Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Successful Treatment of Concurrent Bullous Pemphigoid and Psoriasis Vulgaris with Abrocitinib: A Case Report and Literature Review
Authors Hu YQ ![]() , Zhang JZ, Zhao Y
, Zhang JZ, Zhao Y
Received 15 September 2025
Accepted for publication 12 December 2025
Published 27 January 2026 Volume 2026:19 566664
DOI https://doi.org/10.2147/CCID.S566664
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michela Starace
Yu-Qing Hu, Jian-Zhong Zhang, Yan Zhao
Department of Dermatology, Peking University People’s Hospital, Beijing, People’s Republic of China
Correspondence: Yan Zhao, Department of Dermatology, Peking University People’s Hospital, No. 11 South Avenue, Xi Zhi Men Street, Xicheng District, Beijing, People’s Republic of China, Email [email protected]
Abstract: Bullous pemphigoid (BP) and psoriasis are common immune-related dermatosis. The concurrence of these two diseases is rare. The coexistence of the two conditions imposes a difficult therapeutic challenge. We reported a case of concurrence of BP and psoriasis vulgaris which was successfully treated by abrocitinib. Based on our research, abrocitinib appears to be an effective and safe therapeutic option for patients with concurrent BP and psoriasis.
Keywords: bullous pemphigoid, psoriasis, Janus kinase inhibitors, abrocitinib
Introduction
Bullous pemphigoid (BP) is a type 2 inflammatory skin disease characterized by blister, erythema and eczematous lesions with severe itching.1 Psoriasis is a chronic immune-mediated skin disorder driven by type 3 inflammation, primarily involving the IL-23/Th17 axis.2 The coexistence of the two conditions is rare and might impose a complicated immunological dysregulation. The pathogenesis of the concurrence of psoriasis and BP remains unknown and the treatment may be challenging. Herein, we report a patient with concurrent BP and psoriasis who was successfully treated with abrocitinib.
Case Report
A 58-year-old man presented with erythema, blisters, and pruritus on the trunk for over 2 months. He had plaque psoriasis for 40 years and alcoholic cirrhosis for 2 years. He had been treated with topical steroids without good response. Upon physical examination, tense blisters, bullae, erosion, exudation and crusting were found on the abdomen, while psoriatic lesions distributed on the upper limbs and hands (Figure 1). No mucosal involvement was found. The laboratory examination showed elevated direct bilirubin (7.6 μmol/L), lactic dehydrogenase (LDH, 280 U/L), carcino-embryonic antigen (CEA, 10.10 ng/mL) and total serum IgE level (404.52 IU/mL). The anti-BP180 autoantibody was positive. The antibodies to desmoglein 1 (Dsg1) and desmoglein 3 (Dsg3) were negative. Histopathology showed subepidermal blister and perivascular inflammatory infiltration of neutrophils, eosinophils and plasmocytes (Figure 2).
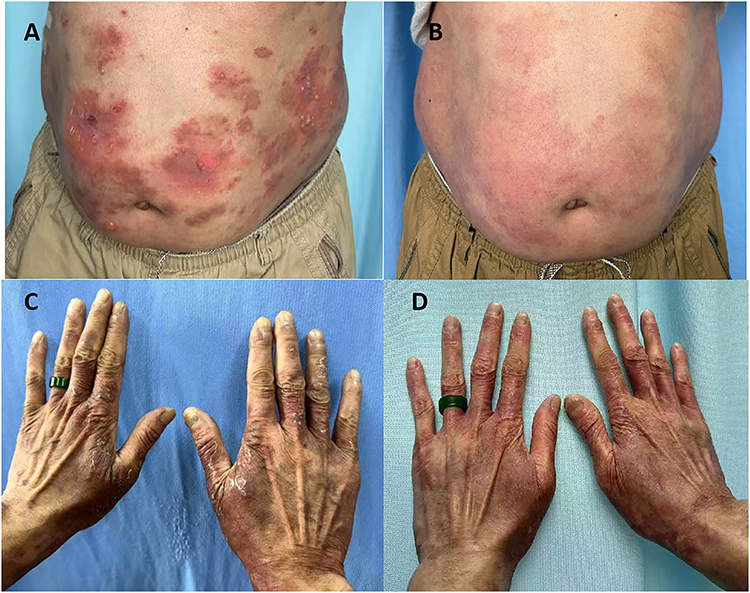 |
Figure 1 (A and B) Lesions of bullous pemphigoid on the abdomen before and after 32 weeks of treatment. (C and D) Psoriasis lesions on the back of the hands before and after 32 weeks of treatment. |
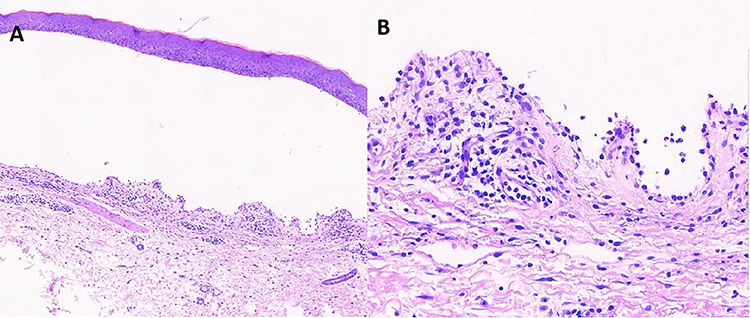 |
Figure 2 (A) Histopathology of the lesions showed subepidermal blisters (HE×40). (B) Superficial perivascular and upper interstitial infiltration of lymphocytes, neutrophils, eosinophils and plasmocytes (HE×200). |
