Back to Journals » Clinical Ophthalmology » Volume 20
Supine and Sitting Intraocular Pressure Measurements Using iCare HOME2 Self-Tonometry and iCare IC200 Rebound Tonometry in Japanese Open-Angle Glaucoma Patients
Authors Nakamura S, Hollό G ![]() , Fukuda Y, Ishida T, Kita Y
, Fukuda Y, Ishida T, Kita Y ![]()
Received 10 April 2026
Accepted for publication 4 June 2026
Published 12 June 2026 Volume 2026:20 616024
DOI https://doi.org/10.2147/OPTH.S616024
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sotiria Palioura
Sho Nakamura,1,* Gábor Holl&oacgr;,2,3,* Yasumasa Fukuda,4 Tomoka Ishida,1 Yoshiyuki Kita1
1Department of Ophthalmology, Kyorin University Suginami Hospital, Tokyo, Japan; 2Tutkimusz Ltd, Solymár, Hungary; 3Ophthalmology Center, Prima Medica Health Centers, Budapest, Hungary; 4Department of Ophthalmology, Kyorin University School of Medicine, Tokyo, Japan
*These authors contributed equally to this work
Correspondence: Yoshiyuki Kita, Department of Ophthalmology, Kyorin University Suginami Hospital, 2-25-1 Wada, Suginami, Tokyo, 166-0012, Japan, Tel +81-3-3383-1281, Fax +81-3-3382-8972, Email [email protected]
Purpose: To evaluate supine and sitting intraocular pressure (IOP) self-measurements using iCare-HOME2 self-tonometry (iCare-HOME2) and to compare the results with corresponding iCare IC200 IOP (iCare) measurements by health care professionals on Japanese glaucoma patients.
Methods: Thirty-six eyes of 36 consecutive primary open-angle and normal-tension glaucoma patients were examined. IOP was measured in sitting position using Goldmann applanation tonometry (GAT), iCare, and iCare-HOME2 self-tonometry, then after a 10-minute supine rest with iCare tonometry and iCare-HOME2 self-tonometry in supine position. ANOVA, intraclass correlation coefficients (ICC) and Bland–Altman analyses were used.
Results: Mean IOPs were 15.8 mmHg (GAT), 13.6 mmHg (iCare), and 14.6 mmHg (iCare-HOME2) in sitting (P ≤ 0.049), and 16.8 mmHg (iCare) and 16.8 mmHg (iCare-HOME2) in supine position (P = 0.99). ICCs between iCare-HOME2 and iCare were 0.899 (95% CI, 0.712– 0.957) in sitting and 0.976 (95% CI, 0.954– 0.988) in supine position. Bland–Altman analysis showed minimal bias in both positions (mean differences: 1.03 mmHg [limits of agreement: − 2.07 to 4.14] in sitting; and − 0.003 mmHg [− 2.18 to 2.17] in supine position).
Conclusion: iCare-HOME2 self-tonometry can accurately measure IOP in both sitting and supine positions. Based on the ICC values, the agreement between IOP values measured by health-care professionals with iCare and by trained open-angle glaucoma patients with iCare HOME2 was higher in the supine position than in the sitting position. Our results suggest that self-measured sitting and supine iCare-HOME2 IOP data are reliable on trained glaucoma patients and may potentially be applied to assist clinical decision making in glaucoma care.
Keywords: iCare IC200, iCare HOME2 self-tonometry, intraocular pressure, glaucoma, rebound tonometry, supine position
Introduction
Intraocular pressure (IOP) measurement remains a most important medical investigation not only to detect glaucoma but also during long-term glaucoma care.1 Elevated IOP values in screening support the detection of glaucoma, and above target IOP values in medically treated glaucoma eyes represent a risk factor for future progression. Goldmann applanation tonometry (GAT) remains the gold standard method for measuring IOP in ophthalmology office conditions in sitting position,2 but it cannot be used for measuring IOP outside the office hours when IOP spikes may also develop. Therefore, other IOP measuring technologies, particularly those that can be used by the trained glaucoma patients, remain in the focus of development.1 Self-tonometry and home tonometry require both precise, reliable, non-invasive and easy to use devices, and sufficiently maintained visual functions (visual acuity and central visual field) from the patient. While the latter needs have not yet been precisely defined the technical development has been continuous in the last decades.1,3,4 Since IOP is higher in supine position compared to sitting position (with an immediate increase of 2.6 ± 2.4 mmHg),5 and IOP elevations may appear during the nighttime (sleep period; increasing from 12.8 to 14.2 mmHg),6 devices suitable to self-tonometry only in sitting position cannot provide full information on the outside office hours IOP and IOP fluctuation. In addition, progression of visual field damage in normal tension glaucoma (NTG) has been reported to be associated with IOP in the supine position and the magnitude of IOP elevation accompanying postural changes.7 Further, IOP measurement which requires topical anaesthesia does not fit to self-tonometry and repeated IOP measurements due to the dose dependent ocular surface toxicity of the anaesthetic eye drops and the risk of corneal injury.
The iCare HOME2 device is a recently developed rebound tonometer,8,9 which does not require topical anaesthesia for the measurements, and according to the information provided by the manufacturer can also be used for supine self-tonometry.10 Thus, this device may potentially be suitable to diurnal self-tonometry in the glaucoma patients’ homes, while the patients follow their routine daily schedules.
