Back to Journals » Patient Preference and Adherence » Volume 17
Medication Adherence and Its Associated Factors Among Outpatients with Heart Failure
Authors Jarab AS ![]() , Al-Qerem WA
, Al-Qerem WA ![]() , Hamam HW
, Hamam HW ![]() , Alzoubi KH
, Alzoubi KH ![]() , Abu Heshmeh SR
, Abu Heshmeh SR ![]() , Mukattash TL
, Mukattash TL ![]() , Alefishat E
, Alefishat E ![]()
Received 28 February 2023
Accepted for publication 28 April 2023
Published 8 May 2023 Volume 2023:17 Pages 1209—1220
DOI https://doi.org/10.2147/PPA.S410371
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Anan S Jarab,1,2 Walid A Al-Qerem,3 Hanan Walid Hamam,1 Karem H Alzoubi,4,5 Shrouq R Abu Heshmeh,1 Tareq L Mukattash,1 Eman Alefishat6– 8
1Department of Clinical Pharmacy, Faculty of Pharmacy, Jordan University of Science and Technology, Irbid, 22110, Jordan; 2College of Pharmacy, Al Ain University, Abu Dhabi, United Arab Emirates; 3Department of Pharmacy, Faculty of Pharmacy, Al-Zaytoonah University of Jordan, Amman, 11733, Jordan; 4Department of Pharmacy Practice and Pharmacotherapeutics, College of Pharmacy, University of Sharjah, Sharjah, United Arab Emirates; 5Faculty of Pharmacy, Jordan University of Science and Technology, Irbid, Jordan; 6Department of Pharmacology, College of Medicine and Health Science, Khalifa University of Science and Technology, Abu Dhabi, 127788, United Arab Emirates; 7Department Biopharmaceutics and Clinical Pharmacy, Faculty of Pharmacy, University of Jordan, Amman, 11942, Jordan; 8Center for Biotechnology, Khalifa University of Science and Technology, Abu Dhabi, 127788, United Arab Emirates
Correspondence: Eman Alefishat, Department of Pharmacology, College of Medicine and Health Science, Khalifa University of Science and Technology, Abu Dhabi, 127788, United Arab Emirates, Tel +971 5 07293877, Email [email protected]
Background: Poor adherence to heart failure (HF) medications represents a major barrier to achieve the desired health outcomes in those patients.
Objective: To assess medication adherence and to explore the factors associated with medication non-adherence among patient with HF in Jordan.
Methods: The current cross-sectional study was conducted at the outpatient cardiology clinics at two main hospitals in Jordan from August 2021 through April 2022. Variables including socio-demographics, biomedical variables, in addition to disease and medication characteristics were collected using medical records and custom-designed questionnaire. Medication adherence was assessed using the 4-item Morisky Medication Adherence Scale. Multinomial logistic regression analysis was performed to identify the factors that are significantly and independently associated with medication non-adherence.
Results: Of the 427 participating patients, 92.5% had low to moderate medication adherence. Results of the regression analysis revealed that that patients who had higher education level (OR=3.36; 95% CI 1.08– 10.43; P=0.04) and were not suffering from medication-related side effects (OR=4.7; 95% CI 1.91– 11.5; P=0.001) had significantly higher odds of being in the moderate adherence group. Patients who were taking statins (OR=16.59; 95% CI 1.79– 153.98; P=0.01) or ACEIs/ ARBs (OR=3.95; 95% CI 1.01– 15.41; P=0.04) had significantly higher odds of being in the high adherence group. Furthermore, Patients who were not taking anticoagulants had higher odds of being in the moderate (OR=2.77; 95% CI 1.2– 6.46; P=0.02) and high (OR=4.11; 95% CI 1.27– 13.36; P=0.02) adherence groups when compared to patients who were taking anticoagulants.
Conclusion: The poor medication adherence in the present study sheds the light on the importance of implementing intervention programs which focus on improving patients’ perception about the prescribed medications particularly for patients who have low educational levels, receive an anticoagulant, and do not receive a statin or an ACEI/ ARB.
Keywords: heart failure, medication adherence, medication necessity, medication concerns, intervention, Jordan
Introduction
Heart Failure (HF) is a serious clinical condition that results from cardiac abnormalities which leads to significant reduction in cardiac function.1 In 2017, 64 million people were suffering from HF worldwide.2 American statistics predicted that between 2012 and 2030, the prevalence of HF would increase by 46%. 3 Furthermore, in 2018, HF was found as the underlying cause of 379,800 deaths.4 In Jordan, recent statistics reported that nearly 37% of overall deaths in the country were attributed to non-communicable diseases and cardiovascular diseases (CVDs), including HF.5 HF has a significant burden on the community. The anticipated cost of HF in 2012 was over 30 billion US dollars, and it is predicted that by 2030, that cost will have risen by almost 127%.3
Despite the significant improvement in HF management and prognosis, mortality and hospitalization rates remain high,6,7 which could be attributed to the inadequate medication adherence.8 The World Health Organization (WHO) defined medication adherence as the extent to which an individual’s behaviour corresponds to a healthcare provider’s recommendations.9 According to the 2016 American College of Cardiology Foundation/American Heart Association Guideline recommendations, medical management of patients with HF has become increasingly complex,10 which is one of the major barriers to medication adherence.11
The medication adherence rates among HF patients are poor. It has been reported that at least one out of four patients with HF are non-adherent,12–14 which could lead to poor prognosis manifested by worsening symptoms, frequent hospitalizations, and eventually death.15 Inconsistent findings have been reported with regard to the factors associated with medication non-adherence among HF patients. A study conducted in the United States reported that the most common factors associated with medication non-adherence were forgetfulness, polypharmacy, and being symptom-free.16 In addition to forgetfulness, a study reported that age, gender, disease characteristics, type of disease, number of medications, frequency of visits to healthcare professionals, and satisfaction with treatment were associated with medication non-adherence.17 A study conducted in Australia revealed that complex medication instructions, disruption in medication supply, and adverse drug reactions were the main reasons behind medication non-adherence among HF patients.18 The diversity of the factors that are associated with medication non-adherence, especially among HF patients, necessitates conducting further studies to reveal the true predictors of medication non-adherence among HF patients. In Jordan, medication adherence among HF has not yet been explored. Therefore, this study aimed to evaluate medication adherence and to explore the factors associated with medication non-adherence among patients with HF in Jordan.
