Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
A Case of Perioral Dermatitis Successfully Treated with Abrocitinib
Authors Teng Y ![]() , Ren M
, Ren M ![]() , Ding Y
, Ding Y ![]() , Yang X, Fan Y, Tao X
, Yang X, Fan Y, Tao X
Received 31 August 2023
Accepted for publication 12 October 2023
Published 24 October 2023 Volume 2023:16 Pages 3035—3038
DOI https://doi.org/10.2147/CCID.S433561
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Yan Teng,1,* Mingyang Ren,2,* Yang Ding,1 Xianhong Yang,1 Yibin Fan,1 Xiaohua Tao1
1Center for Plastic & Reconstructive Surgery, Department of Dermatology, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital of Hangzhou Medical College, Hangzhou, 310014, People’s Republic of China; 2Graduate School of Clinical Medicine, Bengbu Medical School, Bengbu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaohua Tao; Yibin Fan, Center for Plastic & Reconstructive Surgery, Department of Dermatology, Zhejiang provincial people’s hospital, People’s Hospital of Hangzhou Medical College, Tel +86-13505811700 ; +86-18806538451, Email [email protected]; [email protected]
Abstract: Perioral dermatitis (POD) is a chronic inflammatory skin disease that primarily affects females between the ages of 16 and 45. Conventional therapies face the challenge of limited efficacy and a high recurrence rate. In this report, we present the case of a 26-year-old male patient with POD who was successfully treated using the Janus kinase (JAK) inhibitor, abrocitinib. This treatment exhibited both good efficacy and safety. Abrocitinib, as a JAK inhibitor, holds promise as a potential therapy for cases of POD that might be resistant to conventional therapies.
Keywords: JAK inhibitors, abrocitinib, perioral dermatitis
Introduction
The Janus kinase-signal transducer and activator of transcription (JAK-STAT) pathway plays a crucial role in various inflammatory cutaneous disorders. In 2022, the United States Food and Drug Administration approved abrocitinib, an orally administered highly selective JAK-1 inhibitor, for the treatment of refractory moderate-to-severe atopic dermatitis (AD) in adults. Abrocitinib has exhibited high efficacy and a favorable safety profile. It acts by inhibiting several inflammatory cytokines and growth factors that are mediated by the JAK-STAT pathway, which plays a pivotal role in the pathogenesis of AD. Perioral dermatitis (POD) has proven to be a challenging condition to treat, often characterized by a high recurrence rate, particularly when patients cannot avoid the use of topical corticosteroids or potential allergen exposure. In this report, we present a case of refractory POD successfully treated with abrocitinib.
Case Presentation
A 26-year-old female presented with a one-year history of grouped erythematous, scaly, follicular papules, papulovesicles, and papulopustules on the perioral region. She complained of intense pruritus accompanying these lesions, which significantly impacted her quality of life and occasionally led to sleep disturbances. Prior to developing POD, she had intermittently used cosmetics containing corticosteroids for over a year, a duration longer than the course of her disease. Common therapeutic agents, such as moisturizers, topical calcineurin inhibitors, oral tetracycline antibiotics (like doxycycline and minocycline), and hydroxychloroquine, had been tried with limited efficacy. The patients sought further management in our dermatology department (Figure 1A).
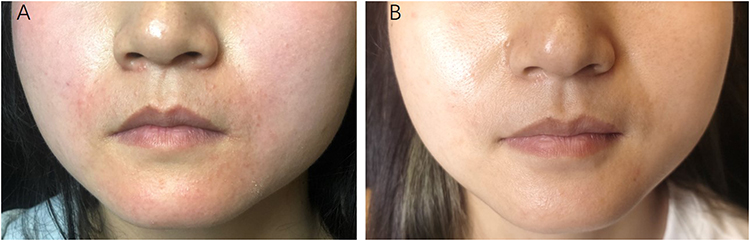 |
Figure 1 The skin lesions before and after abrocitinib therapy. (A) The skin lesions on the perioral region; (B) Two weeks after the abrocitinib therapy. |
Based on the medical history and typical clinical presentation of the patient, we diagnosed the condition as POD. Considering several crucial factors, including the progression of the disease, the ineffectiveness of the routine treatment plan, and the urgent need for relief for the patient, we decided to initiate the oral administration of abrocitinib, a selective JAK-1 inhibitor, following a comprehensive examination to rule out severe infection, coagulation disfunction, hepatic failure, renal disorders, tuberculosis, and other potential concerns. Additionally, we prescribed the patient to discontinue the use of cosmetics containing corticosteroids. Abrocitinib treatment commenced at a dosage of 100 mg per day. Remarkably, the pruritus significantly improved the following day, and after just two weeks, the perioral lesions had almost completely disappeared without any accompanying discomfort (Figure 1B). The abrocitinib therapy was discontinued after a 12-week treatment course, with no reported adverse events. Even after 12 weeks of discontinuation, there were no signs of relapse.
