Back to Journals » Clinical Optometry » Volume 18
Comparison of Effectiveness of Biovance Single and Triple Layer Decellularized Basement Membranes for Treatment of Ocular Surface Disease: A Retrospective Study
Authors Denton M
Received 1 October 2025
Accepted for publication 13 January 2026
Published 5 February 2026 Volume 2026:18 571568
DOI https://doi.org/10.2147/OPTO.S571568
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Chris Lievens
Melanie Denton
University of Alabama School of Optometry; Department of Optometry and Vision Science, Birmingham, AL, USA
Correspondence: Melanie Denton, Salisbury Eyecare and Eyewear, 228 West Council Street, Salisbury, SC, USA, 28144, Tel +1 (704) 310-5002, Email [email protected]
Introduction: Dry eye disease (DED) is a multifactorial disorder characterized by tear film instability, ocular surface inflammation, and epithelial compromise, often predisposing patients to complications such as acute keratitis and persistent corneal epithelial defects. Amniotic membrane therapy has emerged as a valuable treatment modality for DED due to its ability to protect against mechanical trauma, modulate inflammation and fibrosis, promote corneal epithelial migration, and help restore ocular surface homeostasis in refractory cases.
Methods: This retrospective clinical series evaluated the long-term outcomes of a dehydrated, decellularized basement membrane (DBM) allograft (Biovance) used in conjunction with pressure patching in 17 eyes. Patients were treated with either Biovance SL (single-layer DBM) or Biovance Ocular 3L (three-layer DBM), and corneal healing was assessed over a 6-month period.
Results: Both treatment groups demonstrated statistically significant reductions in corneal fluorescein staining at 3 and 6 months. At 6 months, the reduction in corneal staining in the three-layer group was statistically significantly greater than that observed in the single-layer group.
Conclusion: The Biovance 3L Ocular group exhibited a greater magnitude and duration of corneal staining improvement compared to the Biovance SL group; thereby, supporting the enhanced long-term efficacy of the multi-layer DBM construct in the treatment of DED-related epithelial disease.
Keywords: amniotic membrane, dry eye, biovance, decellularization
Introduction
Dry eye disease (DED) is a multifactorial disorder characterized by tear film instability, ocular surface inflammation, and epithelial compromise,1 predisposing to clinical diseases such as acute keratitis associated with persistent corneal epithelial defects (PCED).2 The corneal epithelial cell turnover rate is responsible for facilitating healing of acute corneal epithelial defects.3 Management of moderate to severe DED associated with PCED is challenging and typically consists of stepwise treatments such as lid hygiene, frequent lubrication, immunomodulators, pulse steroids, and recalcitrant cases often require autologous serum or platelet-rich plasma tears or amniotic membrane tissue (AMT).4–7
AMT has been increasingly adopted as a therapy since it acts as a protective covering preventing mechanical disruption, modulates inflammation and fibrosis, supports corneal epithelial migration, and helps restore surface homeostasis in treatment‑refractory DED and related epithelial disease.8–11
Not all AMT is the same. Functionally, AMT fall into three categories based on their preservation technique including 1) cryopreserved, 2) conventional dehydrated, and 3) decellularized basement membrane. Further, AMT is available as a single layer or multilayer grafts; however some multilayer grafts include amnion and chorion whereas decellularized multilayer grafts are essentially several single layers laminated together.12 Further, multilayer AMT has been more effective than autologous serum at healing corneal ulcers caused by herpetic neurotrophic keratitis (NK),13 better for treating deep neurotrophic corneal ulcers14 and recommended for more severe dry eye and NK.12
Amniotic membranes have several layers; however, it is the basement membrane that is the most important structure for re-epithelialization.12 The basement membrane contains extracellular matrix proteins such as elastin and collagen that provide a scaffold for cellular migration and signaling proteins such as fibronectin, laminin, and glycosaminoglycans that produce growth factors and anti-inflammatory cytokines.12
Historically cryopreservation was thought to be the most effective AMT for healing. Mechanical decellularization removes the pro-inflammatory chorion and residual donor cellular debris, thereby reducing immunogenicity while preserving extracellular matrix proteins such as collagen, fibronectin, and laminin, which promote epithelial adhesion and migration.12 However, decellularized basement membrane (Biovance and Biovance Ocular 3L; DefEYE, Inc., Sarasota, FL) has demonstrated more efficient cellular interactions resulting in faster cellular proliferation and migration when compared head-to-head against both conventional dehydrated and cryopreserved AMT.15 The three-layer tissue consists of a single layer of decellularized basement membrane, laminated together without heat or freeze-drying. Further, a recent study by Linsey et al demonstrated that decellularized basement membrane used in DED and NK showed complete epithelial healing of 100% through 1 week follow up versus cryopreserved12 and conventional dehydrated12–17 results of approximately 45% initial epithelial resolution.
