Back to Journals » Patient Preference and Adherence » Volume 20
Supporting Medication Adherence and Patient-Centered Care for Attention-Deficit Hyperactivity Disorder in Taiwan: A Pharmacist-Oriented Perspective Informed by Targeted Evidence
Received 17 December 2025
Accepted for publication 7 February 2026
Published 24 February 2026 Volume 2026:20 589432
DOI https://doi.org/10.2147/PPA.S589432
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ramón Morillo-Verdugo
Yu-Jui Chiu,1 Yen-Ming Huang1– 3
1School of Pharmacy, College of Medicine, National Taiwan University, Taipei City, 100025, Taiwan; 2Graduate Institute of Clinical Pharmacy, College of Medicine, National Taiwan University, Taipei City, 100025, Taiwan; 3Department of Pharmacy, National Taiwan University Hospital, Taipei City, 100229, Taiwan
Correspondence: Yen-Ming Huang, Graduate Institute of Clinical Pharmacy, College of Medicine, National Taiwan University, Taipei City, 100025, Taiwan, Tel +886-2-3366-8784, Email [email protected]
Abstract: Despite the broad coverage offered by Taiwan’s National Health Insurance system, attention-deficit/hyperactivity disorder (ADHD) care continues to face a critical “leaky pipeline” problem. There is a clear gap between diagnostic prevalence and long-term treatment retention. This perspective article applies the SPIDER (Sample, Phenomenon of Interest, Design, Evaluation, Research type) framework to synthesize evidence on the multidimensional factors that contribute to medication non-adherence among Taiwanese children and adolescents. The barriers are grouped into five domains. These domains include medication-related issues such as dosing complexity, child-level developmental challenges related to growing autonomy, family dynamics that reveal a distinctive “socioeconomic status paradox”, stigma within school environments, and vulnerabilities at the healthcare system level. Together, these factors demonstrate that existing hospital-centered care models alone may not sufficient to support sustained treatment engagement. To address this gap, we propose a pharmacist-driven precision approach to improving adherence in ADHD. This approach redefines the pharmacist’s role and emphasizes proactive involvement in ADHD management rather than passive medication dispensing. The proposed approach includes regimen optimization, digital tools that support adolescent self-management, and shared decision-making strategies that respond to family-specific concerns. Because community pharmacists are highly accessible, they can serve as continuity anchors across care settings and developmental stages and help strengthen treatment persistence and therapeutic outcomes.
Keywords: attention-deficit hyperactivity disorder, intervention, medication adherence, pharmacist, shared decision-making
Introduction
Attention-deficit hyperactivity disorder (ADHD) is a common neurodevelopmental condition affecting children and adolescents worldwide, with prevalence estimates ranging from 3.4% to 14.0%.1–4 Pharmacotherapy is widely recognized as a cornerstone in ADHD management. Major clinical guidelines, including those from the American Academy of Pediatrics and the National Institute for Health and Care Excellence, recommend medication as a first-line treatment for school-aged children to prevent long-term complications.5,6 Despite its demonstrated benefits, achieving consistent medication use remains a global challenge. Studies indicate that non-adherence to ADHD medications can range from 4.8% to 77% internationally.7,8
In Taiwan, gaps in ADHD care occur across the entire treatment continuum, from diagnosis to medication initiation and long-term continuation. Although the National Health Insurance provides broad access to care, community-based studies estimate the prevalence of ADHD at approximately 7.5%.9 In contrast, real-world clinical data indicate a much lower diagnosis rate of 1.62% to 2.44%, pointing to substantial under-diagnosis.10 Even among diagnosed youths, the use of ADHD medication is far from optimal. Wang et al found that 40–50% of children with a confirmed diagnosis never receive pharmacotherapy,10 a pattern echoed by Huang et al, who reported a 39.2% non-initiation rate.11 For those who do begin therapy, sustaining therapy is an even greater challenge. Discontinuation is frequent and occurs early. Chen et al reported that 93.2% of patients stopped medication within 1 year.12 Although long-acting methylphenidate has become widely used, recent data indicate that only 19.9% of patients continue therapy for 12 months or longer.11
This “leaky pipeline” of ADHD treatment has serious clinical implications. Nationwide cohort studies in Taiwan show that individuals with ADHD are at increased risks of mortality13 and traumatic brain injury,14 both of which are markedly reduced by consistent medication adherence. Beyond these severe but relatively rare outcomes, poor adherence is associated with impaired academic performance, reduced home functioning, diminished quality of life, and increased caregiver burden and family stress.15 In addition, it is linked to higher risks of adverse social outcomes, including criminality.16,17 These more common consequences highlight the importance of promoting treatment initiation and persistence in pediatric ADHD.