Material and Methods
Study Design and Settings
This cross-sectional study was conducted on patients with HF attending the outpatient cardiology clinics at King Abdullah University Hospital and Al Bashir Hospital in Jordan in the period from August 2021 through April 2022. During the study period, patients who were 18 years or older, had a confirmed diagnosis of HF for at least six months, had a cardiologist’s assignment of New York Heart Association (NYHA) classification, were taking at least one HF medication and agreed to sign a consent form were included in the study. Patients with acute decompensation of HF or an active listing for heart transplantation and patients with cognitive impairment were excluded from the study. Patients who were eligible to participate were informed that participation is voluntary, they have the right to withdraw at any time, their medical care and treatment will not be affected by their participation, and the collected data will only be used for research purposes. The interview took approximately 10–15 minutes to be completed.
Study Instruments
During the outpatient clinic visit, the research pharmacist HH used a custom-designed questionnaire and the medical records to collect information about socio-demographic, disease, and medication related variables. The researcher also collected biomedical data including low-density lipoproteins (LDL), high-density lipoproteins (HDL), triglycerides (TGs), total cholesterol, glycosylated haemoglobin A1c (HbA1c), random blood glucose, systolic blood pressure (SBP), diastolic blood pressure (DBP), ejection fraction (EF%), serum creatinine, white blood cells (WBCs), red blood cells (RBCs), and haemoglobin (Hb). The validated Arabic version of the 4-item Morisky Medication Adherence Scale was used to evaluate patients’ willingness to take the medications as prescribed.19,20 The four items were: Do you forget to take your medications? Are you careless about the time of taking your medications? Do you stop taking your medications when you feel better? Do you stop taking your medications when you feel worse? According to their responses, patients were divided into three groups: patients who reported three or more “yes” responses were considered to have low adherence, those who reported one or two “yes” responses were deemed to have moderate adherence, while those who reported four “no” answers were considered to have high adherence.
Sample Size Calculation
Sample size calculation was conducted to ensure enrolling sufficient patients to produce a model with appropriate statistical power to detect any significant impact. The 50 + 8P equation was used to compute the minimum sample size required to conduct multinomial regression, where P represents the number of predictors. The original aim of the study was to evaluate the association of the forty-seven variables with the medication adherence level. Therefore, the minimum required sample size was 282 patients.21
Data Analysis
The Statistical Package for the Social Sciences (SPSS) version 26 from IBM was used to run descriptive and analytical statistics. Descriptive analysis was used to describe continuous variables in terms of the mean (standard deviations) and the categorical variables in terms of frequencies (percentages). Participants’ differences with regard to medication adherence were tested using ANOVA and Kruskal–Wallis tests for normally and non-normally distributed continuous variables, respectively. Pearson Chi-square test was conducted to explore the association between the categorical variables and medication adherence among the study participants. Variables with a p-value <0.1 at the univariate analysis were included in the multinomial logistic regression to explore significant and independent predictors of medication adherence.
Results
