Back to Journals » Clinical Ophthalmology » Volume 20
Sutureless Amniotic Membrane Grafting in the Management of Corneal Perforations Associated with Severe Ocular Surface Disease
Authors Mancini M ![]() , Palino P
, Palino P ![]() , Valastro A, Scolaro A, Oliverio GW, Mancini A, Aragona P
, Valastro A, Scolaro A, Oliverio GW, Mancini A, Aragona P ![]() , Meduri A
, Meduri A ![]()
Received 13 November 2025
Accepted for publication 10 February 2026
Published 26 February 2026 Volume 2026:20 571757
DOI https://doi.org/10.2147/OPTH.S571757
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Maura Mancini,1,* Paola Palino,1,* Antonio Valastro,2,* Alessia Scolaro,1,* Giovanni William Oliverio,1,* Alessandra Mancini,3,* Pasquale Aragona,1,* Alessandro Meduri1,*
1Department of Biomedical Sciences, Ophthalmology Clinic, University of Messina, Messina, Italy; 2Ophthalmology Department, Beauregard Hospital, Azienda USL Della Valle d’Aosta, Aosta, Italy; 3Department of Ophthalmology, University Magna Graecia of Catanzaro, Catanzaro,Italy
*These authors contributed equally to this work
Correspondence: Paola Palino, Department of Biomedical Sciences, Ophthalmology Clinic, University of Messina, Via Consolare Valeria 1, Messina, 98125, Italy, Tel +39 3403612250, Email [email protected]
Purpose: To assess the safety and clinical outcomes of sutureless amniotic membrane (AM) transplantation in patients with small corneal perforations associated with severe ocular surface disease.
Patients and Methods: This prospective observational study included 50 eyes of 50 patients with autoimmune or inflammatory ocular surface disease presenting with corneal perforations ≤ 3 mm. Under topical anesthesia, a double-layer AM was applied without sutures: one layer as a graft directly over the perforation and a second as a patch. A therapeutic contact lens and temporary eyelid closure were used; no topical medications were prescribed, while oral doxycycline (100 mg twice daily) was given for 15 days. Patients were examined at 1 week, 2 weeks, 1 month, 3 months, and 6 months. Primary outcomes were anatomical closure and corneal thinnest point (swept-source OCT). Secondary outcomes included complications and need for further surgery.
Results: Complete anatomical closure was achieved in all cases (100%), with a mean healing time of 14.2 ± 3.6 days (range 9– 21). Corneal thinnest point increased significantly from 215 ± 38 μm at baseline to 402 ± 39 μm at 6 months (p = 0.000031, repeated-measures ANOVA). No cases of AM displacement, secondary infection, intraocular complications, or re-intervention were observed. The procedure was well tolerated in all patients.
Conclusion: Sutureless AM transplantation is a safe, minimally invasive, and effective option for managing ≤ 3 mm non-infectious corneal perforations in severe ocular surface disease. It enables rapid anatomical restoration, avoids suture-related inflammation, and may be particularly advantageous in fragile or immunocompromised patients.
Keywords: corneal perforation, ocular surface disease, amniotic membrane, sutureless grafting, dry eye, amniotic membrane transplantation, sutureless technique, autoimmune keratopathy, anterior segment optical coherence tomography
Introduction
Corneal perforations represent a potentially devastating and sight threatening ophthalmologic emergency, carrying a significant risk of irreversible visual impairment. Although they may result from a wide spectrum of causes (including infectious, traumatic, or inflammatory causes) an increasing proportion of cases are now attributed to severe ocular surface disease, in which tear film instability and chronic inflammation significantly compromise corneal integrity.1,2
Severe dry eye disease is a multifactorial condition involving chronic epithelial damage, corneal barrier dysfunction, persistent inflammatory activity, and immune dysregulation.3 In the context of systemic autoimmune disorders such as Sjögren’s syndrome or ocular graft-versus-host disease (oGVHD), progressive deterioration of the ocular surface microenvironment, characterized by tear film instability, reduced mucin secretion, altered corneal innervation, and limbal stem cell deficiency occurs. Together, these factors collectively contribute to the development of persistent epithelial defects, stromal ulceration, and, in advanced cases, corneal perforation.4–6
Corneal perforations arising in this context are particularly challenging to manage due to the pro-inflammatory milieu, reduced regenerative potential of the ocular surface, and a high recurrence rate. Conventional treatments—such as cyanoacrylate glue, therapeutic contact lenses, conjunctival patch grafts, or emergency keratoplasty—often fail to provide lasting anatomical and functional stability and are frequently associated with complications.7–9
Management of small corneal perforations remains particularly challenging in patients with severe ocular surface disease, in whom chronic inflammation, tissue fragility, and impaired healing often limit the effectiveness of conventional treatments.