The measurement precision of iCare HOME2 self-tonometry in sitting position has been investigated by several research groups.8,11–13 In general, the results showed a good agreement with both GAT and the operator used version of the iCare tonometer (iCare IC200, iCare Finland Oy, Vantaa, Finland).14–16 The difference between mean IOP measured with GAT and iCare HOME2 self-tonometry in sitting position ranged between 0.17 and 2.2 mmHg in the middle teens to middle twenties IOP range,8,11–13 while it was 0.92 mmHg for the iCare IC200 vs. iCare HOME2 comparison in sitting position in a similar IOP range.12
However, to our knowledge, the precision of IOP values self-measured by glaucoma patients with the iCare HOME2 device in supine position has not yet been investigated. Therefore, in the current study, we investigated the agreement of IOP values measured with iCare IC200 tonometry by an experienced orthoptist and with iCare HOME2 self-tonometry, in both sitting and supine positions on primary open-angle glaucoma (POAG) and NTG patients.
Materials and Methods
The Institutional Review Board of Kyorin University, Tokyo, Japan, approved the research design, and the study adhered to the tenets of the Declaration of Helsinki (Authorization number: 2576). The participants were given full explanation of the research design, and a written informed consent was obtained from all participants prior to the investigation.
Consecutive Japanese patients with POAG or NTG without any experience in self-tonometry were recruited between June 2025 and February 2026. The definitions of POAG and NTG were made according to the current (5th) edition of the Japan Glaucoma Society guidelines for glaucoma.17 All participants were examined in the Department of Ophthalmology of Kyorin University Suginami Hospital, Tokyo, Japan. The following ophthalmologic examinations were performed on both eyes of all participants: determination of best-corrected visual acuity (BCVA), IOP measurement with GAT, slit-lamp biomicroscopy, gonioscopy, visual field (VF) testing using the 24–2 Swedish Interactive Threshold Algorithm standard test (Humphrey Field Analyzer; Carl Zeiss Meditec Inc., Dublin, USA), stereoscopic fundus examination via dilated pupil, central corneal thickness (CCT) measurement with the CASIA2 anterior segment swept-source optical coherence tomography (OCT; Tomey Inc., Nagoya, Japan), circumpapillary retinal nerve fiber layer (cpRNFL) thickness assessment using the OCT-S1 instrument (Canon Meditech Supply Corporation, Kanagawa, Japan), and determination of corneal hysteresis (CH) using the ocular response analyzer (Reichert Inc., Depew, USA). The study eyes’ refraction data were converted into spherical equivalent (SE) expressed as the spherical diopter plus half of the cylindrical dioptric power. The inclusion criteria comprised glaucomatous optic nerve head and RNFL damage, reproducible VF deterioration typical for glaucoma, cylindrical refractive error < 3.0 D, BCVA ≥ 0.7, clear optical media, and open anterior chamber angles (Shaffer’s grade > 2). The exclusion criteria comprised clinically significant cataract, unreliable VF test results (>15% false positives rate or false negatives rate, or >20% fixation losses with the 24–2 test), history of any intraocular surgery or laser procedures, any cornea disease/abnormality, and any eye disease beyond open-angle glaucoma. Mean deviation (MD) was used to quantitatively characterise VF deterioration. Both eyes were investigated in the study process, but only one eye per patient was selected for the evaluation. If only one eye met the inclusion criteria that eye was included. If both eyes were eligible, the right eye was selected. Most patients were under topical IOP lowering medications. Glaucoma drug scores were calculated as follows: monotherapy was assigned 1 point, and topical fixed-dose combination therapy 2 points.
Overview of the IOP Measurements
IOP measurements were performed between 3:00 PM and 5:00 PM. First, blood pressure and pulse rate were measured in sitting position. IOP was measured first in sitting position in the following order: GAT, iCare IC200 tonometry and iCare HOME2 self-tonometry. Then IOP was measured in supine position with iCare IC200 tonometry followed by iCare HOME2 self-tonometry.
Goldmann Applanation Tonometry
One drop of oxybuprocaine hydrochloride 0.04% with fluorescein was instilled in both eyes. Two consecutive IOP measurements were made with a one-minute separation by an ophthalmologist (Y.K.) using a calibrated GAT (AT 900; Haag-Streit, Köniz, Switzerland) and a Tonosafe disposable prism (Haag-Streit, Köniz, Switzerland). During GAT measurements, the proper contact of the forehead and the chin with the slit-lamp head rest was confirmed. The mean values of the two IOP measurements were used for the study.
iCare IC200 Tonometry
The iCare IC200 tonometer is handheld rebound tonometer (TA 031, iCare Finland Oy, Vantaa, Finland).18 One iCare IC200 tonometer session comprises six consecutive IOP measurements, and provides a quality report for each individual IOP reading and their variability when the average value is calculated. For the final, reported IOP result, the highest and lowest individual IOP readings are automatically removed, and the remaining four measurements are averaged and expressed in mmHg with one decimal precision. If the difference between the individual readings is unacceptably high a repeat symbol is displayed. In the current investigation only values with optimally low variability (displayed in green colour) were used for analysis. The same experienced orthoptist (S.N.) made all iCare IC200 IOP measurements. One set of measurements was performed in sitting position and another set in supine position.
