Back to Journals » Clinical Ophthalmology » Volume 16
Triple Fixed-Combination Bimatoprost/Brimonidine/Timolol in Glaucoma and Ocular Hypertension in India: A Multicenter, Open-Label, Phase 3 Study
Authors Menon MG, Goodkin ML ![]()
Received 6 April 2022
Accepted for publication 22 August 2022
Published 20 October 2022 Volume 2022:16 Pages 3559—3569
DOI https://doi.org/10.2147/OPTH.S369626
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Meena G Menon,1 Margot L Goodkin2
1Glaucoma Services, Sankara Eye Hospital, Bangalore, Karnataka, India; 2Ophthalmology Clinical Development, Allergan (an AbbVie Company), Irvine, CA, USA
Correspondence: Meena G Menon, Glaucoma Services, Sankara Eye Hospital, Bangalore, Karnataka, India, Email [email protected]
Introduction: To evaluate the intraocular pressure (IOP)-lowering efficacy and safety of a triple fixed-combination of bimatoprost, brimonidine, and timolol (TFC) in patients with glaucoma or ocular hypertension (OHT) treated with fixed-combination or unfixed brimonidine and timolol therapy (dual-combination therapy).
Methods: In this multicenter, open-label, phase 3 study, patients who received 4– 8 weeks of dual-combination therapy twice daily and had an IOP > 18 and < 34 mmHg in at least one eye were switched (at baseline) to treatment with TFC twice daily for 12 weeks. At Weeks 4, 8, and 12 on TFC, IOP was assessed at Hours 0, 2, and 8. Primary efficacy variable: mean diurnal IOP change from baseline in the study eye at Week 12 (modified intent-to-treat [mITT] population). Sensitivity (per-protocol [PP] population) and subgroup (≤ 65 vs > 65 years) analyses were performed. Safety, including adverse events (AEs), was assessed at each visit.
Results: Of 126 patients enrolled, 121 and 103 formed the mITT/safety and PP populations, including 109 (90.1%) and 94 (91.3%) who completed the study, respectively. In the mITT/safety population, mean age was 58.6 years. Patients had open-angle glaucoma (51.2%), angle-closure glaucoma with patent iridotomy (36.4%), and/or OHT (13.2%). At Week 12, the mean diurnal change in IOP from dual combination-treated baseline was statistically significant (P< 0.001) with TFC in the mITT (– 3.98 mmHg) and PP (– 4.22 mmHg) populations. Results were similar at all visits, regardless of the age subgroup. The most frequent treatment-related AEs were conjunctival hyperemia (14.0%) and dry eye (4.1%); 5.8% of the patients discontinued treatment due to ocular AEs.
Conclusion: TFC offers a beneficial therapeutic alternative for patients with glaucoma or OHT whose IOP is not sufficiently controlled with dual-combination therapy. Safety and efficacy findings support those of published studies of TFC in primary open-angle glaucoma and OHT, despite differences in study designs.
Keywords: glaucoma, intraocular pressure, prostaglandin analog, alpha-agonist, beta-blocker, combination therapy
Introduction
To date, prostaglandin analogs/prostamides (PGAs) remain the most effective intraocular pressure (IOP)-lowering monotherapies for open-angle glaucoma (OAG) and ocular hypertension (OHT).1–6 Nonetheless, use of multiple medications is often required to maintain sufficient IOP lowering, and combination therapies are frequently used to achieve this goal and prevent disease progression.7 Compared with unfixed combinations, fixed combinations increase convenience, reduce costs, and improve treatment adherence, while minimizing medication washout and lowering exposure to preservatives and adverse event (AE) frequency or severity.8–11 PGA-containing dual fixed combinations have been shown to be more effective in lowering IOP than PGA monotherapies.4,12–22 Moreover, there is clinical evidence suggesting that brimonidine (an α-adrenergic agonist) has the potential to provide IOP lowering and neuroprotection.23–26
Two randomized, double-masked, multicenter, phase 3 studies of a triple fixed combination (TFC) containing bimatoprost 0.01%, brimonidine 0.15%, and timolol 0.5% (corresponding to 0.68% timolol maleate in the formulation, and referred to as “timolol 0.5%” hereafter) used twice daily in patients with primary OAG and OHT have demonstrated superiority of TFC over dual fixed-combination brimonidine 0.2%/timolol 0.5%, following washout of prior therapy.27,28 Findings have led to the approval of TFC by regulatory agencies in 5 countries (Brazil, Chile, Colombia, Ecuador, and Mexico). Thus, we hypothesized that TFC may result in additional IOP lowering beyond that of ongoing treatment without causing new, unexpected AEs in patients who were already treated with brimonidine 0.2%/timolol 0.5% dual-combination therapy (fixed or unfixed) at baseline, and who were not subjected to a washout period.
The present study, conducted in India, was designed to evaluate the efficacy and safety of TFC in patients with glaucoma or OHT who continued to have IOP above target after run-in on fixed or unfixed brimonidine 0.2%/timolol 0.5% dual-combination therapy.
Methods
Study Design
This open-label, multicenter, 12-week, phase 3 study (ClinicalTrials.gov identifier: NCT01216943) was conducted between November 29, 2010 and August 18, 2012 at 11 study centers in India.
Study Population
Eligible participants were ≥18 years of age with a diagnosis in each eye of either OHT; chronic or primary OAG; chronic angle-closure glaucoma with patent iridotomy; pseudoexfoliative glaucoma; or pigmentary glaucoma, requiring bilateral administration of IOP-lowering treatment. Additional key inclusion criteria were baseline medicated IOP >18 mmHg and <34 mmHg at Hour 0 (between 6:30 and 9:30 AM) in at least 1 eye after 4 to 8 weeks of treatment with the run-in dual-combination therapy, and best-corrected visual acuity (BCVA) 20/200 or better in both eyes.