Pharmacists are well positioned to improve ADHD medication adherence due to their accessibility, medication expertise, and frequent contact with patients and caregivers.18 Theoretical frameworks, such as the Theory of Planned Behavior (TPB) and the Unified Theory of Behavior Change (UTBC), offer guidance for intervention design to improve medication adherence.19 The TPB emphasizes the influence of attitudes, subjective norms, and perceived behavioral control on medication-taking intentions,20 while the UTBC suggests the roles of knowledge and skills in enhancing willingness and persistence.21 Pharmacists can leverage these frameworks by educating patients and caregivers, addressing beliefs about medication, and providing practical strategies, such as reminders or pill organization, thereby supporting both initiation and sustained therapy.22 Given their underutilization in ADHD care in Taiwan, pharmacists could play a pivotal role in improving medication adherence.
Methods
This article presents a perspective informed by a targeted synthesis of Taiwan-based empirical evidence rather than a formal systematic review. The SPIDER (Sample, Phenomenon of Interest, Design, Evaluation, Research type) framework was used as a conceptual guide to structure the research question and eligibility criteria (Appendix 1).23 The objective was to identify context-specific determinants of ADHD medication adherence relevant to service design.
A PubMed was conducted using Boolean operators (“OR” and “AND”) to combine relevant keywords. Sample terms included “attention deficit disorder with hyperactivity”, “ADHD”, “child”, “adolescent”, “youth”, “parent”, “caregiver”, “family”, “Taiwan”, and “Taiwanese”. Phenomenon-of-Interest terms encompassed “medication adherence”, “compliance”, “persistence”, “drug taking”, “treatment initiation”, “treatment delay”, “discontinuation”, and “continuation”. Design-related terms comprised “observational”, “cohort”, “database study”, “cross-sectional”, “survey”, and “questionnaire”, while evaluation-related terms contained “factor”, “determinant”, “predictor”, “barrier”, “attitude”, “belief”, “stigma”, and “family support” (Appendix 2).
Eligible studies were those that (1) involved children or adolescents diagnosed with ADHD in Taiwan, (2) investigated outcomes related to medication adherence, treatment initiation, or discontinuation, and (3) used quantitative (eg, nationwide database and hospital-based surveys), qualitative, or mixed-methods designs. Review articles, studies not focused on Taiwan, or studies unrelated to medication adherence were excluded. The purpose of this synthesis was to identify recurring determinant domains to inform a conceptual service framework, rather than to generate an exhaustive or fully reproducible evidence map.