Out of 550 patients with HF, a total of 427 patients agreed to participate in the study. The total participants’ mean age was 63 (SD =12) years. The majority of the participants were males (63.8%), married (94.4%), living with their families (94.6%), living in the city (66.8%), did not complete their education (69.4%), unemployed or retired (77.6%), had low monthly income (67.1%), non-smokers (69.9%), and were physically inactive (88.1%). Most of the patients showed moderate adherence to HF medications (83.6%), followed by high (8.9%) and low adherence (7.5%). The participants were stratified based on the adherence level and the results indicated that 31.3% of the high adherence group had college/university degree while only 13.2% of the low adherence group had college/university degree (P <0.1). Furthermore, 50% of the high adherence group were residing in the city, whereas 73.7% of the low adherence group and 67.6% of the moderate adherence group were residents of the city (P <0.1). Other demographic characteristics of the participants are presented in Table 1.
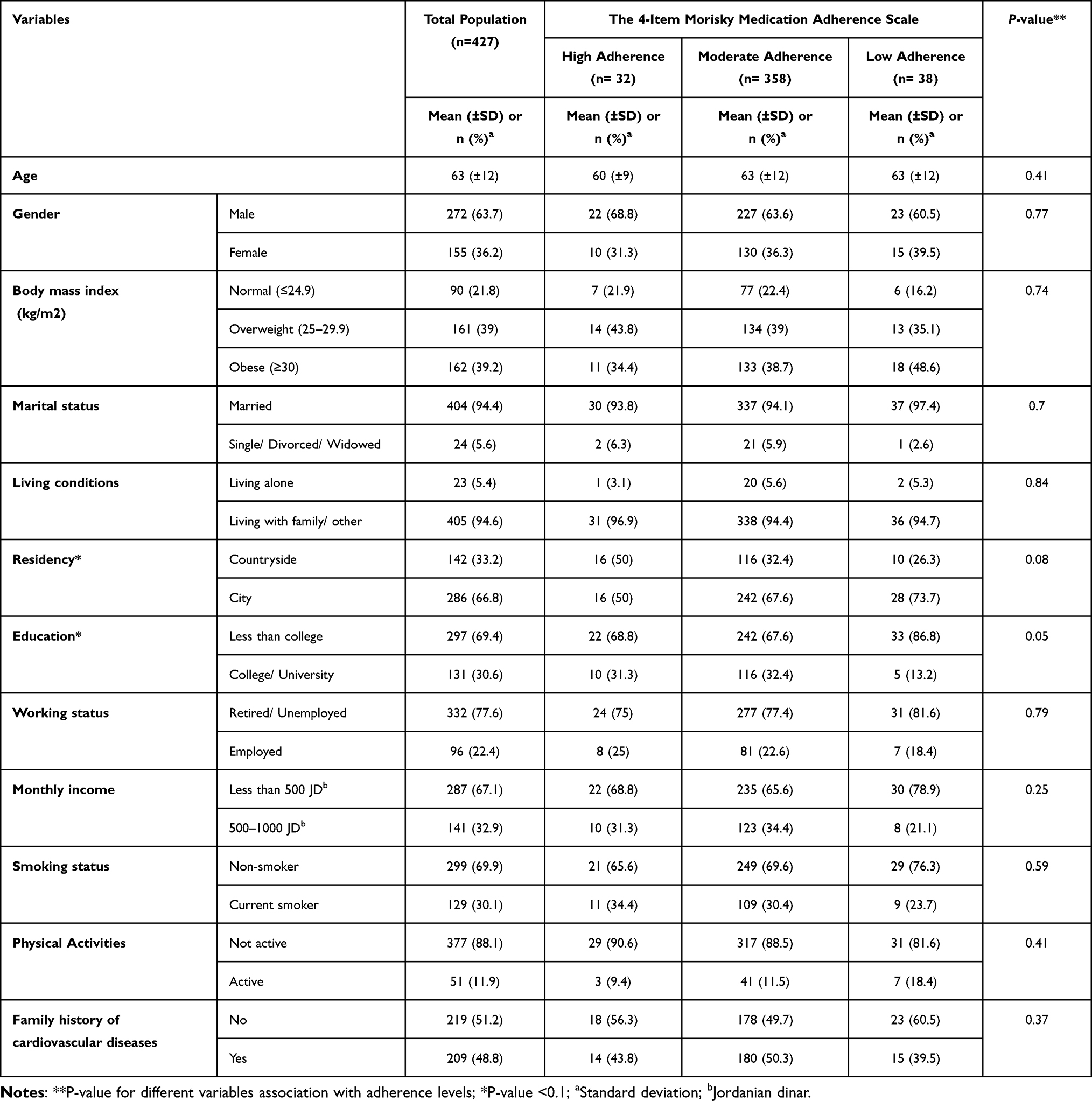 |
Table 1 Demographic Characteristics of the Participants |
As a total, the patients had a mean HF duration of 6.4 (SD = 6.16) years. Most of the patients were classified as group III/IV according to NYHA classification (69.6%), with an average EF% of 42 (SD =10), indicating that the heart on average pumps 42% of the total volume of blood in each beat, and 170 patients (39.7%) had an EF of less than 40%, ie, the heart pumps less than 40% of the total volume of blood in each beat. The mean number of comorbid diseases was 3 (SD =1), and the most common comorbidities were hypertension (77.1%), type 2 diabetes (61.2%), and ischemic heart disease (IHD) (64.3%). The patients were taking 8 (SD =3) medications on average, and the mean number of HF medications was 3 (SD =1). The most prescribed HF medications were beta blockers (88.6%), loop diuretics (67.5%), and angiotensin-converting enzyme inhibitors (ACEIs)/ angiotensin-receptor blockers (ARBs) (66.8%). The majority of the patients were satisfied with their medications (77.3%), had no fears about the side effects of the medications (71.3%), and did not experience side effects (68%). The mean of BP readings was 129 (SD =22) mm HG for SBP and 76 (SD =22) mm HG for DBP. According to adherence levels, 46.9% of the high adherence group were classified I/II according to NYHA, while 21.1% of the moderate adherence patients and 29.9% of the low adherence patients had the same classification (P <0.1). The prevalence of diabetes among the low (71.1%) and moderate (61.7%) adherence groups was higher than that in the high adherence group (43.8%; P <0.1). The percentages of patients who were not having chronic kidney disease was 78.9%, 86.9%, and 96.9% in the low, moderate, and high adherence groups respectively (P <0.1).
Among the patients with high adherence level, 40.6% experienced side effects, while higher percentage was reported in in the low adherence group (60.5% (P <0.1). Similarly, 34.4% of the patients in the high adherence group experienced fears of side effects compared to 55.3% in the low adherence group (P <0.1). Results showed that 52.6% of the patients who reported low medication adherence were taking ACEIs/ARBs, while higher percentages were reported among the patients in the moderate and high adherence groups (67.3% and 78.1% respectively, P<0.1). Moreover, 93.8% of the high adherence group were on statins compared to 63.2% in the low adherence group (P <0.1). On the hand, 31.3% of the high adherence patients were taking anticoagulants, while higher percentage (52.6%) were prescribed anticoagulant in the low adherence group (P <0.1). Other disease and medication characteristics of the study participants are presented in Table 2. As shown in Table 3, the results indicated that mean values for total cholesterol were 4.74 (SD =1.96) in the high adherence group versus 4.6 (SD =1.27) in the low adherence group (P <0.1). Results also showed that mean LDL was 2.97 (SD =1.78) in the high adherence groupversus 2.39 (SD =1.04) in the moderate adherence group (P <0.1).