Key exclusion criteria were as follows: known allergy, hypersensitivity, or contraindication to the study medication or any of its components; active ocular disease other than glaucoma or OHT (except chronic mild blepharitis, cataract, age-related macular degeneration, or background diabetic retinopathy, which could be enrolled at the discretion of the investigator); use of ocular PGAs within 4 weeks prior to baseline; recent or anticipated changes in therapy for chronic conditions with agents that could affect IOP; use of other ocular medications during the study (except intermittent use of artificial tears, topical decongestants or antihistamine >24 h prior to a scheduled study visit); functionally significant visual field loss or evidence of progressive visual field loss within 1 year prior to baseline; corneal abnormalities that could preclude accurate IOP readings with applanation tonometry; use of corticosteroids within defined exclusion periods prior to baseline (depending on the administration route) and through the study period; incisional surgery or laser procedure within defined exclusion periods prior to baseline (depending on the procedure); and ocular hyperemia or other active ocular surface findings ≥+0.5 at baseline.
Treatment
At the prestudy visit, all eligible patients initiated a run-in period (at least 4 and up to 8 weeks) using only the dual-combination therapy (COMBIGAN® [Allergan, an AbbVie company; North Chicago, IL, USA] or two adjunctive monotherapies of brimonidine and timolol) instilled twice daily (between 7:00–10:00 AM and 7:00–10:00 PM) in each eye. Patients who were already using fixed or unfixed brimonidine 0.2%/timolol 0.5% dual-combination therapy at the time of the prestudy visit should have taken this dual combination for at least 4 weeks before the baseline visit. Patients who were taking any other IOP-lowering medications were to discontinue all of these additional medications at the prestudy visit in order to have at least 4 weeks of run-in on dual combination alone before the baseline visit. The last dose of run-in dual-combination therapy was administered after the Hour-0 assessments at the baseline visit (Day 0). The first dose of TFC was instilled the evening of the baseline visit, after completion of the Hour-8 assessments, and then was self-administered twice daily in each eye at 12-hour intervals (as described above) for 12 weeks. On visit days, the morning dose of TFC was instilled at the site after the Hour-0 measurements.
Each study medication kit contained two multidose bottles of TFC (preserved with benzalkonium chloride [BAK] 50 ppm) representing a month’s supply.
Assessments
IOP was determined by Goldmann applanation tonometry at the prestudy visit, as well as Hours 0 (pre-instillation), 2, and 8 at baseline and Weeks 4, 8, and 12. Each IOP assessment consisted of two consecutive measurements in each eye; if the measurements differed by ≤2 mmHg, the IOP value for the given eye was the mean of both measurements. Otherwise, a third measurement was taken, and the IOP value for the given eye was the median of all three measurements. IOP was expected to be assessed at approximately the same time at each visit by the same evaluator. If it was not possible, the evaluators were to overlap (ie, examine the patient together and discuss findings) for at least one visit.
AEs were collected following standard clinical trial procedure and graded as mild, moderate, severe, or “not applicable” (for findings not graded for severity). Biomicroscopic examinations were performed without pupil dilation using a slit lamp, and assessed per a standard 5-point scale (none/0; trace/+0.5; mild/+1; moderate/+2; and severe/+3), except lens status, which was assessed for nuclear, cortical, and posterior subcapsular opacities following pupil dilation, using a 4-point scale (none/0; mild/+1; moderate/+2; and severe/+3). Specific standardized scales with pictorial or published guidelines were used for anterior chamber inflammation (which, if present, was graded based on standardized nomenclature set forth by the SUN Working Group criteria for anterior chamber cells and flare)29; the optic nerve cup/disc ratio (which was reported using the standard 0‒1.0 scale and pictorial Armaly chart provided); and conjunctival hyperemia (assessed using the Allergan Bulbar Hyperemia Grading Guide, which is based on a 5-point photographic grading scale of 0/none [normal]; +0.5/trace [trace flush, reddish pink]; +1/mild [mild flush, reddish color]; +2/moderate [bright red color]; and +3/severe [deep, bright, diffuse redness]). The study eye was the eye that met all eligibility criteria. If both eyes were eligible, the eye with the higher baseline IOP was designated as the study eye; if both eyes had the same IOP, the right eye was selected.
Safety variables included adverse events (AEs), BCVA (in Snellen, per a logarithmic chart for testing at 10 feet), and biomicroscopy findings (based on slit lamp evaluation of the lids, lid margins, conjunctiva, anterior chamber, and cornea without pupil dilation), assessed at each visit, as well as ophthalmoscopy findings (ie, observation of the lens, vitreous, and fundus for pathology through a dilated pupil) and cup/disc ratio (based on direct and indirect ophthalmoscopy) assessed at the prestudy visit, baseline, and Week 12 (after the last IOP reading).
Outcome Measures and Analyses
The primary efficacy outcome measure was the change in mean diurnal IOP from dual combination-treated baseline in the study eye at Week 12 in the modified intent-to-treat (mITT) population, ie, all patients with a baseline evaluation and at least one post-baseline efficacy evaluation. Mean diurnal IOP was the mean of the Hour 0, 2 and 8 values at each visit in the study eye. The null hypothesis was that there was no change in mean diurnal IOP from dual combination-treated baseline at Week 12 in the study eye. The alternative hypothesis was that TFC statistically significantly reduced mean diurnal IOP from the dual combination-treated baseline at Week 12 in the study eye. The null hypothesis was tested using a two-sided, one-sample Student t-test and SAS software version 9.2 (SAS Institute Inc, Cary, North Carolina). If the resulting P value was ≤0.05, the null hypothesis was to be rejected and TFC was to be deemed superior to the dual combination.