In this retrospective clinical series, 17 eyes of patients that received a dehydrated, decellularized basement membrane (DBM) in combination with pressure patching were compared to determine the long-term clinical impact of the Biovance SL (single layer) and the Biovance Ocular 3L (three layer) for continued corneal healing over time.
Method
A retrospective case series study protocol was reviewed by the Institutional Review Board (IRB) at Advarra, and the need for informed consent was determined to be exempt from IRB oversight. The IRB determined that the study met the criteria for a waiver because it was minimal risk to participants, used de-identified data and was a retrospective study. Furthermore, the research adhered to the ethical standards outlined in the Declaration of Helsinki, ensuring compliance with guidelines for conducting research involving human participants.
A retrospective case series was performed that looked at the use of a single-layer Biovance and Biovance Ocular 3L to determine impact on epithelial staining and duration of impact. Patients were seen at baseline and determined to have moderate to severe dry eye and required to be seen in follow up at 3 months and 6 months post amniotic membrane placement. Corneal fluorescein staining was used to grade the severity of persistent epithelial defects at each visit.
Inclusion Criteria
Inclusion Criteria (all criteria apply to each study eye):
- Age 18 years and older of any gender or race.
- Diagnosis of dry eye by the Standard Patient Evaluation of Eye Dryness (SPEED) questionnaire.
- History of artificial tears, lid hygiene, and either cyclosporine or lifitegrast.
- TBUT ≤5 seconds or Schirmer test ≤ 5mm.
- At least 1+ corneal staining using the Oxford Corneal Staining scale.
Exclusion Criteria
Exclusion Criteria (all criteria apply to each study eye):
- Patients with incomplete medical records or missing follow-up data.
- Any of the following active ocular (eye or eyelid) conditions in either eye at the baseline:
- Active ocular infection (eg, viral, bacterial, mycobacterial, protozoan, or fungal infection of the cornea, conjunctiva, lacrimal gland, lacrimal sac, or eyelids including a hordeolum or stye).
- Active ocular inflammation or history of chronic, recurrent ocular inflammation within prior 3 months (eg retinitis, macular inflammation, choroiditis, uveitis, iritis, scleritis, episcleritis, keratitis).
- Moderate to severe (Grade 2–4) allergic, vernal or giant papillary conjunctivitis.
- Lid surface abnormalities (eg, entropion, ectropion, tumor, edema, blepharospasm, lagophthalmos, severe trichiasis, severe ptosis) that affect lid function in either eye
- Contact lens wearers or individuals who have worn contact lenses in the last 30 days or anticipate wearing contact lenses during this study.
All patients received a dehydrated, amniotic decellularized basement membrane (Biovance®, DefEYE, Inc.; Sarasota, FL) applied to the ocular surface in the setting of advanced ocular surface disease caused by DED. Anesthetic was applied to the eye and a topical antibiotic. An eyelid speculum was placed. The corneal surface dried with a sponge. The DBM was placed with toothless forceps and painted down with a wet sponge. The speculum was removed and the eyelids were then gently closed. Two sterile eye pads were positioned over the closed eyelids and the eye taped close. A firm but comfortable external pressure was created to secure the pad in place and provide mild continuous pressure. Care was taken to ensure that the pressure was evenly distributed and that the tape did not cause undue tension on the periocular skin.
For single-layer DBM applications, the pressure patch was maintained for 24 hours, during which time patients were instructed to avoid touching or manipulating the treated eye. For the three-layer DBM, the pressure patch was extended to 72 hours to support enhanced adherence and integration.