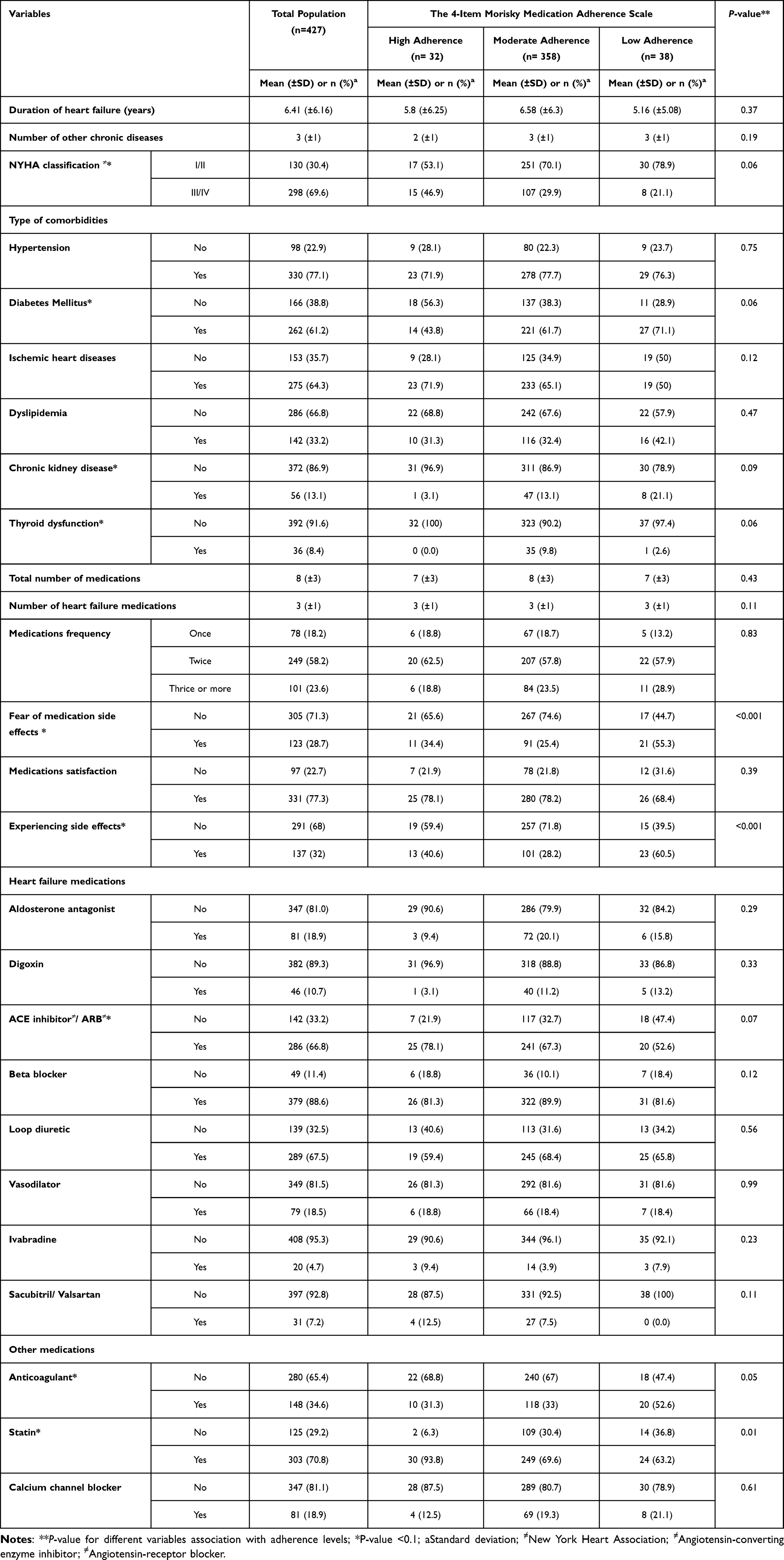 |
Table 2 Disease and Medication Characteristics of the Study Participants |
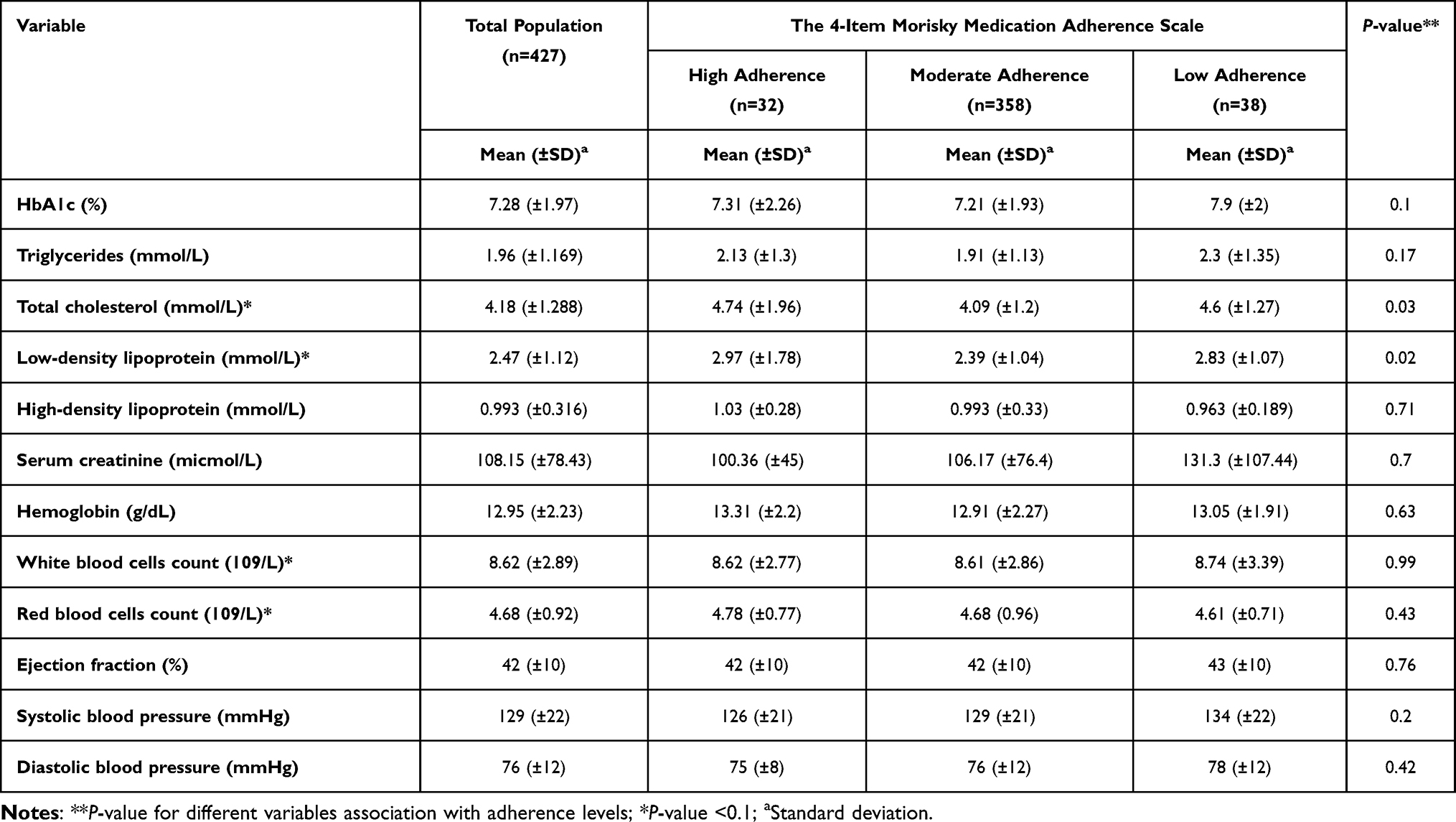 |
Table 3 Biomedical Variables of the Participants |
Results of the regression analysis (Table 4) showed that patients with higher education level had significantly higher odds of being in the moderate adherence group when compared to patients with lower education level (OR=3.36; 95% CI 1.08–10.43; P=0.04). Furthermore, patients who were not suffering from medication-related side effects had higher odds of being in the moderate adherence group when compared to patients who experienced side effects (OR=4.7; 95% CI 1.91–11.5; P=0.001). Patients who were taking statins (OR=16.59; 95% CI 1.79–153.98; P=0.01) or ACEIs/ ARBs (OR=3.95; 95% CI 1.01–15.41; P=0.04) had significantly higher odds of being in the high adherence group. Patients who were not taking anticoagulants had higher odds of being in the moderate adherence group (OR=2.77; 95% CI 1.2–6.46; P=0.02) and high (OR=4.11; 95% CI 1.27–13.36; P=0.02) when compared to patients who were taking anticoagulants.