Cyanoacrylate tissue adhesive is commonly used for small perforations but is frequently associated with local toxicity, inflammation, foreign body sensation, and limited long-term stability, especially in autoimmune or severe dry eye conditions. Recurrent leakage, infectious complications, and the need for repeated applications have also been reported.10–12
Conjunctival flap surgery and tectonic keratoplasty represent alternative options for restoring ocular integrity; however, both approaches are associated with relevant drawbacks in this clinical setting. Conjunctival flaps may compromise visual outcomes and are poorly tolerated in inflamed or cicatrized conjunctiva, while tectonic keratoplasty is invasive and characterized by high rates of graft failure, suture-related complications, and delayed epithelialization in compromised ocular surfaces.13–15
These limitations underscore the need for minimally invasive strategies capable of providing effective tectonic support while minimizing inflammation and surface toxicity. In this context, sutureless amniotic membrane grafting represents a biologically favorable option, combining mechanical sealing with the well-established anti-inflammatory and regenerative properties of the amniotic membrane.16–18,
Within this complex clinical scenario, amniotic membrane (AM) transplantation has gained increasing attention as a regenerative therapeutic option. The AM is a biological tissue with anti-inflammatory, anti-angiogenic, anti-apoptotic, and epithelium-promoting properties, making it particularly well-suited for the treatment of deep corneal lesions and perforations.19–21 In the context of severe inflammatory ocular surface disease, AM acts as a temporary scaffold that modulates the local tissue environment to support epithelial healing and stromal remodeling.22,23
More recently, the development of sutureless AM implantation techniques has expanded the clinical applicability of this treatment. These approaches allow for effective control of corneal perforation while minimizing surgical time, reducing postoperative inflammatory risk, and improving patient comfort.24–26 This is particularly advantageous in fragile patients with systemic comorbidities, in whom more invasive procedures may be contraindicated.
In the present study, we present our clinical experience with sutureless amniotic membrane transplantation for the treatment of corneal perforations in patients with severe dry eye disease. The analysis is based on a prospective database of surgically treated cases from our center, with the aim of evaluating the clinical efficacy, safety, and anatomical stability of this technique in a high-risk therapeutic setting where conventional surgical options are often limited.
Materials and Methods
A prospective observational study was conducted on 50 eyes with corneal perforation in patients affected by severe ocular surface disease. All surgical procedures were performed by the same experienced cornea specialist surgeon at the Ophthalmology Department of the University Hospital of Messina, Italy, between January 2023 and June 2025.
The study was conducted in accordance with the tenets of the Declaration of Helsinki and received approval from the Ethics Committee of the University Hospital of Messina (86/19 of 2 october 2019).
Written informed consent, for processing personal data and for surgical procedure, was obtained from participants to participate in the study.
The inclusion criteria were: Documented corneal perforation with a diameter ≤3 mm; Severe dry eye disease diagnosed both clinically and instrumentally; Presence of ocular surface disease of inflammatory or autoimmune origin; Absence of active ocular infection at the time of surgery; Age ≥18 years. The exclusion criteria were: Corneal perforations >3 mm or associated with massive iris prolapse; Presence of active infectious keratitis; Prior corneal transplantation in the treated eye within the past 3 months.
The underlying conditions of the included patients were: Primary or secondary Sjögren’s syndrome (n = 22), Ocular graft-versus-host disease (oGVHD) (n = 14), Idiopathic severe dry eye (n = 6), Stevens-Johnson syndrome (n = 4) and Post-surgical/iatrogenic dry eye (n = 4).
Severe ocular surface disease was diagnosed based on slit-lamp biomicroscopy (including severe punctate keratopathy/epithelial defects, ocular surface inflammation, and tear film instability).
All patients underwent comprehensive preoperative evaluation including: Slit-lamp biomicroscopy (Topcon SL-D701, Topcon Corp., Tokyo, Japan); Corneal OCT using Triton swept-source OCT (Topcon Corporation, Tokyo, Japan); Fluorescein staining.
Baseline corneal perforation diameter was measured at presentation using anterior segment optical coherence tomography (AS-OCT) with manual caliper-based measurements, relying on the integrated measurement tools of the device to accurately evaluate perforation size and margins prior to surgical intervention (Figure 1).