iCare HOME2 Self-Tonometry
The iCare HOME2 (TA 023, iCare Finland Oy, Vantaa, Finland) is a handheld rebound tonometer designed for home self-tonometry both in sitting and supine positions.10 Similarly to iCare IC200 tonometry IOP is determined from the deceleration of a magnetized probe that bounces back from the cornea. Self-tonometry is made after adjusting the distance of the probe from the cornea and probe alignment using the integrated light guide. The device probe is to be positioned to approximately 5 mm from the cornea for IOP measurement.10 Topical anaesthesia is not required. The measurement quality assessment and the measurement averaging are similar to that described earlier for the iCare IC200 tonometry. The system is supported by a downloadable smart phone application, to assist its accurate use. In the current investigation only values with optimally low variability (displayed in green colour) were used for analysis.10
One set of IOP measurement was performed in sitting and supine positions, with each iCare devices, respectively. Before the IOP measurements, an experienced orthoptist (S.N.) explained the use the iCare HOME2 device to the participants. An approximately 10 to 20 minutes period was spent with the education, practical teaching and training session. The IOP measurement sessions were separated with 5 minutes intervals. First, GAT was performed in sitting position, then iCare IC200 tonometry and iCare HOME2 self -tonometry in sitting and finally in supine position, respectively. The participants remained in supine position for 10 minutes before the supine IOP measurements were started. During the training session, patients continued practicing until they were able to perform six consecutive IOP measurements smoothly, without any assistance by the orthoptist. No time restrictions were made. No patients dropped out during the training session.
Statistical Analysis
Because no previous data regarding supine IOP measurements were available, sample size estimation was based on a previous study comparing iCare HOME2 and iCare IC200 measurements in the sitting position, which reported a mean difference of 0.92 mmHg with a standard deviation of 1.48 mmHg.12 Assuming an alpha level of 0.05 and a power of 80%, the required sample size for paired comparisons was estimated approximately 23 eyes. The normality of the data distribution was assessed using the Shapiro–Wilk test. Differences among the five measurement sessions were analysed using one-way repeated measures analysis of variance (ANOVA). Post-hoc pairwise comparisons were made with Bonferroni adjustment. Inter-device agreement was assessed using a two-way mixed-effects model for absolute agreement intraclass correlation