Analyses were repeated at Weeks 4 and 8 in the mITT population, and at Weeks 4, 8, and 12 in the per-protocol (PP) population, ie, mITT subset without major protocol violations. Missing data were only imputed for the mITT population, using the last-observation-carried-forward method. Safety was assessed at each visit in all treated patients (safety population). Supplemental efficacy and safety analyses were performed on patient subgroups based on age (≤65 vs >65 years).
A sample size of 120 was calculated based on a paired (one-sample) Student t-test for a mean difference, as implemented by MOT1 procedure in nQuery Advisor 6.01,30 as well as the following assumptions, which were based on primary efficacy data from two pivotal studies (NCT00332540 and NCT00332072) of dual fixed-combination bimatoprost/timolol (Ganfort; Allergan, an AbbVie company): difference of ≥1 mmHg in mean IOP change from dual combination-treated baseline after 12 weeks of TFC treatment; standard deviation (SD) value of 3.22 mmHg; one-sided significance level of 0.025; power of 0.90 to detect a mean decrease in IOP of 1 mmHg from dual combination-treated baseline; and discontinuation rate of 7%.
Results
Patient Disposition, Demographics, and Baseline Characteristics
In total, 126 patients were enrolled; 5/126 patients were excluded due to Good Clinical Practice violations at one investigational site, leaving 121/126 patients in the mITT/safety population (Figure 1). Of those 121 patients, 109 (90.1%) completed the study. Sensitivity analyses demonstrated no differences in efficacy and safety when patients from the excluded study site were included.
 |
Figure 1 Patient disposition. AE, adverse event; GCP, Good Clinical Practice; mITT, modified intent-to-treat; PP, per-protocol. |
In the mITT/safety population, mean (SD) age was 58.6 (11.4) years, 62.8% of the patients were male, and the most common diagnosis was OAG (51.2%; Table 1). In the PP population (n=103), patient disposition, demographics, and baseline characteristics were similar to those of the mITT/safety population (Figure 1 and Table 1).
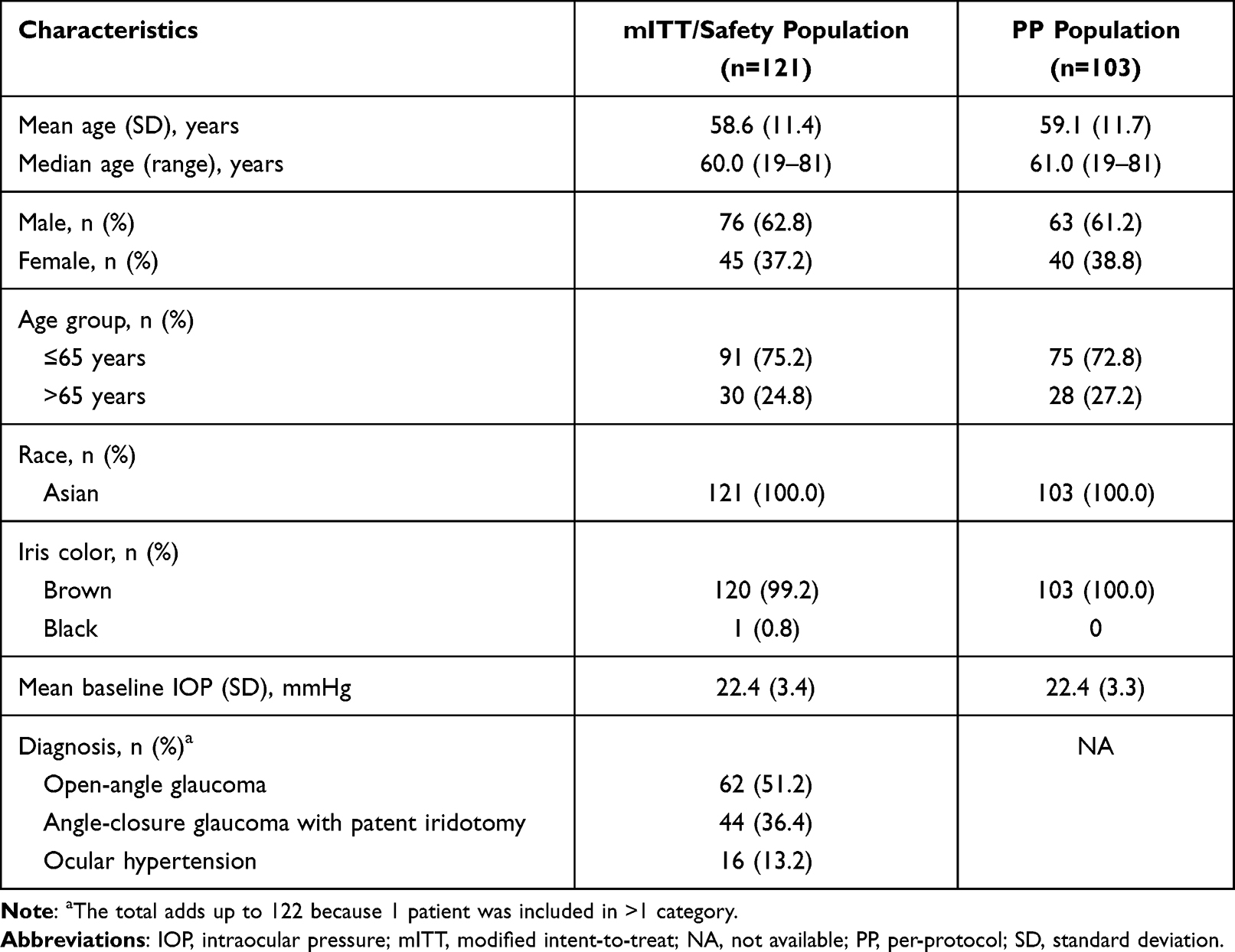 |
Table 1 Baseline Demographics and Characteristics of the mITT/Safety and PP Populations |
Treatment
In the mITT/safety population, the mean (SD) duration of treatment with TFC was 81.9 (17.9) days (range: 8–109 days).
