Back to Journals » Clinical Ophthalmology » Volume 17
Trabeculectomy Vs Non‐penetrating Deep Sclerectomy for the Surgical Treatment of Open-Angle Glaucoma: A Long-Term Report of 201 Eyes
Authors Correia Barbosa R ![]() , Gonçalves R, Bastos R, Alves Pereira S, Basto R, Viana AR, Tenedório P
, Gonçalves R, Bastos R, Alves Pereira S, Basto R, Viana AR, Tenedório P
Received 12 February 2023
Accepted for publication 17 March 2023
Published 6 June 2023 Volume 2023:17 Pages 1619—1627
DOI https://doi.org/10.2147/OPTH.S405837
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Renato Correia Barbosa, Rita Gonçalves, Ricardo Bastos, Sara Alves Pereira, Rita Basto, Ana Rita Viana, Paula Tenedório
Ophthalmology Department, Hospital Pedro Hispano, Unidade Local de Saúde de Matosinhos, Matosinhos, Portugal
Correspondence: Renato Correia Barbosa, Hospital Pedro Hispano, Unidade Local de Saúde de Matosinhos, Rua Dr. Eduardo Torres, Matosinhos, 4464-513, Portugal, Email [email protected]
Introduction: Glaucoma is the second leading cause of vision loss worldwide. The reduction of intraocular pressure remains the backbone of its therapy. Among surgical techniques for its treatment, deep non-penetrating sclerotomy is the most widely practiced non-penetrating surgery. The purpose of this study was to evaluate the long-term efficacy and safety of deep non-penetrating sclerotomy compared to standard trabeculectomy in patients with open-angle glaucoma.
Patients and methods: Retrospective study including 201 eyes with open-angle glaucoma. Closed-angle and neovascular cases were excluded. Absolute success was considered when intraocular pressure under 18 mmHg, or a reduction of at least 20% in patients with a baseline intraocular pressure below 22 mmHg, was obtained after 24 months, without the use of medication. Qualified success was considered when those targets were met with or without the use of hypotensive medication.
Results: Deep non-penetrating sclerectomy showed a slightly lower long-term hypotensive effect compared to standard trabeculectomy, with significant differences at 12 months, but not at 24 months of follow-up. The absolute and qualified success rates were 51.85% and 65.43% for the trabeculectomy group and 50.83% and 60.83% for the deep non-penetrating sclerectomy, without significant differences. Regarding postoperative complications, mainly due to postoperative hypotonia, or related to the filtration bleb, they were significantly different between groups, with 10.8% and 24.7%, in deep-nonpenetrating sclerectomy and trabeculectomy groups, respectively.
Conclusion: Deep non-penetrating sclerectomy seems to be an effective and safe surgical option for patients with open-angle glaucoma unable to be controlled by non-invasive strategies. Data suggests that the intraocular pressure-lowering effect of this technique may be marginally lower than that of trabeculectomy, but the achieved efficacy outcomes were similar, with a significantly lower risk of complications.
Keywords: glaucoma, intraocular pressure, filtering surgery, trabeculectomy
Introduction
Glaucoma is the second leading cause of vision loss worldwide,1 and its prevalence is increasing with the global aging population. Projections predict that by 2040, approximately 112 million patients will be diagnosed with glaucoma, disproportionally affecting people residing in Asia and Africa.2 The risk and subtypes of glaucoma vary among races and countries, with primary open-angle glaucoma (POAG) being more prevalent in individuals of African descent than Caucasians.2
The reduction of intraocular pressure (IOP) remains the backbone of glaucoma therapy. While in many cases medical and LASER techniques provide a reliable, long-term IOP control, surgery is advisable when optimum medical/LASER therapy fails to sufficiently lower IOP, or there is evidence that the patient cannot comply with those therapeutic strategies.3
Trabeculectomy (TB) is considered the standard penetrating surgical procedure for the treatment of glaucoma and has been widely used for over 50 years. IOP is lowered by creating a fistula between the inner compartments of the eye and subconjunctival space, requiring full-thickness penetration of the anterior chamber, under a partial thickness scleral flap.4 This alternative path allows aqueous humor to accumulate under the conjunctiva and form a filtering bleb.5 The fistula is covered by a scleral flap that provides some resistance to the outflow, preventing profound hypotony. However, it is often associated with the development of important postoperative complications attributable to excessive aqueous humour filtration.6
Non-penetrating surgical techniques for glaucoma have been developed to improve the safety of conventional filtering procedures. Deep non-penetrating sclerectomy (DNPS) is the most widely practiced technique and is often associated with a hydrophilic implant under the scleral flap to improve aqueous humour filtration. It prevents the sudden hypotony that occurs after penetrating surgery by creating progressive filtration of aqueous humour without perforating the eye through the preservation of the thin trabeculo-Descemet membrane. Nevertheless, it is technically hard, with a long learning curve, and many authors argue that it is less effective than TB for intraocular pressure reduction on a medium and long-term basis.7–13
To date, only a few studies have directly compared TB and DNPS regarding which technique provides the best results in terms of efficacy and safety,14 and most of them are outdated, have relatively small samples, and do not consider the modern surgical technique, with the use of intrascleral implants and augmentation with antimetabolites.15–20
The purpose of this study was to evaluate the long-term efficacy and safety of DNPS compared to standard TB in patients with open-angle glaucoma.