 |
Table 4 Variables Associated with Medication Non-Adherence* |
Discussion
Evaluation of medication non-adherence and its associated factors is an important preliminary step for the development of future intervention programs which aim at improving medication adherence and health outcomes in HF patients. More than 90% of the present study participants reported low and moderate medication adherence, while only 7.5% reported high adherence, posing a real threat to health outcomes in patients with HF in Jordan. Consistent findings were reported in previous studies conducted in the Arab world and Western countries among patients with CVDs, including HF.22–26 A study conducted on elderly patients with HF who were treated with digoxin found that 90% of the participants were non-adherent to digoxin during one year follow-up period.27 Another study conducted in Tanzania reported that 75% of the participants were found to be non-adherent.28 A study conducted in Thailand revealed that 62% of the participating HF patients were classified as non-adherent.29 On the other hand, an American study reported that only 4% of the patients with HF were found to be non-adherent, 30 and another American study reported a 7% non-adherence rate among patients with HF.31 A systematic review reported that rates of medication adherence among patients with HF varied widely from 10% to 99%.32 The research population’s diversity and the variety of methodologies utilized to measure medication adherence may be the reason behind this notable difference in adherence rates.
Consistent with this study results, a study conducted on African Americans revealed that lower educational attainment was an independent predictor of medication non-adherence among patients with hypertension.33 Another study reported that educational level significantly affected medication adherence in African Americans with hypertension, where lower education was associated with lower adherence in the participating women.34 A previous Jordanian study reported that higher education levels positively affected medication adherence among patients with different chronic diseases.35
The current study found a significant association between experiencing medications’ side effects and medication non-adherence. Consistent with the current study findings, a previous survey showed that medication side effect was one of the most common reasons for medication non-adherence.36
The current study results showed that patients who were not taking statins had significantly lower medication adherence than their counterparts. Consistent with this finding, earlier studies showed that the majority of the patients who were receiving statins had good adherence, especially during the first month of therapy.37–40 Furthermore, it was established that in-hospital prescription of statins was associated with increased adherence rates.41 On the other hand, a previously published study demonstrated low levels of medication adherence among patients who were receiving statins.42 Statins are recommended as first-line lipid-lowering and vascular protective agents for the primary and secondary prevention of atherosclerotic CVDs.43 Therefore, Patients who are prescribed statins usually have a risk of developing CVDs or have an established CVD, and non-adherence to these agents has been associated with negative clinical consequences and cardiovascular events,44,45 which could increase the sense of medication necessity to avoid any potential cardiovascular events.
This study revealed that patients who were taking ACEIs or ARBs had significantly higher medication adherence than their counterparts. Consistent results were found in previous studies.46,47 A possible justification for this association could be related to the numerous benefits these medications possess on cardiac function, symptoms, and patient’ outcomes, as well as their tolerability and fewer side effects when compared to other medications.48 Patients who witnessed these beneficial effects while using ACEIs or ARBs would be more motivated to stick to the therapeutic regimen which made life with HF easier.
A negative association between taking anticoagulants and medication adherence was reported in the present study. Similarly, a study showed that receiving anticoagulants was associated with medication non-adherence in patients with different chronic conditions.49,50 On the other hand, an earlier study reported that taking warfarin for 3–5 years positively affected medication adherence in patients with mechanical heart valves.51 Other studies showed that medication adherence was significantly higher among patients with HF and atrial fibrillation (AF) who were prescribed warfarin therapy at discharge than those who were not.52–54 The negative impact of taking an anticoagulant on medication adherence in the current study could be justified by the patient’s concerns about its side effects, such as the risk of falls and haemorrhagic complications.55
In contrast with earlier research findings, 56–60 polypharmacy manifested by receiving an average of eight medications was not associated with medication non-adherence in the present study. However, polypharmacy was not associated with medication non-adherence in other studies.61,62 The lack of association may be justified by that polypharmacy is often assessed along with multiple other covariates to determine their association with medication adherence, making it difficult to determine the true association between polypharmacy and medication non-adherence. It’s unanimous that selecting the least possible number of prescribed medications seems to be more convenient and limit the chance to develop side effects from the prescribed medications.
Given the sparse information on the factors associated with medication adherence in patients with HF, the present study findings help narrowing down such factors and should provide insight for the development of future interventions which aim at enhancing medication adherence among patients with HF. Healthcare providers should give priority for prescribing ACEIs/ARBs for patients with HF unless contraindicated. They also should select medications with fewer side effects, provide the patients with information about the potential side effects and an advice on coping with them, with a focus on patients with low education level in order to help enhancing medication adherence and hence health outcomes among HF patients.