Efficacy Analyses
At Week 12 (primary efficacy endpoint), TFC produced statistically significant IOP reductions from the already dual combination-treated baseline in both the mITT (–3.98 mmHg) and PP (–4.22 mmHg) populations (Figure 2). Mean (SD) diurnal IOP decreased from 22.4 (3.4) to 18.4 (3.7) mmHg in the mITT population, and from 22.4 (3.3) to 18.1 (3.7) mmHg in the PP population.
 |
Figure 2 Change in mean diurnal IOP from dual combination-treated baseline in the mITT and PP populations after 4, 8, and 12 weeks of treatment with TFC. P<0.001 at each visit, compared with baseline (for both populations).Abbreviations: IOP, intraocular pressure; mITT, modified intent-to-treat; PP, per-protocol; TFC, triple fixed-combination bimatoprost 0.01%/brimonidine 0.15%/timolol 0.5%. |
The change in mean diurnal IOP from the already dual combination-treated baseline was also statistically significant at Weeks 4 and 8 (Figure 2). In the mITT population, mean (SD) diurnal IOP was 17.9 (3.6) mmHg at Week 4 and 18.1 (3.7) mmHg at Week 8. In the PP population, mean (SD) diurnal IOP was 17.6 (3.4) mmHg at Week 4 and 18.3 (3.6) mmHg at Week 8. In both populations, the mean changes from baseline ranged from –4.1 to –4.6 mmHg (Figure 2). In addition, statistically significant IOP reductions from dual combination-treated baseline were observed at all follow-up visits in the mITT population stratified by age (Figure 3). In patients ≤65 years of age, mean (SD) diurnal IOP decreased from 22.5 (3.5) mmHg at baseline to 17.8 (3.8), 18.0 (3.8), and 18.4 (3.8) mmHg at Weeks 4, 8, and 12, respectively. In those >65 years of age, mean (SD) diurnal IOP decreased from 22.1 (3.1) mmHg at baseline to 18.1 (3.0), 18.4 (3.2), and 18.3 (3.5) mmHg at Weeks 4, 8, and 12, respectively. In both age subgroups, the reductions in mean diurnal IOP from dual combination-treated baseline were –3.7 mmHg or greater at all post-baseline visits (P<0.001; Figure 3).
 |
Figure 3 Change in mean diurnal IOP from dual combination-treated baseline after 4, 8, and 12 weeks of treatment with TFC, by age subgroup (mITT population). P<0.001 at each visit, compared with baseline (for both age groups).Abbreviations: IOP, intraocular pressure; mITT, modified intent-to-treat; TFC, triple fixed-combination bimatoprost 0.01%/brimonidine 0.15%/timolol 0.5%. |
Safety Analyses
Overall, 54 (44.6%) patients treated with TFC experienced ≥1 AE(s) during the study, regardless of causality. No serious AEs were reported and only 1 (0.8%) patient experienced a severe AE, glaucoma, which was deemed not treatment related. For all other AEs, the maximum severity was mild for 39 (32.2%) patients and moderate for 14 (11.6%) patients.
Ocular AEs were reported in 49 (40.5%) patients and considered treatment-related in 38 (31.4%) patients (Table 2). The most frequent treatment-related AE was conjunctival hyperemia (14.0%; Table 2). Conjunctival hyperemia was also the most frequently reported AE in the subgroups aged ≤65 years (n=15/91, 16.5%) and >65 years (n=5/30, 16.7%), regardless of causality. Overall, 7 (5.8%) patients discontinued treatment due to AEs, all of which were ocular in nature (Table 2).
 |
Table 2 Adverse Events in the Safety Population |
During the study, 9 (7.4%) patients were reported to have clinically significant biomicroscopy findings (defined as ≥2 full severity grade increase from baseline in either eye during treatment), including conjunctival hyperemia (n=7, 5.8%); conjunctival follicles (n=2, 1.7%); and n=1 each (0.8%) of eyelid erythema, meibomian gland dysfunction, and superficial punctate keratopathy. At study end, ophthalmoscopic examination revealed only 2 new findings (retinal vein occlusion [n=1] and worsening of glaucoma [n=1] reported in different patients), neither of which was considered treatment related. It is worth noting, however, that the worsening of glaucoma was reported in an eye that was on four topical IOP-lowering medication classes prior to study entry, and disease worsening could have been due to insufficient IOP-lowering efficacy in that TFC-treated eye.
Measured BCVA was unchanged in 98 of 108 patients with available data (Figure 4A), and the cup/disc ratio remained stable for all patients, except 1 (0.8%; Figure 4B) who had a worsened ratio (a ≥0.2 increase) not associated with clinical findings of increased IOP.