At the end of the designated patching period, the external patch was removed, and the ocular surface was then examined at the slit lamp to evaluate graft integrity, degree of dissolution, and epithelial healing. Post-patching, patients resumed their standard topical medications (lubricants, anti-inflammatories, or antimicrobials as indicated) and were monitored for clinical improvement over the subsequent days to weeks.
Corneal fluorescein was instilled into the conjunctival sac using an impregnated strip or solution. The patient was asked to blink several times to distribute the dye evenly across the ocular surface. After 1–3 minutes the cornea and conjunctiva were examined under a slit lamp using a cobalt blue light.
The staining severity was scored based on the Oxford Corneal Staining scale, 0 to 5, where a higher number indicates more damage to the ocular surface. These results were recorded at baseline prior to receiving a DBM as well as at 1 month, 3 months, and 6 months.
No topical corticosteroids or bandage contact lenses were applied during the patching period to avoid interference with membrane incorporation or dissolution.
Statistical Analysis
Seventeen eyes from nine patients met inclusion criteria and were divided into two groups: 9 eyes received the single-layer (SL) Biovance DBM and 8 eyes received the three-layer (3L) Biovance Ocular DBM. Corneal fluorescein staining was assessed using the Oxford grading scale (0–5) at baseline, 1 month, 3 months, and 6 months. Paired and independent t-tests were conducted to evaluate within-group changes over time and between-group differences at 3 and 6 month time points. The alpha level was set at 0.05.
Results
Seventeen eyes from 9 patients met the enrollment criteria (see Table 1). Nine eyes received the Biovance (single layer DBM) and 8 eyes received the Biovance 3L Ocular (three-layer DBM). Of the three-layer group, 2/8 patients did not have staining recorded at their 1-month visit.