The current study has some limitations. The social desirability and recall bias associated with the use of a self-report method to assess medication non-adherence could have affected the results. The study was conducted in only two hospital sites, which might limit the generalizability of the study findings. The convenient sampling technique used in this study might cause selection bias. Moreover, the cross-sectional study design cannot confirm the cause-effect relationship, the protopathic bias cannot be excluded and the longitudinal outcomes cannot be measured. Furthermore, although the present study evaluated more than forty variables that may influence medication adherence, other confounding variables, such as the psychological status, which might influence adherence, was not evaluated in the present study.
Conclusions
Based on the study findings, it is clear that medication adherence represents an area for improvement among patients with HF. The current research should provide insight on the factors that should be specifically targeted by the healthcare providers in order to improve medication adherence. Future interventions and HF management programs should prioritize ACEIs/ARBs over the other HF medications, in addition to providing counselling on the potential side effects of the prescribed medications and how to cope with them, particularly for patients with low education level. Further research to evaluate the impact of targeting the factors identified in the present study on adherence level is deemed necessary.
Data Sharing Statement
The data generated and/or analysed during the present study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
Ethical approval was obtained from the Institutional Review Board of KAUH at Jordan University of Science and Technology (Ref. # 32/141/2021). An informed consent form was obtained from each patient agreed to participate in the study. The study has been carried out in accordance with the Declaration of Helsinki (1975) for experiments involving human subjects.
Author Contributions
All authors made a significant contribution with regard to work conception, study design, acquisition, analysis, and interpretation of the data, drafting, revising, or critically reviewing the article. All authors also gave final approval of the version to be published and have agreed on the journal to which the article has been submitted and to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of. Eur Heart J. 2016;37(27):2129–2200m. doi:10.1093/EURHEARTJ/EHW128
2. James SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1789–1858. doi:10.1016/S0140-6736(18)32279-7
3. Heidenreich PA, Albert NM, Allen LA, et al. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6(3):606–619. doi:10.1161/HHF.0B013E318291329A
4. Zambroski CH, Moser DK, Bhat G, Ziegler C. Impact of symptom prevalence and symptom burden on quality of life in patients with heart failure. Eur J Cardiovasc Nurs. 2005;4(3):198–206. doi:10.1016/J.EJCNURSE.2005.03.010
5. World Health Organization. Noncommunicable diseases country profiles 2018. World Health Organization; 2018:223. Available from: http://www.who.int/iris/handle/10665/274512.
6. Goldberg RJ, Ciampa J, Lessard D, Meyer TE, Spencer FA. Long-term survival after heart failure: a contemporary population-based perspective. Arch Intern Med. 2007;167(5):490–496. doi:10.1001/ARCHINTE.167.5.490
7. Ho PM, Magid DJ, Shetterly SM, et al. Medication nonadherence is associated with a broad range of adverse outcomes in patients with coronary artery disease. Am Heart J. 2008;155(4):772–779. doi:10.1016/J.AHJ.2007.12.011
8. Zahwe M, Isma’eel H, Skouri H, et al. Validation of the Arabic version of the Minnesota living with heart failure questionnaire. Hear Lung. 2020;49(1):36–41. doi:10.1016/j.hrtlng.2019.10.006
9. World Health Organization. Adherence to long-term therapies: evidence for action / [edited by Eduardo Sabaté]; 2003. Available from: https://apps.who.int/iris/handle/10665/42682.
10. Yancy CW, Jessup M, Bozkurt B, et al. 2016 ACC/AHA/HFSA focused update on new pharmacological therapy for heart failure: an update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinic. Circulation. 2016;134(13):e282–e293. doi:10.1161/CIR.0000000000000435/-/DC1
11. Mann DM, Allegrante JP, Natarajan S, Halm EA, Charlson M. Predictors of adherence to statins for primary prevention. Cardiovasc Drugs Ther. 2007;21(4):311–316. doi:10.1007/S10557-007-6040-4
12. Calvin JE, Shanbhag S, Avery E, Kane J, Richardson D, Powell L. Adherence to evidence-based guidelines for heart failure in physicians and their patients: lessons from the Heart Failure Adherence Retention Trial (HART). Congest Hear Fail. 2012;18(2):73–78. doi:10.1111/J.1751-7133.2011.00263.X
13. Nieuwenhuis MMW, Jaarsma T, van Veldhuisen DJ, van der Wal MHL. Self-reported versus ‘true’ adherence in heart failure patients: a study using the medication event monitoring system. Netherlands Hear J. 2012;20(7):313–319. doi:10.1007/S12471-012-0283-9
14. Viana M, Laszczynska O, Mendes S, et al. Medication adherence to specific drug classes in chronic heart failure. J Manag Care Spec Pharm. 2015;20(10):1018–1026. doi:10.18553/JMCP.2014.20.10.1018
15. Fitzgerald AA, Powers JD, Ho PM, et al. Impact of medication nonadherence on hospitalizations and mortality in heart failure. J Card Fail. 2011;17(8):664–669. doi:10.1016/J.CARDFAIL.2011.04.011
16. Aggarwal B, Pender A, Mosca L, Mochari-Greenberger H. Factors associated with medication adherence among heart failure patients and their caregivers. J Nurs Educ Pract. 2014;5(3):22. doi:10.5430/JNEP.V5N3P22