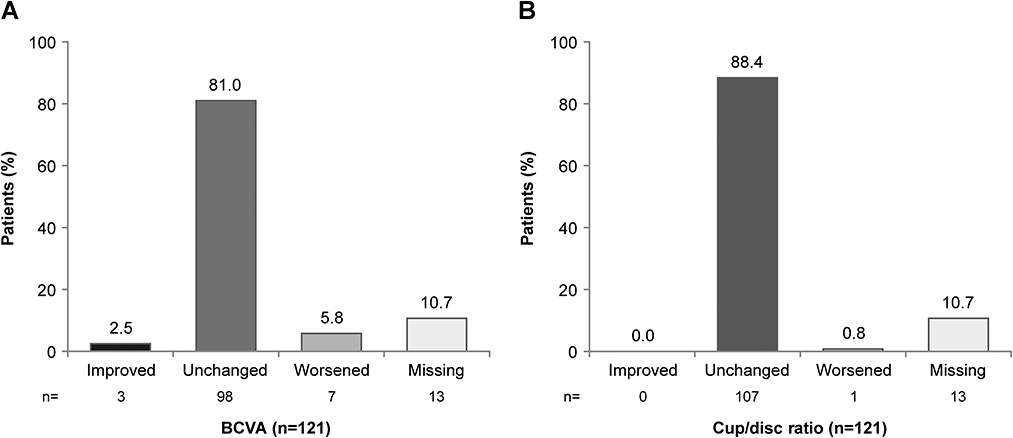 |
Figure 4 Patients with improved, unchanged, and worsened BCVA (A) or cup/disc ratio (B) from baseline after 12 weeks of treatment with TFC (mITT population). Improved and worsened BCVA were defined as increase and decrease of ≥2 lines from baseline, respectively. Improved and worsened cup/disc ratios were defined as decrease and increase of ≥0.2 from baseline, respectively.Abbreviations: BCVA, best-corrected visual acuity; mITT, modified intent-to-treat; TFC, triple fixed-combination bimatoprost 0.01%/brimonidine 0.15%/timolol 0.5%. |
Discussion
In this open-label, multicenter, phase 3 study, patients with glaucoma or OHT who continued to have IOP above target after run-in on brimonidine 0.2%/timolol 0.5% therapy (administered as a fixed combination or adjunctive monotherapies) twice daily were switched at baseline to the PGA-containing TFC treatment twice daily. Clinically meaningful and statistically significant IOP lowering from an already dual combination-treated baseline was reported at all follow-up visits. Results were similar in the mITT and PP populations, as well as the mITT population stratified by age, supporting the IOP-lowering efficacy of TFC used twice daily. TFC also had an acceptable safety/tolerability profile, consistent with that of its individual components; no additional, unexpected AEs were reported.
In the present study, 32.2% of the patients experienced treatment-related AEs with TFC administered twice daily, all mild or moderate in intensity, highlighting the favorable tolerability profile of this triple fixed combination. As expected with a triple combination containing both bimatoprost31 and brimonidine,32 conjunctival hyperemia was the most frequently reported treatment-related AE (14.0%) before and after stratification by age. It is worth noting that other, more recently approved IOP-lowering medications containing fewer (1 or 2) active components than the current triple combination were associated with higher rates of conjunctival hyperemia (≥47%12,13,33–39) than reported herein, further supporting tolerability of TFC.
These findings are clinically relevant because in the landmark Early Manifest Glaucoma Trial, the risk of glaucomatous progression was reduced by an estimated 10% for each IOP decrease of 1 mmHg.40 Moreover, the pivotal Ocular Hypertension Treatment Study has shown that many patients require >2 IOP-lowering agents to reach or maintain their target IOP,7 and yet there are very few triple-fixed combinations available.27,28,41,42 Safety and efficacy findings of this study support those of previously published studies of TFC in primary open-angle glaucoma and OHT,27,28 despite differences in study designs (ie, inclusion of a washout period27,28 or not [current study]), and further confirm that bimatoprost can be administered twice daily when low concentrations of bimatoprost (0.01%) and preservative (BAK, 50 ppm) are combined with adjunctive medications requiring twice-daily administration, as previously reported in preclinical (pharmacokinetic) and clinical evidence.43–45
Phase 3 studies of the original formulation of bimatoprost monotherapy (Lumigan 0.03%; Allergan, an AbbVie company) preserved with 50 ppm BAK have shown that twice-daily administration did not result in greater IOP lowering, compared with once-daily administration.46 After preclinical studies demonstrated that raising the concentration of BAK increased ocular bioavailability of bimatoprost,44 the currently marketed formulation of bimatoprost monotherapy (Lumigan 0.01%; Allergan, an AbbVie company) preserved with 200 ppm BAK was developed to increase tolerability with once-daily use, and was shown to be as effective as the original once-daily formulation.47 Development of TFC was based on a corollary concept implying that the drug dosing regimen/schedule could be manipulated by varying the concentrations of both bimatoprost and BAK. With low concentrations of bimatoprost (0.01%) and BAK (50 ppm) included in TFC, bimatoprost can indeed be used twice daily, consistent with the dosing regimens of the other two IOP-lowering agents included, provide the tolerability expected of the once-daily bimatoprost monotherapy,31 and substantially enhance the IOP lowering obtained with brimonidine and timolol,27,28 with the simplification in dosing regimen to use of one bottle, twice a day.
Potential limitations of the study include the open-label design. However, the study was designed to reflect real-world clinical settings, and switching all patients from their prescribed dual-combination therapy to TFC eliminated patient variation from analysis, while allowing assessment of the additional IOP-lowering enhancing effect obtained by adding bimatoprost on top of the already established efficacy of the dual combination. The fact that the IOP-lowering effect of TFC remained similar at all follow-up visits also suggests that the efficacy of TFC was not overestimated due to carry-over effects from previous treatments with dual-combination therapy. While the long-term use of TFC should be examined further in this patient population, safety after 12 months of continuous use of the TFC was previously described,27 supporting tolerability of this triple combination containing bimatoprost when used twice daily on an ongoing basis.
In summary, TFC offers a convenient, beneficial therapeutic alternative to patients with glaucoma or OHT whose IOP is not sufficiently controlled with dual-combination therapy, with the potential to enhance patient adherence to treatment and –consequently– quality of life by including all three medications in one bottle.
Medical Writing and Editorial Assistance
Medical writing and editorial assistance were provided to the authors by Michele Jacob, PhD, CMPP, of Evidence Scientific Solutions, Inc (Philadelphia, PA, USA) and funded by Allergan (an AbbVie company).
Data Sharing Statement
AbbVie is committed to responsible data sharing regarding the clinical trials we sponsor. This includes access to anonymized, individual and trial-level data (analysis data sets), as well as other information (eg, protocols and Clinical Study Reports), as long as the trials are not part of an ongoing or planned regulatory submission. This includes requests for clinical trial data for unlicensed products and indications. This clinical trial data can be requested by any qualified researchers who engage in rigorous, independent scientific research, and will be provided following review and approval of a research proposal and Statistical Analysis Plan (SAP) and execution of a Data Sharing Agreement (DSA). Data requests can be submitted at any time and the data will be accessible for 12 months, with possible extensions considered. For more information on the process, or to submit a request, visit the following link: https://www.abbvie.com/our-science/clinical-trials/clinical-trials-data-and-information-sharing/data-and-information-sharing-with-qualified-researchers.html.