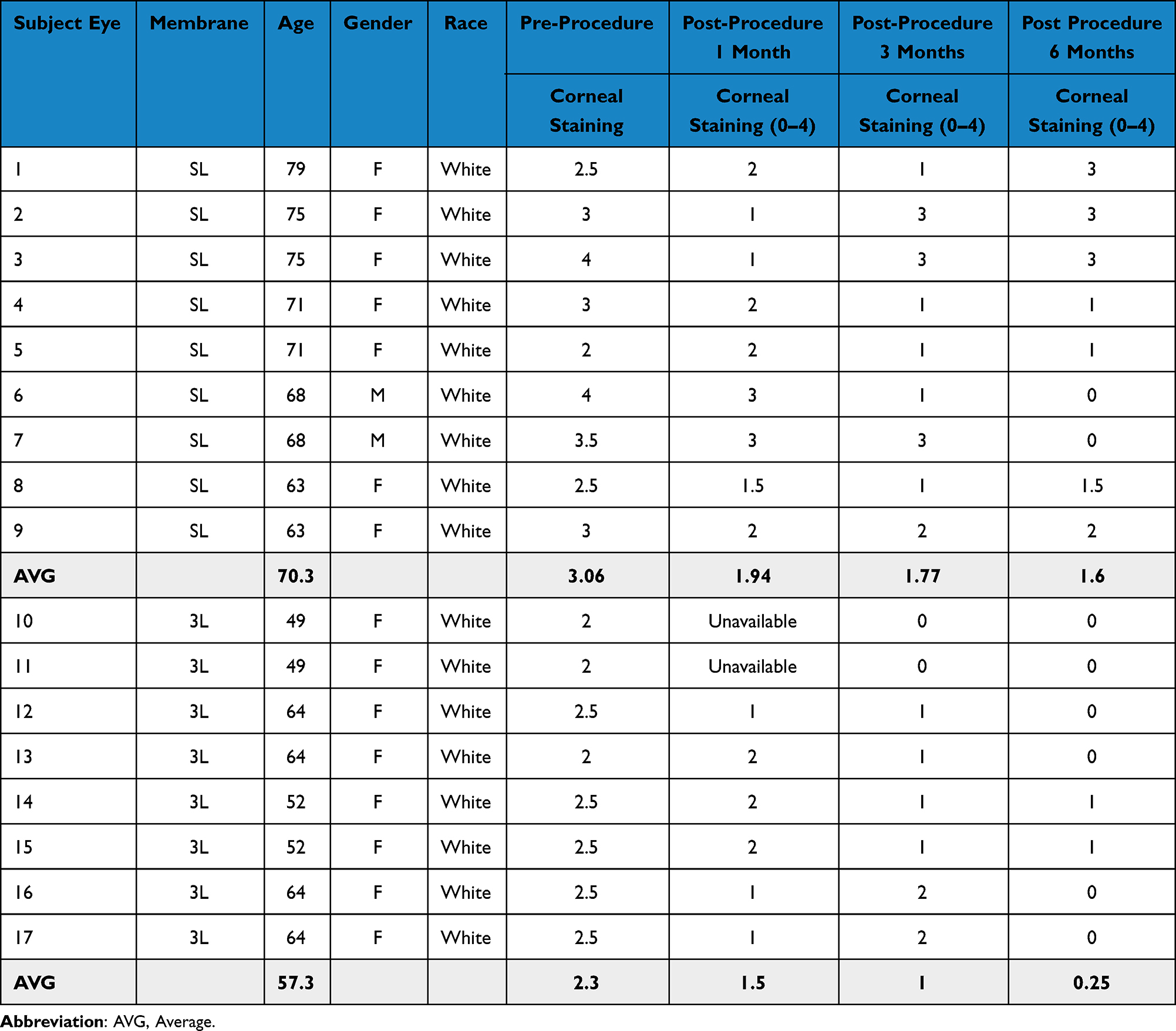 |
Table 1 Demographics and Corneal Staining |
Two of the nine patients studied were male and the average age of the patients receiving the single layer was 70.3 and the average age of those receiving the three-layer tissue was 57.3 years of age. Both the single-layer and three-layer DBM showed continued reduced staining at 1 month, 3 month, and 6 months. The single-layer DBM showed sustained improvement in corneal staining of 42–48% post single layer treatment at 3 and 6 months, respectively. The three-layer DBM showed sustained improvement in corneal staining of 57–89% post 3-layer treatment at 3 and 6 months, respectively (see Figure 1 below).
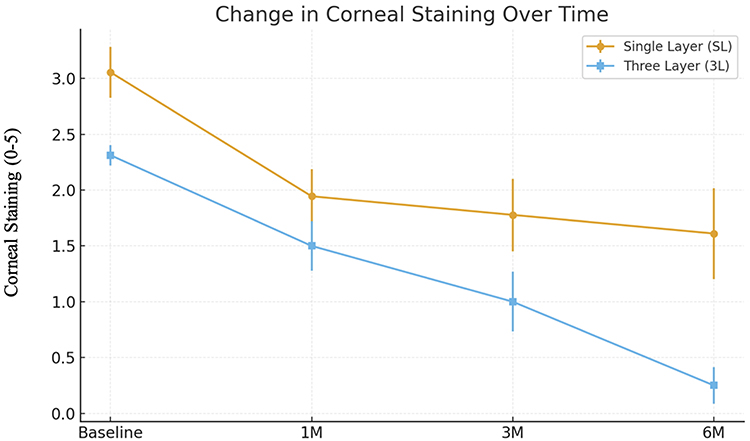 |
Figure 1 Change in Corneal Staining Over Time With Single-Layer (SL) and Three-Layer (3L) Decellularized Amniotic Membrane Grafts. Mean corneal fluorescein staining scores (0–5 scale) are shown at baseline, 1 month (1M), 3 months (3M), and 6 months (6M) following treatment. Error bars represent standard deviations. Both SL and 3L grafts demonstrated progressive reduction in corneal staining over time, indicating improvement in epithelial integrity. The 3L group showed a steeper and more sustained decline, with near-complete resolution by 6 months, whereas the SL group improved steadily but more gradually. |
Each single-layer DBM was fully incorporated within 24 hours and the three-layer DBM achieved complete incorporation by 72 hours. No adverse events including ocular infection, pain, or allergic response were observed in association with the patching protocol.
Both groups showed sustained and statistically significant improvements from baseline at 3 and 6 months (see Table 2). Additionally, when comparing the reduction of the single-layer vs the three-layer DBM, no statistical difference was found at 3 months (p = 0.347) but the three-layer showed a significantly improved reduction in corneal staining at 6 months (p = 0.0036).