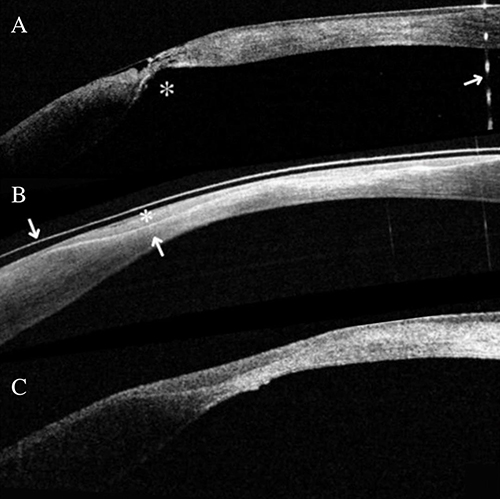 |
Figure 1 (A) Patient number 3, right eye. Anterior segment optical coherence tomography (AS-OCT) showing corneal thinning with residual stromal tissue (asterisk), Seidel positive. A reflex saturation beam artifact is visible as a dashed line (arrow). (B) shows the postoperative outcome at week 1. The therapeutic lens is seen above the corneal epithelium as a hyper-reflective band (arrow). The epithelium regrowth is indicated by a small asterisk and delimited by the Bowman’s membrane, visible as hyper-reflective band (arrow). (C) The post-op outcome at 1 month shows a similar corneal appearance to week 1. |
Corneal perforations were classified according to their location as central, paracentral, or peripheral based on slit-lamp examination and anterior segment optical coherence tomography at presentation. The influence of perforation location on healing time and anatomical outcome was specifically evaluated during follow-up.
Surgical Technique
All procedures were performed in an outpatient setting. After disinfection of the eyelid skin with 5% povidone-iodine, the eye was draped, and a lid speculum was placed. Oxybuprocaine hydrochloride 0.4% (Novesina™, Laboratoires Thea) was used as topical anesthesia. The ocular surface was then disinfected with 5% povidone-iodine for three minutes. A standardized interval of approximately 3 minutes was allowed after membrane placement to promote initial adherence and stabilization prior to eyelid occlusion. The amniotic membrane (AM) used in this study was a commercially available, eye bank–processed, cryopreserved human amniotic membrane, stored under controlled conditions and compliant with international sterility standards. Intraoperatively, the correct orientation of the membrane was carefully verified to ensure that the basement membrane side was positioned facing the corneal surface. The AM was trimmed using Westcott scissors: The first layer, cut to be 4 mm larger in diameter than the perforation site, was applied directly over the perforation as a graft; A second, larger layer was then placed over the first, serving as a patch. (Figure 2) The 4-mm patch size was selected according to our standardized protocol to ensure complete coverage of the perforation with an adequate safety margin.Both layers were positioned with the epithelial side facing up. Prior to amniotic membrane application, limited corneal surface preparation was performed when necessary. Specifically, loose or necrotic epithelium at the margins of the perforation was gently removed to promote membrane adhesion, while aggressive stromal debridement was intentionally avoided in order to preserve residual corneal tissue integrity in eyes with severe ocular surface disease.
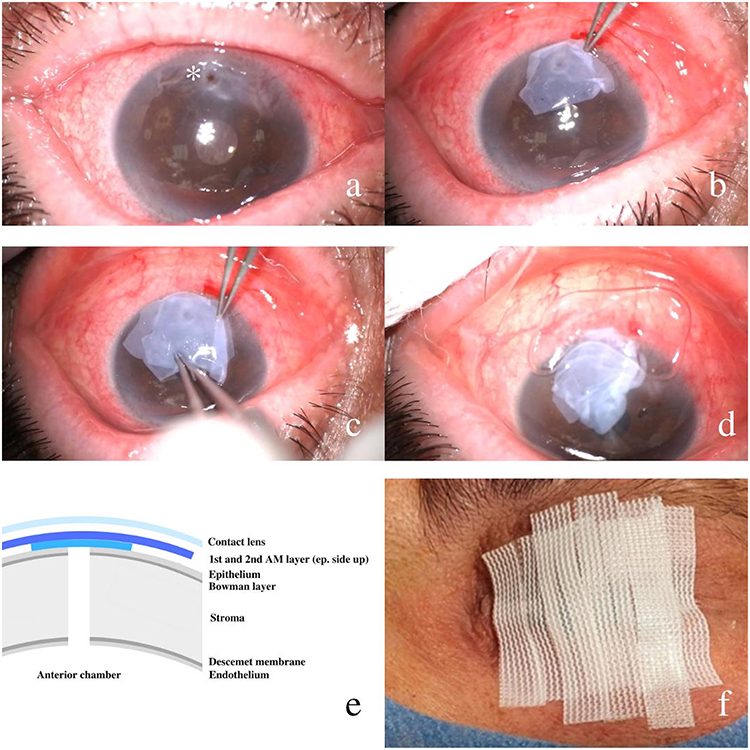 |
Figure 2 Corneal perforation (asterisk) (a). First layer of amnioticmembrane (AM) covering the corneal perforation (b). Second layer of AM placed on top of the first AM layer (c). Contact lens (12 mm diameter) placed above the 2 AM layers (d). Schematic representation of result of the surgical technique showing the 2 layers of AM covering the corneal perforation. The contact lens is shown on top of them (e). Reinforced skin closure strips 100mmx12mm used to close the eyelids (f). |
At the end of the procedure a therapeutic contact lens (Pure Vision 2™, Bausch + Lomb, Bridgewater, NJ, USA; 12 mm diameter) was applied. The eyelids were occluded using a reinforced skin closure strips 100mmx12mm (3M™ Steri-Strip™ R-100 × 12 mm) (Figure 2).