Ethics Approval and Informed Consent
This study was approved by the following independent ethics committee or institutional review board at each investigational site before initiation: Bangalore Central Ethics Committee (registration number, IORG00006039; Meena Nair, Harsh Kumar); Dr. Shroff’s Charity Eye Hospital Ethics Committee (Suneeta Dubey); Ethics Committee, H.V. Desai Eye Hospital (Vidya Chelerkar); Ethics Committee Institutional Review Board, Sankara Eye Care Institutions (registration number, ECR/705/Inst/KA/2015/RR-21; Meena G Menon); Ethics Sub-Committee, Vision Research Foundation (Balekudaru Shantha); Institutional Ethics Committee for Human Research, Bombay City Eye Institute and Research Center (Rajul Parikh); Institutional Review Board, Aravind Eye Care System (Federalwide Assurances number, 00004084; Sharmila Rajendrababu); Institutional Review Board, Aravind Medical Research Foundation (Federalwide Assurances number, 00004084; Ganesh Venkataraman); and Institutional Review Board, L.V. Prasad Eye Institute (Federalwide Assurances number, 00004930; Vanitha Pathak Ray).
The study was conducted in accordance with the Good Clinical Practice guidelines, as well as the Helsinki Declaration of 1964 and its later amendments. All patients provided written informed consent before starting treatment.
Acknowledgments
We acknowledge the following institutions (researchers) for their participation in the study: Aravind Eye Hospital (Sharmila Rajendrababu), Aravind Eye Hospital Post Graduate Institute of Ophthalmology (Ganesh Venkataraman), Bombay City Eye Institute and Research Center (Rajul Parikh), Centre for Sight B-5/24 (Harsh Kumar), Chaithanya Eye Hospital & Research Institute (Meena Nair), Dr. Shroff’s Charity Eye Hospital (Suneeta Dubey), H.V. Desai Eye Hospital (Vidya Chelerkar), Sankara Eye Hospital (Meena G Menon), L.V. Prasad Eye Institute (Vanitha Pathak Ray), and Sankara Nethralaya, A Unit of Medical and Vision Research Foundation (Balekudaru Shantha).
The authors would like to thank all the patients who participated in this study, as well as Trever Todd, PhD (AbbVie Inc.), for his critical review and assistance during manuscript development. Statistical analyses were generated by SIRO Clinpharm Pvt. Ltd (Mumbai, India). This work was partially presented at the 11th European Glaucoma Society Congress (June 7–11, 2014; Nice, France).
Author Contributions
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published. Neither honoraria nor payments were made for authorship.
Funding
This study was sponsored by Allergan (prior to its acquisition by AbbVie, North Chicago, IL, USA). Allergan participated in the study design; conduct of the study; data collection, management, analysis, and interpretation; and preparation, review, and approval of the manuscript. Neither honoraria nor payments were made for authorship.
Disclosure
MLG is an employee of AbbVie Inc and may hold AbbVie stock/share options. The authors report no other conflicts of interest in this work.
References
1. American Academy of Ophthalmology. A preferred practice pattern guidelines. Primary open-angle glaucoma. American Academy of Ophthalmology. Available from: https://www.aao.org/preferred-practice-pattern/primary-open-angle-glaucoma-ppp.
2. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th edition. Br J Ophthalmol. 2021;105(Suppl 1):1–169. doi:10.1136/bjophthalmol-2021-egsguidelines
3. Inoue K, Ishida K, Tomita G, Noma H. A scoping review and network meta-analysis for efficacy and safety of glaucoma medication in Japanese patients. Jpn J Ophthalmol. 2020;64(2):103–113. doi:10.1007/s10384-019-00708-0
4. Li F, Huang W, Zhang X. Efficacy and safety of different regimens for primary open-angle glaucoma or ocular hypertension: a systematic review and network meta-analysis. Acta Ophthalmol. 2018;96(3):e277–e284. doi:10.1111/aos.13568
5. Li T, Lindsley K, Rouse B, et al. Comparative effectiveness of first-line medications for primary open-angle glaucoma: a systematic review and network meta-analysis. Ophthalmology. 2016;123(1):129–140. doi:10.1016/j.ophtha.2015.09.005
6. van der Valk R, Webers CA, Lumley T, Hendrikse F, Prins MH, Schouten JS. A network meta-analysis combined direct and indirect comparisons between glaucoma drugs to rank effectiveness in lowering intraocular pressure. J Clin Epidemiol. 2009;62(12):1279–1283. doi:10.1016/j.jclinepi.2008.04.012
7. Kass MA, Heuer DK, Higginbotham EJ, et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120(6):701–713. doi:10.1001/archopht.120.6.701
8. Higginbotham EJ. Considerations in glaucoma therapy: fixed combinations versus their component medications. Clin Ophthalmol. 2010;4:1–9.