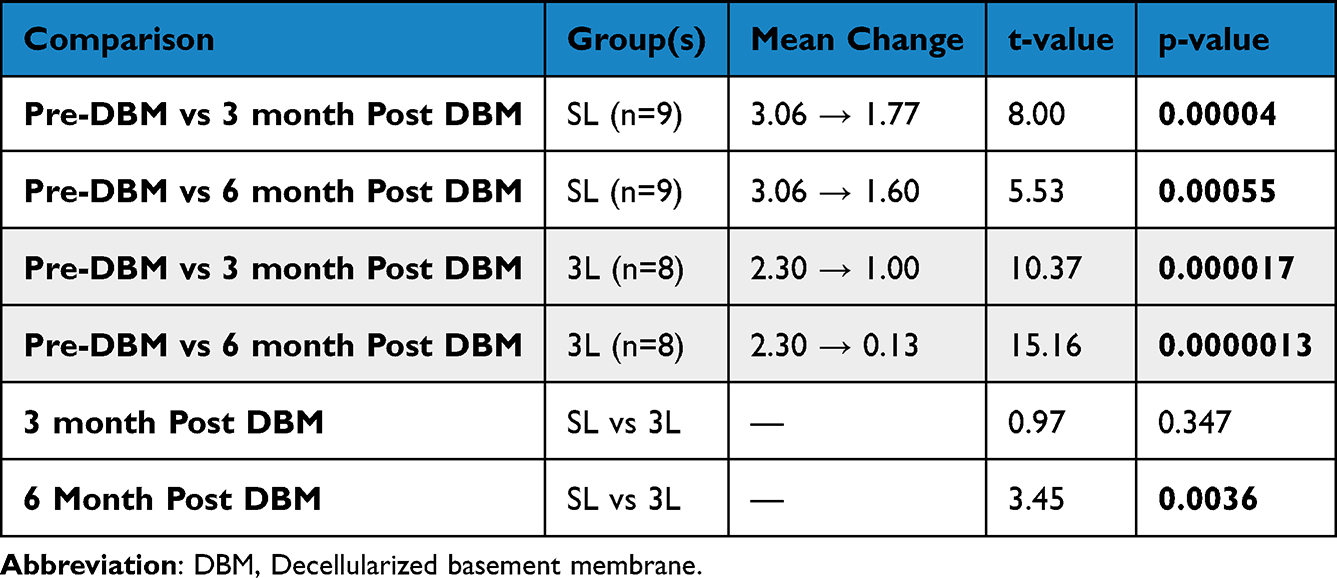 |
Table 2 Summary of Statistical Outcomes |
Although formal a priori power calculations were not feasible due to the retrospective design, a post-hoc assessment demonstrated that a minimum sample size of 7–8 eyes per group was sufficient to detect the large within-subject effect sizes observed in corneal staining reduction (Cohen’s d ≥ 1.2) with 80% power at α = 0.05. The final sample of 17 eyes exceeded this threshold, supporting adequate statistical power for detecting clinically meaningful differences between baseline and follow-up timepoints.
Discussion
Across refractory ocular-surface disease including moderate to severe DED, AMT provides rapid epithelial recovery, with benefits that commonly persist for months. In a multicenter outpatient PED cohort (n=220; 127 cryopreserved AMT; 93 conventional dehydrated AMT), a single application closed 45.5% of PEDs and 77.7% improved or resolved overall, with 55% needing additional AMT.18 In symptomatic DED without frank epithelial breakdown, cryopreserved AMT placed for ~2–7 days yields immediate ocular-surface and staining improvements at removal that remain significant at 1 week, 1 month, and 3 months.10,19 For conventional dehydrated AMT, a 1-month bilateral prospective study documented clinically meaningful symptom reductions lasting 6 months but corneal staining data not available20 while another study confirmed 3–4 months of reduced staining.21
For dehydrated decellularized basement membrane used with a 24–72 h eyelid pressure patch, a large retrospective series (n=144) reported 100% complete epithelial healing by ~1 week with the single-layer and three-layer, albeit with partial residual graft present at the 24 hour visit seen with the three-layer tissue, however long term follow up was not recorded.12
In this retrospective case series of moderate to severe DED, both Biovance SL and 3L DBM supported epithelial recovery and reduced corneal staining over time. Both treatment groups demonstrated statistically significant reductions in corneal fluorescein staining at 3 and 6 months. Notably, the three-layer DBM group exhibited a greater magnitude of improvement at both time points. At 6 months, the reduction in corneal staining in the three-layer group was statistically significantly greater than that observed in the single-layer group, supporting the enhanced long-term efficacy of the multi-layer DBM construct in the treatment of DED-related epithelial disease.