Before eyelid occlusion with reinforced skin closure strips, topical moxifloxacin was administered as perioperative prophylaxis according to the institutional protocol. The eyelids were then closed to maintain correct membrane positioning and to reduce mechanical stress on the ocular surface.
Postoperative Management
No topical eye drops were prescribed postoperatively. The therapeutic contact lens and eyelid closure were maintained for 1 to 2 weeks, based on clinical response. A therapeutic bandage contact lens was applied in extended wear and was removed or replaced according to predefined clinical criteria during follow-up. Postoperative management and timing of device removal were guided by objective clinical criteria, including epithelial integrity on fluorescein staining, a negative Seidel test, and AS-OCT confirmation of stromal continuity.
All patients were prescribed oral doxycycline 100 mg twice daily for 15 days.
Follow-Up and Postoperative Evaluation
Patients were followed up at 1 week, 2 weeks, 1 month, 3 months, and 6 months postoperatively. Follow-up assessments included: Slit-lamp examination (Topcon SL-D701); Evaluation of corneal integrity and epithelial healing with fluorescein; High-resolution corneal OCT (Triton, Topcon) to monitor closure of the perforation and corneal thinnest point; IOP measurement with iCare rebound tonometry.
The primary endpoint of the study was complete anatomical closure of the corneal perforation, defined as restoration of stromal continuity confirmed by a negative Seidel test and anterior segment optical coherence tomography (AS-OCT). Anatomical closure was primarily assessed during the early postoperative period, within the first 2–3 weeks after surgery. Patients were subsequently followed for up to 6 months to monitor stability of closure, corneal thickness remodeling, and the occurrence of any delayed failure or late structural changes.
Epithelial adhesion and healing were evaluated using slit-lamp biomicroscopy with fluorescein staining, assessing complete epithelial coverage and absence of staining over the perforation site. Anatomical closure was confirmed by a negative Seidel test and supported by anterior segment optical coherence tomography (AS-OCT), which documented stromal continuity and integration of the amniotic membrane. The occurrence of delayed epithelialization or recurrent epithelial defects was specifically assessed during follow-up.
Objective imaging (AS-OCT) and standardized clinical assessments were performed by the same experienced personnel whenever feasible, using a consistent acquisition protocol to minimize inter-operator variability.
Statistical Analysis
Data were analysed using SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables are reported as mean ± standard deviation (SD), while categorical variables are expressed as absolute frequencies and percentages. Normality of data distribution was assessed using the Shapiro–Wilk test. Differences in corneal thinnest point across follow-up timepoints were evaluated using repeated-measures analysis of variance (ANOVA), with Greenhouse–Geisser correction applied when assumptions of sphericity were violated. A P value of less than 0.05 was considered statistically significant.
Results
A total of 50 patients (50 eyes) were included in the study. The cohort included 18 males (36%) and 32 females (64%), with a mean age of 62.4 ± 11.7 years (range: 39–82 years). The underlying conditions were distributed as follows: Primary or secondary Sjögren’s syndrome: 22 cases (44%); Ocular graft-versus-host disease (oGVHD): 14 cases (28%); Severe idiopathic dry eye: 6 cases (12%); Stevens-Johnson syndrome: 4 cases (8%); Post-surgical/iatrogenic dry eye: 4 cases (8%).
The mean baseline diameter of the corneal perforations was 2.1 ± 0.6 mm, with all cases falling within the ≤3 mm limit established by the inclusion criteria.
Complete closure of the corneal perforation was achieved in all cases (100%), with a mean closure time of 14.2 ± 3.6 days (range: 9–21 days), as confirmed by high-resolution OCT and absence of fluorescein leakage. No patients developed intraocular complications or required additional surgical interventions.
Complete anatomical closure was achieved in all treated eyes, with no cases of partial closure, recurrence of perforation, or need for re-intervention during the follow-up period. No progressive stromal thinning or late structural failure was observed. No significant procedure-related complications were recorded. In particular, no cases of persistent ocular pain, increased inflammation, epithelial defects adjacent to the amniotic membrane, contact lens–related complications, or eyelid-closure–related adverse events were observed. Structural outcomes were satisfactory in all cases, with no clinically relevant irregular scarring or visually significant astigmatism. The study was designed to collect objective anatomical and imaging-based outcomes, and patient-reported questionnaires such as the Ocular Surface Disease Index (OSDI) were not administered. In patients with Sjögren’s syndrome, a subjective improvement in ocular comfort was noted during follow-up, without evidence of worsening ocular surface inflammation.
The evolution of corneal thinnest point was monitored over time using high-resolution swept-source OCT. (Figure 3) Mean values ± standard deviation at each follow-up point were as follows: Preoperative (baseline): 215 ± 38 µm; After 1 week: 276 ± 41 µm; After 2 weeks: 312 ± 46 µm; After 1 month: 355 ± 50 µm; After 3 months: 388 ± 44 µm; After 6 months: 402 ± 39 µm (Table 1, Figures 1 and 3).