coefficient (ICC). Agreement between the tonometry results was evaluated using the Bland–Altman analysis, and the limits of agreement (LOAs) were defined as the mean difference ± 1.96 SD. Spearman rank correlation coefficients or Pearson correlation coefficient (as needed) were used to analyse correlations between mean between-device IOP difference and the participants’ demographic parameters. All analyses were made with Jamovi software (Version 2.6.44; https://www.jamovi.org), except for the ICC, which was calculated using IBM SPSS Statistics (version 28.0; IBM). The absolute differences between the individual IOP values measured with iCare IC200 and iCare HOME2 in sitting and supine positions, respectively, were compared with the Wilcoxon signed-rank test. Statistical significance was set at P < 0.05. ICC values < 0.50 indicate poor, 0.50–0.75 moderate, 0.75–0.90 good, and >0.90 excellent reliability.19
Results
Thirty-six eyes of 36 consecutive Japanese POAG and NTG patients were examined. The age (mean ± SD) of the patients was 56.8 ± 12.9 years. The spherical equivalent was −4.94 ± 3.50 D. The IOP measured with GAT was 15.8 ± 4.6 (range 10 to 31 mmHg). The demographic characteristics are shown in Table 1. No technical problem or participant complaint occurred during tonometry and self-tonometry.
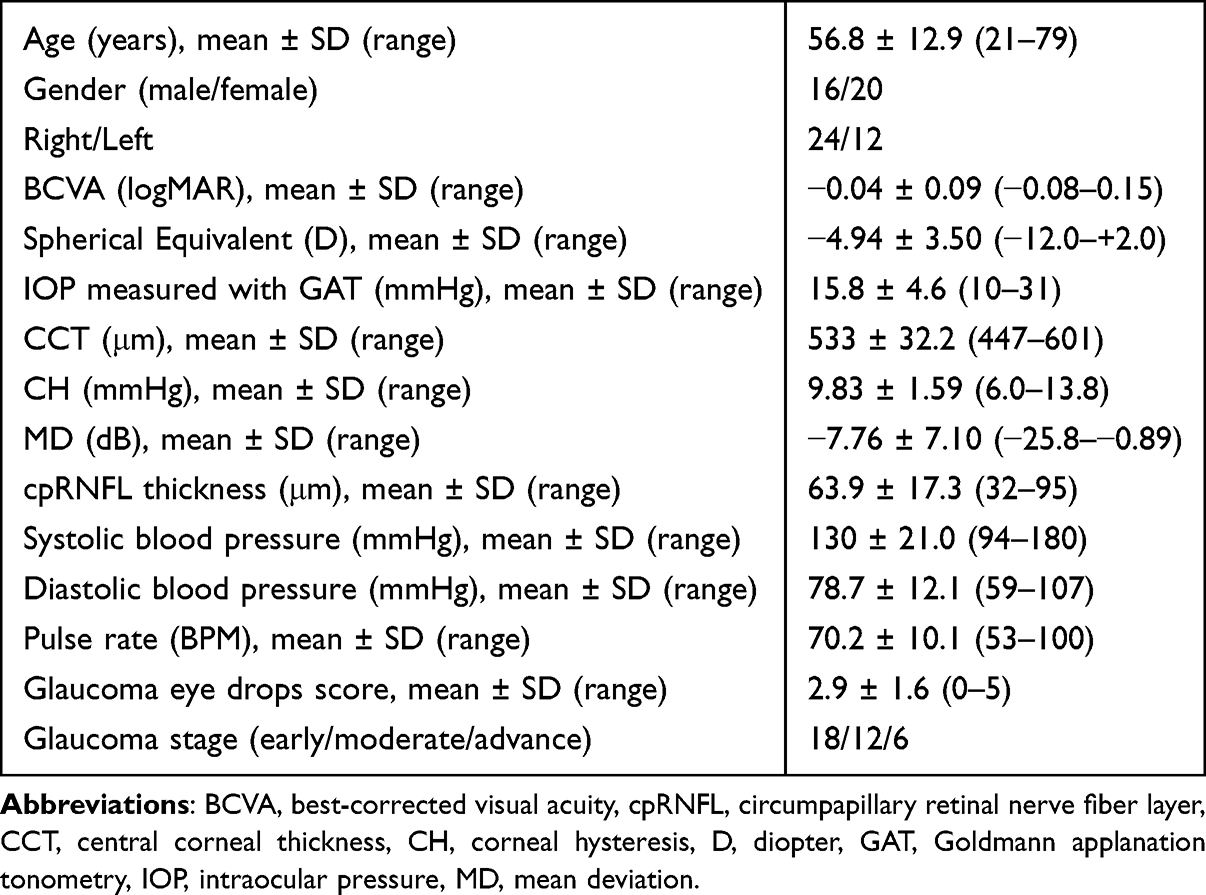 |
Table 1 Characteristics of the Study Participants |
The mean ± SD sitting IOP with GAT, iCare IC200, and iCare HOME2 were 15.8 ± 4.6, 13.6 ± 4.0, and 14.6 ± 4.2 mmHg, respectively (P ≤ 0.049; Table 2). Sitting IOP measured with GAT was significantly higher than sitting IOP measured with both iCare IC200 and iCare HOME 2 (P ≤ 0.017), but significantly lower than supine IOP measured with both iCare IC200 and iCare HOME2 (P ≤ 0.045). The supine IOP measured with iCare IC200 and iCare HOME2 were 16.8 ± 5.1 and 16.8 ± 5.0 mmHg, respectively (P = 0.99). Sitting IOP with both iCare IC200 tonometry and iCare HOME2 self-tonometry was significantly lower than supine IOP with both iCare IC200 and iCare HOME2 tonometry, respectively (P < 0.001 for all comparisons).
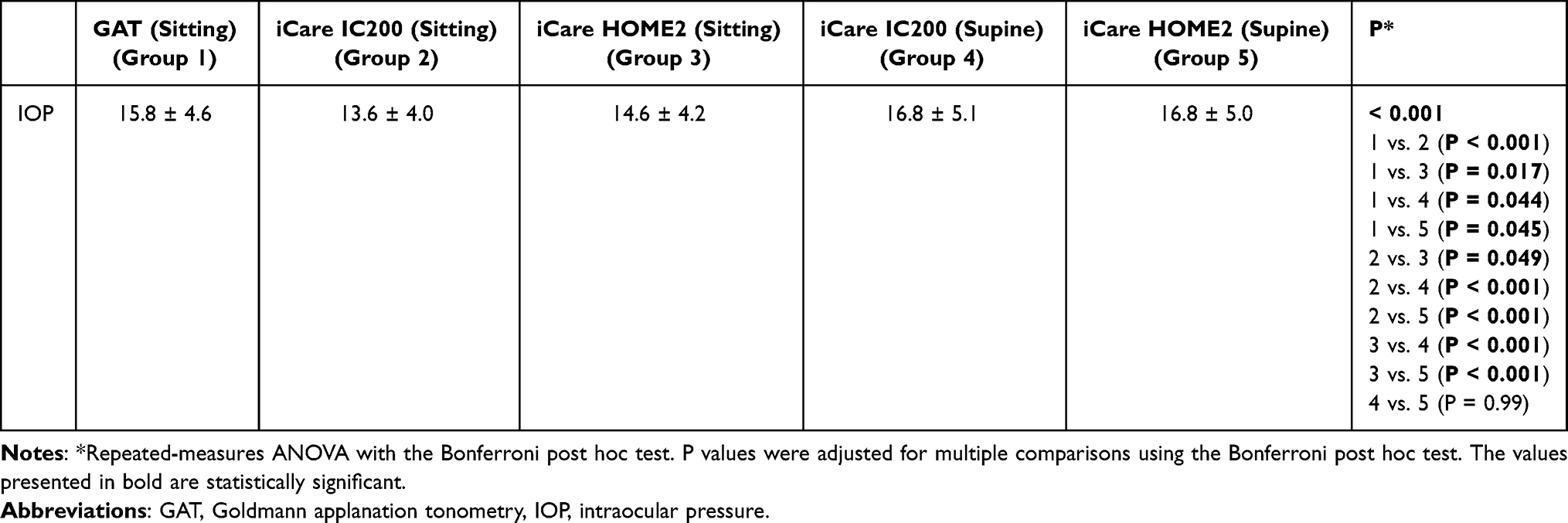 |
Table 2 Comparison of Intraocular Pressure Measurement Results Between the Tonometry Sessions |
In the sitting position, the agreement between the measurement sessions was moderate or good. The ICC between the sitting GAT and iCare IC200 results was 0.704 (95% CI, 0.266–0.870); between the sitting GAT and iCare HOME2 results 0.844 (95% CI, 0.664–0.924), and between the sitting iCare IC200 and iCare HOME2 results 0.899 (95% CI, 0.712–0.957). In the supine position, the agreement between the iCare IC200 and iCare HOME2 results was excellent (ICC 0.976; 95% CI, 0.954–0.988).