Results
The initial search yielded 48 records. Following title and abstract screening, 40 records were excluded due to irrelevant topics (n = 38), review article (n = 1), or lack a Taiwan-specific focus (n = 1). Eight full-text articles were subsequently retrieved and assessed for eligibility. Three were excluded for not addressing medication (n = 2) or adherence-related factors. Ultimately, five studies were included in the final synthesis (Appendix 3).11,12,24–26 Most studies relied on the National Health Insurance Research Database or hospital-based samples. Determinants of adherence identified in nationwide longitudinal studies were grouped into five domains: medication-related, child-related, family-related, school and environmental, and system-level factors (Table 1).
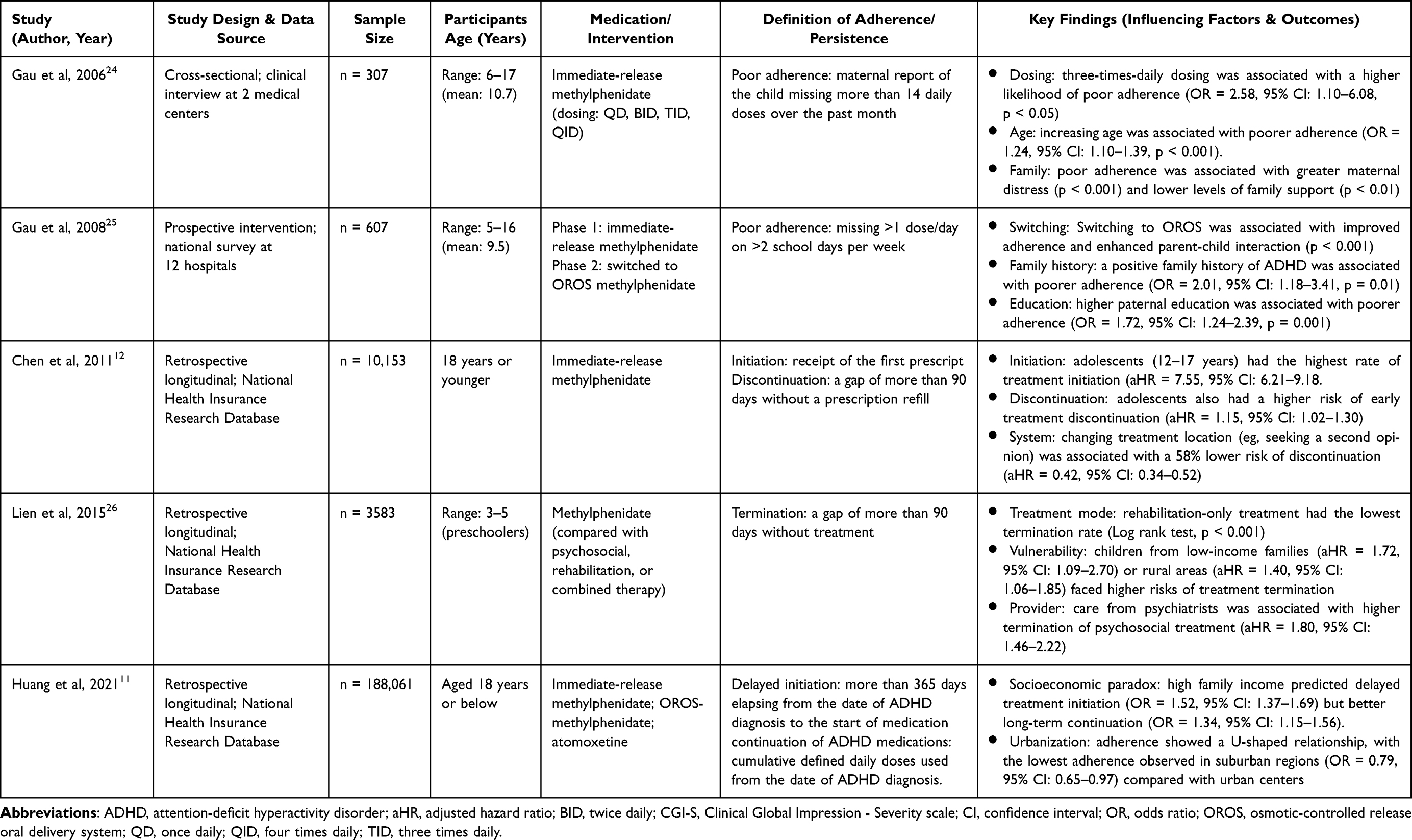 |
Table 1 Summary of Key Evidence on Factors Influencing Attention-Deficit Hyperactivity Disorder Medication Adherence and Related Interventions in Taiwan |
Medication-related factors emerged as particularly influential. Complex dosing regimens, particularly three-times-daily schedules, were strongly associated with poor adherence (OR = 2.58, 95% CI: 1.10–6.08, p < 0.05) compared with once-daily dosing.24 Although long-acting formulations improve convenience, side effects such as appetite loss remain common, affecting approximately 21% of users.25 Additional barriers include unpleasant taste of certain medications and aversion to immediate-release formulations.24,25
Child-related factors also contribute substantially. Developmental stages play a central role, with adolescence (ages 12–17) associated with higher discontinuation risks (aHR = 1.15, 95% CI: 1.02–1.30), despite relatively higher initiation rates.12 Issues of autonomy, such as refusal to take medication (12.7%) and forgetfulness (72.9%), were common challenges.24 Behavioral and clinical characteristics can further influence adherence. Children with oppositional symptoms25 or behavior problems at home24 are more prone to discontinuation. In contrast, some comorbidities may facilitate adherence. For example, children with intellectual disability demonstrated better adherence (OR = 0.32, 95% CI: 0.16–0.60, p < 0.001), likely reflecting increased parental supervision.25 Among adolescents, autism spectrum disorder was associated with longer treatment continuation, whereas anxiety disorders predicted earlier discontinuation.11 This divergence likely occurs because stimulants can exacerbate somatic anxiety symptoms (eg, palpitations), leading to discontinuation, while the behavioral complexity of autism often necessitates sustained pharmacotherapy for symptom stability.