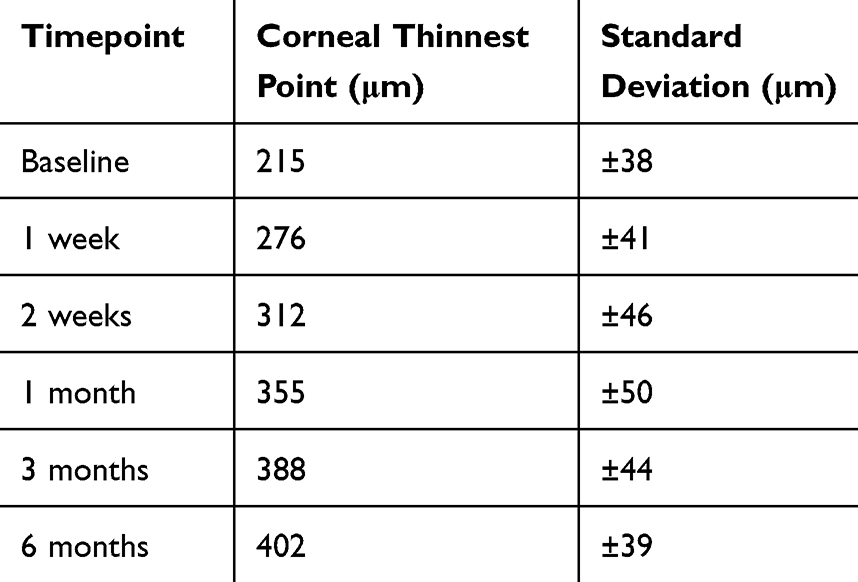 |
Table 1 Evolution of Central Corneal Thinnest Point in Patients Undergoing Sutureless Amniotic Membrane Grafting for Inflammatory-Related Corneal Perforations. Values are Expressed as Mean ± Standard Deviation |
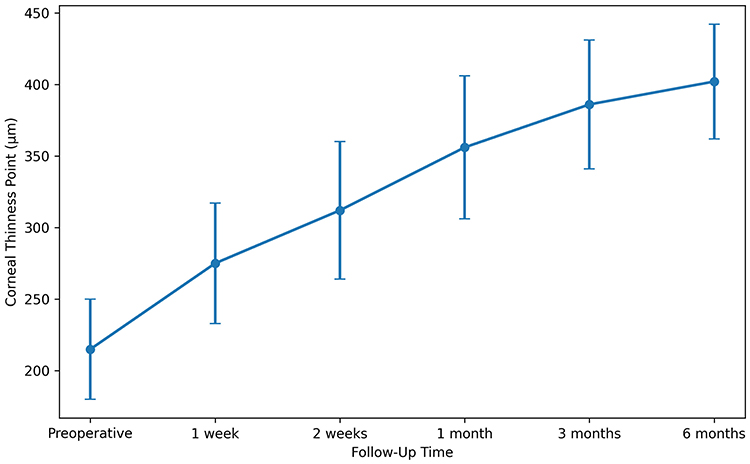 |
Figure 3 Temporal evolution of corneal thinness point measured by OCT in patients with ≤3 mm corneal perforations treated with sutureless amniotic membrane implantation. Values are expressed as mean ± standard deviation at each follow-up time point (preoperative, 1 week, 2 weeks, 1 month, 3 months, 6 months). Repeated-measures analysis of variance (ANOVA-RM) revealed a statistically significant increase in stromal thickness over time (p = 0.000031). |
Repeated-measures analysis of variance (ANOVA-RM) revealed a statistically significant increase in corneal thinnest point over time, with a p-value of 0.000031, supporting a gradual and stable anatomical recovery of the cornea following treatment. The procedure was well tolerated. No cases of infection, amniotic membrane graft dislocation, or acute inflammatory reactions were reported.
Discussion
Corneal perforations associated with autoimmune forms of dry eye disease—such as Sjögren’s syndrome and ocular graft-versus-host disease (oGVHD)—typically arise from chronic epithelial instability, persistent inflammation, and progressive stromal degradation.3,4,6 These conditions are characterized by severe ocular surface alterations including conjunctival inflammation, keratoconjunctivitis sicca, filamentary keratitis, and recurrent epithelial defects. In advanced stages, progressive stromal melting can lead to descemetocele formation and frank perforation. Patients often present with pain, photophobia, ocular redness, and significant visual decline, which may culminate in corneal opacification or irreversible structural damage if left untreated.