The Bland–Altman analysis (Figure 1) showed that in the sitting position, the IOP difference between the iCare IC200 and iCare HOME2 measurements was 1.03 ± 1.60 mmHg (95% CI, 0.49 to 1.57, LOA, −2.07 to 4.14). Interestingly, in the supine position, the difference between IOP results with iCare IC200 tonometry and iCare HOME2 self-tonometry was only 0.00 ± 1.10 mmHg (95% CI, −0.37 to 0.37, LOA, −2.18 to 2.17). No significant correlations were observed between the differences of the two kinds of IOP values and their means (Pearson correlation, P = 0.334 and P = 0.431, respectively).
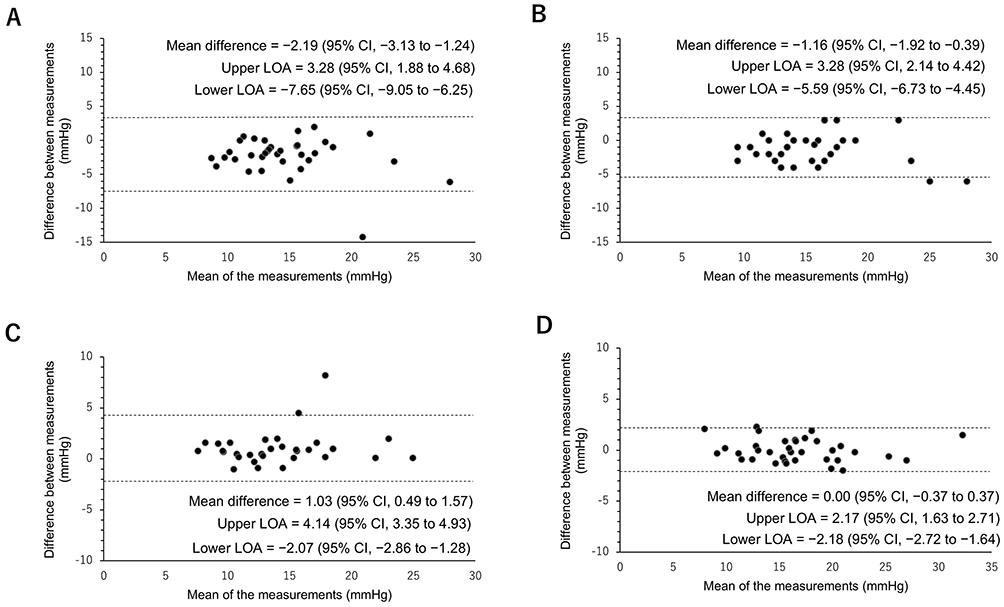 |
Figure 1 Bland–Altman plots for the between-methods comparisons. (A) GAT and iCare IC200 in sitting position. (B) GAT and iCare HOME2 in sitting position. (C) iCare IC200 and iCare HOME2 in sitting position. (D) iCare IC200 and iCare HOME2 in supine position. The upper and lower limits of agreement are indicated with dotted lines above and below the x-axis, respectively. No significant correlation exists between the corresponding IOP difference and mean IOP in any Bland–Altman plot. |
No significant correlation was found between any demographic parameter (age, SE, CCT, CH, MD, cpRNFL thickness, diastolic and systolic blood pressure, pulse rate and glaucoma eye drop score) and the difference of iCare IC200 tonometry and iCare HOME2 self-tonometry results, in any position (P ≥ 0.084). Similarly, no significant correlation was found between the demographic parameters and the sitting IOP difference of GAT and iCare HOME2 self-tonometry (P ≥ 0.156). For all but one demographic parameter, a similar lack of correlation was seen regarding the sitting IOP difference of GAT and iCare IC200 tonometry (P ≥ 0.170), but for CH a significant negative relationship was found (r = −0.411, P = 0.013) showing that the between-methods difference decreases with increasing viscoelastic damping capacity of the cornea.20
The absolute individual IOP differences between iCare IC200 tonometry and iCare HOME 2 self-tonometry were similar in both sitting (median: 0.900, IQR, 1.05) and supine positions (median: 0.900, IQR, 0.980; P = 0.362).
Discussion
In the current cross-sectional study, iCare HOME2 self-tonometry was investigated for its agreement with operator conducted iCare IC200 tonometry in both sitting and supine positions on Japanese POAG and NTG patients. The clinical importance of our study design is explained by the unmet need of reliable HOME tonometry, HOME self-tonometry and in particular HOME self-tonometry in supine position. While office time sitting IOP measurements are reliably made using GAT, which was also included in the current study, sitting and supine self-tonometry are still not routinely included in glaucoma diagnostics, and have not yet received a role in IOP measurement during long-term glaucoma care. Since IOP can considerably fluctuate over day and night, and supine IOP is higher than sitting IOP, the missing information pieces may negatively influence the early detection of IOP spikes in glaucoma eyes under topical medication, and may cause a delay in the detection of IOP related risk factors of future structural progression and functional deterioration.