9. Holló G, Topouzis F, Fechtner RD. Fixed-combination intraocular pressure-lowering therapy for glaucoma and ocular hypertension: advantages in clinical practice. Expert Opin Pharmacother. 2014;15(12):1737–1747. doi:10.1517/14656566.2014.936850
10. Konstas AG, Schmetterer L, Costa VP, et al. Current and emerging fixed combination therapies in glaucoma: a safety and tolerability review. Expert Opin Drug Saf. 2020;19(11):1445–1460. doi:10.1080/14740338.2020.1826928
11. Machen L, Razeghinejad R, Myers JS. Fixed-combination topical anti-hypertensive ophthalmic agents. Expert Opin Pharmacother. 2020;21(10):1269–1282. doi:10.1080/14656566.2020.1743264
12. Brubaker JW, Teymoorian S, Lewis RA, et al. One year of netarsudil and latanoprost fixed-dose combination for elevated intraocular pressure: phase 3, randomized MERCURY-1 study. Ophthalmol Glaucoma. 2020;3(5):327–338. doi:10.1016/j.ogla.2020.05.008
13. Asrani S, Bacharach J, Holland E, et al. Fixed-dose combination of netarsudil and latanoprost in ocular hypertension and open-angle glaucoma: pooled efficacy/safety analysis of phase 3 MERCURY-1 and -2. Adv Ther. 2020;37(4):1620–1631. doi:10.1007/s12325-020-01277-2
14. Liu AW, Gan LY, Yao X, Zhou J. Long-term assessment of prostaglandin analogs and timolol fixed combinations vs prostaglandin analogs monotherapy. Int J Ophthalmol. 2016;9(5):750–756. doi:10.18240/ijo.2016.05.21
15. Xing Y, Jiang FG, Li T. Fixed combination of latanoprost and timolol vs the individual components for primary open angle glaucoma and ocular hypertension: a systematic review and meta-analysis. Int J Ophthalmol. 2014;7(5):879–890. doi:10.3980/j.issn.2222-3959.2014.05.26
16. Realini T, Nguyen QH, Katz G, DuBiner H. Fixed-combination brinzolamide 1%/brimonidine 0.2% vs monotherapy with brinzolamide or brimonidine in patients with open-angle glaucoma or ocular hypertension: results of a pooled analysis of two phase 3 studies. Eye. 2013;27(7):841–847. doi:10.1038/eye.2013.83
17. Spaeth GL, Bernstein P, Caprioli J, Schiffman RM. Control of intraocular pressure and fluctuation with fixed-combination brimonidine-timolol versus brimonidine or timolol monotherapy. Am J Ophthalmol. 2011;151(1):93–99 e94. doi:10.1016/j.ajo.2010.07.024
18. Higginbotham EJ, Olander KW, Kim EE, Grunden JW, Kwok KK, Tressler CS. Fixed combination of latanoprost and timolol vs individual components for primary open-angle glaucoma or ocular hypertension: a randomized, double-masked study. Arch Ophthalmol. 2010;128(2):165–172. doi:10.1001/archophthalmol.2009.384
19. Lewis RA, Gross RL, Sall KN, Schiffman RM, Liu CC, Batoosingh AL. The safety and efficacy of bimatoprost/timolol fixed combination: a 1-year double-masked, randomized parallel comparison to its individual components in patients with glaucoma or ocular hypertension. J Glaucoma. 2010;19(6):424–426. doi:10.1097/IJG.0b013e3181bdb586
20. Sherwood MB, Craven ER, Chou C, et al. Twice-daily 0.2% brimonidine-0.5% timolol fixed-combination therapy vs monotherapy with timolol or brimonidine in patients with glaucoma or ocular hypertension: a 12-month randomized trial. Arch Ophthalmol. 2006;124(9):1230–1238. doi:10.1001/archopht.124.9.1230
21. Craven ER, Walters TR, Williams R, Chou C, Cheetham JK, Schiffman R. Brimonidine and timolol fixed-combination therapy versus monotherapy: a 3-month randomized trial in patients with glaucoma or ocular hypertension. J Ocul Pharmacol Ther. 2005;21(4):337–348. doi:10.1089/jop.2005.21.337
22. Pfeiffer N. A comparison of the fixed combination of latanoprost and timolol with its individual components. Graefes Arch Clin Exp Ophthalmol. 2002;240(11):893–899. doi:10.1007/s00417-002-0553-0
23. Ruiz Lapuente C, Ruiz Lapuente A, Link B. Influence of topical brimonidine on visual field in glaucoma. Eur J Ophthalmol. 2001;11(Suppl 2):S67–71. doi:10.1177/112067210101102S09
24. Evans DW, Hosking SL, Gherghel D, Bartlett JD. Contrast sensitivity improves after brimonidine therapy in primary open angle glaucoma: a case for neuroprotection. Br J Ophthalmol. 2003;87(12):1463–1465. doi:10.1136/bjo.87.12.1463
25. Cantor LB. Brimonidine in the treatment of glaucoma and ocular hypertension. Ther Clin Risk Manag. 2006;2(4):337–346. doi:10.2147/tcrm.2006.2.4.337
26. Sena DF, Lindsley K. Neuroprotection for treatment of glaucoma in adults. Cochrane Database Syst Rev. 2017;1(1):Cd006539. doi:10.1002/14651858.CD006539.pub4
27. Belfort R
28. Hartleben C, Parra JC, Batoosingh A, Bernstein P, Goodkin M. A masked, randomized, phase 3 comparison of triple fixed-combination bimatoprost/brimonidine/timolol versus fixed-combination brimonidine/timolol for lowering intraocular pressure. J Ophthalmol. 2017;2017:4586763. doi:10.1155/2017/4586763
29. Jabs DA, Nussenblatt RB, Rosenbaum JT; and Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140(3):509–516. doi:10.1016/j.ajo.2005.03.057
30. Elashoff J. nQuery advisor version 6.0 user’s guide; 2005. Available from: https://knowledgebase.statsols.com/s/article/nQuery-Manuals.
31. Allergan. Lumigan prescribing information; 2022. Available from: http://www.allergan.com/assets/pdf/lumigan_pi.pdf.
32. Allergan. Alphagan prescribing information; 2013. Available from: http://www.allergan.com/assets/pdf/alphaganp_pi.pdf.
33. Aerie Pharmaceuticals Inc. RHOPRESSA® highlights of prescribing information; 2017. Available from: https://rhopressa.com/assets/pdf/RHOPRESSA-Prescribing-Information.pdf.