In particular, in patients with oGVHD, the frequency of corneal perforations has recently been reported as significantly high, with complication rates that threaten not only vision but also the long-term prognosis of the affected eye.27
Conventional management of autoimmune-related corneal ulcers and perforations involves both local and systemic therapeutic strategies. Lubricating agents, autologous serum tears, topical anti-inflammatory drugs (such as corticosteroids and cyclosporine), and systemic immunosuppression are frequently employed to stabilize the ocular surface and control immune-mediated damage. In cases of corneal thinning or impending perforation, surgical options have included cyanoacrylate glue application, bandage or scleral contact lenses, conjunctival flap procedures, and tectonic keratoplasty.1,2 While these approaches can provide temporary stabilization, their efficacy is often limited in the context of persistent autoimmune activity, and recurrence or progression to perforation remains common. In addition, emergency keratoplasties in autoimmune contexts have been observed to carry a less favorable prognosis, with an increased risk of graft rejection and chronic inflammatory complications, thereby necessitating the use of regenerative therapies such as amniotic membrane transplantation. Within this challenging clinical scenario, amniotic membrane transplantation has emerged as a particularly promising option. The AM serves not only as a physical barrier but also as a biologically active scaffold containing extracellular matrix proteins, growth factors, and protease inhibitors that collectively promote epithelialization and stromal healing, while reducing inflammatory and fibrotic responses.19,20 Its role in ocular surface reconstruction has been widely recognized since early pioneering reports,28 and multiple case series and reviews have confirmed its utility in managing non-infectious corneal ulcers and descemetoceles.29,30 In particular, He et al (2023) described successful multilayer AMT in a patient with oGVHD-related descemetocele, underscoring its relevance in autoimmune settings.31
The use of amniotic membrane has also been supported by high-resolution imaging studies, such as that of Sultana et al (2018), which documented through OCT its ability to integrate and support structural recovery even in cases of advanced descemetocele.30
More recently, a systematic review has confirmed the efficacy of AM even in complex infectious settings, suggesting that its regenerative and anti-inflammatory properties may be extended to a wide range of corneal conditions, including those of autoimmune origin.29
Our present study demonstrates that sutureless AM transplantation represents a safe and effective therapeutic option for the management of small-diameter corneal perforations (≤3 mm) in patients with severe ocular surface disease. The complete anatomical closure observed in all cases, the progressive restoration of corneal thinnest point, and the absence of major postoperative complications confirm the regenerative and anti-inflammatory potential of AM in severely compromised corneal environments.
A previous study from our research group laid the conceptual and methodological foundation for the present work.9 In that study, 12 eyes of 11 patients affected by Sjögren’s syndrome (n = 5) and ocular cicatricial pemphigoid (n = 6) were analyzed, demonstrating the feasibility and efficacy of sutureless amniotic membrane transplantation in inflammatory corneal perforations.9
The present study expands upon those preliminary findings by including a larger and more heterogeneous cohort, consisting of 50 eyes from 50 patients with primary or secondary Sjögren’s syndrome (n = 22), ocular graft-versus-host disease (oGVHD) (n = 14), idiopathic severe dry eye (n = 6), Stevens–Johnson syndrome (n = 4), and postsurgical/iatrogenic dry eye (n = 4). The greater variety of underlying pathologies and the larger sample size provide enhanced statistical and clinical significance to the results compared with the previously published study.
This sutureless AM implantation technique offers several advantages: it represents a minimally invasive approach, as the absence of sutures reduces surgical time, patient discomfort, and postoperative inflammation related to suture material;24,25 it promotes rapid healing and effective biointegration, since a mean closure time of less than 15 days and the absence of membrane dislocation confirm the anatomical reliability of the technique;23 and it simplifies postoperative management, as the lack of topical therapy and the use of oral doxycycline alone made the postoperative regimen more manageable and well tolerated.9
However, the study also presents some limitations: although effective in small perforations, the technique may not be suitable for larger defects (>3 mm), massive iris prolapse, or active infectious keratitis, which require more invasive interventions such as tectonic keratoplasty or multilayer AM grafting.1,8 Furthermore, the study focused on anatomical recovery without evaluating visual or functional parameters; and the absence of a control group treated with sutured AM or other surgical techniques limits the generalizability of the findings.
Our results are consistent with previous observational reports and small-scale clinical studies supporting the use of the sutureless technique for managing persistent epithelial defects and early-stage corneal perforations.21,25 Stamate et al (2019) and Zemanová et al (2021) reported similar anatomical success rates using sutured techniques, which, however, are more invasive and associated with a higher incidence of postoperative inflammation.2,32 Therefore, the sutureless approach may represent a paradigm shift in the acute management of non-infectious corneal perforations, particularly in immunocompromised or systemically fragile patients.
Conclusion
Sutureless amniotic membrane grafting appears to be a safe and effective technique for the management of small corneal perforations in patients with severe ocular surface disease. In this case series, the procedure consistently achieved anatomical closure without intraocular complications and with favorable structural outcomes. This minimally invasive approach may represent a valuable alternative to conventional surgical techniques in selected cases, particularly in fragile ocular surface conditions. Further studies with larger cohorts are warranted to confirm these findings and to better define long-term outcomes.