17. Shaheen H, Haq N, Riaz S, Naseem A, Zarak M. Assessment of medication adherence among non-communicable chronic disease patients in Quetta, Pakistan: predictors of medication adherence. Asian J Med Heal. 2017;4(4):1–9. doi:10.9734/AJMAH/2017/34300
18. Toh CT, Jackson B, Gascard DJ, Manning AR, Tuck EJ. Barriers to medication adherence in chronic heart failure patients during home visits. J Pharm Pract Res. 2010;40(1):27–30. doi:10.1002/J.2055-2335.2010.TB00721.X
19. Elhenawy YI, Abdelmageed RI, Zaafar DK, Abdelaziz AW. Adherence to insulin therapy among children with type 1 diabetes: reliability and validity of the Arabic version of the 4-item morisky medication adherence scale. Patient Prefer Adherence. 2022;16:1415–1421. doi:10.2147/PPA.S341061
20. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67–74. doi:10.1097/00005650-198601000-00007
21. Green SB. How many subjects does it take to do a regression analysis. Multivariate Behav Res. 1991;26(3):499–510. doi:10.1207/S15327906MBR2603_7
22. Awad A, Osman N, Altayib S. Medication adherence among cardiac patients in Khartoum State, Sudan: a cross-sectional study. Cardiovasc J Afr. 2017;28(6):350–355. doi:10.5830/CVJA-2017-016
23. Di Martino M, Alagna M, Cappai G, et al. Adherence to evidence-based drug therapies after myocardial infarction: is geographic variation related to hospital of discharge or primary care providers? A cross-classified multilevel design. BMJ Open. 2016;6(4):e010926. doi:10.1136/BMJOPEN-2015-010926
24. Ezeala-Adikaibe B, Mbadiwe N, Okudo G, Nwosu N, Nwobodo N. Factors associated with medication adherence among hypertensive patients in a tertiary health center: a cross-sectional study. Arch Community Med Public Heal. 2017;3(1):024–031. doi:10.17352/2455-5479.000021
25. Mosleh SM, Almalik MMA. Illness perception and adherence to healthy behaviour in Jordanian coronary heart disease patients. Eur J Cardiovasc Nurs. 2016;15(4):223–230. doi:10.1177/1474515114563885
26. Shin S, Song H, Oh SK, Choi KE, Kim H, Jang S. Effect of antihypertensive medication adherence on hospitalization for cardiovascular disease and mortality in hypertensive patients. Hypertens Res. 2013;36(11):1000–1005. doi:10.1038/hr.2013.85
27. Monane M, Bohn R, Gurwitz J, Glynn R, Avorn J. Noncompliance with congestive heart failure therapy in the elderly. Arch Intern Med. 1994;154(4):433–437. doi:10.1001/archinte.1994.00420040107014
28. Pallangyo P, Millinga J, Bhalia S, et al. Medication adherence and survival among hospitalized heart failure patients in a tertiary hospital in Tanzania: a prospective cohort study. BMC Res Notes. 2020;13(1):1–8. doi:10.1186/S13104-020-04959-W/FIGURES/1
29. Silavanich V, Nathisuwan S, Phrommintikul A, Permsuwan U. Relationship of medication adherence and quality of life among heart failure patients. Hear Lung. 2019;48(2):105–110. doi:10.1016/j.hrtlng.2018.09.009
30. Evangelista LS, Berg J, Dracup K. Relationship between psychosocial variables and compliance in patients with heart failure. Hear Lung J Acute Crit Care. 2001;30(4):294–301. doi:10.1067/mhl.2001.116011
31. Artinian NT, Magnan M, Sloan M, Lange MP. Self-care behaviors among patients with heart failure. Hear Lung J Acute Crit Care. 2002;31(3):161–172. doi:10.1067/mhl.2002.123672
32. Van Der Wal MHL, Jaarsma T, Van Veldhuisen DJ. Non-compliance in patients with heart failure; how can we manage it? Eur J Heart Fail. 2005;7(1):5–17. doi:10.1016/J.EJHEART.2004.04.007
33. Schoenthaler A, Ogedegbe G, Allegrante JP. Self-efficacy mediates the relationship between depressive symptoms and medication adherence among hypertensive African Americans. Heal Educ Behav. 2009;36(1):127–137. doi:10.1177/1090198107309459
34. Braverman J, Dedier J. Predictors of medication adherence for African American patients diagnosed with hypertension. Ethn Dis. 2009;19(4):396–400.
35. Basheti IA, Saqf El Hait S, Qunaibi EA, Aburuz S, Bulatova N. Associations between patient factors and medication adherence: a Jordanian experience. Pharm Pract. 2016;14(1). doi:10.18549/PHARMPRACT.2016.01.639
36. Snyder VL. Improving outcomes in heart failure: an interdisciplinary approach. AORN J. 2001;74(4):558–559. doi:10.1016/S0001-2092(06)61697-9
37. Benner JS, Glynn RJ, Mogun H, Neumann PJ, Weinstein MC, Avorn J. Long-term persistence in use of statin therapy in elderly patients. JAMA. 2002;288(4):455–461. doi:10.1001/JAMA.288.4.455
38. Jackevicius CA, Mamdani M, Tu JV. adherence with Statin therapy in elderly patients with and without acute coronary syndromes. JAMA. 2002;288(4):462–467. doi:10.1001/JAMA.288.4.462
39. Parris ES, Lawrence DB, Mohn LA, Long LB. Adherence to Statin therapy and LDL cholesterol goal attainment by patients with diabetes and dyslipidemia. Diabetes Care. 2005;28(3):595–599. doi:10.2337/DIACARE.28.3.595
40. Pittman DG, Chen W, Bowlin SJ, Foody JM. Adherence to statins, subsequent healthcare costs, and cardiovascular hospitalizations. Am J Cardiol. 2011;107(11):1662–1666. doi:10.1016/j.amjcard.2011.01.052
41. Muhlestein JB, Horne BD, Bair TL, et al. Usefulness of in-hospital prescription of statin agents after angiographic diagnosis of coronary artery disease in improving continued compliance and reduced mortality. Am J Cardiol. 2001;87(3):257–261. doi:10.1016/S0002-9149(00)01354-0
42. Pedan A, Varasteh LT, Schneeweiss S. Analysis of factors associated with Statin adherence in a hierarchical model considering physician, pharmacy, patient, and prescription characteristics. J Manag Care Pharm. 2015;13(6):487–496. doi:10.18553/JMCP.2007.13.6.487
