0%) and sleep disorders (11/39, 28.2%), virological failure in 32/106 (30.2%) and Kaposi sarcoma progression in 5/106 (4.7%).
During treatment with D/C/F/TAF, median follow-up was 10.6 (3.8–26.8) months; virological failure occurred in 11 (10%; 95% CI: 5.7–17.8%) patients, of whom 8 switched to another antiretroviral class regimen, 2 continued their current ART and achieved HIV RNA <50 copies/mL, while 1 potentiated D/C/F/TAF adding dolutegravir.
Significant mean changes per year (95% CI) in safety parameters after switch to D/C/F/TAF are illustrated in Supplementary Table.
Factors associated with switching from a non-PI based regimen to D/C/F/TAF were a longer exposure to infection from HIV diagnosis, a previous diagnosis of AIDS, a more recent calendar year of baseline ART, the use of an InSTI-based regimen at baseline, higher values of triglycerides and alanine aminotransferase (ALT), as shown in Table 2.
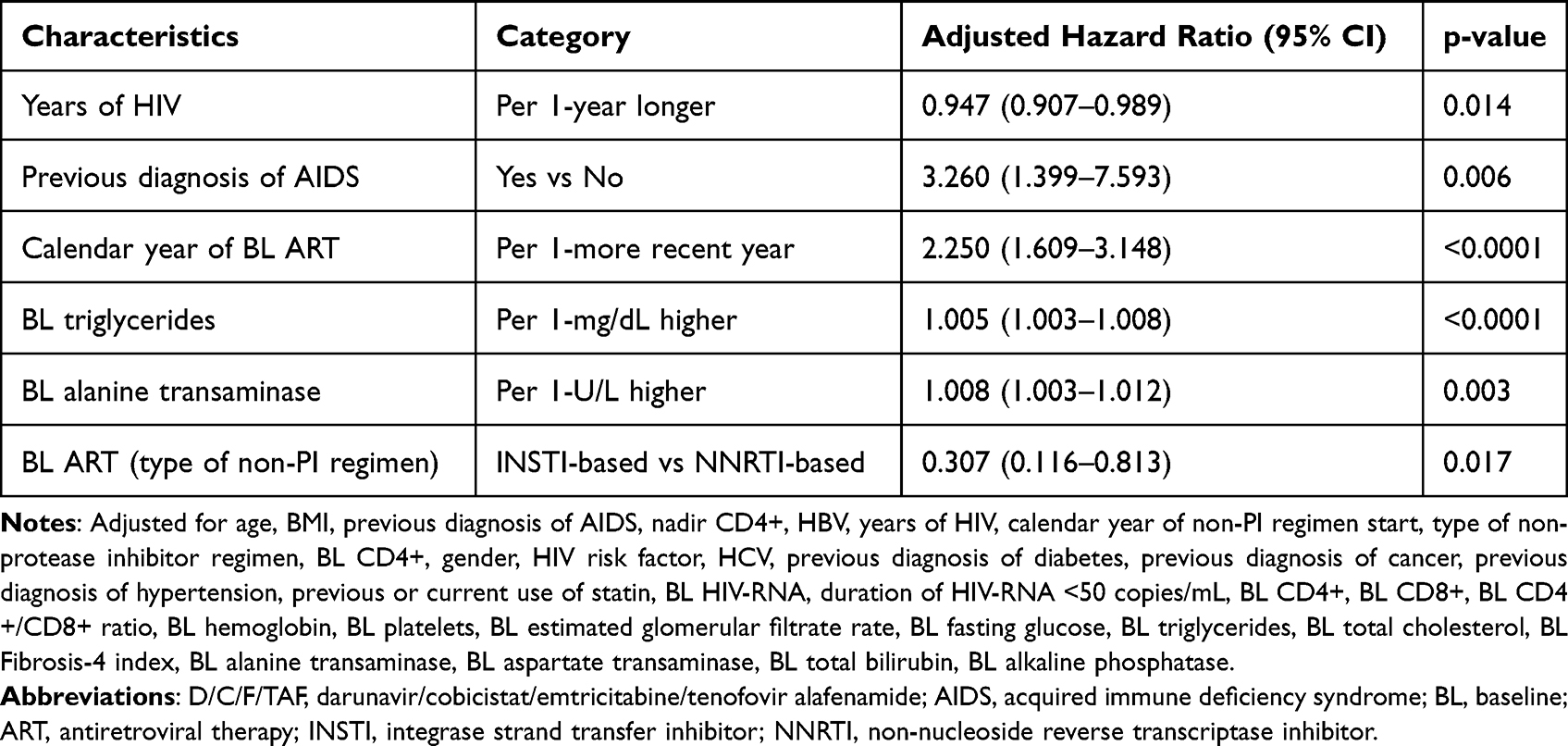 |
Table 2 Factors Associated with the Switch to D/C/F/TAF |
Discussion
Our study has shown that switching from a non PI-based regimen to D/C/F/TAF may be a valid therapeutic strategy in PLWH. ART containing darunavir has been proven to maintain virological suppression and be well tolerated when switching from treatment with NNRTIs or other PIs;7–9 unfortunately, there are not sufficient data available in case of InSTIs’ discontinuation.
Among patients considered in the analysis, neuropsychiatric symptoms represented the main reason to interrupt a non PI-based regimen and switch to D/C/F/TAF. As already described in a large number of studies, some NNRTIs can cause dizziness, hallucinations, sleep or mood disorders and even suicide ideation, with a prevalence of complications up to 70% in PLWH receiving efavirenz;10 however, the overall impact of neurotoxicity related to InSTIs is still debated.