Family-related determinants present a complex and sometimes counterintuitive pattern. Huang et al reported a “socioeconomic status paradox” where higher household income (OR = 1.52, 95% CI: 1.37–1.69) was associated with treatment initiation delays exceeding 1 year.11 This phenomenon likely reflects a “hesitancy gap”, in which resource-rich families prefer to explore non-pharmacological options first or engage in prolonged deliberation about medication safety. Parenting-related factors, including maternal psychological distress, indifferent or overprotective parenting styles, family history of ADHD, and higher paternal education, have also been linked to poor adherence outcomes.24,25 In particular, maternal distress may impair caregivers’ capacity to maintain consistent supervision and routine enforcement of medication use.24 Similarly, the association with higher paternal education may result from greater skepticism about medication necessity or a stronger preference for behavioral interventions among highly educated parents.24,25 Parental beliefs additionally shape treatment decision-making. Common cited reasons for medication discontinuation include fear of side effects, a perceived lack of need for medication, the belief that the child’s symptoms have improved, and judgments that the medication has “no effect”.24,26
School and environmental factors further complicate medication adherence. Stigma associated with taking medication at school, embarrassment, and a lack of supervision for midday doses as frequently reported barriers.24,25 Even teacher objection has been cited as an impediment to consistent treatment, possibly due to a lack of understanding regarding ADHD pharmacotherapy or a cultural preference for behavioral interventions in educational settings.24 Geographic variation is also evident. Chen et al found that children in southern Taiwan initiated treatment earlier,12 while Huang et al reported a U-shaped pattern between urbanization level and treatment continuation, indicating that adherence is consistently higher in both highly urbanized centers (due to resource accessibility) and rural areas (potentially due to stronger community-provider ties), while falling lowest in suburban regions (OR = 0.79, 95% CI: 0.65–0.97 compared to highly urbanized areas).11
Finally, system-level and healthcare-related factors exert substantial influence on treatment retention. Children from structural vulnerable backgrounds, such as those experiencing poverty (aHR = 1.72, 95% CI: 1.09–2.70) or living in rural areas (aHR = 1.40, 95% CI: 1.06–1.85), face higher risks of treatment termination.26 Discontinuation rates are higher in regional (aHR = 1.27, 95% CI: 1.15–1.40) and district hospitals (aHR = 1.32, 95% CI: 1.17–1.49),12 likely reflecting the disparity in specialized mental health resources and titration support compared to medical centers. Notably, switching treatment locations (seeking a second opinion) was associated with a 58% reduction in discontinuation risk (aHR = 0.42, 95% CI: 0.34–0.52).12 This finding does not necessarily indicate fragmented care. Instead, it may reflect proactive care-seeking by families trying to find a provider who better fits their needs. This suggests the importance of provider–family alignment and renewed engagement in treatment. Treatment modality further affects retention, with rehabilitation-only care associated with lower termination rates. This pattern may reflect parental preferences for non-pharmacological interventions perceived as safer or more “natural”, as well as concerns about medication side effects and diagnostic labeling, which can contribute to delayed treatment initiation.26
Discussion
Despite these well-documented challenges, the role of pharmacists in ADHD management in Taiwan remains largely undefined and primarily limited to dispensing. Although continuity of care is essential, there is a notable absence of research describing proactive pharmacist involvement in addressing these multifaceted adherence barriers. This underscores the need for pharmacists to move beyond product-focused roles and toward managing these interacting determinants through a precision and patient-centered intervention model (Figure 1).
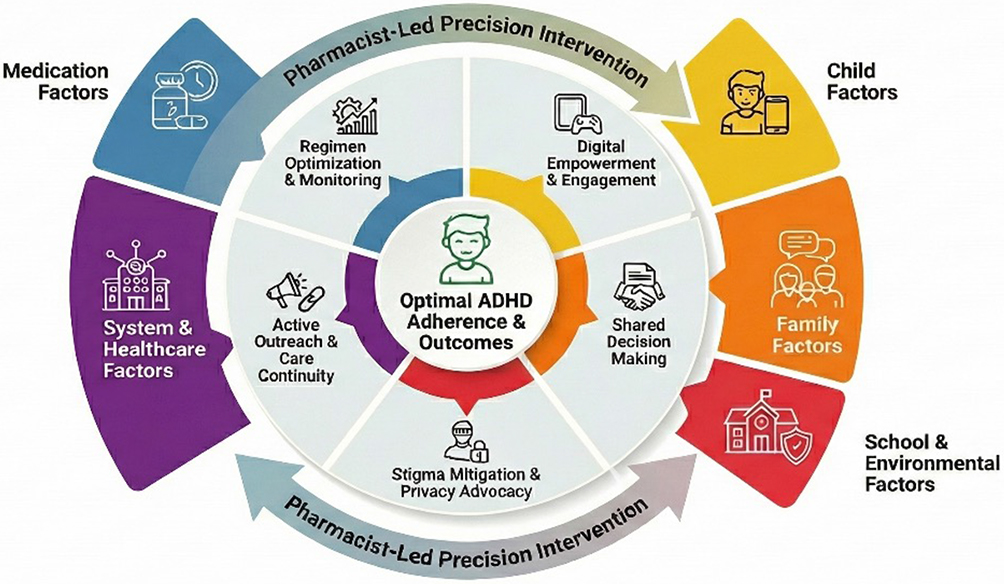 |