Methods
A retrospective study was conducted, including 201 eyes that underwent glaucoma surgery in Hospital Pedro Hispano – Unidade Local de Saúde de Matosinhos between January 2012 and August 2019.
Data included patients diagnosed with open-angle glaucoma, regardless of age, race, or sex. The diagnosis was defined based on: typical optic disc damage, with glaucomatous cupping and loss of neuroretinal rim; visual field defects compatible with glaucomatous optic neuropathy; open-angle objectified by gonioscopy. Cases of pseudoexfoliation glaucoma (PEXG) and pigmentary glaucoma (PG) were considered eligible. Patients diagnosed with closed-angle or neovascular glaucoma were excluded.
Considered interventions were TB and DNPS, with or without intraoperative antimetabolite augmentation. DNPS was always done with the implantation of an intrascleral implant, whether Aquaflow® or Esnoper®.
Patient data were collected preoperatively and 1 week, 1, 6, 12, and 24 months after the procedure, regarding IOP, measured by applanation tonometry, visual acuity (VA), hypotensive medication, and postoperative complications.
The adopted outcome measures, reported after the follow-up period of 2 years, consisted of absolute success, when IOPs below 18 mmHg were reached or, when the baseline IOP was ≤ 21 mmHg, a reduction of at least 20% was obtained, without the usage of hypotensive medication. Qualified success was considered when IOPs below 18 mmHg or, when the baseline IOP was ≤ 21 mmHg, a reduction of at least 20% was obtained with or without medication.
This work was carried out with the agreement of the ethics committee of Hospital Pedro Hispano. Informed consent was obtained from the study participants, and the guidelines outlined in the Declaration of Helsinki were followed.
Statistical analysis was conducted using Statistical Package for the Social Sciences (SPSS) version 23.0 for Macintosh. The assumption of normality of distribution and homogeneity of variance were tested by the Kolmogorov–Smirnov test. When these assumptions were verified, a t-test for paired/independent samples was used. When those assumptions were not proved, the Mann–Whitney test for independent samples was used. Statistical significance was defined as p < 0.05.
Results
A total of 201 eyes were included in this study. Table 1 shows the demographics and characteristics of the patients included in this study, with 48.8% of the patients being male and 51.2% being female. The mean age of the patients was 71.1 ± 9.38 years old. Primary open-angle glaucoma (POAG) was responsible for 63.2% of the cases, while PEXG accounted for 34.8% and PG for 2%. Regarding the surgical technique, TB was performed in 40.3% (n=81) and DNPS in 59.7% (n=120). Both techniques were performed combined with cataract surgery in most cases: 74.1% in TB and 79.2% in DNPS groups. Surgeries were augmented with the use of mitomycin C in 66.2% of the cases, 58% in the TB group, and 71.7% in the DNPS group, with a significant difference between groups (p=0.045). In the TB group, 56.8% of the patients had GPAA, 40.7% had GPEX and 2.5% had PG. In the DNPS, 67.5% had GPAA, 30.1% had GPEX and 1.7% had PG, without significant differences between groups regarding the number of patients with GPAA and GPEX (p=0.134). Before surgery, the average number of hypotensive drops taken by the patients was 2.41 ± 1.15, 2.53 ± 1.11 in the TB group, and 2.32 ± 1.18 in the DNPS group, without significant differences between groups (p=0.204).