In the past decades several devices were developed for HOME tonometry,3,21,22 but none of them gained a wide clinical acceptance due to their technical limitations. The first version of the iCare HOME self-tonometer provided reliable IOP measurements only in sitting position, and the measured IOP values were not displayed for the patients. The measurement results had to be downloaded separately by clinicians.23,24
The iCare HOME2 device, which is a recent development and offers an easy-to-use IOP measurement with a light and small instrument without the need of topical anaesthesia, may potentially fill the gap in HOME tonometry. The few previous publications report on an acceptable agreement with GAT in the sitting position,8,11–13 which was confirmed in our current investigation with the 1.2 mmHg mean between-device IOP difference in sitting position and the corresponding 0.844 ICC value. Although our current results are comparable with the previous reports, our LOA ranged from −2.07 to 4.14 mmHg, which may not be fully satisfactory for clinical use in NTG patients. In addition, the mean IOP difference between GAT and iCare IC200 in the sitting position was relatively large (2.2 mmHg) in our study. However, Sachdeva et al16 also reported a 2.2 mmHg mean difference between their GAT and iCare IC200 IOP results, while Nakakura et al23 reported an even higher (3.0 mmHg) mean difference. Thus, our current results may more reflect to a general clinical problem than a poor technical performance of the current investigators. Compared to the ICC between the GAT and iCare HOME2 results in the sitting position, the ICC between GAT and iCare IC200 was lower. This may be due to the positioning differences of the two iCare devices: during IOP measurement, the iCare HOME2 device contacts both the forehead and cheek at two points, whereas the iCare IC200 contacts only the forehead at a single point. Therefore, the iCare HOME2 device may be less susceptible to hand movements or instability than the iCare IC200 instrument.
However, the primary goal of our investigation was to clarify the agreement of iCare IC200 tonometry and iCare HOME2 self-tonometry in sitting and supine body positions, respectively, on POAG and NTG patients, who received one single training session prior to self-tonometry. As shown in the inclusion criteria and Table 1 the central visual functions of the study eyes were sufficient to optimally positioning the device probe, even if the mean 24-degree VF deterioration ranged between the early and advanced damage categories. While a recent investigation compared the sitting IOP measurement results obtained with iCare IC200 tonometry and iCare self-tonometry, and found a 0.92 mmHg mean between-methods difference,12 to our knowledge no similar comparisons were published for the supine body position IOP values. In our current investigation, the mean sitting IOP was 1.0 mmHg higher with iCare HOME2 self-tonometry than iCare IC200 tonometry. Thus, our mean difference is similar to the previously published mean difference.12 Interestingly, however, in our study the iCare HOME 2 values were higher, while in the previous publication the iCare IC200 tonometry values were greater.12 In our current investigation, the difference between the sitting iCare IC200 and iCare HOME2 IOP values was statistically significant. However, the 1 mmHg between-methods difference does not seem to be clinically significant, and the correlation between the sitting iCare IC200 tonometry and iCare HOME 2 self-tonometry values was good (ICC: 0.899).
No technical problem, subjective complaints or ocular injuries occurred during the self-tonometry session. When the supine IOP results were compared between iCare IC200 tonometry and iCare HOME2 self-tonometry, we found no difference between the methods (mean difference: 0.0 mmHg, ICC = 0.976). This result suggests that the supine body position does not represent an obstacle against accurate IOP self-measurements with the iCare HOME 2 device for trained POAG and NTG patients. One possible explanation for the better agreement observed in the supine position compared with the sitting position is that during supine measurements the head is supported by the bed, which may reduce head movement and allow more stable IOP measurements.
Since no proportional bias was found between the corresponding between-methods mean IOP values and between-methods IOP difference values in any of the between-method comparisons (Figure 1), our results show a clinically satisfactory agreement in the tested 10 to 31 sitting GAT IOP range, for all comparisons.
It is also of clinical importance that no significant relationship was found between any demographic parameter (age, SE, CCT, CH, MD, cpRNFL thickness, diastolic and systolic blood pressure, pulse rate and glaucoma eye drop score) and the between-iCare devices IOP differences. While no correlation was observed between CH and the GAT–sitting iCare HOME2 IOP difference, we found a significant negative correlation between CH and the GAT– sitting iCare IC200 IOP difference. This is similar to the results of an earlier investigation in which a negative correlation between CH and the IOP difference between GAT and the first-generation iCare HOME tonometer was found.25 It has been shown that lower CH is associated with a greater discrepancy between GAT and sitting iCare measurement results: IOP measured with GAT is more strongly influenced by CH than IOP measured with iCare HOME tonometry.25 This suggests that iCare devices are less affected by low CH than GAT, which gains a special importance in patients with low CH. Since in NTG corneal rigidity is lower than in normal subjects and high-tension glaucoma patients,26 and our patient population (similarly to the general population in Japan) contained several NTG patients, our results underline the influence of IOP measurement method on the results. In contrast to our results, in a previous investigation a significant negative correlation was found between CCT and both the GAT−iCare IC200 tonometry and the GAT−iCare HOME2 self-tonometry differences.12 In that study, however, the CCT range was unusually large (445 to 710 µm), while in our investigation it represented a more typical CCT range (447 to 601 µm).