Figure 1 A Pharmacist-driven precision approach to enhancing adherence in attention-deficit/hyperactivity disorder. This conceptual framework illustrates how pharmacists can address multidimensional barriers across five key domains, including medication, child, family, school and environmental, and system and healthcare factors. By implementing targeted strategies such as regimen optimization, digital empowerment, shared decision-making, and active outreach, pharmacists can bridge the care gap and improve treatment outcomes. |
Optimizing Medication Regimens: Simplify and Monitor
As discussed earlier, structural characteristics of ADHD medication regimen, particularly multiple daily dosing and formulation intolerance, are key drivers of non-adherence. Even with the introduction of long-acting formulations, adverse effects such as appetite loss continue to contribute to early discontinuation. This finding aligns with global meta-analyses indicating that adverse effects are a universal barrier to stimulant adherence.27 Pharmacists can address these barriers by proactively identifying patients on complex regimens (eg, more than once daily) and recommending a switch to once-daily formulations (eg, osmotic-controlled release oral delivery system), thereby reducing both logistical and taste-related adherence challenges.28 In addition, active monitoring of side effect is also crucial, and pharmacists can incorporate standardized symptom checklists (eg, side effect domain of the Swanson, Nolan, and Pelham, Version IV scale) into routine refill encounters to track appetite changes or sleep disturbances and offer practical strategies, such as advising dose administration after a high-calorie meal, suggesting evening snacks, or counseling on sleep hygiene and, if appropriate, discussing adjunctive melatonin.29
Empowering Children: Fostering Autonomy and Engagement
Adherence is strongly influenced by developmental stage. Adolescent represents a critical period during which the desire for autonomy often conflicts with sustained medication use, despite high initiation rates.12 Common barriers include child refusal, forgetfulness,24 and the impact of comorbidities, such as intellectual disability or anxiety.11,25 Pharmacists can shift from an adherence-focused model to an empowerment-based approach by leveraging digital tools, such as reminder apps, gamified adherence trackers, and privacy-preserving platforms. These tools allow adolescents to actively manage their own medication schedules and in turn improve engagement and adherence.19,30,31 Autonomy-supportive counseling further transforms medication-taking from a parental mandate to a personal responsibility, respecting their developmental need for adolescents while supporting therapeutic goals.32
Supporting Families: Reducing Hesitancy and Daily Burden
Family dynamics introduce a complex set of challenges in ADHD medication use, with both high-resource and structurally vulnerable families facing distinct barriers. The “socioeconomic status paradox”, where higher-income families delay treatment initiation, points to a hesitancy gap often rooted in decisional conflict and exposure to conflicting information about medication labeling or safety.33 As described by Ahmed et al, many parents enter a prolonged period of deliberation, carefully weighing perceived risks against potential academic benefits.34 Conversely, families dealing with maternal distress, indifferent parenting styles, or a family history of ADHD often struggle with the daily routines required for supporting consistent dosing.24,25 Another common contributor to missed doses or discontinuation is the perception that the medication has “no effect”, which typically reflects misunderstandings about the gradual titration process rather than true pharmacologic failure, a pattern also observed internationally.35
Pharmacists can help resolve these barriers by adopting a targeted and supportive approach. Incorporating shared decision-making helps reduce hesitancy among high-resource families. Evidence shows that simple decision aids (eg, issue cards) improve parental understanding and lower decisional conflict,36 while also ensuring that treatment choices align with family values and preferences.37 For families experiencing substantial stress or when a parent may have ADHD-related symptoms, pharmacists can serve as organizational supports by offering practical tools, such as pill organizers or reminder systems and by delivering instructions that are concise, structured, and visually oriented. Finally, clear expectation-setting is essential. Explaining the titration timeline and emphasizing that clinical benefits may not immediately appear can correct misconceptions and prevent early discontinuation.