The clinical difference between the two DBM appear related to the number of basement layers in each DBM, with the three-layer DBM persisting longer and likely producing more anti-inflammatory cytokines and growth factors than the single-layer. Recent in vitro data demonstrate that Biovance 3L Ocular elicits a significantly reduced pro-inflammatory response while promoting a net anti-inflammatory effect relative to both cryopreserved and conventional dehydrated amniotic membranes. Specifically, Mao et al found that Biovance 3L stimulated lower levels of crucial pro-inflammatory cytokines TNF-α and IL-6 while maintaining higher levels of IL-10, an anti-inflammatory mediator associated with corneal healing.15 This favorable cytokine profile, in conjunction with its denser, multilayered matrix scaffold architecture, likely contributes to slower biodegradation and prolonged contact residence time on the ocular surface. As a result, the three-layer DBM offers an extended therapeutic duration, allowing a greater cell mediated response that includes a sustained release of growth factors and anti-inflammatory cytokines, which supports enhanced epithelial regeneration and immunomodulation in chronic ocular surface disease.
Linsey et al showed that both Biovance SL and Biovance 3L lead to 100% resolution of corneal staining at week 1 but did not follow these patients over time.12 Both Sell and Giannikas showed cryopreserved initial healing of 45% at 30 and 7–14 days, respectively.17,22 In this study, at 6 months the Biovance SL showed 22% with no staining and the Biovance 3L 75% complete lack of staining. This study underscores the chronicity of severe dry eye and suggests a potential additional benefit for the tripled layered DBM grafts and for multiple graft placements over time.
Linsey et al demonstrated that both Biovance SL and Biovance 3L achieved 100% epithelial recovery at 1 week, although longer-term outcomes were not assessed.12 In contrast, studies evaluating cryopreserved or conventional dehydrated AMT report substantially lower early healing rates: Sell et al observed 45.5% PED closure at 30 days with sutureless cryopreserved and dehydrated AMT,17 and Giannikas et al reported approximately 45% initial healing at 7–14 days using cryopreserved (ProKera) and conventional dehydrated (AmbioDisc) for ocular surface disease.22 Similar limitations in early and sustained response have been documented in larger multicenter studies, including the DREAM study, where sutureless cryopreserved AMT resulted in 45.5% complete healing after a single application, 77.7% improved or resolved overall, and 55% required more than one AMT placement.18 Additional cryopreserved AMT studies show early symptom relief at removal with clinically meaningful improvement through 1 week, 1 month, and 3 months, but without the high rates of rapid epithelial closure seen with decellularized basement membrane.10,19 Prospective evaluations of conventional dehydrated AMT for DED, such as the randomized controlled trial by Travé-Huarte et al, further demonstrate durable symptomatic improvement but limited epithelial healing, reinforcing that not all AMT platforms provide equivalent resurfacing outcomes.24
In the present study, at 6 months, complete resolution of corneal staining persisted in 22% of eyes treated with Biovance SL and 75% of eyes treated with Biovance 3L. These long-term outcomes underscore the chronicity and relapsing nature of moderate to severe DED, where early epithelial recovery does not always translate into stable long-term ocular surface restoration. Importantly, the substantially greater sustained healing observed with the three-layer DBM construct aligns with mechanistic evidence from Mao et al, who showed that Biovance 3L generates a more favorable cytokine profile, including reduced TNF-α and IL-6 and higher IL-10 expression compared with cryopreserved and conventional dehydrated AMT.15 This less pro-inflammatory cytokine milieu, together with the enhanced structural density of the multilayer matrix scaffold, likely contributes to slower biodegradation and a longer biologically active therapeutic window, enabling more prolonged epithelial support. Collectively, these findings suggest that multiple or staged DBM placements may be beneficial for patients with chronic epithelial instability, and that multilayer DBM may offer superior long-term efficacy in severe DED, Sjögren’s disease, or cases complicated by neurotrophic dysfunction.12
The variance in magnitude and duration of clinical impact on corneal staining suggests that the single-layer is best suited for less severe ocular surface disease whereas the three-layer graft would be a better option for more severe DED, such as Sjogren’s disease or when there is underlying NK.12 Also, the three-layer DBM requires clinical application with pressure patching for 3 days or in combination with a high water content dissolvable collagen shield, whereas the single-layer DBM can be applied under a pressure patch, dissolvable collagen shield, or high water content bandage contact lens.