The patient was diagnosed as BP associated with psoriasis vulgaris. Considering his complex health conditions (especially alcoholic cirrhosis) and potential adverse effects of systemic steroids, he was treated with abrocitinib 100 mg qod and topical halometasone cream. His pruritus improved within two days. After four weeks of treatment, his blisters and plaques improved significantly and no new blisters and crusts were observed. After 12 weeks treatment, his skin lesional mostly cleared and a complete remission of itching was found. After 24 weeks treatment, complete recovery was found for both BP and psoriatic lesions without any adverse effects. The patient remained in remission of BP and psoriasis at 8 months of follow-up.
Discussion
Bullous pemphigoid (BP) is regarded as a Th2 inflammatory skin disease characterized by the presence of tense blisters on erythematous skin with pruritus.3 The Janus Kinase/Signal Transducer and Activator of Transcription (JAK/STAT) pathway was found to be involved in type 2 inflammation signalings.4 Besides that, elevated expression of STAT proteins and JAK2 and JAK3 was found in BP skin lesions,5 which indicated that JAK inhibitor may be an effective treatment for BP. A literature review reported 17 patients with BP treated with JAK inhibitors and all of them showed good efficacy and safety profile.6
The coexistence of psoriasis with autoimmune bullous diseases (AIBDs), including BP, has been documented. In a retrospective analysis of 145 Japanese patients with psoriasis and AIBDs, psoriasis vulgaris was documented in 84.1% of cases and pustular psoriasis in 9% of cases, while BP was the most common AIBD (63.4%).7 The pathomechanisms underlying the association of BP and psoriasis are still unknown. A hypothesis of “epitope spreading” phenomenon was proposed. The tissue injury secondary to a primary inflammatory process (such as psoriasis) may induce the exposure of sequestered antigens, which evoke a secondary autoimmune disease such as BP.8
Abrocitinib is a high selective JAK1 inhibitor which has been approved for the treatment of atopic dermatitis (AD).9 The JAK/STAT pathway was involved in various inflammation including the downstream cytokine signaling pathway of Th1, Th2 and Th17 cells, which plays important roles in AD, BP and psoriasis.6 By downregulating the JAK/STAT pathway, JAK inhibitors have been used successfully in these diseases. Common therapeutic regimens for BP rely on systematic glucocorticoids which contradicted with the treatment of psoriasis. In recent years, several systemic JAK inhibitors have been proved to be effective in the treatment of BP coexisting with psoriasis, including upadacitinib,10 tofacitinib1 and baricitinib.11 Our study is the first report of the successful treatment of concurrent BP and psoriasis with abrocitinib, which can offer new option with good efficacy and high compliance.
Conclusion
Our study highlights the significance of JAK inhibitors in managing both psoriasis and autoimmune bullous diseases. However, this is a single case with short follow-up. Long-term efficacy and safety are still unknown. Further studies are still needed to investigate the potential mechanisms, safety and efficacy of abrocitinib for long-term use in the treatment of BP in combination with psoriasis.
Data Sharing Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding authors.
Ethics Approval Statement
The patient has provided written informed consent. The study design was approved by the Institutional Ethics Committee of Peking University People’s Hospital.