Navigating School and Environmental Barriers: Protect Privacy and Reduce Stigma
School and environmental contexts frequently create practical and social barriers to adherence. Embarrassment related to public dosing and missed doses at school are common.24,25 Geographic disparities, urbanization-related differences in treatment continuation, further complicate adherence.11 Pharmacists can address these barriers by advocating by recommending privacy-preserving regimens, such as once-daily doses taken at home and ensuring that treatment remains confidential, reducing dependence on school staff or teachers while mitigating stigma.25,38
Bridging System-Level Gaps: Community-Based Continuity
Structural vulnerabilities, including poverty and rural residence, are associated with higher risks of treatment termination.26 The hospital-centric care model shows limitations, with higher discontinuation rates observed in regional hospitals, whereas seeking a second opinion reduces this risk.12 To overcome these systemic barriers, adherence management could shift toward the community. Pharmacists can promote multimodal care by encouraging combined rehabilitation and medication approaches, operating pharmacist-led clinics to enhance monitoring,39 and leveraging the accessibility of community pharmacies for outreach and tele-pharmacy services.40 By acting as a stable, consistent point of care, pharmacists ensure continuity of care, especially for families navigating provider transitions, which evidence shows improved adherence and patient outcomes.41
Implementation Considerations: Feasibility and System Incentives
Although the proposed pharmacist roles are conceptually aligned with identified adherence determinants, their implementation depends on supportive system-level conditions. In Taiwan, community pharmacies are highly accessible and increasingly engaged in chronic disease management; however, ADHD-focused services are not yet part of routine practice.42 Expanding pharmacists’ roles would require targeted training in pediatric mental health communication, workflow adjustments to accommodate time demands, and reimbursement or policy mechanisms that recognize cognitive and counseling services beyond dispensing. Without appropriate structural incentives and clear role delineation clarification, uptake may remain limited despite theoretical feasibility. Therefore, the framework presented here should be viewed as a service development hypothesis that requires alignment with professional scope, funding models, and interprofessional collaboration.
Limitations
This work has several limitations. First, no primary data were collected from pharmacists, patients, or families, and the proposed framework has not yet been implemented or empirically tested. Further evaluation should be conducted. Second, the evidence synthesis was targeted and context-specific rather than comprehensive; additional determinants reported outside biomedical databases may not have been captured. Third, most included studies were observational, and the reported associations should not be interpreted as causal. Finally, the proposed pharmacist-oriented model is grounded in the Taiwanese healthcare context and may not be directly transferable to systems with different pharmacy roles or care delivery structures.
Conclusion
In Taiwan, ADHD medication is readily accessible through National Health Insurance system, yet long-term adherence remains suboptimal due to complex regimens, adolescent autonomy, family dynamics, and school stigma. Pharmacists are well placed to address these gaps by optimizing regimens, addressing safety concerns, and empowering families and adolescents through shared decision-making. These functions extend naturally from pharmacists’ existing responsibilities and may contribute to improved clinical outcomes as well as stronger provider–family relationships. By ensuring continuity of care within the community, pharmacists may reposition pharmacies as accessible, patient-centered care settings that support sustained success in ADHD treatment.
Data Sharing Statement
The study materials and detailed analyses are available from the corresponding author upon reasonable request.
Funding
This study was supported by the National Science and Technology Council (NSTC), Taiwan (NSTC 113-2628-B-002-018-MY3). The funding organization was not involved in the study design, data collection, statistical analysis, result interpretation, or manuscript preparation.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ayano G, Demelash S, Gizachew Y, Tsegay L, Alati R. The global prevalence of attention deficit hyperactivity disorder in children and adolescents: an umbrella review of meta-analyses. J Affect Disord. 2023;339:860–9. doi:10.1016/j.jad.2023.07.071
2. Salari N, Ghasemi H, Abdoli N, et al. The global prevalence of ADHD in children and adolescents: a systematic review and meta-analysis. Ital J Pediatr. 2023;49(1):48. doi:10.1186/s13052-023-01456-1
3. Polanczyk G, de Lima MS, Horta BL, Biederman J, Rohde LA. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry. 2007;164(6):942–948. doi:10.1176/ajp.2007.164.6.942
4. Thomas R, Sanders S, Doust J, Beller E, Glasziou P. Prevalence of attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. Pediatrics. 2015;135(4):e994–e1001. doi:10.1542/peds.2014-3482
5. Wolraich ML, Hagan Jr JF, Allan C, et al. Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics. 2019;144(4):e20192528. doi:10.1542/peds.2019-2528
6. National Institute for Health and Care Excellence (Great Britain). Attention Deficit Hyperactivity Disorder: Diagnosis and Management. National Institute for Health and Care Excellence; 2018.