43. Jellinger PS, Handelsman Y, Rosenblit PD, et al. American Association of Clinical Endocrinologists and American College of Endocrinology guidelines for management of dyslipidemia and prevention of cardiovascular disease. Endocr Pract. 2017;23(2):1–87. doi:10.4158/EP171764.APPGL
44. Chowdhury R, Khan H, Heydon E, et al. Adherence to cardiovascular therapy: a meta-analysis of prevalence and clinical consequences. Eur Heart J. 2013;34(38):2940–2948. doi:10.1093/EURHEARTJ/EHT295
45. Simpson RJ, Mendys P. The effects of adherence and persistence on clinical outcomes in patients treated with statins: a systematic review. J Clin Lipidol. 2010;4(6):462–471. doi:10.1016/j.jacl.2010.08.026
46. Tajeu GS, Kent ST, Huang L, et al. Antihypertensive medication nonpersistence and low adherence for adults. Hypertens. 2019;74(1):35–46. doi:10.1161/HYPERTENSIONAHA.118.12495
47. Kronish IM, Woodward M, Sergie Z, Ogedegbe G, Falzon L, Mann DM. Meta-analysis: impact of drug class on adherence to antihypertensives. Circulation. 2011;123(15):1611. doi:10.1161/CIRCULATIONAHA.110.983874
48. Elliott WJ, Plauschinat CA, Skrepnek GH, Gause D. Persistence, adherence, and risk of discontinuation associated with commonly prescribed antihypertensive drug monotherapies. J Am Board Fam Med. 2007;20(1):72–80. doi:10.3122/JABFM.2007.01.060094
49. Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose regimens and medication compliance. Clin Ther. 2001;23(8):1296–1310. doi:10.1016/S0149-2918(01)80109-0
50. Kneeland PP, Fang MC. Current issues in patient adherence and persistence: focus on anticoagulants for the treatment and prevention of thromboembolism. Patient Prefer Adherence. 2010;4:51–60. doi:10.2147/PPA.S6101
51. Park S, Jang I. Factors affecting medication adherence in patients with mechanical heart valves taking warfarin: the role of knowledge on warfarin, medication belief, depression, and self-efficacy. Int J Environ Res Public Heal. 2021;18(10):5214. doi:10.3390/IJERPH18105214
52. Eapen ZJ, Mi X, Qualls LG, et al. Adherence and persistence in the use of warfarin after hospital discharge among patients with heart failure and atrial fibrillation. J Card Fail. 2014;20(1):23–30. doi:10.1016/J.CARDFAIL.2013.11.006
53. Fuster V, Rydén LE, Cannom DS, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the European society of cardiology committee for practice. Circulation. 2006;114(7). doi:10.1161/CIRCULATIONAHA.106.177292
54. Wann LS, Curtis AB, January CT, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (updating the 2006 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;123(1):104–123. doi:10.1161/CIR.0B013E3181FA3CF4
55. Ogilvie IM, Newton N, Welner SA, Cowell W, Lip GYH. Underuse of oral anticoagulants in atrial fibrillation: a systematic review. Am J Med. 2010;123(7):638–645.e4. doi:10.1016/J.AMJMED.2009.11.025
56. Chapman RH, Petrilla AA, Benner JS, Schwartz JS, Tang SSK. Predictors of adherence to concomitant antihypertensive and lipid-lowering medications in older adults: a retrospective, cohort study. Drugs Aging. 2008;25(10):885–892. doi:10.2165/00002512-200825100-00008
57. Choudhry NK, Fischer MA, Avorn J, et al. The implications of therapeutic complexity on adherence to cardiovascular medications. Arch Intern Med. 2011;171(9):814–822. doi:10.1001/ARCHINTERNMED.2010.495
58. Gray SL, Mahoney JE, Blough DK. Medication adherence in elderly patients receiving home health services following hospital discharge. Ann Pharmacother. 2001;35(5):539–545. doi:10.1345/APH.10295
59. Turner BJ, Hollenbeak C, Weiner MG, Ten Have T, Roberts C. Barriers to adherence and hypertension control in a racially diverse representative sample of elderly primary care patients. Pharmacoepidemiol Drug Saf. 2009;18(8):672–681. doi:10.1002/PDS.1766
60. Stoehr GP, Lu SY, Lavery L, et al. Factors associated with adherence to medication regimens in older primary care patients: the Steel Valley Seniors Survey. Am J Geriatr Pharmacother. 2008;6(5):255–263. doi:10.1016/J.AMJOPHARM.2008.11.001
61. Grant RW, Devita NG, Singer DE, Meigs JB. Polypharmacy and medication adherence in patients with type 2 diabetes. Diabetes Care. 2003;26(5):1408–1412. doi:10.2337/DIACARE.26.5.1408
62. Ownby RL, Hertzog C, Crocco E, Duara R. Factors related to medication adherence in memory disorder clinic patients. Aging Ment Health. 2006;10(4):378–385. doi:10.1080/13607860500410011
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Analysis of Heart Failure with Preserved Vs Reduced Ejection Fraction: Patient Characteristics, Outcomes, Mortality Prediction, and Machine Learning Model Development in the JoHFR
Izraiq M, AlBalbissi K, Alawaisheh R, Toubasi A, Ahmed YB, Mahmoud M, Khraim KI, AL-Ithawi M, Mansour OM, Hamati A, Khraisat FA, Abu-Hantash H
International Journal of General Medicine 2024, 17:3083-3091
Published Date: 15 July 2024
Improving Medication Adherence and Lifestyle Changes: An Image-Based Educational Tool for Patients with Heart Failure
Gao L, Xie Q, Liu T, Liu H, Yan S, Han Y, Zhang M, Zhu D, Guo N, Nicholas S, Maitland E, Wang D
Patient Preference and Adherence 2025, 19:2251-2262
Published Date: 30 July 2025
Medication Adherence Interventions Among People Living with Diabetes: A Systematic Review
Wang M, Lee K, Thew HZ, Sowtali SN, Jiang Q, Cao Y, Lim PY
Patient Preference and Adherence 2025, 19:3095-3112
Published Date: 7 October 2025
Supporting Medication Adherence and Patient-Centered Care for Attention-Deficit Hyperactivity Disorder in Taiwan: A Pharmacist-Oriented Perspective Informed by Targeted Evidence
Chiu YJ, Huang YM
Patient Preference and Adherence 2026, 20:589432
Published Date: 24 February 2026