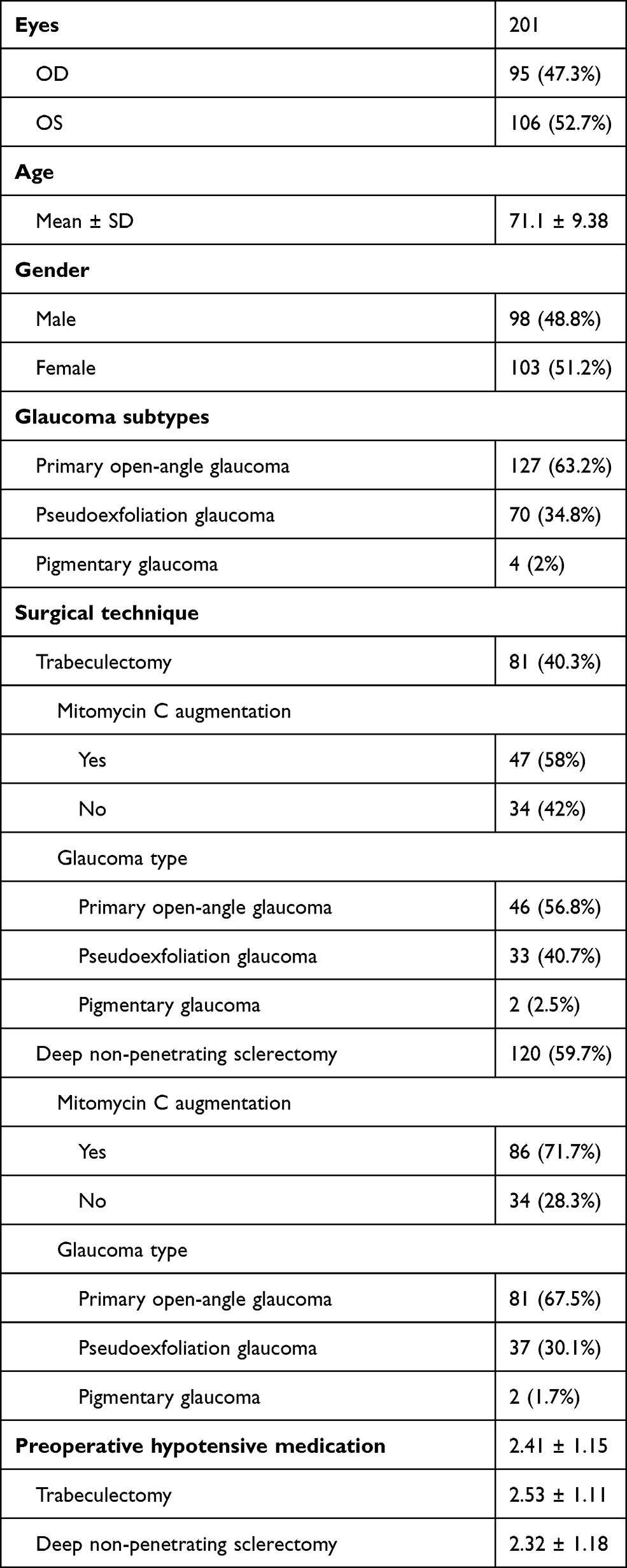 |
Table 1 Demographics and Characteristics of the Study Sample |
As shown in Figure 1, mean IOP values, measured in mmHg, of the trabeculectomy group before, 1 week after, 1, 6, 12, and 24 months after were, respectively, 25.27 ± 10.04; 9.64 ± 4.96; 12.84 ± 4.44; 12.51 ± 4.48; 13.33 ± 4.48; 15.1 ± 5.45. In the DNPS group, these values were 22.01 ± 8.66; 12.11 ± 6.24; 12.35 ± 3.91; 12.86 ± 3.95; 12.87 ± 4.17; 13.64 ± 3.93. The baseline values were statistically significant between groups (p=0.006). There were no statistically significant differences in mean IOP values after 1, 6, 12, or 24 months. Mean IOP reduction achieved was −10.17mmHg in the eyes who underwent TB and −8.37mmHg in the eyes who did DNPS.
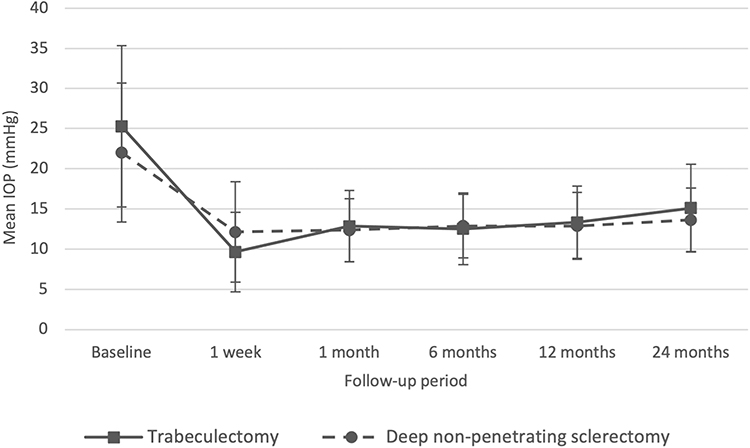 |
Figure 1 IOP values before and after surgery. |
Table 2 shows the IOP outcome differences between several subgroups. Comparing the effects of mitomycin C augmentation in each surgical technique, the TB group showed the mean IOP values at 1 week and 1, 6, 12, or 24 months after the surgery of 10.24 ± 5.35; 12.76 ± 3.33; 12.53 ± 2.95; 13.19 ± 3.29; 14.82 ± 3.18 and 9.20 ± 4.67; 13.17 ± 4.79; 13.02 ± 4.52; 14.00 ± 4.40; 15.30 ± 6.65, without and with the use of mitomycin C, respectively, without statistically significant differences between groups in any of the measurements. In the DNPS group, the IOP values were 12.42 ± 4.05; 11.72 ± 3.33; 13.03 ± 2.61; 14.13 ± 2.74; 14.67 ± 1.97 and 12.00 ± 6.88; 12.58 ± 4.10; 13.09 ± 3.91; 13.18 ± 3.39; 13.82 ± 3.34, without and with the use of mitomycin C, respectively, with a slight tendency to lower IOP values with mitomycin C augmentation, but without statistically significant differences between groups in any of the measurements.