34. Aerie Pharmaceuticals Inc. ROCKLATANTM - highlights of prescribing information; 2019. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/208259s000lbl.pdf.
35. Singh IP, Fechtner RD, Myers JS, et al. Pooled efficacy and safety profile of netarsudil ophthalmic solution 0.02% in patients with open-angle glaucoma or ocular hypertension. J Glaucoma. 2020;29(10):878–884. doi:10.1097/IJG.0000000000001634
36. Walters TR, Ahmed IIK, Lewis RA, et al. Once-daily netarsudil/latanoprost fixed-dose combination for elevated intraocular pressure in the randomized phase 3 MERCURY-2 study. Ophthalmol Glaucoma. 2019;2(5):280–289. doi:10.1016/j.ogla.2019.03.007
37. Khouri AS, Serle JB, Bacharach J, et al. Once-daily netarsudil versus twice-daily timolol in patients with elevated intraocular pressure: the randomized phase 3 ROCKET-4 study. Am J Ophthalmol. 2019;204:97–104. doi:10.1016/j.ajo.2019.03.002
38. Kahook MY, Serle JB, Mah FS, et al. Long-term safety and ocular hypotensive efficacy evaluation of netarsudil ophthalmic solution: Rho Kinase Elevated IOP Treatment Trial (ROCKET-2). Am J Ophthalmol. 2019;200:130–137. doi:10.1016/j.ajo.2019.01.003
39. Serle JB, Katz LJ, McLaurin E, et al. Two phase 3 clinical trials comparing the safety and efficacy of netarsudil to timolol in patients with elevated intraocular pressure: rho kinase elevated IOP treatment trial 1 and 2 (ROCKET-1 and ROCKET-2). Am J Ophthalmol. 2018;186:116–127. doi:10.1016/j.ajo.2017.11.019
40. Leske MC, Heijl A, Hussein M, Bengtsson B, Hyman L, Komaroff E. Factors for glaucoma progression and the effect of treatment: the early manifest glaucoma trial. Arch Ophthalmol. 2003;121(1):48–56. doi:10.1001/archopht.121.1.48
41. Baiza-Durán LM, Alvarez-Delgado J, Contreras-Rubio AY, et al. The efficacy and safety of two fixed combinations: timolol-dorzolamide-brimonidine versus timolol-dorzolamide. A prospective, randomized, double-masked, multi-center, 6-month clinical trial. Ann Ophthalmol. 2009;41(3–4):174–178.
42. García-López A, Paczka JA, Jiménez-Román J, Hartleben C. Efficacy and tolerability of fixed-combination bimatoprost/timolol versus fixed-combination dorzolamide/brimonidine/timolol in patients with primary open-angle glaucoma or ocular hypertension: a multicenter, prospective, crossover study. BMC Ophthalmol. 2014;14:161. doi:10.1186/1471-2415-14-161
43. Shen J, Goodkin ML, Tong W, Attar M. Ocular pharmacokinetics and tolerability of bimatoprost ophthalmic solutions administered once or twice daily in rabbits, and clinical dosing implications. Clin Ophthalmol. 2017;11:1761–1767. doi:10.2147/OPTH.S143428
44. European Medicines Agency. Assessment report for Lumigan; 2010. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Assessment_Report_-_Variation/human/000391/WC500074096.pdf.
45. Laibovitz RA, VanDenburgh AM, Felix C, et al. Comparison of the ocular hypotensive lipid AGN 192024 with timolol: dosing, efficacy, and safety evaluation of a novel compound for glaucoma management. Arch Ophthalmol. 2001;119(7):994–1000. doi:10.1001/archopht.119.7.994
46. Higginbotham EJ, Schuman JS, Goldberg I, et al. One-year, randomized study comparing bimatoprost and timolol in glaucoma and ocular hypertension. Arch Ophthalmol. 2002;120(10):1286–1293. doi:10.1001/archopht.120.10.1286
47. Katz LJ, Cohen JS, Batoosingh AL, Felix C, Shu V, Schiffman RM. Twelve-month, randomized, controlled trial of bimatoprost 0.01%, 0.0125%, and 0.03% in patients with glaucoma or ocular hypertension. Am J Ophthalmol. 2010;149(4):661–671 e661. doi:10.1016/j.ajo.2009.12.003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Patient Tolerability of Omidenepag Isopropyl in the Treatment of Glaucoma and Ocular Hypertension
Matsuo M, Matsuoka Y, Tanito M
Clinical Ophthalmology 2022, 16:1261-1279
Published Date: 26 April 2022
Retrospective Analysis of Switching Bimatoprost 0.01% to Bimatoprost 0.03% in Patients with Various Types of Glaucoma and Ocular Hypertension
Xu KM, Cho R, Chan TYB
Clinical Ophthalmology 2022, 16:2385-2390
Published Date: 29 July 2022
Multicenter Effectiveness and Disease Stability Through 3 Years After iStentTrabecular Micro-Bypass with Phacoemulsification in Glaucoma and Ocular Hypertension
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW
Clinical Ophthalmology 2022, 16:2955-2968
Published Date: 1 September 2022
Trabeculectomy Vs Non‐penetrating Deep Sclerectomy for the Surgical Treatment of Open-Angle Glaucoma: A Long-Term Report of 201 Eyes
Correia Barbosa R, Gonçalves R, Bastos R, Alves Pereira S, Basto R, Viana AR, Tenedório P
Clinical Ophthalmology 2023, 17:1619-1627
Published Date: 6 June 2023
Steroid Response Following Dropless Cataract Surgery Using Subconjunctival Triamcinolone
Wu AM, Pitts KM, Pineda R, Chen SH, Wang M, Johnson G, Shen LQ, Margeta MA
Clinical Ophthalmology 2023, 17:2803-2814
Published Date: 22 September 2023