Our study has limitations. First of all, several glaucoma patients suffer from complex conditions (eg advanced cataract, severe central visual function deterioration, mental conditions or early postoperative status) which do not make self-tonometry possible. For them, our study does not provide clinical benefits. The investigation was made on Japanese POAG and NTG eyes, therefore our results may not be automatically applied to other ethnic populations. At the same time, this is a strength of the study since according to our knowledge no previous investigations with iCare HOME2 self-tonometry were conducted on Asian eyes. Due to our study design, the eyes were topically anaesthetized when both the sitting and the supine iCare HOME2 self-tonometry measurements were made. More than three decades ago one of the current authors has shown that topical anaesthesia leads to a decreased IOP difference from the GAT values, when the Expert Advanced Logic Pneumotonometer is used.27 The difference was attributed to the ocular surface inconvenience caused by the air-puff effect, which was eliminated when topical anaesthesia was used before the IOP measurements. In the current investigation, however, we used a deceleration-based instrument family, which causes no ocular surface/corneal inconvenience. Therefore, we do not think that the topical anaesthesia used before the GAT measurements had any clinically significant effect on the iCare HOME2 self-measurements at ten to twenty minutes after the oxybuprocaine instillation. Since iCare HOME2 self-measurement in the supine position was performed last among the IOP measurements, the better agreement may also have been influenced by a learning effect. Finally, our study design allowed only an approximation of the clinically relevant use of the iCare HOME2 self-tonometer, since the participants performed the test during the day in a supervised manner in a clinical setting and not in their homes, and their technical performance could be better under the above conditions than in the targeted home situation at waking up from sleep during the night.
Conclusion
The current cross-sectional investigation showed that the agreement between GAT, iCare IC200 tonometry and iCare HOME2 self-tonometry is good in sitting position, and it is excellent between iCare IC200 tonometry and iCare HOME2 self-tonometry in supine position. In the 10 to 31 mmHg IOP range, no proportional bias was found, and we did not find any significant correlation between the participants’ and study eyes’ demographic parameters and the between iCare-methods differences. The patient education and training session was short and effective, and no technical problems appeared during the self-tonometry sessions. Even if the current results were not obtained from nighttime unsupervised self-tonometry performed in the patients’ homes, our results suggest that iCare HOME2 self-tonometry may potentially be applied by trained glaucoma patients for home tonometry and nighttime supine self-tonometry and may potentially support clinical decision making in long-term glaucoma management.
Data Sharing Statement
The datasets analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The Kyorin University Institutional Review Board for Human Research approved the study protocol, and the study was conducted according to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all participants before the measurements.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Sho Nakamura reports personal fees from Santen Pharmaceutical Co., Ltd., outside the submitted work. Gábor Hollό reports personal fees for consulting from Thea Laboratoires and personal fees for consulting and honorarias for lectures, presentations, speakers bureaus, manuscript writing or educational events from Santen Pharmaceutical Co., Ltd., outside the submitted work. Tomoka Ishida reports personal fees from Chugai Pharmaceutical Co., Ltd., Santen Pharmaceutical Co., Ltd., Alcon Japan Ltd., and Senju Pharmaceutical Co., Ltd., outside the submitted work. The remaining authors report no conflicts of interest in this work.
References
1. Liang SY, Lee GA, Shields D. Self-tonometry in glaucoma management--past, present and future. Surv Ophthalmol. 2009;54(4):450–9. doi:10.1016/j.survophthal.2009.04.006
2. Pazos M, Traverso CE, Viswanathan A. European glaucoma society - terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1–212. doi:10.1136/bjophthalmol-2025-egsguidelines
3. Kóthy P, Vargha P, Holló G. Ocuton-S self tonometry vs. Goldmann tonometry; a diurnal comparison study. Acta Ophthalmol Scand. 2001;79(3):294–297. doi:10.1034/j.1600-0420.2001.790317.x
4. Quérat L, Chen E. Impact of self-tonometry on glaucoma treatment decision. Acta Ophthalmol. 2023;101(2):e246–e251. doi:10.1111/aos.15256
5. Najmanová E, Pluháček F, Haklová M. Intraocular pressure response affected by changing of sitting and supine positions. Acta Ophthalmol. 2020;98(3):e368–e372. doi:10.1111/aos.14267
6. Moon Y, Lee JY, Jeong DW, Kim S, Han S, Kook MS. Relationship between nocturnal intraocular pressure elevation and diurnal intraocular pressure level in normal-tension glaucoma patients. Invest Ophthalmol Vis Sci. 2015;56(9):5271–5279. doi:10.1167/iovs.15-17062
7. Kiuchi T, Motoyama Y, Oshika T. Relationship of progression of visual field damage to postural changes in intraocular pressure in patients with normal-tension glaucoma. Ophthalmology. 2006;113(12):2150–2155. doi:10.1016/j.ophtha.2006.06.014
8. Quérat L, Chen E. Self-monitoring of the intraocular pressure with iCARE® HOME2 and a smartphone application: feasibility and acceptability. Acta Ophthalmol. 2025;103(1):109–114. doi:10.1111/aos.16789
9. Sabharwal J, Tharp M, Hamilton N, et al. Remote tonometry identifies significant variability in the timing of IOP response to topical medication change. Ophthalmol Glaucoma. 2026. doi:10.1016/j.ogla.2026.05.007
10. iCare Finland Oy. iCare HOME2 instruction manual; Vantaa, Finland. Available from: iCare-HOME2_Instruction_Manual_TA023-078-EN-3.0-low.pdf.