This study has several limitations that include retrospective design, small sample size, and potential selection bias in SL vs 3L assignment. Visit timing variability and documentation limitations may affect precision of time‑to‑healing and staining estimates. Additionally, the patients receiving the single-layer were somewhat older on average and had worse staining at the baseline, which could represent more serious baseline disease.
Conclusions
Given that cryopreserved and conventional dehydrated amniotic membranes typically demonstrate only partial epithelial closure at early follow-up approximately 45% at 1–4 weeks,17,22 the magnitude and durability of healing observed with decellularized basement membrane in this study further underscore its potential superiority as a long-term ocular surface rehabilitation therapy, particularly for chronic dry eye with persistent epithelial compromise. DBMs that preserve the native amniotic basement membrane architecture offer both practical and biologic advantages, including reduced immunogenicity, retention of key structural and signaling components of the extracellular matrix, and facilitation of epithelial cell adhesion, migration, and differentiation.12 In this clinical series, both single-layer and three-layer DBMs demonstrated clinically meaningful and statistically significant improvements in corneal epithelial integrity over time, as evidenced by sustained reductions in corneal fluorescein staining over a thee and six-month period. Notably, the three-layer DBM consistently outperformed the single-layer variant, producing greater and more durable improvements at both the three and six month timepoints. These findings reinforce the therapeutic value of multilayered DBM constructs in promoting long-term ocular surface rehabilitation, particularly in patients with treatment-refractory epithelial disease.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki. An IRB approval waiver was obtained prior to data collection. Since this is a retrospective study, the risk to patients is non-existent, and informed consent was waived as appropriate under IRB guidelines. All patient information was de-identified to protect privacy and confidentiality.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Leong Y-Y, Tong L. Barrier function in the ocular surface: from conventional paradigms to new opportunities. Ocular Surf. 2015;13:103–8. doi:10.1016/j.jtos.2014.10.003
2. Mead OG, Tighe S, Tseng SCG. Amniotic membrane transplantation for managing dry eye and neurotrophic keratitis. Taiwan J Ophthalmol. 2020;10:13–21. doi:10.4103/tjo.tjo_5_20
3. Maqsood S, Elsawah K, Dhillon N, et al. Management of persistent corneal epithelial defects with human amniotic membrane-derived dry matrix. Clin Ophthalmol. 2021;28:2231–2238. doi:10.2147/OPTH.S299141
4. Katzman LR, Jeng BH. Management strategies for persistent epithelial defects of the cornea. Saudi. J Ophthalmol. 2014;28:168–172.