Funding
This research received no specific grant from any funding agency in the public (National Institutes of Health; Wellcome Trust; Howard Hughes Medical Institute; and others), commercial or not-for-profit sectors.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Deshmukh R, Stevenson LJ, Vajpayee R. Management of corneal perforations: an update. Indian J Ophthalmol. 2020;68(1):7–9. PMID: 31856457; PMCID: PMC6951192. doi:10.4103/ijo.IJO_1151_19
2. Stamate AC, Tătaru CP, Zemba M. Update on surgical management of corneal ulceration and perforation. Rom J Ophthalmol. 2019;63(2):166–173. PMID: 31334396; PMCID: PMC6626930. doi:10.22336/rjo.2019.25
3. Akpek EK, Bunya VY, Saldanha IJ. Sjögren’s syndrome: more than just dry eye. Cornea. 2019;38(5):658–661. PMID: 30681523; PMCID: PMC6482458. doi:10.1097/ICO.0000000000001865
4. Soleimani M, Mahdavi Sharif P, Cheraqpour K, et al. Ocular graft-versus-host disease (oGVHD): from A to Z. Surv Ophthalmol. 2023;68(4):697–712. PMID: 36870423; PMCID: PMC10293080. doi:10.1016/j.survophthal.2023.02.006
5. Nair S, Vanathi M, Mukhija R, Tandon R, Jain S, Ogawa Y. Update on ocular graft-versus-host disease. Indian J Ophthalmol. 2021;69(5):1038–1050. PMID: 33913829; PMCID: PMC8186644. doi:10.4103/ijo.IJO_2016_20
6. Singh S, Chaudhary S, Das AV, Basu S. Presentation, aetiology and outcomes of corneal ulceration in Sjogren’s syndrome. Eye. 2023;37(15):3217–3220. PMID: 36944710; PMCID: PMC10564785. doi:10.1038/s41433-023-02494-z
7. Zhang CY, Farooq AV, Harocopos GJ, et al. Corneal perforation in ocular graft-versus-host disease. Am J Ophthalmol Case Rep. 2021;24:101224. PMID: 34805617; PMCID: PMC8586569. doi:10.1016/j.ajoc.2021.101224
8. Ciftci MD, Selver OB. Sandwich technique and amniotic membrane transplantation as an effective method in repairing corneal perforations. Middle East Afr J Ophthalmol. 2024;30(4):246–249. PMID: 39959590; PMCID: PMC11823530. doi:10.4103/meajo.meajo_191_23
9. Meduri A, Valastro A, Inferrera L, et al. Sutureless amniotic membrane transplantation in inflammatory corneal perforations. Applied Sciences. 2022;12(8):3924. doi:10.3390/app12083924
10. Vote BJ, Elder MJ. Cyanoacrylate glue for corneal perforations: a description of a surgical technique and a review of the literature. Clin Exp Ophthalmol. 2000;28(6):437–442. PMID: 11202468. doi:10.1046/j.1442-9071.2000.00351.x
11. Setlik DE, Seldomridge DL, Adelman RA, Semchyshyn TM, Afshari NA. The effectiveness of isobutyl cyanoacrylate tissue adhesive for the treatment of corneal perforations. Am J Ophthalmol. 2005;140(5):920–921. PMID: 16310475. doi:10.1016/j.ajo.2005.04.062
12. Vote BJ, Elder MJ. Cyanoacrylate glue for corneal perforations: a description of techniques and review of outcomes. Cornea. 2000;19:639–643.
13. Gundersen T. Conjunctival flaps in the treatment of corneal disease. Arch Ophthalmol. 1958;60:880–888. doi:10.1001/archopht.1958.00940080900008
14. Shimmura S, Higa A, Omoto M, Shimazaki J, Tsubota K. Deep lamellar keratoplasty in severe ocular surface disease. Nippon Ganka Gakkai Zasshi. 2007;111(5):391–396. PMID: 17536498. Japanese.
15. Dohlman CH, Hashemi H, Piri N, et al. Keratoplasty in inflammatory ocular surface disorders. Cornea. 2010;29:110–116. doi:10.1097/ICO.0b013e3181a0a220
16. Dua HS, Gomes JAP, King AJ, et al. Amniotic membrane transplantation in ophthalmology. Surv Ophthalmol. 2004;49:51–77. doi:10.1016/j.survophthal.2003.10.004
17. Tseng SCG. Amniotic membrane transplantation for ocular surface reconstruction. Ophthalmology. 2001;108:207–217.
18. Mimouni M, Trinh T, Sorkin N, et al. Sutureless dehydrated amniotic membrane for persistent epithelial defects. Eur J Ophthalmol. PMID: 33887988. doi:10.1177/11206721211011354
19. Meller D, Pauklin M, Thomasen H, Westekemper H, Steuhl KP. Amniotic membrane transplantation in the human eye. Dtsch Arztebl Int. 2011;108(14):243–248. PMID: 21547164; PMCID: PMC3087122. doi:10.3238/arztebl.2011.0243
20. Röck T, Bartz-Schmidt KU, Landenberger J, Bramkamp M, Röck D. Amniotic membrane transplantation in reconstructive and regenerative ophthalmology. Ann Transplant. 2018;23:160–165. PMID: 29507278; PMCID: PMC6248296. doi:10.12659/AOT.906856
21. Şapte E, Costea CF, Cărăuleanu A, et al. Histological, immunohistochemical and clinical considerations on amniotic membrane transplant for ocular surface reconstruction. Rom J Morphol Embryol. 2017;58(2):363–369. PMID: 28730219.