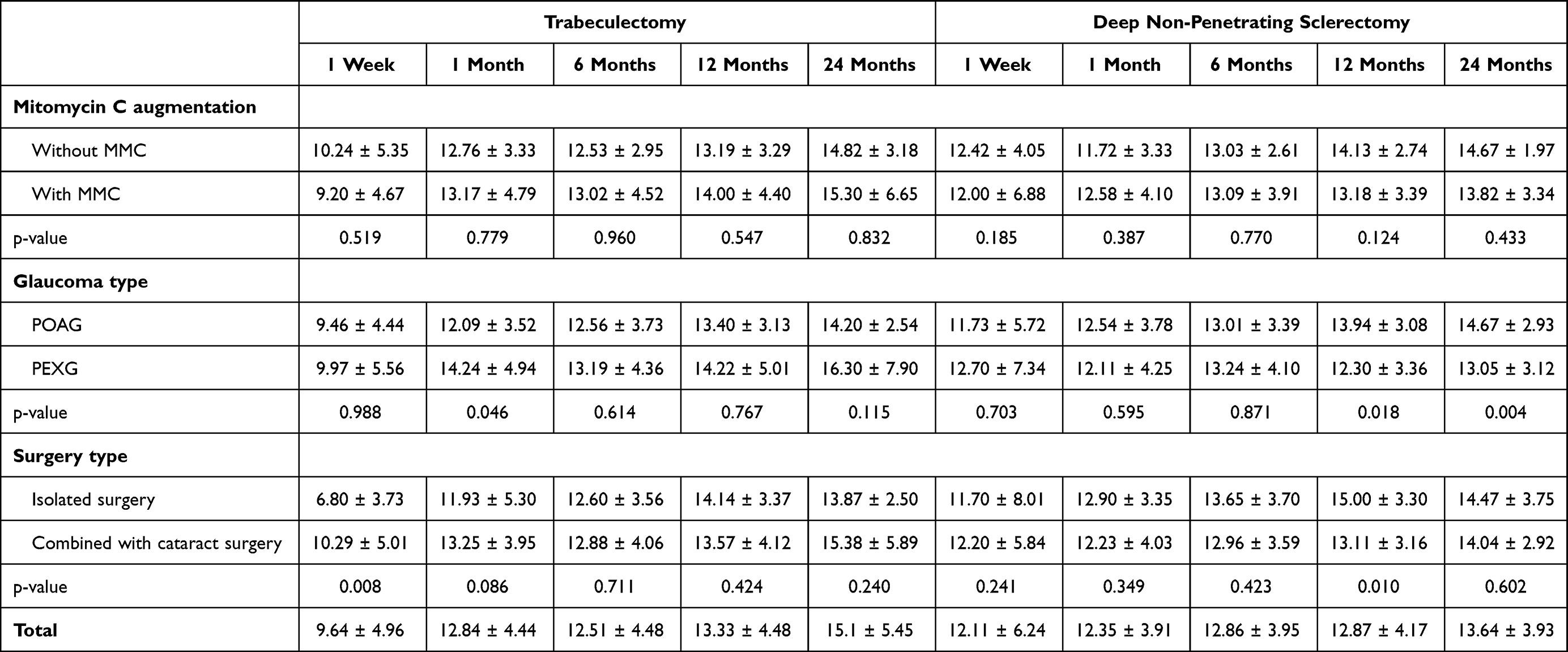 |
Table 2 IOP Values After Surgery Between the Different Subgroups (Mean ± SD, mmHg) |
Regarding the differences in IOP between glaucoma types, with each of the surgeries, in the TB group, postoperative values 1 week and 1, 6, 12, or 24 months after the surgery were 9.46 ± 4.44; 12.09 ± 3.52; 12.56 ± 3.73; 13.40 ± 3.13; 14.2 ± 2.54 and 9.97 ± 5.65; 14.24 ± 4.94; 13.19 ± 4.36; 14.22 ± 5.01; 16.30 ± 7.90, in the POAG and PEXG subgroups, respectively. The values showed a tendency towards higher IOP values in the PEXG group, but statistical differences were only noted in the measurement 1 month after the surgery (p=0.046). In the DNPS, the values were 11.73 ± 5.72; 12.54 ± 3.78; 13.01 ± 3.39; 13.94 ± 3.08; 14.67 ± 2.93, and 12.70 ± 7.34; 12.11 ± 4.25; 13.24 ± 4.10; 12.30 ± 3.36; 13.05 ± 3.12, in the POAG and PEXG subgroups, respectively, with statistically significant differences in the 12 months (p= 0.018) and 24 months (p=0.004) groups. A direct comparison between the two surgical techniques, regarding the outcome in each of the glaucoma types, showed a similar IOP in the POAG patients, with significant differences found in only the 1-week measurement values (p=0.025). In the PEXG group, values were also similar, with significant differences found in the 24 months measurement (p=0.015). Comparing isolated glaucoma surgery with combined cataract surgery, the TB group had values of 1 week and 1, 6, 12, or 24 months after the surgery of 6.80 ± 3.73; 11.93 ± 5.30; 12.60 ± 3.56; 14.14 ± 3.37; 13.87 ± 2.50 and 10.29 ± 5.01; 13.25 ± 3.95; 12.88 ± 4.06; 13.57 ± 4.12; 15.38 ± 5.89, in the isolated glaucoma surgery and combined surgery subgroups, respectively, with significant differences found only in the measurement taken after 1 week (p=0.008). In the DNPS group, the IOL values were 11.70 ± 8.01; 12.90 ± 3.35; 13.65 ± 3.70; 15.00 ± 3.30; 14.47 ± 3.75 and 12.20 ± 5.84; 12.23 ± 4.03 ± 12.96 ± 3.59 ± 13.11 ± 3.16 ± 14.04 ± 2.92 in the isolated glaucoma surgery and combined surgery subgroups, respectively, with significant differences found only in the measurement taken after 12 months.