Discussion
POD, also known as rosacea-like dermatitis or periorificial dermatitis, is a chronic inflammatory skin condition. It is characterized by scaly erythema, often accompanied by small erythematosus papules or papulovesicular, primarily located in the perioral region but can also affect the area around the nose or eyes. This condition predominantly affects females between the ages of 16 and 45. While topical corticosteroids are a common trigger for POD, cosmetics and toothpaste containing chlorine or fluorine can also sometimes contribute to the development of the disease. The treatment of POD typically involves several approaches, including discontinuing the use of topical corticosteroids, avoiding potential allergens that can trigger or worsen POD, and medication. In cases of mild POD, topical therapies such as topical calcineurin inhibitors and topical antibiotics are preferred over systemic treatments. Systemic therapies are generally recommended for moderate-to-severe POD or cases of mild POD that do not respond to topical therapy. Commonly used agents for systemic treatment of POD include oral tetracyclines and macrolides, with the clinical use of ivermectin for POD on the rise.1 While various medications are employed as treatment options, there is no universally standardized and approved treatment regimen for POD, and treatment decisions are often based on clinical experience.2 In this report, we presented a case of a female patient with POD who exhibited a positive response to abrocitinib. We have obtained consent from the patient to publish all photographic materials.
To the best of our knowledge, we present the first case report of POD showing a positive response to abrocitinib. Abrocitinib is a highly selective JAK1 inhibitor that has received approval for the treatment of moderate and severe AD.3 It effectively inhibits numerous critical cytokine signaling pathways, including those mediated by interferon (IFN)-γ, interleukin (IL)-2, IL-4, IL-7, IL-9, IL-15, and IL-17. In addition to its use in AD, abrocitinib has demonstrated effectiveness in treating various other skin disorders, such as alopecia areata,4 plaque psoriasis,5 lichen sclerosus,6 Hailey-Hailey disease,7 necrobiosis lipoidica,8 prurigo nodularis,9 primary cutaneous lichenoid amyloidosis,10 and several others.
In our case, the treatment with abrocitinib resulted in rapid alleviation of pruritus and the complete disappearance of skin lesions after two weeks. After a 12-week follow-up period, there were no signs of recurrence or adverse events. Importantly, alongside medication, the patient completely avoided the use of cosmetics containing corticosteroids. This remarkable efficacy significantly reduced the psychological burden on the patient and allowed her to resume her daily life without being negatively impacted by the disease. One possible explanation for the successful treatment of POD with abrocitinib is its ability to alleviate inflammation by inhibiting a group of inflammatory cytokines and aiding in the restoration of the damaged skin barrier. This suggests the potential involvement of the JAK-STAT pathway in the pathogenesis of POD, although the specific role of JAK signaling in POD remains unclear. However, it is essential to note that while abrocitinib was effective in this case, its efficacy in treating POD may not be universal, and the response to other types of JAK inhibitors may vary in terms of both efficacy and safety. Long-term follow-up is necessary to further evaluate the efficacy and safety of abrocitinib for the treatment of POD and to gain a better understanding of its role in managing this condition.
Conclusion
This case suggests that the JAK-1 inhibitor, abrocitinib, could serve as a potential alternative for refractory POD that might be resistant to conventional therapies. Further studies are required to explore the precise mechanisms involved and to thoroughly assess the long-term efficacy and safety of abrocitinib in treating POD.
Ethics Statement
The publication of images was included in the patient’s consent for publication of the case. The Hospital Ethics Committees of the Affiliated People’s Hospital of Hangzhou Medical College approved publishing the case details.