7. Valaei Sharif N, Ghasemzadeh P, Ghasemzadeh S. A scoping review on strategies that enhance medication adherence in children and adolescents with attention deficit hyperactivity disorder and associated outcomes. Curr Dev Disord Rep. 2024;11(3):113–124. doi:10.1007/s40474-024-00299-7
8. Gajria K, Lu M, Sikirica V, et al. Adherence, persistence, and medication discontinuation in patients with attention-deficit/hyperactivity disorder - a systematic literature review. Neuropsychiatr Dis Treat. 2014;10:1543–1569. doi:10.2147/NDT.S65721
9. Gau SSF, Chong MY, Chen THH, Cheng ATA. A 3-year panel study of mental disorders among adolescents in Taiwan. Am J Psychiatry. 2005;162(7):1344–1350. doi:10.1176/appi.ajp.162.7.1344
10. Wang LJ, Lee SY, Yuan SS, et al. Prevalence rates of youths diagnosed with and medicated for ADHD in a nationwide survey in Taiwan from 2000 to 2011. Epidemiol Psychiatr Sci. 2017;26(6):624–634. doi:10.1017/S2045796016000500
11. Huang KL, Hsu JW, Tsai SJ, et al. Factors Affecting delayed initiation and continuation of medication use for attention-deficit/hyperactivity disorder: a nationwide study. J Child Adolesc Psychopharmacol. 2021;31(3):197–204. doi:10.1089/cap.2020.0136
12. Chen CY, Yeh HH, Chen KH, Chang IS, Wu ECH, Lin KM. Differential effects of predictors on methylphenidate initiation and discontinuation among young people with newly diagnosed attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. 2011;21(3):265–273. doi:10.1089/cap.2010.0107
13. Chen VCH, Chan HL, Wu SI, et al. Attention-deficit/hyperactivity disorder and mortality risk in Taiwan. JAMA Network Open. 2019;2(8):e198714. doi:10.1001/jamanetworkopen.2019.8714
14. Liou YJ, Wei HT, Chen MH, et al. Risk of traumatic brain injury among children, adolescents, and young adults with attention-deficit hyperactivity disorder in Taiwan. J Adolesc Health. 2018;63(2):233–238. doi:10.1016/j.jadohealth.2018.02.012
15. Fridman M, Banaschewski T, Sikirica V, Quintero J, Erder MH, Chen KS. Factors associated with caregiver burden among pharmacotherapy-treated children/adolescents with ADHD in the caregiver perspective on pediatric ADHD survey in Europe. Neuropsychiatr Dis Treat. 2017;13:373–386. doi:10.2147/NDT.S121391
16. Young S, González RA, Fridman M, Hodgkins P, Kim K, Gudjonsson GH. Health-related quality of life in prisoners with attention-deficit hyperactivity disorder and head injury. BMC Psychiatry. 2018;18(1):209. doi:10.1186/s12888-018-1785-9
17. Young S, González RA, Fridman M, Hodgkins P, Kim K, Gudjonsson GH. The economic consequences of attention-deficit hyperactivity disorder in the Scottish prison system. BMC Psychiatry. 2018;18(1):210. doi:10.1186/s12888-018-1792-x
18. Syrnyk M, Glass B. Pharmacist interventions in medication adherence in patients with mental health disorders: a scoping review. Int J Pharm Pract. 2023;31(5):449–458. doi:10.1093/ijpp/riad037
19. Parkin R, Mc Nicholas F, Hayden JC. A systematic review of interventions to enhance adherence and persistence with ADHD pharmacotherapy. J Psychiatr Res. 2022;152:201–218. doi:10.1016/j.jpsychires.2022.05.044
20. Bai GN, Wang YF, Yang L, Niu WY. Effectiveness of a focused, brief psychoeducation program for parents of ADHD children: improvement of medication adherence and symptoms. Neuropsychiatr Dis Treat. 2015;11:2721–2735. doi:10.2147/NDT.S88625
21. Chacko A, Newcorn JH, Feirsen N, Uderman JZ. Improving medication adherence in chronic pediatric health conditions: a focus on ADHD in youth. Curr Pharm Des. 2010;16(22):2416–2423. doi:10.2174/138161210791959908
22. Pringle J, Coley KC. Improving medication adherence: a framework for community pharmacy-based interventions. Integr Pharm Res Pract. 2015;4:175–183. doi:10.2147/IPRP.S93036
23. Cooke A, Smith D, Booth A. Beyond PICO: the SPIDER tool for qualitative evidence synthesis. Qual Health Res. 2012;22(10):1435–1443. doi:10.1177/1049732312452938
24. Gau SSF, Shen HY, Chou MC, Tang CS, Chiu YN, Gau CS. Determinants of adherence to methylphenidate and the impact of poor adherence on maternal and family measures. J Child Adolesc Psychopharmacol. 2006;16(3):286–297. doi:10.1089/cap.2006.16.286
25. Gau SSF, Chen SJ, Chou WJ, et al. National survey of adherence, efficacy, and side effects of methylphenidate in children with attention-deficit/hyperactivity disorder in Taiwan. J Clin Psychiatry. 2008;69(1):131–140. doi:10.4088/jcp.v69n0118