The raw mean IOP reduction, calculated based on the measurements 6, 12, and 24 months after the surgeries was 41.16%; 39.12%; 34.07%, and 35.76%; 31.11%; 27.45% in the TB and DNPS groups, respectively, with a trend towards a higher reduction in the TB group, with significant values in the 12 months measurement (p=0.052; p=0.016; p=0.053).
Absolute success was achieved in 51.85% and 50.83% of the TB and DNPS groups, respectively, without significant differences between groups (p=0.887). Relative success was achieved in 65.43% and 60.83% of the TB and DNPS groups, respectively, also without significant differences between groups (p=0.508) (Figure 2).
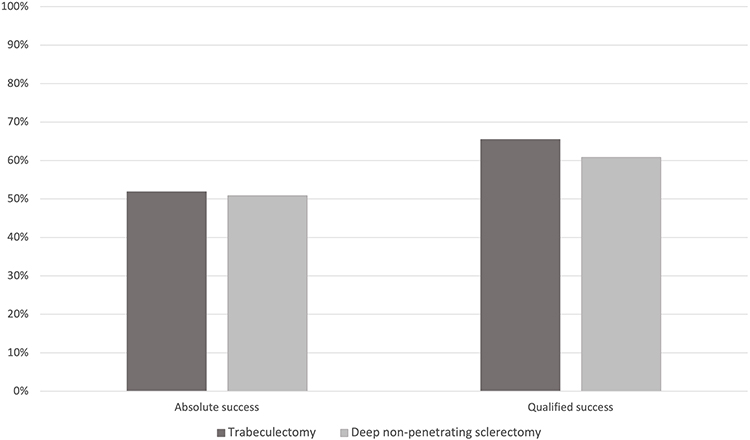 |
Figure 2 Success rates 24 months after surgery. |
Mean values of best-corrected visual acuity [BCVA] before and 2 years after each procedure were 0.63 and 0.75, in the TB group. These values were 0.7 and 0.78 in the DNPS group. The average VA difference was 1.2 lines in the TB group (p=0.002), and 0.8 lines in the DNPS group (p<0.001). Differences in VA improvement between TB and DNPS groups were not statistically significant.
Regarding postoperative complications, as shown in Table 3, they were registered in 24.7% (n=20) of the eyes that underwent TB and 10.8% (n=13) of the eyes that did DNPS, with a significant difference between groups (p=0.007). The most serious complications were observed in the TB group, with 1 case of severe hyphema, 1 case of malignant glaucoma, and 1 case of choroidal detachment in the immediate postoperative period.