22. Thatte S. Amniotic membrane transplantation: an option for ocular surface disorders. Oman J Ophthalmol. 2011;4(2):67–72. PMID: 21897621; PMCID: PMC3160072. doi:10.4103/0974-620X.83656
23. Finger PT, Jain P, Mukkamala SK. Super-Thick amniotic membrane graft for ocular surface reconstruction. Am J Ophthalmol. 2019;198:45–53. PMID: 30312574. doi:10.1016/j.ajo.2018.09.035
24. Kotomin I, Valtink M, Hofmann K, et al. Sutureless fixation of amniotic membrane for therapy of ocular surface disorders. PLoS One. 2015;10(5):e0125035. PMID: 25955359; PMCID: PMC4425509. doi:10.1371/journal.pone.0125035
25. Choi CM, Jeon HS. Clinical outcomes of in-office sutureless amniotic membrane transplantation in persistent epithelial defect. Korean J Ophthalmol. 2022;36(2):87–96. PMID: 34823345; PMCID: PMC9013553. doi:10.3341/kjo.2021.0095
26. Chiu HI, Self-Retained TCC. Sutureless amniotic membrane transplantation for the management of ocular surface diseases. J Clin Med. 2023;12(19):6222. PMID: 37834866; PMCID: PMC10573988. doi:10.3390/jcm12196222
27. Xu Y, Wang YM, Sun ZT, et al. Corneal perforation associated with ocular graft-versus-host disease. Front Oncol. 2022;12:962250. PMID: 36185180. PMCID: PMC9521353. doi:10.3389/fonc.2022.962250
28. Sangwan VS. Amniotic membrane transplantation. Indian J Ophthalmol. 2002;50(3):169–170. PMID: 12355689.
29. Thevi T, Abas AL, Dua HS. Amniotic membrane graft (AMG) for persistent epithelial defects following infective corneal ulcers and keratitis - A systematic review. Indian J Ophthalmol. 2024;73(Suppl 3):S361–S368. PMID: 39257085. doi:10.4103/IJO.IJO_300_24
30. Sultana N, Chaurasia S, Ramappa M. High-resolution optical coherence tomography in a case of descemetocele managed with amniotic membrane transplantation. Indian J Ophthalmol. 2018;66(2):315–317. PMID: 29380791; PMCID: PMC5819128. doi:10.4103/ijo.IJO_697_17
31. He Y, Wong H, Gu J, Lin L. Corneal descemetocele management with multi-layer amniotic membrane transplantation in an ocular graft-versus-host disease case. Medicina. 2023;59(10):1733. PMID: 37893451; PMCID: PMC10607979. doi:10.3390/medicina59101733
32. Zemanová M, Pacasová R, Šustáčková J, Vlková E. Amniotic membrane transplantation at the department of ophthalmology of the university hospital BRNO. Cesk Slov Oftalmol. 2021;77(2):62–71. PMID: 33985335. doi:10.31348/2021/9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Lacrimal Duct Obstruction and Infection Associated with Non-Traumatic Corneal Perforation: A Case Series
Nitta K, Mukai R, Todokoro D, Akiyama H
International Medical Case Reports Journal 2022, 15:313-322
Published Date: 23 June 2022
Ocular Surface Disease Related to the Inflammatory and Non-Inflammatory Phases of Thyroid Eye Disease
Riguetto CM, Barbosa EB, Atihe CC, Reis F, Alves M, Zantut-Wittmann DE
Clinical Ophthalmology 2023, 17:3465-3475
Published Date: 15 November 2023
Shelf-Stable, Cryopreserved Amniotic Membrane for the Management of Ocular Surface Disease: A Retrospective Assessment
Cushman S
Clinical Optometry 2025, 17:409-415
Published Date: 21 December 2025
Comparison of Effectiveness of Biovance Single and Triple Layer Decellularized Basement Membranes for Treatment of Ocular Surface Disease: A Retrospective Study
Denton M
Clinical Optometry 2026, 18:571568
Published Date: 5 February 2026
Management of Stage 1 Neurotrophic Keratopathy with Shelf-Stable, Cryopreserved Amniotic Membrane: A Retrospective Study
Bauza AM
Clinical Ophthalmology 2026, 20:591419
Published Date: 13 April 2026