26. Lien YT, Yeh HH, Soong WT, Jeng SF, Huang N, Chen CY. Factors associated with treatment mode and termination among preschoolers with ADHD in Taiwan. Psychiatr Serv. 2015;66(2):177–185. doi:10.1176/appi.ps.201300501
27. Cortese S, Adamo N, Del Giovane C, et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis. Lancet Psychiatry. 2018;5(9):727–738. doi:10.1016/S2215-0366(18)30269-4
28. Elnaem MH, Irwan NA, Abubakar U, Syed Sulaiman SA, Elrggal ME, Cheema E. Impact of medication regimen simplification on medication adherence and clinical outcomes in patients with long-term medical conditions. Patient Prefer Adherence. 2020;14:2135–2145. doi:10.2147/PPA.S268499
29. Elnaem MH, AbouKhatwa MM, Elrggal ME, Dehele IS. Attention deficit hyperactivity disorder: what are pharmacists’ roles and associated outcomes? Int J Environ Res Public Health. 2023;20(3):2754. doi:10.3390/ijerph20032754
30. Biederman J, Fried R, DiSalvo M, et al. A novel text message intervention to improve adherence to stimulants in adults with attention deficit/hyperactivity disorder. J Clin Psychopharmacol. 2019;39(4):351–356. doi:10.1097/JCP.0000000000001055
31. Wang T, Huang YM, Chan HY. Exploration of features of mobile applications for medication adherence in Asia: narrative review. J Med Internet Res. 2024;26:e60787. doi:10.2196/60787
32. Bussing R, Koro-Ljungberg M, Noguchi K, Mason D, Mayerson G, Garvan CW. Willingness to use ADHD treatments: a mixed methods study of perceptions by adolescents, parents, health professionals and teachers. Soc Sci Med. 2012;74(1):92–100. doi:10.1016/j.socscimed.2011.10.009
33. DosReis S, Mychailyszyn MP, Evans-Lacko SE, Beltran A, Riley AW, Myers MA. The meaning of attention-deficit/hyperactivity disorder medication and parents’ initiation and continuity of treatment for their child. J Child Adolesc Psychopharmacol. 2009;19(4):377–383. doi:10.1089/cap.2008.0118
34. Ahmed R, McCaffery KJ, Aslani P. Factors influencing parental decision making about stimulant treatment for attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. 2013;23(3):163–178. doi:10.1089/cap.2012.0087
35. Adler LD, Nierenberg AA. Review of medication adherence in children and adults with ADHD. Postgrad Med. 2010;122(1):184–191. doi:10.3810/pgm.2010.01.2112
36. Brinkman WB, Hartl Majcher J, Poling LM, et al. Shared decision-making to improve attention-deficit hyperactivity disorder care. Patient Educ Couns. 2013;93(1):95–101. doi:10.1016/j.pec.2013.04.009
37. Fiks AG, Hughes CC, Gafen A, Guevara JP, Barg FK. Contrasting parents’ and pediatricians’ perspectives on shared decision-making in ADHD. Pediatrics. 2011;127(1):e188–196. doi:10.1542/peds.2010-1510
38. Tzang RF, Chang YC, Chen CC. Barriers to seeking help among children with attention deficit hyperactivity disorder in Taiwan. Asia Pac Psychiatry. 2014;6(4):373–378. doi:10.1111/appy.12064
39. Pohl L, El-Kurdi R, Selinger R, Sauls A, Rhodes LA, Marciniak MW. Implementation of a community-based pharmacist-run attention deficit hyperactivity disorder clinic in a college health center. J Am Pharm Assoc. 2021;61(4S):S178–S183. doi:10.1016/j.japh.2021.01.029
40. Ministry of Health and Welfare. Community pharmacy offers comprehensive and varied services in Taiwan. 2017. Available from: https://www.mohw.gov.tw/cp-3425-38871-2.html.
41. McMillan SS, Kelly F, Hattingh HL, Fowler JL, Mihala G, Wheeler AJ. The impact of a person-centred community pharmacy mental health medication support service on consumer outcomes. J Ment Health. 2018;27(2):164–173. doi:10.1080/09638237.2017.1340618
42. Huang YM, Wang YH, Chan HY, et al. Engaging consumers in wise use of over-the-counter medications in Taiwan: development and evaluation of a structured medication counseling approach. Patient Educ Couns. 2022;105(4):942–948. doi:10.1016/j.pec.2021.08.009
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Medication Adherence and Its Associated Factors Among Outpatients with Heart Failure
Jarab AS, Al-Qerem WA, Hamam HW, Alzoubi KH, Abu Heshmeh SR, Mukattash TL, Alefishat E
Patient Preference and Adherence 2023, 17:1209-1220
Published Date: 8 May 2023
Medication Adherence Interventions Among People Living with Diabetes: A Systematic Review
Wang M, Lee K, Thew HZ, Sowtali SN, Jiang Q, Cao Y, Lim PY
Patient Preference and Adherence 2025, 19:3095-3112
Published Date: 7 October 2025