Acknowledgments
We thank Bullet Edits Limited for the linguistic editing and proofreading of the manuscript. Xiaohua Tao and Yibin Fan are co-correspondence authors for this study.
Consent Statement
Informed consent was provided by the patient for publication of the case.
Funding
The research was supported by Young Talents Project of Zhejiang Medicine and Health Science and Technology Project (2022KY049).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Noguera-Morel L, Gerlero P, Torrelo A, Hernández-Martín Á. Ivermectin therapy for papulopustular rosacea and periorificial dermatitis in children: a series of 15 cases. J Am Acad Dermatol. 2017;76(3):567–570. doi:10.1016/j.jaad.2016.10.034
2. Searle T, Ali FR, Al-Niaimi F. Perioral dermatitis: diagnosis, proposed etiologies, and management. J Cosmet Dermatol. 2021;20(12):3839–3848. doi:10.1111/jocd.14060
3. Blauvelt A, Silverberg JI, Lynde CW, et al. Abrocitinib induction, randomized withdrawal, and retreatment in patients with moderate-to-severe atopic dermatitis: results from the JAK1 Atopic Dermatitis Efficacy and Safety (JADE) REGIMEN Phase 3 trial. J Am Acad Dermatol. 2022;86(1):104–112. doi:10.1016/j.jaad.2021.05.075
4. Bennett M, Moussa A, Sinclair R. Successful treatment of chronic severe alopecia areata with abrocitinib. Australas J Dermatol. 2022;63(2):274–276. doi:10.1111/ajd.13836
5. Zhang L, Guo L, Wang L, Jiang X. The efficacy and safety of tofacitinib, peficitinib, solcitinib, baricitinib, abrocitinib and deucravacitinib in plaque psoriasis - A network meta-analysis. J Eur Acad Dermatol Venereol. 2022;36(11):1937–1946. doi:10.1111/jdv.18263
6. Bao C, Xu Q, Xiao Z, et al. Abrocitinib as a novel treatment for lichen sclerosus. Br J Dermatol. 2023;189(1):136–138. doi:10.1093/bjd/ljad129
7. Li Y, Jiang Y, Sun J. Improvement of Hailey-Hailey disease with abrocitinib. Clin Exp Dermatol. 2023;48(5):532–533. doi:10.1093/ced/llad023
8. Arnet L, Erfurt-Berge C. Effect of abrocitinib in a patient with extensive necrobiosis lipoidica. J Eur Acad Dermatol Venereol. 2023;37(10). doi:10.1111/jdv.19189
9. Vander Does A, Yosipovitch G. Failure of dupilimab with severe prurigo nodularis that responded well to abrocitinib. Dermatitis. 2023. doi:10.1089/derm.2022.0065
10. Bai J, Su W, Fang H, Qiao J. Treatment of primary cutaneous lichenoid amyloidosis with abrocitinib: a pilot study in two cases. Int J Dermatol. 2023;62(9). doi:10.1111/ijd.16698
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Successful Treatment of Atopic Dermatitis with a Predominant Nipple Involvement by Abrocitinib During COVID-19 Pandemic: A Case Report
Teng Y, Tang H, Yu Y, Fan Y, Tao X, Xu D
Journal of Asthma and Allergy 2023, 16:789-792
Published Date: 1 August 2023
A Report of Eruptive Pruritic Papular Porokeratosis Treated with Abrocitinib
Xia J, Jiang G
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2223-2227
Published Date: 14 August 2023
Concurrent Refractory Atopic Dermatitis and Generalized Vitiligo Successfully Treated with Abrocitinib: A Case Report
Shao X, Pan X, Chen Y, Zhu Y, Chen S, Chen J
Journal of Asthma and Allergy 2024, 17:1259-1263
Published Date: 3 December 2024
Abrocitinib for Head and Neck Dermatitis: Case Series and Literature Review
Liu C, Pan Y, Xiong J, Saputra AD, Chen S, Cai T
Clinical, Cosmetic and Investigational Dermatology 2025, 18:3093-3102
Published Date: 20 November 2025
Successful Treatment of Concurrent Bullous Pemphigoid and Psoriasis Vulgaris with Abrocitinib: A Case Report and Literature Review
Hu YQ, Zhang JZ, Zhao Y
Clinical, Cosmetic and Investigational Dermatology 2026, 19:566664
Published Date: 27 January 2026