5. Ljubimov AV, Saghizadeh M. Progress in corneal wound healing. Prog Retin Eye Res. 2015;49:17–45. doi:10.1016/j.preteyeres.2015.07.002
6. Rodríguez Calvo-de-Mora M, Domínguez-Ruiz C, Barrero-Sojo F, et al. Autologous versus allogeneic versus umbilical cord sera for the treatment of severe dry eye disease: a double-blind randomized clinical trial. Acta Ophthalmol. 2022;100:e396–e408. doi:10.1111/aos.14953
7. Sánchez-González JM, Alonso-Aliste F, Borroni D, et al. Plasma rich in growth factors (PRGF) in transepithelial photorefractive keratectomy (TPRK). J Clin Med. 2021;10:1939. doi:10.3390/jcm10091939
8. Sheha H, Liang L, Li J, Tseng SC. Sutureless amniotic membrane transplantation for severe bacterial keratitis. Cornea. 2009;28:1118–1123. doi:10.1097/ICO.0b013e3181a2abad
9. Sheha H, Tighe S, Cheng AM, Tseng SC. A stepping stone in treating dendritic keratitis. Am J Ophthalmol Case Rep. 2017;7:55–58. doi:10.1016/j.ajoc.2017.06.002
10. Walkden A. Amniotic membrane transplantation in ophthalmology: an updated perspective. Clin Ophthalmol. 2020;14:2057–2072. doi:10.2147/OPTH.S208008
11. Pogozhykh O, Hofmann N, Gryshkov O, et al. Repeated freezing procedures preserve structural and functional properties of amniotic membrane for application in ophthalmology. Int JMol Sci. 2020;21:4029. doi:10.3390/ijms21114029
12. Linsey K. Use of an eyelid pressure patch concomitantly with a decellularized dehydrated amniotic membrane for ocular surface disease management. Ophthalmol Ther. 2025;14(3):573–584. doi:10.1007/s40123-025-01094-2
13. Turkoglu E, Celik E, Alagoz G. A comparison of the efficacy of autologous serum eye drops with amniotic membrane transplantation in neurotrophic keratitis. Semin Ophthalmol. 2014;29:119–126. doi:10.3109/08820538.2013.768678
14. Sacchetti M, Lambiase A. Diagnosis and management of neurotrophic keratitis. Clin Ophthalmol. 2014;8:571–579. doi:10.2147/OPTH.S45921
15. Mao Y, Protzman NM, John N, et al. An in vitro comparison of human corneal epithelial cell activity and inflammatory response on differently designed ocular amniotic membranes and a clinical case study. J Biomed Mater Res B Appl Biomater. 2023;111:684–700. doi:10.1002/jbm.b.35186
16. Sangwan VS, Burman S, Tejwani S, Mahesh SP, Murthy R. Amniotic membrane transplantation: a review of current indications in the management of ophthalmic disorders. Indian J Ophthalmol. 2007;55:251–260. doi:10.4103/0301-4738.33036
17. Sell S, de la Presa M, Thakur S, et al. Comparison of persistent epithelial defect treatment with sutureless cryopreserved and dehydrated amniotic membrane. Am J Ophthalmol. 2023;251:32–42. doi:10.1016/j.ajo.2022.12.007
18. McDonald MB, Sheha H, Tighe S, et al. Treatment outcomes in the DRy eye amniotic membrane (DREAM) study. Clin Ophthalmol. 2018;12:677–681. doi:10.2147/OPTH.S162203
19. McDonald M, Janik S, Bowden FW, et al. Association of treatment duration and clinical outcomes in dry eye treatment with sutureless cryopreserved amniotic membrane. Clin Ophthalmol. 2023;17:3321–3331. doi:10.2147/OPTH.S423040
20. Travé-Huarte S, Wolffsohn JS. Sutureless dehydrated amniotic membrane (Omnigen) application using a specialised bandage contact lens (OmniLenz) for the treatment of dry eye disease: a 6-month randomised control trial. Medicina. 2024;60(6):985. doi:10.3390/medicina60060985
21. Karaca EE, Asfuroğlu Y, Özek D, Çelik G, Evren Kemer Ö. Application of a practical amniotic membrane ring made on-site for restoration of ocular surface health in dry eye disease. J Fr Ophtalmol. 2024;47(8):104233. doi:10.1016/j.jfo.2024.104233
22. Giannikas C, Udell IJ, Steiner A, Shih C. Sutureless amniotic membrane transplantation for ocular surface disorders: a comparison of prokera to ambioDisc Invest Ophthalmol Vis Sci. 2014;55:4707.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sutureless Amniotic Membrane Grafting in the Management of Corneal Perforations Associated with Severe Ocular Surface Disease
Mancini M, Palino P, Valastro A, Scolaro A, Oliverio GW, Mancini A, Aragona P, Meduri A
Clinical Ophthalmology 2026, 20:571757
Published Date: 26 February 2026