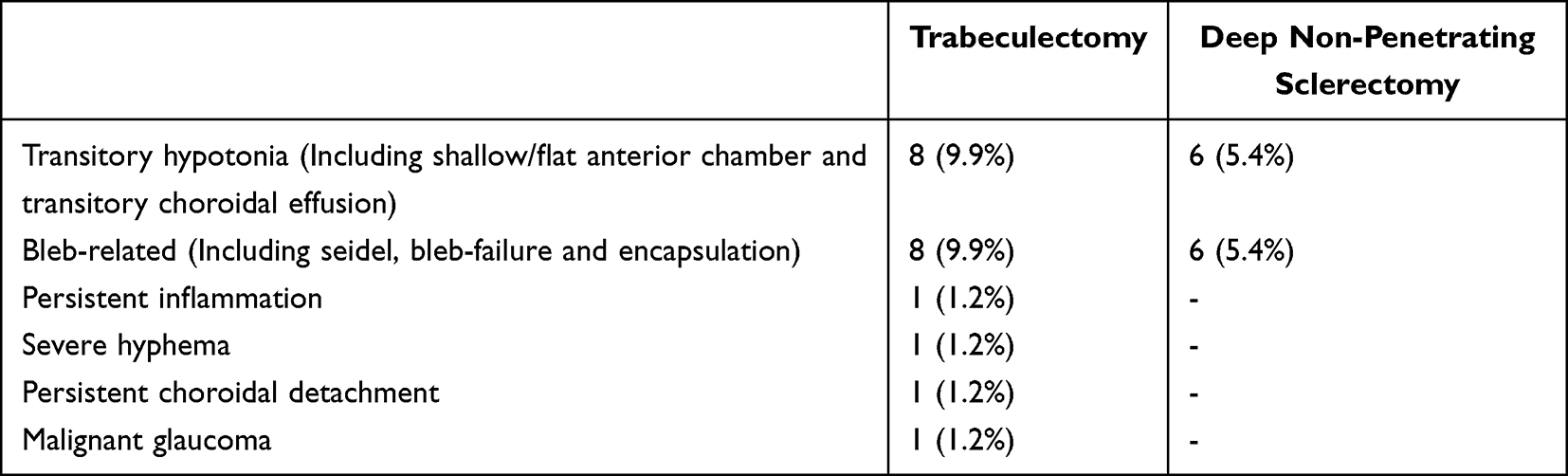 |
Table 3 Postoperative Complications |
The average number of hypotensive medications taken by the patients, reduced from 2.53 to 0.52 in the TB group, and 2.32 to 0.41 in the DNPS group, after 2 years of follow-up, without significant differences between groups at baseline (p=0.204) or after 2 years (p=0.609) (Figure 3).
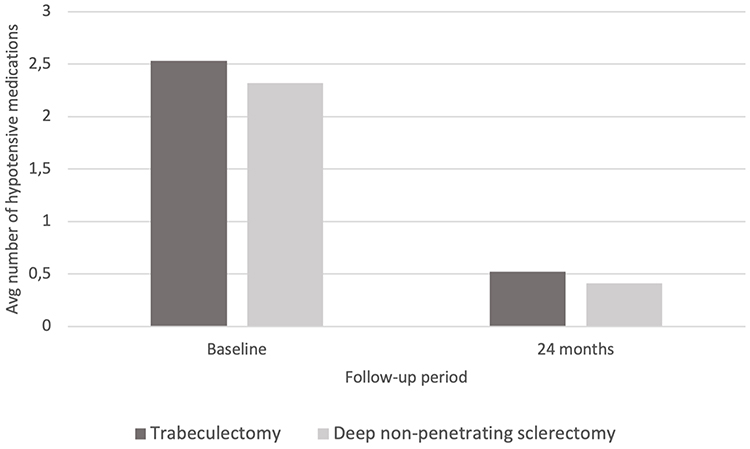 |
Figure 3 Average number of hypotensive medications taken before and after surgery. |
Discussion and Conclusion
According to our results, DNPS showed a slightly lower long-term hypotensive effect, while compared to TB. The differences in raw mean percentage IOP reduction were significantly higher for the TB group in the measurements taken 12 months after the surgery (p=0.016) but did not reach statistical significance in the measurements taken 6 and 24 months after the procedure (p=0.052; p=0.053). The absolute and qualified success rates of 51.85% and 65.43% for the TB and 50.83% and 60.83% for the DNPS groups again showed a slight difference between techniques but did not reach statistical significance (p=0.887; p=0.508). Across the literature, conclusions about the efficacy of both types of surgeries are variable. Some authors suggest that TB leads to a greater decrease in IOP. Rulli E, et al, in a metanalysis published in 2012, involving 18 studies and 945 eyes, concluded that penetrating surgery had a slightly higher, but significant, IOP-lowering effect after a follow-up of 1 year, which was considered potentially relevant in patients requiring a greater IOP reduction.14 On the other hand, Leszczyński and colleagues, in a study involving 78 eyes, found no significant differences regarding the efficacy of both types of surgical techniques, during a 24-month follow-up period.20 These findings were also corroborated by Sayyad, et al, in a 78 eyes study, where each patient required bilateral glaucoma surgery and underwent TB in one eye and DNPS in the other.19 Russo et al, showed, in a sample of 93 eyes, similar IOP-lowering effects, when DNPS was augmented with mitomycin C and SK-GEL scleral implant.15
Two randomized clinical trials with a limited number of patients, and without using the modern surgical technique compared the efficacy of both procedures. Chiselita compared 34 eyes of 17 patients where one eye underwent TB and the other DNPS, objectifying a significantly higher hypotensive effect after TB.18 However, neither surgery was performed with anti-metabolites, and DNPS did not include the implantation of a drainage device, which may have an important influence on the final results. On the other hand, Cillino et al21 analyzed both procedures in a study involving 65 eyes, where they found no significant differences between groups, even considering that no adjuvants, such as anti-metabolites or intrascleral implants, were used. In recent years, all surgeries done in our center have been performed with mitomycin C augmentation. The reported procedures without the use of antimetabolites correspond to surgeries performed mainly before 2015, before its universal use. The use of antimetabolites as adjuvants (mitomycin or 5-fluorouracil) theoretically inhibits conjunctival healing, which improves the surgical outcome and minimizes bleb-related complications. Despite this, the results did not show statistically significant differences in IOP reduction, concerning antimetabolite augmentation.