11. Kratz A, Zbidat R, Kishner R, Cohen M, Shalata W, Goldberg I. Assessment of the iCare HOME2, a new intraocular pressure self-measurement tonometer. J Glaucoma. 2023;32(11):926–929. doi:10.1097/IJG.0000000000002298
12. Romano D, Montesano G, Aminoleslami AA, Colizzi B, Rossetti LM. Reliability of self-monitoring of intraocular pressure with iCare HOME2 rebound tonometry. J Glaucoma. 2025;34(6):447–454. doi:10.1097/IJG.0000000000002560
13. Kuo DS, Rahimy E. Agreement of serial iCare HOME2 and goldmann applanation tonometry. Ophthalmol Glaucoma. 2024;7(5):440–444. doi:10.1016/j.ogla.2024.04.007
14. Rajagopal S, Singh SB, Abhijith JN, Singh RB, Bejan Singh SM. Agreement between rebound (iCare IC200), Goldmann applanation tonometer, and noncontact (air puff) tonometer in the immediate postoperative period following vitrectomy. Indian J Ophthalmol. 2025;73(9):1269–1275. doi:10.4103/IJO.IJO_180_25
15. Badakere SV, Chary R, Choudhari NS, Rao HL, Garudadri C, Senthil S. Agreement of intraocular pressure measurement of iCare IC200 with Goldmann applanation tonometer in adult eyes with normal cornea. Ophthalmol Glaucoma. 2021;4(1):89–94. doi:10.1016/j.ogla.2020.08.004
16. Sachdeva R, Iordanous Y, Lin T. Comparison of intraocular pressure measured by iCare tonometers and Goldmann applanation tonometer. Can J Ophthalmol. 2023;58(5):426–432. doi:10.1016/j.jcjo.2022.06.002
17. Kiuchi Y, Inoue T, Shoji N, Nakamura M, Tanito M. Glaucoma guideline preparation committee, Japan glaucoma society. the Japan glaucoma society guidelines for glaucoma 5th edition. Jpn J Ophthalmol. 2023;67:189–254. doi:10.1007/s10384-022-00970-9
18. iCare Finland Oy. iCare IC200 instruction manual; Vantaa, Finland. Available from: iCare_IC200_instruction_manual_TA031-046-EN-5.0.pdf.
19. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. doi:10.1016/j.jcm.2016.02.012
20. Medeiros FA, Meira-Freitas D, Lisboa R, Kuang TM, Zangwill LM, Weinreb RN. Corneal hysteresis as a risk factor for glaucoma progression: a prospective longitudinal study. Ophthalmology. 2013;120(8):1533–1540. doi:10.1016/j.ophtha.2013.01.032
21. Halkiadakis I, Stratos A, Stergiopoulos G, et al. Evaluation of the iCare-ONE rebound tonometer as a self-measuring intraocular pressure device in normal subjects. Graefes Arch Clin Exp Ophthalmol. 2012;250(8):1207–1211. doi:10.1007/s00417-011-1875-6
22. Dunbar GE, Shen BY, Aref AA. The Sensimed Triggerfish contact lens sensor: efficacy, safety, and patient perspectives. Clin Ophthalmol. 2017;11:875–882. doi:10.2147/OPTH.S109708
23. Nakakura S. iCare® rebound tonometers: review of their characteristics and ease of use. Clin Ophthalmol. 2018;12:1245–1253. doi:10.2147/OPTH.S163092
24. Pons-Talaya C, Pons-Talaya A, Widmer J, et al. Effectiveness and accuracy of iCare HOME tonometer in glaucoma patients: a systematic review. Am J Ophthalmol. 2026;282:69–81. doi:10.1016/j.ajo.2025.10.008
25. Brown L, Foulsham W, Pronin S, Tatham AJ. The influence of corneal biomechanical properties on intraocular pressure measurements using a rebound self-tonometer. J Glaucoma. 2018;27(6):511–518. doi:10.1097/IJG.0000000000000948
26. Xu Y, Ye Y, Chen Z, et al. Corneal stiffness and modulus of normal-tension glaucoma in Chinese. Am J Ophthal. 2022;242:131–138. doi:10.1016/j.ajo.2022.06.014
27. Holló G, Follmann P, Pap G. A clinical evaluation of XPERT NCT (Reichert) for glaucoma screening by optometrists. Int Ophthalmol. 1992;16(4–5):291–293. doi:10.1007/BF00917978
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Patient Tolerability of Omidenepag Isopropyl in the Treatment of Glaucoma and Ocular Hypertension
Matsuo M, Matsuoka Y, Tanito M
Clinical Ophthalmology 2022, 16:1261-1279
Published Date: 26 April 2022
Retrospective Analysis of Switching Bimatoprost 0.01% to Bimatoprost 0.03% in Patients with Various Types of Glaucoma and Ocular Hypertension
Xu KM, Cho R, Chan TYB
Clinical Ophthalmology 2022, 16:2385-2390
Published Date: 29 July 2022
Multicenter Effectiveness and Disease Stability Through 3 Years After iStentTrabecular Micro-Bypass with Phacoemulsification in Glaucoma and Ocular Hypertension
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW
Clinical Ophthalmology 2022, 16:2955-2968
Published Date: 1 September 2022
Triple Fixed-Combination Bimatoprost/Brimonidine/Timolol in Glaucoma and Ocular Hypertension in India: A Multicenter, Open-Label, Phase 3 Study
Menon MG, Goodkin ML
Clinical Ophthalmology 2022, 16:3559-3569
Published Date: 20 October 2022
Trabeculectomy Vs Non‐penetrating Deep Sclerectomy for the Surgical Treatment of Open-Angle Glaucoma: A Long-Term Report of 201 Eyes
Correia Barbosa R, Gonçalves R, Bastos R, Alves Pereira S, Basto R, Viana AR, Tenedório P
Clinical Ophthalmology 2023, 17:1619-1627
Published Date: 6 June 2023