Evidence from clinical practice has reported a higher incidence of central nervous system adverse events in people treated with dolutegravir than in registered trials.11 Focusing attention on long-term tolerability of second-generation InSTIs might help clinicians to better manage future antiretroviral switches.
Although about 40% of PLWH who switched to D/C/F/TAF had no virological suppression under the previous ART regimen, only 10% of participants treated with D/C/F/TAF reported two consecutive HIV RNA values ≥50 copies/mL after the switch. Moreover, starting D/C/F/TAF induced a significant weight loss; since TAF was seen to be involved in weight gain,12 effects of TAF combined with PIs need further investigation.
Switching to D/C/F/TAF was associated with more challenging HIV management (a longer history of infection and a previous diagnosis of AIDS), a recent use of integrase inhibitors and both metabolic and hepatic impairment; these results have shown that D/C/F/TAF was selected by clinicians as a therapeutic strategy for people facing complex situations.
One of the limitations of the study is the retrospective study design; in fact, it does not allow to infer causality and exclude all the residual confounders. Furthermore, patients evaluated in our study were predominantly male and middle-aged; so, these findings may not be generalizable to other populations, such as older people and women.
Major strengths rely on the opportunity to investigate the switch from a non-PI based regimen to D/C/F/TAF in a real-word data setting.
Conclusion
In conclusion, we observed a non-negligible proportion of PLWH on an NNRTI- or an InSTI-based regimen who switched to D/C/F/TAF.
Acknowledgments
The authors thank Camilla Muccini for medical writing on behalf of IRCCS San Raffaele Scientific Institute and Janssen-Cilag SpA.
Funding
This analysis has been funded by Janssen-Cilag SpA.
Disclosure
Dr Nicola Gianotti reports grants from Janssen-Cilag, during the conduct of the study. Dr Vincenzo Spagnuolo reports grants and/or personal fees from Gilead Sciences, ViiV Healthcare, outside the submitted work. Dr Daniela Mancusi is an employee of Janssen-Cilag SpA. Dr Roberta Termini was an employee of Janssen Cilag SpA during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Schwarcz SK, Hsu LC, Vittinghoff E, Katz MH. Impact of protease inhibitors and other antiretroviral treatments on acquired immunodeficiency syndrome survival in San Francisco, California, 1987–1996. Am J Epidemiol. 2000;152(2):178–185. doi:10.1093/aje/152.2.178
2. Tian X, Yao Y, He G, Jia Y, Wang K, Chen L. Systematic analysis of safety profile for darunavir and its boosted agents using data mining in the FDA Adverse Event Reporting System database. Sci Rep. 2021;11(1):12438. doi:10.1038/s41598-021-91549-w
3. Smith SJ, Zhao XZ, Passos DO, Lyumkis D, Burke TR Jr, Hughes SH. Integrase strand transfer inhibitors are effective anti-HIV drugs. Viruses. 2021;13(2):205. doi:10.3390/v13020205
4. Kelly SG, Masters MC, Taiwo BO. Initial antiretroviral therapy in an integrase inhibitor era: can we do better? Infect Dis Clin North Am. 2019;33(3):681–692. doi:10.1016/j.idc.2019.05.003
5. Prosperi MC, Fabbiani M, Fanti I, et al. Predictors of first-line antiretroviral therapy discontinuation due to drug-related adverse events in HIV-infected patients: a retrospective cohort study. BMC Infect Dis. 2012;12(1):296. doi:10.1186/1471-2334-12-296
6. Peñafiel J, de Lazzari E, Padilla M, et al. Tolerability of integrase inhibitors in a real-life setting. J Antimicrob Chemother. 2017;72(6):1752–1759. doi:10.1093/jac/dkx053
7. Orkin C, Molina JM, Negredo E, et al. Efficacy and safety of switching from boosted protease inhibitors plus emtricitabine and tenofovir disoproxil fumarate regimens to single-tablet darunavir, cobicistat, emtricitabine, and tenofovir alafenamide at 48 weeks in adults with virologically suppressed HIV-1 (EMERALD): a Phase 3, randomised, non-inferiority trial. Lancet HIV. 2018;5:e23–e34. doi:10.1016/S2352-3018(17)30179-0
8. Jao J, Yu W, Patel K, et al. Improvement in lipids after switch to boosted atazanavir or darunavir in children/adolescents with perinatally acquired HIV on older protease inhibitors: results from the Pediatric HIV/AIDS Cohort Study. HIV Med. 2018;19(3):175–183. doi:10.1111/hiv.12566
9. Rolle CP, Nguyen V, Hinestrosa F, DeJesus E. Clinical outcomes of HIV-1 infected patients switched from complex multi-tablet regimens to tenofovir alafenamide based single-tablet regimens plus a boosted protease inhibitor in a real-world setting. J Virus Erad. 2020;6:100021. doi:10.1016/j.jve.2020.100021
10. Fumaz CR, Tuldrà A, Ferrer MJ, et al. Quality of life, emotional status, and adherence of HIV-1-infected patients treated with efavirenz versus protease inhibitor-containing regimens. J Acquir Immune Defic Syndr. 2002;29:244–253. doi:10.1097/00042560-200203010-00004
11. Senneker T, Tseng A. An update on neuropsychiatric adverse effects with second-generation integrase inhibitors and nonnucleoside reverse transcriptase inhibitors. Curr Opin HIV AIDS. 2021;16(6):309–320. doi:10.1097/COH.0000000000000705
12. Martínez-Sanz J, Blanco JR, Muriel A, et al. Weight changes after antiretroviral therapy initiation in CoRIS (Spain): a prospective multicentre cohort study. J Int AIDS Soc. 2021;24:e25732. doi:10.1002/jia2.25732
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.