Regarding the analysis of the effects of the procedures on patient subgroups, no statistically significant differences were found in the hypotensive efficacy between different types of open-angle glaucoma, namely POAG and PEXG. Also, no significant differences were found between surgical techniques when performed isolated, or in combination with cataract surgery. A recent multicenter retrospective study involving a total of 117.697 eyes concluded that combined surgery was associated with lower reoperation rates than isolated procedures, but stand-alone procedures resulted in slightly greater IOP reduction.22
Our data did not allow the evaluation of the impact of drainage devices in DNPS, as all were done with the implantation of either Esnoper® or Aquaflow®. Nevertheless, evidence is not entirely clear regarding how much they augment the efficacy of the procedure, which has important clinical implications, because they significantly increase the cost of the surgery, which is otherwise the same as standard TB, as highlighted in the previously cited metanalysis.14
As expected, TB was associated with a higher number and severity of postoperative complications. Regarding our data, the difference between groups was statistically significant, favoring DNPS as the safer option. The most frequent postoperative complications in both groups included transitory hypotony, often accompanied by a shallow or flat anterior chamber, transitory choroidal effusion, and bleb-related complications, consisting mainly of seidel, bleb-failure, and encapsulation. All the complications registered in the DNPS group were transitory. The most serious complications were observed in the TB group, with 1 case of severe hyphema, 1 case of malignant glaucoma, and 1 case of persistent choroidal detachment. This difference in safety is corroborated in every study which compared the rate of postoperative complications between penetrating and non-penetrating techniques.14,18,21 Rulli’s metanalysis reported a higher incidence of short and long-term complications in TB, considering that deep sclerectomy seems to be a clinically reasonable compromise due to its higher safety profile.14
Success rate report, considering VA after 2 years of follow-up, showed that both procedures were associated with a significant visual improvement, with a mean VA improvement of 1.2 lines for TB and 0.8 lines for DNPS, which is explained by the fact that most cases were combined with cataract surgery.
The comparison of data and results from different studies regarding efficacy and safety is made difficult by the fact that most differ in methodology, sample size, population characteristics, follow-up time, use of intrascleral implants, and anti-metabolites. Surprisingly, studies that provide an analysis of the modern technique with the use of intrascleral devices and antimetabolites are scarce.
The limitations of this study include its retrospective design, the fact that the surgeries were performed by 5 different surgeons, the usage of antimetabolites in most, but not all surgeries, and the usage of 2 different implants in DNPS (Aquaflow®, or Esnoper®).
In conclusion, DNPS seems to be a valid and safe alternative to treat patients with open-angle glaucoma, unable to be controlled by non-invasive strategies. Although it is more difficult to perform, requires a long learning curve, and is usually more expensive, our results suggested that its IOP-lowering effect may only be marginally lower than TB, as shown by the absence of significant differences in the absolute or qualified success rates, with a definite lower risk of complications. We believe that we presented a robust sample, broader than that of most studies conducted in this area, which shows the potential efficacy of non-penetrating surgery when performed in an experienced center.
Funding
The authors received no specific funding for this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bourne R. Worldwide glaucoma through the looking glass. Br J Ophthalmol. 2006;90:253–254. doi:10.1136/bjo.2005.083527
2. Tham Y, Li X, Wong TY, et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
3. Spaeth G, Azuara-Blanco A. Surgical Management of Glaucoma: Glaucoma Filtration Surgery. in the Glaucomas: Concepts and Fundamentals. Eid T, Spaeth G eds. Lippincott Williams & Wilkins; 2000.
4. Razghinejad M, Fudemberg S, Spaeth G. The changing conceptual basis of trabeculectomy: a review of past and current surgical techniques. Surv Ophthalmol. 2012;57:1–25. doi:10.1016/j.survophthal.2011.07.005
5. Burney E, Quigley H, Robin A. Hypotony and choroidal detachment as late complications of trabeculectomy. Am J Ophthalmol. 1987;103:685–688. doi:10.1016/S0002-9394(14)74330-2
6. Cairns J. Preliminary report of a new method. Am J Ophthalmol. 1968;66:673–679. doi:10.1016/0002-9394(68)91288-9
7. Dahan E, Ravinet E, Ben-Simon G, Mermoud A. Comparison of the efficacy and longevity of nonpenetrating glaucoma surgery with and without a new, nonabsorbable hydrophilic implant. Ophthalmic Surg Lasers Imaging. 2003;34:457–463. doi:10.3928/1542-8877-20031101-05
8. Chiou A, Mermoud A, Hédiguer S. Ultrasound biomicroscopy of eyes undergoing deep sclerectomy with collagen implant. Br J Ophthalmol. 1996;50:541–544.