Declaration of Patient Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Institutional approval is not required for this case study.
Funding
This study was supported by National Natural Science Foundation of China (No. 82103711) and National Natural Science Foundation of Beijing (No. 7252141).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Li H, Wang H, Qiao G, Liu Y, Zhang F, Pan F. Concurrent bullous pemphigoid and psoriasis vulgaris successfully treated with Janus kinase inhibitor tofacitinib: a case report and review of the literature. Int Immunopharmacol. 2023;122:122110591. doi:10.1016/j.intimp.2023.110591
2. Man AM, Orasan MS, Hoteiuc OA, Olanescu-Vaida-Voevod MC, Mocan T. Inflammation and psoriasis: a comprehensive review. Int J Mol Sci. 2023;24(22):16095. doi:10.3390/ijms242216095
3. Fan B, Wang M. Tofacitinib in recalcitrant bullous pemphigoid: a report of seven cases. Br J Dermatol. 2023;188(3):432–4. doi:10.1093/bjd/ljac078
4. Kalantari Y, Sadeghi S, Asadi D, Goodarzi A. A literature review on Janus kinase (JAK) inhibitors for the treatment of immunobullous disorders. Int Immunopharmacol. 2022;110:108923. doi:10.1016/j.intimp.2022.108923
5. Juczynska K, Wozniacka A, Waszczykowska E, et al. Expression of the JAK/STAT signaling pathway in bullous pemphigoid and dermatitis herpetiformis. Mediators Inflamm. 2017;2017:6716419. doi:10.1155/2017/6716419
6. Lin X, Li X, Zhai Z, Zhang M. JAK-STAT pathway, type I/II cytokines, and new potential therapeutic strategy for autoimmune bullous diseases: update on pemphigus vulgaris and bullous pemphigoid. Front Immunol. 2025;16:1563286. doi:10.3389/fimmu.2025.1563286
7. Ohata C, Ishii N, Koga H, et al. Coexistence of autoimmune bullous diseases (AIBDs) and psoriasis: a series of 145 cases. J Am Acad Dermatol. 2015;73(1):50–55. doi:10.1016/j.jaad.2015.03.016
8. Phan K, Goyal S, Murrell DF. Association between bullous pemphigoid and psoriasis: systematic review and meta-analysis of case-control studies. Australas J Dermatol. 2019;60(1):23–28. doi:10.1111/ajd.12899
9. Deeks ED, Duggan S. Abrocitinib: first approval. Drugs. 2021;81(18):2149–2157. doi:10.1007/s40265-021-01638-3
10. Su F, Wang T, Qin Q, Xie Z. Upadacitinib for the management of bullous pemphigoid coexisting with psoriasis vulgaris: a case report and literature review. J DermatolTreat. 2024;35(1):2302394. doi:10.1080/09546634.2024.2302394
11. Xiao Y, Xiang H, Li W. Concurrent bullous pemphigoid and plaque psoriasis successfully treated with Janus kinase inhibitor Baricitinib. Dermatol Ther. 2022;35(10):e15754. doi:10.1111/dth.15754
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness and Safety of Deucravacitinib for the Management of Psoriasis: A Review of the Current Literature
Potestio L, Ruggiero A, Fabbrocini G, Martora F, Megna M
Psoriasis: Targets and Therapy 2023, 13:19-26
Published Date: 4 May 2023
Successful Treatment of Atopic Dermatitis with a Predominant Nipple Involvement by Abrocitinib During COVID-19 Pandemic: A Case Report
Teng Y, Tang H, Yu Y, Fan Y, Tao X, Xu D
Journal of Asthma and Allergy 2023, 16:789-792
Published Date: 1 August 2023
A Report of Eruptive Pruritic Papular Porokeratosis Treated with Abrocitinib
Xia J, Jiang G
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2223-2227
Published Date: 14 August 2023
A Case of Perioral Dermatitis Successfully Treated with Abrocitinib
Teng Y, Ren M, Ding Y, Yang X, Fan Y, Tao X
Clinical, Cosmetic and Investigational Dermatology 2023, 16:3035-3038
Published Date: 24 October 2023
Concurrent Refractory Atopic Dermatitis and Generalized Vitiligo Successfully Treated with Abrocitinib: A Case Report
Shao X, Pan X, Chen Y, Zhu Y, Chen S, Chen J
Journal of Asthma and Allergy 2024, 17:1259-1263
Published Date: 3 December 2024