9. Loscos-Arenas J, Parera-Arranz A, Romera-Romera P, Castellvi-Manent J, Sabala-Llopart A, de la Cámara-Hermoso J. Deep Sclerectomy With a New Nonabsorbable Uveoscleral Implant (Esnoper-Clip): 1-Year Outcomes. J Glaucoma. 2015;24(6):421–425. doi:10.1097/IJG.0000000000000253
10. Shaarawy T, Mansouri K, Schnyder C, et al. Long-term results of deep sclerectomy with collagen implant. J Cataract Refract Surg. 2004;30(6):1225–1231. doi:10.1016/j.jcrs.2003.10.035
11. Roy, Deep Sclerectomy. in Glaucoma. Shaarawy T, eds. 945–959. Elsevier Inc; 2015.
12. Carassa R. Non-Penetrating Surgery. in Ophthalmic Surgery: Principles and Practice. Spaeth Geds. Elsevier Inc; 2011.
13. Roy S, Mermoud A. Deep Sclerectomy. Dev Ophthalmol. 2017;59:36–42.
14. Rulli E, Biagioli E, Riva I, et al. Efficacy and safety of trabeculectomy vs nonpenetrating surgical procedures: a systematic review and meta-analysis. JAMA Opthalmol. 2013;131:1573–1582. doi:10.1001/jamaophthalmol.2013.5059
15. Russo V, Scott IU, Stella A, et al. Nonpenetrating deep sclerectomy with reticulated hyaluronic acid implant versus punch trabeculectomy: a prospective clinical trial. Eur J Ophthalmol. 2008;18(5):751–757. doi:10.1177/112067210801800515
16. Cillino S, Di Pace F, Casuccio A, Cillino G, Lodato G. Deep sclerectomy versus trabeculectomy with low-dosage mitomycin C: four-year follow-up. Ophthalmologica. 2008;222:81–87. doi:10.1159/000112623
17. Ambresin A, Shaarawy T, Mermoud A. Deep sclerectomy with collagen implant in one eye compared with trabeculectomy in the other eye of the same patient. J Glaucoma. 2002;11:214–220. doi:10.1097/00061198-200206000-00009
18. Chiselita D. Non-penetrating deep sclerectomy versus trabeculectomy in primary open-angle glaucoma surgery. Eye. 2001;15:197–201. doi:10.1038/eye.2001.60
19. Sayyad F, Helal M, El-Kholify H, El-Maghraby A. Nonpenetrating deep sclerectomy versus trabeculectomy in bilateral primary open-angle glaucoma. Ophthalmology. 2000;107(9):1671–1674. doi:10.1016/S0161-6420(00)00263-3
20. Leszczyński R, Formińska-Kapuścik M, Bubała-Stachowicz B, et al. Nonpenetrating very deep sclerectomy with hyaluronic acid implant vs trabeculectomy-A 2-year follow-up. Graefes Arch Clin Exp Ophthalmol. 2012;250(12):1835–1841. doi:10.1007/s00417-012-1985-9
21. Cillino S, Di Pace F, Casuccio A. Deep sclerectomy versus punch trabeculectomy with or without phacoemulsification: a randomized clinical trial. J Glaucoma. 2004;13:500–506. doi:10.1097/01.ijg.0000137869.18156.81
22. Ciociola E, Yang S, Hall N, Lorch A, Miller W. Effectiveness of Trabeculectomy and Tube Shunt with versus without Concurrent Phacoemulsification: intelligent Research in Sight Registry Longitudinal Analysis. Ophthalmol Glaucoma. 2023;6:42–53. doi:10.1016/j.ogla.2022.07.003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Patient Tolerability of Omidenepag Isopropyl in the Treatment of Glaucoma and Ocular Hypertension
Matsuo M, Matsuoka Y, Tanito M
Clinical Ophthalmology 2022, 16:1261-1279
Published Date: 26 April 2022
Retrospective Analysis of Switching Bimatoprost 0.01% to Bimatoprost 0.03% in Patients with Various Types of Glaucoma and Ocular Hypertension
Xu KM, Cho R, Chan TYB
Clinical Ophthalmology 2022, 16:2385-2390
Published Date: 29 July 2022
Multicenter Effectiveness and Disease Stability Through 3 Years After iStentTrabecular Micro-Bypass with Phacoemulsification in Glaucoma and Ocular Hypertension
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW
Clinical Ophthalmology 2022, 16:2955-2968
Published Date: 1 September 2022
Triple Fixed-Combination Bimatoprost/Brimonidine/Timolol in Glaucoma and Ocular Hypertension in India: A Multicenter, Open-Label, Phase 3 Study
Menon MG, Goodkin ML
Clinical Ophthalmology 2022, 16:3559-3569
Published Date: 20 October 2022
Steroid Response Following Dropless Cataract Surgery Using Subconjunctival Triamcinolone
Wu AM, Pitts KM, Pineda R, Chen SH, Wang M, Johnson G, Shen LQ, Margeta MA
Clinical Ophthalmology 2023, 17:2803-2814
Published Date: 22 September 2023